NEURAL REGENERATION RESEARCH
自然科学核心期刊A类、B类、C类(2016年适用)

内江师范学院自然科学技术类核心期刊目录(使用时间:2016年1月1日-2016年12月31日)一、A类1.Acta Mathematica Scientia2.Journal of Computer Science and Technology3.Chinese Physics Letters Communications in Theoretical Physics4.Chinese Optics Letters5.Acta Mechanica Sinica6.Chinese Chemical Letters7.Rare Metals8.Acta Pharmacologica Sinica9.Journal of Integrative Plant Biology10.Acta Biochimica et Biophysica Sinica11.Cell Research12.Biomedical and Environmental Sciences13.Journal of Environmental Sciences-China14.中国激光15.高能物理与核物理16.应用数学学报17.红外与毫米波学报18.力学学报19.数学年刊20.电子学报21.通信学报22.自动化学报23.化学学报24.高分子学报25.物理化学学报26.无机化学学报27.科学通报28.分析化学29.催化学报30.化工学报31.金属学报32.无机材料学报33.稀有金属材料与工程34.计算机学报35.软件学报36.药学学报37.中国科学38.动物学报39.微生物学报40.中国生物化学与分子生物学报41.物理学报42.遗传学报43.数学学报44.光学学报45.水生生物学报46.生理学报47.食品科学48.营养学报49.中国环境科学50.生态学报51.环境科学学报52.环境科学53.系统工程学报54.地理学报55.地球物理学报56.水利学报57.中国农业科学二、B类1.《半导体学报》2.《兵工学报》3.《病毒学报》4.《材料研究学报》5.《草业学报》6.《测绘学报》7.《城市规划》8.《大气科学》9.《地理科学》10.《地理研究》11.《地震学报》12.《第四纪研究》13.《地质论评》14.《地质学报》15.《电子显微学报》16.《动物分类学报》17.《纺织学报》18.《分析测试学报》19.《作物学报》20.《复合材料学报》21.《高等学校化学学报》22.《工程热物理学报》23.《古生物学报》24.《固体力学学报》25.《光谱学与光谱分析》26.《光子学报》27.《硅酸盐学报》28.《海洋与湖沼》29.《海洋学报》30.《焊接学报》31.《航空动力学报》32.《航空学报》33.《核农学报》34.《环境化学》35.《机械工程学报》36.《计量学报》37.《计算机研究与发展》38.《计算机与应用化学》39.《计算数学》40.《计算物理》41.《建筑结构学报》42.《结构化学》43.《解剖学报》44.《经济地理》45.《空气动力学学报》46.《昆虫学报》47.《林业科学》48.《林业科学研究》49.《煤炭学报》50.《摩擦学学报》51.《模式识别与人工智能》 52.《农业工程学报》 53.《农业机械学报》 54.《气象学报》55.《生物化学与生物物理进展》 56.《生物化学与生物物理学报》 57.《声学学报》 58.《石油学报》 59.《实验生物学报》 60.《兽类学报》 61.《数学进展》 62.《数学物理学报》 63.《数学研究与评论》64.《数值计算与计算机应用》 65.《水产学报》 66.《水科学进展》 67.《水土保持学报》 68.《太阳能学报》 69.《天文学报》 71.《铁道学报》 72.《土木工程学报》 73.《土壤学报》74.《系统科学与数学》 75.《畜牧兽医学报》 76.《岩石学报》 77.《遥感学报》 78.《仪器仪表学报》 79.《应用化学》 80.《应用生态学报》 81.《应用数学和力学》 82.《有机化学》 83.《宇航学报》 84.《园艺学报》 85.《云南植物研究》 86.《植物保护学报》 87.《植物病理学报》88.《植物分类学报》89.《植物生理与分子生物学学报》 90.《植物生态学报》 91.《植物学报》92.《中国电机工程学报》 93.《中国公路学报》94.《中国寄生虫学与寄生虫病杂志》 95.《中国免疫学杂志》 96.《中国生物医学工程学报》 97.《中国中西医结合杂志》 98.《中国中药杂志》 99.《中华病理学杂志》 100.《中华传染病杂志》 101.《中华儿科杂志》102.《中华耳鼻咽喉科杂志》 103.《中华放射学杂志》 104.《中华妇产科杂志》105.《中华结核和呼吸杂志》 106.《中华口腔医学杂志》 107.《中华老年医学杂志》 108.《中华流行病学杂志》 109.《中华内科杂志》 110.《中华皮肤科杂志》 111.《中华外科杂志》 112.《中华消化杂志》113.《中华心血管病杂志》 114.《中华血液学杂志》 115.《中华眼科杂志》 116.《中华医学杂志》117.《中华预防医学杂志》 118.《中华肿瘤杂志》 119.《自然灾害学报》 120.《自然资源学报》 121. 《清华大学学报》(自) 122. 《北京大学学报》(自)三、C 类Acta Automatica Sinica1874-1029 CActa Geologica Sinica1000-9515 CActa Mathematica Sinica. English Series 1439-8516 C Acta Mathematicae Applicatae Sinica 0168-9673 C Acta Mechanica Solida Sinica0894-9166 CActa Metallurgica Sinica(English Letters) 1006-7191 C Acta Pharmaceutica Sinica B2211-3835 CActa Pharmacologica Sinica Advances in Atmospheric Sciences Advances in Climate Change Research Advances in Manufacturing Algebra Colloquium Analysis in Theory and Applications Applied GeophysicsApplied Mathematics and Mechanics0253-4827 C Applied Mathematics. Series B, A Journal of C 1005-1031 C Asian Herpetological Research 2095-0357 C Asian Journal of Andrology1008-682X C Atmospheric and Oceanic Science Letters 1674-2834 CAvian Research 1674-7674 CBone Research2095-4700 CBuilding Simulation1996-3599 CCancer Biology and Medicine2095-3941 CCellular & Molecular Immunology1672-7681 CChemical Research in Chinese Universities 1005-9040 C China City Planning Review 1002-8447 CChina Communications 1673-5447 CChina Ocean Engineering0890-5487 CChinese Annals of Mathematics. Series B 0252-9599 C Chinese Geographical Science 1002-0063 CChinese Journal of Acoustics 0217-9776 C Chinese Journal of Aeronautics1000-9361 CChinese Journal of Biomedical Engineering 1004-0552 CChinese Journal of Cancer1000-467X C Chinese Journal of Cancer Research1000-9604 CChinese Journal of Chemical Engineering 1004-9541 CChinese Journal of Chemical Physics 1674-0068 CChinese Journal of Chemistry 1001-604X C Chinese Journal of Electronics 1022-4653 C Chinese Journal of Geochemistry1000-9426 CChinese Journal of Integrative Medicine 1672-0415 CChinese Journal of Mechanical Engineering 1000-9345 CChinese Journal of Natural Medicines 1875-5364 CChinese Journal of Oceanology and Limnology 0254-4059 C Chinese Journal of Polymer Science0256-7679 C Chinese Journal of Structural Chemistry 0254-5861 CChinese Journal of Traumatology 1008-1275 CChinese Medical Journal0366-6999 CChinese Medical Sciences Journal 1001-9294 CChinese Physics Letters 0256-307X CChinese Physics. B 1674-1056 C Chinese Physics. C1674-1137 CCommunications in Mathematical Research 1674-5647 CCommunications in Theoretical Physics 0253-6102 CControl Theory and Technology 2095-6983 CCurrent Zoology 1674-5507 C Defence Technology2214-9147 CEarthquake Engineering and Engineering Vibration 1671-3664 CEarthquake Research in China 0891-4176 CEarthquake Science1674-4519 CEntomotaxonomia Forest Ecosystems Friction Frontiers in Biology Frontiers in Energy Frontiers of Architectural Research Frontiers of Chemical Science and Engineering Frontiers of Computer Science Frontiers of Earth Science Frontiers of Environmental Science & Engineering Frontiers of Information Technology & Electronic Engineering Frontiers of Materials Science Frontiers of Mathematics in China Frontiers of Mechanical Engineering Frontiers of Medicine Frontiers of Optoelectronics Frontiers of Physics Frontiers of Structural and Civil Engineering Genomics, Proteomics & Bioinformatics Geoscience Frontiers Geo-spatial Information Science Hepatobiliary & Pancreatic Diseases International High Power Laser Science and Engineering Insect Science Integrative Zoology International Journal of Automation and Computing International Journal of Digital Earth International Journal of Disaster Risk Science International Journal of Minerals, Metallurgy and MaterialsInternational Journal of Mining Science and Technology International Journal of Oral Science International Soil and Water Conservation Research Journal of Acupuncture and Tuina Science Journal of Advanced Ceramics Journal of Animal Science and Biotechnology Journal of Arid Land Journal of Bionic Engineering Journal of Central South University of Technology Journal of Chinese Pharmaceutical Sciences Journal of Computational Mathematics Journal of Earth Science Journal of Electronic Science and Technology Journal of Energy Chemistry Journal of Environmental SciencesJournal of Forestry Research 1007-662X C Journal of Genetics and Genomics 1673-8527 CJournal of Geographical Sciences 1009-637X CJournal of Geriatric Cardiology 1671-5411 C Journal of Hydrodynamics1001-6058 C Journal of Integrative Agriculture 2095-3119 CJournal of Integrative Medicine2095-4964 C Journal of Iron and Steel Research, International 1006-706X C Journal of Marine Science and Application1671-9433 C Journal of Materials Science & Technology 1005-0302 CJournal of Mathematical Research with Applications 2095-2651 CJournal of Measurement Science and Instrument 1674-8042 CJournal of Meteorological Research 2095-6037 CJournal of Molecular Cell Biology 1674-2788 CJournal of Mountain Science 1672-6316 CJournal of Otology1672-2930 C Journal of Palaeogeography2095-3836 CJournal of Partial Differential Equations 1000-940X CJournal of Pharmaceutical Analysis 1671-8267 C Journal of Plant Ecology 1752-9921 CJournal of Rare Earths1002-0721 CJournal of Reproduction and Contraception 1001-7844 C Journal of Resources and Ecology1674-764X C Journal of Rock Mechanics and Geotechnical Engineering 1674-7755 C Journal of Semiconductors1674-4926 C Journal of Systematics and Evolution 1674-4918 C Journal of Systems Engineering and Electronics 1004-4132 C Journal of Systems Science and Complexity 1009-6124 C Journal of Systems Science and Information 1478-9906 C Journal of Systems Science and Systems Engineering 1004-3756 C Journal of the Operations Research Society of China 2194-668X C Journal of Thermal Science1003-2169 C Journal of Traditional Chinese Medicine 0255-2922 C Journal of Zhejiang University. Science A1673-565X C Journal of Zhejiang University. Science B 1673-1581 C Landscape Architecture Frontiers 2095-5405 C Light:Science & Applications 2095-5545 C Molecular Plant 1674-2052 C Nano Research1998-0124 C National Science Review2095-5138 C Neural Regeneration Research 1673-5374 C Neuroscience Bulletin1673-7067 C Nuclear Science and Techniques1001-8042 C Numerical Mathematics Theory, Methods and Applications 1004-8979 C Particuology 1674-2001 C Pedosphere1002-0160 C Petroleum Science Photonic Sensors Plasma Science & Technology Progress in Natural Science: Materials International Protein & Cell Quantitative Biology Research in Astronomy and Astrophysics Rice Science Science Bulletin Science China. Chemistry Science China. Earth Sciences Science China. Information Sciences Science China. Life Sciences Science China. Mathematics Science China. Physics, Mechanics & Astronomy Science China. Technological Sciences Science China. Materials Sciences in Cold and Arid Regions Shanghai Archives of Psychiatry The Crop Journal The Journal of Biomedical Research The Journal of China Universities of Posts and Telecommunications Theoretical and Applied Mechanics Letters Transactions of Nanjing University of Aeronautics and Astronautics Transactions of Nonferrous Metals Society of China Tsinghua Science and Technology Virologica Sinica Water Science and Engineering World Journal of Acupuncture-Moxibustion World Journal of Pediatrics Wuhan University Journal of Natural Sciences Zoological Research Zoological Systematics 安全与环境学报 爆炸与冲击北京大学学报. 医学版 北京航空航天大学学报 北京化工大学学报. 自然科学版 北京科技大学学报 北京理工大学学报 北京林业大学学报 北京师范大学学报. 自然科学版 北京邮电大学学报北京中医药大学学报冰川冻土1000-0240 C 兵器材料科学与工程 1004-244X C 材料保护 1001-1560 C 材料导报 1005-023X C 材料工程1001-4381 C 材料科学与工程学报 1673-2812 C 材料科学与工艺 1005-0299 C 材料热处理学报 1009-6264 C 草地学报 1007-0435 C 草业科学 1001-0629 C 测绘科学1009-2307 C 测绘科学技术学报 1673-6338 C 测绘通报 0494-0911 C 茶叶科学 1000-369X C 沉积学报1000-0550 C 成都理工大学学报. 自然科学版 1671-9727 C 传感技术学报 1004-1699 C 船舶力学1007-7294 C 大地测量与地球动力学 1671-5942 C 大地构造与成矿学 1001-1552 C 大连理工大学学报 1000-8608 C 弹道学报 1004-499X C 地层学杂志 0253-4959 C 地理科学进展1007-6301 C 地理与地理信息科学 1672-0504 C 地球化学 0379-1726 C 地球科学 1000-2383 C 地球科学进展 1001-8166 C 地球物理学进展 1004-2903 C 地球信息科学学报 1560-8999 C 地球学报 1006-3021 C 地球与环境1672-9250 C 地下空间与工程学报 1673-0836 C 地学前缘 1005-2321 C 地震1000-3274 C 地震地质 0253-4967 C 地震工程学报1000-0844 C 地震工程与工程振动 1000-1301 C 地质科技情报 1000-7849 C 地质科学 0563-5020 C 地质力学学报 1006-6616 C 地质通报1671-2552 C 第二军医大学学报 0258-879X C 第三军医大学学报 1000-5404 C 电波科学学报 1005-0388 C 电工技术学报1000-6753 C电机与控制学报 电力系统及其自动化学报 电力系统自动化 电网技术 电子测量与仪器学报 电子科技大学学报 电子与信息学报 东北大学学报. 自然科学版 东华大学学报. 自然科学版 东南大学学报. 自然科学版 动力工程学报 动物学杂志 动物营养学报 发光学报 防灾减灾工程学报 飞行力学 飞行器测控学报 非金属矿 分析科学学报 分析试验室 分子催化 分子植物育种 辐射防护 辐射研究与辐射工艺学报 腐蚀科学与防护技术 复旦学报. 医学版 复旦学报. 自然科学版 复杂系统与复杂性科学 干旱地区农业研究 干旱区地理 干旱区研究 钢铁 钢铁研究学报 高等学校计算数学学报 高电压技术 高分子材料科学与工程 高分子通报 高校地质学报 高校化学工程学报 高校应用数学学报. A 辑 高压物理学报 高原气象 工程地质学报 工程力学 工程设计学报 工程数学学报公路交通科技 1002-0268 C 功能高分子学报 1008-9357 C 古地理学报 1671-1505 C 古脊椎动物学报 1000-3118 C 固体火箭技术 1006-2793 C 光电工程 1003-501X C 光电子·激光 1005-0086 C 光学技术 1002-1582 C 光学精密工程 1004-924X C 硅酸盐通报1001-1625 C 国防科技大学学报 1001-2486 C 国际药学研究杂志 1674-0440 C 国土资源遥感 1001-070X C 果树学报 1009-9980 C 过程工程学报1009-606X C 哈尔滨工程大学学报 1006-7043 C 哈尔滨工业大学学报 0367-6234 C 海洋地质与第四纪地质 0256-1492 C 海洋湖沼通报 1003-6482 C 海洋环境科学 1007-6336 C 海洋科学进展 1671-6647 C 海洋通报 1001-6392 C 海洋渔业 1004-2490 C 含能材料 1006-9941 C 航空材料学报 1005-5053 C 航天控制1006-3242 C 航天医学与医学工程1002-0837 C 河海大学学报. 自然科学版 1000-1980 C 核动力工程0258-0926 C 核化学与放射化学 0253-9950 C 核技术0253-3219 C 核聚变与等离子体物理 0254-6086 C 核科学与工程 0258-0918 C 红外技术1001-8891 C 红外与激光工程 1007-2276 C 湖泊科学1003-5427 C 湖南大学学报. 自然科学版 1674-2974 C 湖南农业大学学报. 自然科学版 1007-1032 C 华北农学报1000-7091 C 华东理工大学学报. 自然科学版 1006-3080 C 华东师范大学学报. 自然科学版 1000-5641 C 华南理工大学学报. 自然科学版 1000-565X C 华南农业大学学报 1001-411X C 华西口腔医学杂志 1000-1182 C 华西药学杂志1006-0103 C 华中科技大学学报. 自然科学版1671-4512 C 华中农业大学学报 化工进展 化工新型材料 化学工程 化学进展 化学通报 环境工程学报 环境科学研究 环境科学与技术 环境污染与防治 火炸药学报 机器人 机械科学与技术 机械设计 基础医学与临床 基因组学与应用生物学 激光与光电子学进展 激光与红外 吉林大学学报. 地球科学版 吉林大学学报. 工学版 吉林大学学报. 理学版 极地研究 计算机辅助设计与图形学学报 计算机工程与科学 计算机集成制造系统 计算机科学与探索 计算力学学报 建筑材料学报 交通运输工程学报 交通运输系统工程与信息 解放军医学杂志 介入放射学杂志 金属热处理 精细化工 军事医学 菌物学报 空间科学学报 空间控制技术与应用 控制工程 控制理论与应用 控制与决策 矿床地质 矿物学报 矿物岩石 矿物岩石地球化学通报 兰州大学学报. 自然科学版离子交换与吸附 1001-5493 C 力学进展1000-0992 C 林产化学与工业 0253-2417 C 临床儿科杂志 1000-3606 C 临床放射学杂志 1001-9324 C 临床麻醉学杂志1004-5805 C 临床与实验病理学杂志 1001-7399 C 麦类作物学报 1009-1041 C 煤炭转化 1004-4248 C 密码学报 2095-7025 C 棉花学报 1002-7807 C 免疫学杂志 1000-8861 C 模糊系统与数学 1001-7402 C 膜科学与技术 1007-8924 C 南方水产科学 2095-0780 C 南方医科大学学报1673-4254 C 南京大学学报. 自然科学版 0469-5097 C 南京航空航天大学学报1005-2615 C 南京理工大学学报. 自然科学版 1005-9830 C 南京林业大学学报. 自然科学版 1000-2006 C 南京农业大学学报1000-2030 C 南开大学学报. 自然科学版 0465-7942 C 内燃机工程 1000-0925 C 内燃机学报 1000-0909 C 泥沙研究 0468-155X C 农药学学报1008-7303 C 农业环境科学学报 1672-2043 C 农业生物技术学报 1674-7968 C 气候变化研究进展 1673-1719 C 气候与环境研究 1006-9585 C 汽车工程1000-680X C 强激光与粒子束 1001-4322 C 燃料化学学报 0253-2409 C 燃烧科学与技术 1006-8740 C 热带海洋学报 1009-5470 C 热带气象学报1004-4965 C 热带亚热带植物学报 1005-3395 C 热固性树脂 1002-7432 C 人工晶体学报 1000-985X C 人类学学报 1000-3193 C 色谱1000-8713 C 厦门大学学报. 自然科学版 0438-0479 C 山地学报1008-2786 C 山东大学学报. 理学版1671-9352 C 陕西师范大学学报. 自然科学版 1672-4291 C 上海交通大学学报1006-2467 C上海交通大学学报. 医学版 肾脏病与透析肾移植杂志 生理科学进展 生态毒理学报 生态环境学报 生态学杂志 生态与农村环境学报 生物多样性 生物工程学报 生物物理学报 生物医学工程学杂志 湿地科学 石油地球物理勘探 石油化工 石油勘探与开发 石油实验地质 石油天然气学报 石油物探 石油学报. 石油加工 石油与天然气地质 实验力学 实验流体力学 实用口腔医学杂志 食品与发酵工业 食品与机械 食品与生物技术学报 食用菌学报 世界地震工程 数据采集与处理 数学年刊. A 辑 水动力学研究与进展. A 辑 水力发电学报 水利水电科技进展 水文地质工程地质 四川大学学报. 工程科学版 四川大学学报. 医学版 四川大学学报. 自然科学版 塑料工业 塑性工程学报 探测与控制学报 天津大学学报. 自然科学与工程技术版 天然产物研究与开发 天然气地球科学 天然气工业 天文学进展 天文研究与技术同济大学学报. 自然科学版 0253-374X C 土木建筑与环境工程 1674-4764 C 土壤0253-9829 C 土壤通报 0564-3945 C 推进技术 1001-4055 C 微波学报 1005-6122 C 微生物学通报 0253-2654 C 微体古生物学报 1000-0674 C 卫生研究1000-8020 C 武汉大学学报. 理学版 1671-8836 C 武汉大学学报. 信息科学版 1671-8860 C 物理学进展1000-0542 C 西安电子科技大学学报1001-2400 C 西安建筑科技大学学报. 自然科学版 1006-7930 C 西安交通大学学报0253-987X C 西北大学学报. 自然科学版 1000-274X C 西北工业大学学报1000-2758 C 西北农林科技大学学报. 自然科学版 1671-9387 C 西北植物学报 1000-4025 C 西南交通大学学报0258-2724 C 西南石油大学学报. 自然科学版 1674-5086 C 稀有金属 0258-7076 C 系统仿真学报 1004-731X C 系统工程1001-4098 C 系统工程理论与实践 1000-6788 C 系统工程与电子技术 1001-506X C 细胞与分子免疫学杂志 1007-8738 C 纤维素科学与技术 1004-8405 C 现代地质 1000-8527 C 现代化工0253-4320 C 小型微型计算机系统 1000-1220 C 心理科学 1671-6981 C 心理科学进展 1671-3710 C 心理学报 0439-755X C 新疆石油地质 1001-3873 C 新型炭材料 1007-8827 C 信号处理 1003-0530 C 信息与控制 1002-0411 C 烟草科技 1002-0861 C 岩矿测试0254-5357 C 岩石矿物学杂志 1000-6524 C 岩石力学与工程学报 1000-6915 C 岩土工程学报 1000-4548 C 岩土力学 1000-7598 C 岩性油气藏 1673-8926 C 眼科1004-4469 C遥感技术与应用 遥感信息 药物分析杂志 冶金分析 医用生物力学 遗传 影像科学与光化学 应用光学 应用基础与工程科学学报 应用科学学报 应用昆虫学报 应用力学学报 应用气象学报 应用与环境生物学报 油气藏评价与开发 油气地质与采收率 有色金属工程 渔业科学进展 宇航材料工艺 原子核物理评论 原子能科学技术 原子与分子物理学报 云南大学学报. 自然科学版 运筹学学报 运筹与管理 杂交水稻 载人航天 长安大学学报. 自然科学版 长江流域资源与环境 浙江大学学报. 工学版 浙江大学学报. 理学版 浙江大学学报. 农业与生命科学版 浙江大学学报. 医学版 浙江农林大学学报 浙江农业学报 针刺研究 振动、测试与诊断 振动工程学报 振动与冲击 植物分类与资源学报 植物科学学报 植物研究 植物遗传资源学报 植物营养与肥料学报 植物资源与环境学报 质谱学报智能系统学报 1673-4785 C 中草药0253-2670 C 中国癌症杂志 1007-3639 C 中国安全科学学报1003-3033 C 中国安全生产科学技术 1673-193X C 中国表面工程 1007-9289 C 中国病理生理杂志 1000-4718 C 中国草地学报 1673-5021 C 中国超声医学杂志 1002-0101 C 中国当代儿科杂志 1008-8830 C 中国地质 1000-3657 C 中国肺癌杂志1009-3419 C 中国腐蚀与防护学报 1005-4537 C 中国感染与化疗杂志 1009-7708 C 中国给水排水 1000-4602 C 中国骨质疏松杂志 1006-7108 C 中国惯性技术学报1005-6734 C 中国海洋大学学报. 自然科学版 1672-5174 C 中国海洋药物 1002-3461 C 中国环境监测 1002-6002 C 中国机械工程 1004-132X C 中国急救医学 1002-1949 C 中国脊柱脊髓杂志 1004-406X C 中国矫形外科杂志1005-8478 C 中国介入影像与治疗学 1672-8475 C 中国康复理论与实践 1006-9771 C 中国康复医学杂志1001-1242 C 中国科学技术大学学报 0253-2778 C 中国科学院大学学报 2095-6134 C 中国科学院院刊 1000-3045 C 中国空间科学技术1000-758X C 中国矿业大学学报. 自然科学版 1000-1964 C 中国粮油学报1003-0174 C 中国临床解剖学杂志 1001-165X C 中国临床心理学杂志 1005-3611 C 中国临床药理学与治疗学 1009-2501 C 中国临床药理学杂志 1001-6821 C 中国脑血管病杂志 1672-5921 C 中国农业大学学报 1007-4333 C 中国农业气象1000-6362 C 中国人口·资源与环境 1002-2104 C 中国人兽共患病学报 1002-2694 C 中国沙漠1000-694X C 中国神经精神疾病杂志 1002-0152 C 中国生态农业学报 1671-3990 C 中国生物防治学报2095-039X C中国生物工程杂志 中国石油大学学报. 自然科学版 中国实验血液学杂志 中国实用妇科与产科杂志 中国实用内科杂志 中国实用外科杂志 中国食品学报 中国兽医科学 中国水产科学 中国水稻科学 中国水土保持科学 中国塑料 中国糖尿病杂志 中国疼痛医学杂志 中国铁道科学 中国图象图形学报 中国土壤与肥料 中国微创外科杂志 中国稀土学报 中国细胞生物学学报 中国心理卫生杂志 中国新药与临床杂志 中国修复重建外科杂志 中国血吸虫病防治杂志 中国循环杂志 中国循证儿科杂志 中国烟草科学 中国烟草学报 中国药科大学学报 中国药理学通报 中国药理学与毒理学杂志 中国药学杂志 中国医学计算机成像杂志 中国医学科学院学报 中国医学影像技术 中国医学影像学杂志 中国医药工业杂志 中国应用生理学杂志 中国油料作物学报 中国油脂 中国有色金属学报 中国预防兽医学报 中国造船 中国针灸 中国真菌学杂志 中国肿瘤生物治疗杂志11中国组织化学与细胞化学杂志 1004-1850 C 中华超声影像学杂志 1004-4477 C 中华创伤骨科杂志 1671-7600 C 中华创伤杂志 1001-8050 C 中华地方病学杂志2095-4255 C 中华耳鼻咽喉头颈外科杂志 1673-0860 C 中华耳科学杂志1672-2922 C 中华放射医学与防护杂志 0254-5098 C 中华放射肿瘤学杂志 1004-4221 C 中华肝胆外科杂志 1007-8118 C 中华肝脏病杂志 1007-3418 C 中华高血压杂志 1673-7245 C 中华骨科杂志 0253-2352 C 中华护理杂志 0254-1769 C 中华急诊医学杂志 1671-0282 C 中华检验医学杂志 1009-9158 C 中华精神科杂志 1006-7884 C 中华临床营养杂志 1674-635X C 中华麻醉学杂志 0254-1416 C 中华泌尿外科杂志 1000-6702 C 中华男科学杂志 1009-3591 C 中华内分泌代谢杂志 1000-6699 C 中华器官移植杂志 0254-1785 C 中华烧伤杂志 1009-2587 C 中华神经科杂志 1006-7876 C 中华神经外科杂志 1001-2346 C 中华肾脏病杂志1001-7097 C 中华实验和临床病毒学杂志 1003-9279 C中华实验眼科杂志 中华手外科杂志 中华糖尿病杂志 中华危重病急救医学 中华微生物学和免疫学杂志 中华胃肠外科杂志 中华物理医学与康复杂志 中华显微外科杂志 中华消化外科杂志 中华小儿外科杂志 中华胸心血管外科杂志 中华眼底病杂志 中华眼视光学与视觉科学杂志 中华医学遗传学杂志 中华整形外科杂志 中南大学学报. 医学版 中南大学学报. 自然科学版 中山大学学报. 医学科学版 中山大学学报. 自然科学版 中文信息学报 中药材 中药新药与临床药理 中药药理与临床 肿瘤 重庆大学学报. 自然科学版 重庆医科大学学报 重庆邮电大学学报. 自然科学版 资源科学 四、备注 (一)D 类1.以《中文核心期刊要目总览》(科技处网页下载区和科研管理系统均可下载)最新版所收录核心期刊为准。
针灸治疗腓总神经损伤验案1_则

Advances in Clinical Medicine 临床医学进展, 2023, 13(8), 12782-12786 Published Online August 2023 in Hans. https:///journal/acm https:///10.12677/acm.2023.1381792针灸治疗腓总神经损伤验案1则陈慧彬1*,郭 璨1,李 俐2#1福建中医药大学针灸学院,福建 福州 2福建中医药大学附属第二人民医院针灸科,福建 福州收稿日期:2023年7月15日;录用日期:2023年8月6日;发布日期:2023年8月15日摘要 腓总神经损伤是针灸治疗的优势病种之一,其近年来发生率不断升高,对患者的日常生活造成严重影响,临床上针灸治疗腓总神经损伤可以有效改善失神经区运动功能及感觉障碍,减轻患者痛苦,有助于神经功能恢复。
本文主要介绍李俐主任运用针灸综合疗法治疗腓总神经损伤验案1则,以期为临床提供参考。
关键词腓总神经损伤,温针灸,电针,浅针,验案Acupuncture Treatment of Common Peroneal Nerve Injury: A Case StudyHuibin Chen 1*, Can Guo 1, Li Li 2#1College of Acupuncture and Moxibustion, Fujian University of Traditional Chinese Medicine, Fuzhou Fujian 2Department of Acupuncture and Moxibustion, The Second People’s Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fuzhou Fujian Received: Jul. 15th , 2023; accepted: Aug. 6th , 2023; published: Aug. 15th , 2023AbstractCommon peroneal nerve injury is one of the advantages of acupuncture and moxibustion treat-ment of diseases, the incidence of which has been increasing in recent years, causing serious im-pact on patients’ daily life, clinical acupuncture treatment of common peroneal nerve injury can effectively improve the motor function of the denervation area and sensory disorders, reduce the pain of patients, contribute to the recovery of nerve function. This article mainly introduces 1 case *第一作者。
浙江大学一级学术期刊和核心期刊目录
浙江大学一级学术期刊和核心期刊目录(2008版)一、国内一级期刊340种(其中带*号的为人文社科权威级期刊19种):1 法学研究*2 管理世界*3 教育研究*4 经济研究*5 历史研究*6 社会学研究*7 体育科学*8 外国文学评论*9 外语教学与研究*10 文学评论*11 心理学报*12 新华文摘*13 新闻与传播研究*14 哲学研究*15 政治学研究*16 中国社会科学*17 中国社会科学文摘*18 中国图书馆学报*19 中国语文*20 半导体学报21 北京体育大学学报22 比较教育研究23 兵工学报24 病毒学报25 材料研究学报(材料科学进展)26 财贸经济27 蚕业科学28 测绘学报29 茶叶科学30 城市规划31 传感技术学报32 催化学报33 大气科学34 大学图书馆学报35 当代电影36 当代语言学(原为:国外语言学)37 档案学通讯38 低温工程39 地理科学40 地理学报41 地理研究42 地球化学43 地球物理学报44 地震学报45 地质科学46 地质学报47 电工技术学报48 电力系统自动化49 电路与系统学报50 电信科学51 电子学报52 电子与信息学报(原名电子科学学刊)53 动力工程54 动物学报55 动物学研究56 动物营养学报57 敦煌研究58 纺织学报59 分析化学60 复合材料学报61 钢铁62 高等工程教育研究(武汉)63 高等教育研究(武汉)64 高等学校化学学报65 高分子学报66 高能物理与核物理67 高校化学工程学报68 高校应用数学学报69 工程热物理学报70 古汉语研究71 古生物学报72 固体力学学报73 管理科学学报74 光电工程75 光电子·激光76 光学学报77 光子学报78 硅酸盐学报79 国际贸易问题80 国际问题研究81 果树学报(原名:果树科学)82 海洋工程83 海洋学报84 海洋与湖沼85 航空学报86 航天医学与医学工程87 核农学报88 红外与毫米波学报89 化工学报90 化学物理学报91 化学学报92 环境科学93 环境科学学报94 会计研究95 机械工程学报96 计量学报97 计算机辅助设计与图形学学报98 计算机集成制造系统99 计算机科学技术学报(英文版) 100 计算机学报101 计算机研究与发展102 计算数学103 建筑结构学报104 建筑学报105 教育发展研究106 解剖学报107 金融研究108 金属学报109 近代史研究110 经济地理111 经济理论与经济管理112 经济社会体制比较113 经济学家114 菌物学报(原名:菌物系统) 115 考古学报116 科学通报117 科学学研究118 科研管理119 空间科学学报120 空气动力学学报121 控制理论与应用122 控制与决策123 矿物学报124 昆虫分类学报125 昆虫学报126 力学学报127 林业科学128 马克思主义研究129 麦类作物学报130 煤炭学报131 美术研究132 棉花学报133 民族研究134 模式识别与人工智能135 摩擦学学报136 内燃机工程137 内燃机学报138 农药学报139 农业工程学报140 农业机械学报141 农业经济问题142 农业生物技术学报143 气象学报144 汽车工程145 强激光与粒子束146 情报学报147 燃料化学学报148 热力发电149 人口研究150 软件学报151 社会科学战线152 生理学报153 生态学报154 生物多样性155 生物工程学报156 生物化学与生物物理学报157 生物物理学报158 声学学报159 石油学报160 实验生物学报161 史学理论研究162 世界经济163 世界经济与政治164 世界历史165 世界宗教研究166 兽类学报167 数量经济技术经济研究168 数学进展169 数学年刊(A、B辑)170 数学物理学报171 数学学报172 水产学报173 水动力学研究与进展(英文版) 174 水科学进展175 水力发电学报176 水利学报177 水生生物学报178 水土保持学报179 台湾研究180 太阳能学报181 天文学报182 通信学报183 统计研究184 土木工程学报185 土壤学报186 外国文学187 外国文学研究188 外国语189 微波学报190 微生物学报191 文史(中华书局)192 文献193 文学遗产194 文艺理论研究195 文艺研究196 无机材料学报197 无机化学学报198 物理化学学报199 物理学报200 系统工程理论与实践201 系统科学与数学202 细胞生物学杂志203 现代外语204 心理科学205 新美术206 畜牧兽医学报207 学术月刊208 岩石力学与工程学报209 岩石学报210 岩土工程学报211 遥感学报212 药物分析杂志213 药学学报214 仪器仪表学报215 遗传216 遗传学报217 应用生态学报218 应用数学学报219 应用数学与力学(英文版)220 应用心理学221 营养学报222 有机化学223 宇航学报224 语言研究225 园艺学报226 浙江大学学报(人文社会科学版)227 浙江大学学报(工学版)228 浙江大学学报(英文版)229 真空科学与技术学报230 振动工程学报231 政法论坛232 植物保护学报233 植物病理学报234 植物分类学报235 植物生理与分子生物学学报(原名:植物生理学报) 236 植物生态学报237 植物学报238 植物营养与肥料学报239 中草药240 中共党史研究241 中国病理生理杂志242 中国出版243 中国电机工程学报244 中国法学245 中国翻译246 中国腐蚀与防护学报247 中国高教研究248 中国工业经济249 中国公路学报250 中国光学快报(英文版)251 中国广播电视学刊252 中国化学快报(英文版)253 中国环境科学254 中国机械工程255 中国激光256 中国寄生虫学与寄生虫病杂志257 中国经济史研究258 中国科学(A-G)辑259 中国粮油学报260 中国农村经济261 中国农业科学262 中国人口科学263 中国人民大学报刊复印资料(全文复印) 264 中国社会科学季刊(香港)现已停刊265 中国社会科学评论(香港)266 中国生物防治267 中国生物化学与分子生物学报268 中国生物医学工程学报269 中国食品学报270 中国史研究271 中国兽医学报272 中国水稻科学273 中国体育科技274 中国图像图形学报275 中国土地科学276 中国物理快报(英文版)277 中国稀土学报278 中国现代文学研究丛刊279 中国畜牧杂志280 中国药理学报281 中国药理学与毒理学杂志282 中国药学杂志283 中国音乐学284 中国应用生理学杂志285 中国有色金属学报286 中国预防兽医学报287 中国运动医学杂志288 中国中西医结合杂志289 中国中药杂志290 中华病理学杂志291 中华超声影像学杂志292 中华传染病杂志293 中华创伤杂志294 中华儿科杂志295 中华耳鼻咽喉头颈外科杂志296 中华放射学杂志297 中华放射医学与防护杂志298 中华妇产科杂志299 中华骨科杂志300 中华护理杂志301 中华急诊医学杂志(原名: 急诊医学) 302 中华检验医学杂志303 中华结核和呼吸杂志304 中华精神科杂志305 中华口腔医学杂志306 中华劳动卫生职业病杂志307 中华流行病学杂志308 中华麻醉学杂志309 中华泌尿外科杂志310 中华内分泌代谢杂志311 中华内科杂志312 中华皮肤科杂志313 中华普通外科杂志314 中华烧伤杂志315 中华神经科杂志316 中华神经外科杂志317 中华肾脏病杂志318 中华外科杂志319 中华微生物学和免疫学杂志320 中华物理医学与康复杂志321 中华消化杂志322 中华小儿外科杂志323 中华心血管病杂志324 中华胸心血管外科杂志325 中华血液学杂志326 中华眼科杂志327 中华医学遗传学杂志328 中华医学杂志329 中华医院管理杂志330 中华预防医学杂志331 中华整形外科杂志332 中华肿瘤杂志333 中外法学334 自动化学报335 自然辩证法通讯336 自然辩证法研究337 自然科学进展338 自然灾害学报339 自然资源学报340 作物学报注:被IM收录的论文视同国内一级期刊论文。
高凯鸣个人简历

个人简历高凯鸣,男,手外科、显微外科医学博士。
任职情况:♦中华医学会手外科学分会第八届青年委员♦中华医学会手外科学分会秘书;♦International Member of the American Society for Surgery of the Hand (ASSH);♦上海医师协会手外科医师分会第一届委员兼秘书♦中华医学会手外科学分会华东地区第十届青年委员会副主任委员;♦中华医学会手外科学分会华东地区第八、第九届青年委员会委员;♦中华医学会手外科学分会华东地区学术委员会秘书;♦中国医师协会骨科学分会外固定与肢体重建委员会第一届委员;♦国际肢体延长与重建学会(ILLRS)、国际Ilizarov技术研究与应用学会(ASAMI)第一届中国部委员;♦中国医师协会手外科医师分会工作秘书;♦上海医师协会骨科医师分会第一届手外科工作组秘书;复旦大学附属华山医院手外科教学秘书。
学习经历:于2000年进入复旦大学上海医学院(原上海医科大学)临床医学系7年制学习;2005年毕业于复旦大学医学院获学士学位,直接进入华山医院手外科攻读硕士学位;2007年毕业获硕士学位,并在手外科工作至今;2009年开始在职攻读博士学位,于2013年获得博士学位;2016年在美国Johns Hopkins Hospital 访问学习。
2017年在美国Louisville Hand Center访问学习。
专业特长:长期从事于周围(臂丛)神经损伤及卡压的临床治疗和科研研究工作,在臂丛及周围神经损伤的修复重建方面投入了主要的精力,并作了较多的相关基础和临床研究,在国内外杂志发表了多篇文章。
另外,在上肢骨关节损伤修复以及微创治疗领域也有较为丰富的临床经验。
所获荣誉2009年获得华东地区手外科年会优秀论文二等奖2010年获得全国手外科年会秀论文二等奖2012年获得上海市三学会优秀论文一等奖2014年获得华东地区手外科年会秀论文一等奖2016年获得全国手外科年会秀论文一等奖2013年参加在印度举办的第12届IFSSH大会并作大会发言2016年作为亚太地区代表(亚太地区共2人)参加在阿根廷举办的第13届IFSSH 大会论文竞赛2018年参加在丹麦举办的第23届FESSH大会并作大会发言论文发表情况(仅第一作者):高凯鸣,劳杰,顾玉东,张丽银,虞聪,赵新. 健侧颈7移位术后远期功能随访.中华手外科杂志,2006;22(4):195-197.高凯鸣, 劳杰, 赵新,顾玉东. 选择性健侧C7移位术后的远期功能随访. 中华手外科杂志,2010(6):324-327.Gao KM, Lao J, Zhao X, Gu YD. Outcome after transfer of intercostal nerves to the nerve of triceps long head in 25 adult patients with total brachial plexus root avulsion injury. J Neurosurgery. 2013;118:606-610.Gao KM, Lao J, Zhao X, Gu YD. Outcome of contralateral C7 transfer to two recipient nerves in 22 patients with the total brachial plexus avulsion injury. Microsurgery. 2013;33(8):606-611Gao KM, Lao J, Zhao X, Gu YD. Outcome of contralateral C7 nerve transferring to median nerve. Chin Med J (Engl). 2013;126(20):3865-3868.高凯鸣,劳杰,赵新,方有生,刘靖波. 带血管蒂尺神经前置术治疗重度肘管综合征的临床疗效观察. 中华手外科杂志,2017;33(6):462-464 Gao KM, Lao J, Guan WJ, Hu JJ. Is it necessary to use the entire root as a donor when transferring contralateral C7 nerve to repair median nerve? Neural Regeneration Research. 2018;13(1):94-99.Gao KM, Hu JJ, Lao J, Zhao X. Evaluation of nerve transfer options for treating total brachial plexus avulsion injury: a retrospective study of 73 participants. Neural Regeneration Research. 2018;13(3):470-476.高凯鸣,劳杰,庄永青,赵新,方有生,刘靖波. 利用经皮克氏针联合微型外固定支架技术治疗第五掌骨基底部骨折的临床疗效. 中华手外科杂志,2018;34(4):222-224.科研成果:获得2015年度国家自然科学基金青年基金(不同健侧颈7神经根切取方式对手术效果的影响及其发生机制的研究,81501871,项目负责人)。
脑脊液可通过嗅觉通路系统回流到颈部淋巴系统
NEURAL REGENERATION RESEARCHVolume 7, Issue 10, April 2012Cite this article as: Neural Regen Res. 2012;7(10):766-771.766 Haisheng Liu☆, M.D., Ph.D., Associate professor, Department of Neurosurgery, Yuquan Hospital, Tsinghua University, Beijing 100049, ChinaCorresponding author: Zhili Ni, Department of Otorhinolaryngology and Head & Neck Surgery, Xuanwu Hospital, Capital Medical University, Beijing 100053, ChinaNzl301@ Received: 2011-09-24 Accepted: 2011-11-22(N20110916004/H)Liu HS, Ni ZL, Chen YT, Wang D, Qi Y, Zhang QH, Wang SJ. Olfactory route for cerebrospinal fluid drainage into the cervical lymphatic system in a rabbit experimental model. Neural Regen Res.2012;7(10):766-771.doi:10.3969/j.issn.1673-5374. 2012.10.009Olfactory route for cerebrospinal fluid drainage into the cervical lymphatic system in a rabbit experimental model***☆Haisheng Liu1, Zhili Ni2, Yetao Chen1, Dong Wang1, Yan Qi2, Qiuhang Zhang2, Shijie Wang21Department of Neurosurgery, Yuquan Hospital, Tsinghua University, Beijing 100049, China2Department of Otorhinolaryngology and Head & Neck Surgery, Xuanwu Hospital, Capital Medical University, Beijing 100053, China AbstractThe present study analyzed the anatomical association between intracranial subarachnoid spaceand the cervical lymphatic system. X-ray contrast medium and Microfil® (Microfil compounds fill andopacify microvascular and other spaces of non-surviving animals and post-mortem tissue underphysiological injection pressure) were injected into the cisterna magna of the rabbit, and perineuralroutes of cerebrospinal fluid outflow into the lymphatic system were visualized. Under a surgicaloperating microscope, Microfil was found within the subarachnoid space and along the olfactorynerves. At the nasal mucosa, a lymphatic network was identified near the olfactory nerves, whichcrossed the nasopharyngeal region and finally emptied into the superficial and deep cervical lymphnodes. Under a light microscope, Microfil was visible around the olfactory nerves and withinlymphatic vessels. These results suggested that cerebrospinal fluid drained from the subarachnoidspace along the olfactory nerves to nasal lymphatic vessels, which in turn, emptied into the cervicallymph nodes. This anatomical route, therefore, allowed connection between the central nervoussystem and the lymphatic system.Key Words:central nervous system; cerebrospinal fluid; lymph; subarachnoid spaceAbbreviations: CSF, cerebrospinal fluid; SAS, subarachnoid spaceINTRODUCTIONUnder normal conditions, the cerebrospinal fluid (CSF) is produced mainly via a process of ultrafiltration at the non-tight junction level of capillary endothelial walls in the choroid plexus. However, very little evidence is available that supports a role for arachnoid villi and granulations in this process. Recent studies have suggested that CSF movement directly into the cranial venous system might only occur under high pressure, which suggests that arachnoid projections might exhibit accessory functions, rather than representing primary locations where CSF is absorbed[1-2].According to the traditional theory, the central nervous system is regarded as an immune-exempt organ. Lymphatic vessels do not exist within the parenchyma of the central nervous system[3]. CSF is typically thought to be absorbed through arachnoid villi. However, a relatively large volume of literature supports an anatomical association between CSF and the lymph system[4-6]. Alternative routes for CSF drainage into the peripheral lymphatic system exist. Among them, the route along the fila olfactoria and olfactory nerves hasbeen suggested to be a main route of CSFdrainage from the subarachnoid space (SAS)into nasal lymphatics[7-9].The present study analyzed the anatomicaland histological characteristics of theolfactory route for CSF drainage intoperipheral lymphatic vessels. The olfactoryroute was initially revealed by X-raycisternography and subarachnoid injectionof Microfil®. Subsequently, the ultrastructureof olfactory nerves and nasal mucosa, inrelation to cerebrospinal fluid drainage, was demonstrated.RESULTSQuantitative analysis of experimentalanimalsA total of ten male and ten female NewZealand white rabbits were included in thepresent study. Five male and five femalerabbits, respectively were infused withmedical contrast medium for cisternography,and the remaining ten rabbits were injectedat the subarachnoid space for Microfilexaminations. One rabbit injected withMicrofil into the cisterna magna wasexcluded, because Microfil did not properly767distribute. Microfil was observed throughout thesubarachnoid compartment at the base of the brain and in the orbit.CisternographyConventional radiographs, taken 30 minutes after cisternal infusion of 3 mL contrast medium, revealed perineural routes of CSF outflow into the lymphatic system. Contrast medium was observed in the orbit, nasal cavities, and subsequently in the hard and soft palate (Figure 1). Details of CSF outflow were detected by direct magnification of the X-ray technique: lateral projections during the first minute of infusion revealed contrast medium sinking downwards into the spinal compartment. The medium filled the basal cisterns first and then spread in the direction of the cribriform plate. Reaching the cribriform plate at 10 minutes after start of infusion, the contrast medium leaked immediately into the nasal cavities.Macroscopic distribution of MicrofilUnder macroscopic examination, some contrast agent filled and opacified the head and cervical superficiallymphatic vessels, and was also located in subcutaneous tissues of both ears, as well as periorbital and nasalregions. Simultaneously, lymphatic vessels located beneath the submaxillary gland and cervical skin were slightly opacified by Microfil. However, the majority of Microfil was found in deep cervical lymphatic vessels along the posterior pharyngeal wall to the cervical lymphatic trunks and thoracic duct (Figure 2). After the animals were decapitated, Microfil was observed clustered along the sagittal sinus, cisterna magna, and olfactory bulb under a surgical operating microscope. In addition, Microfil was distributed in a patchy pattern along the fila olfactoria external to the cranium, as well as in extensive lymphatic networks associated with the submucosa of the olfactory epithelium, ethmoid turbinates, and adjacent nasal septum (Figure 3).Microfil was detected within the SAS of the optic nerve sheath and accumulated in the conjunction optic nerve of the retina. In addition, lymphatics containing Microfil were observed in mucosa of the lateral wall of the dorsum nasi, close to the nostrils. These vessels penetrated through cartilage of the lateral wall and joined larger superficial lymphatic ducts in subcutaneous adipose tissue. The arterial vessels of these preparations were filled with blue Microfil via injection into both carotid arteries, and the CSF compartment was infused with a yellow agent.Results demonstrated yellow lymphatic vessels that were clearly discernable from the blue blood vessels (Figure 4). Microscopic distribution of MicrofilUnder microscopic histological examination, Microfil was detected in a patchy distribution along the fila olfactoria as it exited the cribriform plate. The yellow Microfil appeared dark-brown after fixation. Microfil was observed in perineurial spaces and was particularly concentrated around emerging olfactory nerve roots. Microfil was associated closely with fila olfactoria located free in perineurial spaces or contained within endothelial lined vessels (Figure 5). Most lymphatic vessels within the olfactory submucosa appeared to comprise a single layer of endothelial cells, which resembled lymphaticFigure 1 Cisternography of X-ray.In conventional radiographs, the contrast medium(Omnipaque) is injected into the cisterna magna, and the perineural routes of contrast medium outflow into the lymphatic system are visualized.The picture is taken 30 minutes after cisternal infusion of 3-mL contrast medium. The contrast medium is visible in the orbit, nasal cavities, and subsequently in the hard and soft palate. Figure 2 Macroscopic view of Microfil distribution in cervical lymphatic vessels. some Microfil fills and opacifies the head and cervical superficial lymphatic vessels. However, the majority of Microfil is observed in deep cervical lymphatic vessels along the posterior pharyngeal wall to the cervical lymphatic trunks and thoracic duct. Figure 3 Microscopic view of Microfil distribution in nasal and anterior skull base region.Microfil is visible in a patchy distribution along the fila olfactoria external to the cranium, as well as in extensive lymphatic networks associated with the submucosa of the olfactory epithelium, ethmoid turbinates, and adjacent nasal septum.vessels (Figure 6). Microfil-filled lymphatic vessels wereparticularly conspicuous around the fila olfactoria, close to the point of exit from the cribriform plate. However, lymphatics filled with contrast agent were observed scattered throughout the olfactory submucosa. There was no Microfil in arteries or veins of the olfactory submucosa.DISCUSSIONResults from the present study suggested that a significant portion of CSF was removed from the subarachnoid space by peripheral lymphatic vessels, particularly in nasal lymphatic vessels. These conclusions were based on experiments and intensive analysis to explore CSF transport routing, which spanned over 100 years and was conducted in various experimental animals, such as dogs, rabbits, rats, and sheep[10-13]. The methods for determining passage between SAS and lymphatic vessels included subarachnoid injection of ink, X-ray contrast, and Microfil. All experimental results demonstrated that the olfactory route was a major passage for CSF absorption through the lymphatic system.Microfil compounds, which are based on silicone rubber, can fill and opacify microvasculars and other spaces of non-surviving animals and post-mortem tissue under physiological injection pressure. The continuous, closed, vascular system lends itself to flow through injection or perfusion techniques. Following injection, Microfil compounds form a three-dimensional cast of the vasculature. Johnston et al [6] showed that this was possible in sheep, pigs, rabbits, rats, mice, monkeys, and humans; immediately upon sacrifice (or up to 7 hours after death in humans), yellow Microfil was injected into the CSF compartment. Microfil was observed primarily in the subarachnoid space around the olfactory bulbs and cribriform plate. Along the olfactory nerves, the contrast agent entered extensive lymphatic networks in the submucosa, which were associated with olfactory and respiratory epithelium. Results suggested that CSF absorption into the nasal lymphatic vessels is a characteristic feature of all mammals, including humans. In the present study, Microfil injections into the cistern magna of rabbits revealed a similar phenomenon in all animals but one.Under macroscopic examination, Microfil in the SAS was primarily distributed along the cistern magna, skull base, sagittal sinus, optic nerve, olfactory bulb, and extracranial, mostly along the fila olfactoria. Some Microfil filled and opacified the head and cervical superficial lymphatic vessels. However, the majority of Microfil was observed in deep cervical lymphatic vessels along the posterior pharyngeal wall to the cervical lymphatic trunks and thoracic duct. Morphological analysis revealed that the olfactory route was the main route for CSF drainage into lymphatic vessels, particularly the primary route went into the deep lymphatic vessels system.Under light microscopic histological analysis, Microfil was observed in perineurial spaces and was particularly concentrated around emerging olfactory nerve roots. Microfil-filled lymphatics were particularly conspicuous around the fila olfactoria, close to the point of exit from the cribriform plate. However, lymphatics filled with theFigure 4 Varied colored Microfil display in nasal septum lymphatic vessel and artery.When arterial vessels are filled with blue Microfil via injection into both carotid arteries and the cerebrospinalfluid compartment is infused with yellow agent, the yellow lymphatic vessels are clearly discernable from theblue-colored blood vessels.Figure 5 Histological observation of Microfil in olfactory nerve (hematoxylin-eosin staining, × 100).The yellow Microfil (red arrow) appears dark-brown after fixation. Microfil is observed in perineurial spaces. Figure 6 Histological observation of Microfil in nasal septum lymphatic vessels (hematoxylin-eosin staining, ×400).Most lymphatic vessels within the olfactory submucosa comprise a single layer of endothelial cells, which is characteristic of lymphatic vessels. Dark-brown Microfil (red arrow) is visible in lymphatic vessels.768contrast agent were observed scattered throughout the olfactory submucosa, which suggested that thehigh-injection pressure destroyed the lymphatic vessels. There was no Microfil in the arteries or veins of olfactory submucosa.The mechanism of CSF drainage into lymphatic vessels via the olfactory route remains controversial[5, 7, 14-15]. Different models have been proposed by various scholars: (1) the SAS is present along olfactory nerves in the cribriform plate and continues with lymphatic vessels of the nasal mucosa; (2) the SAS extends along the nerve to the nasal mucosa. From this space, cerebrospinal fluid leaks out into nasal mucosa and enters lymphatic vessels; (3) the SAS is continuous with the perineurial space of the olfactory nerves. The CSF reaches nasal mucosa through this space and disperses through connective tissue and enters lymphaticvessels[7, 14]; and (4) the SAS is continuous with the perineurial space and with nasal lymphatic vessels[14-16]. Microfil is a relatively viscous silastic material, which would not be expected to be readily absorbed from an interstitial compartment. Therefore, results from the present study suggested that the hypothesis proposedby Johnston et al [6] was most likely; either a direct connection or labyrinth structure must exist between the CSF and lymph compartments to facilitate uptake of intracisternally administered Microfil into lymphatic vessels.CSF drainage into lymphatic vessels is significant for the physiology and pathophysiology of the central nervous system and related disease. Lymphatic CSF transport influences intracranial pressure and CSF circulation: Mollanji et al [17] concluded that sealing the cribriform plate extracranially impairs the ability of CSFpressure-regulating systems to compensate for volume infusions in a sheep model. The time spent for India ink to move from the CSF into the cervical lymph nodes increase was shown to be dependent on the model of transforming growth factor-β1 induced hydrocephalus in a mouse model[18]. This suggested that thecribriform-lymphatic connection is disrupted in these animals.The blockage of lymphatic CSF transport impacts functions of the central nervous system. Sun et al [19] observed the influence of cerebral lymphatic drainage blockade on regional cerebral blood flow and brain edema in a rat model of experimental subarachnoid hemorrhage, concluding that a blocked cerebral lymphatic drainage pathway further deteriorates secondary cerebral ischemia and brain edema following subarachnoid hemorrhage.A lymphatic-CSF relationship also implies an immunological relationship. Induction of experimental autoimmune encephalomyelitis in a rat model results in a severe immune response, followed by cerebral lesions. Removal of deep and superficial cervical lymph nodes following induction of autoimmune encephalomyelitis significantly reduces pathological severity[20-21]. Therefore, the cervical lymph nodes could provide the prime immune cells needed for targeting the brain. Previous results have suggested that lymphatic drainage of brain antigens contributes to the pathogenesis of Alzheimer's disease and multiple sclerosis[22].In conclusion, results from the present study demonstrated the presence of an olfactory route for cerebrospinal fluid drainage into the nasal lymphatics. According to radiographs and Microfil data, these pathways could be used for high-flow CSF absorption. In rabbits, the lymphatic pathways were as important as the absorption route, which was considered to be important for cerebrospinal fluid absorption and antigen movement from the subarachnoid space to the cervical lymph nodes, where the immune response occurred.MATERIALS AND METHODSDesignA contrasting, observational, animal experiment.Time and settingThis study was performed at the Laboratory of Yuquan Hospital, China from March to October 2009.MaterialsTo avoid the influence of animal gender, ten male and ten female New Zealand white rabbits, weighing 2-3 kg and aged 4-6 months, were used for the experiments. The rabbits were purchased from the Fangyuanyuan Breeding Farm of Beijing (license No. SCXK (Jing)2009-0014). All experimental procedures were conducted in accordance with the Institutional Guidelines for the Care and Use of Laboratory Animals in Yuquan Hospital, Beijing, China, and conformed to the National Institutes of Health Guide for Care and Use of Laboratory Animals.MethodsCisterna magna punctureThe rabbits were placed into a stereotactic frame in a prone position, and the atlanto-occipital membrane was exposed by a midsagittal incision of the scalp. A22-gauge venous indwelling trocar was introduced into the cisterna magna at an angle of 30° between the trocar and horizontal plane. Clear CSF discharge from the trocar demonstrated that the puncture was successful (Figure 7). The troca was fixed along the skull bone and the skin with chemical glue. X-ray contrast and Microfil were injected into the cisterna magna via the troca. CisternographyAt the start of examination, the rabbits were anesthetized with 1% pentobarbital (1 mL/kg) intravenous injection, and the injection was repeated every 30 minutes with half of the initial dosage. During this process, aself-made microcatheter was connected to the troca, and a pressure transducer was connected to the cisternal catheter via a three-way stopcock. Using an adjustable syringe pump, 0.1 mL/min of X-ray contrast medium, Omnipaque (Shanghai GE Healthcare, Shanghai, China), was infused over 60 minutes. The infusion was769interrupted when intracranial pressure reached >2.67 kPa. X-ray (DigiArc-100, Beijing East Whale Imaging Technology, Beijing, China) studies were performed at 1, 10, 20, 30, and 60 minutes, respectively, after infusion. The contrast medium reached the cribriform plate at 10 minutes and the distal optic nerve at 20 minutes, respectively. The medium then leaked into the nasal cavities and opacified the cervical lymphatic vessels at 30 minutes after start of infusion.Subarachnoid injection of MicrofilAt the start of preparation, the rabbits were intraperitoneally anaesthetized with 1 mL/kg 1% pentobarbital (Beijing Double-Crane Pharmaceutical, Beijing, China). Subsequently, the rabbits were euthanized with an intraperitoneal injection of 1% pentobarbital (3 mL/kg). Microfil was used to fill vascular and other spaces of non-surviving animals(, Flow Tech, Carver, MA, USA). It was available in a variety of colors and was designed to facilitate visual and microscopic analysis of microcirculation. A volume of 10 mL yellow Microfil was manually infused into the cisterna magna over 5-10 minutes; 3 mL of diluent was used for each 1 mL of yellow Microfil, and the material catalyzed with 10% (of total volume) of the curing agent. In two male and three female rabbits, respectively, blue Microfil was injected into the blood vasculature, and yellow Microfil was simultaneously injected into the CSF compartment. The carotid arteries were catheterized and 10 mL blue Microfil (MV-120) was simultaneously infused into both arteries. An injection was considered successful if the Microfil fully filled and stained the nasal lymphatic vessel. Histological assessmentsAfter the infusions were complete, the Microfil was allowed to set for 2 hours. The anterior cervical skin was incised midsaggitally from the incisor to suprasternal fossa. The superficial and deep lymphatic vessel was observed step by step. After cervical anatomical dissection was complete, the animals were sacrificed. The skin was removed and the heads were cut along a parasagittal plane. Partial dissection was performed under a surgical operating microscope (Leica MS-II Leica, Nussloch, Germany). Subsequently, the olfactory bulbs and olfactory tracts were removed from the cribriform plate and the subjacent parts of the nasal mucosa. Tissues were harvested and fixed in 10% formalin for48 hours. Prior to sectioning for histology, the samples were processed through 70%, 95%, and 100% ethanol, as well as methylbenzene and wax. Paraffin-embedded samples were cut into 4-µm sections using a microtome (Leica, Nussloch, Germany), and were stained with hematoxylin-eosin. Histological assessments were performed using an Olympus light microscope (Olympus, Tokyo, Japan).Funding:The study was supported by the National Natural Science Foundation of China, No. 30700858; the Research Fund of Capital Medical Development, No. 2009-3047; and Wushunde Medical Research Fund of Tsinghua University in 2011.Author contributions:This study was designed by Haisheng Liu, Qiuhang Zhang, performed by Zhili Ni, Yetao Chen, Dong Wang, and Yan Qi, and evaluated by Shijie Wang, who were blinded to the experimental design.Conflicts of interest: None declared.Ethical approval: The experiments were performed with the Institutional Guidelines for the Care and Use of Laboratory Animals Yuquan Hospital, Tsinghua University, China.REFERENCES[1] Johanson CE. Ventricles and Cerebrospinal fluid. In: Conn PM, ed.Neuroscience in Medicine. Philadelphia: J.B. Lippincott Company.1995.[2] Papaiconomou C, Zakharov A, Azizi N, et al. Reassessment ofthe pathways responsible for cerebrospinal fluid absorption in theneonate. Childs Nerv Syst. 2004;20(1):29-36.[3] Brinker T, Lüdemann W, Berens von Rautenfeld D, et al. Dynamicproperties of lymphatic pathways for the absorption ofcerebrospinal fluid. Acta Neuropathol. 1997;94(5):493-498.[4] Mollanji R, Papaiconomou C, Boulton M, et al. Comparison ofcerebrospinal fluid transport in fetal and adult sheep. Am J Physiol Regul Integr Comp Physiol. 2001;281(4):1215-1223.[5] Weller RO, Kida S, Zhang ET. Pathways of fluid drainage from thebrain-morphological aspects and immunological significance in rat and man. Brain Pathol. 1992;2(4):277-284.[6] Johnston M, Zakharov A, Koh L, et al. Subarachnoid injection ofMicrofil reveals connections between cerebrospinal fluid andnasal lymphatics in the non-human primate. Neuropathol ApplNeurobiol. 2005;31(6):632-640.[7] Johnston M, Zakharov A, Papaiconomou C, et al. Evidence ofconnections between cerebrospinal fluid and nasal lymphaticvessels in humans, non-human primates and other mammalianspecies. Cerebrospinal Fluid Res. 2004;10(1):2.[8] Zakharov A, Papaiconomou C, Djenic J, et al. Lymphaticcerebrospinal fluid absorption pathways in neonatal sheeprevealed by subarachnoid injection of Microfil. Neuropathol ApplNeurobiol. 2003;29(6):563-573.[9] Kapoor KG, Katz SE, Grzybowski DM, et al. Cerebrospinalfluid outflow: an evolving perspective. Brain Res Bull. 2008;77(6):327-334.Figure 7 Cisterna magna puncture in a rabbit model. The rabbits were fixed in a prone position and the atlanto-occipital membrane was exposed.A 22-gauge venous indwelling trocar was introduced into the cisterna magna at an angle of 30° between the trocar and horizontal plane. Clear cerebrospinal fluid discharge from the trocar was considered a successful puncture.770[10] Greitz D, Greitz T, Hindmarsh T. A new view on theCSF-circulation with the 7. potential for pharmacologicaltreatment of childhood hydrocephalus. Acta Paediatr. 1997;86(2):125-132.[11] Zakharov A, Papaiconomou C, Koh L, et al. Integrating the rolesof extracranial lymphatics and intracranial veins in cerebrospinalfluid absorption in sheep. Microvasc Res. 2004;67(1):96-104. [12] Johnston M, Papaiconomou C. Cerebrospinal fluid transport: alymphatic perspective. News Physiol Sci. 2002;17(6):227-230. [13] Koh L, Zakharov A, Johnston M. Integration of the subarachnoidspace and lymphatics: is it time to embrace a new concept ofcerebrospinal fluid absorption? Cerebrospinal Fluid Res.2005;20;2:6.[14] Kida S, Pantazis A, Weller RO. CSF drains directly from thesubarachnoid space into nasal lymphatics in the rat. Anatomy,histology and immunological significance. Neuropathol ApplNeurobiol. 1993;19(6):480-488.[15] Bradbury MW, Westrop RJ. Factors influencing exit of substancesfrom cerebrospinal fluid into deep cervical lymph of the rabbit. JPhysiol. 1983;339(1):19-34.[16] Gomez DG, Fenstermacher JD, Manzo RP, et al. Cerebrospinalfluid absorption in the rabbit: olfactory pathways. Acta Otolaryngol.1985;100(1):29-36. [17] Mollanji R, Bozanovic-Sosic R, Zakharov A, et al. Blockingcerebrospinal fluid absorption through the cribriform plateincreases resting intracranial pressure. Am J Physiol Regul Integr Comp Physiol. 2002;282(6):R1593-1599.[18] Moinuddin SM, Tada T. Study of cerebrospinal fluid flow dynamicsin TGF-beta 1 induced chronic hydrocephalic mice. Neurol Res.2000;22(2):215-222.[19] Sun BL, Xia ZL, Wang JR, et al. Effects of blockade of cerebrallymphatic drainage on regional cerebral blood flow and brainedema after subarachnoid hemorrhage. Clin Hemorheol Microcirc.2006;34(1-2):227-232.[20] Harling-Berg C, Knopf PM, Merriam J, et al. Role of cervical lymphnodes in the systemic humoral immune response to human serum albumin microinfused into rat cerebrospinal fluid. J Neuroimmunol.1989;25(2-3):185-193.[21] Weller RO, Galea I, Carare RO, et al. Pathophysiology of thelymphatic drainage of the central nervous system: Implications for pathogenesis and therapy of multiple sclerosis.Pathophysiology. 2010;17(4):295-306.[22] Weller RO, Djuanda E, Yow HY, et al. Lymphatic drainage of thebrain and the pathophysiology of neurological disease. ActaNeuropathol. 2009;117(1):1-14.(Edited by Zhao XX, Xiao N/Su LL/Song LP)771。
Modified contralateral C7 nerve transfer
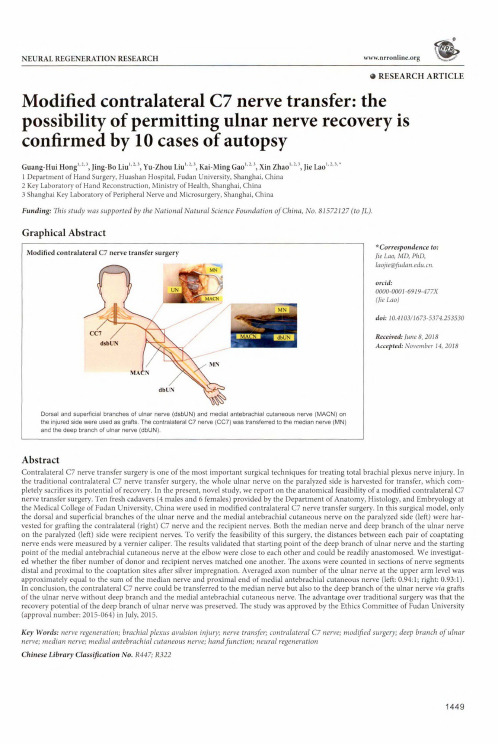
NEURAL REGENERATION RESEARCH 0RESEARCH ARTICLE Modified contralateral C7nerve transfer:the possibility of permitting ulnar nerve recovery is confirmed by10cases of autopsyGuang-Hui Hong1'2,3,Jing-Bo Liu1,2'3,Yu-Zhou Liu1,2,3,Kai-Ming Gao12\Xin Zhao1213,Jie Lao1231Department of Hand Surgery,Huashan Hospital,Fudan University,Shanghai,China2Key Laboratory of Hand Reconstruction,Ministry of Health,Shanghai,China3Shanghai Key Laboratory of Peripheral Nerve and Microsurgery,Shanghai,ChinaFunding:This study was supported by the National Natural Science Foundation of China,No.81572127(to JL).Graphical AbstractModified contralateral C7nerve transfer surgery *Correspondence to: lie Lao,MD,PhD, laojie@.orcid:0000-0001-6919-477X(Jie Lao)doi:10.4103/1673-5374.253530Received:June8,2018Accepted:November14,2018 Dorsal and superficial branches of ulnar nerve(dsbUN)and medial antebrachial cutaneous nerve(MACN)onthe injured side were used as grafts.The contralateral C7nerve(CC7)was transferred to the median nerve(MN)and the deep branch of ulnar nerve(dbUN).AbstractContralateral C7nerve transfer surgery is one of the most important surgical techniques for treating total brachial plexus nerve injury.In the traditional contralateral C7nerve transfer surgery,the whole ulnar nerve on the paralyzed side is harvested for transfer,which completely sacrifices its potential of recovery.In the present,novel study,we report on the anatomical feasibility of a modified contralateral C7 nerve transfer surgery.Ten fresh cadavers(4males and6females)provided by the Department of Anatomy,Histology,and Embryology at the Medical College of Fudan University,China were used in modified contralateral C7nerve transfer surgery.In this surgical model,only the dorsal and superficial branches of the ulnar nerve and the medial antebrachial cutaneous nerve on the paralyzed side(left)were harvested for grafting the contralateral(right)C7nerve and the recipient nerves.Both the median nerve and deep branch of the ulnar nerve on the paralyzed(left)side were recipient nerves.To verify the feasibility of this surgery,the distances between each pair of coaptating nerve ends were measured by a vernier caliper.The results validated that starting point of the deep branch of ulnar nerve and the starting point of the medial antebrachial cutaneous nerve at the elbow were close to each other and could be readily anastomosed.We investigated whether the fiber number of donor and recipient nerves matched one another.The axons were counted in sections of nerve segments distal and proximal to the coaptation sites after silver impregnation.Averaged axon number of the ulnar nerve at the upper arm level was approximately equal to the sum of the median nerve and proximal end of medial antebrachial cutaneous nerve(left:0.94:1;right:0.93:1). In conclusion,the contralateral C7nerve could be transferred to the median nerve but also to the deep branch of the ulnar nerve via grafts of the ulnar nerve without deep branch and the medial antebrachial cutaneous nerve.The advantage over traditional surgery was that the recovery potential of the deep branch of ulnar nerve was preserved.The study was approved by the Ethics Committee of Fudan University (approval number:2015-064)in July,2015.Key Words:nerve regeneration;brachial plexus avulsion injury;nerve transfer;contralateral C7nerve;modified surgery;deep branch of ulnar nerve;median nerve;medial antebrachial cutaneous nerve;hand f unction;neural regenerationChinese Library Classification No.R447;R3221449Hong GH,Liu JB,Liu YZ,Gao KM,Zhao X,Lao J(201刃Modified contralateral C7nerve transfer:the possibility of p ermitting ulnar nerve recovery is confirmed by10cases of autopsy.Neural Regen Res14(8):1449-1454.doi:10.4103/1673-5374.253530IntroductionBrachial plexus avulsion injury is a most devastating injury to the upper extremity.Treatment is even more difficult when the supply of donor nerves is limited.Patients will completely or partially lose their motor and sensory functions of the affected side and suffer from serious physical and psychological harm(Hu et al…2014;Wang et al.,2014; Yang et al.,2015a).Donor nerves from the brachial plexus, such as the phrenic nerve,accessory nerve,and intercostal nerves,are used to repair total brachial plexus avulsion injury(Gao et al.,2013b,2018a).Contralateral C7nerve(CC7) transfer surgery is one of the most important treatments. The first case of CC7transfer was reported by Gu et al.in 1991and later adopted by many other centers(Gu et al., 1991;Terzis et al.,2009;Wang et al.,2013,2018;Tu et al., 2014;Vanaclocha et al.,2015).The CC7on the intact side provided an abundant source of motor nerve fibers allowing some to be donated without permanent damage to the donor limb(Spinner et al.,2005;Chen et al.,2007;Li et al., 2017;Zheng et al.,2018).However,the traditional method using the whole ulnar nerve as a graft has some shortcomings.The traditional CC7transfer surgery is performed in separate stages.In the first stage,the distal end of ulnar nerve(UN)on the paralyzed side is anastomosed with CC7; in the second stage,the proximal end of UN is anastomosed with a recipient nerve such as the median nerve(MN)(Gao et al.,2006;Chuang et al.,2012).The disadvantage of using the whole UN as a graft is that the possibility of recovery of the intrinsic muscles innervated by UN is completely sacrificed.On the other hand,as the CC7transfer contains a large amount of nerve fibers,it has been suggested that it could be used for restoring more than one recipient nerve (Shin et al.,2005;Gao et al.,2018b).In view of the drawbacks of traditional CC7transfer surgery,we designed a modified CC7transfer procedure.In this procedure,the deep branch of the ulnar nerve(dbUN) on the injured side was preserved,while the dorsal and superficial branches of the ulnar nerve(dsbUN)were used as grafts.The medial antebrachial cutaneous nerve(MACN) was also used to bridge the gap between the proximal end of ulnar nerve(peUN)and the proximal end of dbUN.In this way,both the dbUN and MN were innervated.The present study aimed to investigate the feasibility of this modified CC7transfer surgery in cadavers.The axons were counted to study the degree of matching in the number of donor and recipient nerve fibers.A completely new design was used in modifying traditional CC7nerve transfer surgery.Although it was traditionally supposed that it would be impossible to recover the function of the ulnar nerve after total brachial plexus avulsion injury, there remained the possibility of using the ulnar nerve as a graft without sacrificing the whole nerve.Materials and MethodsMaterialsA total of20upper extremities in10fresh cadavers that have been dead for5-10days(4males and6females;aged70.6±6.6years old,ranged from59to82years old),provided by the Department of Anatomy,Histology,and Embryology at the Medical College of Fudan University,China,were dissected.This study was carried out in the Anatomy Department of Shanghai Medical College,Fudan University. The study was approved by the Ethics Committee of Fudan University(approval number:2015-064)in July,2015. Surgical techniqueThe modified CC7transfer surgery was carried out in four steps.In the first step,dbUN was fully separated from the UN under a5x magnification loupe and disassociated as distally as possible.The sample was sectioned at the point when it could not be further separated from the UN.In this way,the neuromuscular junction between dbUN and the intrinsic muscles was preserved(Figure1A).In the second step,the dsbUN was dissected at the proximal end of Guyon's Canal where i:was sectioned.The dsbUN was drawn to the contralateral side through the subcutaneous route and then anastomosed w让h CC7(Figure IB).In the third step, the proximal end of UN(peUN)was sectioned and anastomosed with the MN and proximal end of MACN(peMACN) (Figure1C).In the last step,the distal end of MACN (deMACN)was anastomosed with dbUN(Figure ID).The schematic diagram comparing the traditional and modified CC7transfer surgeries is shown in Figure2.Distances from dbUN and peMACN to the midpoint of the line between the medial and lateral epicondyles of the humerus were recorded respectively.It was decided that it would be feasible to suture the deMACN and dbUN directly.In the traditional CC7transfer surgery,the CC7on the intact side was also transected proximal to the point where it joined with other nerves.The whole UN on the injured side was transected at the wrist level and drawn to the supraclavicular area on the intact side through the subcutaneous tunnel.The distal end of CC7was anastomosed with the distal end of the reversed UN.The peUN was anastomosed with the peMN(Figure2B)or other targets(such as musculocutaneous nerve).Silver impregnationAfter these four steps,the axon numbers of bilateral C7 nerves,dsbUN,peUN,peMACN,peMN,deMACN,and dbUN were harvested and stained by the silver impregnation method.The specimens of nerve tissues were obtained and fixed with formalin and then embedded in paraffin blocks.The paraffin blocks were sliced into sections5-8pm thick for pathological studies and mounted on slides.The sections were then gently placed in xylol for5minutes,absolute alcohol for5minutes,95%alcohol for5minutes and washed in distilled water.They were immersed in a mordant,which contained30mL silver nitrate,10drops of2%pyridine and 15drops of absolute alcohol,at60°C until they turned yellow.The samples were quickly washed in95%alcohol,and then impregnated in a solution containing30mL Hortega's strong silver carbonate,10drops pyridine and15drops of absolute alcohol at60°C until they darkened.After rapid washing in95%alcohol,the sample were reduced in10% formol for one to tv/o minutes,washed in distilled water, and left in a2%oxalic acid solution for a few minutes until the sections turned reddish.This step accentuated the1450Hong GH,Liu JB,Liu YZ,Gao KM,Zhao X,Lao/(201刃Modified contralateral C7nerve transfer:the possibility of p ermitting ulnar nerve recovery is confirmed by10cases of autopsy.Neural Regen Res14(8):1449-1454.doi:1 OAl03/1673-5374.253530staining of axons.The sample was fixed,if desired,in a5% solution of sodium thiosulfate,washed in distilled water,dehydrated,cleared and mounted in balsam.All the reagents were provided by the Sinopharm Chemical Reagent Co., Ltd.,Shanghai,China.Axon countingThe total number of axons was calculated for each specimen and counted under200x magnification with Leica Microsystems(LeicaDWLB2,Leica,Heidelberg,Germany).The axon ratio of CC7to dsbUN,peUN axons to the sum of peMACN and peMN,and deMACN to dbUN were calculated. Images were taken using a Motic Med6.0digital medical image analysis system(Xiamen Motic Software Engineering Co.,Ltd.,Xiamen,China),at200x magnification and the number of axons were counted by clicking one by one.The distance between either of two coaptating nerve ends in the bilateral upper extremities of each cadaver was the primary outcome.The numbers of axons in nerve segments distal and proximal to the coaptation sites were also counted. Statistical analysisResults were expressed as the mean±SD,and analyzed using SPSS17.0software(SPSS Inc.,Chicago,IL,USA). ResultsDistances between either of two coaptating nerve endsIn all of the10cadavers,CC7could be transferred to the MN and dbUN on the paralyzed side together with the combined nerve grafts of dsbUN and MACN.The distance between the starting point of dbUN and the midpoint of the line between the medial and lateral epicondyles of the humerus were close to the distance between the branching point of the MACN and the midpoint of the line between the medial and lateral epicondyles of the humerus(Table1).Therefore,the distal end of MACN and the proximal end of dbUN were close to each other,and close to the line between the medial and lateral epicondyles of the humerus,allowing direct suturing between them.This exploratory study of modified CC7transfer surgery was successfully performed in10cadavers.Axon number countingThe representative cross sections of nerve segments were shown in Figure3.The axon numbers were presented in Table2.The matching degree of axonal counts proximal and distal to the anastomosed sites was presented as ratios.The ratio of right C7nerve root to the left dsbUN was19:1.The ratio of left C7nerve root to right dsbUN was17:1.The ratio of peUN to the sum of peMN and peMACN was0.94:1on the left side and0.93:1on right side.The ratio of deMACN to dbUN was0.61:1on the left side and0.65:1on the right side. DiscussionThe traditional CC7transfer surgery,first reported by Gu et al.,has been one of the most important treatments for total brachial plexus avulsion injury(Gu et al.,1991).It has also been performed in many clinical centers all over the world (Yang et al.,2015b;Jiang et al.,2016).It is especially useful when other donor nerves(such as the accessory nerve, phrenic nerve and intercostal nerves)are also injured or not sufficient for repairing all the target nerves.In these cases, no donor nerves are available from the ipsilateral side therefore the CC7from the intact side becomes the best available source for transfer(Cambon-Binder et al.,2018;Dahlin et al.,2018;Socolovsky et al.,2018).According to Terzis et al.'s report,fair(M2+to M3),good(M3*to M4)and excellent (M4f to M5)outcomes have been achieved in a total of56 cases of brachial plexus nerve injuries where the functional recovery rates(M3or more)were74%in biceps,57%in triceps,50%in deltoids,62%in wrists and finger flexors,and 50%in wrists and finger extensors,respectively(Terzis et al., 2000).In the traditional technique of CC7transfer surgery, Gu and co-workers(1991)used the entire CC7elongated by a vascularized ulnar nerve graft from the paralyzed upper extremity.Therefore,the recovery potential of the intrinsic muscles innervated by the UN was completely sacrificed,as the physical connectivity between dbUN and the intrinsic muscles is the primary foundation for the restoration of the hand functions.However,the C7nerve contains27,000-41,000nerve fibers,which is an abundant source to reconstruct not only a single recipient but also multiple recipients(Chen et al., 2007;Xu et al.,2008).Gao et al.(2013a)reported that acceptable outcomes have been achieved by CC7transferred to the musculocutaneous nerve and MN.This meant that the benefit of CC7transfer grew from repairing a single nerve to multiple nerves.However,in the traditional CC7 transfer surgery,the whole UN was harvested as the grafted nerve to restore the function of a single MN on the paralyzed side.Although this might have wasted some of the fibers of the CC7nerve,it was trad让ionally supposed that it was impossible for the UN on the injured side to recover after high-level injury(Woo et al.,2015;Bertelli et al.,2018). Therefore,the whole UN was sacrificed and used as a graft. As the microsurgical techniques and research in the nerve regeneration have progressed(such as brain reorganization theory,nerve conduit,electrical nerve stimulation,stem cell transplantation,ultrasound treatment,and tissue engineering techniques),it was realized that there was greater potential for the recovery of the UN(Li et al.,2015;Zhang et al., 2015;Geuna et al.,2016;Jiang et al.,2017;Zhou et al.,2017;Bergmeister et al.,201&Choi et al.,201&Yu et al.,2018). Therefore,there was a need to devise a method to preserve the recovery possibility of the UN nerve on the injured side. The present study provided a strategy for modifying the traditional method of CC7transfer.In our study on cadavers,we have verified that the connection between dbUN and intrinsic muscles could be retained,thus the recovery potential of dbUN was preserved.A combination of dsbUN and MACN was used as nerve grafts for reinnervating both the MN and dbUN simultaneously.Through this modified CC7transfer surgery,we aimed to preserve innervation of the hypothenar,adductor pollicis,palmar interosseous,dorsal interosseous and the3/4 of the lumbrical muscles.The cut ends of dbUN and MACN were located at the elbow so that they could be directly anastomosed without1451Hong GH,Liu JB,Liu YZ,Gao KM,Zhao X,Lao J(2019)Modified contralateral C7nerve transfer:the possibility of p ermitting ulnar nerve recovery is confirmed by10cases of autopsy.Neural Regen Res14(8):1449-1454.doi:10.4103/1673-5374.253530Figure1Demonstration of modified contralateral C7(CC7)nerve root transfer.(A)Exposure of the full length of ulnar nerve(UN)and the medial antebrachial cutaneous nerve(MACN).The deep branch of UN(dbUN) was separated from the main trunk.The distal and superficial branches of UN(dsbUN)were transected at the wrist level.(B)The contralateral C7nerve was transected proximal to the point where it joined with other nerves.The distal end of the dsbUN was drawn to the supraclavicular area of the contralateral side through the subcutaneous tunnel and anastomosed with the CC7.(C)The UN was reversed and the proximal end of ulnar nerve(peUN)was transected and anastomosed with the proximal end of MACN(peMACN)and proximal end of median nerve(peMN)simultaneously at the upper arm level.(D)The distal end of MACN(deMACN)was anastomosed w让h proximal end of dbUN.CC7IdsbUNpeMACN’Figure2Comparison of the modified and traditional contralateralC7(CC7)nerve transfer surgeries.(A)Demonstration of modified CC7nerve transfer 7on the intact side was transected proximal to the point where it joined with other nerves.The distal and superficial branches of ulnar nerve (dsbUN)on the injured side were transected at the wrist level and drawn to the supraclavicular area of the contralateral side through the subcutaneous tunnel.The deep branch of UN(dbUN)was dissected from the main trunk of ulnar nerve(UN).The distal end of CC7was anastomosed with the dsbUN.The proximal end of UN(peUN)was anastomosed w让h both the proximal end of median nerve(peMN)and the proximal end of medial antebrachial cutaneous nerve(peMACN). The distal end of medial antebrachial cutaneous nerve(deMACN)was then anastomosed with the dbUN.(B)Demonstration of traditional CC7nerve transfer surgery.The CC7on the intact side was also transected proximal to the point where it joined w让h other nerves.The whole UN was transected at the wrist level and drawn to the supraclavicular area of the contralateral side through the subcutaneous tunnel. The distal end of CC7was anastomosed with the distal end of the reversed UN.Then the peUN was anastomosed with the peMN.The continuous lines indicated the nerve path after nerve transfer surgery. The dash line indicated the original position of the UN before nerve transfer surgery.additional nerve grafts.In the axon count study,the number of axons in CC7was sufficient to be used as a donor.Moreover,the sum of MN and dbUN axon numbers matched with that of the nerve grafts,i.e.the combination of MACN and dsbUN.At the medial aspect of the paralyzed upper arm,we simultaneously anastomosed peUN w让h peMN and peMACN.The axon number of peUN also matched with the sum of peMN and peMACN.As MACN and UN originate from the medial cord of brachial plexus,UN could be readily anastomosed with MACN at the same level of the upper arm.Since the axon number of deMACN and dbUN roughly matched(0.6:1),dbUN could be anastomosed with deMACN after separation.Therefore,it was anatomically feasible to anastomose deMACN w让h dbUN,according to the principle that the axon number of donor nerve should equal to at least3C%of that in the recipient nerve(Zhang et al.,2011;Chuang et al.,2012;Benedikt et al.,2017).There were several advantages using dsbUN combined with MACN as the grafzed nerve to reinnervate multiple recipient nerves using this modified CC7transfer surgery.First,the dbUN was preserved so that the recovery potential of intrinsic muscles innervated by dbUN was not completely sacrificed. Second,the anatomical location of the grafted nerve remains unchanged.Third,the blood supply of the grafted nerve could be largely preserved.Finally,no extra incisions were needed and the source of CC7was fully utilized.The modified CC7transfer surgery still has some shortcomings.The deep,superficial and dorsal branches of the UN were very complex at the meeting point,i.e.,10cm proximal to the wrist,making it difficult to dissect from the main trunk of UN.The dissecting procedure should be carried out carefully under the loupe magnification to acquire as many nerve bundles as possible.After separation of the dbUN,nerve fibers on the distal end of UN left for grafting was less than those in the traditional method.Whether让would eventually Table1Distances from the deep branch of ulnar nerve(dbUN)and the proximal end of medial antebrachial cutaneous nerve(peMACN) to the midpoint of the line between the medial and lateral epicondyles of the humerusCadaver No.dbUN(mm)peMACN(mm)Left Right Left Right 141312218 239411919 349523529 451422835 539312928 654433631 747473735 853384028 943393229 1049344323Mean±SD46.5±5.6439.8±6.7532.1±7.6727.5±5.89 Numbers indicate a distance proximal to the line between the medial and lateral epicondyles of the humerus.1452Hong GH,Liu JB,Liu YZ,Gao KM,Zhao X,Lao J(201刃Modified contralateral C7nerve transfer:the possibility of p ermitting ulnar nerve recovery is confirmed by10cases of autopsy.Neural Regen Res14⑻:1449-1454.doi:10.4103/1673-5374.253530Figure3Histology of axons in the nerves after silver impregnation under optical microscope involved in the modified contralateral C7nerve transfer surgery.All axons of involved nerves were stained by silver impregnation.(A) Cross-sectional view of the C7nerve root;(B)cross-sectional view of dorsal and superficial branches of ulnar nerve;(C)cross-sectional view of proximal end of ulnar nerve;(D)cross-sectional view of the proximal end of median nerve;(E)cross-sectional view of the proximal end of medial antebrachial cutaneous nerve;(F)cross-sectional view of the distal end of medial antebrachial cutaneous nerve;(G)cross-sectional view of the deep branch of ulnar nerve;(H)demonstration of the Leica Microsystems used in the slice observation.Yellow arrows indicate axons in cross sections of nerves.Original magnification:200x.Scale bars:200pm.affect the functional recovery of the recipient nerve or not would need clinical evaluation.The comparison of advantages and disadvantages of the modified and traditional CC7transfer surgeries has been presented in Table3.When this modified CC7transfer surgery is applied in clinical practice,a two-stage surgery is suggested for the modified CC7transfer.In the first stage,the dbUN is labeled and fixed subcutaneously by a suturing line nearby the elbow joint.The dsbUN should be drawn to the contralateral side through anterior cervical subcutaneous tunnel and anastomosed with CC7nerve.In the second stage,the peUN is anastomosed with MN and peMACN simultaneously and then deMACN was anastomosed with dbUN,which has been labeled a suturing line.This surgical approach is clinically feasible. However,the present study was only an anatomical investigation.There might still be limitations for extrapolating this surgery in clinical practice.Recovery of the intrinsic muscles in the injured upper extremity is still uncertain due to the long distance from the donor nerve to the recipient nerve.The restoration of intrinsic muscle of the paralyzed hand is still a difficult problem for total brachial plexus avulsion injuries(Giuffre et al.,2010;Aszmann et al.,2015; Dy et al.,2015;Franzblau et al.,2015;Yang et al.,2016). The present study verified the feasibility of a modified CC7 transfer surgery on cadavers.In conclusion,it is anatomically feasible that the CC7can be transferred to the MN and the dbUN grafted by dsbUN combined with MACN from the paralyzed side.This approach may provide a theoretical and practical basis for preserving the recovery potential of the intrinsic muscles with a modified CC7transfer surgery. Author contributions:Study design:]L and GHH;experimental implementation:GHH and KMG;data analysis and paper writing:JBL,YZL and XZ. All authors approved the final version of t he paper.Conflicts of interest:The authors declare that there are no conflicts of interest associated with this manuscript.Financial support:This study was supported by the National Natural Science Foundation of China,No.81572127(to JL).The funder played no role in the study conception and design,collection,analysis and interpretation of data in the writing of the paper,and in the decision to submit the paper for publication.Institutional review board statement:The study protocol was approved byTable2Number of axons in the nerves involved in the modified contralateral C7nerve root transfer surgeryC7nerve root dsbUN peUN peMN peMACN deMACN dbUNLeft23496±31021284±2093602±1622372±2691424±192862±961411±186Right24831±291021389±2353186±1292163±2131245±176897±861371±148Data are expressed as the mean±SD.dsbUN:Dorsal and superficial branches of ulnar nerve;peUN:proximal end of ulnar nerve;peMN:proximal end of median nerve; peMACN:proximal end of medial antebrachial cutaneous nerve;deMACN:distal end of medial antebrachial cutaneous nerve;dbUN:deep branch of ulnar nerve. Table3Comparison of advantages and disadvantages between modified and traditional contralateral C7nerve transfer surgeries Modified contralateral C7nerve transfer surgery Traditional contralateral C7nerve transfer surgery Advantages(1)Deep branch of ulnar nerve on the injured side is spared to preserve the(1)The whole lunar nerve is used to maximize the possibility of potential recovery of intrinsic muscles.grafting pathway.(2) Anatomical location of grafted nerve is retained.(2)Procedure of disassociation of deep branch from(3) Blood supply of the grafted nerve can be largely preserved.the main trunk of ulnar nerve is spared.(4) No extra incisions are needed and the source of contralateral C7is fully utilized.(3)Shorter operating duration and less skill demanding. Disadvantages(1)Demands more skill and time consuming;The function of the original target of the donor nerve(2)Whether it would eventually affect the functional recovery of the recipient nerve(ulnar nerve)is completely sacrificed,or not needs further evaluations.1453Hong GH,Liu JB,Liu YZ,Gao KM,Zhao X,Lao J(201刃Modified contralateral C7nerve transfer:the possibility of p ermitting ulnar nerve recovery is confirmed by10cases of autopsy.Neural Regen Res14(8):1449-1454.doi:10.4103/1673-5374.253530the Ethics Committee of F udan University of C hina(approval number:2015-064)in July,2015.Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.Data sharing statement:Datasets analyzed during the current study are available f rom the corresponding author on reasonable request.Plagiarism check:Checked twice by iThenticate.Peer review:Externally peer reviewed.Open access statement:This is an open access journal,and articles are distributed under the terms of t he Creative Commons Attribution-^on-Com-mercial-ShareAlike4.0License,which allows others to retnix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms. ReferencesAszmann OC,Roche AD2,Salminger S et al.(2015)Bionic reconstruction to restore hand function after brachial plexus injury:a case series of three patients.Lancet385:2183-2189.Benedikt S,Parvizi D,Feigl G,Koch H(201刀Anatomy of the medial antebrachial cutaneous nerve and its significance in ulnar nerve surgery:an anatomical study.J Plast Reconstr Aesthet Surg70:1582-1588.Bergmeister KD,Daeschler SC,Rhodius P,Schoenle P,Bocker A,Kneser U,Har-haus L(2018)Promoting axonal regeneration following nerve surgery:a perspective on ultrasound treatment for nerve injuries.Neural Regen Res13:1530-1533.Bertelli JA,Tavares KE(2018)Little finger abduction and adduction testing in ulnar nerve lesions.Hand Surg Rehabil doi:10.1016/j.hansur.2018.09.006. Cambon-Binder A,Preure L,Dubert-Khalifa H,Marcheix PS,Belkheyar Z(2018) Spinal accessory nerve repair using a direct nerve transfer from the upper trunk:results with2years follow-up.J Hand Surg Eur43:589-595.Chen L,Gu YD,Hu SN,Xu JG,Xu L,Fu Y(2007)Contralateral C7transfer for the treatment of brachial plexus root avulsions in children:a report of12cases.J Hand Surg Am32:96-103.Choi J,Kim JH,Jang JW,Kim HJ,Choi SH,Kwon SW(2018)Decellularized sciatic nerve matrix as a biodegradable conduit for peripheral nerve regeneration.Neural Regen Res13:1796-1803.Chuang DC,Hernon C(2012)Minimun4-year follow-up contralateral C7nerve transfers for brachial plexus injuries.J Hand Surg Am37:270-276.Dahlin LB,Andersson G,Backman C,Svensson H,Bjorkman A(2018)Rehabilitation,using guided cerebral plasticity,of a brachial plexus injury treated with intercostal and phrenic nerve transfers.Front Neurol8:72.Dy CJ,Garg R,Lee SK,Tow P,Mancuso CA,Wolfe SW(2015)A systematic review of outcomes reporting for brachial plexus reconstruction.I Hand Surg Am40:308-313.Franzblau LE,Maynard M,Chung KC,Yang LJ(2015)Medical treatment decision making after total avulsion brachial plexus injury:a qualitative study.J Neurosurg122:1413-1420.Gao KM,Lao J,Gu YD(2006)Long-term outcome of contralateral C7nerve transfer.Chin J Hand Surg22:195-197.Gao KM,Lao J,Zhao X,Gu YD(2013a)Outcome of contralateral C7transfer to two recipient nerves in22patients with the total brachial plexus avulsion injury.Microsurgery33:605-611.Gao KM,Lao J,Zhao X,Gu Y(2013b)Outcome after transfer of intercostal nerves to the nerve of triceps long head in25adult patients with total brachial plexus root avulsion injury.J Neurosurg118:606-610.Gao KM,Hu JJ,Lao J,Zhao X(2018a)Evaluation of nerve transfer options for treating total brachial plexus avulsion injury:a retrospective study of73participants.Neural Regen Res13:470-476.Gao KM,Lao J,Guan WJ,Hu JJ(2018b)Is it necessary to use the entire root as a donor when transferring contralateral C7nerve to repair median nerve?Neural Regen Res13:94-99.Geuna S,Raimondo S,Fregnan F,Haastert-Talini K,Grothe C(2016)In vitro models for peripheral nerve regeneration.Eur J Neurosci43:287-296.Giuffre JL,Kakar S,Bishop AT,Spinner RJ,Shin AY(2010)Current concepts of the treatment of adult brachial plexus injuries.J Hand Surg Am35:678-688.Gu YD,Zhang GM,Chen DS,Cheng XM,Zhang LY,Yan JG(1991)Cervical nerve root transfer from contralateral normal side for treatment of brachial plexus root avulsions.Chin Med J(Engl)104:208-211.Hu SN,Gu YD(2014)Contralateral C7transfer for treatment of brachial plexus root avulsion.Handchir Mikrochir Plast Chir46:80-84.Huang J,Zhang Y,Lu L,et al(2013)Electrical stimulation accelerates nerve regeneration and functional recovery in delayed peripheral nerve injury in rats.Euro J Neurosci38:3691-3701.Jiang L,Jones S,Jia X(2C17)Stem cell transplantation for peripheral nerve regeneration:current options and opportunities.Int J Mol Sci18:94.Jiang Y,Wang L,Lao J,Zhao X(2016)Comparative study of intercostal nerve transfer to lower trunk and contralateral C7root transfer in repair of total brachial plexus injury in rats.J Plast Recon s tr Aesthet Surg69:623-628.Li T,Hua X,Zheng M,Wang W,Xu J,Gu Y,Xu W(2015)Different cerebral plasticity of intrinsic and extrinsic hand muscles after peripheral neurotization in a patient with brachial plexus injury:a TMS and fMRI study.Neurosci Lett 604:140-144.Li WJ,He LY,Chen SL,et al(2017)Contralateral C7Nerve Root Transfer for Function Recovery in Adults:A Meta-analysis.Chin Med J(Engl)130:2960-2968.Shin AY,Spinner RJ,Steinmann SP,Bishop AT(2005)Adult traumatic brachial plexus injuries.J Am Acad Orthop Surg13:382-396.Socolovsky M,Malessy M,Bonilla G,Di Masi G,Conti ME,Lovaglio A(2018) Phrenic to musculocutaneous nerve transfer for traumatic brachial plexus injuries:analyzing respiratory effects on elbow flexion control.J Neurosurg doi:10.3171/2018.4.JNS173248.Spinner RJ,Shin AY,Bishop AT(2005)Update on brachial plexus surgery in adults.Tech Hand Up Ext r em Surg9:220-230.Terzis JK,Papakonstantinou KC(2000)The surgical treatment of brachial plexus injuries in adults.Plast Reconstr Surg106:1097-1122.Terzis JK,Kokkalis ZT(2C09)Selective contralateral C7transfer in posttraumatic brachial plexus injuries:a report of56cases.Plast Reconstr Surg123:927-938. Tu YK,Tsai YJ,Chang CH,Su FC,Hsiao CK,Tan JS(2014)Surgical treatment for total root avulsion type brachial plexus injuries by neurotization:a prospective comparison study between total and hemicontralateral C7nerve root transfer.Microsurgery34:91-101.Vanaclocha V,Herrera JM,Verdu-Lopez F,Gozalbes L,Sanchez-Pardo M,Rivera M(2015)Transdiscal C6-C7contralateral C7nerve root transfer in the surgical repair of brachial plexus avulsion injuries.Acta Neurochir(Wien)157:2161-2167.Wang G,Yu A,Ng CY,Lei G,Wang X,Qiu Y,Feng J,Li T,Chen Q,He Q, Ding F,Cui S,Gu Y,Xu J,Jiang S,Xu W(2018)Contralateral C7to C7nerve root transfer in reconstruction for treatment of total brachial plexus palsy: anatomical basis and preliminary clinical results.J Neurosurg Spine doi:10.3171/2018.3.SPINE171251.Wang L,Jiang Y,Lao J,Zhao X(2014)Contralateral C7transfer to lower trunk via the prespinal route in the repair of brachial plexus injury:an experimental study in rats.J Plast Reccnstr Aesthet Surg67:1282-1287.Wang SF,Li PC,Xue YH,Yiu HW,Li YC,Wang HH(2013)Contralateral C7 nerve transfer with direc:coaptation to restore lower trunk function after traumatic brachial plexus avulsion.J Bone Joint Surg Am95:821-827.Woo A,Bakri K,Moran SL(2015)Management of ulnar nerve injuries.J Hand Surg Am40:173-81.Xu L,Gu Y,Xu J,Lin S,Chen L,Lu J(2008)Contralateral C7transfer via the prespinal and retropharyngeal route to repair brachial plexus root avulsion:a preliminary report.Neurosurgery63:553-558.Yang G,Chang KW,Chung KC(2015a)A systematic review of outcomes of contralateral c7transfer for the treatment of traumatic brachial plexus injury:part2.donor-site morbidity.Plast Reconstr Surg136:480e-489e.Yang G,Chang KW,Chung KC(2015b)A systematic review of contralateral c7 transfer for the treatment of traumatic brachial plexus injury:part1.overall outcomes.Plast Reconstr Surg136:794-809.Yang H,Gil Y,Kim S,Bang J,Choi H,Lee HY(2016)From the brachial plexus to the hand,multiple connections between the median and ulnar nerves may serve as bypass routes for nerve fibres.J Hand Surg Eur Vol41:648-656.Yu AP,Qiu YQ,Li J,Shen YD,Wang XM,Cong M,He QR,Chen Q乙Ding F,Gu YD,Xu JG,Jiang S,Xu WD(2018)Comparative effects of implanted electrodes with differing contact patterns on peripheral nerve regeneration and functional recovery.Neurosci Res doi:10.1016/j.neures.2018.08.007.Zhang CG,Gu YD(2011)Contralateral C7nerve transfer-Our experiences over past25years.J Brachial Plex Peripher Nerve Inj6:10.Zhang J,Chen L,Gu Y(2015)Influence of contralateral homologous cortices on motor cortical reorganization after brachial plexus injuries in rats.Neurosci Lett606:18-23.Zheng MX,Hua XY,Feng JT,Li T,Lu YC,Shen YD,Cao XH,Zhao NQ,Lyu JY, Xu JG,Gu YD,Xu WD(2018)Trial of contralateral seventh cervical nerve transfer for spastic arm paralysis.N Engl J Med378:22-34.Zhou J,Cui H,Lu H,Xu Z,Feng W,Chen L,Jin X,Yang X,Qi Z(2017)Muscle-derived stem cells in peripheral nerve regeneration:reality or illusion?Regen Med12:459-472.C-Editor:Zhao M;S-Editors:Wang/,Li CH;L-Editors:Dawes EA,Qiu Y,Song LP;T-Editor:Liu XL1454。
浙江大学一级学术期刊和核心期刊目录

浙江大学一级学术期刊和核心期刊目录(2008版)一、国内一级期刊340种(其中带*号的为人文社科权威级期刊19种):1 法学研究*2 管理世界*3 教育研究*4 经济研究*5 历史研究*6 社会学研究*7 体育科学*8 外国文学评论*9 外语教学与研究*10 文学评论*11 心理学报*12 新华文摘*13 新闻与传播研究*14 哲学研究*15 政治学研究*16 中国社会科学*17 中国社会科学文摘*18 中国图书馆学报*19 中国语文*20 半导体学报21 北京体育大学学报22 比较教育研究23 兵工学报24 病毒学报25 材料研究学报(材料科学进展)26 财贸经济27 蚕业科学28 测绘学报29 茶叶科学30 城市规划31 传感技术学报32 催化学报33 大气科学34 大学图书馆学报35 当代电影36 当代语言学(原为:国外语言学)37 档案学通讯38 低温工程39 地理科学40 地理学报41 地理研究42 地球化学43 地球物理学报44 地震学报45 地质科学46 地质学报47 电工技术学报48 电力系统自动化49 电路与系统学报50 电信科学51 电子学报52 电子与信息学报(原名电子科学学刊)53 动力工程54 动物学报55 动物学研究56 动物营养学报57 敦煌研究58 纺织学报59 分析化学60 复合材料学报61 钢铁62 高等工程教育研究(武汉)63 高等教育研究(武汉)64 高等学校化学学报65 高分子学报66 高能物理与核物理67 高校化学工程学报68 高校应用数学学报69 工程热物理学报70 古汉语研究71 古生物学报72 固体力学学报73 管理科学学报74 光电工程75 光电子·激光76 光学学报77 光子学报78 硅酸盐学报79 国际贸易问题80 国际问题研究81 果树学报(原名:果树科学)82 海洋工程83 海洋学报84 海洋与湖沼85 航空学报86 航天医学与医学工程87 核农学报88 红外与毫米波学报89 化工学报90 化学物理学报91 化学学报92 环境科学93 环境科学学报94 会计研究95 机械工程学报96 计量学报97 计算机辅助设计与图形学学报98 计算机集成制造系统99 计算机科学技术学报(英文版) 100 计算机学报101 计算机研究与发展102 计算数学103 建筑结构学报104 建筑学报105 教育发展研究106 解剖学报107 金融研究108 金属学报109 近代史研究110 经济地理111 经济理论与经济管理112 经济社会体制比较113 经济学家114 菌物学报(原名:菌物系统) 115 考古学报116 科学通报117 科学学研究118 科研管理119 空间科学学报120 空气动力学学报121 控制理论与应用122 控制与决策123 矿物学报124 昆虫分类学报125 昆虫学报126 力学学报127 林业科学128 马克思主义研究129 麦类作物学报130 煤炭学报131 美术研究132 棉花学报133 民族研究134 模式识别与人工智能135 摩擦学学报136 内燃机工程137 内燃机学报138 农药学报139 农业工程学报140 农业机械学报141 农业经济问题142 农业生物技术学报143 气象学报144 汽车工程145 强激光与粒子束146 情报学报147 燃料化学学报148 热力发电149 人口研究150 软件学报151 社会科学战线152 生理学报153 生态学报154 生物多样性155 生物工程学报156 生物化学与生物物理学报157 生物物理学报158 声学学报159 石油学报160 实验生物学报161 史学理论研究162 世界经济163 世界经济与政治164 世界历史165 世界宗教研究166 兽类学报167 数量经济技术经济研究168 数学进展169 数学年刊(A、B辑)170 数学物理学报171 数学学报172 水产学报173 水动力学研究与进展(英文版) 174 水科学进展175 水力发电学报176 水利学报177 水生生物学报178 水土保持学报179 台湾研究180 太阳能学报181 天文学报182 通信学报183 统计研究184 土木工程学报185 土壤学报186 外国文学187 外国文学研究188 外国语189 微波学报190 微生物学报191 文史(中华书局)192 文献193 文学遗产194 文艺理论研究195 文艺研究196 无机材料学报197 无机化学学报198 物理化学学报199 物理学报200 系统工程理论与实践201 系统科学与数学202 细胞生物学杂志203 现代外语204 心理科学205 新美术206 畜牧兽医学报207 学术月刊208 岩石力学与工程学报209 岩石学报210 岩土工程学报211 遥感学报212 药物分析杂志213 药学学报214 仪器仪表学报215 遗传216 遗传学报217 应用生态学报218 应用数学学报219 应用数学与力学(英文版)220 应用心理学221 营养学报222 有机化学223 宇航学报224 语言研究225 园艺学报226 浙江大学学报(人文社会科学版)227 浙江大学学报(工学版)228 浙江大学学报(英文版)229 真空科学与技术学报230 振动工程学报231 政法论坛232 植物保护学报233 植物病理学报234 植物分类学报235 植物生理与分子生物学学报(原名:植物生理学报) 236 植物生态学报237 植物学报238 植物营养与肥料学报239 中草药240 中共党史研究241 中国病理生理杂志242 中国出版243 中国电机工程学报244 中国法学245 中国翻译246 中国腐蚀与防护学报247 中国高教研究248 中国工业经济249 中国公路学报250 中国光学快报(英文版)251 中国广播电视学刊252 中国化学快报(英文版)253 中国环境科学254 中国机械工程255 中国激光256 中国寄生虫学与寄生虫病杂志257 中国经济史研究258 中国科学(A-G)辑259 中国粮油学报260 中国农村经济261 中国农业科学262 中国人口科学263 中国人民大学报刊复印资料(全文复印) 264 中国社会科学季刊(香港)现已停刊265 中国社会科学评论(香港)266 中国生物防治267 中国生物化学与分子生物学报268 中国生物医学工程学报269 中国食品学报270 中国史研究271 中国兽医学报272 中国水稻科学273 中国体育科技274 中国图像图形学报275 中国土地科学276 中国物理快报(英文版)277 中国稀土学报278 中国现代文学研究丛刊279 中国畜牧杂志280 中国药理学报281 中国药理学与毒理学杂志282 中国药学杂志283 中国音乐学284 中国应用生理学杂志285 中国有色金属学报286 中国预防兽医学报287 中国运动医学杂志288 中国中西医结合杂志289 中国中药杂志290 中华病理学杂志291 中华超声影像学杂志292 中华传染病杂志293 中华创伤杂志294 中华儿科杂志295 中华耳鼻咽喉头颈外科杂志296 中华放射学杂志297 中华放射医学与防护杂志298 中华妇产科杂志299 中华骨科杂志300 中华护理杂志301 中华急诊医学杂志(原名: 急诊医学) 302 中华检验医学杂志303 中华结核和呼吸杂志304 中华精神科杂志305 中华口腔医学杂志306 中华劳动卫生职业病杂志307 中华流行病学杂志308 中华麻醉学杂志309 中华泌尿外科杂志310 中华内分泌代谢杂志311 中华内科杂志312 中华皮肤科杂志313 中华普通外科杂志314 中华烧伤杂志315 中华神经科杂志316 中华神经外科杂志317 中华肾脏病杂志318 中华外科杂志319 中华微生物学和免疫学杂志320 中华物理医学与康复杂志321 中华消化杂志322 中华小儿外科杂志323 中华心血管病杂志324 中华胸心血管外科杂志325 中华血液学杂志326 中华眼科杂志327 中华医学遗传学杂志328 中华医学杂志329 中华医院管理杂志330 中华预防医学杂志331 中华整形外科杂志332 中华肿瘤杂志333 中外法学334 自动化学报335 自然辩证法通讯336 自然辩证法研究337 自然科学进展338 自然灾害学报339 自然资源学报340 作物学报注:被IM收录的论文视同国内一级期刊论文。
湖南省职称论文认可期刊

16
Journal of Genetics and Genomics遗传学报(英文版)
11-5450/R
17
Journal of Integrative Medicine结合医学学报(英文)(曾用刊名中西医结合学报)
31-2083/R
18
Journal of Otology中华耳科学杂志(英文版)
13-1214/R
168
河南大学学报(医学版)
41-1361/R
169
河南科技大学学报(医学版)
41-1363/R
170
河南外科学杂志
41-1235/R
171
河南医学研究
41-1180/R
172
河南预防医学杂志
41-1220/R
173
河南职工医学院学报
41-1292/R
174
河南中医
41-1114/R
44-1550/R
197
华西口腔医学杂志
51-1169/R
198
华西药学杂志
51-1218/R
199
华西医学
51-1356/R
200
华夏医学
45-1236/R
201
华中科技大学学报(医学版)
42-1678/R
202
华中科技大学学报(医学英德文版)
42-1679/R
203
化工与医药工程(曾用刊名医药工程设计)
附件
湖南省卫生计生系列高级职称评审论文发表
认可期刊目录
序号
期刊名称
期刊号
1
Asian Journal of Andrology亚洲男性学杂志(英文版)
31-1795/R
枸杞多糖对周围神经损伤修复的研究进展

Doi:10.13621/j.1001-5949.2020.10.0960•综述.枸杞多糖对周围神经损伤修复的研究进展张立鹏",彭凯",张博闻1,2,黄永禄",巩凡1,2,李晓亮",高剑1,2,丁一1,2,张汉霖】,2,杨海蓉3,赵飞1,2[关键词]枸杞多糖;周围神经;损伤修复[中图分类号]R745.3[文献标识码]A枸杞既可食用又可药用,作为中药材在我国具有悠久的使用历史。
枸杞多糖作为枸杞的活性成分,在促进造血、降低血脂、保护肝脏、抗击癌症及修复周围神经方面有广泛的药理学作用[1-2]o近年来,枸杞多糖的研究已逐步开展,并有大量实验数据证实了枸杞多糖的功效。
本文就枸杞多糖对周围神经的修复的研究进展进行综述,为此方面进一步研究而提供参考或依据。
1通过免疫调节研究发现周围神经受损伤后,免疫系统发生着一连串复杂的病理生理改变,例如神经末梢变性、髓鞘损伤、T细胞浸润、巨噬细胞聚集及免疫球蛋白沉积等一系列免疫反应,从而影响神经修复和再生。
当鼠坐骨神经损伤后,受伤局部的血-神经屏障会被破坏,致神经丧失免疫豁免功能,使受伤局部免疫反应增强,阻碍神经细胞的再生与修复叫在大鼠坐骨神经损伤急慢性期内的细胞免疫反应中CD4、CD s在促进坐骨神经修复过程中具有协调免疫反应的功效⑷。
程爱华等⑸通过动物实验研究表明,小鼠坐骨神经损伤后,激活机体的免疫活性及功能,IL-2增多,抑制坐骨神经的恢复,而枸杞多糖可在坐骨神经损伤后,机体免疫反应增强时,它可适当调节并降低机体的免疫反应,降低IL-2含量,促进受损神经组织细胞的功能恢复。
2通过抑制氧化应激氧化应激反应是身体为适应外部环境变化的应激状态,主要表现为自由基和超氧化物(ROS)的产生和去除之间的动态平衡被破坏,导致体内活性氧的大量积累,引起膜内外物质的交换异常,产生神经毒性作用,使周围神经细胞损伤。
经动物实验证实枸[基金项目]宁夏自然科学基金项目(NZ16177、NZ17197);卫生部 手功能重建重点实验室及上海市周围神经显微外科重点实验室开放课题(DDZ2270500);中央高校基本科研业务费专项资金项目(21920190181);宁夏回族自治区医院培育振兴项目(2018014)[作者单位]1.宁夏回族自治区人民医院手、足和重建显微外科,宁夏银川7500022•西北民族大学第一附属医院,宁夏银川750002[通讯作者]赵飞,Email:***************杞多糖清除氧自由基的作用较强,不仅通过抑制氧自由基的生成来保证细胞正常代谢和功能,而且通过协调体内自由基的代谢,大大减少氧自由基对人体的过氧化损伤卩保证细胞正常生理功能,也稳定了受损神经细胞的代谢。
脑卒中的辅助治疗:重复经颅磁刺激
NEURAL REGENERATION RESEARCH Volume 7, Issue 8, March 2012Cite this article as: Neural Regen Res. 2012;7(8):627-634.627Joonho Shin ☆, M.D.,Department of Rehabilitation Medicine, Bundang Hospital, College of Medicine, Seoul National University, Seongnam 463-707, Republic of KoreaCorresponding author:Nam-Jong Paik, M.D., Ph.D., Department of Rehabilitation Medicine, Bundang Hospital, College of Medicine, Seoul National University, 300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do, 463-707, Republic of Korea njpaik@snu.ac.krReceived: 2011-11-05 Accepted: 2012-02-03 (NY20111011004/H)Shin J, Yang EJ, Cho KH, Barcenas CL, Kim WJ, Min Y , Paik NJ. Clinical application of repetitive transcranial magnetic stimulation instroke rehabilitation. Neural Regen Res.2012;7(8):627-634.doi:10.3969/j.issn.1673-5374.2012.08.011Clinical application of repetitive transcranial magnetic stimulation in stroke rehabilitation*☆●Joonho Shin, EunJoo Yang, KyeHee Cho, Carmelo L Barcenas, Woo Jin Kim, Yusun Min, Nam-Jong PaikDepartment of Rehabilitation Medicine, Bundang Hospital, College of Medicine, Seoul National University, Seongnam 463-707, Republic of KoreaAbstractProper stimulation to affected cerebral hemisphere would promote the functional recovery ofpatients with stroke. Effects of repetitive transcranial magnetic stimulation on cortical excitability can be can be altered by the stimulation frequency, intensity and duration. There has been no consistent recognition regarding the best stimulation frequency and intensity. This study reviews the intervention effects of repetitive transcranial stimulation on motor impairment, dysphagia,visuospatial neglect and aphasia, and summarizes the stimulation frequency, intensity and area for repetitive transcranial magnetic stimulation to yield the best therapeutic effects.Key Words: stroke; repetitive transcranial magnetic stimulation; rehabilitation; reviewAbbreviations: rTMS, repetitive transcranial magnetic stimulation; TBS, theta burst stimulation; fMRI, functional magnetic resonance imagingINTRODUCTIONMany interventions, such as pharmacological treatments, physical and behavioral therapies have been largely applied to improve diverse post-stroke neurologic deficits, including visuospatial neglect, aphasia, dysphagia and motor impairment, using brain plasticity [1]. Occurrence of cortical reorganization after stroke [2] has beenreported in previous studies and suggested that increased cortical activity in the affected cerebral hemispheres would promote recovery from stroke [3].Repetitive transcranial magnetic stimulation (rTMS) has gained growing importance in the field of stroke rehabilitation. Based on the ability to modulate excitability, the useful therapeutic effect of TMS has beenproposed by many studies as a potential treatment for various disorders of stroke [4], such as motor performance [5-8], dysphagia [9] and neglect [10]. Although the concepts of interhemispheric inhibition and change in synaptic plasticity are considered possible mechanisms, no complete interpretation of rTMS has been formulated [11-12].Effects of rTMS on cortical excitability can be altered by the stimulation frequency, intensity and duration [13]. However, a recent review concluded that the evidence remains insufficient regarding the optimum frequency or ‘dose’ of rTMS [14]. In this article, the effects of rTMS on various dysfunctionspost-stroke in adult patients are reviewed.EFFECTS OF RTMS ON MOTOR IMPAIRMENT POST-STROKE(Table 1)Natural recovery is no longer expected in many chronic stroke patients. Sustained improvement for up to 3 months was observed in one study [15]. rTMS exhibits much stronger and longer lasting effects in patients with acute stroke. Khedr et al [16] demonstrated that the yield of 1 Hz rTMS was 48.3% larger than sham stimulation, in terms of Barthel index in acute stroke, and the sustained effects lasted for over 1 year beyond the stimulation [6].The results were consistent regardless of injury site, showing improvement in not only cortical, but subcortical stroke and pontine hemorrhagic patients, due to the control of corticospinal excitability, although no direct stimulation to deep structure prevailed [7, 17]. However, some studies showed a gap between the functional results andcorticospinal excitability [5, 18], and the results of rTMS in stroke patients did not seem to be related to the regional blood flow. The mechanism underlying the motor recovery after rTMS application needs further investigation. Various frequencies between 1 to 20 Hz had been tried. Typically, low-frequency rTMS reduces excitability while high-frequency rTMS exerts facilitatory effects.628The use of 1 Hz rTMS has been proven to be effective, although there is some discrepancy among measurement tools[7-8, 15-17]. Low-frequency rTMS on unaffected hemisphere produces better effects than high-frequency rTMS on affected hemisphere[15-16]. Khedr et al [16] reported that 1 Hz stimulation on unaffected hemisphere exhibited greater motor function improvement than 3 Hz stimulation. This occurs because 3 Hz stimulation over the affected hemisphere only increased the cortical excitability of affected hemisphere without changes of unaffected hemisphere. Evidence exists that low-frequency rTMS changed cortical excitability in bilateral hemispheres at the same time, whereas high-frequency rTMS is successful only on the affected hemisphere[7]. Application ofhigh-frequency rTMS alone on the affected hemisphere would not produce consistent results[19-20]. Recently, high-frequency combined with low-frequency rTMS is better than low-frequency rTMS alone in recovery of motor function[19]. Theta burst stimulation (TBS) is a pattern of rTMS that can facilitate M1 excitability when delivered intermittently or suppress M1 excitability when delivered continuously. Although interhemispheric inhibition is considered as one of the mechanisms of rTMS, continuous TBS (cTBS) shows no relationship between motor function improvement and interhemispheric inhibition[2], and even causes deteriorated motor activity[1, 21]. Therefore, TBS is considered against the simple application of the concept of interhemispheric inhibition.Nonetheless, TBS has an advantage in safety, because it employs lower intensity compared to the usual rTMS, allowing it to be safer and more effective after securing the underlying mechanism and the precise usage[22]. Therefore, further research is needed to find out the optimal TBS protocols to induce better motor recovery. The intensity of the stimulation might play a highly critical role. Subthreshold stimulation may act by local effect of the stimulation area, but a suprathreshold stimulation may change not only the stimulation area but also the opposite homogenous motor cortex[5-8]. Pomeroy et al[18] found that motor function did not change after suprathreshold (120%) stimulation. Effects of rTMS using different measurement tools were various, as shown in one study where outcomes of dexterity and grip strength were different[17].Choice reaction time, grip strength and cognitive performance[7, 23] are seldomly improved, which can be explained by activation of more distributed cortical areas for such parameters.rTMS has been shown to be effective for spasticity, hyperkinetic disorder and simple motor function[22, 24]. rTMS has proved its effectiveness while conventional rehabilitation results in unsatisfactory outcomes, so rTMS is speculated to be a superb[25]. T ask-specific rehabilitation combined with rTMS can improve motor function[23-24]. The capability of rTMS to facilitate motor learning through motor cortex excitability[26] is one of the important elements of rehabilitation, and therefore can be applied as an adjuvant therapy for the treatment of motor impairment.A limitation of the review is the relatively small sample size. The outcomes are collected and analyzed within a short period of time. In addition, the protocols in each study[5-8, 15-22] are not standardized. For this reason, the rTMS effects would not be better demonstrated. Further studies involving larger number of patients and using standard assessment of functional outcomes are needed.EFFECTS OF RTMS ON DYSPHAGIA(Table 2)Dysphagia can be managed by modified diet, compensatory swallowing technique and training[9]. rTMS has been tried to treat dysphagia, since it can stimulate the cortical input to the swallowing center[9]. Khedr et al[9] reported that post-stoke dysphagia improved after daily treatment sessions using rTMS, with an excitatory frequency of 3 Hz on the esophageal motor area of affected hemisphere.629Based on this research, Khedr et al[27] tested the effectsof 3 Hz rTMS on the esophageal motor cortex of bilateral hemispheres in patients with vertebrobasilar stroke, which induces severe dysphagia symptoms. All patients recovered swallowing function immediately after five sessions of rTMS applied on bilateral hemispheres with the same frequency. Although swallowing is controlled by bilateral hemispheres, interhemispheric asymmetry exists[29-30], allowing swallowing function to be controlled by either direct inhibition of unaffected hemisphere or facilitation of affected hemisphere. Based on the interhemipheric rivalry concept, the unaffected hemisphere was stimulated with a frequency of 1 Hz[28], whereas the esophageal motor cortex of affected hemisphere was stimulated with a frequency of 3 Hz[9]. According to the studies, various recovery mechanisms have been suggested, including increased excitability of the corticobulbar projections from bilateral hemispheres[9]or activation of remaining unaffected premotor cortex and contralateral medulla[27]. While motor area of cerebral cortex controls swallowing initiation, brainstem has a role in the swallowing reflex. Since rTMS exerts corticobulbar tract through the cerebral cortex, it activates both oral and pharyngeal stages of the coordinated swallowing process at the same time[28]. Thus, rTMS might be a better adjuvant therapy, compared to the swallowing functional electrical stimulation. EFFECTS OF RTMS ON VISUOSPATIAL NEGLECT(Table 3)Visuospatial neglect is a common, yet frequently overlooked, neurological disorder following stroke characterized by a deficit in attention and appreciation of stimuli on the contralesional side of the body[31]. It is common, with an incidence of 24.7% in acute stroke patients[32]. In addition to a number of treatments attempted over the last few years, including scanning, limb activation, eye patching, neck vibration and prism[33], rTMS also has been used as an adjuvant therapy for neglect.Initial studies demonstrated that rTMS of the unaffected hemisphere during the execution of a line bisection task transiently decreased the magnitude of neglect, followed by sustained effects after stimulation[34-40]. 25 Hz rTMS on unaffected parietal cortex was performed by means of an online approach by Oliveri et al [34]. Low-frequency rTMS on the unaffected hemisphere was used in five[35-39] out of seven[36-41] studies, and the effect was explained by the control of interhemispheric rivalry. Koch et al[35] applied 1 Hz rTMS (600 pulses, 90% resting motor threshold) over the unaffected posterior parietal cortex, to evaluate the sustained effect after the stimulation period, and showed reduction of the pathological hyperactivity of the intact hemisphere and improved performance immediately after rTMS.630Song et al [36] applied low-frequency rTMS on unaffected posterior parietal cortex twice a day for 2 weeks, (0.5 Hz, 90% motor threshold) and reported significant improvement for 2 weeks. In contrast, Oliveri et al [34] revealed the beneficial effects of high-frequency rTMS on unaffected hemisphere, contradicting the findings from other studies. The same parameters should be applied with caution, since it was the only study to use high-frequency rTMS for neglect. Nyffeler et al [40] applied cTBS over unaffected hemisphere with different numbers of trains and reported that repeated applications of TBS over the contralesional posterior parietal cortex on the same day specifically and significantly improved the perception of visual targets presented on the left side up to 32 hours. Most of the studies demonstrated positive results for visuospatial neglect[33-36, 38-40]. Song et al[36] demonstrated that 20 sessions of low-frequency rTMS over the unaffected hemisphere improved line cancellation and bisection. However, dissociations were found among different types of measurement tools, because of varying sensitivities for the diagnosis of neglect[41]. It was well known that there were dissociations between two cardinal diagnostic tests, i.e. cancellation and line bisection[42]. Furthermore, the heterogeneous mechanisms of visuospatial neglect are thought to be another cause for such differences in results. Attention was one of the mechanisms that build up neglect, and rTMS improved attention to greater extent than visuospatial function[37-38]. Long-term effect after rTMS stimulation wasinvestigated[36-37, 39]. Peak behavioral inattention test score of the patients at 6 weeks after rTMS stimulation remained better than that of pre-rTMS stimulation[36]. rTMS exhibits longer after-effect on visuospatial neglect than other treatment modalities. A direct comparison would be necessary, since no such comparison has been attempted. Koch et al[35] found that 1 Hz rTMS over left primary parietal cortex inhibited the over-excitability of left posterior parietal cortex-primary motor cortex circuits and also impacted visual neglect. However, the improvement did not correlate with the size of the normalization of the over-excitability. Further studies are necessary to elucidate the effects and mechanisms, and to establish the optimal protocols of rTMS for visuospatial neglect improvement. The effects of affected hemisphere stimulation should be identified, and it is preferable to compare the effects of rTBS with other types of TMS. EFFECTS OF RTMS ON APHASIA(Table 4)631The effectiveness of widely used speech-language therapy is generally known to diminish, as gradually moving on from acute to chronic stage in stroke patients[50]. Studies showed that recovery could take place for extended period of time after stroke in patients who received conventional aphasia rehabilitation[51-53]. rTMS can be considered a novel therapy for aphasia because it can promote recovery of chronic aphasia. rTMS used for up to 11 years showed effects in chronic aphasic patients[43-45], even in those who showed stable deficits of elicited propositional speech[46]. rTMS has effects on a variety of language problems, ranging from naming difficulty to speech arrest, depending on the stimulation parameter and area of rTMS.rTMS applied to an anterior portion of right Broca's homologue has shown to affect language behaviors, including naming, in stroke patients with chronic, nonfluent aphasia[43-45], with a frequency of 1 Hz. The mechanism of this protocol is to reduce interhemispheric inhibition towards the left hemisphere, which contains the main language area. On the contrary, Kakuda et al [47] applied low-frequency rTMS at Wernicke’s area for sensory aphasia patients. Winhuisen et al[48] applied4 Hz rTMS over activated region on positron emission tomography during semantic matching task and showed improvement of verb generation. Bilateral hemispheres were thought to have roles in supporting language recovery as proved by functional magnetic resonance imaging (fMRI) study[49]. Therefore, rTMS using the simple concept of interhemispheric inhibition might deteriorate recovery of aphasia. Kakuda et al [47] revealed that 1 Hz rTMS applied to the area homologous to the most activated site on fMRI seemed to be a feasible approach for post-stroke aphasic patients.The frameless stereotaxic system was used to guide the specific area on the scalp during rTMS application for aphasia. Bashir et al [54] proved the superiority of navigated rTMS in terms of both physiologic and behavioral effects[54] by maximizing accurate and consistent targeting. Therapeutic applications of rTMS are expected to benefit greatly with navigating electric field. As the recovery of language function was mediated by different parts of brain at different stages in terms of time[55], new therapeutic strategies, combining with fMRI or neuronavigation system, should be established for enhanced aphasia treatment in the future. CONCLUSIONReviewing the studies on effects of rTMS in post-stroke patients, the role of rTMS as an adjuvant therapy can be reaffirmed despite some conflicting outcomes. Nonetheless, it is imperative to further establish rTMS protocols including frequency, intensity and location to maximize the benefits of rTMS.All the studies with the use of 1 Hz rTMS were proven to be effective and low-frequency rTMS on unaffected hemisphere was better than high-frequency rTMS on affected hemisphere[15-16]. In addition, high-frequency combined with low-frequency rTMS was better thanlow-frequency rTMS alone, in terms of motor training[19]. Suprathreshold stimulation may change not only the stimulation site but also the opposite homogenous motor cortex[5-8, 18] and showed less effectiveness compared with the subthreshold stimulation.Swallowing function can be controlled by either direct inhibition of unaffected hemisphere or facilitation of affected hemisphere[28-29]. A previous study using TMS demonstrated that post-stroke dysphagia recovery was asymmetric between two hemispheres and was accompanied with activation of the unaffected hemisphere[56]. Application of 5 Hz rTMS to the unaffected pharyngeal motor cortex increased pharyngeal cortical excitability and improved swallowing behavior[57]. Similar findings have been identified by other studies using brain imaging techniques[58-59]. Such asymmetries have been explained by a lack of transcallosal inhibition between hemispheres in swallowing function[60-61]. Based on the interhemipheric rivalry concept, the unaffected hemisphere was stimulated with low-frequency rTMS[30], whereas the affected hemisphere was stimulated with high-frequency rTMS[9]. Both hemispheres have roles and recently rTMS is applied over the most activated sites on functional image during task[52]. In the future, optimal stimulation of rTMS using fMRI or neuronavigation system should be established for clinical application for the stroke patients. Funding: This study was supported by grant of the Korea Healthcare technology R&D Project, Ministry of Health & Welfare, Republic of Korea, No. A101901.Author contributions: Joonho Shin and KyeHee Cho were responsible for data acquisition. Joonho Shin, EunJoo Yang and Nam-Jong Paik were in charge of study concept and design. All authors participated in manuscript development, oversight and instruction.Conflicts of interest: None declared.REFERENCES[1] Johansson BB. Brain plasticity and stroke rehabilitation. The willislecture. Stroke. 2000;31(1):223-230.[2] Ward NS, Cohen LG. Mechanisms underlying recovery of motorfunction after stroke. Arch Neurol. 2004;61(12):1844-1848.[3] Williams JA, Imamura M, Fregni F. Updates on the use ofnon-invasive brain stimulation in physical and rehabilitationmedicine. J Rehabil Med. 2009;41(5):305-311.[4] Khedr EM, Rothwell JC, Ahmed MA, et al. Modulation of motorcortical excitability following rapid-rate transcranial magneticstimulation. Clin Neurophysiol. 2007;118(1):140-145.[5] Khedr EM, Ahmed MA, Fathy N, et al. Therapeutic trial ofrepetitive transcranial magnetic stimulation after acute ischemicstroke. Neurology. 2005;65(3):466-468.[6] Khedr EM, Etraby AE, Hemeda M, et al. Long-term effect ofrepetitive transcranial magnetic stimulation on motor functionrecovery after acute ischemic stroke. Acta Neurol Scand.2010;121(1):30-37.[7] Fregni F, Boggio PS, Valle AC, et al. A sham-controlled trial of a5-day course of repetitive transcranial magnetic stimulation of theunaffected hemisphere in stroke patients. Stroke. 2006;37(8):2115-2122.632[8] Takeuchi N, Chuma T, Matsuo Y, et al. Repetitive transcranialmagnetic stimulation of contralesional primary motor corteximproves hand function after stroke. Stroke. 2005;36(12):2681-2686.[9] Khedr EM, Abo-Elfetoh N, Rothwell JC. Treatment of post-strokedysphagia with repetitive transcranial magnetic stimulation. ActaNeurol Scand. 2009;119(3):155-161.[10] Cazzoli D, Muri RM, Hess CW, et al. Treatment of hemispatialneglect by means of rTMS--a review. Restor Neurol Neurosci.2010;28(4):499-510.[11] Johansson BB. Current trends in stroke rehabilitation. A reviewwith focus on brain plasticity. Acta Neurol Scand. 2011;123(3):147-159.[12] Hoogendam JM, Ramakers GM, Di Lazzaro V. Physiology ofrepetitive transcranial magnetic stimulation of the human brain.Brain Stimul. 2010;3(2):95-118.[13] Pape TL, Rosenow J, Lewis G. Transcranial magnetic stimulation:A possible treatment for TBI. Head Trauma Rehabil. 2006;21(5):437-451.[14] Hiscock A, Miller S, Rothwell J, et al. Informing dose-findingstudies of repetitive transcranial magnetic stimulation to enhance motor function: A qualitative systematic review. NeurorehabilNeural Repair. 2008;22(3):228-249.[15] Emara TH, Moustafa RR, Elnahas NM, et al. Repetitivetranscranial magnetic stimulation at 1Hz and 5Hz producessustained improvement in motor function and disability afterischaemic stroke. Eur J Neurol. 2010;17(9):1203-1209.[16] Khedr EM, Abdel-Fadeil MR, Farghali A, et al. Role of 1 and 3 Hzrepetitive transcranial magnetic stimulation on motor functionrecovery after acute ischaemic stroke. Eur J Neurol. 2009;16(12): 1323-1330.[17] Liepert J, Zittel S, Weiller C. Improvement of dexterity by singlesession low-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex in acute stroke: Adouble-blind placebo-controlled crossover trial. Restor NeurolNeurosci. 2007;25(5-6):461-465.[18] Pomeroy VM, Cloud G, Tallis RC, et al. Transcranial magneticstimulation and muscle contraction to enhance stroke recovery: A randomized proof-of-principle and feasibility investigation.Neurorehabil Neural Repair. 2007;21(6):509-517.[19] Takeuchi N, Tada T, Toshima M, et al. Repetitive transcranialmagnetic stimulation over bilateral hemispheres enhances motorfunction and training effect of paretic hand in patients after stroke.J Rehabil Med. 2009;41(13):1049-1054.[20] Malcolm MP, Triggs WJ, Light KE, et al. Repetitive transcranialmagnetic stimulation as an adjunct to constraint-induced therapy: An exploratory randomized controlled trial. Am J Phys MedRehabil. 2007;86(9):707-715.[21] Ackerley SJ, Stinear CM, Barber PA, et al. Combining theta burststimulation with training after subcortical stroke. Stroke. 2010;41(7):1568-1572.[22] Di Lazzaro V, Dileone M, Pilato F, et al. Repetitive transcranialmagnetic stimulation of the motor cortex for hemichorea. J Neurol Neurosurg Psychiatry. 2006;77(9):1095-1097.[23] Talelli P, Greenwood RJ, Rothwell JC. Exploring theta burststimulation as an intervention to improve motor recovery inchronic stroke. Clin Neurophysiol. 2007;118(2):333-342.[24] Izumi S, Kondo T, Shindo K. Transcranial magnetic stimulationsynchronized with maximal movement effort of the hemiplegichand after stroke: A double-blinded controlled pilot study. JRehabil Med. 2008;40(1):49-54.[25] Mally J, Dinya E. Recovery of motor disability and spasticity inpost-stroke after repetitive transcranial magnetic stimulation(rTMS). Brain Res Bull. 2008;76(4):388-395.[26] Pascual-Leone A, Tarazona F, Keenan J, et al. Transcranialmagnetic stimulation and neuroplasticity. Neuropsychologia.1999;37(2):207-217.[27] Khedr EM, Abo-Elfetoh N. Therapeutic role of rtms on recovery ofdysphagia in patients with lateral medullary syndrome andbrainstem infarction. J Neurol Neurosurg Psychiatry. 2010;81(5):495-499. [28] Verin E, Leroi AM. Poststroke dysphagia rehabilitation byrepetitive transcranial magnetic stimulation: A noncontrolled pilotstudy. Dysphagia. 2009;24(2):204-210.[29] Khedr EM, Abo-Elfetoh N, Ahmed MA, et al. Dysphagia andhemispheric stroke: A transcranial magnetic study. NeurophysiolClin. 2008;38(4):235-242.[30] Hamdy S, Aziz Q, Thompson DG, et al. Physiology andpathophysiology of the swallowing area of human motor cortex.Neural Plast. 2001;8(1-2):91-97.[31] Heilman KM, Valenstein E. Mechanisms underlying hemispatialneglect. Ann Neurol. 1979;5(2):166-170.[32] Ringman JM, Saver JL, Woolson RF, et al. Frequency, risk factors,anatomy, and course of unilateral neglect in an acute strokecohort. Neurology. 2004;63(3):468-474.[33] Pierce SR, Buxbaum LJ. Treatments of unilateral neglect: Areview. Arch Phys Med Rehabil. 2002;83(2):256-268.[34] Oliveri M, Bisiach E, Brighina F, et al. Rtms of the unaffectedhemisphere transiently reduces contralesional visuospatialhemineglect. Neurology. 2001;57(7):1338-1340.[35] Koch G, Oliveri M, Cheeran B, et al. Hyperexcitability ofparietal-motor functional connections in the intact left-hemisphere of patients with neglect. Brain. 2008;131(Pt 12):3147-3155. [36] Song W, Du B, Xu Q, et al. Low-frequency transcranial magneticstimulation for visual spatial neglect: A pilot study. J Rehabil Med.2009;41(3):162-165.[37] Lim JY, Kang EK, Paik NJ. Repetitive transcranial magneticstimulation to hemispatial neglect in patients after stroke: Anopen-label pilot study. J Rehabil Med. 2010;42(5):447-452. [38] Shindo K, Sugiyama K, Huabao L, et al. Long-term effect oflow-frequency repetitive transcranial magnetic stimulation overthe unaffected posterior parietal cortex in patients with unilateralspatial neglect. J Rehabil Med. 2006;38(1):65-67.[39] Brighina F, Bisiach E, Oliveri M, et al. 1 Hz repetitive transcranialmagnetic stimulation of the unaffected hemisphere amelioratescontralesional visuospatial neglect in humans. Neurosci Lett.2003;336(2):131-133.[40] Nyffeler T, Cazzoli D, Hess CW, et al. One session of repeatedparietal theta burst stimulation trains induces long-lastingimprovement of visual neglect. Stroke. 2009;40(8):2791-2796. [41] Milner AD, McIntosh RD. The neurological basis of visual neglect.Curr Opin Neurol. 2005;18(6):748-753.[42] Adair JC, Barrett AM. Spatial neglect: Clinical and neurosciencereview: A wealth of information on the poverty of spatial attention.Ann N Y Acad Sci. 2008;1142:21-43.[43] Naeser MA, Martin PI, Nicholas M, et al. Improved picture namingin chronic aphasia after tms to part of right broca's area: Anopen-protocol study. Brain Lang. 2005;93(1):95-105.[44] Martin PI, Naeser MA, Ho M, et al. Research with transcranialmagnetic stimulation in the treatment of aphasia. Curr NeurolNeurosci Rep. 2009;9(6):451-458.[45] Martin PI, Naeser MA, Theoret H, et al. Transcranial magneticstimulation as a complementary treatment for aphasia. SeminSpeech Lang. 2004;25(2):181-191.[46] Hamilton RH, Sanders L, Benson J, et al. Stimulatingconversation: Enhancement of elicited propositional speech in apatient with chronic non-fluent aphasia following transcranialmagnetic stimulation. Brain Lang. 2010;113(1):45-50.[47] Kakuda W, Abo M, Uruma G, et al. Low-frequency rtms withlanguage therapy over a 3-month period for sensory-dominantaphasia: case series of two post-stroke Japanese patients. BrainInj. 2010;24(9):1113-1117.[48] Winhuisen L, Thiel A, Schumacher B, et al. Role of thecontralateral inferior frontal gyrus in recovery of language function in poststroke aphasia: A combined repetitive transcranialmagnetic stimulation and positron emission tomography study.Stroke. 2005;36(8):1759-1763.[49] Kakuda W, Abo M, Kaito N, et al. Functional mri-basedtherapeutic rtms strategy for aphasic stroke patients: A caseseries pilot study. Int J Neurosci. 2010;120(1):60-66.633。
neural regeneration research, -回复

neural regeneration research, -回复什么是神经再生研究?为什么这个领域的研究如此重要?我们目前对神经再生的了解如何?仍然存在的挑战是什么?未来如何推动神经再生研究的发展?本文将逐步回答这些问题。
神经再生研究旨在研究和探索激活和促进受损神经系统恢复功能的机制和方法。
神经再生是指受损的神经细胞重新生长、恢复其结构和功能的过程。
这个领域的研究对于治疗神经系统疾病和创伤具有巨大的潜力,比如中风、脊髓损伤和神经退行性疾病。
神经系统是人体最复杂的系统之一,包括大脑、脊髓和周围神经。
与其他器官和组织不同的是,神经系统的细胞有非常有限的再生能力。
因此,一旦神经细胞受到损伤或死亡,其功能可能无法恢复。
这是为什么神经再生研究如此重要的原因。
目前,我们对于神经再生的了解仍然有限。
然而,科学家们已经取得了一些重要的进展。
研究发现,神经干细胞在一定程度上具有再生神经细胞和修复神经连接的能力。
这些神经干细胞存在于不同的部位,包括大脑、脊髓和周围神经。
此外,研究还发现,神经细胞的环境和周围组织对于其再生的影响非常重要。
神经损伤后,炎症反应会发生,这可能对神经细胞的再生产生负面影响。
因此,研究人员致力于寻找方法来抑制这种炎症反应,并提供有利于神经细胞再生的环境。
然而,神经再生研究仍然面临一些挑战。
一方面,神经系统的复杂性使得研究变得困难。
另一方面,神经细胞的再生受到内外环境的复杂调控。
因此,我们需要深入研究神经细胞再生的分子机制和信号通路,以便更好地促进神经再生。
未来,推动神经再生研究的发展需要综合多种方法和技术。
一方面,基础研究将为我们提供有关神经再生机制的更多了解。
这包括揭示神经干细胞的分化和再生能力的机制,以及环境和其他因素对神经细胞再生的影响。
另一方面,临床研究将测试和开发新的治疗方法和技术。
干细胞治疗被认为是一种很有前景的策略,可以通过植入干细胞来促进神经细胞的再生和恢复功能。
此外,基因编辑和基因治疗技术也可能为神经再生研究带来新的突破。
Neural Regeneration Research (NRR)

s b s in p e e iwe sa e r n o y s lc e o rv e o r a il .I o ra il s a c p e ,i wi e p b ih d wi i 2 — u miso . e rr ve r r a d ml e e t d t e i w y u r c e fy u r c e i c e td t l b u l e t n 1 0 t t l s h
维普资讯
Ne r l g n r t nRee rh( R) u a e e ai sa c NR Re o
N R是一本在神经再生研究 领域具有 国际水平 的以国际通用语 言英语 为沟通平 台的专业杂志 。 R N R由卫生部 主管 、 R 中国康复 医学会主办 , 中国神经再生研究 ( 《 英文 版 )杂志社编辑 出版 , 》 电子版由 Esv rSnaoe l i (igpr) ee
时效 0 10天 。 2—5
N R具有 良好的 国际影响力及学科专业影响力 , R 已被下列 国际及 国内的著数据库收录 : ● Esve 电子期刊全文数据库 Sine i cO S eS O ) l i e r cecDr t n i ( D S ( e t 文章出版后 1 周内可在线 阅读)
Pe t. 。月 刊, t Ld出版 全球 范围内公开发行。C 1 4 2 IS 6 3 3 4 N 1 口5 2 / S N17 口5 7 。 R,
neural regeneration research分区 -回复

neural regeneration research分区-回复中括号内的主题:神经再生研究(Neural Regeneration Research)。
引言:神经再生研究是生物学和医学领域的重要研究方向之一。
随着人们对神经系统和神经退行性疾病的深入了解,探索神经再生的方法和机制变得愈发重要。
本文将逐步讨论神经再生研究的最新进展,包括神经干细胞疗法、生物材料的应用和电生物学技术的发展。
一、神经干细胞疗法神经干细胞是一类具有自我更新和多向分化潜能的细胞,可在受损的神经系统中改善修复过程。
近年来,神经干细胞疗法在神经再生研究中成为热点。
研究人员发现,将神经干细胞移植到受损的区域,可促进神经元再生和功能恢复。
通过体外培养和脱分化,可以从多种来源获得神经干细胞,如胎儿神经组织、成年脑组织和诱导多能干细胞。
在实际应用中,神经干细胞疗法面临许多挑战。
首先,植入的神经干细胞在宿主组织中生存和存活率较低。
其次,植入后的细胞可能会引起免疫系统的反应。
此外,研究人员还需要解决神经干细胞的定向分化和迁移问题。
二、生物材料在神经再生中的应用生物材料的应用是神经再生研究中的另一个重要方向。
生物材料通过提供支架和促进细胞生长的微环境,可以帮助神经组织的再生和修复。
已经使用的生物材料包括天然材料(如胶原蛋白和凝胶材料)和人工合成材料(如聚合物和纳米材料)。
研究表明,生物材料的物理和化学特性可以影响神经细胞的黏附、扩散和分化。
合理选择和组合生物材料,可以提高神经组织的再生效果。
此外,生物材料也可以用于释放生长因子和药物,以促进神经细胞的生长和分化。
三、电生物学技术在神经再生中的发展电生物学技术是近年来在神经再生领域取得进展的一项技术。
这种技术通过电刺激神经细胞,促进其生长和再生。
电生物学技术可以分为两大类:外部电刺激和内部电极植入。
外部电刺激主要通过低频、中频或高频电流刺激神经组织,以改善其功能和再生。
内部电极植入则是将微小电极植入到受损的神经组织中,直接刺激神经细胞。
麻醉药物在甲状腺术中对喉返神经监测影响的研究进展

麻醉药物在甲状腺术中对喉返神经监测影响的研究进展依据最近的流行病学调查研究,发现甲状腺疾病的患病率高达19%-67%,而手术治疗仍为甲状腺疾病治疗的首选方法[1-2]。
外科医生在进行甲状腺手术时最重要并发症之一是损伤喉返神经,而喉返神经的损伤率可高达为1.0%-9.5%[3],而随着近年来电生理监测技术和监控设备的进步和快速发展,术中采用神经监测也越来越成熟并得到了进一步推广[4-6]。
目前,术中神经监测(intraoperative neuromonitoring,IONM)主要通过间断刺激神经的方式,以此来监测神经是否完整性和功能是否存在。
在已经存在声带麻痹、甲状腺癌或复杂的二次甲状腺术中,IONM为外科医生保驾护航,已成为甲状腺手术的导航仪[7-9]。
一、喉返神经监测技术在甲状腺术中的影响因素甲状腺手术中影响喉返神经监测的因素:①患者自身的因素:包括血浆PH、血糖、体温、血压异常以及术前已存在的喉返神经受损。
②手术操作因素:术中过度牵拉、钳夹、吸引、电灼、压迫和切割等均可以引起喉返神经损伤,继而检测到的肌电信号强度会减弱甚至消失。
③气管插管技巧及定位:根据我们的经验,气管导管的错位是导致监测失败的主要原因,因此准确的气管插管是神经监测的关键。
只有最恰当的深度和角度才能让肌电信号传导。
另外插管时逆时针旋转导管30º,以减少插管时可能发生的旋转,插管完成后将导管固定于右嘴角。
插管深度:据Lu[10]等研究女性适宜的插管深度为(19.6±1.0)cm,男性的适宜的插管深度为(20.6±0.97)cm,且身高越高,插入深度越深。
④麻醉药物的因素:术中使用的肌松药、吸入麻醉药等均会影响到喉返神经的检测。
二、吸入麻醉和静脉麻醉对神经监测的影响的对比夏莉[11]等研究对比了静-吸复合麻醉和全凭静脉麻醉对脑干听觉诱发电位、躯体感觉诱发电位及肌电图的影响,该项研究中未使用肌松药物,得出比较适用于需要行神经电生理监测的脑干肿瘤切除手术。
中国计量大学学位与研究生教育期刊目录(2014、2015版)

中国计量学院学位与研究生教育期刊目录(2014)一、国内一级学术期刊目录(339种)1 半导体学报2 北京体育大学学报3 比较教育研究4 兵工学报5 病毒学报6 材料研究学报(材料科学进展)7 财贸经济8 蚕业科学9 测绘学报10 茶叶科学11 城市规划12 传感技术学报13 催化学报14 大气科学15 大学国书馆学报16 当代电影17 当代语言学(原为:国外语言学)18 档案学通讯19 低温工程20 地理科学21 地理学报22 地理研究23 地球化学24 地球物理学报25 地震学报26 地质科学27 地质学报28 电工技术学报29 电力系统自动化30 电路与系统学报31 电信科学32 电子学报33 电子与信息学报(原名电子科学学刊)34 动力工程35 动物学报36 动物学研究37 动物营养学报38 敦煌研究39 法学研究40 纺织学报41 分析化学42 复合材料学报43 钢铁44 高等工程教育研究(武汉)45 高等教育研究(武汉)46 高等学校化学学报47 高分子学报48 高能物理与核物理49 高校化学工程学报50 高校应用数学学报51 工程热物理学报52 古汉语研究53 古生物学报54 固体力学学报55 管理科学学报56 管理世界57 光电工程58 光电子·激光59 光学学报60 光子学报61 硅酸盐学报62 国际贸易问题63 国际问题研究64 果树学报(原名:果树科学)65 海洋工程66 海洋学报67 海洋与湖沼68 航空学报69 航天医学与医学工程70 核农学报71 红外与毫米波学报72 化工学报73 化学物理学报74 化学学报75 环境科学76 环境科学学报77 会计研究78 机械工程学报79 计量学报80 计算机辅助设计与图形学学报81 计算机集成制造系统82 计算机科学技术学报(英文版)83 计算机学报84 计算机研究与发展85 计算数学86 建筑结构学报87 建筑学报88 教育发展研究89 教育研究90 解剖学报91 金融研究92 金属学报93 近代史研究94 经济地理95 经济理论与经济管理96 经济社会体制比较97 经济学家98 经济研究99 菌物学报(原名:菌物系统)100 考古学报101 科学通报102 科学学研究103 科研管理104 空间科学学报105 空气动力学学报106 控制理论与应用107 控制与决策108 矿物学报109 昆虫分类学报110 昆虫学报111 力学学报112 历史研究113 林业科学114 马克思主义研究115 麦类作物学报116 煤炭学报117 美术研究118 棉花学报119 民族研究120 模式识别与人工智能121 摩擦学学报122 内燃机工程123 内燃机学报124 农药学报125 农业工程学报126 农业机械学报127 农业经济问题128 农业生物技术学报129 气象学报130 汽车工程131 强激光与粒子束132 情报学报133 燃料化学学报134 热力发电135 人口研究136 软件学报137 社会科学战线138 社会学研究139 生理学报140 生态学报141 生物多样性142 生物工程学报143 生物化学与生物物理学报144 生物物理学报145 声学学报146 石油学报147 实验生物学报148 史学理论研究149 世界经济150 世界经济与政治151 世界历史152 世界宗教研究153 兽类学报154 数量经济技术经济研究155 数学进展156 数学年刊(A、B辑)157 数学物理学报158 数学学报159 水产学报160 水动力学研究与进展(英文版)161 水科学进展162 水力发电学报163 水利学报164 水生生物学报165 水土保持学报166 台湾研究167 太阳能学报168 体育科学169 天文学报170 通信学报171 统计研究172 土木工程学报173 土壤学报174 外国文学175 外国文学评论176 外国文学研究177 外国语178 外语教学与研究179 微波学报180 微生物学报181 文史(中华书局)182 文献183 文学评论184 文学遗产185 文艺理论研究186 文艺研究187 无机材料学报188 无机化学学报189 物理化学学报190 物理学报191 系统工程理论与实践192 系统科学与数学193 细胞生物学杂志194 现代外语195 心理科学196 心理学报197 新华文摘198 新美术199 新闻与传播研究200 畜牧兽医学报201 学术月刊202 岩石力学与工程学报203 岩石学报204 岩土工程学报205 遥感学报206 药物分析杂志207 药学学报208 仪器仪表学报209 遗传210 遗传学报211 应用生态学报212 应用数学学报213 应用数学与力学(英文版)214 应用心理学215 营养学报216 有机化学217 宇航学报218 语言研究219 园艺学报220 哲学研究221 浙江大学学报(人文社会科学版)222 浙江大学学报(工学版)223 浙江大学学报(英文版)224 真空科学与技术学报225 振动工程学报226 政法论坛227 政治学研究228 植物保护学报229 植物病理学报230 植物分类学报231 植物生理与分子生物学学报(原名:植物生理学报)232 植物生态学报233 植物学报234 植物营养与肥料学报235 中草药236 中共党史研究237 中国病理生理杂志238 中国出版239 中国电机工程学报240 中国法学241 中国翻译242 中国腐蚀与防护学报243 中国高教研究244 中国工业经济245 中国公路学报246 中国光学快报(英文版)247 中国广播电视学刊248 中国化学快报(英文版)249 中国环境科学250 中国机械工程251 中国激光252 中国寄生虫学与寄生虫病杂志253 中国经济史研究254 中国科学(A-G)辑255 中国粮油学报256 中国农村经济257 中国农业科学258 中国人口科学259 中国人民大学报刊复印资料(全文复印)260 中国社会科学261 中国社会科学评论(香港)262 中国社会科学文摘263 中国生物防治264 中国生物化学与分子生物学报265 中国生物医学工程学报266 中国食品学报267 中国史研究268 中国兽医学报269 中国水稻科学270 中国体育科技271 中国图书馆学报272 中国图像图形学报273 中国土地科学274 中国物理快报(英文版)275 中国稀土学报276 中国现代文学研究丛刊277 中国畜牧杂志278 中国药理学报279 中国药理学与毒理学杂志280 中国药学杂志281 中国音乐学282 中国应用生理学杂志283 中国有色金属学报284 中国语文285 中国预防兽医学报286 中国运动医学杂志287 中国中西医结合杂志288 中国中药杂志289 中华病理学杂志290 中华超声影像学杂志291 中华传染病杂志292 中华创伤杂志293 中华儿科杂志294 中华耳鼻咽喉头颈外科杂志295 中华放射学杂志296 中华放射医学与防护杂志297 中华妇产科杂志298 中华骨科杂志299 中华护理杂志300 中华急诊医学杂志(原名: 急诊医学)301 中华检验医学杂志302 中华结核和呼吸杂志303 中华精神科杂志304 中华口腔医学杂志305 中华劳动卫生职业病杂志306 中华流行病学杂志307 中华麻醉学杂志308 中华泌尿外科杂志309 中华内分泌代谢杂志310 中华内科杂志311 中华皮肤科杂志312 中华普通外科杂志313 中华烧伤杂志314 中华神经科杂志315 中华神经外科杂志316 中华肾脏病杂志317 中华外科杂志318 中华微生物学和免疫学杂志319 中华物理医学与康复杂志320 中华消化杂志321 中华小儿外科杂志322 中华心血管病杂志323 中华胸心血管外科杂志324 中华血液学杂志325 中华眼科杂志326 中华医学遗传学杂志327 中华医学杂志328 中华医院管理杂志329 中华预防医学杂志330 中华整形外科杂志331 中华肿瘤杂志332 中外法学333 自动化学报334 自然辩证法通讯335 自然辩证法研究336 自然科学进展337 自然灾害学报338 自然资源学报339 作物学报注:1、被IM收录的论文视同国内一级期刊论文。
SCI 论文投稿如何挑选审稿人

SCI 论文投稿如何挑选审稿人发表SCI论文过程中,最痛苦不是收集数据或英文写作。
根据1000名意诺客户反馈的意见,最让他们痛苦的是所投的稿件被杂志社分配给一个态度恶劣的审稿人。
这些审稿人往往因为一些小小的问题就无情的把自己辛苦一两年做的研究就否定了。
大部分科研工作者在投稿时没有意识到,其实您是可以自己挑选对自己有利的审稿人的。
有些SCI杂志在您投稿的时候,直接让您在投稿信里推荐几名审稿人。
遗憾的是,很多人为省事顺便写下本领域内自己不认识的人,从而浪费了一个挑选对自己有利的审稿人的机会。
有些SCI 杂志,没有让您推荐审稿人。
也不要放过这个机会。
您最好在投稿信里,指明几个和自己领域相关的,并对自己友好的同行,推荐他们作为自己的审稿人。
如果您认识的人里没有您要投稿的杂志编辑和审稿人,您也不要担心,意诺可以免费帮您。
意诺的几十名编辑目前在为200多家SCI杂志审稿。
您可以挑选他们作为您的审稿人,他们将为您提供很友好的审稿意见。
部分意诺编辑审稿的SCI杂志列举如下,后面相应的是意诺编辑本人名字的英文简写和他们供职的单位。
如果这些杂志里有您要投稿的杂志,请和意诺的客服联系,获取相应编辑的详细信息。
杂志名;姓名的缩写;就职单位Acta Pharmacologica Sinica; SY; University of FloridaInorganic Chemistry; ZB; Massachusetts Institute of Technology (MIT) Academic Journal Review Panel Membership; YS; Duke UniversityActa Pharmacologica Sinica; NL; Yale UniversityAdvances in Psychological Science; NL; Yale UniversityAmerican Journal of Epidemiology; CZ; Harvard UniversityAnalyst; SY; University of MichiganAnalyst; YS; Duke UniversityAnalytical Methods; YS; Duke UniversityApplied Optics; SY; University of MichiganApplied Optics; CM; California Institute of TechnologyApplied Optics; JH; University of DelawareApplied Soil Ecology; ZC; Columbia UniversityArabian Journal of Chemistry; GZ; University of ChicagoBehavioural Pharmacology; NL; Yale UniversityBiochemistry; ST; New York UniversityBiomedical Optics Express; SY; University of MichiganBiomedical Optics Express; CM; California Institute of Technology Biometrics; CZ; Harvard UniversityBioorganic and Medicinal Chemistry; GZ; University of Chicago Biophysical Journal; JD; Stanford UniversityBlood; HL; Cleveland ClinicBMC Research Notes; CZ; Harvard UniversityBritish Journal of Urology International; TA; Brown Universitycancer prevention research ; XL; National Institutes of Health (NIH)cancer research; XL; National Institutes of Health (NIH)Central European Journal of Chemistry; GZ; University of ChicagoChem. Phys; BD; Cornell UniversityChemical Society Reviews; GZ; University of ChicagoChemistry of Heterocyclic Compounds; GZ; University of ChicagoChinese Optics Letters; SY; University of Michiganclinical cancer research; XL; National Institutes of Health (NIH) Combinatorial Chemistry & High Throughput Screening; YS; Duke UniversityCompost Science and Utilization; ZC; Columbia UniversityCurrent Bioactive Compounds; GZ; University of ChicagoCurrent Biology; JL; Harvard UniversityCurrent Drug Metabolism; YS; Duke UniversityDepression and Anxiety; CZ; Harvard UniversityDrug Metabolism Letters; YS; Duke UniversityEcological Engineering; ZC; Columbia UniversityEuropean Journal of Medicinal Chemistry; GZ; University of Chicago European Journal of Organic Chemistry; GZ; University of ChicagoEuropean Journal of Pharmacology; NL; Yale UniversityFEBS Letter; NW; University of PennsylvaniaFEBS letter; HL; Cleveland ClinicGenes & Dev; ST; New York UniversityGenome Biology; NW; University of PennsylvaniaIEEE Journal of Selected Topics in Quantum Electronics; SY; University of MichiganIEEE Photonics Journal; JH; University of DelawareIEEE Photonics Technology Letters; JH; University of DelawareIEEE Transactions on Biomedical Engineering; SY; University of Michigan Industrial & Engineering Chemistry; ZB; Massachusetts Institute of Technology (MIT)Infectious Disorders-Drug T argets; YS; Duke Universityinternational journal of cancer; YL; Vanderbilt UniversityInternational Journal of Computational Science; CZ; Harvard University International Journal of Neuropsychopharmacology; NL; Yale University International Journal of Radiation Biology; JD; Stanford University International Journal of Urology; TA; Brown UniversityJBC; ST; New York UniversityJournal of Applied Electrochemistry; BD; Cornell UniversityJournal of Applied Physics; CM; California Institute of TechnologyJournal of Bioterrorism & Biodefence (Environmental Sciences Group); ZC; Columbia UniversityJournal of Environmental Engineering; ZC; Columbia UniversityJournal of Forestry; ZC; Columbia UniversityJournal of Materials Chemistry; ZB; Massachusetts Institute of Technology (MIT) Journal of Medical Case Reports; TA; Brown UniversityJournal of Molecular Biology; NW; University of PennsylvaniaJournal of Nanomaterials; JD; Stanford UniversityJournal of Nanoscience and Nanotechnology; JD; Stanford UniversityJournal of Nanoscience and Nanotechnology; ZB; Massachusetts Institute of Technology (MIT)Journal of Optics A: Pure and Applied Optics; SY; University of Michigan Journal of Physical Chemistry; JD; Stanford UniversityJournal of Soils and Sediments; ZC; Columbia UniversityJournal of the Optical Society of America A; CM; California Institute of TechnologyJournal of the Optical Society of America B; JH; University of Delaware Journal of Thermdynamic & Catalysis; GZ; University of Chicago Journal of Urology; TA; Brown UniversityJournal of Chemical Biology; GZ; University of ChicagoJournal of Psychopharmacology; NL; Yale UniversityJournal ofNanophotonics; CM; California Institute of Technology Langmuir; ZZ; George Institute of TechnologyLasers in Surgery and Medicine; SY; University of Michigan Measurement Science and Technology; SY; University of Michigan Medicinal Chemistry; GZ; University of ChicagoModern Physics Letters B; JD; Stanford UniversityMol cell; ST; New York UniversityMolecular Biology of Cell; NW; University of PennsylvaniaMolecular Cell; NW; University of PennsylvaniaMolecular Cellular Biology; NW; University of PennsylvaniaMolecular Diversity; GZ; University of ChicagoNano Letters; ZB; Massachusetts Institute of Technology (MIT) Nanoscale; JD; Stanford UniversityNanotoxicology; ZB; Massachusetts Institute of Technology (MIT) Nature; ST; New York UniversityNature Cell biology; ST; New York UniversityNature chemical biology; ST; New York UniversityNature Communications; JD; Stanford UniversityNature Protocols; CZ; Harvard UniversityNature Structural & Molecular Biology; JD; Stanford UniversityNeural Regeneration Research; NL; Yale UniversityNeuropharmacology; NL; Yale UniversityNeuropharmacology; CZ; Harvard UniversityNeuroscienceLetters; NL; Yale UniversityNew Journal of Physics; SY; University of MichiganNorthern Journal of Applied Forestry; ZC; Columbia UniversityNucleic Acids Research; CZ; Harvard Universityoncogene; YL; Vanderbilt UniversityOpen Access Journal of Urology; TA; Brown UniversityOptical Materials; JH; University of DelawareOptical Materials Express; JH; University of DelawareOptics Communications; CM; California Institute of TechnologyOptics Communications; JH; University of DelawareOptics Express; CM; California Institute of TechnologyOptics Express; JH; University of DelawareOptics Express, Optics Letters; SY; University of MichiganOptics Letters; CM; California Institute of TechnologyOptics Letters; JH; University of DelawareOrganic & Biomolecular Chemistry; ZB; Massachusetts Institute of Technology (MIT)Pest Management Science; ZC; Columbia UniversityPhys. Chem; BD; Cornell UniversityPhysical Review Letters; SY; University of MichiganPhysics in Medicine and Biology; SY; University of MichiganPlant Cell; NW; University of PennsylvaniaPlant Journal; NW; University of PennsylvaniaPLoS Biology; JL; Harvard UniversityPLoS ONE; JL; Harvard UniversityPNAS; NW; University of PennsylvaniaProceedings of the National Academy of Sciences; JD; Stanford University Progress in Neuro-Psychopharmacology and Biological Psychiatry; NL; Yale UniversityProtein & Peptide Letters ; JD; Stanford UniversityPsychiatry and Clinical Neuroscience; NL; Yale UniversityScience; NW; University of PennsylvaniaScience; ST; New York UniversityStructure; NW; University of Pennsylvania。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
NEURAL REGENERATION RESEARCHV olume 5, Issue 1, January 2010Cite this article as: Neural Regen Res. 2010;5(1):58-63.58Li’an Huang☆, Doctor,Associate chief physician,Department of Neurology,First Affiliated Hospital ofJinan University, Guangzhou510632, GuangdongProvince, ChinaCorresponding author: Li’anHuang, Doctor, Associatechief physician, Departmentof Neurology, First AffiliatedHospital of Jinan University,Guangzhou 510632,Guangdong Province, Chinahuanglianfujian@hotmail.comSupported by: MedicalScientific and TechnologicalResearch Foundation ofGuangdong Province, No.2007332*; 2009360*; theNatural Science Foundationof Guangdong Province, No.9451063201002951*Received: 2009-07-04Accepted: 2009-10-24(N20090508001/WLM)Huang LA, Song XW, Xu AD,Ling XY, Lin ZC. Cerebralperfusion in correspondingblood supply areas oftransient ischemic attackpatients with intracranialstenosis: seven cases ofdiamox-perfusion verified bymagnetic resonance-perfusion- weighted imaging.Neural Regen Res.2010;5(1):58-63.doi:10.3969/j.issn.1673-5374.2010.01.010Cerebral perfusion in corresponding blood supplyareas of transient ischemic attack patients withintracranial stenosisSeven cases of diamox-perfusion verified by magneticresonance-perfusion-weighted imaging***☆Li’an Huang1, Xuewen Song1, Anding Xu1, Xueying Ling2, Zhichao Lin21Department of Neurology, First Affiliated Hospital of Jinan University, Guangzhou 510632, Guangdong Province, China2Department of Radiology, First Affiliated Hospital of Jinan University, Guangzhou 510632, Guangdong Province, ChinaAbstractBACKGROUND: Due to collateral circulation and cerebrovascular reserve, arterial stenosis and reduced cerebral blood flow may not necessarily indicate impaired cerebral perfusion. Therefore, according to degree of stenosis and clinical symptoms, interventional surgery to relieve arterial stenosis in transient ischemic attack (TIA) patients with major intracranial stenosis is imprudent. Rather, cerebral perfusion and reserve capacity are direct indicators for the assessment of degree and presence of cerebral ischemia.OBJECTIVE: To evaluate cerebral perfusion and reserve in TIA patients with major intracranial stenosis or occlusion using magnetic resonance-perfusion-weighted imaging (MR-PWI) data prior toand following diamox administration.DESIGN, TIME AND SETTING: A self-comparative, neuroimaging observation was performed atthe Neurological Department and Radiological Center of the First Affiliated Hospital of Jinan Uni- versity between December 2007 and April 2009.PARTICIPANTS: Seven acute TIA patients, who were admitted to the Neurological Department of the First Affiliated Hospital of Jinan University between December 2007 and April 2009, were en- rolled in the present study. Magnetic resonance imaging confirmed that no acute cerebral infarctionhappened, nor did bleeding exist. Magnetic resonance angiography, transcranial Dopplerultrasound,and/or digital subtraction angiography confirmed the presence of major intracranial arterial stenosis.Clinical symptoms corresponded to blood supplying regions of the arterial stenosis. METHODS: Baseline MR-PWI was performed on seven patients with intracranial stenosis or occlu-sion. Two grams of acetazolamide (diamox) were orally administered after 2 days. A second PWI was performed after 2 hours to compare cerebral perfusion parameters prior to and following diamoxadministration.MAIN OUTCOME MEASURES: PWI results of cerebral perfusion prior to and following diamox administration.RESULTS: The baseline PWI from five patients indicated decreased cerebral perfusion areas. Fol- lowing oral administration of diamox, cerebral perfusion significantly decreased in those areas. Moreover, new areas of decreased cerebral perfusion were observed in two out of the five patients. In one patient, no significant decrease in cerebral perfusion was found. In another patient, baseline PWI indicated decreased cerebral perfusion in the left hemisphere. However, normal perfusion wasobserved in both cerebral lobes following diamox administration.CONCLUSION: TIA patients with intracranial stenosis, who are diagnosed by PWI and exhibited decreased cerebral perfusion and reserve, might require further treatment such as intervention by angioplasty.Key Words: transient ischemic attack; stenosis; magnetic resonance-perfusion-weighted imaging; diamox; cerebral perfusion; cerebral reserve capacity。