健康险中英文理赔申请书
健康保险理赔申请书范本
健康保险理赔申请书范本尊敬的保险公司:您好!我是贵公司的投保人,保单号为XXXXXXXXXXX。
在此,我向您提交一份健康保险理赔申请书,希望能得到您的关注和支持。
一、事故经过于XXXX年XX月XX日,我因突发疾病,被送往XXXX医院就诊。
经诊断,我患有XXXX病。
在治疗期间,我总共花费了XXXX元。
根据我国健康保险相关规定,我希望能获得贵公司的理赔支持。
二、理赔依据1. 投保单:我于XXXX年XX月XX日与贵公司签订了健康保险合同,保单号为XXXXXXXXXXX。
2. 身份证明:我已提供有效的身份证件,以证明我是贵公司的投保人。
3. 医院出具的病历资料:我已提供XXXX医院出具的病历资料,包括诊断书、住院记录、医疗费用清单等,以证明我确实患有XXXX病,并进行了相关治疗。
4. 医疗费用发票:我已提供医疗费用发票,金额为XXXX元,以证明我在治疗期间产生的实际费用。
三、理赔请求根据我国健康保险相关规定和贵公司保险合同的约定,我希望贵公司能尽快核实我的理赔申请,并按照合同约定支付我的医疗费用。
具体理赔金额为XXXX元,其中包括住院费用、药品费用、检查费用等。
四、承诺1. 我承诺所提供的信息真实、完整,无任何虚假陈述。
2. 我承诺在收到贵公司理赔款项后,不再就此次事故向贵公司提出任何索赔。
3. 我承诺在此次理赔过程中,遵守法律法规,服从贵公司的理赔决定。
五、联系方式为确保贵公司能尽快核实理赔申请,特此提供以下联系方式:联系电话:XXXXXXXXXXX联系地址:XXXXXXXXXXX邮编:XXXXXX敬请贵公司尽快核实并处理我的理赔申请,感谢您的关注和支持!此致敬礼!投保人:(签名)XXXX年XX月XX日。
医疗责任险索赔申请书
医疗责任险索赔申请书英文回答:Medical Malpractice Claim Application.This application is to be used to file a claim for damages resulting from medical malpractice. Please complete all sections of the application and submit it to the appropriate party.Section 1: Patient Information.Patient Name:Date of Birth:Address:Phone Number:Email Address:Section 2: Provider Information. Physician/Provider Name:Medical Facility Name:Address:Phone Number:Email Address:Section 3: Incident Information. Date of Incident:Time of Incident:Location of Incident:Description of Incident:Names of witnesses:Section 4: Medical Records.Please attach a copy of your medical records relatedto the incident.Section 5: Damages.Please describe the damages you have suffered as a result of the medical malpractice. This may include medical expenses, lost wages, pain and suffering, and other damages.Section 6: Signature.By signing below, you are certifying that the information provided in this application is true and accurate to the best of your knowledge.Signature:Date:Contact Information.If you have any questions or need assistance completing this application, please contact the following:Name:Phone Number:Email Address:中文回答:医疗责任险索赔申请书。
2012年中英人寿理赔申请书

V团体医疗保险理赔申请书一
■出险人信息
■事故经过及申请险种
事故经过描述:
申请险种:
■其它告知事项:
被保险人是否已获得/正在申请/准备申请其他保险公司、社保、其他福利保障计划或第三者的给付或补
偿:。
是O否■若为是,清详述其它公司或机构名
I称:O
■声明与授权:(签名前请再次核对所填资料是否完整无误)
1、本人声明所提交的全部证明文件资料(包括本中清书填写的内容)均属实,并作为保险事故的凭据;
2、本人授权中英人寿保险有限公司及代表向任何医院、医生、公安部门、保险公司或相关组织机构查询、复印或以其他方式取得
有关保险事故的相关材料;
3、本人授权中英人寿保险有限公司将理赔款项划帐至指定银行帐户,若转帐成功即视为本人已领取相应款项。
开户户名,银行名称,
开户网点,省(市) __________________________ 地市(请填写具体网点)
帐号,存折□银行卡口(请勾选)
4、本人己知悉贵公司理赔完毕后将保留已报销的票据并不接受退还票据的申请。
投保单位盖章:
申请人签名: 日期:。
中英人寿理赔申请书(新版)

事故者(被保险人)资料:投保人名称保险单号被保险人姓名性别年龄证件号码事故类型医疗医疗原因:○疾病门诊○疾病住院○意外伤害门诊○意外伤害住院就诊时间:年月日就诊医院:若住院,入/出院日期:年月日至年月日有无手术:○有○无重大疾病疾病名称:就诊医院:确认日期:残疾残疾原因:○疾病○残疾残疾程度:身故身故原因:○疾病○意外身故日期:年月日身故地点:保险金及领取方式:索赔金额:元单据数量:张领取方式:授权中英人寿保险有限公司银行自动转帐银行名称:○中国工商银行○招商银行○其他:户名(保险金受益人):账号:开户银行所在地市:卡折标志:○银行存折○银行卡授权声明:1)本人授权中英人寿将相应理赔款直接划入授权账户;2)本人尽量保持领款授权账号的一致性,如有不同,请中英人寿以最后一次提供的授权账号为准;3)中英人寿将相应款项成功划账至上述授权账户,即视为本人已领取相应款相。
授权人签名:日期:年月日注:如果提供其他银行帐号,请详细填写:XX银行XX分行XX支行XX储蓄所团体保险理赔申请书保险事故经过及结果描述:受益人资料:姓名证件号码与被保险人关系联系电话被保险人是否已获得/正在申请/准备申请其它保险公司、社保、其它福利保障计划或第三者的给付或补偿:○是否若为是,请详述其它公司或机构名称:1、本人声明所提交的全部证明文件资料均属实、本申请书上填写的内容详尽确实,并作为保险事故的证据;2、本人授权中英人寿保险有限公司及其代表向任何医院、公安部门、其他组织机构及个人查询、调阅、摘抄、复印/制或取得任何有关事故人的所有健康及其他相关资料,本人愿承担由此产生的一切法律后果;3、本已知悉贵公司理赔完毕后将保留已报销的票据并不接受退还票据的申请。
申请人签名:联系电话:日期:年月日投保人证明或意见:投保人盖章:说明:1、请逐项如实填写并由申请人(受益人或其法定监护人)本人亲笔签名确认;2、请您参照下表提供您所能提供的完整相关资料。
健康保险理赔申请书范本
健康保险理赔申请书范本尊敬的保险公司:我是您公司的保险客户,持有健康保险合同,合同编号为[合同编号]。
我不幸遭受疾病/意外事故,需要根据合同规定向您提出理赔申请。
根据您公司要求,我特此向您提交申请并提供相关资料,希望能够得到您的快速处理和赔付。
一、个人信息姓名:[被保险人姓名]证件类型:[身份证/护照/驾驶证等]证件号码:[证件号码]联系地址:[联系地址]联系电话:[联系电话]手机号码:[手机号码]电子邮箱:[电子邮箱]二、理赔事故信息理赔类型:[医疗费用/住院津贴/手术津贴/重大疾病/身故/残疾等]事故发生时间:[事故发生时间]事故地点:[事故地点]事故详细描述:[事故详细描述]三、就诊信息就诊医院名称:[就诊医院名称]就诊科室:[就诊科室]就诊医生姓名:[就诊医生姓名]诊断结果:[诊断结果描述]四、理赔费用信息申请理赔金额:[申请理赔的具体金额]费用详细清单:1. 医疗费用:- 项目1:[费用1]- 项目2:[费用2]- ...2. 住院津贴:- 入院日期:[入院日期]- 出院日期:[出院日期]- 津贴金额:[津贴金额]- 津贴天数:[津贴天数]3. 手术津贴:- 手术名称:[手术名称]- 手术日期:[手术日期]- 津贴金额:[津贴金额]4. 其他费用:- 描述:[费用描述]- 金额:[费用金额]五、附件清单以下是我提交的相关附件,请查收:1. 身份证/护照/驾驶证复印件2. 就诊医院的诊断证明/病历/出院小结复印件3. 费用发票原件及复印件4. 医疗费用明细报告及复印件5. 其他相关证明材料请您在收到本申请书和相关附件后,尽快审查并给予回复。
如有需要,我愿意配合提供进一步的资料或进行面谈。
我希望您能够尽快处理我的理赔申请,遵守合同约定,按时支付理赔款项。
特此申请。
申请人签名:日期:[申请日期]。
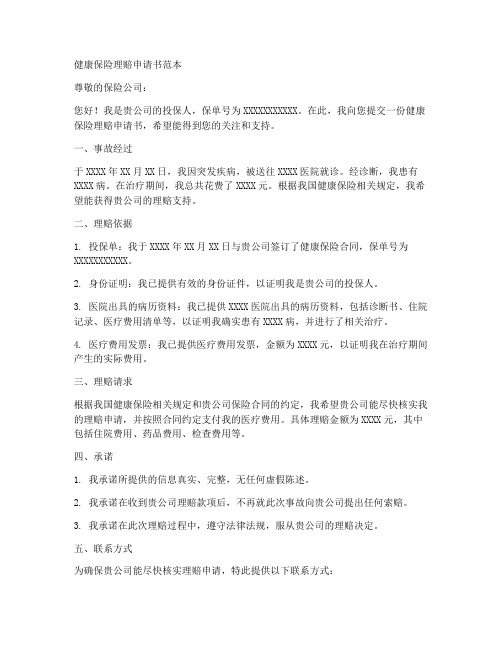
医疗理赔申请书 Claim Application-中国平安健康保险股份有限公司
该理赔申请书适用于住院 /门诊医疗费用、住院津贴、重疾理赔申请。 This document is an application form for claim settlement of all inpatient and outpatient medical expenses, inpatient allowance and claims for Critical Illness policies. 您需要做的: 步骤一:请您用正楷填写此表格 步骤二:请附加如下理赔申请材料: ▲ 1. 被保险人的身份证明 复印件(与投保 时一致) 2. 医疗费用收据(发票)原件 * 3. 费用明细清单复印件 ** 4. 医疗资料复印件,包含但不限于: 出院小结(住院理赔) 门诊病历资料 与之相关的检查结果,如 X 线检查、病理检查等。 5. 如账户信息第一次使用,请提供账户信息复印件 步骤三: 您可以使用以下任意一种方式提交表格 如果您是团体客户,请将理赔材料提交至您的人事部联系人 向您认识的平安健康险业务员提交理赔材料 将所有理赔材料邮寄至保单承保所在地的平安机构 (机构地址详见 ) 注意: *申请住院津贴请提供复印件 **申请住院津贴无需提供费用清单 **重疾申请无需提供费用收据及清单 ▲中国大陆二代身份证请提供正反面复印件 What you should do: Step 1: Fill in this Claim Application Form using block letters. Step 2: Attach the following materials to this Claim Application Form:
1、出险者信息 Details of the insured
出险者姓名 Full Name 证件类型 ID Type 证件号码 ID Number 联系电话 Telephone Number 电子邮件 Email Address 分单号 Sub-Policy Number
理赔申请书英文

理赔申请书英文Dear Sir/Madam,I am writing to formally submit a claim for reimbursement under my insurance policy number [Policy Number], which I believe is applicable to the recent incident that occurred on [Date of Incident].The unfortunate event that has prompted this claim took place at [Location of Incident], where my [describe the item or situation] was [describe the incident briefly]. I have taken the necessary steps to mitigate the damage and have gathered all relevant documentation to support my claim.Enclosed with this letter, you will find a detailed account of the incident, including photographs of the damage, a police report if applicable, and an itemized list of the costs incurred as a result of the incident. I have also attached a copy of my insurance policy and proof of payment for the premiums.I trust that you will find the enclosed documentation sufficient for the processing of my claim. I am eager to resolve this matter promptly and am available for any further clarification or information that may be required.Thank you for your attention to this matter. I look forward to a favorable and expeditious resolution.Sincerely,[Your Name][Your Contact Information]。
意外健康险理赔申请书范本

意外健康险理赔申请书范本
尊敬的保险公司:
我是贵公司的客户,保单号为XXXXXXXXXXX,我在此就我在XXXX年XX月XX日发生的一起意外事故提出理赔申请。
事故发生当天,我在家中进行日常清洁时,不慎滑倒,导致右腿骨折。
我立即被送往附近的医院进行治疗,经过医生的诊断,我需要接受手术治疗,并需要一定时间的康复。
在治疗期间,我共计花费了医疗费用人民币XXXX元,其中包括手术费、住院费、药品费等。
我持有所有的医疗单据和费用清单,以供贵公司审核。
作为一名意外健康保险的客户,我希望贵公司能够根据保险合同的约定,对我的医疗费用进行赔付。
我在投保时,是根据贵公司的保险条款和费率进行投保的,我相信贵公司会履行合同义务,对我的理赔申请给予积极的处理。
在此,我提供了所有必要的文件和证明材料,包括事故报告、医疗单据、费用清单等。
我希望贵公司能够尽快审核我的理赔申请,并给予合理的赔付。
我对贵公司的服务一直抱有良好的信任和评价,我相信贵公司会以专业的态度和高效的服务,处理我的理赔申请。
感谢贵公司对此事的关注和处理,我期待着贵公司的回复。
此致
敬礼
申请人:(签名)
XXXX年XX月XX日。
2024年健康保险索赔申请书信模板

2024年健康保险索赔申请书信模板尊敬的保险公司管理团队:我是您公司的保险投保人之一,持有有效的健康保险政策。
我在此信中向贵公司提出索赔申请,详细情况如下:1. 被保险人信息:姓名:性别:出生日期:保险单号:联系地址:联系电话:2. 患病/受伤情况:我于2024年XX月XX日(病情发生的具体时间)因(病情或受伤原因)导致了(所诊断的疾病或损伤)。
3. 就医信息:医疗机构名称:医生姓名:就诊日期:就诊科室:诊断结果:4. 检查和治疗信息:我接受了以下的检查和治疗(列举具体项目和日期)。
这些检查和治疗的费用已经支付,我现在希望能够得到相应的保险赔付。
5. 费用结算情况:我已经支付了上述的医疗费用,并附上了相关的费用凭证和发票。
以下是这些费用的详细清单:费用类型费用金额(人民币)日期----------------------------------------------------------------------检查费用:治疗费用:药品费用:其他费用:6. 附加材料:我还随信附上了以下的文件和材料,以支持我的索赔申请:- 医生的诊断证明和医疗记录- 检查和治疗的费用发票和凭证- 其他支持申请的文件和证据我诚恳地希望贵公司能够尽快处理我的索赔申请,并及时支付相应的保险赔付款项。
我深信,在贵公司专业和高效的处理下,我的申请将得到公正的评估和妥善的处理。
如有需要,我愿意提供进一步的文件或信息以支持我的索赔申请。
您可以通过以下联系方式与我取得联系:联系人:联系地址:联系电话:再次感谢您的关注和支持。
期待您的积极回复。
此致,保险投保人签名日期。
人保健康理赔申请书模板
人保健康理赔申请书模板:尊敬的人保健康保险公司:您好!我是贵公司的保险客户,保单号为(填写保单号),在此向您提交我的理赔申请。
请您予以审核并给予相应的理赔处理。
一、出险情况(1)出险时间:____年__月__日 __时__分(2)出险地点:____________________(3)出险经过:____________________(4)出险结果:____________________二、申请理赔项目(1)医疗费用:____________________(2)住院费用:____________________(3)重大疾病保险金:____________________(4)身故保险金:____________________(5)其他费用:____________________三、理赔资料1. 保险合同原件及复印件2. 身份证件原件及复印件3. 银行卡/存折原件及复印件4. 医院出具的病历报告、诊断书、发票等原件及复印件5. 出险事故报告及相关证明材料6. 其他贵公司要求提供的资料四、理赔方式(1)银行转账:____________________(2)支付宝/微信转账:____________________(3)现金支付:____________________(4)其他方式:____________________五、申请理赔金额(1)医疗费用:人民币(大写):____________________元整(2)住院费用:人民币(大写):____________________元整(3)重大疾病保险金:人民币(大写):____________________元整(4)身故保险金:人民币(大写):____________________元整(5)其他费用:人民币(大写):____________________元整总金额:人民币(大写):____________________元整六、申请人声明本人承诺所提供的资料真实有效,如有虚假陈述,本人愿意承担相应的法律责任。
平安个人医疗保险理赔申请书模板

英文回答:I am writing to formally submit a claim for reimbursement of my medical expenses under the Ping An personal medical insurance policy. I underwent a surgical procedure for a chronic illness and believe that these expenses are covered under the terms of my insurance policy. Enclosed, please find all necessary documentation including medical bills, physician's diagnosis, and any other pertinent information to substantiate my claim. I trust that the insurancepany will expeditiously process my claim and provide the appropriate reimbursement for my medical expenses. Thank you for your prompt attention to this matter.现函正式提出平安个人医疗保险保单报销医疗费用要求。
我接受过慢性病的手术并相信这些开支在我的保险单条款。
随函附上一切必要文件,包括医疗账单、医生诊断和任何其他相关资料,以证实我的说法。
我相信,保险公司将迅速处理我的索赔,并适当偿还我的医疗费用。
谢谢你迅速关注此事。
Hey, I just want to let you know that I've been a loyal customer of Ping An for years. I always make sure to pay my premiums on time and I've never had to make a claim before. I'm pretty sure I've met all the requirements in my policy to get reimbursed formy medical expenses. I really hope the insurancepany takes all this into consideration and gives me the help I need with my claim. Thanks!嘿,我只是想告诉你,我多年来一直是平安的忠实客户。
理赔申请书申请事项

理赔申请书申请事项English: When completing a claims application, it is important to provide accurate and detailed information regarding the incident that led to the claim. This includes providing the date and time of the incident, a clear description of what happened, and any supporting evidence such as photographs or witness statements. Additionally, it is necessary to provide all relevant personal information, such as the policyholder's name, contact details, and policy number. If there are any injuries or medical expenses involved, it is crucial to provide all relevant medical documentation and receipts. It is also important to include any other relevant documents, such as police reports or repair estimates for property damage. It is crucial to submit the claims application as soon as possible, as delays may affect the processing time. When filling out the claims application, it is important to be honest and thorough, providing all necessary information without exaggeration or omission. This will help ensure a smooth and efficient claims process.中文翻译: 在填写理赔申请书时,提供关于导致理赔所需的事故的详细准确信息非常重要。
脚踏空扭伤理赔申请书

脚踏空扭伤理赔申请书【中英文版】**Application for Compensation Due to Sprained Ankle from Falling** 尊敬的保险公司,我谨以此信向贵公司提出一次意外伤害理赔申请。
具体情况如下:**On the morning of March 15th, while walking in our office building, I accidentally stepped on an uneven floor and suffered a sprained ankle.The incident occurred at approximately 10:00 AM.**2023年3月15日早晨,在我走进我们办公楼的时候,我不小心踩到了一个不平衡的地板,导致我脚踝扭伤。
这一事件大约发生在上午10点。
**The pain was immediate and severe, causing me to visit the nearest hospital for medical attention.After examination, the doctor diagnosed a moderate sprain and recommended rest, ice packs, and elevation for the next few days.**受伤后,我立刻感到剧痛,因此我前往最近的医院接受治疗。
经过检查,医生诊断我为中度扭伤,建议我接下来几天休息,并使用冰袋冷敷,抬高伤脚。
**I have followed the doctor"s orders and am currently unable to perform my regular duties.As a result, I am seeking compensation for the medical expenses incurred, loss of wages during my recovery period, and any other related costs.**我已经按照医嘱进行治疗,目前无法正常工作。
北京普惠健康保理赔申请书

北京普惠健康保理赔申请书
尊敬的北京普惠健康保理赔部门:
我是[XXXXX](申请人姓名),身份证号码XXXXXXXXXXXXXXXXXX,联系电话XXXXXXXXXXX。
我为被保险人[XXXXX](被保人姓名)提交此次理赔申请。
被保人身份证号码为XXXXXXXXXXXXXXXXXX,联系电话XXXXXXXXXXX。
本次申请的事由是被保人在XXXX年XX月XX日至XXXX年XX月XX日期间,因患有XX病在XX医院接受了治疗。
就诊期间,被保人共计花费了医疗费用XXX元,其中包括住院费用XXX元和门诊费用XXX元。
我请求贵部门对被保人所发生的医疗费用进行理赔。
我已经收集了相关的医疗费用单据和发票,包括住院发票、门诊发票以及医生的诊断证明和治疗记录等。
所有提供的资料都是真实、完整、准确的,并加盖了医院的公章。
被保人所接受的治疗和使用的药品均符合保险责任范围。
其中,使用的特殊药品和进口设备都经过了国家相关部门的批准和认证。
我也将提供相应的证明文件。
为了尽快获得理赔款项,我请求贵部门给予快速且合理的审批待遇。
我相信贵部门会秉持公正原则,对本次理赔申请进行审批。
在此,我承诺所提供的一切资料和信息都是真实、准确的,如有虚假,愿意承担相应的法律责任。
同时,我也期待贵部门能够提供优质的服务,确保本次理赔申请能够顺利完成。
最后,我衷心希望贵部门能够及时处理并支付已通过审核的理赔款,以缓解我们当前的经济困境。
申请人:[XXXXX]
联系电话:XXXXXXXXXXX 日期:XXXX年XX月XX日。
索赔申请书

索赔申请书英文回答:Dear [Insurance Company Name],。
I am writing to submit a claim for [type of claim] that occurred on [date of claim]. I was involved in an accident at [location of accident] at approximately [time of accident].The accident involved [other vehicle(s)/object(s) involved]. I was driving a [make and model of vehicle]. The other vehicle(s)/object(s) involved was/were [make and model of other vehicle(s)/object(s)].I was injured in the accident and was taken to [hospital name] for treatment. I was diagnosed with [injuries sustained]. I am currently receiving medical treatment for my injuries.The accident was caused by the negligence of the other driver(s)/object(s). I was driving carefully and obeyingall traffic laws when the accident occurred.I am attaching the following documents to support my claim:A copy of the police report。
英语作文索赔信万能模板
英语作文索赔信万能模板[Title] Claim Letter Universal Template。
[Salutation]Dear [Insurance Company Name],。
I am writing this letter to file a claim for [nature of the claim, e.g. car accident, property damage, medical expenses, etc.]. The incident occurred on [date of the incident] and I am seeking compensation for the damages and losses incurred as a result.I am a policyholder with your company and have been faithfully paying my premiums for [duration of the policy]. I believe that the terms of my insurance policy cover the damages and losses that I have suffered, and I am therefore requesting that you process my claim in a timely manner.[Description of the Incident]Provide a detailed account of the incident, including the date, time, and location. If applicable, include any relevant information about the other party involved, such as their contact information and insurance details. Be sure to include any supporting documentation, such as police reports, medical records, or photographs, to substantiate your claim.[Extent of Damages]Detail the extent of the damages and losses you have suffered as a result of the incident. This may include property damage, medical expenses, lost wages, or any other relevant costs. Provide a breakdown of the expenses and attach any supporting documentation, such as repair estimates, medical bills, or pay stubs, to validate your claim.[Policy Coverage]Reference the specific sections of your insurance policy that you believe cover the damages and losses incurred. Provide a clear and concise explanation of how the incident falls within the scope of your policy coverage and why you are entitled to compensation.[Requested Compensation]Clearly state the amount of compensation you are seeking and provide a rationale for this amount. This may include a breakdown of the expenses incurred, as well as any additional compensation for pain and suffering, inconvenience, or other non-monetary losses.[Contact Information]Include your contact information, including your full name, policy number, address, phone number, and email address. This will ensure that the insurance company can easily reach you to discuss your claim and request any additional information or documentation if necessary.[Closing]Thank you for your prompt attention to this matter. I trust that you will process my claim fairly and expeditiously. I look forward to a swift resolution and am available to provide any further information or assistance that may be required.Sincerely,。
索赔申请书范文英文模板

赔偿申请书范本(英文)[Your Name][Your Address][City, State, ZIP Code][Email Address][Phone Number][Date][Recipient's Name][Recipient's Title][Company/Organization Name][Company/Organization Address][City, State, ZIP Code]Subject: Claim for CompensationDear [Recipient's Name],I am writing to formally submit a claim for compensation regarding the incident that occurred on [date of the incident]. As a loyal customer of [Company/Organization Name], I have always trusted in the quality and reliability of your products/services. However, my recent experience has left me disappointed and entitled to compensation.To provide some context, on [date of the incident], I purchased a [product/service] from [Company/Organization Name]. The item/service was specifically designed and advertised to meet certain specifications and standards. Unfortunately, upon using the product/service, I discovered several deficiencies and defects that rendered it unusable and unsatisfactory.The specific issues that I encountered are as follows:1. [Describe the first issue encountered]2. [Describe the second issue encountered]3. [Describe the third issue encountered]These issues not only caused inconvenience but also resulted in additional expenses and damages. As a result, I have suffered financial losses and personal inconvenience due to the faulty product/service provided by your company.In light of the aforementioned circumstances, I kindly request that [Company/Organization Name] addresses this matter promptly and fairly. I believe that it is only reasonable to compensate me for the inconvenience, additional expenses, and damages incurred as a direct result of the defective product/service.I haveattached all relevant documentation and evidence, including purchase receipts, photographs, and any other supporting materials, to support my claim. I真诚希望 [Company/Organization Name] will take my claim seriously and handle it with the urgency and importance it deserves.I would appreciate the opportunity to discuss this matter further and explore possible solutions. Please let me know the appropriate steps to take in order to facilitate a prompt and amicable resolution.Thank you for your attention to this matter, and I look forward to your prompt response.Sincerely,[Your Name]。
重疾险理赔申请书模板

尊敬的保险公司:
您好!我是贵公司的投保人,保单号码为:【保单号码】,在此,我向您提交我的重疾险理赔申请。
一、理赔背景
我在【投保日期】向您投保了【保险金额】元的重疾险,根据保险合同的约定,我享有在确诊患有合同约定的重大疾病时获得保险金赔付的权利。
近日,我在【就诊医院】进行了体检,并被诊断为【诊断疾病名称】。
根据医生的建议,我需要进行长期的治疗和康复。
在此,我向您提交重疾险理赔申请,希望能够得到贵公司的支持和帮助。
二、理赔材料
1. 保险合同原件及复印件;
2. 我的身份证件原件及复印件;
3. 理赔申请书,已填写完毕并签字;
4. 就诊医院的诊断证明书原件及复印件;
5. 相关的医疗费用清单、检查报告等,已加盖医院有效签章;
6. 其他与本次理赔相关的材料。
三、理赔请求
根据保险合同的约定,我已经满足了合同约定的重大疾病理赔条件。
在此,我恳请贵公司尽快审核我的理赔申请,并按照合同约定给予保险金赔付。
我深知重疾的治疗和康复过程需要大量的经济支持,希望能够得到贵公司的帮助,让我能够专心治疗,尽快康复。
四、声明
1. 我保证所提供的材料真实、完整、准确,如有任何虚假陈述,我愿意承担相应的法律责任;
2. 我授权贵公司查询、使用我的医疗信息,以便进行理赔审核;
3. 我同意贵公司按照合同约定处理我的理赔申请,并保密我的个人信息。
最后,再次感谢贵公司对我一直以来的关心和支持,期待您的回复,祝您工作顺利!此致
敬礼!
投保人:【投保人姓名】
联系方式:【投保人电话】
日期:【日期】。
理赔信函英语作文模板

理赔信函英语作文模板英文回答:Dear [Insurance Company Name],。
I am writing to file a claim for [type of claim]. I ama policyholder with your company under policy number [policy number].The incident occurred on [date of incident] at [location of incident]. I was [what you were doing when the incident occurred]. The incident resulted in [what happened as a result of the incident].I have enclosed the following documentation to support my claim:Copy of the police report (if applicable)。
Medical records (if applicable)。
Repair estimates or invoices (if applicable)。
Photographs of the damage (if applicable)。
I understand that I am required to cooperate fully with your investigation. I will provide any additional information or documentation that you may require.I am requesting reimbursement for the following expenses:[Expense 1][Expense 2][Expense 3]I believe that my claim is valid and should be covered under my policy. Thank you for your time and attention to this matter.Sincerely,。
英文理赔函作文范文

英文理赔函作文范文英文回答:Dear [Claim Adjuster's Name],。
I am writing to submit a claim for damages sustained to my property located at [address] as a result of [event that caused the damage].The incident occurred on [date] at approximately [time]. While I was [location or activity when the damage occurred], I noticed [signs of damage] and immediately contacted the authorities. The damage was caused by [cause of damage].I have attached several photographs and videos of the damage for your review. As you can see, the damage is extensive and has made my property uninhabitable. The following is a detailed list of the damages:[List of damages, including estimated cost of repairsor replacement]I have taken reasonable steps to mitigate the damage, such as [actions taken to mitigate the damage]. However, the damage remains significant and has caused me substantial financial loss.I am requesting that you promptly process my claim and reimburse me for the cost of repairs or replacement. I am available to provide any additional information or documentation that you may require.Thank you for your time and consideration.Sincerely,。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
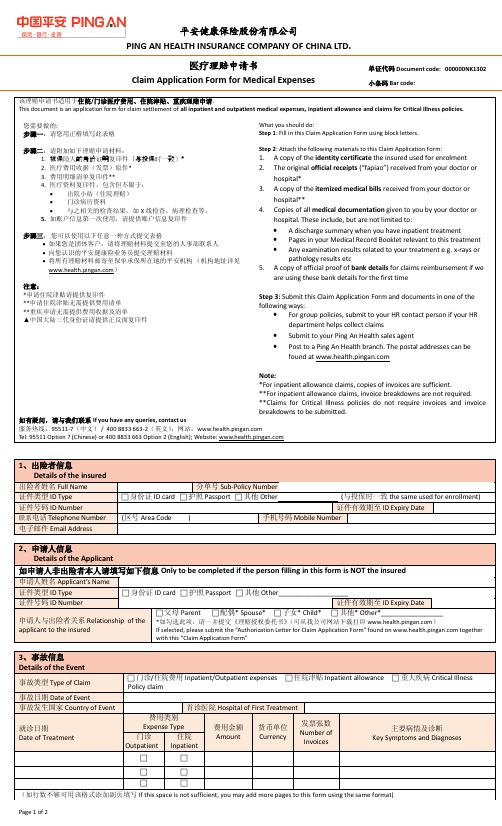
理 赔 申 请 书
年龄 Age
以 下 栏 目 请 申 请 人 填 写 / To be completed by Insured:
性别 Gender 事故地点 Incident Place 身份证号码 ID No. 现状 Status 是否异地理赔 Whether submit to other Branch □意外身故 / Incidental Death □意外残疾 / Incident Disability □重大疾病 / Major Disease □疾病医疗 / Disease Medical Treatment □是 / Y □否 / N
领款方式 / Payment: 人民币开户行 RMB Bank A / C 外币开户行 Foreign Currency Bank A / C
续 上
外币账号 Foreign Currency A / C No. 外币账户类型 Type of Foreign Currency A / C □现钞 / Cash □现汇 / Spot Exchange
申请人姓名 Applicant Name 联系地址 Address 申请人身份 Applicant ID 是否委托办理 Entrust or Not □被保险人 / Insured □法定受益人 / Legal Beneficiary □是 / Y □否 / N 被委托人姓名 Trustee Name 身份证号码 ID No.
□指定受益人 / Designated Beneficiary □受益人的监护人 / Guardian of Beneficiary 联系电话 Phone ) )
被委托人身份 Trustee ID
业务员( 代码: Agent( Agent Code: □家属 / Dependents □律师 / Lawyer □ □现金 / Cash
提交人签名 / Submitted by: 日期 / Date: 理赔申请材料退件签收栏 / Returned Claim Documentation:
公司签收人 / Received by: 日期 / Date:
签收人 / Received by:
日期 / Date:
本公司现收到理赔申请材料如下 / We received claim documentation as following: □保单凭证 / Insurance Policy □医疗费收据 / Medical Service Charge Receipt □事故者身份证明 / Insureds ID Certificate □残疾鉴定报告 / Handicapped Identification Report □处方 / Prescription □疾病诊断书 / Disease Diagnosis □医疗费结算明细表 / Settlement List for Medical Service Charges □受益人身份证明 / Beneficiary ID Certificate □病历、出院小结 / Diagnosis Record and Discharge Summary □居民死亡证明 / Resident Death Certificate □受益人关系证明 / Beneficiary Relationship Identification □病理、血液 X 光报告 / Pathological, Blood and Xray Report □丧葬、火化证明 / Funeral / Cremation Identification □授权委托书 / Power of Attorney □意外事故证明 / Accident Identification □户口注销证明 / Certificate for Annulment of Household Registration □代理人身份证明 / Agent ID Certificate □银行存折 / Bank Deposit Book □公司审批表 / Company Approval □其它 / Others:
原件 / Original ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 复印件 / Copy ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份 ( )份
事故详细经过 / Incident in Detail:
事故者是否在其他保险公司投保人身保险?
□否 □是
承保公司: □Y Company Name: 联系电话 Phone 邮政编码 Zip Code
Whether the insured has applied life insurance in other insurance company? □N
声明 / Statement: 1. 本人在理赔申请书上所填写内容详尽真实。 / I certify that the information shown on this form is true, accurate and complete; 2. 同意平安健康保险股份有限公司向医疗及其他有关单位和个人调阅、摘抄、复印与本理赔申请相关的资料,本人愿承担由此产 生的 一 切 法 律 后 果。 / I agree that Ping An Health Insurance Company, LTD may collect, excerpt and photocopy documentations related to this application from any hospital, organization or individual to complete my claim, I will responsible for any law dispute caused by this matter. 3. 选择转账领款方式的,本人授权贵公司将给付款项直接划至本申请书中所提供的银行账号中。 / I authorize Ping An Health Insurance Company, LTD to remit the claim benefit directly to the designated banking account which is shown on this form. 4. 因本人提供账号错误导致转帐不成功的责任或因委托人没有将代领的赔付金交给本人的责任由本人承担,贵公司不承担责任。 I agree that Ping An Health Insurance Company, Ltd. will not be responsible for the failure of receiving reimbursement in the situation of: A, incorrectly provide bank account details by claim applier, B, trustee fail to give the reimbursement to claim applier.
申请人 / Applicant Signature:
年
月
日 / Date:
B.
以 下 栏 目 由 公 司 理 赔 受 理 人 员 填 写 、 申 请 人 确 认 。 保 单 号 码 : To be completed by insurance employee,reviewed by applicant. Policy No. :
单 / D"#$%&'( C"*& : 000000,-./00
P"#$%A#%H(A)*H%I,I-./A,0(%0C2PA,P%CO%0HIn ( 含资料调阅授权书) ( Including authorization of collecting Personal Medical Records) A.
营业区、部: Business Zone / Department: □同事 / Colleague □朋友 / Friend □其他 / Others: □转账 / Transfer 户主 A / C Owner 外币户主 A / C Owner □银行代付 / Via Bank 账号 A / C No. 币种 Currency
事故者姓名 Insureds Name 事故日期 Incident Date 事故原因 Incident Causes 申请类型 Incident Type
□疾病身故 / Disease Death □疾病残疾 / Disease Disability □意外医疗 / Accident Medical Treatment □其他 / Others