太平人寿保险有限公司团体人身保险投保单
太平人寿电子投保确认书
E 保确@回国末m CHINA TAIPI ~J.::节9嘿险有限公司URANCE CO.,LTD.认书本人《人身保险投保单(时)>>投保单号:I根据《人身保险新型产品信息披露管理办法》规定,如投保的险种中包括分红保险、万能保险或投资连结保险请在下方空格抄录:本人已阅1卖保险条款、产口口口说E 刀目书和投保t 工足日刁τ书,了解本产口口口的特占和保单中'f'11叫u 益向S~μJ 不确足~性。
投保人签名被保险人(或其法定监护人)签名代理人签名一一一年一一一月一一一日签署日期h O 寸,..o N(3)如果您选择购买万能保险产品,请您注意以下事项:万能保险产品通常有最低保证利率的约定,最低保证利率仅针对投资账户中资金。
您应当详细了解万能保险的费用扣除情况,包括初始费用、死亡风险保险费、保单管理费、手续费、退保费用等。
您应当要求销售人员将万能保险账户价值的详细计算方怯对您进行解释。
万能保险产品的技资回报具有不确定性,您要承担部分投资风险。
保险公司每月公布的结算利率只能代表一个月的投资情况,不能理解为对全年的预期,结算利率仅针对技资账户中的资金,不针对全部保险费。
产品说明书或保险利益测算书中关于未来保险合同利益的预测是基于公司精算假设,最低保证利率之上的投资收益是不确定的,不能理解为对未来的预期。
如果您选择灵活交费方式的,您应当要求销售人员将fg停止交费可能产生的风险和不利后果对您进行解释。
七、请您正确认识人身保险新型产品与其他金融产品分红保险、投资连结保险、万能保险等人身保险新型产品兼具保险保障功能和投资功能,不同保险产品对于保障功能和投资功能侧重不同,但本质上属于保险产品,产品经营主体是保险公司。
您不宜将人身保险新型产品与银行存款、国债、基金等金融产品进行片面比较,更不要仅把它作为银行存款的替代品。
八、选择健康保险产品时请您注意产品特性和条款具体约定健康保险产品是具布较强风险保障功能的产品,既有定额给付性质的,也有费用补偿性质的。
2023版人身保险个人投保单范本

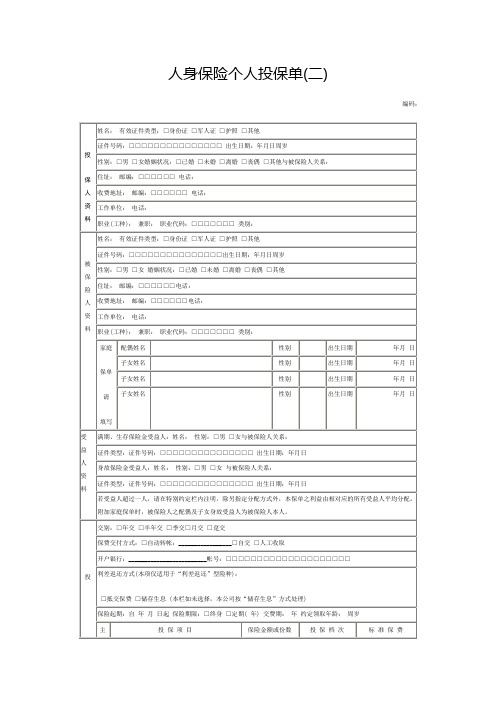
2023版人身保险个人投保单范本兹拟向某某保险公司投保人身保险,内容如下:投保单编号:保险种类投保人情况:姓名身份证号码与被保险人关系地址邮编电话被保险人情况:姓名年龄性别身份证号码地址邮编电话保险年期保险份数受益人领取日期领取年龄领取方式领取金额保险期限自____年____月____日中午12时起至____年____月____日中午12时止基本保险金额附加保险金额意外伤残保额意外身故保额疾病伤残保额疾病身故保额满期保险金额生存给付金费率附加险别保额费率附加险别保额费率保险费保险本金缴费形式一次性缴费□年缴□半年缴□季缴□月缴□其他:付款方式币种开户银行帐号特别约定:被保险人健康状况:1.目前尚在病假中□有□无2.因病休或因病减轻劳动量□有□无3.因患有其他慢性病而不能全勤工作或经常缺勤□有□无4.有无严重病史□有□无5.癌症、肝硬化、癫痫病、脑震荡、精神病、心脏病、高血压病、血管硬化、性病等□有□无投保人是否健康□是□否投保声明:1)本投保单所填写的各项内容,均属真实,可作为你公司签发保单的根据,并成为双方合约的组成部分,如日后发现与事实不符,即使保单签发,你公司仍可不负任何责任。
2)本投保单方格内填(可删改)相关文章一(各银行贷款用)个人收入证明范文个人收入证明致交通银行支行(部):________________兹证明______________先生/女士,系我单位(1、正式工;2、合同工;3、临时工),已在我单位工作 ________年,现任职务,其身份证号码为_____________________,其个人月收入为人民币(大写) ________元,年总收入为人民币(大写) ________元,以上情况属实。
本单位对该证明的真实性负责!特此证明单位地址:________________单位电话:________________ 单位联系人:________________________年 ________月 ________日职业及收入证明中国______________公司_______支行:________________兹证明______________系本单位职工(有效身份证号码:________________),性别_______,年龄______________岁,工作年限 ________年,现任______________职务,已获得______________职称,月收入为人民币(大写) ________元整。
太平人寿保险有限公司意外伤害保险条款
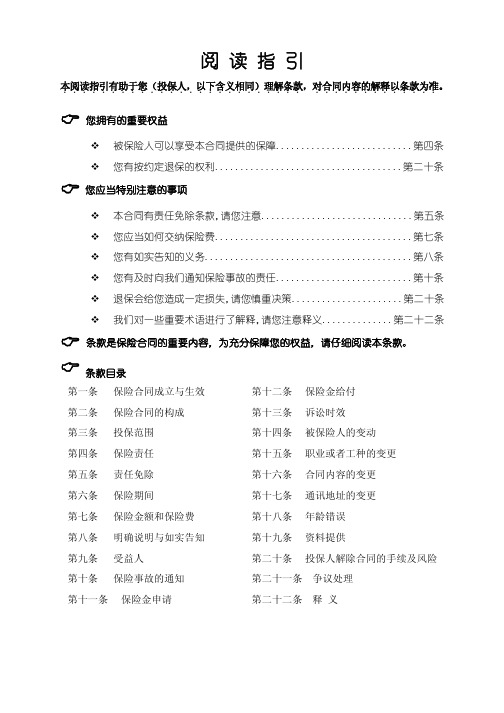
第六部分 您必须了解的其它事项............................................................................................................................ 7
第十八条
明确说明与如实告知 ................................................................................................................................................. 7
第三部分 如何交纳保险费........................................................................................................................................ 5
第四条
保险责任 ..................................................................................................................................................................... 3
第六条
保险合同成立与生效 ................................................................................................................................................. 4
人寿保险投保单(通用3篇)
人寿保险投保单(通用3篇)人寿保险投保单篇1人寿保险投保单人寿保险投保单┏━━━━━━━━┯━━━┓┃保险单编号│no.:┃┠────────┼───┨┃投保单编号│no.:┃┗━━━━━━━━┷━━━┛□体检□免体检------------------------------------------------------------------------公司提示:请您在仔细阅读保险条款、投保须知后用钢笔填写本投保单,您必须在此投保单上填报一切有关事实,因为您与本公司之合约将以这些事实为根据,否则所签保单将告无效。
如您不清楚某一事项是否重要或如何填写,请与本公司业务员联系。
------------------------------------------------------------------------第一部分------------------------------------------------------------------------1.被保险人姓名身份证号码出生日期年月日------------------------------------------------------------------------年龄民族单身□已婚□职业职业编码(此内容由本公司人员填写)------------------------------------------------------------------------住所(如无特别注明,将以此为通讯地址)邮编-----------------------------------------------------------------------电话号码(宅)(办)与投保人关系------------------------------------------------------------------------2.投保人姓名身份证号码性别出生日期年月日------------------------------------------------------------------------民族单身□已婚□职业职业编码(此内容由本公司人员填写)------------------------------------------------------------------------住所(如无特别注明,将以此为通讯地址)邮编------------------------------------------------------------------------电话号码(宅)(办)------------------------------------------------------------------------3.受益人姓名身份证号码性别年龄住所与被保险人关系受益份额*受益人为数人且未确定受益份额的,受益人按照相等份额享有受益权。
个人人身保险投保单(2016版)@太平人寿保险有限公司
特别约定
声明与授权
1、贵公司所提供的投保单已附保险条款,已对保险合同的条款内容履行了说明义务,并对免除保险人责任的条款履行了提示和明确说明义务。本人所填投保单各 项及告知事项均属事实并确无欺瞒。上述一切陈述及本声明将成为贵公司承保的依据,并作为保险合同一部分。如有不实告知,贵公司有权在法定期限内解除 合同,并依法决定是否对合同解除前发生的保险事故承担保险责任。 2、本人谨此授权凡知道或拥有任何有关本人健康及其它情况的任何医生、医院、保险公司、其它机构或人士,均可将有关资料提供给贵公司。此授权书的影印本 也同样有效。 3、本人已知晓: (1)具有续保条款的意外险或健康险产品,贵公司将按续保保险期间开始时被保险人的年龄和职业、上年度保额等费率计算因子重新计算续保合同保费,并保留 拒绝续保、对承保条件做出相应调整的权利。 (2)具有续保条款的意外险或健康险产品,如果被保险人的职业(或工种)、健康状况等发生变化或在保险期间发生保险事故,本人有义务在续保之前以书面形 式如实告知贵公司。 4、投保授权声明(投保人非被保险人本人或法定监护人时填写): 作为被保险人本人或法定监护人,本人同意投保人(姓名) 并同意本投保单中设定的受益人、受益顺序及受益份额。 授权人签名: 投保人签章: 被保险人(或监护人)签章: 授权日期: 年 月 日 为被保险人投保贵公司的保险产品及基本保险金额,
保险 保障
投保贷款人意险请 填写本栏
发放贷款机构 贷款金额 旅行社名称 旅行区域 行驶证车主 旅行行程 车牌号
贷款合同号 贷款期限 旅 类 行 型 年 月 日至 年 月 日
投保旅游意外险请 填写本栏 约定使用车辆 请填写本栏
□境内旅游 □境外旅游 □商务旅行 □境外留学 □境外探亲 □其他 座
核 准 座 位 数
人身保险个人投保单模板
被保险人
询问事项
有 无
有 无
□ □
□ □
1.近期体况:
最近6个月内是否有新发的或以往既有的任何身体不适症状或体症如反复持续头痛、眩晕、胸痛、咯血、气喘、腹痛、便血、紫斑、消瘦(体重短期内下降超过5公斤)、视力下降。
□ □
□ □
2.近期诊治:
最近6个月内是否接受过医师的诊察、治疗、用药,对其结果医师是否提出检查、治疗、住院或手术建议
收费地址: 邮编:□□□□□□电话:
工作单位: 电话:
职业(工种): 兼职: 职业代码:□□□□□□□ 类别:
家庭
保单
请
填写
配偶姓名
性别
出生日期
年月 日
子女姓名
性别
出生日期
年月 日
子女姓名
性别
出生日期
年月 日
子女姓名
性别
出生日期
年月 日
受 益 人 资 料
满期、生存保险金受益人:姓名: 性别:□男 □女与被保险人关系:
□ □
□ □
年内健康检查:
过去2年内接受的健康检查(如血压、尿液、血液、肝功能、肾功能、心电图、X光、B超、CT、核磁共振、脑部等)检查结果有无异常情形或被医师建议接受其他检查
□ □
□ □
4.住院史:过去5年内曾否住院
□ □
□ □
5.过去曾否患有下列疾病
霍乱、肺结核、脊髓灰质炎、肝炎病毒携带;癌症、肿瘤、何杰金氏病、囊肿、结石;甲状腺疾病、糖尿病、甲状旁腺疾病、肾上腺疾病、高脂血症、痛风;贫血、血友病、紫癜、脾脏疾病;精神疾患、抑郁症、神经官能性疾患、儿童多动症;脑膜炎、脑炎、脊髓炎、神经麻痹、癫痫、脑部疾病、脊髓疾病、白内障、青光眼、视网膜或视神经病变;风湿热、风湿性心脏病、高血压病、继发性高血压、冠心病、肺心病、心肌炎、传导阻滞、心律失常、心脏病、脑中风、血管疾病、下肢静脉曲张;肺炎、支气管炎、肺气肿、哮喘、支气管扩张、肺大泡、胸膜炎、气胸;慢性胃炎、肠炎、消化道溃疡或出血、疝、肠梗阻、肝炎、脂肪肝、肝肿大、肝硬化、肝功异常、胆石病、胰腺疾病;肾炎、肾病、肾衰竭、肾盂积水、多囊肾、性病;红斑狼疮、脊椎疾病、类风湿性关节炎、风湿病、肌肉、骨骼、关节疾病;结缔组织疾病;自体免疫性疾病;先天性疾病、遗传性疾病;脑外伤后综合症、内脏损伤、中毒。
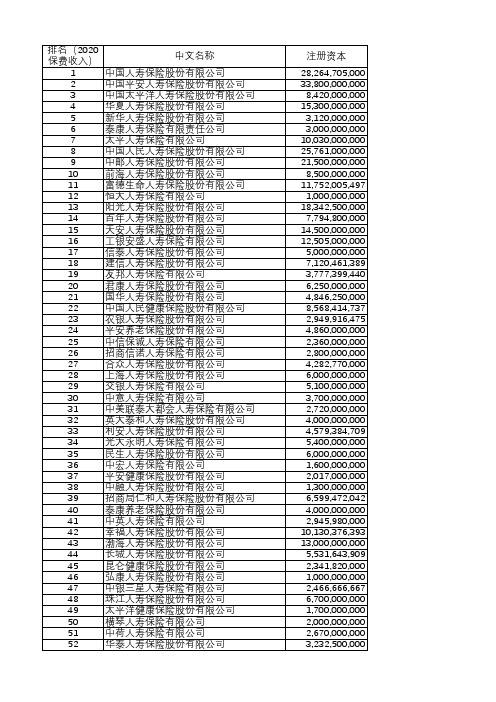
人身险公司排名(按保费收入)
53
同方全球人寿保险有限公司
54
中德安联人寿保险有限公司
55
太平养老保险股份有限公司
56
恒安标准人寿保险有限公司
57
东吴人寿保险股份有限公司
58
信美人寿相互保险社
59
爱心人寿保险股份有限公司
60
中华联合人寿保险股份有限公司
61
陆家嘴国泰人寿保险有限责任公司
62
北大方正人寿保险有限公司
63
中国人寿养老保险股份有限公司
44
长城人寿保险股份有限公司
45
昆仑健康保险股份有限公司
46
弘康人寿保险股份有限公司
47
中银三星人寿保险有限公司
48
珠江人寿保险股份有限公司
49
太平洋健康保险股份有限公司
50
横琴人寿保险有限公司
51
中荷人寿保险有限公司
52
华泰人寿保险股份有限公司
注册资本
28,264,705,000 33,800,000,000
500,000,000 2,000,000,000 1,000,000,000 1,500,000,000 3,000,000,000 2,167,000,000 1,025,000,000 3,463,479,370 1,500,000,000 1,500,000,000 1,500,000,000 1,000,000,000 1,800,000,000 1,500,000,000
800,000,000 1,871,000,000 4,000,000,000
500,000,000 1,250,000,000 5,000,000,000 3,000,000,000 20,360,502,599
301_太平盛世团体意外伤害保险条款
第三条 投保范围 一、 年龄在 16 周岁至 65 周岁,身体健康,能正常工作或劳动的在职员工,可作为被保险人参加本 保险。被保险人的配偶和子女,经本公司审核同意,可作为附属被保险人参加本保险。 二、 经被保险人同意,被保险人所在团体可作为投保人。团体投保时,其在职人员必须 75%以上投 保,且符合投保条件的人数不低于 5 人。
本页内容结束太平盛世团体意外伤害保险第人身保险残疾程度与保险金给付比例表等级项目给付比例双目永久完全失明的注1两上肢腕关节以上或两下肢踝关节以上缺失的一上肢腕关节以上及一下肢踝关节以上缺失的一目永久完全失明及一上肢腕关节以上缺失的一目永久完全失明及一下肢踝关节以上缺失的四肢关节机能永久完全丧失的注2咀嚼吞咽机能永久完全丧失的注3中枢神经系统机能或胸腹部脏器机能极度障碍终身不能从事任何工作为维持生命必要的日常生活活动全需他人扶助的注4100两上肢或两下肢或一上肢及一下肢各有三大关节中的两个关节以上机能永久完全丧失的注5十手指缺失的注675十一十二十三十四十五一上肢腕关节以上缺失或一上肢的三大关节全部机能永久完全丧失的一下肢踝关节以上缺失或一下肢的三大关节全部机能永久完全丧失的双耳听觉机能永久完全丧失的注7十手指机能永久完全丧失的注8十足趾缺失的注950十六十七十八十九二十二一二二一目永久完全失明的一上肢三大关节中有二关节之机能永久完全丧失的一下肢三大关节中有二关节之机能永久完全丧失的一手含拇指及食指有四手指以上缺失的一下肢永久缩短5公分以上的语言机能永久完全丧失的注10十足趾机能永久完全丧失的30二三二四二五二六二七二八二九一上肢三大关节中有一关节之机能永久完全丧失的一下肢三大关节中有一关节之机能永久完全丧失的两手拇指缺失的一足五趾缺失的两眼眼睑显著缺失的注11一耳听觉机能永久全丧失的鼻部缺损且嗅觉机能遗存显著障碍的注1220三十三一三二一手拇指及食指缺失或含拇指或食指有三个或三个以上手指缺失的一手含拇指或食指有三个或三个以上手指机能永久完全丧失的一足五趾机能永久完全丧失的15三三三四一手拇指或食指缺失或中指无名指和小指中有二个或二个以上手指缺失的一手拇指及食指机能永久完全丧失的10注
太平综合意外伤害保险2006条款
第十条
保险事故通知........................................................................................................................................................... 6
第十一条
诉讼时效................................................................................................................................................................... 6
第一条
保险合同的构成....................................................................................................................................................... 3
第六条
保险合同成立与生效............................................................................................................................................... 5
第四条
保险责任................................................................................................................................................................... 3
团体人身意外伤害保险投保单

团体人身意外伤害保险投保单一、保险人基本信息保险人(个人或企业):投保人(个人或企业):保单签订日期:保险起始日期:保险终止日期:投保人保证:二、被保险人基本信息姓名:证件类型:证件号码:性别:出生日期:职业:联系电话:邮政编码:电子邮箱:三、保险责任被保险人在保险期内,因突发意外导致意外身体伤害或死亡,由保险公司按照保险合同约定承担保险赔偿责任。
四、保险费用及交费方式以下费用根据实际情况填写:1.保险金额:2.保险期间:3.保险费用:4.付款方式:5.告知义务:保险人有义务如实告知被保险人的健康状况等情况。
6.人身保险分红:本保险不涉及分红。
五、其他特别约定保险单编号:保险合同起始日至终止日内,若被保险人逝世,保险公司应按照合同规定向其合法继承人支付保险金。
六、投保人声明投保人已于保险公司就所购买保险等有关事项进行充分了解,截断不实情况并已如实告知,且无任何其他约定。
七、注意事项1.本保险不承担以下保险责任:(1)意外事故发生前已经患有疾病或者身体缺陷,确诊或推定为疾病或缺陷的;(2)意外事故发生时,被保险人正在吸食、注射毒品、酗酒、醉酒或未按规定使用法定药物的;(3)意外事故发生时被保险人犯罪、从事危险运动或者危险职业的;(4)意外事故发生时被保险人自杀或自伤的;2.请认真核对保险单上的信息,如有错误请及时联系保险公司更正。
八、法律声明本合同适用中国法律。
因本合同引起的一切争议,各方应通过友好协商解决,如无法协商解决,则提交有管辖权的人民法院诉讼解决。
九、保险公司声明1.保险公司承保以上风险责任,现确认并保证,在正常解决投保人、被保险人提出的保险权益申请、索赔、告知等保险理赔事项时,保险公司会遵守各项保险经营法规,确保被保险人资金安全合理。
2.保险公司声明:本保险单系本公司在根据投保人的申请,根据保险的规定所制订的保险合同,在签名盖章之前,请投保人认真阅读本投保单及相关的凭证,一经签名盖章,即为投保人自愿接受本合同的全部条款和内容,不得撤销。
太平人寿保险有限公司资料
太平人寿历史悠久,1929年始创于上海,1956年移师海外专营寿险业务,曾是中国近现代史上实力最强、规模最大、市场份额最多的民族保险企业之一,也是现今中国保险市场上经营时间最长和品牌历史最悠久的中资寿险公司之一。
2001年11月,中国保险(控股)有限公司(2009年6月更名为中国太平保险集团公司,简称“中国太平”)以“太平人寿”名义,全面恢复经营国内人身保险业务。
复业后的“太平人寿”是我国第六家全国性寿险公司,也是国有四大保险集团之一,直接隶属于国务院管理的金融机构,是中国目前唯一拥有境内外双平台的保险公司,也是中国第一家在海外上市的跨国金融集团,国际信誉评级全国第一,公司具有专业、稳定的股东架构,第一大股东是中国太平保险控股有限公司,第二大股东是中国太平保险集团公司,第三大股东是富通保险国际。
目前,公司注册资本金37.3亿元人民币,总部设在上海,已在国内27个省、自治区和直辖市开设34家分公司和700余家三、四级机构,服务网络基本覆盖全国。
复业以来,太平人寿以科学发展观为统领,以人为本,以创新为突破,形成并强化核心竞争优势,实现跨越式发展。
目前,公司总资产突破1000亿元人民币,2006年—2009年公司的总资产分别是295亿、460亿、560亿、799亿,公司总资产历年平均增长速度保持在100%以上。
客户总量超过1000万,总承保金额累计突破14800亿元人民币,稳居国内中大型寿险公司行列。
2010年3月19日,太平人寿保费收入仅用78天就实现百亿平台突破,达到日均保费收入1.29亿元,自2001年复业以来,保费收入年复合增长率始终保持在50%左右,是市场同期增长率的两倍以上,自2006年开始连续四年实现香港会计准则和中国会计准则下的“双盈利”。
2007年至2010年,太平人寿连续四年跻身“中国企业500强”和“中国服务业企业500强”。
2009年,亚洲寿险公司综合竞争力由第26位跃居第9位,2010年,继连续六年为太平人寿做出BBB+评级后,国际权威评级机构惠誉国际(FITCH)将太平人寿评级由BBB+上调至A-级,评级展望为“稳定”,认为公司有较好的商誉、管理水平、经营环境和发展前景,具有较强的偿付能力和抗风险能力。
团体人身意外伤害保险投保单

中国太平洋财产保险股份有限公司投保单
投保单编号:
填写说明:1. 请务必准确填写标注“”的信息,如需要电子保单的,请务必准确填写联系人“电子邮箱”地址;
2.如曾经填写过相关信息的,仅需填写名称全称、组织机构代码,以及新增或变更的信息;
3.如在所提供的证照复印件及其他投保材料上已有的信息,可不必填写;
投保人、被保险人补充信息团体客户
特别提示:根据反洗钱相关监管要求,客户应提供身份信息及身份证明文件,配合金融机构履行客户身份识别工作;
团体人身意外伤害保险承保信息
如填写不下,可另附页。
人身保险个人投保单范本

人身保险个人投保单范本兹拟向某某保险公司投保人身保险,内容如下:投保单编号:保险种类投保人情况:姓名身份证号码与被保险人关系地址邮编电话被保险人情况:姓名年龄性别身份证号码地址邮编电话保险年期保险份数受益人领取日期领取年龄领取方式领取金额保险期限自____年____月____日中午12时起至____年____月____日中午12时止基本保险金额附加保险金额意外伤残保额意外身故保额疾病伤残保额疾病身故保额满期保险金额生存给付金费率附加险别保额费率附加险别保额费率保险费保险本金缴费形式一次性缴费□年缴□半年缴□季缴□月缴□其他:付款方式币种开户银行帐号特别约定:被保险人健康状况:1.目前尚在病假中? □有□无2.因病休或因病减轻劳动量? □有□无 3.因患有其他慢性病而不能全勤工作或经常缺勤? □有□无4.有无严重病史? □有□无5.癌症、肝硬化、癫痫病、脑震荡、精神病、心脏病、高血压病、血管硬化、性病等? □有□无投保人是否健康? □是□否投保声明:1)本投保单所填写的各项内容,均属真实,可作为你公司签发保单的根据,并成为双方合约的组成部分,如日后发现与事实不符,即使保单签发,你公司仍可不负任何责任。
2)本投保单方格内填列者,即作为本投保人“同意”或“是”的答复。
3)保户在投保时应填具确实年龄,保户年龄计算以身份证为根据,计算办法以保户在起保日最后一个生日时的足岁年龄计算,如误将年龄报小,应随时申请更正,并补缴保费及其利息,否则在发生给付时,其应得利益当按保户所付保费与实际年龄应付保费之比例计算。
投保人(签章)____年____月____日(以下由保险公司填写)审核意见:审核人(签章)________公司章____保险单号码:________签单人代码:____签单日期:____年____月____日相关阅读人身保险个人投保单_合同范本全文兹拟向中国平安保险股份有限公司投保人身保险,内容如下: 投保单编号:----------------------------------------------------| 保险种类| |--------|-----------------------------------------| |投保人| 姓名| 身份证号码| 与被保险人关系|| |----|--------------------------------|--------| |情况| 地址|邮编| |电话||---|----|-----------------|---|-------|-----------| |被保险| 姓名| 年龄|性别|身份证号码|| |----|-----------------|---|-------|-----------||人情况| 地址|邮编|电话|--------|-----------------|-----------|-----------| | 保险年期| 保险份数|受益人|领取日期||--------|-----|------|----|----|------------------| | 领取年龄| 领取方式|领取金额||--------------------------------------------------| | 保险期限自年月日中午12时起至年月日中午12时止|--------------------------------------------------| | 基本保险金额附加保险金额|----------------------------------|---------------| | 意外伤残保额| 附加险别|| 意外身故保额| 保额|| 疾病伤残保额| 费率|| 疾病身故保额||| 满期保险金额||| 生存给付金| 附加险别||| 保额|| 费率| 费率||---------|----------------------------------------| | 保险费||---------|----------------------------------------| | 保险本金||---------|----------------------------------------|| 缴费形式 |一次性缴费□年缴□半年缴□季缴□月缴□其他: |---------|----------------------------------------|| 付款方式| 币种||---------|------------------------|------|--------|| 开户银行| 帐号|---------------------------------------------------- --------------------------------------------------- |特别约定:||||-------------------------------------------------| |被保险人健康状况:| 1.目前尚在病假中? □有□无| 2.因病休或因病减轻劳动量? □有□无| 3.因患有其他慢性病而不能全勤工作或经常缺勤? □有□无| 4.有无严重病史? □有□无| 5.癌症、肝硬化、癫痫病、脑震荡、精神病、心脏病、高血压病、血管硬化、性病等? □有□无||投保人是否健康? □是□否||-------------------------------------------------||投保声明:| 1)本投保单所填写的各项内容,均属真实,可作为你公司签发保单的根据,并成为双方合约的组|成部分,如日后发现与事实不符,即使保单签发,你公司仍可不负任何责任。
(整理)太平保险财产综合险投保单填写模版
财产综合险投保单尊敬的客户,感谢您在我公司投保!请您仔细阅读保险条款,尤其是黑体字标注部分的条款内容,并听取保险公司业务人员的说明,如对保险公司业务人员的说明不明白或有异议的,请在填写本投保单之前向保险公司业务人员进行询问,如未询问,视同已经对条款内容完全理解并无异议(如有风险调查问卷,风险调查问卷亦作为本投保单的有效组成部分).太平财产保险有限公司财产综合险条款总则(盖章处)第一条本保险合同由保险条款、投保单、保险单或其他保险凭证以及批单组成。
凡涉及本保险合同的约定,均应采用书面形式。
保险标的第二条本保险合同载明地址内的下列财产可作为保险标的:(一)属于被保险人所有或与他人共有而由被保险人负责的财产;(二)由被保险人经营管理或替他人保管的财产;(三)其他具有法律上承认的与被保险人有经济利害关系的财产。
第三条本保险合同载明地址内的下列财产未经保险合同双方特别约定并在保险合同中载明保险价值的,不属于本保险合同的保险标的:(一)金银、珠宝、钻石、玉器、首饰、古币、古玩、古书、古画、邮票、字画、艺术品、稀有金属等珍贵财物;(二)堤堰、水闸、铁路、道路、涵洞、隧道、桥梁、码头;(三)矿井(坑)内的设备和物资;(四)便携式通讯装置、便携式计算机设备、便携式照相摄像器材以及其他便携式装置、设备;(五)尚未交付使用或验收的工程。
第四条下列财产不属于本保险合同的保险标的:(一)土地、矿藏、水资源及其他自然资源;(二)矿井、矿坑;(三)货币、票证、有价证券以及有现金价值的磁卡、集成电路(IC)卡等卡类;(四)文件、账册、图表、技术资料、计算机软件、计算机数据资料等无法鉴定价值的财产;(五)枪支弹药;(六)违章建筑、危险建筑、非法占用的财产;(七)领取公共行驶执照的机动车辆;(八)动物、植物、农作物。
保险责任第五条在保险期间内,由于下列原因造成保险标的的损失,保险人按照本保险合同的约定负责赔偿:(一)火灾、爆炸;(二)雷击、暴雨、洪水、暴风、龙卷风、冰雹、台风、飓风、暴雪、冰凌、突发性滑坡、崩塌、泥石流、地面突然下陷下沉;(三)飞行物体及其他空中运行物体坠落。
人身保险投保单(电子版).pdf
投保单号:人身保险投保单(电子版)■ 我已阅读人身保险投保提示 预选保险合同号码投保人资料姓 名: 性别: 出生日期: 年 月 日婚姻状况: 国籍: 户籍: 省 市 文化程度:证件类型: 证件有效期至:年 月 日证件号码 职业代码:单位名称: 在职情况: 部门及工作内容:单位电话: 住址电话: 移动电话:与被保险人关系: E-mail:现住址或单位地址: 邮编:联系电话:被保险人资料姓 名: 性别: 出生日期:年 月 日婚姻状况: 国籍: 户籍: 省 市 文化程度:证件类型: 证件有效期至:年 月 日证件号码: 职业代码:单位名称: 在职情况: 部门及工作内容:现住址或单位地址: 邮编:单位电话: 住址电话: 移动电话:受益人资料姓名 性别 出生日期证件类型 证件号码 与被保险人关系受益顺序 受益份额(%)身故保险金满期/生存保险金/生存年金1.若未指定身故保险金受益人,则身故保险金作为被保险人的遗产,依法给付。
2.若未指定受益顺序及受益份额,则保险金由所有指定受益人平均分配。
3.其他保险金受益人为被保险人本人。
601120000000312 A65787654小王男19810720已婚中国北京北京本科台湾通行证长期12345674030504新光海航人寿保险在职 保险************本人北京市朝阳区建国路100022************小王男19810720已婚中国北京北京本科台湾通行证长期12345674030504新光海航人寿保险在职 保险北京市朝阳区建国路100022************保障计划险种名称保险期间交费期间 基本保额/份数/档次保险费主险附加险保险费合计(以人民币“元”的整数为计算单位;角、分数须四舍五入)(人民币大写) 仟 佰 拾 万 仟 佰 拾 元整 ¥ 元交费方式: 一年期主险/一年期附加险申请续保: 首期保险费交费途径: 续期保险费交费途径:选择保险费自动垫交功能:生存保险金约定年龄:生存年金领取方式:红利选择方式:保险费授权转账账户 开户银行: 银行 省 市 网点名称:户名(即投保人): 账号告知内容 (以下资料是否书面如实告知,将直接影响您的申请是否通过核保及获得理赔,请您仔细阅读,如实填写。
太平人寿电子投保确认书
E 保确@回国末m CHINA TAIPI ~J.::节9嘿险有限公司URANCE CO.,LTD.认书本人《人身保险投保单(时)>>投保单号:I根据《人身保险新型产品信息披露管理办法》规定,如投保的险种中包括分红保险、万能保险或投资连结保险请在下方空格抄录:本人已阅1卖保险条款、产口口口说E 刀目书和投保t 工足日刁τ书,了解本产口口口的特占和保单中'f'11叫u 益向S~μJ 不确足~性。
投保人签名被保险人(或其法定监护人)签名代理人签名一一一年一一一月一一一日签署日期h O 寸,..o N(3)如果您选择购买万能保险产品,请您注意以下事项:万能保险产品通常有最低保证利率的约定,最低保证利率仅针对投资账户中资金。
您应当详细了解万能保险的费用扣除情况,包括初始费用、死亡风险保险费、保单管理费、手续费、退保费用等。
您应当要求销售人员将万能保险账户价值的详细计算方怯对您进行解释。
万能保险产品的技资回报具有不确定性,您要承担部分投资风险。
保险公司每月公布的结算利率只能代表一个月的投资情况,不能理解为对全年的预期,结算利率仅针对技资账户中的资金,不针对全部保险费。
产品说明书或保险利益测算书中关于未来保险合同利益的预测是基于公司精算假设,最低保证利率之上的投资收益是不确定的,不能理解为对未来的预期。
如果您选择灵活交费方式的,您应当要求销售人员将fg停止交费可能产生的风险和不利后果对您进行解释。
七、请您正确认识人身保险新型产品与其他金融产品分红保险、投资连结保险、万能保险等人身保险新型产品兼具保险保障功能和投资功能,不同保险产品对于保障功能和投资功能侧重不同,但本质上属于保险产品,产品经营主体是保险公司。
您不宜将人身保险新型产品与银行存款、国债、基金等金融产品进行片面比较,更不要仅把它作为银行存款的替代品。
八、选择健康保险产品时请您注意产品特性和条款具体约定健康保险产品是具布较强风险保障功能的产品,既有定额给付性质的,也有费用补偿性质的。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
2
F、注意事项(NOTES)
以下注意事项需要您特别关注:
The following notes are brought up to your attention.
* 所有保费、保障利益和保额在报价时以人民币为单位
All premiums, benefits and policy limits will be quoted in RMB¥.
精选型 Select
Insurance program 舒适型 菁英型 Premier Elite
其他 Others
环球 Worldwide
承保区域 Geographical area
环球(不包含美国以及加勒比海) Worldwide excluding USA & the Caribbean
合计人数 Total:
单位名称
Company Name
单位地址
Address
邮政编码
Postcode
单位总人数
Number of
行业类别
Nature of business
机构分布区域
Company
单位性质
Company
□ 地市 local □ 省/市 Provincial □区域 Regional□全国 Nationwide □跨国 Worldwide □其他 Other
未决赔款 Outstanding claims
reserves
投保员工人数
Number of employees insured
目前的保险方:
Current Insurer:
在此次投保的被保险员工中,是否有个人理赔金额在某年超过或预计将超过 8 万元人民币的情况?
Among all employee covered in this scheme,do any of the years include individual claims which exceed or are expected to exceed RMB80,000 ?
合计人数 Total:
备注:* 各投保计划类型以及承保区域的人数均为合计值。
* 如为定制计划,请在投保计划“其他”中填写。
Note: * The numbers of insured under each insurance program and geographic area are the total.
□ 国有 State-owned □集体 collectively-owned □私营 Private □个体 Individual □股份制 Joint-stock □ 三资 Joint-venture□政府机关 Governmental □事业单位 Organizational □社会团体 Social Group □其他
付款方式
□现金 Cash □现金支票 Draft □ 转帐支票 Transfer Check
Payment Method
□转帐 Transfer
□其它 Other
C、保费及承担比例(premium & premium contribution)
□ 单位全额承担/Non-Contributory(employer pays only)
保险联系人
Contact Person
电子邮箱
职务/部门
Job
手机
Mobile Phone
联系电话
Contact Phone
传真
Fax
B、保险期限与交费信息(COMMENCEMENT DATE AND PREMIUM PAYMENT)
生效日期
年
月
日零时起
Commencement Date
□ 个人按比例分担/ Contributory and the employee pays
%
□ 个人承担/ Contributory and the employee pays only
□ 合计保费 premium total:
1
D、被保险人投保汇总信息(CENSUS)
* 所有投保人员的详细信息请在“被保险人清单”或“员工申请表”中填写。
Please complete the details of applicants in the separate “INSURED NAME LIST” or “EMPLOYEE APPLICATION FORM”.
投保员工人数信息 (Number of employee)
投保计划
等级 Sub-group
* 中文内容具有法律效力,英文翻译仅供参考。
The English wordings used in this form is for reference only.Should there be any discrepancies in language.Please refer to Chinese wordings.
本公司已完全了解并明白,有关保险条款以及相关情况,是本公司与太平人寿之间合同有效的基础,保障责任只有在太平人寿 确认保费已经到帐,并且向本公司提供书面确认后方可生效。
We understand that the information provided, together with the Policy Terms and Conditions forms the basis of the contract between the Employer and TAIPING LIFE. Coverage under the policy is only effective when written confirmation is provided by TAIPING LIFE and the premium has been settled in full.
* 我们所假定 19 岁以上子女是指接受全日制教育,在经济上依赖他们的父母。若情况不是这样,请提供更详细的信息。
It is assumed that all children over 19 years of age are in full time education and are financially dependent on their parent(s). If this is not the case, further information will be required.
Is there an existing scheme for medical care? YES
NO
If yes, please complete details below.
保险期间 (近两年)
Period of experience
合计保费
Total premium
合计理赔金额
Total claims paid
在近 12 个月的时间里,任何投保保险的员工或其附属被保险人是否发生过身体健康方面的问题?
Are you aware of any employees or dependents to be insured who have experienced any health problems in the last 12 months?
附属被保险人人数信息 (Number of dependant)
投保计划
Insurance program
精选型
舒适型
菁英型
Select
Premier
Elite
其他 Others
环球 Worldwide
承保区域 Geographical area
环球(不包含美国以及加勒比海) Worldwide excluding USA & the Caribbean
若是,请另附表格描述详情
是□ 否
(详细信息应包含:理赔日期、申请人、原因、现有理赔金额、应赔付未赔付以及预计赔款)
YES No
If yes, please provide details on a separate sheet.
Details should include the date of claim, claimant, cause, amount paid and due to be paid and current prognosis
条形码:10 流水+2 位校验+050
业务员 1 姓名:
业务员 2 姓名: 销售渠道:
业务员 1 代码:
业务员 2 代码: 中介机构代码:
太平人寿保险有限公司团体人身保险投保单
GROUP INSURANCE APPLICATION CERTIFICATE
A、投保单位资料(DETAILS OF INSURED COMPANY)
* 只有在所有保障计划中员工都是管理层的情况下,条款保费才可以适用。对于直接从事危险性、体力劳动的员工只有 在提供进一步信息后方可考虑承保。
Premiums are quoted on the assumption that all employees to be covered are administrative staff only. If any employees are directly involved in hazardous or manual work, further information will be required.
是
否
若是,请另附页说明详细情况.
YES
NO
If YES, please attach details.
声明事项:(DECLARATION)
本公司声明所作陈述均真实可信。.
We declare that the statements made are correct to the best of our knowledge and belief.