注射用美罗培南说明书
注射用美罗培南
注射用美罗培南Zhusheyong MeiluopeinanMeropenem for Injection书页号:中国药典2005年版二部—447[修订]本品为美罗培南加适量无水碳酸钠制成的灭菌粉末。
含美罗培南(C17H25N3O5S)应为标示量的90.0%~110.0%。
有关物质取本品适量,加0.1%三乙胺溶液(取三乙胺1.0ml,加水900ml,用磷酸溶液(1→10)调节pH为5.0±0.1,加水稀释至1000ml)制成每1ml中含美罗培南5mg的溶液,作为供试品溶液;精密量取适量,用0.1%三乙胺溶液稀释制成每1ml中含美罗培南25μg的溶液,作为对照溶液。
照美罗培南项下的方法检查,供试品溶液色谱图中如有杂质峰,单个杂质不得大于对照溶液主峰面积(0.5%),各杂质峰面积的和不得大于对照溶液主峰面积的3倍(1.5%)。
含量均匀度以含量测定项下测得的每瓶含量计算,应符合规定(附录Ⅹ E)。
无菌取本品规定量,用0.1%蛋白胨溶液充分溶解并稀释成约20mg/ml的溶液,作为供试液。
采用薄膜过滤法(每膜过滤量不大于3g供试品),用0.1%无菌蛋白胨溶液冲洗,冲洗量500ml/膜,分5次冲洗(每次100ml),细菌采用含青霉素酶(大于100万单位/100ml)的硫乙醇酸盐流体培养基培养。
金黄色葡萄球菌作为阳性对照。
依法检查(附录Ⅺ H),应符合规定。
【含量测定】本品10瓶,分别加0.1%三乙胺溶液(取三乙胺1.0ml,加水900ml,用磷酸溶液(1→10)调节pH为5.0±0.1,加水稀释至1000ml)溶解并定量稀释制成每1ml中含美罗培南0.5mg的溶液,作为供试品溶液。
照美罗培南项下的方法测定,即得并求出10瓶的平均含量。
[增订]【鉴别】(2)①薄层色谱供试品溶液:取本品1瓶,加水5ml振摇使溶解,再加75%的乙醇制成每1ml约含美罗培南10mg的溶液。
对照品溶液:取美罗培南对照品适量,先加少量水使溶解,再加75%的乙醇制成每1ml约含美罗培南10mg的溶液。
美平

美平/注射用美罗培南(日本住友制药株式会社)适应症肺炎包括院内获得性肺炎、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
【成份】美罗培南【适应症】肺炎包括院内获得性肺炎、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
【规格】0.25g × 1【用法用量】成人:给药剂量和时间间隔应根据感染类型、严重程度及病人的具体情况而定。
推荐日剂量如下:1、肺炎、尿路感染、妇科感染(如子宫内膜炎)、皮肤或软组织感染,每8小时给药一次,每次500mg,静脉滴注。
2、院内获得性肺炎、腹膜炎、中性粒细胞减少患者的合并感染、败血症的治疗,每8小时给药一次,每次1g,静脉滴注。
3、脑膜炎患者,推荐每8小时给药一次,每次2g。
儿童:年龄3个月-12岁的儿童,根据感染类型的严重程度、致病菌敏感性和病人的具体情况,每8小时规定按剂量10-20mg/kg给药,体重超过50kg的儿童,按成人剂量给药。
脑膜炎儿童患者的治疗,剂量按每8小时40mg/kg 给药。
目前尚无儿童肾功能不全的使用经验。
婴幼儿:年龄3个月以下婴幼儿,本品疗效和耐受性不清楚,因此,年龄在3个月以下的婴幼儿,不推荐使用美罗培南,肝、肾功能异常儿童未使用过美罗培南进行治疗。
4、肾功能不全成人的剂量调整:肌酐清除率51ml/min病人按下面的规定减少剂量。
肌酐清除率(ml/min)剂量(单位剂量500mg、1g、2g)时间间隔26-50 1个单位剂量每12小时10-25 1/2个单位剂量每12小时101/2个单位剂量每24小时·用法:5、美罗培南静脉推注的时间应大于5分钟,静脉滴注时间大于15-30分钟。
美罗培南推注时,应使用无菌注射用水配制(每5ml含水量250mg本品),浓度约50mg/ml。
美罗培南静脉滴注时,可先用注射用水或其它合适的液体配制,再用合适的液体稀释至50-200ml使用。
注射用美罗培南说明书

注射用美罗培南说明书一、药品名称通用名称:注射用美罗培南二、成分本品主要成分为美罗培南。
三、性状本品为白色至微黄色结晶性粉末。
四、适应症1、用于成人和儿童由单一或多种对美罗培南敏感的细菌引起的感染:肺炎(包括院内获得性肺炎)、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
2、经验性治疗中性粒细胞减少患者的发热。
3、用于在耐甲氧西林金黄色葡萄球菌(MRSA)和多重耐药菌感染高发医疗机构中,进行某些手术前的预防用药。
五、规格以美罗培南计,常见规格有 025g、05g、10g 等。
六、用法用量1、成人11 肺炎、尿路感染、妇科感染、皮肤软组织感染:每 8 小时给药一次,每次 05g 10g,静脉滴注。
111 脑膜炎:每 8 小时给药一次,每次 20g,静脉滴注。
112 败血症:每 8 小时给药一次,每次 10g 20g,静脉滴注。
2、儿童21 体重小于 50kg 的儿童,按每次 10 20mg/kg 计算剂量,每 8 小时给药一次。
211 体重超过 50kg 的儿童,用法用量同成人。
七、不良反应1、常见不良反应11 皮疹、瘙痒、红斑等过敏反应。
111 恶心、呕吐、腹泻等胃肠道反应。
112 肝功能异常,如转氨酶升高等。
113 肾功能异常,血肌酐和血尿素氮升高。
2、少见不良反应21 头痛、头晕、失眠等神经系统症状。
211 口腔念珠菌感染。
212 静脉炎。
八、禁忌对美罗培南或其他碳青霉烯类抗生素过敏者禁用。
九、注意事项1、对青霉素类或其他β内酰胺类抗生素过敏者,使用本品时应谨慎。
2、长期使用本品可能导致耐药菌的产生,应严格按照适应证和用法用量使用。
3、肝肾功能不全者应根据情况调整剂量。
4、本品与丙戊酸钠合用时,可能导致丙戊酸钠血药浓度降低,增加癫痫发作的风险。
5、配制好的药液应立即使用,如需存放,应在室温下不超过 8 小时,冷藏条件下不超过 24 小时。
十、孕妇及哺乳期妇女用药1、孕妇11 尚无足够的孕妇使用本品的临床数据,只有在潜在益处大于对胎儿的潜在风险时,方可使用。
注射用美罗培南粉针剂静脉滴注使用配置流程及注意事项1

注射用美罗培南粉针剂静脉滴注使用配置流程及注意事项1注射用美罗培南粉针剂静脉滴注使用配置流程美罗培南粉针在临床应用中,主要是进行静脉滴注(俗称:吊瓶),在实际的使用和操作过程中,我们的配置使用流程如下:一、以0.25克为例:(2支,4支的使用)1、取少量输液液体稀释美罗培南粉针从病人使用的输液瓶或软袋输液中,(一般常用0.9%生理盐水或5%的葡萄糖100毫升、或250毫升)按每只3毫升的剂量,(如:一次使用2支,即可抽取6毫升,一次使用4支就抽取12毫升)抽取原输液分别加入到美罗培南粉针安瓶中进行稀释;2、震荡摇匀稀释的美罗培南粉针将抽取的输液原液分别注入各美罗培南粉针安瓶后,进行稀释溶解,此时溶液会有轻微浑浊,需轻微震荡摇匀;3、稀释的美罗培南药液返注入原输液液体中分别抽取安瓶内稀释溶解的美罗培南液体,返注入到输液瓶或软袋输液中,放置3分钟,输液液体澄明无色。
注:出现浑浊是正常现象原因理由如下:A、同批次的厂检显示,澄清度与颜色的检测标准是≦1号,而我们的检测结果是≦0.5号,符合国家药典标2005版规定;B、同批次上海市的检验报告书中,澄清度与颜色的检测结果:符合国家药典2005版规定)。
C、美罗培南以游离羧酸形式存在,略溶于水,为增加其溶解度,在美罗培南粉针剂制备过程中,加入了20%有碳酸钠,使美罗培南溶解时成盐便于溶解。
美罗培南粉针在安瓶内稀释溶解时,由于溶剂量小,只有部分成盐溶解,尚有部分美罗培南仍以游离的羧酸形式存在,故安瓶内的美罗培南稀释液有轻微浑浊现象,当把安瓶内稀释的美罗培南药液返注入原输液液体中,以游离的羧酸形式存在的美罗培南全部成盐溶解,输液液体澄明无色。
二、以0.5克为例:(1支,2支,4支的使用)1、取少量输液液体稀释美罗培南粉针(一般常使用0.9%生理盐水或5%的葡萄糖100毫升,从病人使用的输液瓶或软袋输液中,或250毫升)按每只5毫升的剂量,(如:一次使用2支,即可抽取10毫升,一次使用4支就抽取20毫升)抽取原液分别加入到美罗培南的粉针瓶中;2、震荡摇匀稀释的美罗培南粉针将抽取的输液原液分别注入各美罗培南粉针安瓶后,进行稀释溶解,此时溶液会有轻微浑浊,需轻微震荡摇匀。
注射用美罗培南需要注意哪些问题
注射用美罗培南需要注意哪些问题注射用美罗培南主要成份为美罗培南,为白色至微黄色粉末状。
适用于成人以及儿童感染性肺炎,尿路肺炎等。
用药时要仔细阅读药品说明书,严格按照说明书用药。
切记不可乱用药品,毕竟是药三分毒。
用药的不恰当严重时可能会造成生命危险。
本药品孕妇及哺乳期妇女不可使用,老人及儿童可根据医嘱调节用量。
药品的用法一定要注意用量以及用法,下面就让我们一起来了解一下注射用美罗培南的注意事项吧!★(一)用法用量 美罗培南静脉推注的时间应大于5分钟,静脉滴注时间大于15~30分钟。
美罗培南推注时,应使用无菌注射用水配制(每5ml含250mg本品),浓度约50mg/ml。
美罗培南可使用下列输液溶解:0.9%氯化钠溶液、5%或者10%葡萄糖溶液、5%葡萄糖溶液(碳酸氢钠浓度0.02%)、0.9%氯化钠溶液和5%葡萄糖溶液、5%葡萄糖溶液(氯化钠浓度0.225%)、5%葡萄糖溶液(氯化钾浓度0.15%)25%或10%甘露醇溶液。
★用量:成人:给药剂量和时间间隔应根据感染类型、严重程度及病人的具体情况而定。
推荐日剂量如下:肺炎、尿路感染、妇科感染(如子宫内膜炎)、皮肤或软组织感染,每8小时给药一次,每次500mg,静脉滴注。
院内获得性肺炎、腹膜炎、中性粒细胞减少患者的合并感染、败血症的治疗,每8小时给药一次,每次1g,静脉滴注。
脑膜炎患者推荐每8小时给药一次,每次2g。
肾功能不全成人的剂量调整:肌酐清除率<51ml/min病人按下面的规定减少剂量。
★(二)不良反应主要不良反应:皮疹、腹泻、软便、恶心、呕吐。
另外实验室检查值主要异常有GOT升高,GPT升高,ALP升高,嗜酸性粒细胞增多。
1.在应用美罗培南的患者中出现的严重不良反应:过敏性休克、急性肾衰等严重肾功能障碍、伴有血便的重症结肠炎如伪膜性结肠炎等、间质性肺炎、PZF综合症、痉挛、意识障碍等中枢神经系统症状、中毒性表皮坏死症(LYELL综合症)、Stevens-Johnson综合症、全血细胞减少,无粒细胞症,白细胞减少,肝功能障碍,黄疸,在同类药品中还有溶血性和血栓静脉炎的报道。
注射用美罗培南(倍能)说明书
注射用美罗培南说明书请仔细阅读说明书并在医师指导下使用【中文名称】注射用美罗培南【产品英文名称】Meropenem for Injection【生产企业】深圳市海滨制药有限公司【功效主治】美罗培南适用于成人和儿童由单一或多种对美罗培南敏感的细菌引起的感染:肺炎(包括院内获得性肺炎)、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
经验性治疗,对成人粒细胞减少症伴发热患者,可单独应用本品或联合抗病毒药或抗真菌药使用。
美罗培南单用或与其它抗微生物制剂联合使用可用于治疗多重感染。
对于中性粒细胞减少或原发性、继发性免疫缺陷的婴儿患者,目前尚无本品的使用经验。
【化学成分】本品主要成份为:美罗培南。
其化学名称为:(-)-(4R,5S,6S)-3-{[(3S,5S)-5-(二甲胺基甲酰基)-3-吡咯烷基]硫}-6-[(1R)-1-羟基乙基]-4-甲基-7-氧代-1-氮杂双环[3,2,0]庚-2-烯-2-羧酸三水合物。
【分子式】C12H25N3O5S·3H2O 【分子量】437.51 【药理作用】美罗培南为人工合成的文谱碳青霉烯类抗生素,通过抑制细菌细胞壁的合成而产生抗菌作用,美罗培南容易穿透大多数革兰氏阳性和阴性细菌的细胞壁,而达到其作用靶点青霉素结合蛋白(PBPs)。
除金属β-内酰胺酶以外,其对大多数β-内酰胺酶(包括由革兰氏阳性菌及阴性菌所产生的青霉素酶和头孢菌素酶)的水解作用具有较强的稳定性。
美罗培南不宜用于治疗对甲氧西林耐药的葡萄球菌感染,有时对其它碳青霉烯类的耐药菌株亦表现出交叉耐药性。
体外试验显示,对一些绿脓杆菌的分离菌株,美罗培南与氨基糖甙类抗生素合用可产生协同作用。
体外试验和临床感染应用中均表明美罗培南对以下大多数微生物有活性:(1)革兰氏阳性需氧菌:肺炎链球菌(不包括青霉素耐药性菌株)、草绿色链球菌。
(2)革兰氏阴性需氧菌:大肠杆菌、流感嗜血杆菌(β-内酰胺酶阳性菌株及β-内酰胺酶阴性菌株)、肺炎克雷伯菌、绿脓假单胞菌、脑膜炎奈瑟菌。
注射用美罗培南儿童用药剂量
注射用美罗培南儿童用药剂量
注射用美罗培南治疗皮肤软组织感染、脑膜炎、败血症等感染性疾病效果非常显著,但是使用本药物出现的不良症状比较多。
使用丙戊酸的病人严禁使用该药物,而且孕妇不宜使用本药物,除非可证实使用该药时对胎儿的影响利大于弊,哺乳期的女性也不推荐使用该药物。
那么儿童使用美罗培南的用药剂量是多少呢?
注射用美罗培南儿童用药剂量
儿童:年龄3个月~12岁的儿童,根据感染类型的严重程度、致病菌敏感性和病人的具体情况,每8小时按剂量10~20mg/kg给药,体重超过5 0kg的儿童,按成人剂量给药。
脑膜儿童患者的治疗,剂量按每8小时4 0mg/kg给药。
目前尚无儿童肾功能不全的使用经验。
婴幼儿:年龄3个月以下婴幼儿,本品疗效和耐受性尚不清楚,因此,年龄在3个月以下的婴幼儿,不推荐使用美罗培南,肝、肾功能异常儿童未使用过美罗培南进行治疗。
美罗培南注射液Merrem(Meropenem)使用说明

【药品名称】英文药名: Merrem(Meropenem)中文药名: 美罗培南注射液【药理作用】本品为细菌细胞壁合成抑制剂。
体外比较本品和Imipenem、Cefotaxime(头孢噻肟)及Ceftazidine(头孢他定),发现本品对革兰氏阴性菌抑制作用最强。
它的抗菌谱包括所有肠杆菌科的细菌(99.7%对本品小于4μg/ml浓度药物敏感)、假单胞菌属和不动杆菌属。
对革兰氏阴性菌的作用强度和抗菌谱不及Imipenem,但优于Ceftazidine(头孢他定)。
本品浓度0.5μg/ml时可抑制90%的金黄色葡萄球菌、肺炎双球菌和溶血链球菌等。
本品对厌氧菌的作用强于Metronidazol(甲硝唑)和Clindamycin(氯洁霉素)。
本品对肠杆菌科特别有效,MIC90均小于或等于0.125μg/ml,抗普通变形菌、奇异变形菌和摩氏摩根菌的MIC90,本品为0.125μg/ml,而Imipenem 为4μg/ml。
本品容易透入大肠杆菌和绿脓杆菌,对大肠杆菌的渗透性更强。
【适应症】用于治疗下呼吸道、尿路、腹内、妇科和皮肤感染以及细菌性脑膜炎等。
【包装规格】·1 gm(克) 1支x 30ml·1 gm(克) 5 (支)·500mg(毫克) 5 (支)【用法用量】应用本品原则上不可超过2周。
最初三日给药后观察是否有效,以决定是否继续给药或更换其它药物。
通常成人1日0.5~1.0g,分2~3次,静脉点滴,每次30分钟以上。
可按年龄、病情增减剂量。
重症,顽固性感染可增至1日2g。
使用时用生理盐水或5%葡萄糖注射液溶解,每0.5g本品稀释到100ml以上,不用注射用水稀释。
谨遵医嘱!【如何购买】好医友美国药房提供专科药物、处方药物、非处方药物、药物配置、药物注射以及各类非住院患者的药物分发、咨询、配送等各项服务。
如今国内患者可以依托科技,实现远程的病历交互,由美国医生根据患者病情开具电子处方,以正规渠道在美国药房购买到处方药。
注射用美罗培南说明书-倍能

注射用美罗培南说明书【药品名称】通用名:注射用美罗培南英文名:Meropenem for Injection汉语拼音:Zhusheyong Meiluopeinan商品名:倍能【成份】本品主要成份为美罗培南。
辅料为无水碳酸钠。
化学名称:(-)-(4R,5S,6S)-3{[(3S,5S)-5-(二甲胺基甲酰基)-3-吡咯烷基]硫}-6-[(1R)-1-羟基乙基]-4-甲基-7-氧代-1-氮杂双环[3.2.0]庚-2-烯-2-羧酸三水合物。
化学结构式:分子式:C17H25N3O5S·3H2O分子量:437.51Cas No:96036-03-2【性状】本品为白色至微黄色粉末。
【适应症】美罗培南适用于成人和儿童由单一或多种对美罗培南敏感的细菌引起的感染:肺炎(包括院内获行性肺炎)、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
经验性治疗,对成人粒细胞减少症伴发热患者,可单独应用本品或联合抗病毒药或抗真菌药使用。
美罗培南单用或与其它抗微生物制剂联合使用可用于治疗多重感染。
对于中性粒细胞减少或原发性、继发性免疫缺陷的婴儿患者,目前尚无本品的使用经验。
【规格】按C17H25N3O5S计0.5g。
【用法与用量】用法:美罗培南静脉推注的时间应大于5分钟,静脉滴注时间大于15~30分钟。
美罗培南推注时,应使用无菌注射用水配制(每5ml含250mg本品),浓度约50mg/ml。
美罗培南可使用下列输液溶解:0.9%氯化钠溶液、5%或者10%葡萄糖溶液、5%葡萄糖溶液(碳酸氢钠浓度0.02%)、0.9%氯化钠溶液和5%葡萄糖溶液、5%葡萄糖溶液(氯化钠浓度0.225%)、5%葡萄糖溶液(氯化钾浓度0.15%)25%或10%甘露醇溶液。
用量:成人:给药剂量和时间间隔应根据感染类型、严重程度及病人的具体情况而定。
推荐日剂量如下:肺炎、尿路感染、妇科感染(如子宫内膜炎)、皮肤或软组轵感染,每8小时给药一次,每次500mg,静脉滴注。
注射用美罗培南需要注意哪些问题
注射用美罗培南需要注意哪些问题关于《注射用美罗培南需要注意哪些问题》,是我们特意为大家整理的,希望对大家有所帮助。
注射用美罗培南关键成分为美罗培南,为乳白色至微淡黄色粉状。
适用成年人及其少年儿童感染性肺炎,尿道肺炎等。
服药时要认真阅读药品标签,严苛依照使用说明服药。
谨记不能滥用药物,终究是药三分毒。
服药的不适当比较严重时可能会导致生命威胁。
本药物孕妇及哺乳期间不能应用,老年人及少年儿童可依据医生叮嘱调整使用量。
药物的使用方法一定要留意使用量及其使用方法,下边就要我们一起来了解一下注射用美罗培南的常见问题吧!(一)使用方法使用量美罗培南静脉推注的時间应超过5分鐘,静脉滴注時间超过15~30分钟。
美罗培南推注时,应应用无菌检测注射自来水配置(每5ml含250Mg本产品),浓度值约50Mg/ml。
美罗培南可应用以下打点滴融解:0.9%氯化钠溶液、5%或是10%葡萄糖溶液、5%葡萄糖溶液(碳酸氢纳浓度值0.02%)、0.9%氯化钠溶液和5%葡萄糖溶液、5%葡萄糖溶液(氯化钠浓度0.225%)、5%葡萄糖溶液(氯化钾浓度值0.15%)25%或10%甘露醇水溶液。
使用量:成年人:给药使用量和间隔时间应依据感染种类、比较严重水平及患者的详细情况而定。
强烈推荐日使用量以下:肺炎、尿道感染、妇科感染(如子宫内膜炎)、皮肤或软组织感染,每8钟头给药一次,每一次500mg,静脉滴注。
院中得到性肺炎、腹膜炎、单核细胞降低病人的合拼感染、败血症的医治,每8钟头给药一次,每一次1g,静脉滴注。
脑膜炎病人强烈推荐每8钟头给药一次,每一次2g。
肾功能不全成年人的使用量调节:肌酐清除率<51ml/min患者按下边的要求降低使用量。
(二)副作用关键副作用:皮疹、腹泻、软便、恶心想吐、呕吐。
此外实验室检查值关键出现异常有GOT上升,GPT上升,ALP上升,嗜酸性粒细胞增加。
1.在运用美罗培南的病人中出現的比较严重副作用:过敏性休克、急性肾衰等比较严重肾脏功能阻碍、伴随脓血便的危重症结肠炎如伪膜性结肠炎等、间质性肺炎、PZF综合征、筋挛、意识障碍等神经中枢系统病症、中毒副作用外皮坏死症(LYELL综合征)、Stevens-Johnson综合征、全红细胞降低,无粒细胞症,白细胞减少,肝功能检查阻碍,黄疸,在类似药物中也有溶血性和静脉血栓静脉炎的报导。
注射用美罗培南不良反应有哪些
注射用美罗培南不良反应有哪些
注射用美罗培南的主要成分是美罗培南,辅料为无水碳酸钠,为白色
至微黄色粉末,使用时需要配合无菌注射用水进行使用。
本药品主要
应用于抗感染几倍,常见病种有:皮肤软组织感染、脑膜炎、败血症等,不同人群使用美罗培南的方法和用量有着很大的差别,而且使用
丙戊酸的病人禁止使用本药物。
注射用美罗培南用法
美罗培南静脉推注的时间应大于5分钟,静脉滴注时间大于15~30分钟。
美罗培南推注时,应使用无菌注射用水配制(每5ml含250mg本品),
浓度约50mg/ml。
美罗培南可使用下列输液溶解:0.9%氯化钠溶液、5%
或者10%葡萄糖溶液、5%葡萄糖溶液(碳酸氢钠浓度0.02%)、0.9%氯
化钠溶液和5%葡萄糖溶液。
注射用美罗培南用量
成人:给药剂量和时间间隔应根据感染类型,严重程度及病人具体情
况而定。
肺炎、尿路感染、妇科感染(如子宫内膜炎)、皮肤或软组
织感染,每8小时给药一次,每次500mg,静脉滴注。
院内获得性肺炎、腹膜炎、中性粒细胞减少患者的合并感染、败血症的治疗,每8小时给
药一次,每次1g,静脉滴注。
脑膜炎患者,推荐每8小时给药一次,每
次2g。
注射用美罗培南说明书

【不良反应】
调查总例数7925例中,998例(12.6%)出现包括实验室检查值异常在内的 不良反应。主要不良反应为:皮疹41例(0.5%)、腹泻24例(0.3%)、 AST(GOT)升高333例(4.2%)、ALT(GPT)升高377例(4.8%)、 Al-P升高127例(1.6%)等。另外,以儿童为对象的临床研究中,总病例 数755例中,130例(17.2%)出现包括实验室检查值异常在内的不良反应。 主要不良反应为:腹泻16例(2.1%),呕吐8例(1.1%),AST(GOT) 升高23 例(3.1%),ALT(GPT) 升高29例(3.8%),血小板增多18例(2.4%),嗜酸性 粒细胞增多10例(1.3%)等。
分 子 式:C17 H25 N3 O5 S·3H2 O 分 子 量:437.51 辅 料:无水碳酸钠
【性 状】 白色至淡黄白色结晶性粉末。
【适应症】 由单一或多种敏感细菌引起的成人及儿童的下列感染 肺炎及院内获得性肺炎 尿路感染 腹腔内感染 妇科感染(例如子宫内膜炎) 皮肤及软组织感染 脑膜炎 败血症 对于被推断患有感染的伴中性粒细胞减低的发热病人(成人),可用美 平®作为单方经验性治疗或联合应用抗病毒或抗真菌药物治疗。 已经证实,单独应用美平®或联合应用其它抗微生物制剂治疗多重感染 有效。目前,尚缺乏在患有中性粒细胞减低或原发/继发免疫功能缺陷的 儿科患者中应用本药的经验。
(8) 肝功能障碍(0.1~5%)、黄疸(<0.1%) 定期做肝功能检查,密切观察,如有异常现象发生时,应停药并进行适 当处理。
Vabomere药品说明书
.106.World Notes on Antibiotics, 2019, Vol.40, No.2Vabomere 药品说明书黄志伟编译,张菁**校审 (复旦大学附属华山医院抗生素研究所,上海20040)收稿日期:2018-12-15基金项目:科技部“重大新药创制”科技重大专项资助(2017ZX09304005)。
作者简介:黄志伟,研究生,主要研究方向为药物I 期临床试验。
*通信作者:张菁,教授,主要研究方向为抗菌药物临床药理学研究。
摘要:受助于美国FDA 优先审评资格,美国制药公司The Medicines Company 的Vabomere 注射剂(美罗培南+Vaborbactam )进入临床开发不到8年时间,就于2017年8月29日,被批准用于成人复杂性尿路感染(complicated urinary tract infections, cUTI )的治疗,为严重细菌感染患者提供了一种额外的治疗方案。
为方便国内学者了解Vabomere 的特性,特对其说明书进行翻译,包括适 应证、用法用量、不良反应、药物相互作用、药理毒理、微生物学和临床研究等。
关键词:Vabomere ;复杂性尿路感染;不良反应;药理毒理;微生物学;临床研究中图分类号:R978.1 文献标识码:A 文章编号:1001-8751(2019)02-0106-092017年8月29H ,美国食品和药品监督管理 局批准了美国制药公司The Medicines Company 的Vabomere 注射剂1(美罗培南+Vaborbactam )用于成人复杂性尿路感染的治疗,Vabomere 是由合成的青霉烯类抗菌药物美罗培南和一种环硼酸卩-内酰胺酶抑制剂Vaborbactam 组合成的产品,用于静脉给药。
为方 便国内学者了解Vabomere 的特性,特对其说明书进 行翻译。
1适应证及用途Vabomere 适用于下列敏感菌引起的18岁及以 上患者复杂性尿路感染,包括肾盂肾炎:大肠埃希菌、肺炎克雷伯菌和阴沟肠杆菌。
注射用美罗培南粉针剂静脉滴注使用配置流程及注意事项1
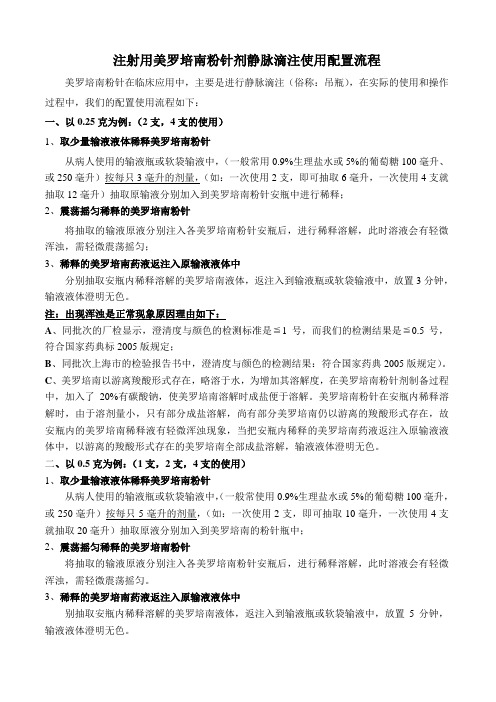
注射用美罗培南粉针剂静脉滴注使用配置流程美罗培南粉针在临床应用中,主要是进行静脉滴注(俗称:吊瓶),在实际的使用和操作过程中,我们的配置使用流程如下:一、以0.25克为例:(2支,4支的使用)1、取少量输液液体稀释美罗培南粉针从病人使用的输液瓶或软袋输液中,(一般常用0.9%生理盐水或5%的葡萄糖100毫升、或250毫升)按每只3毫升的剂量,(如:一次使用2支,即可抽取6毫升,一次使用4支就抽取12毫升)抽取原输液分别加入到美罗培南粉针安瓶中进行稀释;2、震荡摇匀稀释的美罗培南粉针将抽取的输液原液分别注入各美罗培南粉针安瓶后,进行稀释溶解,此时溶液会有轻微浑浊,需轻微震荡摇匀;3、稀释的美罗培南药液返注入原输液液体中分别抽取安瓶内稀释溶解的美罗培南液体,返注入到输液瓶或软袋输液中,放置3分钟,输液液体澄明无色。
注:出现浑浊是正常现象原因理由如下:A、同批次的厂检显示,澄清度与颜色的检测标准是≦1号,而我们的检测结果是≦0.5号,符合国家药典标2005版规定;B、同批次上海市的检验报告书中,澄清度与颜色的检测结果:符合国家药典2005版规定)。
C、美罗培南以游离羧酸形式存在,略溶于水,为增加其溶解度,在美罗培南粉针剂制备过程中,加入了20%有碳酸钠,使美罗培南溶解时成盐便于溶解。
美罗培南粉针在安瓶内稀释溶解时,由于溶剂量小,只有部分成盐溶解,尚有部分美罗培南仍以游离的羧酸形式存在,故安瓶内的美罗培南稀释液有轻微浑浊现象,当把安瓶内稀释的美罗培南药液返注入原输液液体中,以游离的羧酸形式存在的美罗培南全部成盐溶解,输液液体澄明无色。
二、以0.5克为例:(1支,2支,4支的使用)1、取少量输液液体稀释美罗培南粉针从病人使用的输液瓶或软袋输液中,(一般常使用0.9%生理盐水或5%的葡萄糖100毫升,或250毫升)按每只5毫升的剂量,(如:一次使用2支,即可抽取10毫升,一次使用4支就抽取20毫升)抽取原液分别加入到美罗培南的粉针瓶中;2、震荡摇匀稀释的美罗培南粉针将抽取的输液原液分别注入各美罗培南粉针安瓶后,进行稀释溶解,此时溶液会有轻微浑浊,需轻微震荡摇匀。
美罗培南用法
美罗培南用法
美罗培南是一种用于治疗皮肤炎症的外用药物,是一种合成皮肤保护和缓解剂,由美国Mylan公司生产。
美罗培南的主要成分是避孕药服用的同一组成成分:美罗培南醇和美罗培南乙醇,它们都是合成激素。
这种药物可以有效地减轻皮肤炎症,如皮肤中出现的瘙痒、疼痛和红肿等症状。
它还可以预防皮肤上的感染,抑制皮肤上的损伤反应,并有助于加快皮肤的修复和愈合。
美罗培南的使用方法很简单,只需将药物均匀地涂抹在皮肤上,每次使用量不超过1克。
如果是治疗小面积的皮肤炎症,每次可用量约为0.5克,当服用多天后,可以根据皮肤炎症的症状和恢复情况调整用药量。
如果是治疗大面积皮肤炎症,每次可用量约为2-3克,可以每3-4天使用一次,也可以根据皮肤炎症的症状和恢复情况调整用药量和次数。
使用美罗培南时,要尽量避免皮肤的刺激,避免温度过高的地方,以免皮肤受损和药效减弱。
使用该药物时,要避免与眼睛、口腔、膀胱等接触,以防止毒物流入体内引发不良反应。
此外,还要适当保湿皮肤,以免皮肤受损和药效减弱。
美罗培南可以用来治疗许多皮肤炎症,但是有时可能会发生不良反应,例如皮肤过敏、发红和肿胀等,此时应立即停止使用,并向医生求助。
因此,在使用美罗培南时,应当遵守正确的使用方法,以确保治疗的有效性和安全性。
美罗培南国外说明书
MERREM® I.V.(meropenem for injection)FOR INTRAVENOUS USE ONLYTo reduce the development of drug-resistant bacteria and maintain the effectiveness of MERREM® I.V. (meropenem for injection) and other antibacterial drugs, MERREM I.V. should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONMERREM® I.V. (meropenem for injection) is a sterile, pyrogen-free, synthetic, broad-spectrum, carbapenem antibiotic for intravenous administration. It is (4R,5S,6S)-3-[[(3S,5S)-5-(Dimethylcarbamoyl)-3-pyrrolidinyl]thio]-6-[(1R)-1-hydroxyethyl]-4-methyl-7-oxo-1-azabicyclo[3.2.0]hept-2-ene-2-carboxylic acid trihydrate. Its empirical formula is C17H25N3O5S•3H2O with a molecular weight of 437.52. Its structural formula is:MERREM I.V. is a white to pale yellow crystalline powder. The solution varies from colorless to yellow depending on the concentration. The pH of freshly constituted solutions is between 7.3 and 8.3. Meropenem is soluble in 5% monobasic potassium phosphate solution, sparingly soluble in water, very slightly soluble in hydrated ethanol, and practically insoluble in acetone or ether.When constituted as instructed (see DOSAGE AND ADMINISTRATION; PREPARATION OF SOLUTION), each 1 g MERREM I.V. vial will deliver 1 g of meropenem and 90.2 mg of sodium as sodium carbonate (3.92 mEq). Each 500 mg MERREM I.V. vial will deliver 500 mg meropenem and 45.1 mg of sodium as sodium carbonate (1.96 mEq).CLINICAL PHARMACOLOGYAt the end of a 30-minute intravenous infusion of a single dose of MERREM I.V. in normal volunteers, mean peak plasma concentrations are approximately 23 µg/mL (range 14-26) for the 500 mg dose and 49 µg/mL (range 39-58) for the 1 g dose. A 5-minute intravenous bolus injection of MERREM I.V. in normal volunteers results in mean peak plasma concentrations of approximately 45 µg/mL (range 18-65) for the 500 mg dose and 112 µg/mL (range 83-140) for the 1 g dose.Following intravenous doses of 500 mg, mean plasma concentrations of meropenem usually decline to approximately 1 µg/mL at 6 hours after administration.In subjects with normal renal function, the elimination half-life of MERREM I.V. is approximately 1 hour. Approximately 70% of the intravenously administered dose is recovered as unchanged meropenem in the urine over 12 hours, after which little further urinary excretion is detectable. Urinaryconcentrations of meropenem in excess of 10 µg/mL are maintained for up to 5 hours after a 500 mg dose. No accumulation of meropenem in plasma or urine was observed with regimens using 500 mg administered every 8 hours or 1 g administered every 6 hours in volunteers with normal renal function.Plasma protein binding of meropenem is approximately 2%.There is one metabolite that is microbiologically inactive.Meropenem penetrates well into most body fluids and tissues including cerebrospinal fluid, achieving concentrations matching or exceeding those required to inhibit most susceptible bacteria. After a single intravenous dose of MERREM I.V., the highest mean concentrations of meropenem were found in tissues and fluids at 1 hour (0.5 to 1.5 hours) after the start of infusion, except where indicated in the tissues and fluids listed in the table below.Table 1. Meropenem Concentrations in Selected Tissues(Highest Concentrations Reported)Tissue I.V. Dose (g) Number ofSamplesMean [µg/mLor µg/(g)]*Range [µg/mLor µg/(g)]Endometrium 0.5 7 4.2 1.7-10.2 Myometrium 0.5 15 3.8 0.4-8.1Ovary 0.582.80.8-4.8 Cervix 0.527.05.4-8.5 Fallopian tube 0.5 9 1.7 0.3-3.4Skin 0.5223.30.5-12.6 Interstitial fluid†0.5 9 5.5 3.2-8.6Skin 1.0105.31.3-16.7 Interstitial fluid† 1.0 5 26.3 20.9-37.4Colon 1.022.62.5-2.7 Bile 1.0714.6(3h)4.0-25.7 Gall bladder 1.0 1 - 3.9Peritoneal fluid 1.0 9 30.2 7.4-54.6Lung 1.0 2 4.8 (2 h) 1.4-8.2Bronchial mucosa 1.0 7 4.5 1.3-11.1Muscle 1.0 2 6. 1 (2 h) 5.3-6.9Fascia 1.098.81.5-20 Heart valves 1.0 7 9.7 6.4-12.1Myocardium 1.0 10 15.55.2-25.5CSF (inflamed) 20 mg/kg‡40 mg/kg§ 851.1 (2 h)3.3 (3 h)0.2-2.80.9-6.5CSF (uninflamed) 1.0 4 0.2 (2 h) 0.1-0.3*at 1 hour unless otherwise noted†obtained from blister fluid‡in pediatric patients of age 5 months to 8 years§in pediatric patients of age 1 month to 15 yearsThe pharmacokinetics of MERREM I.V. in pediatric patients 2 years of age or older are essentially similar to those in adults. The elimination half-life for meropenem was approximately 1.5 hours in pediatric patients of age 3 months to 2 years. The pharmacokinetics are linear over the dose range from 10 to 40 mg/kg.Pharmacokinetic studies with MERREM I.V. in patients with renal insufficiency have shown that the plasma clearance of meropenem correlates with creatinine clearance. Dosage adjustments are necessary in subjects with renal impairment. (See DOSAGE AND ADMINISTRATION - Use in Adults with Renal Impairment.) A pharmacokinetic study with MERREM I.V. in elderly patients with renal insufficiency has shown a reduction in plasma clearance of meropenem that correlates with age-associated reduction in creatinine clearance.Meropenem I.V. is hemodialyzable. However, there is no information on the usefulness of hemodialysis to treat overdosage. (See OVERDOSAGE.)A pharmacokinetic study with MERREM I.V. in patients with hepatic impairment has shown no effects of liver disease on the pharmacokinetics of meropenem.MicrobiologyMeropenem is a broad-spectrum carbapenem antibiotic. It is active against Gram-positive and Gram-negative bacteria.The bactericidal activity of meropenem results from the inhibition of cell wall synthesis. Meropenem readily penetrates the cell wall of most Gram-positive and Gram-negative bacteria to reach penicillin-binding-protein (PBP) targets. Its strongest affinities are toward PBPs 2, 3 and 4 of Escherichia coli and Pseudomonas aeruginosa; and PBPs 1, 2 and 4 of Staphylococcus aureus. Bactericidal concentrations (defined as a 3 log10 reduction in cell counts within 12 to 24 hours) are typically 1-2 times the bacteriostatic concentrations of meropenem, with the exception of Listeria monocytogenes, against which lethal activity is not observed.Meropenem has significant stability to hydrolysis by β-lactamases of most categories, both penicillinases and cephalosporinases produced by Gram-positive and Gram-negative bacteria. Meropenem should not be used to treat methicillin-resistant staphylococci (MRSA).In vitro tests show meropenem to act synergistically with aminoglycoside antibiotics against some isolates of Pseudomonas aeruginosa.Mechanism of ActionMeropenem exerts its action by penetrating bacterial cells readily and interfering with the synthesis of vital cell wall components, which leads to cell death.ResistanceMechanism of ResistanceThere are several mechanisms of resistance to carbapenems: 1) decreased permeability of theouter membrane of Gram-negative bacteria (due to diminished production of porins) causingreduced bacterial uptake, 2) reduced affinity of the target penicillin binding proteins (PBP), 3)increased expression of efflux pump components, and 4) production of antibiotic-destroyingenzymes (carbapenemases, metallo-β-lactamases).Cross-ResistanceCross resistance is sometimes observed with isolates resistant to other carbapenems.Lists of MicroorganismsMeropenem has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.Aerobic and facultative Gram-positive microorganismsEnterococcus faecalis (excluding vancomycin-resistant isolates)Staphylococcus aureus(β-lactamase and non-β-lactamase producing, methicillin-susceptible isolates only)Streptococcus agalactiaeStreptococcus pneumoniae (penicillin-susceptible isolates only)NOTE: Penicillin-resistant isolates had meropenem MIC90 values of 1 or 2 µg/mL, which is above the 0.12 µg/mL susceptible breakpoint for this species.Streptococcus pyogenesViridans group streptococciAerobic and facultative Gram-negative microorganismsEscherichia coliHaemophilus influenzae (β-lactamase and non-β-lactamase producing)Klebsiella pneumoniaeNeisseria meningitidisPseudomonas aeruginosaProteus mirabilisAnaerobic microorganismsBacteroides fragilisBacteroides thetaiotaomicronPeptostreptococcus speciesThe following in vitro data are available, but their clinical significance is unknown.At least 90% of the following microorganisms exhibit an in vitro minimum inhibitory concentration (MIC) less than or equal to the susceptible breakpoints for meropenem. However, the safety and effectiveness of meropenem in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled trials.Aerobic and facultative Gram-positive microorganismsStaphylococcus epidermidis(β-lactamase and non-β-lactamase-producing, methicillin-susceptible isolates only).Aerobic and facultative Gram-negative microorganismsAcinetobacter species Aeromonas hydrophila Campylobacter jejuni Citrobacter diversus Moraxella catarrhalis(β-lactamase andnon-β-lactamase-producing isolates)Citrobacter freundii Morganella morganii Enterobacter cloacae Pasteurella multocidaHaemophilus influenzae(ampicillin-resistant,non-β-lactamase-producing isolates[BLNAR isolates]) Proteus vulgaris Salmonella species Serratia marcescensHafnia alvei Shigella speciesKlebsiella oxytoca Yersinia enterocoliticaAnaerobic microorganismsBacteroides distasonis Eubacterium lentumBacteroides ovatus Fusobacterium speciesBacteroides uniformis Prevotella biviaBacteroides ureolyticus Prevotella intermediaBacteroides vulgatus Prevotella melaninogenicaClostridium difficileClostridium perfringensPorphyromonas asaccharolyticaPropionibacteriumacnesSUSCEPTIBILITY TEST METHODSWhen available, the clinical microbiology laboratory should provide cumulative results of in vitro susceptibility test results for antimicrobial drugs used in local hospitals and practice areas to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.Dilution techniques:Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method1,3 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of meropenem powder. The MIC values should be interpreted according to the criteria provided in Table 2.Diffusion techniques:Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure2,3 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 10-µg of meropenem to test the susceptibility of microorganisms to meropenem. The disk diffusion interpretive criteria are provided in Table 2.Streptococcus pneumoniae isolates should be tested using 1-µg/mL oxacillin disk. Isolates with oxacillin zone sizes of ≥20 mm are susceptible (MIC ≤ 0.06 µg/mL) to penicillin and can beconsidered susceptible to meropenem for approved indications, and meropenem need not be tested. A meropenem MIC should be determined on isolates of S. pneumoniae with oxacillin zone sizes of≤19 mm. The disk test does not distinguish penicillin intermediate isolates (i.e., MICs = 0.12-1.0 µg/mL) from isolates that are penicillin resistant (i.e., MICs ≥ 2 µg/mL). Viridans group streptococci should be tested for meropenem susceptibility using an MIC method. Reliable disk diffusion tests formeropenem do not yet exist for testing streptococci.Anaerobic techniques:For anaerobic bacteria, the susceptibility to meropenem as MICs can be determined by standardized test methods4. The MIC values obtained should be interpreted according to the criteria provided in Table 2.Table 2. Susceptibility Interpretive Criteria for MeropenemSusceptibility Test Result Interpretive CriteriaMinimum Inhibitory Concentrations (µg/mL) Disk Diffusion (zone diameters in mm)Pathogen S I R* S I R* Enterobacteriaceae, Acinetobacterspp. and Pseudomonas aeruginosa ≤ 4 8 ≥ 16 ≥ 16 14-15 ≤ 13 Haemophilus influenzae ≤ 0.5 -- -- ≥ 20 -- -- Staphylococcus aureus†≤ 4 8 ≥ 16 ≥ 16 14-15 ≤ 13 Streptococcus pneumoniae‡≤ 0.12 -- --Streptococcus agalactiae‡ andStreptococcus pyogenes‡≤ 0.5 -- --Anaerobes§ ≤ 4 8 ≥ 16*The current absence of data on resistant isolates precludes defining any category other than “Susceptible.” If isolates yield MIC results other than susceptible, they should be submitted to a reference laboratory for further testing.†Staphylococci that are resistant to methicillin/oxacillin must be considered resistant to meropenem.‡ No Disk diffusion (zone diameter) interpretative criteria have been established for testing Streptococcus pneumoniae, Streptococcus agalactiae, and Streptococcus pyogenes. Use Dilution (MICs) techniques results.§ MIC values using either Brucella blood or Wilkins Chalgren agar (former reference medium) are considered equivalent, based upon published in vitro literature and a multicenter collaborative trial for these antimicrobial agents.No interpretative criteria have been established for testing enterococci and Neisseria meningitidis.A report of Susceptible indicates that the antimicrobial is likely to inhibit growth of the pathogen if the antimicrobial compound in the blood reaches the concentrations usually achievable. A report of Intermediate indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where a high dosage of drug can be used. This category also provides a buffer zone that prevents small uncontrolled technical factors from causing major discrepancies in interpretation. Areport of Resistant indicates that the antimicrobial is not likely to inhibit growth of the pathogen if the antimicrobial compound in the blood reaches the concentrations usually achievable; other therapy should be selected.Quality control:Standardized susceptibility test procedures require the use of quality control microorganisms to control the technical aspects of the test procedures. Standard meropenem powder should provide the following range of values noted in Table 3.Table 3. Acceptable Quality Control Ranges for MeropenemQC Strain Minimum InhibitoryConcentrations (MICs = µg/mL) Disk Diffusion (Zone diameters in mm)Staphylococcus aureusATCC 292130.03-0.12Staphylococcus aureusATCC 2592329-37Streptococcus pneumoniaeATCC 496190.06-0.25 28-35Enterococcus faecalisATCC 292122.0-8.0Escherichia coliATCC 259220.008-0.06 28-34Haemophilus influenzaeATCC 497660.03-0.12Haemophilus influenzaeATCC 4924720-28Pseudomonas aeruginosaATCC 278530.25-1.0 27-33Bacteroides fragilis*ATCC 252850.03-0.25Bacteroides thetaiotaomicron*ATCC 297410.125-0.5Eubacterium lentum*ATCC 430550.125-1INDICATIONS AND USAGETo reduce the development of drug-resistant bacteria and maintain the effectiveness of MERREM I.V. and other antibacterial drugs, MERREM I.V. should only be used to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.MERREM I.V. is indicated as single agent therapy for the treatment of the following infections when caused by susceptible isolates of the designated microorganisms:Skin and Skin Structure InfectionsComplicated skin and skin structure infections due to Staphylococcus aureus (β-lactamase and non-β-lactamase producing, methicillin susceptible isolates only), Streptococcus pyogenes, Streptococcus agalactiae, viridans group streptococci, Enterococcus faecalis (excluding vancomycin-resistantisolates), Pseudomonas aeruginosa, Escherichia coli, Proteus mirabilis, Bacteroides fragilis, and Peptostreptococcus species.Intra-abdominal InfectionsComplicated appendicitis and peritonitis caused by viridans group streptococci, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Bacteroides fragilis, B. thetaiotaomicron, and Peptostreptococcus species.Bacterial Meningitis (Pediatric patients > 3 months only)Bacterial meningitis caused by Streptococcus pneumoniae‡, Haemophilus influenzae (β-lactamase and non-β-lactamase-producing isolates), and Neisseria meningitidis.‡ The efficacy of meropenem as monotherapy in the treatment of meningitis caused by penicillin nonsusceptible isolates of Streptococcus pneumoniae has not been established.MERREM I.V. has been found to be effective in eliminating concurrent bacteremia in association with bacterial meningitis.For information regarding use in pediatric patients (3 months of age and older) see PRECAUTIONS - Pediatrics, ADVERSE REACTIONS, and DOSAGE AND ADMINISTRATION sections. Appropriate cultures should usually be performed before initiating antimicrobial treatment in order to isolate and identify the organisms causing infection and determine their susceptibility to MERREM I.V.MERREM I.V. is useful as presumptive therapy in the indicated condition (i.e., intra-abdominal infections) prior to the identification of the causative organisms because of its broad spectrum of bactericidal activity.Antimicrobial therapy should be adjusted, if appropriate, once the results of culture(s) and antimicrobial susceptibility testing are known.CONTRAINDICATIONSMERREM I.V. is contraindicated in patients with known hypersensitivity to any component of this product or to other drugs in the same class or in patients who have demonstrated anaphylactic reactions to β-lactams.WARNINGSSERIOUS AND OCCASIONALLY FATAL HYPERSENSITIVITY (ANAPHYLACTIC) REACTIONS HAVE BEEN REPORTED IN PATIENTS RECEIVING THERAPY WITH β-LACTAMS. THESE REACTIONS ARE MORE LIKELY TO OCCUR IN INDIVIDUALS WITH A HISTORY OF SENSITIVITY TO MULTIPLE ALLERGENS.THERE HAVE BEEN REPORTS OF INDIVIDUALS WITH A HISTORY OF PENICILLIN HYPERSENSITIVITY WHO HAVE EXPERIENCED SEVERE HYPERSENSITIVITY REACTIONS WHEN TREATED WITH ANOTHER β-LACTAM. BEFORE INITIATING THERAPY WITH MERREM I.V., CAREFUL INQUIRY SHOULD BE MADE CONCERNING PREVIOUS HYPERSENSITIVITY REACTIONS TO PENICILLINS, CEPHALOSPORINS, OTHERβ-LACTAMS, AND OTHER ALLERGENS. IF AN ALLERGIC REACTION TO MERREM I.V. OCCURS, DISCONTINUE THE DRUG IMMEDIATELY. SERIOUS ANAPHYLACTIC REACTIONS REQUIRE IMMEDIATE EMERGENCY TREATMENT WITH EPINEPHRINE, OXYGEN, INTRAVENOUS STEROIDS, AND AIRWAY MANAGEMENT, INCLUDING INTUBATION. OTHER THERAPY MAY ALSO BE ADMINISTERED AS INDICATED.Seizures and other CNS adverse experiences have been reported during treatment with MERREM I.V. (See PRECAUTIONS and ADVERSE REACTIONS.)Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including MERREM I.V., and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.PRECAUTIONSGeneral:Prescribing MERREM I.V. in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.Seizures and other adverse CNS experiences have been reported during treatment with MERREM I.V. These experiences have occurred most commonly in patients with CNS disorders (e.g., brain lesions or history of seizures) or with bacterial meningitis and/or compromised renal function.During clinical investigations, 2904 immunocompetent adult patients were treated for infections outside the CNS, with the overall seizure rate being 0.7% (based on 20 patients with this adverse event). All meropenem-treated patients with seizures had pre-existing contributing factors. Among these are included prior history of seizures or CNS abnormality and concomitant medications with seizure potential. Dosage adjustment is recommended in patients with advanced age and/or reduced renal function. (See DOSAGE AND ADMINISTRATION - Use in Adults with Renal Impairment.)Close adherence to the recommended dosage regimens is urged, especially in patients with known factors that predispose to convulsive activity. Anticonvulsant therapy should be continued in patients with known seizure disorders. If focal tremors, myoclonus, or seizures occur, patients should be evaluated neurologically, placed on anticonvulsant therapy if not already instituted, and the dosage of MERREM I.V. re-examined to determine whether it should be decreased or the antibiotic discontinued.In patients with renal dysfunction, thrombocytopenia has been observed but no clinical bleeding reported. (See DOSAGE AND ADMINISTRATION - Use in Adults with Renal Impairment.) There is inadequate information regarding the use of MERREM I.V. in patients on hemodialysis.As with other broad-spectrum antibiotics, prolonged use of meropenem may result in overgrowth of nonsusceptible organisms. Repeated evaluation of the patient is essential. If superinfection does occur during therapy, appropriate measures should be taken.Laboratory Tests:While MERREM I.V. possesses the characteristic low toxicity of the beta-lactam group of antibiotics, periodic assessment of organ system functions, including renal, hepatic, and hematopoietic, is advisable during prolonged therapy.Drug Interactions:Probenecid competes with meropenem for active tubular secretion and thus inhibits the renal excretion of meropenem. This led to statistically significant increases in the elimination half-life (38%) and in the extent of systemic exposure (56%). Therefore, the coadministration of probenecid with meropenem is not recommended.There is evidence that meropenem may reduce serum levels of valproic acid to subtherapeutic levels (therapeutic range considered to be 50 to 100 µg/mL total valproate).Carcinogenesis, Mutagenesis, Impairment of Fertility:Carcinogenesis:Carcinogenesis studies have not been performed.Mutagenesis:Genetic toxicity studies were performed with meropenem using the bacterial reverse mutation test, the Chinese hamster ovary HGPRT assay, cultured human lymphocytes cytogenic assay, and the mouse micronucleus test. There was no evidence of mutagenic potential found in any of these tests. Impairment of fertility:Reproductive studies were performed with meropenem in rats at doses up to 1000 mg/kg/day, and cynomolgus monkeys at doses up to 360 mg/kg/day (on the basis of AUC comparisons, approximately 1.8 times and 3.7 times, respectively, to the human exposure at the usual dose of 1 g every 8 hours). There was no reproductive toxicity seen.Pregnancy Category B:Reproductive studies have been performed with meropenem in rats at doses of up to 1000 mg/kg/day, and cynomolgus monkeys at doses of up to 360 mg/kg/day (on the basis of AUC comparisons, approximately 1.8 times and 3.7 times, respectively, to the human exposure at the usual dose of 1 g every 8 hours). These studies revealed no evidence of impaired fertility or harm to the fetus due to meropenem, although there were slight changes in fetal body weight at doses of 250 mg/kg/day (on the basis of AUC comparisons, 0.4 times the human exposure at a dose of 1 g every 8 hours) and above in rats. There are, however, no adequate and well-controlled studies in pregnant women. Because animalreproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.Pediatric Use:The safety and effectiveness of MERREM I.V. have been established for pediatric patients ≥ 3 months of age. Use of MERREM I.V. in pediatric patients with bacterial meningitis is supported by evidence from adequate and well-controlled studies in the pediatric population. Use of MERREM I.V. in pediatric patients with intra-abdominal infections is supported by evidence from adequate and well-controlled studies with adults with additional data from pediatric pharmacokinetics studies and controlled clinical trials in pediatric patients. Use of MERREM I.V. in pediatric patients with complicated skin and skin structure infections is supported by evidence from an adequate and well-controlled study with adults and additional data from pediatric pharmacokinetics studies. (See CLINICAL PHARMACOLOGY, INDICATIONS AND USAGE, ADVERSE REACTIONS, DOSAGE AND ADMINISTRATION, and CLINICAL STUDIES sections.)Nursing Mothers:It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when MERREM I.V. is administered to a nursing woman. Geriatric Use:Of the total number of subjects in clinical studies of MERREM I.V., approximately 1100 (30%) were 65 years of age and older, while 400 (11%) were 75 years and older.Additionally, in a study of 511 patients with complicated skin and skin structure infections 93 (18%) were 65 years of age and older, while 38 (7%) were 75 years and older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects; spontaneous reports and other reported clinical experience have not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.A pharmacokinetic study with MERREM I.V. in elderly patients with renal insufficiency has shown a reduction in plasma clearance of meropenem that correlates with age-associated reduction in creatinine clearance. (See DOSAGE AND ADMINISTRATION; Use in Adults with Renal Impairment). MERREM I.V. is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.Information For Patients:Patients should be counseled that antibacterial drugs including MERREM I.V. should only be used to treat bacterial infections. They do not treat viral infections (eg, the common cold). When MERREM I.V. is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by MERREM I.V. or other antibacterial drugs in the future.Diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and。
注射用美罗培南说明书--中诺

注射用美罗培南说明书【药品名称】通用名:注射用美罗培南英文名:Meropenem for Injection汉语拼音:Zhusheyong Meiluopeinan商品名:中诺舒罗克【成份】本品主要成份为美罗培南。
辅料为无水碳酸钠。
化学名称:(-)-(4R,5S,6S)-3{[(3S,5S)-5-(二甲胺基甲酰基)-3-吡咯烷基]硫}-6-[(1R)-1-羟基乙基]-4-甲基-7-氧代-1-氮杂双环[3.2.0]庚-2-烯-2-羧酸三水合物。
化学结构式:分子式:C17H25N3O5S·3H2O分子量:437.51Cas No:96036-03-2【性状】本品为白色至微黄色粉末。
【适应症】美罗培南适用于成人和儿童由单一或多种对美罗培南敏感的细菌引起的感染:肺炎(包括院内获行性肺炎)、尿路感染、妇科感染(如子宫内膜炎和盆腔炎)、皮肤软组织感染、脑膜炎、败血症。
经验性治疗,对成人粒细胞减少症伴发热患者,可单独应用本品或联合抗病毒药或抗真菌药使用。
美罗培南单用或与其它抗微生物制剂联合使用可用于治疗多重感染。
对于中性粒细胞减少或原发性、继发性免疫缺陷的婴儿患者,目前尚无本品的使用经验。
【规格】按C17H25N3O5S计0.5g。
【用法与用量】用法:美罗培南静脉推注的时间应大于5分钟,静脉滴注时间大于15~30分钟。
美罗培南推注时,应使用无菌注射用水配制(每5ml含250mg本品),浓度约50mg/ml。
美罗培南可使用下列输液溶解:0.9%氯化钠溶液、5%或者10%葡萄糖溶液、5%葡萄糖溶液(碳酸氢钠浓度0.02%)、0.9%氯化钠溶液和5%葡萄糖溶液、5%葡萄糖溶液(氯化钠浓度0.225%)、5%葡萄糖溶液(氯化钾浓度0.15%)25%或10%甘露醇溶液。
用量:成人:给药剂量和时间间隔应根据感染类型、严重程度及病人的具体情况而定。
推荐日剂量如下:肺炎、尿路感染、妇科感染(如子宫内膜炎)、皮肤或软组轵感染,每8小时给药一次,每次500mg,静脉滴注。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
注射用美罗培南说明书
【商品名】美乐平干粉注射剂
【商品英文名】Mexopem powder for Injection
【通用名】注射用美罗培南
【英文名】Meropenem for Injection
【汉语拼音】Zhusheyong Meiluopeinan
【生产企业】政德制药股份有限公司
【功效主治】美罗培南临床上主要适用于敏感菌引起的下列感染:1、呼吸系统感染,如慢性支气管炎、肺炎、肺脓疡、脓胸等。
2、腹内感染,如胆囊炎、胆管炎、肝脓疡、腹膜炎等。
3、泌尿、生殖系统感染,如肾孟肾炎、复杂性膀胱炎、子宫附件炎、子宫内感染、盆腔炎、子宫结缔组织炎等。
4、骨、关节及皮肤、软组织感染,如蜂窝组织炎、肛门周围脓肿、骨髓炎、关节炎、外伤创口感染、烧伤创面感染、手术切口感染、颌骨及颌骨周围蜂窝组织炎等。
5、眼及耳鼻喉感染。
6、其他严重感染,如脑膜炎、败血症等。
【化学成分】
本品主要成分为美罗培南,其化学名称为3-[[5-[(二甲氨基)羰基]-3-吡咯烷基]硫代]-6-(1-羟乙基)-4-甲基-7-氧代-1-氮杂双环[3,2,0]庚-2-烯-2-羧酸。
【药理作用】
美罗培南通过其共价键与参与细胞壁合成的青霉素结合蛋白(PBP S)结合,从而抑制细菌细胞壁的合成,起抗菌作用。
美罗培南对革兰阳性菌、革兰阴性菌均敏感。
尤其对革兰阴性菌又很强的抗菌活性。
对约90%肠杆菌属的最小抑菌浓度(MIC)为0.08~0.15mg/L;90%以上的铜绿假单胞菌菌株对其高度敏感,最小抑菌浓度(MIC)为0.06~1mg/L;淋球菌对美罗培南也高度敏感,其活性强于亚胺培南15倍;表皮葡萄球菌、腐生葡萄球菌和其他凝固酶阴性葡萄球菌对美罗培南敏感;粪肠球菌的大多数菌株对美罗培南高度或中度敏感;美罗培南可抑制几乎全部的脆弱拟杆菌;厌氧菌如消化链球菌属、丙酸杆菌属、放线菌属等也对美罗培南铭感。
【药物相互作用】
1、丙磺舒和本品联合用药可降低本品的血浆清除率。
同时延长本品的半衰期。
2、本品与伤寒疫苗同用,可能会干扰伤寒活疫苗的免疫反应。
3、有报道抗癫痫药与本品合用可使抗癫痫药的血浆浓度降低。
【不良反应】
1、过敏反应:主要有皮疹、瘙痒、药热等过敏反应;偶见过敏性休克。
2、消化系统:主要有腹泻、恶心、呕吐、便秘等胃肠道症状。
3、肝脏:偶见肝功异常、胆汁郁积型黄疸等。
4、肾脏:偶见排尿困难和急性肾衰。
5、中枢神经系统:偶见失眠、焦虑、意识模糊、眩晕、神经过敏、感觉异常、幻觉、抑郁、
痉挛、意识障碍等中枢神经系统症状。
国外有报道,用药后后可诱发癫痫发作。
6、血液系统:偶见胃肠道出血、鼻出血和腹腔积血等出血症状。
7、注射给药时可致局部疼痛、红肿、硬结,严重者可致血栓性静脉炎。
【禁忌症】
孕妇及哺乳期妇女慎用。
对本品过敏者禁用。
老年人因半衰期延长,应减少剂量。
【产品规格】
0.25g、0.5g、1.0g
【用法用量】
静脉给药:
1、成人,常规剂量:每8小时给药500~1000mg。
(1)脑膜炎:每8小时给药2000mg。
(2)
有发热特征的中性粒细胞减少症的癌症患者:每8小时给药1000mg。
(3)合并腹内感染和热敏·敏感菌引起的腹膜炎:每8小时给药1000mg。
(4)皮肤和软组织感染:每8小时给药500mg。
(5)尿路感染:一次500mg,一日2次。
2、肾功能不全时剂量:肌酐清除率为26~50ml/min者,每12小时给药1000mg;肌酐清除
率为10~25ml/min者,每12小时给药500mg;肌酐清除率小于10ml/min者,每24小时给药500mg;
3、肝功能不全时剂量:轻度肝功不全患者不需要调剂量。
4、透析时剂量:透析患者在血液透析时建议增加剂量。
5、小儿剂量:按体重一次10~20mg/kg,一日3次。
【贮藏方法】
室温下保存,有效期3年。
【注意事项】
1、慎用:(1)对β-内酰胺抗生素过敏患者慎用。
(2)严重肝、肾功能障碍者慎用。
(3)支
气管哮喘、皮疹、荨麻疹等过敏体质患者慎用。
(4)癫痫、潜在神经疾患患者慎用。
2、药物对检验值或诊断的影响:少数患者用药后可出现丙氨酸氨基转移酶、门冬氨酸氨基
转移酶升高。
3、长期用药时应注意检测肝、肾功能和血象。
4、由于本品有广谱抗菌活性,因此在尚未确定致病菌前,本品可单独使用。
5、本品与齐多夫定、昂单司琼、多种维生素、多西环素、地西泮、葡萄糖酸钙和阿昔洛韦
等药有配伍禁忌。
6、溶液的配置:以适宜溶液稀释后在15~30分钟内静脉滴注或用无菌注射用水稀释后在
3~5分钟内静脉注射。