中英文对照医院体检表(出国办签证所用)
英国签证申请人结核筛查体检登记表
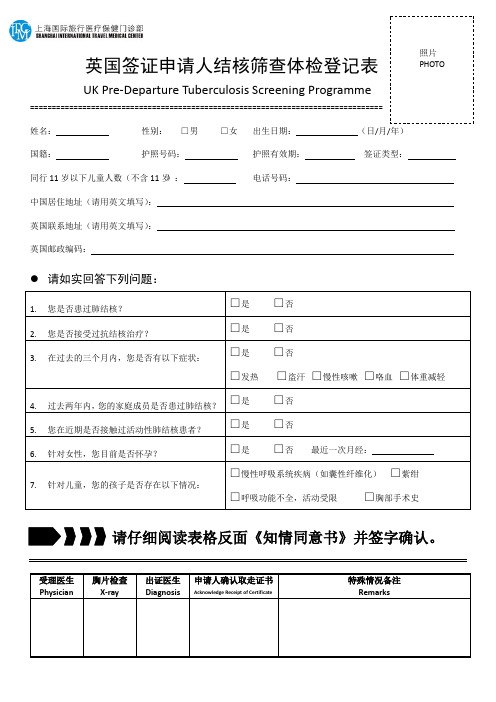
英国签证申请人结核筛查体检登记表UK Pre-Departure Tuberculosis Screening Programme=================================================================================姓名:性别: □男 □女 出生日期: (日/月/年) 国籍: 护照号码: 护照有效期: 签证类型: 同行11岁以下儿童人数(不含11岁): 电话号码:中国居住地址(请用英文填写):英国联系地址(请用英文填写): 英国邮政编码:请如实回答下列问题:请仔细阅读表格反面《知情同意书》并签字确认。
申请人申明:本人已了解下述情况:•在申请入境英国前,我必须接受肺结核筛查(X光检查),并可能进一步接受痰液检查;•如果胸部X光检查发现异常,医师将对我进行单独询问并告知我进一步检查的步骤;•如果我的胸部X光检查结果为异常,无论是新发病灶或陈旧病灶,只要该病变提示结核可能,或者存在其他临床表现提示结核可疑,我都必须提供三次痰液标本供结核菌涂片和培养检测。
痰培养检查结果需10周时间,我对此表示接受。
•如果需要进行痰液检查,我应在胸部X光检查后7天内返回进行留痰,采痰需在连续3天早晨进行。
如果不能在7天内返回留痰,我将无法获得签证用“医学证明”。
•如果痰涂片或培养显示有结核杆菌存在,我须接受抗结核治疗,治疗费用将由我自行承担。
我还应告知承担抗结核治疗的医疗机构,与我密切接触的家庭成员可能需要进行相关的结核病评估。
•我有权拒绝接受结核病筛查或抗结核治疗,但该行为可能影响申请赴英签证。
•医务人员对于是否给予医学证明具有最终决定权,我对此表示接受。
女性申请人:所有的女性申请人都将被询问末次月经时间以便确定是否妊娠。
•如果我已怀孕,以下几个检查方案可供我选择:⑴穿上铅保护裙后进行胸部X光检查;⑵将胸部X光检查(和结核病筛查)推迟到分娩后再进行;⑶连续留三次痰液标本用于实验室检查。
新西兰留学签证 体检表INZ1007[1]
![新西兰留学签证 体检表INZ1007[1]](https://img.taocdn.com/s3/m/82a297ed9b89680203d82540.png)
You may not need a new medical certificate if you have submitted a medical certificate completed and dated by an approved medical practitioner within the last 36 months with a previous application, and that information has been retained by Immigration New Zealand*. If a new certificate is required, you are responsible for ny registered medical practitioner is able to complete this certificate. If you do not have a doctor
* Immigration New Zealand does not necessarily retain medical information about applicants.
• Do not have alcohol or high fat meals 48 hours before your blood tests.
• Do not consume kava for 48 hours before your blood tests.
What do I bring?
• This certificate with sections A and I completed, and your name at the top of each page where indicated.
体检项目英文对照表
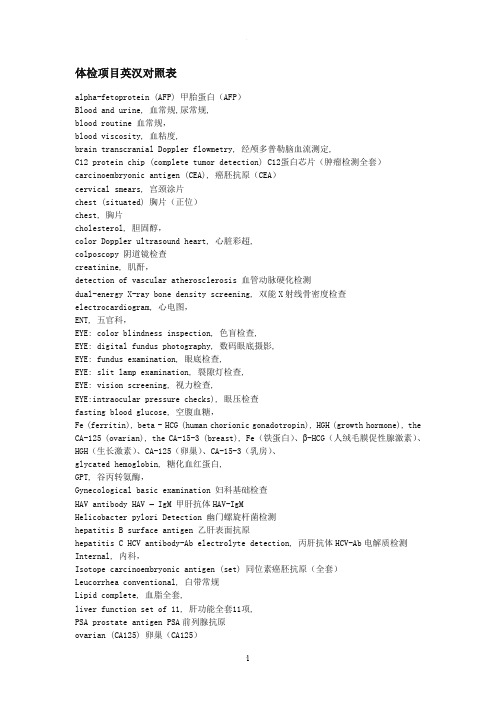
体检项目英汉对照表alpha-fetoprotein (AFP) 甲胎蛋白(AFP)Blood and urine, 血常规,尿常规,blood routine 血常规,blood viscosity, 血粘度,brain transcranial Doppler flowmetry, 经颅多普勒脑血流测定,C12 protein chip (complete tumor detection) C12蛋白芯片(肿瘤检测全套)carcinoembryonic antigen (CEA), 癌胚抗原(CEA)cervical smears, 宫颈涂片chest (situated) 胸片(正位)chest, 胸片cholesterol, 胆固醇,color Doppler ultrasound heart, 心脏彩超,colposcopy 阴道镜检查creatinine, 肌酐,detection of vascular atherosclerosis 血管动脉硬化检测dual-energy X-ray bone density screening, 双能X射线骨密度检查electrocardiogram, 心电图,ENT, 五官科,EYE: color blindness inspection, 色盲检查,EYE: digital fundus photography, 数码眼底摄影,EYE: fundus examination, 眼底检查,EYE: slit lamp examination, 裂隙灯检查,EYE: vision screening, 视力检查,EYE:intraocular pressure checks), 眼压检查fasting blood glucose, 空腹血糖,Fe (ferritin), beta - HCG (human chorionic gonadotropin), HGH (growth hormone), the CA-125 (ovarian), the CA-15-3 (breast), Fe(铁蛋白)、β-HCG(人绒毛膜促性腺激素)、HGH(生长激素)、CA-125(卵巢)、CA-15-3(乳房)、glycated hemoglobin, 糖化血红蛋白,GPT, 谷丙转氨酶,Gynecological basic examination 妇科基础检查HAV antibody HAV – IgM 甲肝抗体HAV-IgMHelicobacter pylori Detection 幽门螺旋杆菌检测hepatitis B surface antigen 乙肝表面抗原hepatitis C HCV antibody-Ab electrolyte detection, 丙肝抗体HCV-Ab电解质检测Internal, 内科,Isotope carcinoembryonic antigen (set) 同位素癌胚抗原(全套)Leucorrhea conventional, 白带常规Lipid complete, 血脂全套,liver function set of 11, 肝功能全套11项,PSA prostate antigen PSA前列腺抗原ovarian (CA125) 卵巢(CA125)prostate bladder B ultrasound 前列腺膀胱B超protein chip C12 C12蛋白芯片serum glucose, 空腹血糖,stomach Helicobacter pylori (antibody), 胃幽门螺旋杆菌(抗体)super microscope Subhealthy detection, 超高倍显微亚健康检测,surgery, 外科,the high-resolution microscope detection (a blood disease detection) 高分辨显微镜检测(一滴血疾病检测)three renal function, 肾功能3项,trace elements 微量元素Transvaginal Ultrasound 阴道彩超triglyceride, 甘油三脂,tumor detection screening (qualitative), 肿瘤筛选检测(定性)cardiovascular function diagnosis, 心血管功能诊断two pairs of semi - hepatitis B 乙肝两对半ultrasound (splenorenal major abdominal), B超(肝胆胰脾肾),unmarried female B ultrasound - (uterus, annex), 未婚女性B超(子宫,附件)urea nitrogen, 尿素氮,urine routine, 尿常规,whole blood viscosity 5. 全血粘度等5项,医院常用中英文对照汇编-供查询公共空间大厅Hall中药局ChineseMedicinePharmacy公用电话PublicTelephone/PayPhone/Telephone/PublicPhone日常生活训区DailyActivityTraining日间门诊ClinicArea日间院AdultDayCareCenter日间照护DayCareCenter出院室DischargeOffice加护病房IntensiveCareUnit(ICU)打卡刷卡区ClockIn/Out民众意箱Suggestions各科门诊Out-PatientDepartments(OPD)早产儿室PrematureBabies自动提款机ATM住院室Admissions佛堂BuddhistPrayerRoom吸烟区SmokingArea志工服务台VolunteerServices志工室Volunteers衣室DressingRoom巡箱PatrolBox夜间门诊EveningClinic居家护HomeHealthCare居家护室HomeHealthCare服务台(询问处)Information注射室Injections治室TreatmentRoom社福卫教室SocialWorkandHealthEducation门诊大厅OutpatientHall门诊注射室OutpatientInjection门诊部Out-patient门诊满意调查回收意箱SuggestionBox门诊检验OPDLaboratory待产室LaborRoom急诊暂观察室ERObservationRoom恢室RecoveryRoom候诊区WaitingArea员工意箱Suggestions晒衣场ClothesDrying气喘卫教室AsthmaHealthEducationRoom消毒室Sterilization消毒锅区EquipmentSterilization病房Ward病毒室ViralLaboratory健儿门诊WellBabyClinic医院常用中英文对照汇编公共空间健保卡换卡服务中心NationalHealthInsuranceCardRenewal 健检中心PhysicalExaminationCenter健检室PhysicalExamination产后妇中心PostpartumCareCenter产后护之家PostpartumCare发烧筛检站FeverClinic诊室ConsultingRoom新生儿病房NeonatalWard隔检疫舍QuarantineHouse团体治室GroupTherapy语言治室SpeechTherapy药处MedicineReceiving卫教公布HealthEducationBulletinBoard卫教室HealthEducationOffice婴儿室BabyRoom检查室ExaminationRoom总层引FloorPlan转诊中心ReferralCenter药物谘询DrugInformation药库DrugStorage护之家NursingHome台Terrace接待,服务及休闲区水间Kitchen/Drinkingwater/HotWater 饮水机DrinkingFountain配膳间MealChecking发厅Barbershop美发(容)院BeautySalon商店街ShoppingArcade员工餐厅StaffRestaurant/Cafeteria餐厅Restaurant西餐厅WesternRestaurant贵宾室GuestRoom/Reception会客室ReceptionRoom休息室Lounge家属休息室Lounge图书室Library阅览室ReadingRoom放映室ProjectionRoom影印室CopyRoom育婴室NurseryRoom/MotherandBabyRoom哺乳室NurseryRoom值班室DutyRoom驻警室Security警卫室SecurityRoom接待,服务及休闲区停管中心ParkingServiceCenter调室DispatchRoom司机室/司机调室Drivers‘Lounge值日室DutyRoom值班休息室DutyOffice医师休息室Physicians‘Lounge宿舍Dormitory儿童游戏场RecreationArea医器材贩卖部MedicalSupplyDispensary爱心椅CourtesyWheelchairs椅借用区MovableBeds政单位人资源部HumanResourcesDepartment人事室PersonnelOffice人事组PersonnelSection人事处DepartmentofPersonnel公安室IndustrialSafetyOffice工务科Maintenance公关室PublicRelationsRoom(Office)文卷室DocumentationandArchivesOffice主计室ComptrollerOffice出纳室Cashier出纳课CashierSection民诊处CivilianAdministrationDivision企划室StrategyPlanningOffice企划组PlanningSection企划组PlanningandManagementSection企划管部PlanningandManagementDivision安全卫生室LaborSafetyandHygiene成本执组CostManagementSection收发室MailRoom政副院长室AdministrativeDeputySuperintendent 政管中心Administration住/出/转院Admission/Discharge/Transfer住院病组InpatientRecordsUnit兵役复检室MilitaryServiceExamination批价柜台Cashier系统组SystemEngineeringSection防台中心TyphoonEmergencyCenter社会服务室SocialWorkerRoom社区副院长室CommunityDeputySuperintendent社会服务科SocialServiceSection门诊病组OutpatientRecordsUnit保险作业组InsuranceDeclarationSection急诊批价ERCashier科主任办公室Dept.ChiefOffice政单位疾病分析组DiseasesClassificationUnit 病室/组MedicalRecordsRoom/Unit/Section医院常用中英文对照汇编门诊组OutpatientUnit/Section住院组InpatientAdmissions秘书室AdministrationOffice院长室Superintendent挂号柜台Registration采购组ProcurementSection教学组TeachingSection工安全卫生室OccupationalSafetyOffice安室WorkSafetyOffice安课LaborSafetySection程式组ApplicationProgrammingSection勤务中心ServiceOffice感染控制委员会InfectionControlCommission会计室AccountingOffice会计组AccountingSection资讯管部InformationManagementDivision稽核组AuditingSection卫材供应组MedicalSupplySection档案室Archives营养部Food&NutritionDepartment总务室GeneralAffairsOffice总务组GeneralAffairsSection医品组QualityAssuranceSection医勤组MedicalServiceSection医学工程室MedicalEngineeringOffice医副院长室MedicalDeputySuperintendent药剂科主任室PharmacyChief床科部中医科ChineseMedicine中医科-内科ChineseInternalMedicine中医科-针灸科ChineseAcupuncture小儿科Pediatrics小儿科-心脏PediatricCardiology小儿科-外科PediatricSurgery小儿科-心肺PediatricCardiopulmonary小儿科-感染PediatricInfectiousDiseases小儿科-胃肠PediatricGastroenterology小儿科-眼科PediatricOphthalmology小儿科-神经科PediatricNeurology小儿科-遗传科PediatricGenetics小儿科-预防注射PediatricVaccinations床科部小儿科-一般门诊Pediatrics医院常用中英文对照汇编小儿科-青少门诊AdolescentHealth小儿科-过敏免疫风湿科PediatricAllergyImmunology 小儿科-血液肿瘤科PediatricHematology&Oncology 小儿科-科PediatricUrology小儿科-内分科PediatricEndocrinology小儿科-重症医学科PediatricIntensiveCare新生儿科加护病房NewbornICU小儿加护病房PediatricICU儿童急救加护医学科PediatricEmergencyandCriticalCareMedicine 小儿心肺功能室PediatricPFT优生保健科PerinatalGenetics内科InternalMedicine内科-一般门诊InternalMedicine:General内科-日间化学治DayChemotherapy内科-胃肠科Gastroenterology内科-胸腔科PulmonaryMedicine内科-肾脏科Nephrology内科-内分科Endocrinology内科-内分暨代谢科EndocrinologyandMetabolism内科-心脏(血管)内科CardiologyDept.内科-血液肿瘤科HematologyandOncology内科-人医学门诊Geriatrics内科-过敏免疫风湿科Rheumatology/Immunology/Allergy内科-神经Neurology内科加护病房MICU内科-肝胆胰内Hepatic-biliary-pancreaticMedicine内科-感染科InfectiousDisease牙科Dentistry(Dental)Dept.家庭牙医科FamilyDentistry牙科-特别门诊DentalSpecialtyClinic牙科一般门诊(初诊)DentalClinic-InitialVisit牙科复诊(约诊)DentalClinic-AppointmentOnly口腔颚面外科OralMaxillo-facialSurgery口腔病诊断科OralPathology齿颚矫正科Orthodontics儿童牙科PediatricDentistry牙周病科Periodontics补缀科Prosthodontics外科Surgery外科-小儿PediatricSurgery外科-骨科Orthopedics外科-神经Neurosurgery外科-手外科HandSurgery外科-消化系GastrointestinalSurgery外科-一般门诊Surgery-GeneralClinic床科部外科-大肠直肠Colo-rectalSurgery外科-整形PlasticSurgery医院常用中英文对照汇编外科-甲腺乳腺ThyroidandBreastSurgery外科-乳房BreastSurgeryClinic外科-心脏CardiacSurgery外科-心脏血管CardiovascularSurgery外科-胸腔ThoracicSurgery外科-美容外科CosmeticSurgery外科-肝胆HepaticSurgery外科-肝胆胰外Hepatic-biliary-pancreaticSurgery 外科-重建整形Plastic&ReconstructiveSurgery外科-胃肠及一般Gastroenterology&GeneralSurgery 骨外伤科OrthopedicTraumatology外科加护病房SurgeryICU皮肤科Dermatology皮肤科-一般门诊Dermatology-GeneralClinic皮肤科-职业性皮肤病OccupationalDermatology耳鼻喉科ENTDept.(Otolaryngology)耳鼻喉科-一般门诊GeneralENTClinic耳鼻喉科-门诊小手术MinorSurgery耳鼻喉科-鼻窦内视镜门诊SinusEndoscopy科Urology科-一般门诊Urology-GeneralClinic科-性失禁IncontinenceClinic科-男性孕症MaleInfertilityClinic科-性功能障碍SexualDysfunctionClinic孕症学科Infertility妇产科ObstetricsandGynecology妇产科-孕症InfertilityClinic妇产科-子宫颈癌CervicalCarcinomaClinic妇产科-羊水穿Amniocentesis妇产科-妇科肿瘤GynecologicalOncology妇产科-子宫颈病变CervicalDysphasiaClinic妇产科-妇期MenopauseClinic妇产科-快速子宫颈抹片ExpressSmearService妇产科-抹片及乳房检查PapSmear妇癌科GynecologicOncology妇科学科GynecologyUrology眼科Ophthalmology眼科-青光眼GlaucomaClinic眼科-斜弱视StrabismusandAmblyopia眼科-视网膜RetinaSection眼科-一般门诊Optometry-GeneralClinic眼科-兵役检查MilitaryServiceEyeExam眼科-配光检查Optometry眼科-视保健VisionProtectionClinic床科部眼科-萤光摄影FluorescentPhotography眼科射OphthalmologicLaserTherapy精神科Psychiatry医院常用中英文对照汇编精神科-身心内科PsychosomaticClinic精神科-焦虑忧郁失眠门诊AnxietyandInsomniaClinic精神科-癌症团体心治GroupCancerTherapy精神科-儿童青少特别门诊(限18岁以下)YouthPsychiatry 放射线科Radiology核医科NuclearMedicine疼痛科PainManagement麻醉科Anesthesiology(Anesthesia)Dept.健科Rehabilitation解剖病科AnatomicalPathology预防注射科ProphylacticImmunization病科Pathology青少谘询特别门诊JuvenilePsychiatryDepartment肿瘤科Oncology神经内科Neurology神经外科Neurosurgery家庭医学科FamilyMedicine社区医学部CommunityMedicine心血管加护病房CardiacCU(CCU)心血管中心CardiovascularCenter心脏血管外科加护病房CardiovascularSurgeryICU急诊EmergencyDept.急诊医学科EmergencyMedicine内视镜科EndoscopySection血液透析Hemodialysis肝胆科Hepatology高危险妊娠症学科High-riskPregnancy安护HospiceCenter职业病科OccupationalMedicine放射肿瘤科RadiationOncology保健科PreventiveMedicine运动医学科SportMedicine肺结核加护病房TBICU外伤加护病房TraumaICU健康检查中心HealthEvaluationCenter脑血管中心CerebralVascularClinic神经医学中心BrainCenter烧伤中心BurnCenter癌症中心Cancercenter癌症防治中心CancerControlandPreventionCenter高压氧治中心HyperbaricOxygenTherapyCenter肥胖防治中心WeightReducing床科部洗肾中心HemodialysisCenter医学美容中心MedicalCosmeticCenter医学影像中心MedicalImageCenter运动健中心Rehabilitation-ExerciseCenter医院常用中英文对照汇编病人保健推广中心DiabeticCenter中西合作医中心Chinese-WesternCooperativeTreatmentCenter社区护HomeCare护之家NursingHome护部NursingDept./NursingDepartment护长室HeadNurse医技术CT登记处CTAdmissionX光摄影室(借片室)X-rayRoom孕症谘询室InfertilityConsultationRoom内分检查室EndocrineExaminationRoom内科诊查室InternalMedicineClinic内视镜室Endoscopy化学治Chemo-Therapy心电图室EKG心导管室CardiacCatheterizationRoom心脏血管中心CardiovascularCenter心脏血管检查室CardiovascularExaminations心脏超音波HeartEcho水室Hydrotherapeutics生化实验室BiochemicalLab生检查科PhysiologicalExam皮肤病诊断中心DermologicalPathologicalCenter 石膏室PlasterRoom光子刀治中心PhotonKnifeCenter多功能超音波室Multi-FunctionEchoRoom肌电图室EMG血库BloodBank血液肿瘤科Hematology血清免疫学实验室Immu-serologicalLab血管功能检查室VascularFunctionTest血管摄影室CardiacAngiography动检查室UrokineticExam.Room技术室TechnicalSupportDivision乳房超音波BreastEcho乳房摄影室Mammography儿童治室PediatricTherapyRoom儿童物治室PediatricPhysicalTherapy儿童职能治室PediatricOccupationalTherapy 呼吸治RespiratoryTherapy放射免疫分析室RadioimmunoassayUnit放射科登记室RadiologyRegistration医技术放射线治科Radiotherapy科微波热室GenitouroUrologic超音波UrologyEcho物治PhysicalTherapy物职能治室OccupationalandPhysicalTherapy 医院常用中英文对照汇编肺功能PFT肺功能室PulmonaryFunctionTesting门诊检验OupatientCheck-UPS门诊体检PhysicalCheck-Ups急诊X光室ERX-RayRoom胃镜室EndoscopyRoom胎儿影像中心3DLiveImageCenter气管镜室BronchoscopyRoom特殊检查室SpecialExamination胸部超音波ChestEcho闪烁摄影室DiagnosticImagingUnit骨质密检查室BoneDensity骨骼肌肉超音波室EchoforSkeletalMuscles 采室UrineCollectionRoom产房DeliveryRoom细胞遗传室Cytogenetics细菌研究室BacterialLaboratory麻醉科实验室AnesthesiologyLaboratory健科治室RehabilitationTherapy紫外线光室UltravioletTherapy肾功能室RenalFunction肾脏超音波RenalEcho视检查室Check-upforEyeSight周边血管室PeripheralVascularExamination 微生物实验室MicrobiologicalLab新生儿观察室ObservationRoom-NewBornBabies 眩检查室VertigoTest准分子射室LaserTreatment腹部超音波Abdominalecho腹膜透析室CAPD脑波室EEGUnit解剖病科实验室AnatomicalPathologyLaboratory 运动治室TherapeuticExerciseRoom射治室LaserTherapy电脑断层摄影室CTScanUnit电室ElectrotherapyRoom磁振造影扫描室MRIUnit膀胱功能室BladderFunctionTest膀胱镜室CystoscopyRoom语言治SpeechTherapy器官移植OrganizationTransplantation医技术检伤分Triage检验室Laboratory检验科LaboratoryMedicine检体收发室SpecimenCollection检体受紧急报告取EmergencyProcedure检体处室LabSamples医院常用中英文对照汇编营养室NutritionDept.床病室ClinicalPathology职能治OccupationalTherapy医务室(医站)Clinic药剂科(药局)Pharmacy摄影室DigitalImage听检查室HearingExam.Room体外震波碎石机Lithotripsy机械及电器场所总机PhoneOperator‘sRoom库房/储藏室/材库Storeroom/Storage卸货区LoadingArea变电室TransformerRoom/Substation/PowerRoom变电站PowerSub-station电气室ElectricalControlRoom/ElectricRoom配电室ElectricalDistributionFacilities中控室CentralControlRoom中央控制室ControlCenter能源设施部PowerSupplyDivision机械室MachineRoom工具间ToolRoom电脑机房ComputerFacilities资讯室机房DataProcessing发电机房Generators空调机房AirConditioningFacilities空调机械室AirConditioningFacilities/Air-conPlant 紧急出口/安全门EmergencyExit安全门Exit避难方向EvacuationRoute灭火器FireExtinguisher缓机/缓梯EscapeSling消防箱FireHose/Hydrant逃生梯EmergencyLadder通报设备AlertFacilities紧急照明EmergencyLight消防设备/消防栓Hydrant紧急电源EmergencyPower紧急避难梯EmergencyLadder/EmergencyStaircase防空避难处Air-raidShelter会议场所及教室会议室ConferenceRoom简报室BriefingRoom讨室MeetingRoom/SeminarRoom阅览室ReadingRoom研讨室MeetingRoom,SeminarRoom医师研究室Physicians‘Office医师讨室Physicians‘MeetingRoom医院常用中英文对照汇编研究室StudyRoom音控室AudioContralRoom演讲厅(大堂)Auditorium演讲室LectureRoom国际会议厅ConferenceHall第一会议室ConferenceRoomI第二会议室ConferenceRoomII会议室及图书室ConferenceRoomandLibrary盥洗场所化妆室/厕所Women‘sRestroom/Ladies‘Restroom 男化妆室/男厕所Men‘sRestroom/Gentlemen‘sRestroom 洗手间/盥洗室Restroom身心障碍专用厕所DisabledRestroom浴室Shower储藏及仓库中央供应室CentralSupplyCenter中央库房CentralStorage供应室SupplyRoom清洁工具室JanitorsRoom急诊清洁室ERJanitor洗衣房Laundry汅物间SoiledMaterials清洁班CleaningCrew告示或警告标示施工中UnderConstruction禁止吸烟NoSmoking禁止饮食NoFoodorDrink禁食槟榔Chewingbetelnutisprohibited禁止携带物NoPets严禁烟火NoOpenFlames请勿(禁止)进入NoEntry闲人勿进AuthorizedPersonnelOnly节约用水PleaseConserveWater请勿攀爬NoClimbing请用雨伞套PleaseUsePlasticUmbrellaCover随手关门KeepClosed随手关灯TurnOffLightsWhenLeaving高压危险,有电勿靠近KeepClear-HighVoltage电器设备,严禁擅入Donotenter!PowerEquipment告示或警告标示请取号码牌,静候叫号时迳往挂号处挂号Takeanumber.Gotocounterwhennumberiscalled.防火门火警时随手关门FireEscape-PleaseKeepClosed避难出口高逃生缓机EmergencyExit&EscapeSling紧急疏散方向图EvacuationPlan禁止将投手伸出扶梯外Pleasedonotstretchoutyourhandorhead您的位置Youarehere电梯内请勿交谈,请戴口罩Donottalkinelevator,Pleaseputonrespirator医院常用中英文对照汇编严禁工作人员戴手套触摸按钮Employee,pushingbuttomwithyourgroveonis prohibited资源回收及垃圾资源回收/垃圾分Recycling塑胶Plastic垃圾桶Trash垃圾处室DisposalArea特殊空间太平间Morgue其它药物医药分业谘询专线MedicalandPharmaceuticalConsultationInquiries 申诉案件及政革新专线Citizens‘Hotline身体健康检查谘询预约服务专线PhysicalExamination出入口及专用道请勿停NoParking请勿暂停NoStanding身心障碍专用坡道DisabledRamp入口Entrance出口Exit/WayOut(标示於地面)遵方向ThisWay汽出入口VehiclesExiting入口道ParkingEntrance位已满请勿进入NoVacancy限高MaxHeadroom停场停场(区)ParkingLot平面停场ParkingLot地下停场UndergroundParking体停场ParkingTower宾专用停位ReservedParking机停位MotorcycleParking身心障碍专用停位DisabledParkingOnly院内员工专用停场StaffOnly计程招呼站TaxiStand停场救护Ambulance电(扶)梯及梯电梯Elevator电扶梯Escalator紧急用电梯EmergencyElevator梯Stairs访客电梯VisitorElevator本电梯直达6-12Floor6and12Only本电梯限停1-5层1,2,3,4,5Only医院常用中英文对照汇编书表慢性病续处方笺ChronicIllnessPrescriptionSlip 慢性病续处方笺ChronicContinuousPrescription慢性病续处方笺RefillPresriptionsForChroniDisease 诊断书MedicalCertificate挂号费RegistrationFee证明费CertificationFee费AmbulanceFee特定医费SpecialMedicalFee部份负担费Self-PaymentFee诊察费DiagnosticFee病房费WardFee伙食费DietFee检查费LaboratoryFee放射线诊费X-RayFee治处置费TherapeuticTreatmentFee手术费OperationFee健治费RehabilitationTherapy血液血浆费BloodProductFee血液透析费HemodialysisFee麻醉费AnestheticFee特殊材费SpecialMedicalSupplyFee药费MedicineFee。
英文健康体检表 CERTIFICATE OF HEALTH
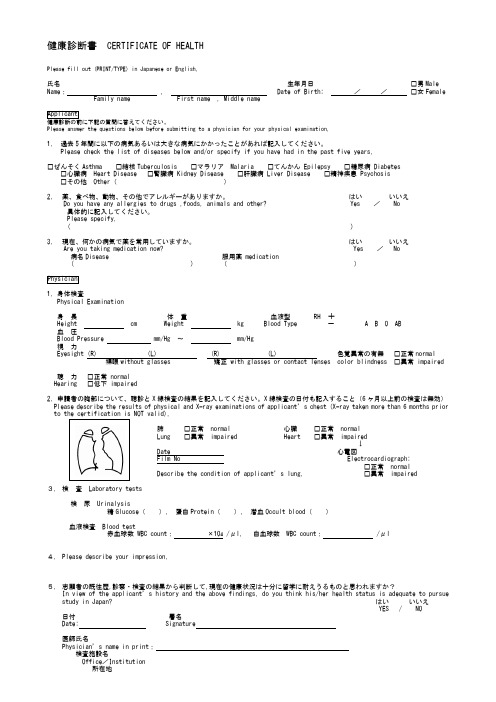
健康診断書CERTIFICATE OF HEALTHPlease fill out (PRINT/TYPE) in Japanese or English.氏名生年月日□男Male Name: , Date of Birth: //□女Female Family name First name , Middle nameApplicant健康診断の前に下記の質問に答えてください。
Please answer the questions below before submitting to a physician for your physical examination.1. 過去5年間に以下の病気あるいは大きな病気にかかったことがあれば記入してください。
Please check the list of diseases below and/or specify if you have had in the past five years.□ぜんそくAsthma □結核Tuberculosis □マラリアMalaria □てんかん Epilepsy □糖尿病 Diabetes □心臓病Heart Disease □腎臓病 Kidney Disease □肝臓病 Liver Disease □精神疾患 Psychosis□その他Other()2.薬、食べ物、動物、その他でアレルギーがありますか。
はいいいえDo you have any allergies to drugs ,foods, animals and other? Yes /No具体的に記入してください。
Please specify.( )3.現在、何かの病気で薬を常用していますか。
はいいいえAre you taking medication now? Yes / No 病名Disease 服用薬 medication( ) ()Physician1. 身体検査Physical Examination身長体重血液型 RH +Height cm Weight kg Blood Type - A B O AB血圧Blood Pressure mm/Hg ~mm/Hg視力Eyesight (R) (L) (R) (L) 色覚異常の有無□正常normal 裸眼without glasses 矯正 with glasses or contact lenses color blindness □異常 impaired聴力□正常 normalHearing □低下 impaired2. 申請者の胸部について、聴診とX線検査の結果を記入してください。
中英文体检表格
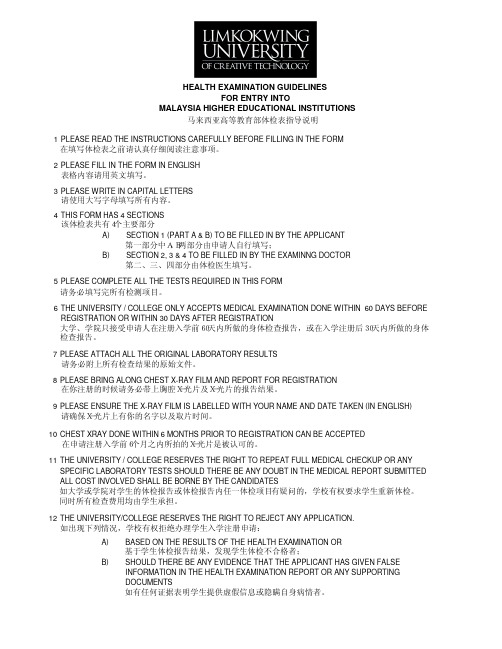
MALAYSIA HIGHER EDUCATIONAL INSTITUTIONS 马来西亚高等教育部体检表指导说明
1 PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM 在填写体检表之前请认真仔细阅读注意事项。
Date
Signature of candidate
2
SECTION 2 - PHYSICAL EXAMINATION To be filled by examining doctor
1. BASIC MEASUREMENT
HEIGHT : __________________ m WEIGHT : __________________ kg
____________________________________ ____________________________________
IMMUNIZATION HISTORY (where applicable)
1. Yellow Fever 2. BCG 3. Meningitis (Quadrivalent) 4. Hepatitis B 5. Others:
MEDICAL PROBLEMS
1. Congenital or inherited disorder 2. Allergy 3. Mental illness 4. Fits, stroke, other neurological disease 5. Diabetes Mellitus 6. Hypertension 7. Heart or vascular disease 8. Asthma 9. Thyroid disease 10. Kidney disease 11. Cancer 12. Tuberculosis 13. Drug addiction 14. AIDS, HIV 15. History of surgery 16. Other illnesses
出国免疫接种情况表中文翻译
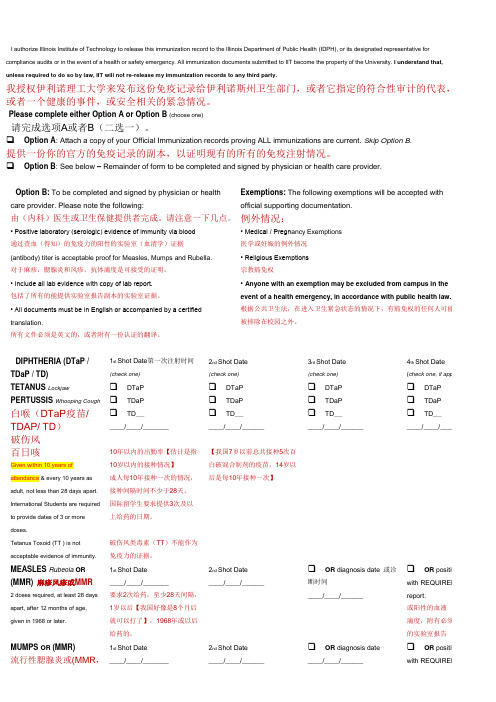
I authorize Illinois Institute of Technology to release this immunization record to the Illinois Department of Public Health (IDPH), or its designated representative for compliance audits or in the event of a health or safety emergency. All immunization documents submitted to IIT become the property of the University. I understand that, unless required to do so by law, IIT will not re-release my immunization records to any third party.我授权伊利诺理工大学来发布这份免疫记录给伊利诺斯州卫生部门,或者它指定的符合性审计的代表,或者一个健康的事件,或安全相关的紧急情况。
Please complete either Option A or Option B (choose one)请完成选项A或者B(二选一)。
❑ Option A: Attach a copy of your Official Immunization records proving ALL immunizations are current. Skip Option B.提供一份你的官方的免疫记录的副本,以证明现有的所有的免疫注射情况。
❑ Option B: See below – Remainder of form to be completed and signed by physician or health care provider.Option B: To be completed and signed by physician or health care provider. Please note the following: Exemptions: The following exemptions will be accepted with official supporting documentation.由(内科)医生或卫生保健提供者完成。
出国(境)人员健康体检必查项目
出国(境)人员健康体检必查项目
出国(境)人员健康体检必查项目
一、常规检查项目
(一)内科常规检查:身高、体重、腹围、血压、既往史。
(二)外科常规检查:脊柱、四肢、甲状腺、淋巴结,乳腺(女)。
(三)眼科检查:眼底。
(四)妇科检查(女)。
二、生化检验项目
(一)肝功能:谷草转氨酶、谷丙转氨酶、总蛋白、白蛋白、球蛋白、白/球、总胆红素、直接胆红素、间接胆红素、r-转肽酶、碱性磷酸酶、总胆汁酸。
(二)肾功能:尿素、肌酐、尿酸。
(三)空腹血糖。
(四)血脂:胆固醇、甘油三脂、载脂蛋白A1、载脂蛋白B、高密度脂蛋白、低密度脂蛋白。
(五)心肌酶谱:磷酸肌酸激酶同工酶、乳酸脱氢酶、磷酸肌酸激酶、a-羟丁酸脱氢酶。
(六)血常规、尿常规、便常规+潜血。
(七)类风湿因子、抗链“O”、C-反应蛋白、血沉。
(八)凝血四项。
马来西亚博特拉大学(UPM)体检表(英文版)

HEALTH EXAMINATION REPORT FOR INTERNATIONAL STUDENTAND ACCOMPANYING PERSONPLEASE USE CAPITAL LETTERSSECTION 1 (To be completed by candidate)(PART A)FULL NAME (AS IN PASSPORT)INTERNATIONAL PASSPORT NO.NATIONALITY CONTACT NUMBERDATE OF BIRTH AGE SEX MARITAL STATUSMALE SINGLE D D M M Y Y FEMALE MARRIEDACADEMIC YEARSTUDENT IDPROGRAMME OF STUDY PROGRAMME CODENEXT OF KINNEXT OF KIN’S ADDRESSNEXT OF KIN’S CONTACT NUMBER ./SECTION 1(PART B) – Please tick ( √ ) in the relevant boxDeclaration of self and family illness. Explain in full if you or your family has any of the following illnesses. * Immediate family refers to father, mother, brothers / sistersSELF IMMEDIATE FAMILYMEDICAL PROBLEMSYes No Yes NoIf “Yes” please state.1. Congenital or inherited disorder2. Allergy3. Mental illness4. Fits, stroke, other neurological disease5. Diabetes Mellitus6. Hypertension7. Heart or vascular disease8. Asthma9. Thyroid disease10. Kidney disease11. Cancer12. Tuberculosis13. Drug addiction14. AIDS, HIV15. History of surgery16. Other illnessesCurrent medication (Long term)____________________________________ ____________________________________ ____________________________________ ____________________________________IMMUNIZATION HISTORY(where applicable)DATE IMMUNIZED1. Yellow Fever2. BCG3. Meningitis (Quadrivalent)4. Hepatitis B5. Others:I hereby certify that the information given above is true. I understand that my application will berejected if there is any false information given.Date Signature of candidateSECTION 2 - PHYSICAL EXAMINATIONTo be filled by examining doctor1. BASIC MEASUREMENTHEIGHT : __________________ m BLOOD PRESSURE : ______________ mmHg WEIGHT : __________________ kg PULSE RATE : ______________ / minVISION TEST : Unaided : (R) _______ (L) ________ Aided : (R) _______ (L) ________ COLOUR VISION TEST :NORMAL / ABNORMAL2. GENERAL EXAMINATIONITEM YES NO COMMENTa. DEFORMITIESb. PALLORc. CYANOSISd. JAUNDICEe. OEDEMAf. SKIN DISEASES3. SYSTEMIC EXAMINATIONITEM NORMAL ABNORMAL COMMENTa. EYES (including funduscopy)b. EARSc. NOSEd. ORAL CAVITY / THROATe. NECKf. HEARTg. LUNGSh. ABDOMEN / HERNIA ORIFICESi. NERVOUS SYSTEMj. MENTAL CONDITIONk. MUSCULOSKELETAL SYSTEMSECTION 3 - INVESTIGATIONSURINE TESTITEM DATE TAKEN RESULTa. ALBUMINb. SUGARc. MICROSCOPICd. MORPHINEe. CANNABISf. AMPHETAMINES TYPESTIMULANTBLOOD TESTITEM DATE TAKEN RESULTa. HEPATITIS Bs ANTIGENb. HEPATITIS Cc. HIVd. VDRL / TPHAe. MALARIAL PARASITECHEST X-RAY INFORMATIONCHEST X-RAY NO.DATE TAKENPLACE TAKENREPORTSECTION 4 - CERTIFICATION BY THE EXAMINING DOCTORPlease tick (√) in the appropriate boxI certify that I have on this date ___________________ examinedMr / Ms ___________________________________ Passport No. ____________________ and found him / her :-Date Signature of Doctor : Name of Doctor : Qualification : Hospital / ClinicRegistration Number :Official stamp:_________________________________________________________________________Remarks By University/College Official :IN GOOD HEALTHHAVING THE FOLLOWING MEDICAL COMPLICATION(S) (Please State)____________________________________________________ ____________________________________________________ ____________________________________________________UNDERGOING TREATMENT FOR: (Please State)____________________________________________________ ____________________________________________________ ____________________________________________________。
中英文对照体检表
腹 部 超 检 查
Abdominal colour to exceed examinati
on
结果(Test results):正常 Normal
医师签字(Signature of physician):
Medical conclusio ns and recommend ations
体检结论(Medical conclusion):体检结果正常。
Medical results normal.
保健建议(Care advice):
主检医师签字(Signature of physician):
医院盖章
2013年月日
检验项目
Blood test projects
血 常 规
Routine
(-)
脾Spleen
(-)
其他Other
(-)
建议Proposal
正常Normal
医师签字Signature of physician
外
科Surgical
病史(history):(-)
甲状腺
Thyroid
(-)
淋巴结
Lymph node
(-)
脊柱Spine
(-)
皮肤Skin
(-)
四肢关节Limb joints
体检编号:
Physical examination No.:
xxxxx
XXXX Hospital
体检表
Examination table
XXXXXX医院2013年制
姓 名
Name
性 另
Gender
年龄Age
体检项目中英文对照表
体检项目对照表
T1:物理体检、尿检(含镜检)、静止心电图
T2:T1+血液检查(HbsAg、ALT、AST、Glu、HDL、CHO、TG、r-GT)、
血常规
中文名称
英文缩写 备注 乙肝表面抗原 HbsAg 丙氨酸氨基转移酶 ALT 天门冬氨酸氨基转移酶 AST 葡萄糖(空腹血糖) GLu 高密度脂蛋白胆固醇 HDL 同HDL-C 总胆固醇 CHO 同TCHO 甘油三酯 TG 谷氨酰转肽酶 r-GT
T3:T2+血液检查(乙肝二对半、AKP、TBIL、DBIL、TP、A/G)、
肾功能(BUN、Cr)、腹部(妇科)B超(说明:腹部B超所含项目为:肝、胆、胰、脾、双肾、前列腺(>50周岁,男))
中文名称
英文缩写 备注 乙型肝炎病毒表面抗原 HBsAg 乙肝二对半
乙型肝炎病毒表面抗体 HBsAb 乙型肝炎病毒 e 抗原 HBeAg 乙型肝炎病毒 e 抗体 HBeAb 乙型肝炎病毒核心抗体 HBcAB 碱性磷酸酶 AKP ALP 总胆红素 TBIL 直接胆红素
DBIL
总蛋白 TP
白/球比值 A/G
尿素 BUN
肾功能 肌酐 Cr(CREA)
¾T4:T3+血液检查HCV-抗体、HIV、HBA1C(糖化血红蛋白)、胸片
中文名称 英文缩写 备注 丙肝抗体 HCV-抗体
艾滋病抗体 HIV
糖化血红蛋白 HBA1C
¾T5:T4+血液检查AFP、CEA、肺功能、运动平板心电图
中文名称 英文缩写 备注 甲胎蛋白 AFP
癌胚抗原 CEA。
英文健康体检表 CERTIFICATE OF HEALTH常用

英文健康体检表CERTIFICATE OF HEALTH (可以直接使用,可编辑优质资料,欢迎下载)健康診断書CERTIFICATE OF HEALTHPlease fill out (PRINT/TYPE) in Japanese or English.氏名生年月日□男MaleName: , Date of Birth: //□女FemaleFamily nameFirst name,Middle nameApplicant健康診断の前に下記の質問に答えてください。
Please answer the questions below before submitting to a physician for your physical examination.1. 過去5年間に以下の病気あるいは大きな病気にかかったことがあれば記入してください。
Please check the list of diseases belowand/or specify if you have had in the past five years.□ぜんそくAsthma □結核Tuberculosis □マラリアMalaria □てんかん Epilepsy □糖尿病 Diabetes □心臓病Heart Disease □腎臓病 Kidney Disease □肝臓病 Liver Disease□精神疾患 Psychosis□その他Other()2.薬、食べ物、動物、その他でアレルギーがありますか。
はいいいえDo you have any allergies to drugs ,foods, animals and other? Yes /No具体的に記入してください。
Please specify.( )3.現在、何かの病気で薬を常用していますか。
はいいいえAre you taking medication now? Yes / No 病名Disease 服用薬medication( ) ()Physician1. 身体検査Physical Examination身長体重血液型 RH +Height cm Weight kg Blood Type - AB O AB血圧Blood Pressure mm/Hg ~mm/Hg視力Eyesight (R) (L) (R) (L) 色覚異常の有無□正常normal裸眼without glasses 矯正 with glasses or contact lenses color blindness □異常 impaired聴力□正常 normalHearing □低下 impaired2. 申請者の胸部について、聴診とX線検査の結果を記入してください。
中英文对照医院体检表(出国办签证所用)
体检编号:Physical Examination No:体检表Examination tableXXX医院2015年制编号/N0:姓名/Given Names:出生日期/Date性别/Sex:国籍血型/Blood Type:签证地址/Address of issue一般检查/General Check身高/Height: 厘米/cm 体重Weight:千克/kg 脉搏/Pulse rate:血压BP:毫米汞柱mmHg 体温Temperature: ℃内外科/Medicine & Surgery皮肤、巩膜、淋巴结/Skin,Sclera,Lymph Nodes:头部和颈部/Head &Neck:胸部和肺部/Chest &Lungs:心脏/Heart:腹部/Abdomen:脊柱和四肢/Spine & Extremities:神经精神系统/Neuropsychiatric System:泌尿生殖系统/Genitourinary System:五官科/E.E。
N。
T裸眼视力/Innc.Vision 左/Left: 右/Right: 矫正视力/Corr。
Vision 左/Left:右/Right:辨色力/Color Sense:听力/Hearing 左/Left: 右/Right:眼、耳、鼻、喉/Eyes,Ears,Nose,Throat:心电图/ECG胸部X线/Chest X—ray:实验室检查/Laboratory Tests:艾滋病病毒抗体/Anti—HIV:梅毒血清学检测/Syphilis Serology:乙型肝炎表面抗体/HBsAg:丙型肝炎抗体/Anti—HCV:丙氨酸氨基转移酶/ALT(GPT):血常规/Blood Routine:白细胞总数/WBC:红细胞总数/RBC:血小板总数/PLT:血红蛋白/HGB:粉细胞百分比/NEUT%:淋巴细胞百分比%:结论/General Comments:负责医生姓名印章Name of doctor in charge Official stamp负责医生签名Signature of doctor in charge签发日期Date of issue。
29国中英文对照出入境单!不收藏后悔呀!!
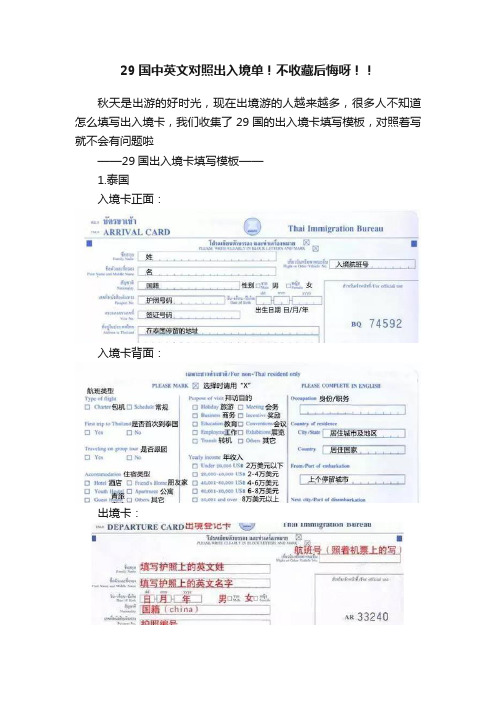
29国中英文对照出入境单!不收藏后悔呀!!秋天是出游的好时光,现在出境游的人越来越多,很多人不知道怎么填写出入境卡,我们收集了29国的出入境卡填写模板,对照着写就不会有问题啦——29国出入境卡填写模板——1.泰国入境卡正面:入境卡背面:出境卡:2.巴厘岛巴厘岛入境卡:巴厘岛海关申报单:3.越南越南入境卡:越南海关申报卡:4.菲律宾菲律宾入境卡:菲律宾海关申报单:5.马来西亚马来西亚入境卡:马来西亚海关申报单:6.新加坡新加坡入境卡:7.塞班岛塞班岛入境卡:8.马尔代夫马尔代夫入境卡:马尔代夫健康卡:9.埃及埃及入境卡:10.柬埔寨柬埔寨入境卡:柬埔寨海关申报单:11.老挝老挝出入境卡:12.斐济斐济出入境卡:13.韩国韩国入境卡:韩国入境物品申报单:14.印度印度入境卡:印度出境卡:15.印度尼西亚印度尼西亚入境卡:印度尼西亚海关申报单:16.毛里求斯毛里求斯入境卡:毛里求斯健康卡:17.尼泊尔尼泊尔入境卡:尼泊尔出境卡:18.南非南非入境卡:19.肯尼亚肯尼亚入境卡:20.阿根廷阿根廷入境卡:21.澳大利亚澳大利亚入境卡:澳大利亚出境卡:22.新西兰新西兰入境卡:23.法国法国入境卡:24.加拿大加拿大入境卡:25.美国美国入境卡:26.英国英国入境卡:27.斯里兰卡斯里兰卡入境卡:28.日本日本入境卡:29.秘鲁秘鲁入境卡:秘鲁海关申报单:——出入境填表常用词汇——姓:Family name,Surname名:First Name,Given name性别:sex,gender男:male;女:female国籍:nationality,country of citizenship 护照号:passport number航班号:Flight number原住地:country of origin前往国:destination country登机城市:city where you boarded签证签发地:city where visa was issued 签发日期:date of issue出生日期:date of birth,birth date 年:year;月:month;日:day偕行人数:accompanying number签名:signature官方填写:official use only职业:occupation护照:Passport;签证:Visa登机、启程:Embarkation登岸:Disembarkation商务签证:Business Visa观光签证:T ourist Visa。
出入境人员体检申请表doc
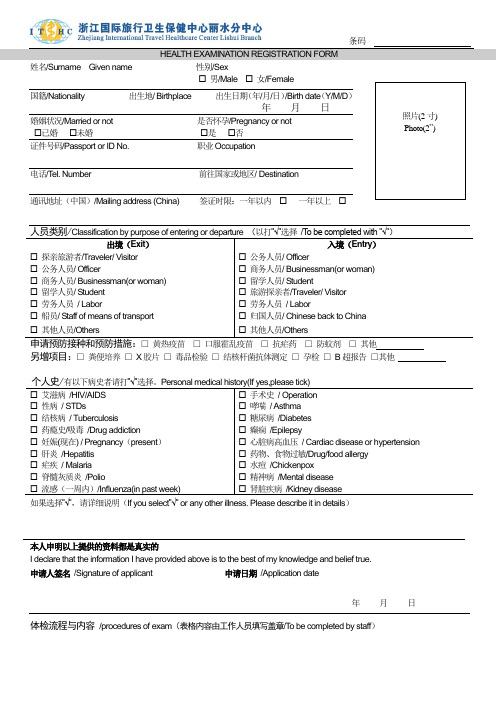
姓名/Surname Given name 性别/Sex ☐ 男/Male ☐ 女/Female 国籍/Nationality 出生地/ Birthplace 出生日期(年/月/日)/Birth date (Y/M/D ) 年 月 日 婚姻状况/Married or not 是否怀孕/Pregnancy or not ☐已婚 ☐未婚 ☐是 ☐否 证件号码/Passport or ID No. 职业Occupation电话/T el. Number 前往国家或地区/ Destination通讯地址(中国)/Mailing address (China) 签证时限:一年以内 ☐ 一年以上 ☐出境(Exit )入境(Entry )☐ 探亲旅游者/Traveler/ Visitor ☐ 公务人员/ Officer☐ 公务人员/ Officer☐ 商务人员/ Businessman(or woman) ☐ 商务人员/ Businessman(or woman) ☐ 留学人员/ Student☐ 留学人员/ Student ☐ 旅游探亲者/Traveler/ Visitor ☐ 劳务人员 / Labor☐ 劳务人员 / Labor☐ 船员/ Staff of means of transport ☐ 归国人员/ Chinese back to China ☐ 其他人员/Others☐ 其他人员/Others□ 黄热疫苗 □ 口服霍乱疫苗 □ 抗疟药 □ 防蚊剂 □ 其他另增项目:□ 粪便培养 □ X 胶片 □ 毒品检验 □ 结核杆菌抗体测定 □ 孕检 □ B 超报告 □其他个人史/☐ 艾滋病 /HIV/AIDS ☐ 手术史 / Operation ☐ 性病 / STDs ☐ 哮喘 / Asthma ☐ 结核病 / Tuberculosis ☐ 糖尿病 /Diabetes ☐ 药瘾史/吸毒 /Drug addiction ☐ 癫痫 /Epilepsy ☐ 妊娠(现在) / Pregnancy (present ) ☐ 心脏病高血压 / Cardiac disease or hypertension ☐ 肝炎 /Hepatitis ☐ 药物、食物过敏/Drug/food allergy ☐ 疟疾 / Malaria ☐ 水痘 /Chickenpox ☐ 脊髓灰质炎 /Polio ☐ 精神病 /Mental disease ☐ 流感(一周内)/Influenza(in past week) ☐ 肾脏疾病 /Kidney disease 如果选择”√”,请详细说明(If you select ”√” or any other illness. Please describe it in details )本人申明以上提供的资料都是真实的I declare that the information I have provided above is to the best of my knowledge and belief true. 申请人签名 /Signature of applicant 申请日期 /Application date年 月 日体检流程与内容 /procedures of exam (表格内容由工作人员填写盖章/T o be completed by staff )照片(2寸) Photo(2”)咨询填表Fill in your form人像登记form-photo登记缴费registration采血/phlebotomize以下服务不分先后/In no particular order服务项目体检结果描述医师签字/盖章内科/Internal medicine心率次/分bmp;血压 mmHg外科/Surgery身高 CM 体重 Kg五官科/ E.N.T视力:左右听力:左右心电图/ECGX 摄片/X-ray(怀孕者务必申明/Pregnancy must be declared)B 超/B-Ultrasound妇科/Gynecology咨询窗口/Registration Room领尿杯/Urine check 免费早点/Free breakfast注意:体检完毕请将此体检卡交回咨询窗口,以免耽误证件制作,谢谢合作!Notice: Please hand in the form to registration Room, thank you!﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉﹉温馨提示Tips for physical exam★体检前需空腹,携带护照或身份证原件;★孕妇和14周岁以下儿童不宜接受X光胸片检查,请及时告知窗口工作人员;1. ★前往非洲、南美洲国家需接种“黄热疫苗”请及时与咨询人员联系;2. ★出国留学人员预防接种要求请与咨询人员联系并确定目的地国学校的要求,已经接种的项目请提供当地社区医院预防接种原始记录后换签;3. ★领证时间:10:30之前体检者当日下午4:00后取证,10:30之后体检者第二个工作日下午4:00后取证,领取证书需凭交费发票。
赴美移民体检信息登记表

11377
1.23美领所在地(城市/国家)
U.S. Consul (City, Country)
广州,GUANGZHOU
1.24上次移民体检的日期(月/日/年),如果有
Date of Prior pre-visa medical Exam, if any (mm-dd-yyyy)
赴美移民体检信息登记表
Panel Exam Registration for U.S.-bound Applicants
1.1姓名(姓,名)
Name (Last, First, MI)
1.2性别
Sex
1.3出生地(城市和国家)*
Birthplace (City, Country)
(中英文、英文大写)
1.20计划在美国居住的城市*
Intended US City(英文大写)
1.21电子邮件
E-mail Address
1.22美国居住地址的邮编*
Intended US Postal Code
1.23美领所在地(城市/国家)
U.S. Consul (City, Country)
1.24上次移民体检的日期(月/日/年),如果有*
1.4签证类型:
Visa Category
1.5职业
Occupation
1.6文化程度
Degree of education
1.7去领馆面谈日期
Date of interview
1.8档案号码◆
Alien (Case) Number
1.9护照号码
Passport Number
1.10出生日期(月-日-年)
1.16计划在美国居住的地址*
医院科室牌标牌中英文对照表
医院科室牌标牌中英文对照表病房楼楼层总索引Layout of Inpatient Building大厅 Lobby卫事中心 Patient-aid center小卖部 Buffet出院病人领取费用清单 List of expenses for discharged patients普通病人出院结帐 Check-out for common discharged patients住院登记收费 Check-in for inpatients医保社保出院结帐 Check-out for patients with medical / social insurance 病区药房 Ward dispensary输血科 Transfusion section急诊化验 Emergency lab急诊手术室 Emergency operating theatre门诊手术室 Clinic operating theatre出入院病人接待处 Reception of inpatients(二病区)重症监护 ICU ( Area 2 )外科示教室 Surgery demo room妇科示教室 Gynecology demo room仓库 Warehouse特殊感染病室 Special infection diseases主任办公室 Director office治疗室 Therapeutic room护士长办公室 Head nurse office医生办公室 Doctor office护士站 Nurse station(三病区)儿科Pediatrics Dept (Area 3)电脑中心 Computer center更衣室 Change room儿科教研室 Pediatrics teaching & research section婴儿洗澡间 Infant bathroom新生婴儿监护室 Neonatus wardship新生婴儿室 Neonatus room重症室 ICU诊疗室 Consulting room(四病区)产科Obstetrical Dept (Area 4)机房 Machine room婴儿抚触中心 Infant-stroking center(五病区)产房 Obstetrical Ward (Area 5)分娩室 Delivery room隔离分娩室 Isolation delivery room陪伴分娩室(一)Delivery room with companion (1)陪伴分娩室(二)Delivery room with companion (2)护士值班室 Nurse on duty医生值班室 Doctor on duty单床间 Single-bed room(六病区)妇科 Gynecology ( Area 6)妇科教研室 Gynecology teaching and research section换药室 Dressing room(七病区)骨科 Orthopedics Dept ( Area 7)(八病区)普外(肝、胆、胰、肛肠)科General Surgical Dept (Liver, Gallbladder, Pancreas, Anorectum (Area 8) 外科教研室 Surgery teaching & research section(九病区)心胸(肿瘤)外科Cardiothoracic Surgery (Tumor) ( Area 9)(十病区)普外(泌尿)科General Surgical Dept (Urinary system) (Area 10)(十一病区)耳鼻咽喉科、眼科、口腔科 ( Area 11)E.N.T. Dept, Ophthalmology Dept, Stomatology Dept眼科暗房 Ophthalmological dark room(十二病区)神经外科Surgical Dept of Neurology (Area 12)麻醉科 Anesthesiology dept示教室 Demo room麻醉医生办公室 Office of anesthesia doctor医生休息室 Doctor rest room女更衣室 Change room (F)男更衣室 Change room (M)有菌手术室 Non aseptic operating theatre手术取材室 Operation material room麻醉器械储藏室 Storeroom of anesthesia instrument非限制区 Unrestricted area半限制区 Semi-restricted area换鞋处 Shoe-changing配电室 Distribution room手术室 Operating theatre石膏房 Gypsum room手术准备室 Operation preparation清洗间 Cleaning room麻醉准备室 Anesthesia preparation麻醉器械室 Anesthesia instrument room限制区 Restricted area精密仪器室 Precision instrument room无菌室 Asepsis room护士登记室 Nurse registration room复苏室 Anabiosis room麻醉清洗消毒室 Anesthesia cleaning and sterilizing room等候室 Waiting room存放间 Storage room后勤楼楼层分布 Layout of Logistic Building病案统计室 Medical record statistics room图书室 Library后勤服务管理中心 Logistic service and management center设备科 Equipment section工程维修部 Engineering maintenance dept基建科 Capital construction section供应服务部 Supply service dept实习生值班室(1)Probationer night shift room (1)门诊楼楼层总索引 Layout of Outpatient Building本层科室分布 Layout of sections开水间 Boiled water检验科Laboratory section抽血化验 Blood test门诊药房 Clinic dispensary大小便、白带化验 Test of stool, urine, leukorrhea药房 Dispensary体液实验室 Humoral lab放射影像科 Radio & Image dept放射科登记处 X-ray registration放射科X-ray dept摄片 2 (X-ray 2)挂号收费 Registration charging内科(二)Internal medicine dept ( 2 )门诊办公室 Outpatient office老干部门诊 Veteran carder clinic老年专科 Special section of geriatric diseases糖尿病专科 Diabets special section内科专家门诊1 Expert clinic of internal medicine ( 1 )专家门诊 Expert clinic专科门诊 Clinic of special section高血压专科 Hypertension special sectionC T 室 CT room换药室 Dressing room肛肠科 Anorectum section肝胆专科专家门诊 Expert clinic of liver and gallbladder section 骨科 Orthopedics dept腰腿痛专科 Lumbago & Skelalgia special section脑外科Cerebral surgery疼痛专科 Special section of pains普外科 General surgical dept皮肤科 Dermatology dept性病专科 Special section of VD儿科专家门诊 Expert clinic of pediatrics儿科Pediatrics dept中药房 TCM dispensary耳鼻咽喉专家门诊 Expert clinic of E.N.T耳鼻咽喉科 E.N.T. dept中医科 TCM dept眼科检查室(眼电生理) Ophthalmology check room (EOG)眼科专家门诊 Ophthalmologic expert clinic煎药室 Herb decocting room眼科治疗室 Therapeutic room of ophthalmology眼科检查室(眼压验光视野)Examination room of ophthalmology (intraocular tension, optometry, visual field) 声阻抗室 Acoustic impedance room电测听室 Electrometric hearing test助听器选配室 Hearing aid selection眼科诊室(常规诊室) Ophthalmology clinic (Routine clinic)宣教室 Publicizing and education胸外肿瘤专科 Special section of thoracic tumor皮肤性病科专家门诊 Expert clinic of dermatosis and VD人流室 Induced Abortion Room介入门诊 Intervention clinic妇产科专家门诊 Expert clinic of gynecology & obstetrics高危妊娠门诊 High-danger pregnancy clinic妇产科 Gynecology & obstetrics dept仓库 Warehouse心室晚电位 Ventricle late potential动态血压 Dynamic blood pressure动态心电图室 Dynamic ECG心向量 Vectorcardiogram心电图室 ECG room心电图科ECG section超声科 Ultrasonographic section彩色B超 Color B-Ultrasonography理疗推拿科 Physical therapy & manipulation section儿科示教室 Demo room of pediatrics盆腔炎治疗室 Therapeutic room of PID儿童生长发育门诊 Children growth clinic急诊B超 Emergency B-Ultrasonography胃镜肠镜预约窗口 Reservation of gastroscope and enteroscope examination脑电图 Electroemcephalogram (缩写EEG)脑地形图 Emcepholo topography红外线乳腺诊断室Infrared light diagnosis of glandula mammaria 颅脑超声 Craniocerebral Ultrasonographic examination消化科 Digestion section心理测验室 Psychological test room专家门诊 Expert clinic心理咨询科 Psychological consult section中西医结合 Combination of TCM and Western medicine病理科 Pathologic section细胞学室 Cytology room技术室 Technical room 免疫组化室 Immunohistochemistry room档案室 Archives room巨检室 Gross examination room诊断室 Diagnosis room口腔科 Stomatology dept胃镜肠镜检查室Gastroscope and enteroscope examination康复科 Rehabilitation section碎石科 Lithotriptic section输液室 Infusion room化液室 Infusion preparation泌尿外科 Urologic surgery dept肌注皮试 Intracutaneous test of intramuscular injection小儿输液室 Children's infusion room成人输液室 Adults' infusion room针灸推拿 Acupuncture & manipulation生活皮肤美容 Skin beauty腰突症 Protrasion of the lumbar intervertebral disci保健按摩 Healthcare massage针炙减肥 Acupuncture weight-reducing医保办 Medical insurance office放免实验室 Radioimmunoassay room防保科 Prophylactic section院感科 Section of inner infection prevention医学美容 Medical cosmetology微生物实验室 Microbioloy Laboratory room检验医学中心 Clinical laboratory medicine centerHIV实验室 HIV Laboratory room血液学实验室 Haematology Laboratory room主任办公室 The office director免疫学实验室 Lmmunology Laboratory room生物化学实验室 Biochemistry Laboratory room档案库房 Archives storeroom信息科 Information section综合档案室 Comprehensive archives room临床系办公室 Clinic dept office文印室 typing and printing room护理部 Nursing department科教科 Scientific education section院办公室 Hospital office书记室 Secretary office人事科 Personnel section院长室 President office副院长室 Vice president office会议室 Meeting room医务科 Section of medical affairs保安部 Security dept顾问室 Consultant office医疗服务质量监控办公室 Medical service supervision office教室 Class room出纳室 Paybox会计室 Accounting house核算办 Accounting office工会 Trade union医疗纠纷接侍室 Reception of medical disputes财务科长室 Finance section chief外科病房楼楼层总索引 Layout of Inpatient Building of Internal Medicine Dept 发热呼吸道门诊 Fever and Respiratory tract clinic体检中心 Physical examination center跟车医师 Ambulance doctor肝炎门诊 Hepatitis clinic值班室(内科) Night shift room (Dept of internal medicine)值班室(外科)Night shift room (Surgical dept)急诊外科 Emergency surgical dept急诊内科 Emergency internal medicine dept值班室(驾驶员) Night shift room (Driver)急诊输液室 Emergency infusion room肠道门诊 Intestinal tract clinic急诊分诊台 Guide to emergency急诊儿科 Emergency pediatrics污物间 Feculence room清创室 Trauma cleaning room输液台 Infusion table急诊挂号收费 Emergency registration charging肠道门诊观察室 Observation ward of intestinal tract clinic急诊指挥中心 Emergency command center夜间药房 Night dispensary主任办公室 Director office监护室 ICU治疗室 Therapeutic room护士办公室 Nurse office观察室 2 Observation ward 2抢救室 Salvaging room观察室 1 Observation ward 1肝炎门诊观察室 Observation ward of Hepatitis clinic干部病房 Cardre Ward心内科 Cardiac internal medicine dept医生办公室 Doctor office诊疗室 Consulting room心血管 Cardiovascular (怎么没有科或室?)呼吸内科 Respiration internal medicine心脏介入中心 Cardio intervention center内分泌内科 Incretion internal medicine血液 Blood (怎么没有科或室?)消化 Digestion (怎么没有科或室?)肾内科 Kidney internal medicine血液层流病房 Aseptic ward介入治疗中心 Intervention therapy center水处理间 Water treatment room手术室 Operating theatre准备室 Preparation room仓库更衣室 Warehouse change room病人更衣室 Patient change room家属接待室 Reception room of patients' relative内科示教室 Demo room of internal medicine操作室 Operating theatre透析室( 1) Dialysis room (1)透析室 (2) Dialysis room (2)药剂科 Medicament Section腰突症专科 Special section of protrasion of the lumbar intervertebral disci 保健按摩专科 Special section of healthcare massage针灸推拿专科 Special section of acupuncture and manipulation老年病专科 Special section of geriatric diseases针灸(中医)减肥专科 Special section of acupuncture weight-reducing (TCM) 生活皮肤护理美容室 Skin care and cosmetology心电图检查室 ECG examination脑电图检查室 EEG examination脑地形图检查室 Encephalo topography examination颅脑超声检查室 Craniocerebral Ultrasonographic examination红外线检查室 Infrared ray examination精神、心理咨询科 Mental and psychological consultation彩色B超检查室Color B- Ultrasonographic examination肝病专家门诊 Expert clinic of hepatitis diseases中西医结合专科 Special section in combination of TCM and western medicine 理疗推拿专科 Special section of physical therapy & manipulation皮肤、性病科 Skin and VD section肝胆外科专家门诊 Expert clinic of liver and gallbladder surgery放射介入治疗专科 Special section of X-ray intervention therapy高血压专科 Hypertension special section碎石治疗中心 Lithotriptic therapy center肾病专家门诊 Expert clinic of kidney diseases糖尿病专科 Diabetes special section康复、理疗科 Rehabilitation and physical therapy section医学美容专科 Special section of medical cosmetology医学影像中心 Medical image center放射介入治疗室 X-ray intervention therapeutic room心血管专科急诊 Cardiovascular emergency肝炎门诊 Hepatitis clinic肌电图检查室 Electromyogram examination呼吸道感染门诊 Respiratory tract infection clinic血透室 Blood dialysis胫镜中心 Anticnemion endoscope center中内科 TCM internal medicine西内科 Western internal medicine乳房外科 Breast surgery手外科 Hand surgery骨伤科 Bone injuries中医妇科 TCM gynecology dept.中西药库 Drug storeroom血库 Blood bank骨髓室 Marrow room留观室 Observation room临床药学室 Clinical pharmacy room社区卫生服务工作办公室 Community Health Service Office信息资料室 Information Archives计划生育技术指导室 Family Planning Technique Consultation Office全科门诊 General Clinic肿瘤科 Tumor dept母婴健康中心 Mother & Baby health center婴儿游泳抚触 Baby swimming-stroking生活用品代办处 Service for daily-use articles待产室 Delivery waiting room配奶间 Milk preparation room驾驶班 Driver team住院部药房 Inpatient dispensary医疗质量管理科 Medical Quality Management Department病理贮片室 Pathological Section Storeroom颈肩腰腿痛专科 Department for Neck, Shoulder, Waist and Leg Pains 儿童活动室 Children's Playing Room电透室 TV Examination Room谈话间 Conversation Room衣帽发放处Coats and Caps Issuing Office器械打包间 Medical Devices Packing Room小孩洗涤室Children’s Washing Room样品接收 Sample Receipt结核菌 Tubercle Bacillus发放厅 Issuing Hall敷料打包间 Dressing-Packing Room污染区 Polluted Area灭菌区 Sterilized Area切洗室 Cutting and Washing Room人工肝室 Artificial Liver Room消控中心 Control Center for Fire Prevention冷冻机房 Freezing Machine Room物流传输机房 Logistical Transmission Machine Room职工自行车库 Employees' Bicycle Storeroom高低配电室 High/Low Voltage Switchouse服务台 Information Desk导医导诊 A Guide to Clinic方便门诊 Simple Clinic健康宣教 Health Education便民服务 Service for the Public取报告单 Examination Report预约审批 Appointment Approval行政后勤区 Administrative Logistic Area预防保健区 Prevention and Healthcare Area医疗康复区 Medical Rehabilitation Area祝您健康 May you a good health后勤保障部 Logistics Guarantee Dept社区卫生服务科 Community Health Service Section全科(24小时门诊)General Clinic (Around the Clock)高电位治疗室 High Potential Therapeutic Room健康教育室 Health Education Room探视制度 Visit Rules挂号须知 Notes for Registration农村合作医疗住院报销窗口Reimbursement for Inpatients of Rural Cooperative Medical Service医保投诉咨询接待室Complaint & Consultation of Medical Insurance腰腿疼痛科 Lumbago and Skelalgia Clinic心理咨询室Psychological Consultation高危门诊 Hazard-Disease Clinic严禁胎儿性别鉴定Fetus sex identifying strictly prohibited卡介苗专室 BCG Vaccine Room合作医疗门诊报销窗口Reimbursement for outpatients of cooperative medical service 医务人员通道Passage for Medical Personnel小儿体检 Infant Physical Examination电透析Electrodialyzing Room电透照镜检查Electrodiaphanoscopy中草药配方 Prescription of Chinese herb medicine西药、中成药配方 Prescription of Western medicine and Chinese patent drugs麻醉药品专用窗口 Special window for anaesthetic药事咨询窗口 Consultation of medicine administration老、弱、病重专区 Special area for the old and weaker, and severely sick persons. 请保持室内清洁 Keep Clean病理贮片室 Pathologic film store room细胞室 Cell Puncture Room牵引室 Traction Room腰、腿、疼痛科Lumbago, Skelalgia and Pains Clinic配餐室 Assorted Meal Preparation陪客休息室 Rest Room for Guests医疗固体处置室 Medical Solid Waste Disposal麻醉恢复室Anaesthesia Recovery Room材料室Material Room引产清宫室Induced Labor Room大厅 Lobby卫事中心 Patient-aid center小卖部 Buffet出院病人领取费用清单 List of expenses for discharged patients普通病人出院结帐 Check-out for common discharged patients住院登记收费 Check-in for inpatients医保社保出院结帐 Check-out for patients with medical / social insurance病区药房 Ward dispensary输血科 Transfusion section急诊化验 Emergency lab急诊手术室 Emergency operating theatre门诊手术室 Clinic operating theatre出入院病人接待处 Reception of inpatients(二病区)重症监护 ICU ( Area 2 )外科示教室 Surgery demo room妇科示教室 Gynecology demo room仓库 Warehouse特殊感染病室 Special infection diseases主任办公室 Director office治疗室 Therapeutic room护士长办公室 Head nurse office医生办公室 Doctor office护士站 Nurse station(三病区)儿科Pediatrics Dept (Area 3)电脑中心 Computer center更衣室 Change room儿科教研室 Pediatrics teaching & research section婴儿洗澡间 Infant bathroom新生婴儿监护室 Neonatus wardship新生婴儿室 Neonatus room重症室 ICU诊疗室 Consulting room(四病区)产科Obstetrical Dept (Area 4)机房 Machine room婴儿抚触中心 Infant-stroking center(五病区)产房 Obstetrical Ward (Area 5)分娩室 Delivery room隔离分娩室 Isolation delivery room陪伴分娩室(一)Delivery room with companion (1)陪伴分娩室(二)Delivery room with companion (2)护士值班室 Nurse on duty医生值班室 Doctor on duty单床间 Single-bed room(六病区)妇科 Gynecology ( Area 6)妇科教研室 Gynecology teaching and research section换药室 Dressing room(七病区)骨科 Orthopedics Dept ( Area 7)(八病区)普外(肝、胆、胰、肛肠)科General Surgical Dept (Liver, Gallbladder, Pancreas, Anorectum (Area 8)外科教研室 Surgery teaching & research section(九病区)心胸(肿瘤)外科Cardiothoracic Surgery (Tumor) ( Area 9)(十病区)普外(泌尿)科General Surgical Dept (Urinary system) (Area 10)(十一病区)耳鼻咽喉科、眼科、口腔科 (Area 11)E.N.T. Dept, Ophthalmology Dept, Stomatology Dept眼科暗房 Ophthalmological dark room(十二病区)神经外科Surgical Dept of Neurology (Area 12) 麻醉科 Anesthesiology dept示教室 Demo room麻醉医生办公室 Office of anesthesia doctor医生休息室 Doctor rest room女更衣室 Change room (F)男更衣室 Change room (M)有菌手术室 Non aseptic operating theatre手术取材室 Operation material room麻醉器械储藏室 Storeroom of anesthesia instrument非限制区 Unrestricted area半限制区 Semi-restricted area换鞋处 Shoe-changing配电室 Distribution room手术室 Operating theatre石膏房 Gypsum room手术准备室 Operation preparation清洗间 Cleaning room麻醉准备室 Anesthesia preparation麻醉器械室 Anesthesia instrument room限制区 Restricted area精密仪器室 Precision instrument room无菌室 Asepsis room护士登记室 Nurse registration room复苏室 Anabiosis room麻醉清洗消毒室 Anesthesia cleaning and sterilizing room 等候室 Waiting room存放间 Storage room后勤楼楼层分布 Layout of Logistic Building病案统计室 Medical record statistics room图书室 Library后勤服务管理中心 Logistic service and management center 设备科 Equipment section工程维修部 Engineering maintenance dept基建科 Capital construction section供应服务部 Supply service dept实习生值班室(1)Probationer night shift room (1)门诊楼楼层总索引 Layout of Outpatient Building本层科室分布 Layout of sections开水间 Boiled water检验科Laboratory section抽血化验 Blood test门诊药房 Clinic dispensary大小便、白带化验 Test of stool, urine, leukorrhea药房 Dispensary体液实验室 Humoral lab放射影像科 Radio & Image dept放射科登记处 X-ray registration放射科X-ray dept摄片 2 (X-ray 2)挂号收费 Registration charging内科(二)Internal medicine dept ( 2 )门诊办公室 Outpatient office老干部门诊 Veteran carder clinic老年专科 Special section of geriatric diseases糖尿病专科 Diabets special section内科专家门诊1 Expert clinic of internal medicine ( 1 )专家门诊 Expert clinic专科门诊 Clinic of special section高血压专科 Hypertension special sectionC T 室 CT room换药室 Dressing room肛肠科 Anorectum section肝胆专科专家门诊 Expert clinic of liver and gallbladder section骨科 Orthopedics dept腰腿痛专科 Lumbago & Skelalgia special section脑外科Cerebral surgery疼痛专科 Special section of pains普外科 General surgical dept皮肤科 Dermatology dept性病专科 Special section of VD儿科专家门诊 Expert clinic of pediatrics儿科Pediatrics dept中药房 TCM dispensary耳鼻咽喉专家门诊 Expert clinic of E.N.T耳鼻咽喉科 E.N.T. dept中医科 TCM dept眼科检查室(眼电生理) Ophthalmology check room (EOG)眼科专家门诊 Ophthalmologic expert clinic煎药室 Herb decocting room眼科治疗室 Therapeutic room of ophthalmology眼科检查室(眼压验光视野)Examination room of ophthalmology (intraocular tension, optometry, visual field)声阻抗室 Acoustic impedance room电测听室 Electrometric hearing test助听器选配室 Hearing aid selection眼科诊室(常规诊室) Ophthalmology clinic (Routine clinic)宣教室 Publicizing and education胸外肿瘤专科 Special section of thoracic tumor皮肤性病科专家门诊 Expert clinic of dermatosis and VD人流室 Induced Abortion Room介入门诊 Intervention clinic妇产科专家门诊 Expert clinic of gynecology & obstetrics高危妊娠门诊 High-danger pregnancy clinic妇产科 Gynecology & obstetrics dept仓库 Warehouse心室晚电位 Ventricle late potential动态血压 Dynamic blood pressure动态心电图室 Dynamic ECG心向量 Vectorcardiogram心电图室 ECG room心电图科ECG section超声科 Ultrasonographic section彩色B超 Color B-Ultrasonography理疗推拿科 Physical therapy & manipulation section儿科示教室 Demo room of pediatrics盆腔炎治疗室 Therapeutic room of PID儿童生长发育门诊 Children growth clinic急诊B超 Emergency B-Ultrasonography胃镜肠镜预约窗口 Reservation of gastroscope and enteroscope examination 脑电图 Electroemcephalogram (缩写EEG)脑地形图 Emcepholo topography红外线乳腺诊断室Infrared light diagnosis of glandula mammaria颅脑超声 Craniocerebral Ultrasonographic examination消化科 Digestion section心理测验室 Psychological test room专家门诊 Expert clinic心理咨询科 Psychological consult section中西医结合 Combination of TCM and Western medicine病理科 Pathologic section细胞学室 Cytology room技术室 Technical room免疫组化室 Immunohistochemistry room档案室 Archives room巨检室 Gross examination room诊断室 Diagnosis room口腔科 Stomatology dept胃镜肠镜检查室Gastroscope and enteroscope examination康复科 Rehabilitation section碎石科 Lithotriptic section输液室 Infusion room化液室 Infusion preparation泌尿外科 Urologic surgery dept肌注皮试 Intracutaneous test of intramuscular injection 小儿输液室 Children's infusion room成人输液室 Adults' infusion room针灸推拿 Acupuncture & manipulation生活皮肤美容 Skin beauty腰突症 Protrasion of the lumbar intervertebral disci保健按摩 Healthcare massage针炙减肥 Acupuncture weight-reducing医保办 Medical insurance office放免实验室 Radioimmunoassay room防保科 Prophylactic section院感科 Section of inner infection prevention医学美容 Medical cosmetology微生物实验室 Microbioloy Laboratory room检验医学中心 Clinical laboratory medicine centerHIV实验室 HIV Laboratory room血液学实验室 Haematology Laboratory room主任办公室 The office director免疫学实验室 Lmmunology Laboratory room生物化学实验室 Biochemistry Laboratory room档案库房 Archives storeroom信息科 Information section综合档案室 Comprehensive archives room临床系办公室 Clinic dept office文印室 typing and printing room护理部 Nursing department科教科 Scientific education section院办公室 Hospital office书记室 Secretary office人事科 Personnel section院长室 President office副院长室 Vice president office会议室 Meeting room医务科 Section of medical affairs保安部 Security dept顾问室 Consultant office医疗服务质量监控办公室 Medical service supervision office 教室 Class room出纳室 Paybox会计室 Accounting house行风办 Trade Service Normalization office核算办 Accounting office工会 Trade union医疗纠纷接侍室 Reception of medical disputes财务科长室 Finance section chief外科病房楼楼层总索引 Layout of Inpatient Building of Internal Medicine Dept 发热呼吸道门诊 Fever and Respiratory tract clinic体检中心 Physical examination center跟车医师 Ambulance doctor肝炎门诊 Hepatitis clinic值班室(内科) Night shift room (Dept of internal medicine)值班室(外科)Night shift room (Surgical dept)急诊外科 Emergency surgical dept急诊内科 Emergency internal medicine dept值班室(驾驶员) Night shift room (Driver)急诊输液室 Emergency infusion room肠道门诊 Intestinal tract clinic急诊分诊台 Guide to emergency急诊儿科 Emergency pediatrics污物间 Feculence room清创室 Trauma cleaning room输液台 Infusion table急诊挂号收费 Emergency registration charging肠道门诊观察室 Observation ward of intestinal tract clinic急诊指挥中心 Emergency command center夜间药房 Night dispensary主任办公室 Director office监护室 ICU治疗室 Therapeutic room护士办公室 Nurse office观察室 2 Observation ward 2抢救室 Salvaging room观察室 1 Observation ward 1肝炎门诊观察室 Observation ward of Hepatitis clinic干部病房Cardre Ward心内科 Cardiac internal medicine dept医生办公室 Doctor office诊疗室 Consulting room呼吸内科 Respiration internal medicine心脏介入中心 Cardio intervention center内分泌内科 Incretion internal medicine肾内科 Kidney internal medicine血液层流病房 Aseptic ward介入治疗中心 Intervention therapy center水处理间 Water treatment room手术室 Operating theatre准备室 Preparation room仓库更衣室 Warehouse change room病人更衣室 Patient change room家属接待室 Reception room of patients' relative内科示教室 Demo room of internal medicine操作室 Operating theatre透析室( 1) Dialysis room (1)透析室 (2) Dialysis room (2)药剂科 Medicament Section腰突症专科 Special section of protrasion of the lumbar intervertebral disci 保健按摩专科 Special section of healthcare massage针灸推拿专科 Special section of acupuncture and manipulation老年病专科 Special section of geriatric diseases针灸(中医)减肥专科 Special section of acupuncture weight-reducing (TCM) 生活皮肤护理美容室 Skin care and cosmetology心电图检查室 ECG examination脑电图检查室 EEG examination脑地形图检查室 Encephalo topography examination颅脑超声检查室 Craniocerebral Ultrasonographic examination红外线检查室 Infrared ray examination精神、心理咨询科 Mental and psychological consultation彩色B超检查室Color B- Ultrasonographic examination肝病专家门诊 Expert clinic of hepatitis diseases中西医结合专科 Special section in combination of TCM and western medicine 理疗推拿专科 Special section of physical therapy & manipulation皮肤、性病科 Skin and VD section肝胆外科专家门诊 Expert clinic of liver and gallbladder surgery放射介入治疗专科 Special section of X-ray intervention therapy高血压专科 Hypertension special section碎石治疗中心 Lithotriptic therapy center肾病专家门诊 Expert clinic of kidney diseases糖尿病专科 Diabetes special section康复、理疗科 Rehabilitation and physical therapy section医学美容专科 Special section of medical cosmetology医学影像中心 Medical image center放射介入治疗室 X-ray intervention therapeutic room心血管专科急诊 Cardiovascular emergency肝炎门诊 Hepatitis clinic肌电图检查室 Electromyogram examination呼吸道感染门诊 Respiratory tract infection clinic血透室 Blood dialysis胫镜中心 Anticnemion endoscope center中内科 TCM internal medicine西内科 Western internal medicine乳房外科 Breast surgery手外科 Hand surgery骨伤科 Bone injuries中医妇科 TCM gynecology dept.中西药库 Drug storeroom血库 Blood bank骨髓室 Marrow room留观室 Observation room临床药学室 Clinical pharmacy room社区卫生服务工作办公室 Community Health Service Office信息资料室 Information Archives计划生育技术指导室 Family Planning Technique Consultation Office 全科门诊 General Clinic肿瘤科 Tumor dept母婴健康中心 Mother & Baby health center婴儿游泳抚触 Baby swimming-stroking生活用品代办处 Service for daily-use articles待产室 Delivery waiting room配奶间 Milk preparation room驾驶班 Driver team住院部药房 Inpatient dispensary医疗质量管理科 Medical Quality Management Department病理贮片室 Pathological Section Storeroom颈肩腰腿痛专科 Department for Neck, Shoulder, Waist and Leg Pains 儿童活动室 Children's Playing Room电透室 TV Examination Room谈话间 Conversation Room衣帽发放处Coats and Caps Issuing Office器械打包间 Medical Devices Packing Room小孩洗涤室Children’s Washing Room样品接收 Sample Receipt结核菌 Tubercle Bacillus发放厅 Issuing Hall敷料打包间 Dressing-Packing Room污染区 Polluted Area灭菌区 Sterilized Area切洗室 Cutting and Washing Room人工肝室 Artificial Liver Room消控中心 Control Center for Fire Prevention冷冻机房 Freezing Machine Room物流传输机房 Logistical Transmission Machine Room职工自行车库 Employees' Bicycle Storeroom高低配电室 High/Low Voltage Switchouse服务台 Information Desk导医导诊 A Guide to Clinic方便门诊 Simple Clinic健康宣教 Health Education便民服务 Service for the Public取报告单 Examination Report预约审批 Appointment Approval行政后勤区 Administrative Logistic Area预防保健区 Prevention and Healthcare Area医疗康复区 Medical Rehabilitation Area祝您健康 May you a good health后勤保障部 Logistics Guarantee Dept社区卫生服务科 Community Health Service Section全科(24小时门诊)General Clinic (Around the Clock)高电位治疗室 High Potential Therapeutic Room健康教育室 Health Education Room探视制度 Visit Rules挂号须知 Notes for Registration农村合作医疗住院报销窗口Reimbursement for Inpatients of Rural Cooperative Medical Service医保投诉咨询接待室Complaint & Consultation of Medical Insurance腰腿疼痛科 Lumbago and Skelalgia Clinic心理咨询室Psychological Consultation高危门诊 Hazard-Disease Clinic严禁胎儿性别鉴定Fetus sex identifying strictly prohibited卡介苗专室 BCG Vaccine Room合作医疗门诊报销窗口Reimbursement for outpatients of cooperative medical service 医务人员通道Passage for Medical Personnel小儿体检 Infant Physical Examination电透析Electrodialyzing Room电透照镜检查Electrodiaphanoscopy中草药配方 Prescription of Chinese herb medicine西药、中成药配方 Prescription of Western medicine and Chinese patent drugs麻醉药品专用窗口 Special window for anaesthetic药事咨询窗口 Consultation of medicine administration老、弱、病重专区 Special area for the old and weaker, and severely sick persons. 请保持室内清洁 Keep Clean病理贮片室 Pathologic film store room细胞室 Cell Puncture Room牵引室 Traction Room腰、腿、疼痛科Lumbago, Skelalgia and Pains Clinic 配餐室 Assorted Meal Preparation陪客休息室 Rest Room for Guests医疗固体处置室 Medical Solid Waste Disposal麻醉恢复室Anaesthesia Recovery Room材料室Material Room引产清宫室Induced Labor Room。
日本三田医院体检报告中文

日本的精密体检可谓一炮打响,很多中国人也都是纷纷慕名而去,当然如果日本医院没有一点“真才实学”是不可能在圈子里久负盛名的。
厚朴方舟在日本开设了分公司,就是为了给更多出国看病、出国体检的客户带来方便。
我们提供3种套餐方案可供客户选择,每一种都包括重大疾病的诊断,因为这也是大家出国体检的重点所在,出国体检就是为了防“大病”的。
日本体检可以发现5mm以下癌症早在三十年前,日本就确定了举国防癌的决心和纲领,三十年的举国潜心钻研,造就了世界领先的癌症防治体系,使日本成功成为世界癌症防治最先进的国家。
在日本,大概80%的癌症发现处于早初期,其中80%的人可以得到治愈。
在中国则是相反的,80%以上的癌症确诊发现为癌症中晚期,80%的病人无法治愈。
日本的癌症治愈率达到68%,中国平均治愈率是20%。
日本在癌症诊断、治疗方面,尤其是早期癌症的发现,领跑于世界各国,它保持着发现癌症的世界记录——发现毫米级别以下的早初期癌症。
这种精密防癌检查,可以发现5mm以下的毫米、微米级绝大部分可能的早期癌症或超初期癌症,让癌细胞无处可藏。
而世界水平的癌症检查,可以发现15毫米以上的癌症,而在中国,通过仪器可以发现的,大概是几厘米以上的中晚期癌细胞。
日本除了技术先进还提供精益求精的服务“日本有些体检技术很先进,但是医疗水平高低并不是很重要,我们国家人多,要做到像日本那样,两天才把一个人的体检做完,一次全身ct扫描做4个小时,的确难以实现。
最重要的区别是态度问题,医生用不用心,细节做得到位不到位。
”这是厚朴方舟的一位老会员陈芳(为保证客户隐私,名字均为化名)介绍的,她认为日本人的服务更多体现在细节上,往往能设身处地从顾客需求出发,给人超乎预期的惊喜和被尊重感。
本次体检仅是陈女士“自由行”中的一项,“自由行”方式让他更加深度体验到日本的人文,“精益求精,用心至极”感受无处不在。
当你认为马桶盖不干净时就能找到放在旁边的消毒纸巾。
在酒店前台和楼层当你觉得手不干净时你会突然发现一瓶精致好用的消毒液就摆在你面前。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
体检编号:
Physical Examination No:
体检表
Examination table
XXX医院2015年制
编号/N0
姓
/Surname
名/Given Names 出生日期/Date 性别/Sex 国籍/Nationality 血型/Blood Type 签证地址/Address of issue
一般检查/General Check
身高/Height: 厘米/cm 体重Weight : 千克/kg 脉搏/Pulse rate : 血压BP : 毫米汞柱mmHg 体温Temperature : ℃
内外科/Medicine & Surgery
皮肤、巩膜、淋巴结/Skin ,Sclera ,Lymph Nodes : 头部和颈部/Head & Neck : 胸部和肺部/Chest & Lungs :
心脏/Heart :
腹部/Abdomen :
脊柱和四肢/Spine & Extremities :
神经精神系统/Neuropsychiatric System :
泌尿生殖系统/Genitourinary System :
五官科/E.E.N.T
裸眼视力/Innc.Vision 左/Left : 右/Right: 矫正视力/Corr.Vision 左/Left : 右/Right: 辨色力/Color Sense :
听力/Hearing 左/Left : 右/Right: 眼、耳、鼻、喉/Eyes ,Ears ,Nose ,Throat :
心电图/ECG
胸部X线/Chest X-ray:
实验室检查/Laboratory Tests:
艾滋病病毒抗体/Anti-HIV:
梅毒血清学检测/Syphilis Serology:
乙型肝炎表面抗体/HBsAg:
丙型肝炎抗体/Anti-HCV:
丙氨酸氨基转移酶/ALT(GPT):
血常规/Blood Routine:
白细胞总数/WBC:
红细胞总数/RBC:
血小板总数/PLT:
血红蛋白/HGB:
粉细胞百分比/NEUT%:
淋巴细胞百分比%:
结论/General Comments:
负责医生姓名印章
Name of doctor in charge Official stamp
负责医生签名
Signature of doctor in charge
签发日期
Date of issue。