PPI VS 氯吡格雷 ——当常规遇上指南
急性冠脉综合征非血运重建患者抗血小板治疗中国专家共识
服用阿司匹林和(或)氯吡格雷时,不推荐常规服用质子泵抑制剂(PPI)以预防胃肠道不良反应,对于高胃肠道风险的患者可考虑更换其他抑酸药如组胺H2受体拮抗剂;对于有消化道溃疡需要服用PPI的ACS患者,建议由心内科、消化内科以及普内科医师共同评估,制定治疗方案。
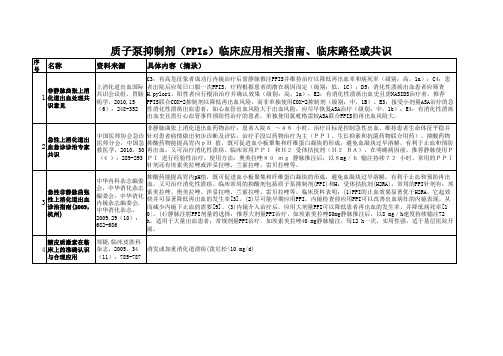
2005年CPACS (中国急性冠脉综合征临床路径研究) 63%ACS患者接受了单纯药物治疗
63%
PCI或CABG
52%
PCI或 CABG
单纯药物 治疗
3级医院
单纯药物治疗
80%
PCI或CABG
2级医院
入组2,823ACS患者
入组1731ACS患者
入组1092ACS患者
Ruilin G, et al. Heart published online 11 Oct 2007; doi:10.1136/hrt.2007.119750
ACS的病理生理基础
2、急性血栓形成 男性68%首发AMI和心脏猝死 出现在冠脉狭窄<50%的病例。 女性50%首发AMI和心脏猝死
ACS的病理生理基础
一旦斑块破裂,便激活血小板和凝血系统,在破裂斑块的基础上形成富含血小板的止血血栓。 当损伤严重,则在血小板血栓的基础上形成以纤维蛋白和红细胞为主的闭塞性血栓—红色血栓,冠脉血流完全中断,ECG一般表现为ST段抬高。 当损伤较轻,形成的血栓为非闭塞性,以血小板为主—白色血栓。形成白色血栓时,冠脉血流没有完全中断,可以冲击血栓而栓塞末梢小动脉,表现为UA或NSTEMI。
氯吡格雷及其治疗建议
NSTEACS患者中不准备进行早期(5d内)诊断性冠脉造影或冠状动脉旁路移植术(CABG)的患者,立即给予氯吡格雷负荷剂量300mg,继以75mg/d。除非有高出血风险,建议持续应用12个月。 ST段抬高心肌梗死(STEMI)患者无论是否采用纤溶治疗,应该给予氯吡格雷75mg/d,至少持续14d,并且建议长期治疗,如1年。如患者<75岁给予负荷剂量300mg(75岁以上和出血高危的患者不用负荷剂量)。 正在服用氯吡格雷,拟行择期CABG的患者,建议术前停用氯吡格雷至少5d,除非急诊手术。
抗凝药物消化道出血指南
抗凝药物消化道出血指南
指南1:消化道出血是抗血小板治疗最常见的不良反应,应该基于出血风险合理选择,重视防范。
指南2:对于有消化道出血风险的抗栓治疗患者,推荐常规联用PPI和抗血小板药物。
指南3:不同PPI对氯吡格雷抗血小板作用的影响存在差异,但尚无临床预后终点研究证据。
与氯吡格雷合并用药时,不推荐特定的PPI。
PPI对替格瑞洛抗血小板作用无影响。
指南4:新型DOACs胃肠道出血风险较华法林未见明显降低,长期用药患者应该重视防范消化道出血;如需抗凝联合抗血小板治疗应更严格掌握适应证,并重视预防出血。
指南5:不建议对血小板计数正常的消化道出血患者输注血小板。
指南6:消化道出血后输血应该采用限制性输血;对于血压下降的大量活动性出血患者,可能需要更个体化的输血策略。
2023 ESC指南老年人抗血栓药物治疗方案具体内容
2023 ESC指南老年人抗血栓药物治疗方案具体内容1.建议采用药物和非药物治疗策略来提高老年人的治疗依从性,例如减少药物处方、使用单片复方制剂、提醒工具和教育干预。
研究显示,减少不恰当的多药治疗,使用单片复方制剂可提高约30%的用药依从性,并减少不良心血管事件,且不会显着增加大出血事件风险。
2.尽管抗栓治疗可使老年心血管疾病(CVD)患者净临床获益,但血栓风险随年龄增加而增加,因此建议老年患者进行系统性出血风险评估。
3.对于CVD二级预防,长期低剂量阿司匹林与不使用抗血小板药物的获益与风险概况在老年人和年轻人中均有优势。
4.与年轻患者相比,≥75岁老年患者进行抗血小板治疗所导致的致残或致命性出血的长期风险升高,且50%的出血发生在上消化道。
因此,建议常规应用质子泵抑制剂(PPI)进行治疗。
对于进行氯吡格雷治疗的患者,指南倾向于推荐泮托拉唑或雷贝拉唑,避免使用奥美拉唑或艾司奥美拉唑。
5.对于CVD一级预防,在年龄≥70岁,无动脉粥样硬化性心血管疾病(ASCVD)证据,且预计不良心血管事件(MACE)<1%的人群中,不推荐常规应用阿司匹林治疗。
CVD风险较高、出血风险不高的老年患者或可在阿司匹林一级预防中获益。
6.ACS和/或PCI后,抗栓治疗的疗效和安全性评估有助于促进P2Y12抑制剂的选择。
对于年龄≥75岁的行PCI的ACS患者,可进行氯吡格雷或降低剂量的普拉格雷(5 mg/d)治疗;行PCI的慢性冠状动脉综合征(CCS)患者可进行氯吡格雷治疗。
对于年龄≥75 岁的患者,通常不建议在PCI后进行双联抗血小板治疗(DAPT)>12个月,高出血风险患者可缩短至1个月。
7.除外ST段抬高心肌梗死(STEMI)患者,合并ACS和/或PCI的老年患者,在进行血管造影前避免应用P2Y12抑制剂是合理的,患者可进行抗血小板药物降阶治疗;或在DAPT 1-3个月后进行单联抗血小板治疗(如阿司匹林、氯吡格雷、替格瑞洛),以降低出血风险。
阿司匹林和氯吡格雷临床应用比较
阿司匹林和氯吡格雷临床应用比较1.多个最新卒中指南推荐,卒中急性期尽早给予阿司匹林治疗卒中发病24--48小时内给予口服阿司匹林(起始剂量325mg)氯吡格雷对急性缺血性卒中的疗效尚不明确,对于不符合溶栓适应证,且无禁忌的缺血性脑卒中患者,应在发病后尽早给予口服阿司匹林150—300mg/d。
急性期后可改为预防剂量,50-150mg/d2.卒中急性期双联抗血小板应用探讨缺血性卒中分型及分布,TIA/小卒中双联抗血小板应用大动脉粥样硬化型卒中双联抗血小板应用心源性卒中双联抗血小板应用。
3.TIA的定义TIA是一种血管原因所致的突发性局灶性神经功能障碍,(脑.脊髓.视网膜)持续时间小于24h。
影像学未见梗死病灶。
4.TIA短期卒中风险评估年龄>60岁1分血压:收缩压>140mmh,舒张压>90mmhg1分临床症状单侧无力2分不伴有无力的言语障碍1分症状持续时间>60分钟2分10-59分钟1分糖尿病1分5.CHANCE研究设计小卒中/TIA{首剂:阿司匹林75—300mg-----阿司匹林75mg/d&&&7&&首剂:氯吡格雷300mg---氯吡格雷+阿司匹林,氯吡格雷75mg/d}主要疗效点,缺血或出血性脑卒中,次要疗效重点卒中,脑梗死血管性死亡复合终点。
实际双抗治疗21天。
氯吡格雷单用3个月。
小卒中/TIA患者,早起双抗治疗较单抗治疗减低新发血管事件-----下降31%6.卒中/STA二级预防新增推荐*对主要颅内动脉重度狭窄(70%---90%)的近期卒中或TIA患者(30天以内)推荐阿司匹林联用75mg/d的氯吡格雷治疗21天*主要颅内动脉中度狭窄,(50%---69%)的卒中或TIA患者,不建议使用血管成形及支架置入术,因药物治疗卒中风险较低*主要颅内动脉重度狭窄,(70%---90%)的卒中或TIA患者,不建议支架作为初始治疗,即使对服用抗血栓药物期间,发生卒中和TIA的患者。
PPI相关指南
制剂(PPl)治疗。
11
慢性胃炎诊疗指 南
第三次全国幽门
12 螺杆菌感染若干
问题共识报告
中华中医药学会, 中国中医药现代远 程教育,2011,9 (10):123-125
中成药:肝气犯胃证①气滞胃痛冲剂,冲服,1次5次,1日3次;②胃苏冲剂,冲服,1次5g,1日3次。寒邪客胃证,胃 气止痛丸,口服,1次6g,1日3次。饮食伤胃证①加味保和丸,口服,1次6g,1日3次; ②越鞠保和丸,口服,1次6g,1日3次。湿热阻胃证:肠胃康冲剂,冲服,1次1包,1日3次。瘀血停胃证:脾胃虚寒 证:①理中丸,口服,1次9g,1日2次;②温胃舒胶囊,口服,1次4粒,1日2次。胃阴亏虚证:养胃舒胶囊,口服,1 次4粒,1日2次。其他治法:验方,针刺、推拿和刮痧。
疗程7d或10d(对于耐药严重的地区,可考虑适当延长至14d,但不要超过14d)。服药方法:PPI早晚餐前服用,抗生素餐
后服用。PPI :目前有埃索美拉唑( E)20mg、雷贝拉唑(R)10mg、兰索拉唑(L)30 mg、奥美拉哇(O)20 mg和泮托拉唑
(P)40 mg,,RBC(雷 尼替丁拘椽酸铋)350m g.C:克拉霉素;A:阿莫西林;M:甲硝唑;F:呋喃唑酮;T:四环素;L:左氧氟沙
星;B:铋剂(构椽酸铋钾、果胶铋等)。
中国消化不良的
13 诊治指南( 2007
大连)
中华医学会消化病 2.抑酸剂:目前广泛应用于FD的治疗,适用于非进餐相关消化不良中以上腹痛、烧灼感为主要症状者。常用抑酸剂包括
学分会胃肠动力学 H2受体拮抗剂(H2RA) 和质子泵抑制剂(PPI) 两大类。H2RA 可有效治疗FD, 常用药物有西米替丁、雷尼替丁和法莫替
针剂还有埃索美拉唑或泮妥拉唑、兰索拉唑、雷贝拉唑等。
缺血性卒中二级预防:阿司匹林vs.氯吡格雷

缺血性卒中二级预防:阿司匹林vs.氯吡格雷北京时间2009年6月21日下午,中国规模最大的卒中会议——天坛国际脑血管病会议,就“缺血性卒中二级预防抗血小板药物应首选氯吡格雷还是阿司匹林”组织了一场辩论,辩论双方阵容强大,各由4位心脑血管领域著名专家辩手组成,就这一论题充分阐述了自己的观点并分析了对方观点的矛盾之处。
在愉悦而充满火药味的现场,本报记者亲历了整个辩论过程,现将最精彩部分呈现给读者。
套用正方辩手之一的高旭光教授的一句话(医师报,第118期,22版),“科学研究提倡异想天开,但更要脚踏实地!有想法是可以的,但一定要有客观可信的证据。
”主持人:王拥军姜卫剑甲方:缺血性卒中二级预防抗血小板药物应首选氯吡格雷乙方:缺血性卒中二级预防抗血小板药物应首选阿司匹林甲方一辩:James WangPK 乙方一辩:David Wang甲方二辩:张微微乙方二辩:史旭波甲方三辩:高旭光乙方三辩:赵虹茹甲方一辩:新药之所以能够存在,必定有其“过人”之处卒中二级预防抗血小板药物的最佳选择就是氯吡格雷。
从药物的发展史看,1977年阿司匹林被发现可以预防卒中,1980年正式批准用于临床。
但是它对卒中的二级预防作用有限,只有13%左右的疗效。
增加剂量也不能增加疗效,只能增加不良反应,最大副作用就是胃肠出血。
因此,开始寻找更好的阿司匹林的替代药物。
经过多年的努力,1991年,美国FDA批准了抵克力得,它的作用好于阿司匹林,但它有一个严重的副作用,就是中性粒细胞减少。
探索的步伐没有停止,1998年,FDA批准了一个疗效和安全性更好的药:氯吡格雷。
回顾阿司匹林的临床试验,我们会发现,这些试验多排除了高危高龄的患者,而实际上,这些高危高龄的患者更需要疗效更好的抗血小板药物。
因此,不能不说,阿司匹林的临床试验是有偏向性的临床试验。
CAPRIE研究显示,对于高危患者,氯吡格雷可使血管事件风险降低8.7%。
阿司匹林和氯吡格雷的作用机制不同,将两药联用是否更好呢?答案是否定的。
氯吡格雷与质子泵抑制剂的相互作用
氯吡格雷与质子泵抑制剂的相互作用摘要氯吡格雷能够降低冠心病患者再次发生心肌梗死的风险,故广泛用于急性冠脉综合征和经皮冠脉介入术后的患者。
临床相关指南建议,氯吡格雷应与质子泵抑制剂(proton pump inhibitor,PPI)合用以减少氯吡格雷的胃肠道不良反应。
但是,氯吡格雷需经肝脏细胞色素P450酶的同功酶CYP 2C19代谢才能转化为活性产物发挥作用,而PPI同样主要由CYP 2C19代谢。
药代动力学研究显示,氯吡格雷与奥美拉唑合用会发生药物相互作用、由此降低氯吡格雷的抗血小板作用,而泮托拉唑与氯吡格雷的相互作用不明显。
发表于2009年的系列回顾性病例对照研究表明,氯吡格雷与PPI合用会增加心血管不良事件的发生风险。
但这一研究结果并未得到前瞻性的随机、对照研究和荟萃分析的证实。
因此,目前仍需进行大规模的前瞻性的随机、对照试验来分析氯吡格雷和PPI合用与心血管不良事件风险间的相关性。
鉴于临床上有大量服用氯吡格雷的患者需合用PPI来降低胃肠道出血风险,建议现最好选用与氯吡格雷相互作用较小的泮托拉唑。
关键词质子泵抑制剂氯吡格雷药物相互作用Interaction of clopidogrel and proton pump inhibitorsJIANG Weiru*,ZHONG Liang(Department of Gastroenterology,Huashan Hospital,Fudan University,Shanghai 200040,China)Abstract Clopidogrel is considered as a standard medical treatment for acute coronary syndrome and patients having percutaneous coronary intervention in order to reduce the risk of new ischemic events. Combination of clopidogrel with proton pump inhibitor (PPI)is recommended by clinical guidelines in order to prevent gastrointestinal side effects. Clopidogrel needs metabolic activation predominantly by the hepatic cytochrome P450 isoenzyme 2C19 and PPI are extensively metabolized by the same isoenzyme as well. Pharmacodynamic studies showed that a potential clopidogrel-PPI interaction occurred,resulting in a significant decrease of the clopidogrel platelet antiaggregation effect in case of combination of clopidogrel with omeprazole,but not with pantoprazole. A series of retrospective case-control studies published in 2009 reported that combination of clopidogrel with PPI could increase the risk of adverse cardiovascular events. However,the result of this study has not been confirmed by prospectively randomized and controlled studies and meta-analysis. So,a large-scale prospectively randomized and controlled trial should be performed in order to analyze the risk of cardiovascular adverse events associated with the combination of clopidogrel with PPI. Since many patients taking clopidogrel need to take PPI to reduce the risk of gastrointestinal bleeding,combination of clopidogrel with pantoprazole possessing less drug interaction should be recommended.Key words proton pump inhibitors;clopidogrel;interaction急性冠脉综合征(acute coronary syndrome,ACS)和经皮冠状动脉介入治疗术(percutaneous coronary intervention,PCI)后的患者具有很高的再次发生心肌梗死的风险。
老年人质子泵抑制剂合理应用

老年人质子泵抑制剂合理应用质子泵抑制剂(proton pumpinhibitors,PPIs)自上世纪80年代问世至今20多年来,显着地改善了酸相关性疾病的临床结局,对酸相关性疾病的治疗具有里程碑式的意义。
由于其突出的疗效和良好的安全性,在临床上的应用范围不断扩大,处方量与日俱增。
但是近几年来,PPIs过度使用(超适应证、超剂量、超疗程)的问题日益突出,潜在的不良反应也备受重视。
PPIs是老年人的常用药物之一,老年人共病多,常多重用药,药物间相互作用机会多,药物不良反应发生率高。
因此,老年患者如何科学、合理应用PPIs也尤为重要。
常用PPIs的标准剂量(常规剂量)分别为:奥美拉唑20 mg/d,兰索拉唑30mg/d,泮托拉唑40mg/d,雷贝拉唑10 mg/d,埃索美拉唑20 mg/d;艾普拉唑10 mg/d。
一、老年人PPIs的药代动力学特点及作用机制老年肝脏对药物的代谢转化能力降低,肾脏对药物的清除能力降低,药物半衰期延长、肾毒性增加。
PPIs在体内代谢迅速,血浆半衰期在2 h以内,蛋白结合率均在90%以上。
PPIs 主要通过细胞色素P450系统中的CYP2C19和CYP3A4在肝内代谢,并经肾脏清除。
CYP2C19是大部分PPIs在肝内代谢的主要途径,80%以上的奥美拉唑、50%以上的埃索美拉唑和兰索拉唑经CYP2C19代谢,其次是经CYP3A4、CYPlA2代谢;泮托拉唑虽主要经CYP2C19代谢,但对其亲和力较低,且其特有的二相代谢,也降低了其对CYP2C19的依赖性;雷贝拉唑要经烟酰胺嘌呤二核苷酸磷酸(NADP)代谢,其次经CYP3A4、CYP2C19代谢;由此可见,常用的5种PPls对CYP2C19的依赖性存在差异,泮托拉唑和雷贝拉唑对CYP2C19的依赖性较低[昏7。
老年人肾功能不全和轻中度肝功能不全患者的PPIs药代动力学与青年人相似,所以无需调整剂量;但严重肝功能不全患者,其最大曲线下面积(AUCmax)值为肝功能正常者的2~3倍,血浆半衰期明显延长,应用PPIs应相应减量。
最新氯吡格雷的临床药理学进展

氯吡格雷是前体药物,经①CYP3A4/5, CYP2C19,CYP2C9, CYP2B6,CYP1A2;②CYP2C19 和CYP2B6两步,代谢激活后发挥抗血小板聚集 作用。因此,CYP3A4、CYP2C19抑制剂可能影 响氯吡格雷的疗效。
例如,诊断为脑梗塞后遗症、高血压病、抑郁 症、淋巴结炎。处方为氯吡格雷片75 mg qd, 缬沙坦胶囊80 mg qd,帕罗西汀片20 mg qd, 克拉霉素缓释片0.5 g qd。 如何改进?
氯吡格雷的临床药理学进展
波立维(Clopidogrel Sulf)与它的血小板受体的结 合及继发的ADP介导的糖蛋白GPIIb/IIIa复合物 的活化,因此可抑制血小板聚集。 氯吡格雷对血小板ADP受体的作用是不可逆的, 因此暴露于氯吡格雷的血小板的整个生命周期 都受到影响,血小板正常功能的恢复速率同血 小板的更新一致。
关于剂量问题
Kenichi等 对氯吡格雷150 mg负荷量的抑制作 用进行了研究。将40例冠状动脉支架术后的患 者分为两组分别使用300和150 mg负荷量,在 用药后2、4、6和8 h分别用5和20μmol/L的 ADP诱导光学法血小板聚集作为血小板抑制程 度的判断指标。 结果发现:150 mg负荷量与300 mg负荷量相比, 不能起到快速抑制血小板的作用,因此300 mg 氯吡格雷负荷量在东方人中也是必需的。
CYP2C19*2基因携带者15例发生死亡,心肌梗塞 和急性冠状动脉血运重建事件,非携带者11例 发生上述事件(HR 3.69,95%CI 1.69~8.05, p=0.005); 携带者8例发生支架血栓事件,非携带者4例发 生支架血栓事件(HR 6.02,95%CI 1.81~20.04, p=0.0009)。 经多变量分析,CYP2C19*2基因变异是唯一独立 的心血管事件预测因子。 年轻患者发生心肌梗塞后,CYP2C19*2基因变异 是决定服用氯吡格雷远期疗效的决定因子。 来源:Lancet 2009: 373; 309–17
178.)PPI对氯吡格雷的影响临床药师论坛投稿
质子泵抑制剂(PPIs)对氯吡格雷的影响吴雪梅,郑敬旭,刘茂柏福建医科大学附属协和医院临床药师培训基地摘要:尽管抗血小板药物可有效降低血栓事件的发生,但出血风险增加。
加用PPI可避免抗血小板治疗所导致的胃肠黏膜损害,但因PPI在肝脏的代谢具有与氯吡格雷相同的代谢途径,从而有可能降低氯吡格雷的抗血小板效益并导致不良心血管事件的危险增加。
最近的研究发现不同的质子泵抑制剂影响程度不同,泮托拉唑和埃索美拉唑对氯吡格雷作用影响较小,而奥关拉唑、雷贝拉唑和兰索拉唑对氯吡格雷的抗血小板活性抑制作用较大。
关键词:质子泵抑制剂;氯吡格雷;药物相互作用《不稳定性心绞痛和非ST段抬高心肌梗死诊断与治疗指南》推荐给予急性冠状动脉综合征(ACS)患者双重抗血小板治疗,即在应用小剂量阿司匹林的基础上加用氯吡格雷,二者联合应用可以明显减少心血管事件发生率,但同时增加消化道出血的风险。
临床上通常给予该类患者联用质子泵抑制剂(PPI)预防消化道出血。
而近期的一些研究表明,质子泵抑制剂影响氯吡格雷的抗血小板聚集作用,增加临床事件。
另外一些研究表明质子泵抑制剂不影响氯吡格雷的抗血小板聚集作用,目前对质子泵抑制剂是否会影响氯吡格雷的抗血小板聚集作用尚无统一观点。
1.氯吡格雷和PPIs体内作用的机制1.1氯吡格雷的体内作用机制氯吡格雷是噻吩并吡啶类二磷酸腺苷(ADP)受体拮抗剂,它是一种前体药物,须在体内经过一系列生物转化形成活性产物而发挥抗血小板作用。
氯吡格雷在体内通过氧化、水解两步连锁反应后形成一种硫醇衍生物,此衍生物与位于血小板上的ADP受体P2Y12不可逆结合,抑制纤维蛋白原受体GpⅡb/Ⅲa的活化,从而起到抑制血小板聚集的作用。
这一过程受细胞色素P450同工酶系统的影响,包括同工酶CYPlA2、CYP2B6、CYP2C9、CYP3A4、CYP2C19,而CYP2C19在这一过程中起主要作用[1]。
氯吡格雷的易损性在于它激活的方式,它激活的两步连锁反应过程都依赖于CYP2C19的功能。
重视抗血小板药物消化道并发症的防治

重视抗血小板药物消化道并发症的防治——中国专家共识讨论会报道大量循证医学证据显示,抗血小板治疗对于血栓栓塞性疾病的一级预防和二级预防有益,阿司匹林(75~325 mg)已广泛用于冠心病、脑血管病和外周动脉病患者。
尤其对于急性冠脉综合征(ACS)和置入药物洗脱支架(DES)的患者,更强调双重抗血小板治疗的重要性。
但是,抗血小板药物是一把“双刃剑”。
阿司匹林通过抑制前列腺素的生成发挥作用,一方面能抑制血小板活化和血栓形成,另一方面则损伤胃肠道黏膜,导致溃疡形成和出血。
其他抗血小板药物如氯吡格雷也能加重胃肠道出血。
临床医生掌握长期抗血小板治疗的益处和风险至关重要。
为此,中国医师学会心血管内科医师分会、中华医学会消化病学分会和《中华内科杂志》共同组织制订一项专家共识,关注心血管疾病治疗中抗血小板药物消化道并发症的预防和治疗,希望以此更好地敦促心血管内科医生在处方抗血小板药物的同时,兼顾预防胃肠道副作用,并与消化科医生协作,减少胃肠道并发症,使小剂量阿司匹林为心血管疾病患者带来更大益处。
2009年3月4日,来自心血管内科和消化内科领域的20余位专家共聚一堂,在胡大一、林三仁教授的主持下,与会专家肯定了小剂量阿司匹林预防和治疗血栓栓塞性疾病的基石作用,并就如何预防和治疗消化道并发症进行了深入、全面地讨论,包括制订完善的评估、预防和治疗方案,使心血管医生在临床工作中更好地控制血栓事件的同时,降低消化道出血风险。
平衡获益与风险,更好地使用抗栓“利刃”胡大一教授提出,小剂量阿司匹林用于心脑血管事件一级预防和二级预防的益处肯定。
面对我国约2亿心脑血管事件高危人群,阿司匹林的使用日益普及,同时,为预防置入DES后支架内血栓形成,联合使用阿司匹林和氯吡格雷的情况也越来越多。
在接受抗血小板药物治疗患者群不断扩大的背景下,抗血小板药物的消化道并发症问题也引起了广泛关注。
众所周知,血栓栓塞性事件可以导致死亡,消化道出血也同样可以导致死亡。
胃酸抑制剂药物联用氯吡格雷是可取的

致命或非致命性心脏病发作的风险 。因
此 ,氯 吡格 雷 成 为美 国 医生 最 常开 的药
物 之一 。
然 而 ,氯 吡格 雷 和 阿 司匹林 均 可 引
起 胃肠道 出血 。若 胃肠 道 有 出血 风 险 增
加 ,可以使用质子泵抑制剂 P I减少 胃 Ps
酸 的产 生 。数 百万 消 化性 溃 疡 和 胃食 管
YNYOAHN 用药导航 I OGADO AG
胃 酸 抑 制 剂 联 用 氟 毗 格 雷 是 可 取 的
● 吕 悦 然
没有确凿 的证据显示两者联合使用
有 危险 。
反 流疾病患者在 服用这类 常用药物 , 其
中包 括奥 美拉唑 f 品名 :roe)艾 美拉 商 Pi sc、 l
如果 你 的冠 脉植 入 有 改善 血 流 的 支 架 , 或许正在服用氯吡格雷( 品名 : 你 商 波 立 维 ) 阿 司匹林 , 防支 架 内形 成 血 和 以 凝 。药物 的联合 使 用 已被 证 实 可 以降低
丰到答亲 芡
最 近 ,一 项 由哈 佛研 究 人 员牵 头 的
GAI0AG j Y ( A H 用药导航 Y o ) )
研 究 并 未发 现 同 时服 用氯 吡格 雷 和奥 美 拉 唑 可 增加 心 脏病 发 作 、中风 或死 亡 风 险 。卑 赫 尼 ( ht 是 弗 吉尼 亚 州波 士 顿 B at ) 保 健 系 统心 脏病 学 主 任 ,以及 哈佛 大 学 医学 院 副教 授 ,他 希 望这 项 研究 可 以让 大 众 的担忧 告一 段 落 。 “ 测试 管 内是有 药 物 与药 物 间 的 检 反 应 ,但 未 有 随机 临 床试 验 显示 临床会
受 到 同样 的影 响 。” 说 道 。“ P 类 药 物 他 PI
氯吡格雷与PPI联用安全性

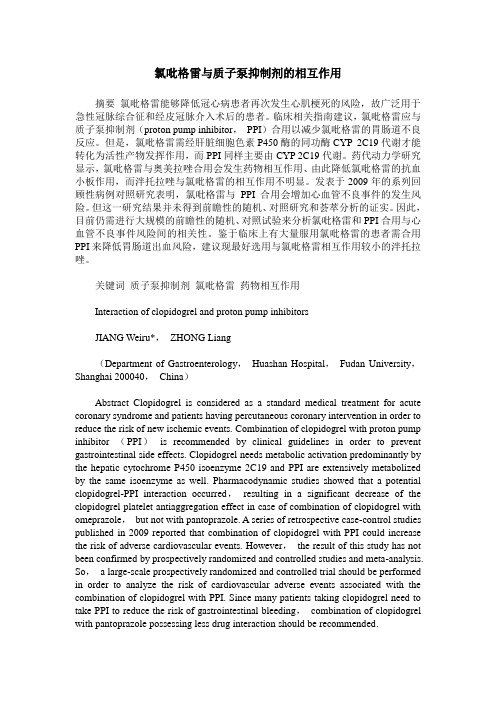
2011年发表的研究
** *
* P=0.805 **P=0.456
• 前瞻性研究 (台湾) • 患者/方法:165例长期使用氯
吡格雷治疗的患者,予以埃索 美拉唑+氯吡格雷或仅予以氯
Eso VS Pan:3篇,对血小板活性 的影响,2个药物之间没有差异
注意:血小板的功能与临床结果之间的关系尚不明确
Chun Shing Kwok et al. Drug Saf 2012; 35 (2)
风险比 Ome 1.226 Eso 1.005 Lan 0.964 Rab 1.182 Pan 1.013
Lin et al. Br J Clin Pharmacol / 74:5 / 825
2010年发表的研究---目前唯一一项随机对照研究
前瞻性,随即,双盲,III期临床研究 (COGENT 研究) 患者/方法:3873例需要接受双抗治疗的 患者,予以奥美拉唑或安慰剂治疗 终点:严重的心血管事件 结果:奥美拉唑的使用不会增加心血管事 件再发风险
数据解读
以实验室指标为终点的研究
2
2009年发表的研究
前瞻性队列研究 患者/方法:300例 PCI术后患者,随机予以 Pan+Clop+ASA或Eso+Clop+ASA 或 Clop+ASA 主要指标:ADP诱导的血小板聚集度和血小 板反应指数(PRI) 结果: ADP诱导的血小板聚集度和PRI在 Pan组以及Eso组或对照组中的没有差异
风险比 Eso 0.71 Ome 0.79 Pan 1.08 Rab 0.54 Lan 1.06
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
OBJECTIVE: To evaluate the interaction between clopidogrel and proton pump inhibitors (PPIs). DATA SOURCES: Literature retrieval was accessed through PubMed (1980- January 2009), abstracts from 2008 American Heart Association and 2009 Society of Cardiovascular Angiography and Interventions Scientific Sessions, and media press releases using the terms clopidogrel, proton pump inhibitors, cytochrome 2C19, genetic cytochrome P450 polymorphisms, and drug interaction. In addition, reference citations from publications identified in the search were reviewed. STUDY SELECTION AND DATA EXTRACTION: Relevant original research articles and review articles were evaluated. Articles were selected if they were published in English and focused on any of the key words or appeared to have substantial content addressing the drug interaction. DATA SYNTHESIS: Recent attention has been placed on a potential interaction observed between clopidogrel and the widely used PPIs. Preliminary evidence suggests that omeprazole interacts with clopidogrel, reducing clopidogrel's antiplatelet effects as measured by various laboratory tests. Most data indicate that the interaction involves the competitive inhibition of the CYP2C19 isoenzyme. The interaction appears to be clinically significant, as several retrospective analyses have shown an increase in adverse cardiovascular outcomes when PPIs and clopidogrel are used concomitantly. However, this may not be a class effect. CONCLUSIONS: Available data suggest that omeprazole is the PPI most likely to have a significant interaction with clopidogrel. Further studies are needed to determine that an interaction between the other PPIs and clopidogrel does not exist. In situations in which both clopidogrel and a PPI are indicated, pantoprazole should be used since it is the PPI least likely to interact with clopidogrel.
暨南大学第三附属医院 珠海市人民医院心内科 石理
冤家对头—东窗事发
为了降低抗血小板治疗患者的消化道出血风险,加用质子
泵抑制剂(PPI)似乎已成为临床常规,但今年初《加拿大 医学会杂志》[CMAJ 2009,180(7):713]和《美国医学会杂 志》[JAMA 2009,301(9):937]发表的两项大规模回顾性研 究对这一用法提出了质疑。两项研究均显示,氯吡格雷与 PPI联用增加心血管事件发生风险。此后美国FDA也发出警 告,提醒医生警惕以上两药联用的风险。
CYP2C19抑制效力小的泮托拉唑,从而最大程度地减少药物不良反应和心血管不良事件
的发生;
氯吡格雷与PPI的多代谢途径,不能简单禁止氯吡格雷与PPI联用; 药理理论研究不能完全代替临床试验,还是需要大规模临床试验结果。
百家争鸣之心血管
目前大部分ACS患者会接受阿司匹林联合氯吡格雷抗血小板治疗; 德里(Derry)等的研究表明,长期使用阿司匹林致消化道出血的发生
5种PPI的药代动力学和药物间相互作用比较(Drug Safety 2006,29:769-784)
冠心病患者使用PPI的证据
消化道出血率高
全球急性冠脉综合征注册研究(GRACE)显示:ACS患者合并大出血的发生率为
2.3%~4.8%,最常见的出血部位为消化道,占所有出血部位的31.5%。也有回顾性
双抗治疗支持PPI使用证据
双抗治疗支持PPI使用证据
双抗治疗不支持PPI使用证据
双抗Байду номын сангаас疗不支持PPI使用证据
思考
PPI真的死刑?
PPI究竟怎么用?
不能使用PPI,心内科医生还能做什么?
心血管、消化科、临床药学三方讨论
百家争鸣之消化界
为了预防长期服用NSAIDs引起的胃肠道不良反应,首选PPI是消化界共
研究表明,ACS患者合并严重胃肠道出血的发生率为3%。
消化道出血死亡率高
ACS合并胃肠道出血的患者预后差,死亡率高达36.3%,与未合并胃肠道出血
的ACS患者相比具有显著差异。
出血的高危因素
既往有上消化道出血病史、活动性消化性溃疡、既往有消化性溃疡史(特别是具
有溃疡并发症者)、已知的胃息肉和恶性肿瘤等。
识;
权衡抗血小板治疗降低“心血管缺血风险”和 增加“消化道出血风险”
的利弊以及应用PPI有利止血和其减弱氯吡格雷作用之利弊应侧重考虑
心血管缺血风险;
PPI预防性用药需有针对性:消化性溃疡病史无出血但有幽门螺杆菌感
染;近年有消化道溃疡出血病史;需双重抗血小板制剂。超过下列一项 因素者:年龄≥60岁、应用皮质激素超过6日或更长时间、脓毒症患者, 也应考虑应用PPI。一般疗程不超过8周;
百家争鸣之心血管
2009年4月发表于《血栓与止血学》杂志上的一项研究表明,仅奥美拉唑会减
弱氯吡格雷的抗血小板作用,而泮托拉唑和埃索美拉唑不会增加再发心梗风 险,相对安全有效 另一项研究也证实,泮托拉唑不会升高急性心梗患者的再 梗死率。因此,基于当前证据,不推荐ACS患者联用氯吡格雷与奥美拉唑;
PPI 相关指南与共识
2007年美国心脏病学会/美国心脏学会(ACC / AHA)发表指南指出,既往有消
化道出血病史者,在单独或联用阿司匹林和氯吡格雷时,可加用质子泵抑制剂 (PPI)以降低再出血风险;
Aspirin plus PPI safer than clopidogrel if there is history of GI bleeding. N Engl
而发生药物相互作用,其程度取决于与CYP450同工酶相对亲合力的大
小,高亲和力化合物将与酶结合并抑制低亲和力化合物的生物转化。
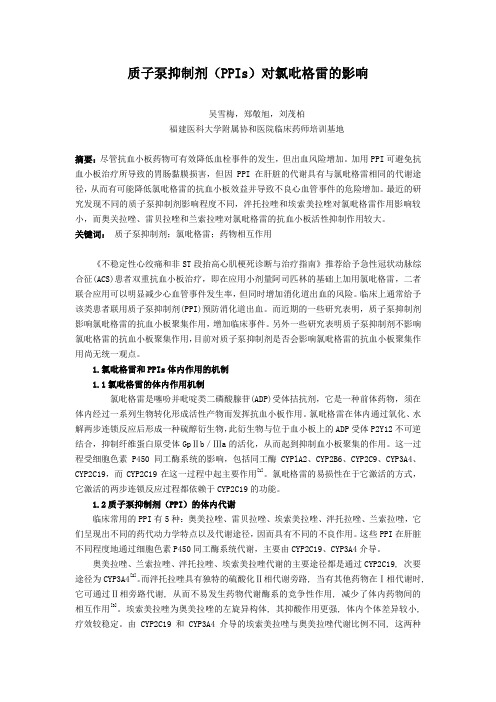
PPI与氯吡格雷的药代学影响
Ki值越小表示对该同工酶抑制效力越强
PPI与氯吡格雷的药代学影响
对CYP2C19的抑制强度:兰索拉唑>奥美拉唑>埃索美拉唑>泮托拉唑>雷贝拉唑
最新资料
Ann Pharmacother. 2009 May 26. [Epub ahead of print] Links Drug-Drug Interaction Between Clopidogrel and the Proton Pump Inhibitors (July/August)(CE). Norgard NB, Mathews KD, Wall GC. School of Pharmacy and Pharmaceutical Sciences, University at Buffalo, Buffalo, NY.
J Med. 2005 Jan 20;352(3):238-44.
2008年美国心脏病学会基金会(ACCF)/美国胃肠病学会(ACG)/AHA联合公布
的专家共识对氯吡格雷替代阿司匹林提出质疑,建议有消化道溃疡复发风险者
采用阿司匹林联合PPI治疗,另外,急性心梗后服用阿司匹林的患者同时加用质
子泵抑制剂(PPI)。
氧化水解形成具有药理活性的硫醇衍生物,该活性代谢产物不可逆地 与血小板二磷酸腺苷受体P2Y12结合,最终抑制纤维蛋白原受体
GPⅡb/Ⅲa活化,从而抑制血小板聚集。
PPI也主要通过CYP2C19和CYP3A4同工酶在肝脏代谢。 PPI与氯吡格雷合用时可能会因共同竞争CYP450同工酶的相同结合位点
PCI术后患者接受阿司匹林和氯吡格雷抗血小板治疗的同时,为预防其
胃肠道不良反应,选用PPI中的雷贝拉唑较为合适。如果选用H2受体 拮抗剂,则须剂量加倍;