2015年国际腹水俱乐部共识建议:肝硬化患者急性肾损伤的诊断与管理 王帅 译
肝肾综合征的中西医结合诊治
!()*+!肝肾综合征的中西医结合诊治梁家琦,刘 汶首都医科大学附属北京中医医院感染科,北京100010摘要:肝肾综合征(HRS)是终末期肝病常见的并发症,是在严重肝病基础上发生的功能性急性肾衰竭,是以肾功能不全、内源性血管活性物质异常和动脉循环血流动力学改变为特征的一组临床综合征。
HRS较为理想的治疗是肝移植或同时肾移植,优化药物与非药物治疗方法是治疗HRS的关键。
本文对目前中西医诊断和治疗HRS的现状予以回顾总结。
关键词:肝肾综合征;诊断;中西医结合疗法IntegratedtraditionalChineseandWesternmedicinediagnosisandtreatmentofhepatorenalsyndromeLIANGJiaqi,LIUWen.(DepartmentofInfectiousDiseases,BeijingHospitalofTraditionalChineseMedicine,CapitalMedicalUniversity,Beijing100010,China)Correspondingauthor:LIUWen,lwsxp2@126.com(ORCID:0000-0003-1669-4855)Abstract:Asacommoncomplicationofend-stageliverdisease,hepatorenalsyndrome(HRS)isfunctionalacuterenalfailurethatoccursonthebasisofsevereliverdiseasesandisagroupofclinicalsyndromescharacterizedbyrenalinsufficiency,abnormalendogenousvascularsubstances,andhemodynamicchangesofarterialcirculation.TheidealtreatmentmethodforHRSislivertransplantationorsimultaneouskidneytransplantation,andoptimizationofdrugandnon-drugtherapiesisthekeytothetreatmentofHRS.ThisarticlereviewsthecurrentstatusoftheintegratedtraditionalChineseandWesternmedicinediagnosisandtreatmentofHRS.Keywords:HepatorenalSyndrome;Diagnosis;TCMWMTherapyDOI:10.3969/j.issn.1001-5256.2022.09.005收稿日期:2022-05-31;录用日期:2022-07-01通信作者:刘汶,lwsxp2@126.com 肝肾综合征(hepatorenalsyndrome,HRS)是一种在严重肝病基础上导致全身循环功能障碍引起的急性肾功能恶化疾病,作为肝硬化的并发症之一,其预后差,存活率低。
肝硬化肝肾综合征型急性肾损伤的诊治进展 宋廷雪
㊀㊀肝硬化腹水患者常出现少尿和水钠潴留, 且需使 用利尿 剂 以 增 加 尿 量, 故 收 集 到 的 尿 量 并 不 准 确。 I C A的 A K I 诊断标准对尿量未作出明确要求。肝硬
8 ] C r 常维持在稳定水平 [ , 故I C A的 A K I 诊断 化患者 S
K e yw o r d s : l i v e c i r r h o s i s ;h e p a t o r e n a l s y n d r o m e ;d i a g n o s i s ;t h e r a p y ;r e v i e w
㊀㊀在中国, 急性肾损伤( a c u t ek i d n e yi n j u r y , A K I ) 诊 断常被延误 倍
3 ] 持肾脏血流灌注 [ , 治疗 H R S-A K I 。常用血管收缩
剂包括特利加压素、 米多君、 奥曲肽、 多巴胺和去甲肾 上腺素。 3 . 1 ㊀特利加压素㊀特利加压素是一种抗利尿激素的 衍生物, 通过作用于 V 1受体加强血管收缩, 增加内脏 血管阻力而使血流重新分布, 进而增加肾脏灌注, 改 善肾功能。肝硬化患者血浆白蛋白减少, 应用白蛋白 主要在于提高胶体渗透压, 以改善血流动力学。 S a n
[ 2 ] [ 1 ]
于肝硬化所导致的肾功能性病变, 故未列入本文的讨 论范畴。 1 ㊀肝硬化 A K I 定义 国际腹水俱乐部( I C A ) 于2 0 1 5年对肝硬化 A K I
7 ] 作出了定义 [ : 4 8h内 S C r 水平增长超过 0 . 3m g / d l
, 每延误 1 2h , 其住院病死率增加 2 . 7
特利加压素在7种肝硬化并发症的临床应用

特利加压素在7种肝硬化并发症的临床应用1.肝硬化伴食管胃静脉曲张出血指导声明1 推荐特利加压素用于治疗肝硬化急性食管胃静脉曲张出血。
急性消化道出血是肝硬化常见的严重并发症之一,食管胃静脉曲张出血是其最常见的病因。
特利加压素已被推荐用于肝硬化伴急性食管胃静脉曲张出血的一线药物治疗。
欧洲肝病学会(European Association for the Study of the Liver,EASL)和美国肝病学会指南推荐,特利加压素的常用剂量为2 mg/次,每4 h 1次,静脉注射,持续2~5 d。
有研究表明,持续静脉输注特利加压素可以使降低门静脉压力的作用更加平稳,防止用药间期门静脉压力反弹,提高治疗成功率。
结合我国临床实践情况,推荐首次剂量为4 h内1~2 mg,缓慢静脉注射(注射时间需>1 min)或静脉持续输注;维持剂量为1~2 mg/次,每6 h 1次,静脉持续输注,持续3~5 d,可根据出血严重情况和患者状态调整用药剂量和时长,一般用药时长≤5 d,每日最大剂量≤150 μg/kg。
指导声明2 对于肝硬化急性消化道出血患者,若怀疑出血来源为食管胃静脉曲张破裂,则可在内镜检查前考虑使用特利加压素。
肝硬化患者中,一部分消化道出血的原因为非静脉曲张性,包括消化性溃疡、门静脉高压性胃病、胃和十二指肠黏膜糜烂性疾病等。
内镜检查是明确消化道出血原因的最重要手段。
然而,在临床实践中,并非所有急性消化道出血患者都接受了急诊内镜检查,尤其是在一些缺少内镜设备和(或)经验丰富的内镜医师的基层医院。
真实世界研究也显示,急性消化道出血患者中60%~80%接受了内镜检查。
因此,仍有一部分急性消化道出血的原因未能明确。
虽然急性非静脉曲张性消化道出血的一线治疗药物为高剂量质子泵抑制剂,但考虑到肝硬化患者的急性消化道出血60%以上为食管胃静脉曲张破裂所致,故临床医师在接诊尚未明确病因的肝硬化急性消化道出血患者时也常立即予以血管活性药物治疗,在内镜检查后再调整治疗方案。
肝肾综合征诊断及治疗研究进展

ChineseHepatology,Jan.2020,Vol.25,No.1·综 述·肝肾综合征诊断及治疗研究进展张军昌 牟劲松 林芳 陈素红 作者单位:100039 北京 中国人民解放军总医院第五医学中心重症医学中心通信作者:牟劲松,Email:Jinsongmu@126.com 肝肾综合征(Hepatorenalsyndrome,HRS)是发生在重症肝病如肝硬化合并腹水、急性肝衰竭和酒精性肝炎患者中以肾功能损伤为主要表现的一种严重并发症[1]。
目前治疗HRS的主要药物是血管收缩剂如特利加压素和人血白蛋白,其治疗有效率仅为40%~50%,而且治疗有效的患者中有50%可能会复发。
所有HRS患者在没有禁忌证时都应考虑首选行肝移植手术[2]。
HRS是临床诊断,其定义根据最近急性肾损伤(acutekidneyinjury,AKI)标准进行了更新并且使用生物标志物来帮助鉴别诊断。
关于对HRS的研究旨在进一步提高HRS诊断的准确性及探求新的治疗方法。
本文对肝肾综合征的诊断及治疗研究进展予以综述。
一、HRS流行病学Fede等学者研究报道,大约有20%肝硬化合并腹水而且对利尿剂抵抗的患者有可能发展为HRS[3]。
Ginès等学者研究,229例肝硬化患者中,在一年内有18%患者发展为HRS,在确诊后的5年内上升到39%[4]。
Wong等学者研究报道,HRS发病率随着肝脏疾病进展而增加,在等待肝移植的患者中其发病率为48%[5]。
尽管文献数据存在差异,但近年来肝肾综合征的发病率有所下降,这可能是由于对其病理生理学和临床治疗办法的更好理解[6]。
二、HRS诊断目前最新的诊断标准是国际腹水俱乐部(theInternationalClubofAscites,ICA)制定的,肝硬化HRS AKI诊断标准具体如下[7]:①肝硬化和腹水诊断明确;②符合ICA AKI诊断标准;③停用利尿剂并输注白蛋白(1g/kg)两天无效;④无休克;⑤目前或近期未使用肾毒性药物;⑥无蛋白尿(尿蛋白≤500mg/d)、无微量血尿(≤50红细胞/高倍视野),肾脏超声检查正常。
【共识意见】辨证论治:肝硬化腹水

【共识意见】辨证论治:肝硬化腹⽔肝硬化腹⽔是⼀种常见的慢性进⾏性、弥漫性肝病终末期阶段的并发症,可由病毒性肝炎、酒精性肝炎、胆汁淤积性肝病、⾃⾝免疫性肝炎、药物性肝炎、⾮酒精性脂肪性肝炎、⾎吸⾍病等引起。
当腹腔内出现过多游离液体(>50 ml)时称为腹⽔。
中国武汉地区的年均肝硬化住院率为23/10万,年死亡率8.5/10万。
腹⽔是肝硬化的常见并发症之⼀,占住院肝硬化患者的67.3%;约50%的代偿期肝硬化患者10年内会出现腹⽔,有腹⽔的患者预后差,肝硬化腹⽔患者1年后病死率为15%,5年病死率可⾼达44%。
中医药治疗对促进腹⽔消退、预防腹⽔复发等⽅⾯具有重要作⽤。
中华中医药学会脾胃病分会于2012年公布了《肝硬化腹⽔中医诊疗规范专家共识意见》。
随着肝硬化腹⽔中医研究的进展,有必要对该诊疗共识意见进⾏更新,以满⾜临床诊治和科研的需要。
辨证论治⽓滞⽔停证治法:疏肝理⽓,⾏⽔散满。
主⽅:柴胡疏肝散(《景岳全书》)合胃苓汤(《普济⽅》)。
药物:柴胡、枳壳、芍药、⽢草、⾹附、川芎、茯苓、苍术、陈⽪、⽩术、官桂、厚朴、泽泻、猪苓、⽣姜、⼤枣。
加减:腹胀明显者,加⼤腹⽪、莱菔⼦、⽊⾹;两胁胀满疼痛者,加郁⾦、延胡索、苏⽊。
脾虚⽔停证治法:温中健脾,⾏⽓利⽔。
主⽅:四君⼦汤(《太平惠民和剂局⽅》)合实脾饮(《济⽣⽅》)。
药物:⼈参、⽩术、茯苓、炙⽢草、附⼦、⼲姜、厚朴、⽊⾹、草果、槟榔、⽊⽠、⽣姜、⼤枣。
加减:湿浊中阻,恶⼼呕吐者,加陈⽪、⽵茹;肢体沉困,⼩便短少者,加车前⼦、泽泻。
湿热⽔停证治法:清热利湿,攻下逐⽔。
主⽅:中消分满丸(《兰室秘藏》)合茵陈蒿汤(《伤寒论》)。
药物:厚朴、枳实、黄芩、黄连、知母、法半夏、陈⽪、茯苓、猪苓、泽泻、砂仁、⼲姜、姜黄、⼈参、⽩术、⽢草。
加减:⼩便⾚涩不利者,加滑⽯、通草;下肢浮肿明显者,加车前草、⾚⼩⾖。
⾎瘀⽔停证治法:活⾎化瘀,⾏⽓利⽔。
主⽅:调营饮(《证治准绳》)或膈下逐瘀汤(《医林改错》)。
急性肾损伤的肾功能的检测评估新进展
急性肾损伤的肾功能的检测评估新进展作者:朱峰王智峰李峻岭来源:《中国实用医药》2010年第29期【摘要】随着对急性肾损伤认识的不断深化,如何早期评定肾脏功能,相关检测方法日益得到重视,本文从菊粉清除率、内生肌酐清除率等目前流行的测定方法进行系统性概述,希冀为急性肾损伤的检测提供新的思路。
【关键词】急性肾损伤;肾小球滤过率内生肌酐清除率急性肾损伤是一个综合征,是由各种原因使两肾排泄功能在短期内(数小时到数周)迅速减退,肾小球滤过功能短期内迅速下降,血尿素氮及血肌酐迅速升高并引起水、电解质及酸碱平衡失调及急性尿毒症症状。
肾小球滤过率(GFR)是反映肾小球滤过功能的直接指标,是肾功能分期的主要依据,准确的检测和评估肾小球滤过率对于急性肾衰的早期诊断、及时治疗和随访观察有十分重要的意义。
GFR不能直接测定,但可以通过测定某种滤过标志物的滤过率得到。
其分为外源性和内源性两种,前者包括菊粉、同位素标记物,后者包括尿素氮(BUN)、肌酐(Cr)及低分子量蛋白如半胱氨酸蛋白酶抑制剂 cystatin C、α1-MG、-MG等,但小分子蛋白质被肾小球滤过后,将被肾小管重吸收或分解代谢,只能测血清浓度来反映小球滤过功能,而不能测其血浆清除率。
1 菊粉清除率Homer Smith于1938年提出用菊粉清除率(Cin)检测GFR。
菊粉为从植物块茎中提取的不带电荷的果糖聚合物,分子量5200 d。
其清除只从肾小球滤过而不被肾小管重吸收或排泌,体内不能合成也不能分解。
2 BUN、Cr及其清除率Scr和内生肌酐清除率(Ccr)是临床上最常用的反映肾功能指标。
Ccr经典测定法:素食3 d 后,收集24 h全部尿液,在收集尿液结束时取血,测血、尿肌酐定量,按Ucr*V/Pcr公式计算Ccr,并根据体表面积校正[1]。
采取测清晨空腹血及取血前后共4 h全部尿进行Ccr测定以减小上述误差。
目前提出了大量用血肌酐计算GFR和肌酐清除率的方程,如Cockroft-Gault和MDRD公式,但其应用的前提要求机体处于稳态,并能够估算肌酐的平均生成量,如果GFR是快速变化的,那么这样的估算就是不可靠的。
2015肝硬化腹水知识讲座解析
限钠
限制钠盐可以减少利尿剂用量,更快缓解腹水,缩短住院 时间。饮食钠盐应限制在90mmol/d(5.2g盐)。
一些药物,尤其是泡腾片,钠含量较高。静脉应用的抗生 素通常每克含2.1-3.6mmol钠,环丙沙星每200ml(400mg) 含30mmol钠。 原则上腹水患者避免输入含钠盐的液体,但有些情况,如 肝肾综合征和肾功能不全伴严重低钠血症时,应当输入晶 体液和胶体液进行扩容。对肝肾综合征患者,国际腹水协 会推荐输入正常钠盐。
利尿治疗中低钠血症的处理
低钠血症:<135mmol/l
血钠>125mmol/l 血钠≤125mmol/l
血钠>125mmol/l
腹水患者若血钠>125mmol/l,不必限水,可 安全使用利尿剂,只要肾功能没有明显恶化。
血钠≤125mmol/l
中度低钠血症(血钠121-125mmol/l)有争议。 英国的意见是,一旦血钠≤125mmol/l,应停用利尿剂并继 续观察。本领域的共识是血钠≤120mmol/l是必须停用利尿 剂。 如果血肌酐明显升高或血肌酐>150μmmol/l,建议扩容。 琥珀明胶(Gelofusine)、聚明胶肽(Haemaccel)、4.5% 的白蛋白溶液,含有和生理盐水相同的钠浓度。 扩容会加重水钠潴留,但正常肾功能伴有腹水比肾衰好。
腹穿步骤
腹穿要严格无菌,穿刺套管应多孔以防止肠管阻 塞。 通常采用Z型轨道穿入,即垂直穿入皮肤后斜进针, 再垂直穿透腹膜,以保证皮肤和腹膜的穿刺孔不 重叠,防止渗漏。 腹穿后如有渗漏,应反向卧位2h,穿刺点周围缝 合(最好荷包缝线)。
腹水检查
中性粒细胞计数 SBP 培养 蛋白 SA-AG 淀粉酶 细胞学
肝硬化腹水、自发性细菌性腹膜炎、肝肾综合征的处理-34页精选文档
EASL临床实践指南;肝硬化腹水、自发性细菌性腹膜炎、肝肾综合征的处理欧洲肝脏研究学会腹水是肝硬化最常见的并发症,在其病程中,约60%的代偿期肝硬化患者在10年内发生腹水[1]。
腹水仅在门脉高压形成时才会出现[2],主要与无法排泄适量的钠进入尿液有关,从而导致正钠平衡。
大量证据表明,肝硬化患者肾钠潴留继发于内脏动脉血管舒张,随动脉和心肺容量受体激活导致有效动脉血容量下降,以及血管收缩神经和钠潴留系统(交感神经系统和肾素-血管紧张素-醛固酮系统)稳态激活。
肾钠潴留引起细胞外液体量增加以及腹水和水肿的形成[3-5]。
肝硬化患者腹水的发生与不良预后以及生活质量的受损有关[6,7]。
因此,腹水的患者一般应考虑转诊行肝移植。
由于成功的治疗可以改善转归和症状,处理肝硬化患者的腹水就有明确的理由。
在2019—2009年期间,欧洲肝脏研究学会(EASL)理事会选择的一个专家小组举行了若干次会议,讨论并撰写了这些指南。
指南根据从PubMed检索到的已发表研究文献而撰写。
指南中提及的证据和推荐意见按照GRADE系统(推荐分级的评估,制定与评价)进行分级。
表1;证据质量和建议 (改编自GRADE系统)注释证据质量高(A)进一步研究不可能改变我们在疗效评估中的信心中(B)进一步研究可能对我们在疗效评估中的信心有重要影响,并且可改变评估低或非常低(C)进一步研究非常可能对我们在疗效评估中的信心有重要影响,并且可能改变评估,任何疗效评估都是不确定的分级建议强(1)影响推荐强度的因素包括:证据质量、推测的患者重要转归,和费用弱(2)意愿和价值观具有可变性,或更多的不确定性,更可能的弱的推荐。
推荐强度不确定,高费用或资源消耗证据强度分为3种水平:A,高;B,中;C,低质量证据,同时推荐意见分为2种:强与弱(见表1)。
在没有明确证据的情况下,这些推荐意见则基于文献中和写作委员会中专家们的共识意见无并发症的腹水腹水患者的评估大约75%的西欧或美国腹水患者有肝硬化这一基础病因。
肝肾综合征定义、分型及病理生理新进展
肝脏2020年1月第25卷第1期·前沿与探索·肝肾综合征定义、分型及病理生理新进展宦红娣 陈成伟 作者单位:200235 上海 中国人民解放军海军第九○五医院 肝肾综合征(hepatorenalsyndrome,HRS)曾被认为是功能性肾功能异常,表现为全身动脉血管扩张及内源性血管活性系统异常,常无实质性肾损伤。
随着对急性肾损伤(acutekidneyinjury,AKI)认识的不断深入,2015年国际腹水俱乐部(internationalclubofascites,ICA)建议将AKI概念及分期引入到肝硬化患者肾衰竭的诊断及治疗中,认为HRS不能涵盖所有的肾脏并发症,其只是AKI的一种功能形式。
过去的20年里认为HRS的发病机制是内脏动脉扩张理论,HRS只发生在内脏/系统动脉扩张及心输出量下降导致有效循环容量明显下降时。
目前认为除了血流动力学异常外,系统性炎症、氧化应激及胆汁酸盐的直接肾小管毒性作用等共同参与了HRS的发生、发展。
重新修订HRS的诊断及分型标准势在必行,本文就HRS的定义、分型、诊断标准、发病机制、治疗等新进展作一综述。
一、HRS定义及分型2007年ICA建议HRS分为1型和2型。
1型HRS表现为肾功能快速进展,2周内血清肌酐(serumcreatinine,Scr)升高2倍(>2.5mg/dL),常与一些促发因素紧密相关。
2型HRS肾功能中度缓慢进展(Scr<2.5mg/dL),常表现为顽固性腹水。
2015年ICA修订了HRS的诊断标准[1],和原先标准有些混淆。
目前认为HRS只是肝病患者肾功能不全的一种表现形式,可以由肝性(酒精、药物、肝炎复发)和/或肝外(细菌感染和/或细菌易位)因素诱发或加重。
HRS的分型基于肾功能异常是急性、亚急性或慢性分别定义为AKI、急性肾脏病(acutekidneydisease,AKD)或慢性肾脏病(chronickidneydisease,CKD)。
2015+ICA共识建议:肝硬化患者急性肾损伤的诊断和管理

Diagnosis and management of acute kidney injury in patientswith cirrhosis:Revised consensus recommendations ofthe International Club of Ascites qPaolo Angeli 1,⇑,Pere Ginès 2,3,4,5,Florence Wong 6,Mauro Bernardi 7,Thomas D.Boyer 8,Alexander Gerbes 9,Richard Moreau 10,11,12,Rajiv Jalan 13,Shiv K.Sarin 14,Salvatore Piano 1,Kevin Moore 15,Samuel S.Lee 16,Francois Durand 17,18,Francesco Salerno 19,Paolo Caraceni 7,W.Ray Kim 20,Vicente Arroyo 2,3,4,Guadalupe Garcia-Tsao 211Unit of Hepatic Emergencies and Liver Transplantation,Department of Medicine—DIMED,University of Padova,Padova,Italy;2Liver Unit,Hospital Clinic,University of Barcelona,Barcelona,Spain;3Institut d’Investigacions Biomediques Agust Pi i Sunyer (IDIBAPS),Barcelona,Spain;4Centro de Investigación Biomédica en Red en Enfermedades Hepáticas y Digestivas (CIBEREHD),Barcelona,Spain;5Instituto Reina Sofia d’Investigación en Nefrologia (IRSIN),Barcelona,Spain;6Division of Gastroenterology,Department of Medicine,University of Toronto,Toronto,Canada;7Dipartimento di Scienze Mediche e Chirurgiche,Alma Mater Studiorum,University of Bologna,Bologna,Italy;8Department of Medicine,Liver Research Institute,University of Arizona,College of Medicine,Tucson,Arizona,USA;9Liver Unit,Klinikum Munich,Ludwig Maximilian University of Munich,Munich,Germany;10Inserm U1149,Centre de recherche sur l’Inflammation (CRI),Paris,France;11UMR S_1149,UniversitéParis Diderot,Paris,France;12DHU UNITY,Service d’hépatologie,Hôpital Beaujon,APHP,Clichy,France;13Liver Failure Group,UCL Institute for Liver and Digestive Health,UCL Medical School,Royal Free Hospital,London,UK;14Department of Hepatology,Institute of Liver and Biliary Sciences,New Delhi,India;15UCL Institute of Liver and Digestive Health,Royal Free Campus,University College London,London,UK;16Liver Unit,University of Calgary,Calgary,Canada;17Hepatology and Liver Intensive Care Unit,Hospital Beaujon,Clichy,France;18INSERM U773,Centre de Recherche Biomédicale Bichat Beaujon CRB3,Clichy,France;19Policlinico IRCCS San Donato,Medicina Interna ed Epatologia,Universitàdi Milano,Milan,Italy;20Division of Gastroenterology and Hepatology,Stanford University Medical School,Palo Alto,California,USA;21Division ofDigestive Diseases,Yale University School of Medicine,New Haven,Connecticut,USAIntroductionAcute renal failure (ARF)is a common complication in patients with decompensated cirrhosis.The traditional diagnostic criteria of renal failure in these patients were proposed in 1996[1]and have been refined in subsequent years [2].According to these cri-teria,ARF is defined as an increase in serum creatinine (sCr)of P 50%from baseline to a final value >1.5mg/dl (133l mol/L).However,the threshold value of 1.5mg/dl (133l mol/L)sCr to define renal failure in patients with decompensated cirrhosis has been challenged [3,4].In addition,the timeframe to distinguish acute from chronic renal failure has not been clearly identified,the only exception being type 1hepatorenal syndrome (HRS).Meanwhile,new definitions for ARF,now termed acute kidney injury (AKI),have been proposed and validated in patients without cirrhosis [5–7].Recently these new criteria were also proposed and applied in the diagnosis of AKI in patients with cirrhosis [3,8–15].Thus,in December 2012,the InternationalClub of Ascites (ICA)organised a consensus development meeting in Venice,Italy,in order to reach a new definition of AKI in patients with cirrhosis.The discussion among the experts continued thereafter for 2years,both online and through several meetings,between those experts who had different positions on crucial points on the subject.This paper reports the scientific evidence supporting the final proposal of a new approach to the diagnosis and treatment of this condition,on which the experts agreed.Diagnostic criteria of AKI and their application in patients with cirrhosisAKI is defined as an acute significant reduction in the glomerular filtration rate (GFR).sCr remains the most practical biomarker of renal function in patients with ARF (with or without cirrhosis).However,sCr as a biomarker of renal function has many limita-tions in clinical practice since it is influenced by body-weight,race,age,and gender.The use of sCr in patients with cirrhosis is also affected by:(1)decreased formation of creatinine from creatine in muscles,secondary to muscle wasting [16];(2)increased renal tubular secretion of creatinine [17];(3)the increased volume of distribution in cirrhosis that may dilute sCr;(4)interference with assays for sCr by elevated bilirubin [18].As a consequence,measurement of sCr in patients with cirrhosis overestimates GFR or kidney function.Therefore,theJournal of Hepatology 2015vol.62j968–974Ó2015BMJ Publishing Group Ltd,British Society of Gastroenterology and European Association for the Study of the Liver.Published by Elsevier B.V.All rights reserved.Received 17December 2014;accepted 17December 2014qThis article is being published jointly in Gut and Journal of Hepatology .⇑Corresponding author.Address:Department of Medicine (DIMED)and Unit of Hepatic Emergencies and Liver Transplantation,University of Padova,Via Giustiniani 2,Padova 35100,Italy.E-mail address:pangeli@unipd.it (P.Angeli).PositionPaperuse of afixed threshold of sCr at1.5mg/dl(133l mol/L)to define AKI in cirrhosis[1,2]is problematic,because of two crucial prob-lems.Thefirst is that an sCr value of1.5mg/dl(133l mol/L)often signifies that GFR is markedly decreased(to 30ml/min)[19]; secondly,thefixed threshold does not take into account the dynamic changes in sCr that occur in the preceding days or weeks,which are needed to distinguish between acute and chronic kidney injury.Since the use of a single value of sCr is not sufficient to diagnose AKI,a dynamic definition referring to an acute increase of sCr to P50%from baseline to afinal value P1.5mg/dl(133l mol/L)has been used in several clinical studies in patients with cirrhosis(Table1).AKI,as defined by these crite-ria,was a strong predictor of in-hospital mortality in patients with cirrhosis[20–23].In recent years,diagnostic criteria have been proposed for the diagnosis of ARF in non-cirrhotic patients, now termed AKI.In particular,two separate bodies developed and published two consensus definitions of AKI:the Acute Dialy-sis Quality Initiative group for the Risk,Injury,Failure,Loss of Renal Function and End-Stage Renal Disease(RIFLE)criteria; and the Acute Kidney Injury Network(AKIN)group for the AKIN criteria(Table1)[5,6].More recently,a panel of experts has sug-gested combining part of the AKIN criteria(increase of sCr of 0.3mg/dl(26.5l mol/L)within48h or by P50%from baseline together with a reduction in urine output to<0.5ml/kg/h for >6h)with part of the RIFLE criteria(increase of sCr P50%within 1week or a reduction in GFR by>25%together with a reduction in urine output to<0.5ml/kg/h for>6h),thus leading to the proposal of the Kidney Disease Improving Global Outcome(KDI-GO)criteria[7](Table1).However,the use of a reduction of urine output in patients with cirrhosis and ascites as a diagnostic criterion is a problem, since these patients are frequently oliguric with avid sodium retention and yet may maintain a relatively normal GFR[24]. Conversely,these patients may have an increased urine output because of diuretic treatment.Thus,urine collection is often inac-curate in clinical practice and the use of kinetic changes in sCr becomes the crux of the definition for the diagnosis of AKI in cir-rhosis.The main differences between these new criteria over the conventional criteria in patients with cirrhosis are the following: (1)an absolute increase in sCr is considered;(2)the threshold of sCr P1.5mg/dl(133l mol/L)is abandoned;and(3)a staging sys-tem of AKI,based on a change in sCr over a slightly longer time frame,arbitrarily set at1week to enable assessment for progres-sion of stage(modified from AKIN staging)as well as a regression of stage(Table1).AKIN criteria have been shown to be a good predictor of mortality in large cohorts of hospitalised cirrhotic patients,including those in intensive care units[25]and the crit-ically ill[26].More recently,AKI as diagnosed with AKIN criteria has been shown to be associated with increased mortality in patients with cirrhosis who were hospitalised in regular wards in an AKIN stage-dependent fashion[8–13,15].Further,the pro-gression of AKI through stages(e.g.,from stage1to2or stage2Table1.Current diagnostic criteria for acute kidney injury(AKI)in the general population and in patients withcirrhosis.AKIN,Acute Kidney Injury Network;GFR,glomerularfiltration rate;KDIGO,Kidney Disease Improving Global Outcome;RIFLE,Risk,Injury,Failure,Loss,End stage renal disease;sCr,serumcreatinine.JOURNAL OF HEPATOLOGY Journal of Hepatology2015vol.62j968–974969to 3)was strongly correlated with an increased mortality in these patients [8–10].Nevertheless,a comparison of the prognostic accuracy of the conventional criteria and the new criteria in patients with cirrhosis was considered crucial for the develop-ment of a new algorithm for the management of AKI and was pro-posed by the ICA in 2011[3].However,the cut-off value of 1.5mg/dl (133l mol/L)still has important resonance with many clinicians.Two prospective studies have recently shown that a cut-off value of sCr of 1.5mg/dl (133l mol/L)is useful to predict progression of AKI and consequently the prognosis in patients with cirrhosis [9,10].Thus,an sCr P 1.5mg/dl (133l mol/L)was the only pre-dictive factor for progression of the initial AKI stage (AKI stage at the first fulfilment of AKIN criteria)to a higher AKI stage during hospitalisation (peak AKI stage).Thereafter,it was also shown that the cut-off value of sCr P 1.5mg/dl (133l mol/L)was important when patients with peak AKI stage 1were considered.In fact,patients with AKI stage 1could be divided into two groups:those whose peak sCr did not exceed 1.5mg/dl (stage 1-A),whose short term mortality might be similar to those without AKI and in whom regression might occur more frequently [9,10];and those whose peak sCr exceeded 1.5mg/dl (stage 1-B),whose short term mortality was higher than those without AKI [9,10].Patients with AKI stage 2and 3have the highest mortality [8–10].However,whether these observations can be generalised to all hospitalised patients with cirrhosis should be assessed in future studies.In fact,as far as the impact of peak AKI stage 1on in-hospital mortality,it has recently been observed that in patients who developed AKI as a consequence of a bacterial infection,those with stage 1AKI and a final sCr 61.5mg/dl (133l mol/L)had a higher short term mortality compared to those without AKI [13,27].In addition,regarding regression of AKI stage,it has recently been observed (in non-hospitalised patients)that despite reso-lution of most AKI episodes in patients with advanced cirrhosis,a gradual and significant increase in sCr and a gradual reduc-tion in mean arterial pressure were observed during follow-up,associated with a significant reduction in mid-term survival compared with non-AKI patients [11].Indeed,the main lessonlearnt from the application of AKIN criteria is that even a small increase in sCr should be identified as early as possible for potential early interventions.Why do we need to change the conventional diagnostic criteria for AKI?A recent editorial on the topic of AKI in cirrhosis [28]asked the question:‘‘Should we change current definition and diagnostic criteria of renal failure in cirrhosis?’’Currently,studies on AKI in patients with cirrhosis showed that AKI defined by an abso-lute increase in sCr P 0.3mg/dl (26.5l mol/L)and/or P 50%from baseline is associated with a higher probability of the patients being transferred to the intensive care unit,a longer hospital stay,and an increased in-hospital as well as 90-day and mid-term mortality [8–15].On the basis of this evidence,all the experts agreed that it was time to change our current definition of renal failure by introducing a modified version of the KDIGO criteria for the diagnosis of AKI in patients with cirrhosis (Table 2).In the new ICA criteria for the diagnosis of AKI,the use of urine output as one of the criteria has been removed since it does not apply to patients with cirrhosis (ie,many patients are oliguric but have preserved kidney function)and it has never been investigated.Further,two other changes to the KDIGO criteria were adopted,namely:(1)a sCr within the last 3months before admission is considered a baseline value for the diagnosis of AKI when a value within the previous 7days is not available;and (2)the calculation of the baseline sCr by the reverse application of the Modification of Diet in Renal Disease (MDRD)formula,using an arbitrarily defined normal value of GFR of 75ml/min/1.73m 2,was not included.These two points are specifically discussed in the next section.Definition of baseline serum creatinine for the diagnosis of AKIThe first step in applying the ICA-AKI criteria is to define a baseline sCr.It has been stated that a renal disease process that results in a change in sCr over several weeks cannot be defined as AKI,Table 2.International Club of Ascites (ICA-AKI)new definitions for the diagnosis and management of AKI in patients withcirrhosis.AKI,acute kidney injury;RRT,renal replacement therapy;sCr,serumcreatinine.Position Paper970Journal of Hepatology 2015vol.62j 968–974although it may still represent an important clinical entity[7].Nev-ertheless,as with any clinical scenario,the timeframe for the defi-nition of AKI is somewhat arbitrary,and it is mainly suitable for the diagnosis of AKI in hospitalised patients using a sCr value on or after admission as baseline(hospital-acquired AKI).However,as in the general population,many patients with cirrhosis can develop AKI before admission to hospital(community-acquired AKI).Indeed,in previous studies where pre-admission values of sCr were used as baseline,the rate of AKI was higher than in those based on sCr on admission as baseline(47%vs.26%)[9,10].Thus, the diagnosis of community-acquired AKI on admission is related to two possible scenarios:(1)the patient with an available sCr value before admission;and(2)the patient without an sCr value before admission.The use of pre-admission values of sCr poses a great dilemma:how far back can a baseline value of sCr be retrieved and still be expected to be‘valid’for the definition of AKI?In the general population,it is reasonable to assume that sCr will be stable over several months or even years,so that an sCr obtained6months or even1year previously would reasonably reflect the patient’s premorbid baseline[7,29].In patients with cir-rhosis,an application of a more rigorous time frame for the defini-tion of AKI seems even more important.In fact,in these patients, impairment of renal function may progress gradually as they go from a compensated to a decompensated state and then more rap-idly as the decompensated state worsens.In addition,it should be considered that almost all patients with cirrhosis and ascites receive diuretics that can transiently impair renal function and, thus,increase sCr.Furthermore,it is important to emphasise the variability in sCr measurements from laboratory to laboratory or even within the same laboratory due to,for example,fluctuations in serum biliru-bin in patients with cirrhosis[30].A sCr obtained<7days before admission would be the ideal condition to use the ICA-AKI criteria, but this timeframe seems unfeasible in most cases.Thus,taking into account the previous experiences,we conclude that use of the last value of sCr within the last3months before admission seems more feasible[10,13].In this scenario,a community-acquired AKI may be diagnosed in the case of an increase in sCr P50%from the last sCr value(Table2).For patients without an available sCr before hospitalisation,the use of an estimated value of sCr as the baseline,calculated by the reverse application of the MDRD formula using a predetermined value of GFR(75ml/min), has been suggested for the general population of patients[7].How-ever,it is well known that the MDRD formula is inaccurate in the estimation of GFR in patients with cirrhosis,particularly in those with ascites[31].As a result,its reverse application in these patients may only add further biases.Preliminary data from the Padua centre suggest that a diagnosis of AKI based on an computed value of sCr as baseline identifies<25%of patients with a measured GFR<60ml/min on admission(Angeli P et al.,unpublished obser-vations).However,among patients without an sCr value before admission,one scenario deserves specific mention,and that is the case of the patient with an sCr P1.5mg/dl(133l mol/L)at admission.The management of such a patient should be based not only on a formal definition of AKI,but also on clinical judgment. Therefore,in a patient with impairment of renal function and a clearly identifiable precipitating event,it would be reasonable to assume that the renal failure represents AKI.Alternatively,the ini-tial sCr may be used as the baseline value,and if AKI criteria are met subsequently then the patient has AKI.This approach was com-monly used previously for the diagnosis of type1HRS[32].A new algorithm for the management of AKI in patients with cirrhosisAccording to the new ICA-AKI diagnostic criteria for AKI,we pro-pose a new algorithm for the management of AKI in patients with cirrhosis(Fig.1).The algorithm is based on the new staging of AKI.We recommend that patients with cirrhosis and ascites with initial ICA-AKI stage1should be managed as soon as possible with the following measures:1)Review drug chart:review of all medications(including over-the-counter(OTC)drugs),reduction or withdrawal of diuretictherapy,withdrawal of all potentially nephrotoxic drugs,vaso-dilators or non-steroidal anti-inflammatory drugs(NSAIDs).2)Plasma volume expansion in patients with clinically sus-pected hypovolaemia(with crystalloids or albumin orblood(in patients who had AKI as a result of gastrointesti-nal bleeding)according to clinical judgment).3)Prompt recognition and early treatment of bacterial infec-tions when diagnosed or strongly suspected.Patients who respond with a return of sCr to a value within 0.3mg/dl(26.5l mol/L)of the baseline value should be followed closely(assessment of sCr every2–4days during the hospitalisa-tion and checked as outpatients at least every2–4weeks during thefirst6months after the discharge)for early identification of potential new episodes of AKI[11].In those cases where there is progression of the AKI stage,the patients should be treated as patients who present with ICA-AKI stage2and3.This treat-ment should include the withdrawal of diuretics,if this had not been previously implemented,as well as the expansion of plasma volume with intravenous albumin at the dose of1g per kg bodyweight per day for two consecutive days,in order to treatJOURNAL OF HEPATOLOGYJournal of Hepatology2015vol.62j968–974971pre-renal AKI and to allow differential diagnosis of AKI (Box 1).The maximal dose per day of albumin should not exceed 100g as previously suggested [2].Further management of patients who do not respond to diuretic withdrawal and plasma volume expansion will obviously depend on the final diagnosis of the AKI type and,pragmatically,on the differential diagnosis between an HRS-AKI,an intrinsic AKI,and post-renal-AKI (Box 1).Thus,another major contribution of this new algorithm is to accelerate the differential diagnostic process among the dif-ferent types of AKI.However,it should be highlighted that several steps of this algorithm are not based on evidence but just on experts’opinion,and that it should be validated in future pro-spective clinical studies.In particular,in patients with AKI stage 1who do not respond but who do not progress to a higher stage,no consensus was obtained among the experts on the specific treatment.All experts agreed to treat these patients according to the right side of the algorithm when the final value of sCr is P 1.5mg/dl (133l mol/L).Some experts favour the treatment of patients with AKI stake 1and sCr <1.5mg/dl (133l mol/L)in the same way.However,most of the experts did not agree on this because they had concerns about the early use of vasoconstric-tors (terlipressin or norepinephrine or midodrine plus octreotide)in these patients in case of HRS-AKI.Thus,further clinical con-trolled studies are needed to address this relevant issue.In the meantime,decisions about the treatment of these patients should be taken on a case-by-case basis evaluating the aetiology of AKI,the presence or absence of precipitating factors,other organ fail-ures,or comorbid conditions that may contra-indicatetreatment.Why do we need to change the diagnostic criteria of HRS in the setting of AKI?A major critical point in the management of AKI in patients with decompensated cirrhosis is whether the diagnostic criteria of type 1HRS should be revised in light of the new definitions of AKI.The current criteria include a time interval (2weeks)over which sCr must double to a value >2.5mg/dl for the diagnosis of type 1HRS [1,2].A revision of these criteria is needed because the current definition of type 1HRS does not allow physicians to initiate potentially effective treatment,specifically vasoconstric-tors and albumin,until the sCr increases to P 2.5mg/dl.Since it has been observed that in patients with type 1HRS,a higher sCr at the beginning of treatment leads to a lower probability of response to terlipressin and albumin,the most investigated and effective treatment of type 1HRS [33,34],it seems prudent not to wait until the sCr increases beyond 2.5mg/dl before start-ing the treatment.According to the new proposed algorithm,when AKI is characterised by an initial ICA-AKI stage 2or 3or by progression of the initial stage despite general therapeutic measures,patients who meet all other diagnostic criteria of HRS provided by the previous definition [2]should receive vaso-constrictors and albumin,irrespective of the final value of sCr.This makes it possible to remove a barrier to the achievement of a pharmacological response that was linked to the rigid sCr cut-off value of >2.5mg/dl in the definition of type 1HRS.The potential advantage of the algorithm is that its application may allow earlier treatment of patients with type 1HRS,leading to a better outcome as compared with the current approach.How-ever,we lack studies where vasoconstrictors were used in the treatment of HRS with lower values of sCr,and caution should be exercised in the use of vasoconstrictors in these patients pend-ing further controlled trials.Nevertheless,all the experts agreed on the removal of a fixed cut-off value of sCr from the diagnostic criteria of HRS.This is the only change that they wanted to introduce in the current diag-nostic criteria for HRS.As a consequence,all the remaining criteria are maintained (Box 1).However,these criteria do not rule out the possibility of renal parenchymal damage [35].Thus,all the experts agreed on the potential role of new urinary biomarkers in the differential diagnosis of the different types of AKI in patients with cirrhosis.Several urinary biomarkers of tubular damage,such as neutrophil gelatinase-associated lipocalin (NGAL),kidney injury molecule-1(KIM-1)interleukin-18(IL-18),and liver fatty acid-binding protein (L-FABP),have been discovered in recent years.Preliminary experiences from Europe and the USA showed that the use of NGAL [36]and/or the combination of urinary bio-markers (NGAL,KIM-1,IL-18,L-FABP and albuminuria)[37]may be useful in the differential diagnosis of AKI in patients with cir-rhosis.These findings need to be confirmed in future studies.The removal of a fixed cut-off value of sCr from the diagnostic criteria of HRS in the setting of AKI has important implications in the management of these patients.Thus,there is a need to change the definition of response to the pharmacologic treatment of HRS.Full response will be defined by return of sCr to a value within 0.3mg/dl (26.5l mol/L)of the baseline value.Partial responses will be defined by a regression of at least one AKI stage with a fall in the sCr value to P 0.3mg/dl (26.5l mol/L)above the baseline value.Nevertheless,we should recognise that preliminary data suggest that even a partial decrease of sCr from baseline may be associated with improved short term survival,irrespectiveofPosition Paper972Journal of Hepatology 2015vol.62j 968–974whether or not the patient achieves HRS reversal(sCr<1.5mg/dl) [38].These data suggest that the degree of improvement in sCr may be more relevant than achieving afinite level of renal function.Conclusions and future perspectivesBased on the most recent studies on AKI in patients with cirrhosis and ascites,a new algorithm for the management of AKI in these patients is proposed for clinical practice and for future research. The main innovative aspects of this new algorithm are the following:The adoption of the main point derived from the applica-tion of the KDIGO criteria in the definition of AKI inpatients with cirrhosis,namely,use of dynamic changesof sCr.A more structured diagnostic process,in order to allow arational application of the therapeutic resources,avoidingpotentially undesirable consequences of overtreatment ofAKI as a result of indiscriminant use of KDIGO criteria.The definitive removal of any cut-off value of sCr from the criteria for diagnosis of HRS in the setting of AKI,butmaintaining the remaining previous criteria(Box1).Several issues remain to be addressed:(1)the impact of the management of AKI according to the new algorithm on the out-come of these patients should be tested in future prospective studies;and(2)the role of the new biomarkers of renal tubular damage in predicting the progression and prognosis of AKI,and in the differential diagnosis of the different types of AKI[36,37].In summary,the results of the latest consensus conference of the ICA introduces a new dynamic definition of AKI in patients with cirrhosis,on which a new treatment algorithm is based,rep-resenting a substantial change from the traditional criteria used until now in the definition of AKI and type1HRS.Financial supportPG:Research funding from Sequana Medical,Grifols SA;Consul-tancy Advisor to Ferring Pharmaceuticals;Competitive Public Grant Funding from:Fondos de Investigación Instituto de Salud CarlosIII(FIS12/0330)and Agència de Gestiód’Ajuts Universitaris i de Recerca(2014SGR708).MB:Consultant to CSL Behring GmbH,Baxter Healthcare SA;speaker to Behring GmbH,Baxter Healthcare SA,PPTA Europe.AG:Consultant to CSL Behring.RJ: Consultant to Ocera Therapeutics Inc,Conatus Pharmaceuticals Inc;Research grant from:Grifols Inc,Gambro AB,Sequana Med-ical AG,Norgine BV,Ocera Therapeutics Inc(the latterfive com-panies are all involved in research collaboration);Speaker to Grifols Inc;Norgine BV;Inventors of Ornithine Phenylacetate licensed by UCL to Ocera Therapeutics;UCL spinout Yaqrit which will in-licencefive of the following inventions in which R Jalan is the main inventor:YAQ001nanoporous carbons for prevention of gut bacterial translocation,UCL liver dialysis device,DASIMAR biomarker for liver failure,Neutrophil for test:biomarker for pre-dicting infection in decompensated cirrhotic patients,Urinary toll-like receptor4:for differential diagnosis of renal dysfunction of cirrhosis.SSL:Consultant to Ikaria and Grifols.PC:Lecturer to Baxter Healthcare SA,Kedrion,Grifols.VA:Received grant and research support from Grifols.Conflict of interestNone.Author’s contributionsOrganisation of the meeting:PA;Analysis of data from the litera-ture:PA,PG,FW,MB,TDB,AG,RM,RJ,SKS,SP,KM,SSL,FD,FS,PC, WRK,VA,GG;Drafting and writing the manuscript:PA,PG,FW, MB,SP,GG;Critical revision of data and manuscript revision:PA, PG,FW,MB,TDB,AG,RM,RJ,SKS,SP,KM,SSL,FD,FS,PC,VA,GG. References[1]Arroyo V,Gines P,Gerbes AL,et al.Definition and diagnostic criteria ofrefractory ascites and hepatorenal syndrome in cirrhosis.Hepatology 1996;23:164–176.[2]Salerno F,Gerbes A,Gines P,et al.Diagnosis,prevention and treatment of thehepatorenal syndrome in cirrhosis a consensus workshop of the Interna-tional Ascites Club.Gut2007;56:1310–1318.[3]Wong F,Nadim MK,Kellum JA,et al.Working Party proposal for a revisedclassification system of renal dysfunction in patients with cirrhosis.Gut 2011;60:702–709.[4]Angeli P,Sanyal A,Moller S,et al.Current limits and future challenges in themanagement of renal dysfunction in patients with cirrhosis:report from the International Club of Ascites.Liver Int2013;33:16–23.[5]Bellomo R,Ronco C,Kellum J,et al.Acute renal failure—definition,outcomemeasures,animal models,fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative(ADQI)Group.Crit Care2004;8:R204–R212.[6]Mehta RL,Kellum JA,Shah SV,et al.Acute Kidney Injury Network:report ofan initiative to improve outcomes in acute kidney injury.Crit Care2007;11: R31.[7]Kidney Disease:Improving Global Outcomes(KDIGO)Acute Kidney InjuryWork Group.KDIGO Clinical Practice Guideline for Acute Kidney Injury.Kidney Int2012;2(Suppl.):1–138.[8]Belcher JM,Garcia-Tsao G,Sanyal AJ,et al.Association of AKI with mortalityand complications in hospitalized patients with cirrhosis.Hepatology 2013;57:753–762.[9]Piano S,Rosi S,Maresio G,et al.Evaluation of the Acute Kidney InjuryNetwork criteria in hospitalized patients with cirrhosis and ascites.J Hepatol 2013;59:482–489.[10]Fagundes C,Barreto R,Guevara M,et al.A modified acute kidney injuryclassification for diagnosis and risk stratification of impairment of kidney function in cirrhosis.J Hepatol2013;59:474–481.[11]Tsien CD,Rabie R,Wong F.Acute kidney injury in decompensated cirrhosis.Gut2013;62:131–137.[12]de Carvalho JR,Villela-Nogueira CA,Luiz RR,et al.Acute kidney injurynetwork criteria as a predictor of hospital mortality in cirrhotic patients with ascites.J Clin Gastroenterol2012;46:e21–e26.[13]Wong F,O’Leary JG,Reddy KR,et al.New consensus definition of acutekidney injury accurately predicts30-day mortality in patients with cirrhosis and infection.Gastroenterology2013;145:1280–1288.[14]Altamirano J,Fagundes C,Dominguez M,et al.Acute kidney injury is an earlypredictor of mortality for patients with alcoholic hepatitis.Clin Gastroen-terol Hepatol2012;10:65–71.[15]Angeli P,Rodríguez E,Piano S,et al.Acute kidney injury and acute-on-chronic liver failure classifications in prognosis assessment of patients with acute decompensation of cirrhosis.Gut2014./10.1136/ gutjnl-2014-307526.[16]Sherman DS,Fish DN,Teitelbaum I.Assessing renal function in cirrhoticpatients:problems and pitfalls.Am J Kidney Dis2003;41:269–278.[17]Caregaro L,Menon F,Angeli P,et al.Limitations of serum creatinine level andcreatinine clearance asfiltration markers in cirrhosis.Arch Intern Med 1994;154:201–205.JOURNAL OF HEPATOLOGYJournal of Hepatology2015vol.62j968–974973。
急性肾损伤可预测肝硬化合并细菌感染的死亡率
急性肾损伤可预测肝硬化合并细菌感染的死亡率2013年12月发表在《Gastroenterology》的一项研究显示,针对肝硬化合并细菌感染的患者提出的新的急性肾损伤(AKI)共识定义比现行的较严格的定义能更准确地预测该患者人群的30天死亡率和其他不良结局。
NEJM Journal Watch 消化内科副主编Atif Zaman 教授(医学博士&公共卫生学硕士)对该项研究做了回顾与点评,内容如下:这个重新定义的新指标成功确诊了细菌感染住院患者中器官功能衰竭风险及死亡风险高的患者。
肾功能是肝硬化患者的一个强效预后指标。
即使肌酐小幅升高,也能反映该人群的肾功能不全情况。
最近,国际腹水协会和急性透析质量倡议(ADQI)小组提出,肝硬化患者的AKI应被重新定义为48 h内血清肌酐水平增加≥0.3 mg/dl,或过去6个月内血清肌酐水平相对稳定基线值增加50%.研究人员对新型AKI定义是否有助于预测肝硬化高风险患者(那些细菌感染住院患者)的预后进行了前瞻性评估。
研究纳入12家医学中心的337例肝硬化患者,其中166例符合AKI标准。
调整终末期肝病评分模型后,与无AKI患者相比,AKI患者的30天死亡率较高(34%vs.7%,P< 0.0001),住院时间较长(平均天数,17.8 vs.13.3,P<0.0001),新发器官功能衰竭率较高(77%vs.46%,P=0.0003)。
AKI患者中,56%的损害为暂时性,28%为持续性,16%需要透析治疗。
肾功能未恢复患者的死亡率为80%.评论研究结果表明,肝硬化合并感染患者的急性肾损伤和死亡率之间有密切联系。
即使肌酐有小幅升高0.3 mg/dL也与不良预后(包括新发器官功能衰竭,高死亡率)有关。
即使是肌酐轻度升高,临床医生也应采取措施如减少容量和使用利尿剂积极治疗。
后续研究应评估肝硬化合并感染患者AKI早期诊断及治疗的意义。
肝硬化合并急性肾损伤及肝肾综合征的治疗与预防在临床上,所谓终末期肝病多指失代偿期肝硬化,除了病因治疗外,其治疗主要针对各种并发症,但这些并发症往往治疗起来困难,患者生活质量和预后已受影响,并且很容易发生死亡。
肝硬化肝肾综合征型急性肾损伤的诊治进展
肝硬化肝肾综合征型急性肾损伤的诊治进展
宋廷雪;祁兴顺;高帆;郭晓钟
【期刊名称】《临床肝胆病杂志》
【年(卷),期】2017(033)003
【摘要】急性肾损伤(AKI)是一种常见的肝硬化并发症,其主要表现为血肌酐迅速升高、肾小球滤过率降低、少尿或无尿.1型肝肾综合征(HRS-1)是AKI的一种特殊类型,未经治疗的HRS-1死亡风险极高,尽早诊断及治疗尤为重要.归纳了肝硬化AKI 及HRS-AKI的最新诊断标准,并总结了有关HRS-1治疗的临床研究进展.
【总页数】5页(P572-576)
【作者】宋廷雪;祁兴顺;高帆;郭晓钟
【作者单位】辽宁中医药大学研究生院,沈阳110032;中国人民解放军沈阳军区总院消化内科,沈阳110840;中国人民解放军沈阳军区总院消化内科,沈阳110840;3解放军第二○二医院医务处,沈阳110003;辽宁中医药大学研究生院,沈阳110032;中国人民解放军沈阳军区总院消化内科,沈阳110840
【正文语种】中文
【中图分类】R575.2
【相关文献】
1.肝硬化急性肾损伤诊治的研究进展 [J], 雷蕾;张虎
2.肝硬化急性肾损伤诊治进展 [J], 于乐成;汪茂荣;何长伦
3.肝硬化低钠血症与肝肾综合征的诊治进展 [J], 曾欣;谢渭芬
4.肝硬化肝肾综合征的诊断与治疗新进展 [J], 王利娜;姜慧卿
5.肝硬化肝肾综合征的临床进展 [J], 李晨; 李文刚; 徐小元
因版权原因,仅展示原文概要,查看原文内容请购买。
急性肾损伤早期生物标志物研究进展
急性肾损伤早期生物标志物研究进展
付锴;赵久阳;滕思远
【期刊名称】《大连医科大学学报》
【年(卷),期】2016(038)004
【摘要】急性肾损伤(acute kidney injury,AKI)的早期诊断对延缓病情进展,改善患者预后具有重要的意义,但目前对AKI的诊断仍然没有早期敏感特异的指标.本文通过对中性粒细胞明胶酶相关载脂蛋白、肾损伤分子1、肝脏型脂肪酸结合蛋白等AKI早期标志物基本特征、基础与临床研究、应用前景等方面的阐述,探讨其在AKI早期诊断、功能分级及预后判断的价值.
【总页数】5页(P392-396)
【作者】付锴;赵久阳;滕思远
【作者单位】大连医科大学附属第二医院肾内科,辽宁大连116027;大连医科大学附属第二医院肾内科,辽宁大连116027;大连医科大学附属第二医院肾内科,辽宁大连116027
【正文语种】中文
【中图分类】R692
【相关文献】
1.肝硬化并发急性肾损伤早期诊断生物标志物研究进展 [J], 欧进军;韩焕钦;郑伟强
2.对比剂相关急性肾损伤早期诊断生物标志物的研究进展 [J], 王淑霞;韩洁
3.心脏术后相关性急性肾损伤早期生物标志物研究进展 [J], 陈志强
4.新型生物标志物在危重症患者急性肾损伤早期诊断中的研究进展 [J], 常雪妮;董晨明
5.急性肾损伤早期诊断生物标志物的研究进展 [J], 丁丰;沈华江
因版权原因,仅展示原文概要,查看原文内容请购买。
肝硬化急性肾损伤新标准(ICA2015)下治疗应答和预后的回顾性分析及影响因素研究
肝硬化急性肾损伤新标准(ICA2015)下治疗应答和预后的回顾性分析及影响因素研究尹伟;李成忠;邹多武【期刊名称】《肝脏》【年(卷),期】2018(023)003【摘要】目的观察肝硬化急性肾损伤(AKI)新诊断标准和治疗管理流程下(ICA2015)治疗应答和预后的情况,并分析相关的影响因素.方法回顾性分析2016年7月至2017年6月在海军军医大学长海医院感染科住院的220例肝硬化失代偿期患者.收集住院期间的数据,评估疗效及短期预后.通过Logistic回归和ROC曲线分析明确AKI及预后的影响因素.结果共纳入肝硬化(失代偿期)患者220例,住院期间AKI的发生率为27.7%(61/220).1期AKI患者39例,37例有治疗应答,33例预后良好,2例患者出院后再发AKI;2期AKI患者19例,16例有治疗应答,12例预后良好,2例患者出院后再发AKI;3期AKI患者3例,1例治疗应答(完全应答),但均于住院期间或出院3个月内死亡.并发AKI的影响因素为:MELD评分、基线SCr、是否存在感染;并发AKI的患者预后的影响因素为:TBil、Alb、INR、AKI治疗应答;但肝硬化(失代偿期)患者的整体预后仅与 TBil、ALT、并发症的数量相关.结论 ICA 更新的肝硬化急性肾损伤诊断和管理流程提升了诊断的敏感度和治疗应答的比例,使以往忽略的部分患者得到了及时的处理,改善了预后,但仍存在较多的问题.【总页数】5页(P201-205)【作者】尹伟;李成忠;邹多武【作者单位】200433 上海海军军医大学长海医院感染科;200433 上海海军军医大学长海医院感染科;200433 上海海军军医大学长海医院感染科【正文语种】中文【相关文献】1.急性肾损伤治疗48小时应答与否对HBV相关慢加急性肝衰竭短期预后的影响[J], 翟兴冉; 胡瑾华; 许祥; 陈婧; 穆秀颖; 童晶晶; 苏海滨; 刘晓燕; 关崇丹; 王宇2.肝硬化急性肾损伤发病风险和治疗应答影响因素的前瞻性研究 [J], 尹伟;李成忠3.基于倾向评分匹配法的高血压对妊娠相关性急性肾损伤预后影响的回顾性队列研究 [J], 陈文航;李慧慧;周权;薛静4.HBV相关慢加急性肝衰竭和失代偿期肝硬化患者急性肾损伤预后影响因素分析[J], 王芳;徐杰;杨霞霞;刘宇宏5.肝硬化患者食管静脉曲张硬化治疗术预后的影响因素研究 [J], 刘远志;孙亚男;李鹏;吴燕京;武永乐;曾庆环;张世斌因版权原因,仅展示原文概要,查看原文内容请购买。
肝硬化并发急性肾损伤临床管理现状与挑战
肝硬化并发急性肾损伤临床管理现状与挑战蒋莹莹;丁惠国【期刊名称】《实用肝脏病杂志》【年(卷),期】2022(25)6【摘要】肾损伤是肝硬化常见的并发症或合并症之一,与患者的预后密切相关。
传统上,将血清肌酐(serum creatinine,sCr)≥1.5 mg/dl定义为肾功能障碍,作为1型和2型肝肾综合征诊断的重要依据,其局限性在于肝硬化患者早期肾功能损伤易被漏诊,且器质性肾损伤或慢性肾病患者不能正确地归类。
近年来,根据肾功能受损时间长短,将其分为急性肾损伤(acute kidney injury,AKI)、亚急性(即急性肾脏病,acute kidney diseases,AKD)和慢性肾脏病(chronic kidney disease,CKD)[1],包括了功能性和器质性肾损伤。
按照肝硬化并发肾损伤的新概念,肝肾综合征(hepatorenal syndrome,HRS)的病理生理特征不仅包括内脏血管扩张,肾血流量减少所致的功能性肾功能障碍,还包括了全身炎症反应等所致的器质性肾损伤。
基于这些理论,认为HRS纯粹是一种“功能性”肾功能衰竭的观点是不可靠的,这一概念对于指导肝硬化并发肾损伤的治疗和预后评估具有重要的临床意义。
【总页数】4页(P764-767)【作者】蒋莹莹;丁惠国【作者单位】首都医科大学附属北京佑安医院【正文语种】中文【中图分类】R69【相关文献】1.肝硬化并发急性肾损伤患者的临床预后及影响因素2.乙型肝炎肝硬化并发急性肾损伤患者临床特点及其危险因素分析3.乙型肝炎肝硬化患者并发急性肾损伤危险因素分析4.肝硬化并发急性肾损伤的非血管舒张机制的研究进展5.失代偿肝硬化患者并发急性肾损伤的危险因素及预测价值评估因版权原因,仅展示原文概要,查看原文内容请购买。
肝硬化急性肾损伤要点(全文)
肝硬化急性肾损伤要点(全文)2021年6月,意大利肝病学会(AISF)联合意大利肾病学会(SIN)共同发布了肝肾疾病意见书。
在生理和病理情况下,肝脏和肾脏是以相互作用的方式紧密相连的。
该指南主要介绍了肝肾疾病之间相关性的最新概况,根据GRADE系统对证据质量和推荐强度进行分级。
本文节选了肝硬化急性肾损伤(AKI)这一部分内容,通过指南提出的9个问题及相关推荐建议,帮助大家了解这一疾病。
肝硬化AKI的定义是什么?1.在肝硬化患者中,AKI的诊断基于国际腹水俱乐部(ICA)定义的改善全球肾脏病预后组织(KDIGO)标准[48h内血清肌酐(sCr)升高≥0.3 mg/dL (26.5 μmol/L);或7天内sCr升至≥1.5倍基线值;和/或尿量≤0.5 mL/kg B.W.≥6 h],AKI的诊断同样基于sCr的微小变化(48h内sCr较基线增加≥0.3 mg/dL,或3个月内sCr较基线增加≥50%)(1A)。
2.最近,有证据表明,排尿量(尿量<0.5 mL/kg/h,持续≥6h)在识别AKI患者和预测重症肝硬化患者预后方面具有显著优势(2B)。
3.与一般人群相同,肝硬化患者可发生各种类型的AKI,包括:肾前性、肾性和肾后性AKI。
此外,肝硬化患者可发生特定类型的AKI,即肝肾综合征(HRS)-AKI(1A)。
4.HRS-AKI通过排除并基于修订的ICA标准进行诊断(1B)。
表1 肝硬化HRS-AKI的诊断标准肝硬化AKI的分期是什么?1.AKI分期应基于ICA定义的KDIGO分期系统进行区分(1A):AKI 1期:sCr较基线升高≥0.3 mg/dL(26.5 μmol/L)或sCr较基线升高≥1.5-2倍;AKI 1期根据诊断时的sCr值分为1A期(sCr<1.5 mg/dL)和1B期(≥1.5 mg/dL);AKI 2期:sCr较基线升高>2-3倍;AKI 3期:sCr较基线升高>3倍或sCr≥4.0 mg/dL(353.6 μmol/L)伴sCr急性升高≥0.3 mg/dL(26.5 μmol/L)或开始肾脏替代治疗(RRT)。
肾损伤分子-1、胱抑素C和尿肌酐联合检测对先心病体外循环术所致急性肾损伤的诊断价值
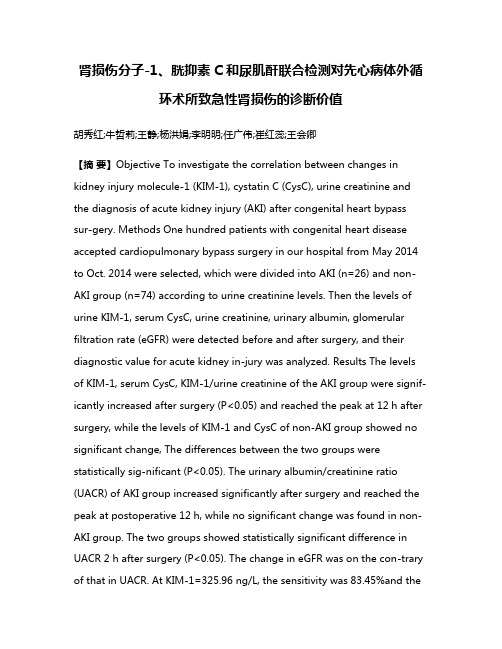
肾损伤分子-1、胱抑素C和尿肌酐联合检测对先心病体外循环术所致急性肾损伤的诊断价值胡秀红;牛哲莉;王静;杨洪娟;李明明;任广伟;崔红蕊;王会卿【摘要】Objective To investigate the correlation between changes in kidney injury molecule-1 (KIM-1), cystatin C (CysC), urine creatinine and the diagnosis of acute kidney injury (AKI) after congenital heart bypass sur-gery. Methods One hundred patients with congenital heart disease accepted cardiopulmonary bypass surgery in our hospital from May 2014 to Oct. 2014 were selected, which were divided into AKI (n=26) and non-AKI group (n=74) according to urine creatinine levels. Then the levels of urine KIM-1, serum CysC, urine creatinine, urinary albumin, glomerular filtration rate (eGFR) were detected before and after surgery, and their diagnostic value for acute kidney in-jury was analyzed. Results The levels of KIM-1, serum CysC, KIM-1/urine creatinine of the AKI group were signif-icantly increased after surgery (P<0.05) and reached the peak at 12 h after surgery, while the levels of KIM-1 and CysC of non-AKI group showed no significant change, The differences between the two groups were statistically sig-nificant (P<0.05). The urinary albumin/creatinine ratio (UACR) of AKI group increased significantly after surgery and reached the peak at postoperative 12 h, while no significant change was found in non-AKI group. The two groups showed statistically significant difference in UACR 2 h after surgery (P<0.05). The change in eGFR was on the con-trary of that in UACR. At KIM-1=325.96 ng/L, the sensitivity was 83.45%and thespecificity was 71.03%, with maxi-mum area under ROC curve. Combined detection of KIM-1, CysC, urine creatinine had maximum area under ROC. Conclusion In the diagnosis of AKI due to congenital heart bypass surgery, combined detection of kidney injury molecule-1, serum cystatin C and urine creatinine may eventually increase the sensitivity and specificity to improve diagnostic accuracy and reduce misdiagnosis rate.%目的:探讨尿肾损伤分子-1(KIM-1)、血清胱抑素C (CysC)和尿肌酐对先心病体外循环术所致急性肾损伤(AKI)的诊断价值。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
王帅, 等. 2 0 1 5年国际腹水俱乐部共识建议: 1 9
准值得探讨。由于临床上肝硬化患者尿量采集的不准确性, S C r 的动态变化则成为诊断 A K I 的关键。对肝硬化患者来说, 以上这些新标准和常规标准的主要区别在于: ( 1 ) S C r 的绝对 值增加受到重视;( 2 ) 放弃了 S C r . 5m g / d l ( 1 3 3μ m o l / L ) ≥1 3 ) 以相对较长时间段 S C r 变化为基础建立 这一临界值标准; ( 了新的 A K I 分期系统, 并将此时间段设定为 7d , 从而能够评 估A K I 分期的进展( 改良自 A K I N标准) 和恢复( 表1 ) 。对于 大样本的肝硬化住院患者( 包括重症监护病房患者和垂危患 者) , A K I N标准已成为其病死率的良好预测因子。最近研究 K I N标准 发现, 对于收住普通病房的肝硬化患者, 如果依据 A 确诊 A K I , 其病死率显著升高。并且, 患者 A K I 分期的进展( 如 从 1期到 2期或 2期到 3期) 与其病死率增加密切相关。2 0 1 1 年I C A建议, 比较 A K I 常规标准和新标准对肝硬化患者预后 判断的准确性对于 A K I 管理系统的建立非常重要。 S C r 临界值 1 . 5m g / d l ( 1 3 3μ m o l / L )仍然得到许多 但是, 临床医师的认可。最近两项前瞻性研究发现, S C r 达到临界值 1 . 5m g / d l ( 1 3 3μ m o l / L ) 对预测 A K I 的进展和肝硬化患者预后 很有价值。因此, S C r . 5m g / d l ( 1 3 3μ m o l / L ) 成为由最初 A K I ≥1 分期( 采用 A K I N标准开始评估时的 A K I 分期) 进展至较高 A K I 分期( A K I 的最高分期) 的唯一预测因子。这也提示当患者 S C r 处于 A K I 1 期的最高点时, 此临界值是非常重要的。实际上, A K I 1 期的患者可以分成 2组: S C r 峰值未超过 1 . 5m g / d l 组 ( s t a g e 1 - A ) , 其短期病死率与未发生 A K I 的患者接近, 并且其 A K I 常常可以恢复; S C r 峰值超过 1 . 5m g / d l 组( s t a g e 1- B ) , 其 短期病死率高于未发生 A K I 的患者。 A K I 2期和 3期的患者 病死率最高。但是, 这些结果是否适用于所有肝硬化住院患者 仍需进一步研究。就 A K I 1期对住院患者病死率的影响而言, K I 的患者, 合并 1期 A K I 最近有学者研究了因细菌感染导致 A 且最终 S C r . 5m g / d l ( 1 3 3μ m o l / L ) 患者的短期病死率比未 ≤1 合并 A K I 的患者要高。另外有研究( 非住院患者) 发现, 尽管 进展期肝硬化患者中大多数的 A K I 发作能够恢复( A K I 分期 下降) , 但随访期间患者 S C r 逐渐并显著升高, 平均动脉压逐渐 K I 的患者相比, 其中期生存率也显著降低。 降低, 与未发生 A K I N标准的应用提示, 即使是 S C r 的轻微升高, 都要 因此, 对A 及早发现并给予尽可能的早期干预。 2 为什么要改变 A K I 的常规诊断标准? 近期一篇关于肝硬化患者并发 A K I 的述评中提出: “ 是否 应该对目前肝硬化合并肾衰竭的定义及诊断标准作出改变? ” 目前对肝硬化患者合并 A K I 的研究表明, 如果以 S C r 绝对值升 高≥0 . 3m g / d l ( 2 6 . 5μ m o l / L ) 和( 或) 较基线值升高 ≥5 0 %为 标准定义 A K I , 则患者 A K I 的发生与其转入重症监护病房比率、 住院时间、 住院率、 9 0d 和中期病死率密切相关。在此证据的 基础上, 专家一致同意应该对肾衰竭的概念进行更新, 新标准 应以肝硬化并发 A K I 的K D I G O标准为基础来建立( 表2 ) 。在 关于 A K I 诊断的 I C A新标准中, 已经剔除了尿排出量指标, 原
K e yw o r d s : l i v e r c i r r h o s i s ;k i d n e yf a i l u r e ,a c u t e ;d i a g n o s i s ;g u i d e l i n e s
急性肾衰竭( a c u t ek i d n e yf a i l u r e ,A R F ) 是失代偿期肝硬 化患者的常见并发症之一。肝硬化患者肾衰竭的诊断标准于 1 9 9 6年颁布, 此后又多次进行更新。在这些标准中, A R F被定 义为血清肌酐( S C r ) 升高基线水平的 5 0 % 以上, 并最终升至 1 5m g / d l ( 1 3 3μ m o l / L ) 以上。然而, 将失代偿期肝硬化患者肾 衰竭的 S C r 临界值定为 1 . 5m g / d l ( 1 3 3μ m o l / L )争议颇多。而 且, 除了Ⅰ型肝肾综合征( h e p a t o r e n a l s y n d r o m e ,H R S ) 以外, 急、 慢性肾衰竭的时限界定也未明确。同时, 非肝硬化患者 A R F的 新标准已被提议并确定, 其命名亦被急性肾损伤( A K I ) 所代替。 K I 近年来, 这些新标准也被部分专家推荐应用于肝硬化患者 A 的诊断。鉴于此, 国际腹水俱乐部( I n t e r n a t i o n a l C l u bo f A s c i t e s , I C A ) 于2 0 1 2 年1 1 月在意大利威尼斯召开共识会议, 主题即为 确定肝硬化患者 A K I 的新定义。由于专家在此问题的关键点 上意见不一, 他们通过在线或会议等方式讨论了 2 年之久。 本文介绍了肝硬化患者 A K I 诊断及治疗的最新推荐建议, 此 建议具有充分的科学证据支持, 也得到了绝大多数专家的认可。 1 肝硬化患者 A K I 的诊断标准和应用 肾小球滤过率( g l o m e r u l a r f i l t r a t i o nr a t e ,G F R ) 急性显著下 降即为 A K I 。一直以来, S C r 一直是反映 A R F ( 有或无肝硬化) 患者肾功能最实用的生物标志物。但是, 由于受体质量、 种族、 年龄及性别等因素影响, S C r 作为肾功能生物标志物在临床上 具有许多局限性。对于肝硬化患者来说, S C r 的应用还受到下 列因素的影响: ( 1 ) 由于患者的肌肉萎缩, 导致肌酸来源的肌 酐生成减少; ( 2 ) 肾小管分泌肌酐的功能增强;( 3 ) 肝硬化患 C r 被稀释; ( 4 )胆红素的升高对肌 者容量分布的增加可能使 S 酐的含量测定造成影响。因此, 依据 S C r 水平可能会对肝硬化 患者的 G F R或肾功能估计过高。同时, 把S C r 1 . 5m g / d l ( 1 3 3 m o l / L )作为肝硬化 A K I 的固定临界值值得商榷, 其中涉及 μ 首先是 S C r 值1 . 5m g / d l ( 1 3 3μ m o l / L ) 以下 2个关键性问题: 通常表示 G F R明显下降( 低至 3 0m l / m i n ) ; 另外, 此固定临界值并 未考虑到过去数天或数周 S C r 的动态变化情况, 而区分急性和慢 C r 值不足以确诊 性肾损伤需要了解这些情况。由于采用单一的 S A K I , 其动态标准确定为 S C r 急性升高并超过基线水平的 5 0 %, 并 最终≥1 . 5m g / d l ( 1 3 3μ m o l / L ) 。此标准在几项关于肝硬化患者 ) 。根据此标准诊断的 A K I 已成为肝硬 的临床研究中被采用( 表1 化住院患者病死率的有效预测因子。近年来, 上述标准已被推荐 R F ( 目前称作 A K I ) 的诊断。特别是两个独 用于非肝硬化患者 A 立的研究团队分别发布了意见一致的 A K I 定义: 急性透析质量倡 议工作组( a c u t e d i a l y s i s q u a l i t y i n i t i a t i v e g r o u p , A D Q I ) 颁布的肾功 r i s k ,i n j u r y ,f a i l u r e ,l o s s 能风险、 损伤、 衰竭、 丧失及终末期肾病( o f r e n a l f u n c t i o na n de n d - s t a g e r e n a l d i s e a s e ,R I F L E ) 标准; 急性肾 损伤网络( a c u t e k i d n e y i n j u r y n e t w o r k , A K I N ) 工作组颁布的 A K I N 标准( 表1 ) 。新近有专家建议, 将A K I N标准的部分内容[ 4 8h 内 S C r 升高 0 . 3m g / d l ( 2 6 . 5μ m o l / L ) 或升高≥基线值 5 0 %, 并且
d o i : 1 0 . 3 9 6 9 / j . i s s n . 1 0 0 1- 5 2 5 6 . 2 0 1 5 . 0 7 . 0 0 5 收稿日期: 2 0 1 5- 0 5- 2 6 ; 修回日期: 2 0 1 5- 0 5- 3 0 。 作者简介: 王帅( 1 9 7 3- ) , 男, 副主任医师, 主要从事慢性肝病的防 治研究。
- 1 - 1 尿量 < 0 . 5m l ·k g ·h 达 6h以上] 和R I F L E标准的一部
分( S C r 7d 内升高 ≥ 基线值 5 0 % 或者 G F R下降 > 2 5 %, 并且
- 1 - 1 0 . 5m l ·k g ·h 达 6h以上) 结合起来, 从而形成了 尿量 <
关键词: 肝硬化; 肾功能衰竭, 急性; 诊断; 指南 中图分类号: R 5 7 5 . 2 文献标志码: B 文章编号: 1 0 0 1- 5 2 5 6 ( 2 0 1 5 ) 0 7- 1 0 1 8- 0 5