Sparticle Reconstruction at LHC
口腔组织病理学单词整理
bifid tongue分叉舌,也称舌裂(cleft tongue,split tongue)branchial arch 鳃弓branchial groove 鳃沟cervical sinus 颈窦cleft jaw 颌裂cleft lip 唇裂cleft palate 腭裂conotruncal 主动脉的copula 联合突DiGeorge 综合征细胞遗传学异常(22q11.2缺失)或酒精中毒引起的发育异常ectomesenchyme 外胚间叶,外间充质。
是来自于神经嵴外胚层的结缔组织的总称。
facial cleft面裂foramen cecum舌盲孔frontonasal process 额鼻突fuse 融合ganglionic placode 神经节原基globular process球状突holoprosencephaly 前脑单脑室畸形incisive canal切牙管,鼻腭管(naso-palatal canal)lateral lingual prominence/swelling 侧舌隆突lateral nasal process 侧鼻突lateral palatal process 侧腭突,也称继发腭(second palate)、腭突(palatine shelf)maxillary process 上颌突Meckel's cartilage 第一鳃弓软骨,下颌软骨medial nasal process中鼻突merge联合nasal fin 鼻鳍nasal pit 鼻凹,嗅窝nasal placode鼻板naso-palatal canal鼻腭管,切牙管(incisive canal)neural crest 神经嵴olfactory placode嗅板oral pit口凹orapharyngeal membrane 口咽膜,也称颊咽膜(orapharyngeal membrane)patterning 模式发育pharyngeal pouch 咽囊,鳃囊primary palate 原发腭,前腭突(median palatine process)Rathke's pouch拉特克囊,也称神经颊囊(craniobuccal pouch),颅颊囊(craniopharyngeal pouch)Reichert软骨第2鳃弓软骨retinoic acid syndrome(RAS)维甲酸综合征,妊娠早期服用过量13-顺-维甲酸引起的发育异常Schwann细胞亦称雪旺细胞,为神经鞘膜细胞secondary palate 继发腭,侧腭突(lateral palatal process),腭突(palatine shelf)stomadeum 原口sulcus terminalis 界沟thyroglossal duct甲状舌管Treacher Collins 综合征(外、中耳轻度发育异常,颧骨对称性发育不全或缺失,上、下颌骨后部发育缺陷,约35%的患者可出现腭裂,以软腭裂为主)tuberculum impar 奇结节返回页首第二章牙的发育ameloblast成釉细胞ameloblastin 成釉蛋白amelogenesis釉质形成bell stage钟状期bud stage蕾状期cap stage帽状期cervical loop颈环dental lamina 牙板dental papilla 牙乳头dental sac牙囊enamel cord釉索enamel knot釉结enamel niche釉龛enamel organ成釉器eruption萌出glycosaminoglycans 氨基葡萄糖、糖氨聚糖gubernacular canal引导管Hertwing epithelial root sheath赫特威上皮根鞘inner enamal epithelium内釉上皮层junctional complex连接复合体Malassez epithelial rest马拉瑟上皮剩余mantle dentin罩牙本质matrix vesicle基质小泡non-collagenous protein NSPs 非胶原蛋白odontoblast成牙本质细胞outer enamal epithelium 外釉上皮层predentin前期牙本质preodontoblast前成牙本质细胞primary epithelial band 原发性上皮带reduced dental epithelium 缩余釉上皮resting odontoblast 静止型成牙本质细胞secretory odontoblast分泌型成牙本质细胞Serre's上皮剩余残留的牙板上皮shedding 脱落,交替stellate reticulum星网状层stratum intermedium 中间层terminal web终棒Tomes processes托姆斯突tuftelin釉丛蛋白返回页首第三章牙体组织abrasion, attrition 磨损acellular afibrillar cementum, AAC 无细胞无纤维牙骨质acellular cementum 无细胞牙骨质acellular extrinsic fiber cementum, AEFC 无细胞外源性纤维牙骨质acellular intrinsic fiber cementum, AIFC 无细胞固有纤维牙骨质ameloblastin 成釉蛋白amelogenins 釉原蛋白appearance of doughnut 油炸圈样biglycan 双糖链蛋白聚糖cariostatic potential 耐龋潜能cell-free zone 乏细胞层、Weil层cell-rich zone 多细胞层cellular cementum 细胞牙骨质cellular intrinsic fiber cementum, CIFC 有细胞固有纤维牙骨质cellular mixed stratified cementum, CMSC 有细胞混合性分层牙骨质cementoid 类牙骨质cementum adhesion protein 牙骨质粘附蛋白cementum growth factor 牙骨质生长因子cementum 牙骨质circumpulpal dentin 髓周牙本质cross striations 横纹dead tract 死区decorin 核心蛋白聚糖dendritic cells 树突状细胞dental pulp 牙髓dentin phosphophoryn 牙本质磷蛋白dentin phosphoproteins,DPP 牙本质磷蛋白dentin sialophosphoproteins 牙本质涎磷蛋白dentin sialoprotein,DSP 牙本质涎蛋白dentin 牙本质dentinal tubule 牙本质小管dentino-cemental junction 牙本质牙骨质界desmosome 桥粒direct innervation theory 神经传导学说enamel cap 釉帽enamel cuticle 釉小皮enamel lamellae 釉板enamel rod sheath 釉柱鞘enamel rod 釉柱enamel spindle 釉梭enamel tufts 釉丛enamel 牙釉质enamel-dentinal junction,EDJ 牙釉质牙本质界、釉牙本质界enamelin 釉蛋白enamelo-cemental junction 牙釉质牙骨质界enamelysin 牙釉质溶解蛋白、基质金属蛋白酶20(matrix metalloproteinases 20,MMP20)enkephalin 脑啡肽fibroblast 成纤维细胞fibronectin 纤维粘连蛋白focal hole, FH 灶性孔gap junction 缝隙连接glycosaminoglycans 糖胺聚糖gnarled enamel 绞釉histiocyte 组织细胞hyaline layer 透明层hydrodynamic theory 流体动力学说incremental lines 生长线、芮氏线(lines of Retzius)interglobular dentin 球间牙本质intermediate cementum 中间牙骨质intermediate junction 中间连接intertubular dentin 管间牙本质intratubular dentin 管内牙本质Korff's fiber 科尔夫纤维, 最先形成的牙本质纤维lamina limitans 限制板mantle dentin 罩牙本质micropore 微孔nanospheres 纳米球neonatal line 新生线Neumann sheath 诺伊曼鞘non-amelogenins 非釉原蛋白odontoblast 成牙本质细胞odontoblastic process 成牙本质细胞突起,也称"Tomes' fiber"osteocalcin 骨钙素osteodentin 骨样牙本质osteonectin 骨连接素osteopontin 骨桥蛋白Owen line 欧文线(加重的生长线),也称"contour line of Owen"parietal layer of nerves 神经壁层,Raschkow 丛perforating fiber 穿通纤维perikymata 牙面平行线、釉面横纹periodontoblastic space 成牙本质细胞突周间隙peritubular dentin 管周牙本质predentin 前期牙本质primary dentin 原发性牙本质,牙发育时期形成的牙本质proteinases 蛋白酶pulp core 髓核pulp proper 固有牙髓pulpo-dentinal complex 牙髓牙本质复合体reaction dentin 反应性牙本质remodeling 重塑reparative dentin 修复性牙本质reversal line 反转线rodless enamel 无釉柱牙釉质Schreger line 施雷格线sclerotic dentin 透明牙本质secondary dentin 继发性牙本质,牙发育完成之后形成的牙本质serine proteinases 丝氨酸蛋白酶(kallikrein-4)Sharpey's fiber 沙比纤维,穿通纤维somatostatin 生长激素抑制素tenascin 腱蛋白tertiary dentin 第三期牙本质the zone of Weil Weil层、乏细胞层tight junction 紧密连接Tomes' granular layer 托姆斯颗粒层Tomes processes pit,TPP 托姆斯突凹transduction theory 转导学说transparent dentin 透明牙本质tropocollagen 原胶原tuftelin 釉丛蛋白undifferentiated mesenchymal cell 未分化间充质细胞vitronectin 玻璃粘连蛋白,细胞外粘附蛋白,副纤维粘连蛋白von Ebner 1ine 牙本质生长线wedge shaped defect 楔状缺损返回页首第四章牙周组织alveolar bone proper固有牙槽骨alveolar bone 牙槽骨alveolar crest group 牙槽嵴组alveolar process 牙槽突alveologingival group 牙槽龈组apical group 根尖组apoptosis 凋亡attached gingiva 附着龈bundle bone 束骨circular group 环行组dentogingival group 龈牙组dentogingival junction 牙龈结合dentoperiosteal group 牙骨膜组elastin fibers 弹力纤维Eluanin纤维牙周膜中两种不成熟的弹力纤维之一free gingiva 游离龈free gingival groove 游离龈沟gingiva 牙龈gingival col 龈谷gingival sulcus龈沟gingval epithelium 牙龈上皮horizontal group 水平组Howship 陷窝骨吸收陷窝interdental papilla 牙间乳头interradicular group 根间组junctional epithelium 结合上皮Malassez 上皮剩余,牙周膜中上皮根鞘的残余细胞oblique group 斜行组oxytalan fibers 不成熟的弹力纤维periodontal membrance 牙周膜salcular epithelium 龈沟上皮stippling 点彩transseptal group 越隔组返回页首第五章口腔粘膜anchoring fibril 锚纤维attachment plaque 附着斑basement membrane zone 基底膜区basement membrane 基底膜cornified envelope 角化包膜cytokeratin细胞角蛋白desmocollins 桥粒胶蛋白desmogleins 桥粒芯蛋白desmoplakins 桥粒斑蛋白epithelial pegs(rete pegs,epithelial ridges)上皮钉突,上皮嵴epithelial ridges(epithelial pegs, rete pegs)上皮嵴,也称上皮钉突fibulin 锚定素filiform papilla 丝状乳头foliate papilla 叶状乳头Fordyce spot 福代斯斑fungiform papilla 菌状乳头involucrin 总苞蛋白keratiocyte角质细胞lamina densa 密板lamina lucida 透明板lamina propria 固有层lamina reticularis 网板Langerhans cell 郎格汉斯细胞linea alba白线lingual crypt 舌隐窝lingual follicle 舌滤泡lining mucosa 被覆粘膜loricrin 兜甲蛋白masticatory mucosa 咀嚼粘膜melanocyte 黑色素细胞Merkel cell 梅克尔细胞nidogen 巢蛋白oral mucosa 口腔粘膜oral mucous membrane口腔粘膜orthokeratinization 正角化parakeratinization 不全角化perlecan 基底膜聚糖,珍珠素plakoglobin 桥粒斑珠蛋白plectin 网蛋白profilagrin 纤丝聚集蛋白原small proline-rich proteins 小富脯蛋白specialized mucosa 特殊粘膜stratum basale基底层,也称"basal layer"stratum corneum 角化层stratum germinativum 生发层stratum granulosum 颗粒层stratum spinosum 棘层submucosa 粘膜下层taste bud 味蕾tonofilament 张力细丝vallate papilla 轮廓乳头返回页首第六章涎腺acinus 腺泡actin 肌动蛋白antiproteolytic protein 抗蛋白溶解蛋白basket cell 篮细胞crystalloids 晶样体demilune 半月板dense body 致密小体excretory duct 排泄管exocytosis 胞吐glucogon-like protein 高血糖素样蛋白goblet cell 杯状细胞gustin 味觉素histidine 富组氨酸holocrine-type secretion全浆分泌intercalated duct 闰管junctional complex 连接复合体lactoferrin 乳铁蛋白merocrine局浆分泌minor salivary gland 小涎腺mixed acinus 混合性腺泡mucin 粘多糖mucous acinus 粘液性腺泡myoepithelial cell 肌上皮细胞myofilament 肌微丝myosin 肌球蛋白oncocyte 嗜酸细胞oncocytoma 嗜酸粒细胞瘤osmic acid 锇酸oxiphilic adenoma 嗜酸性腺瘤parotid gland 腮腺parotin 腮腺素primitive pluripotential salivary duct cells原始多潜能涎腺导管细胞proline-rich protein 富脯氨酸蛋白ptyatin 涎液素rennin 肾素reserve cell 储备细胞salivary gland 唾液腺saliva唾液secretory duct 分泌管secretory unit 分泌单位seromucous cell 浆粘液细胞serous acinus 浆液性腺泡Sjǒgren syndrome 舍格伦综合征stem cell 干细胞Stensen duct 腮腺导管striated duct 纹管sublingual gland 舌下腺submandibular gland 颌下腺tyrosine-rich protein 富酪氨酸蛋白zymogen granule 酶原颗粒返回页首第七章颞下颌关节capsule 关节囊condyle 髁突cellularrich zone多细胞带disc 关节盘fibrocartilaginous zone纤维软骨带fibrous articular surface纤维性关节表面带synovial membrane 滑膜temporo-mandibular joint,TMJ 颞下颌关节zone of calcified cartilage钙化软骨带第八章牙发育异常adontia 无牙amelogenesis imperfecta 牙釉质形成缺陷症brandywine isolate白兰地型,牙本质形成缺陷的一种central cusp deformity 畸形中央尖cervical enamel extension 牙釉质延伸cleidocranial dysplasia 锁骨头颅发育不良,锁骨颅骨发育不全征concrescence 结合牙congenital syphilis 先天性梅毒牙dens evaginatus of anterior teeth 前牙的牙外突dens in dente 牙中牙dens invaginatus 牙内陷dental fluorosis 氟牙症dentin dysplasia type I I型牙本质结构不良dentin dysplasia type II II型牙本质结构不良、冠部牙本质结构不良dentin dysplasia 牙本质结构不良dentin matrix protein 1, DMP1 牙本质基质蛋白1dentin sialoprotein, DSP 牙本质涎蛋白dentinogenesis imperfecta type II 牙本质形成缺陷症II型dilacerations 弯曲牙discoloration of teeth 牙变色distomolar 远中磨牙enamel hypoplasia 牙釉质形成不全enamel opacities 牙釉质混浊症enamel pearl 釉珠fusion 融合牙gemination双生牙ghost teeth 阴影牙、区域性牙发育不良hemifacial hyperplasia 半面过度增生hereditary opalescent dentin 遗传性乳光牙本质hypercementosis 牙骨质过度增生hyperdontia 多生牙hypocalcified type 钙化不全型hypocementosis 牙骨质发育不全hypodontia 少牙hypohidrotic ectodermal dysplasia 少汗外胚层发育不良hypomatuaration type 成熟不全型hypomineralized enamel 牙釉质矿化不全hypomineralized type 矿化不全型hypophosphatasia 低磷酸酯酶症hypoplastic type 形成不全型impaction of teeth 牙阻生lingual cusp deformity 畸形舌侧尖lingual fossa deformity 畸形舌侧窝macrodontia巨牙mesiodens 正中牙microdontia 小牙mottled enamel 斑釉mulberry molar 桑椹牙natal teeth 胎生牙,出生时即已萌出的牙noenatal teeth 新生牙,出生后30天内萌出的牙non-fluoride enamel opacities 非氟性牙釉质浑浊症paramolar 副磨牙persistence of deciduous teeth 乳牙滞留premature eruption 早萌premature loss 过早脱落regional odontodysplasia 区域性牙发育不良、阴影牙retarded eruption 延迟萌出shell-teeth 壳状牙snow-capped 雪帽型supernumerary teeth 多生牙supplemental teeth 附加牙talon cusp 鹰爪尖taurodontism 牛牙症tetracycline stained teeth 四环素牙Turner's teeth Turner 牙,与乳牙有关的感染或创伤引起继生恒牙成釉细胞的损伤,导致继生恒牙牙釉质形成不全或矿化不全water streaming round bouldings 水流围绕圆石,根部牙本质结构不良的表现返回页首第九章龋病A. naeslundii 内氏放线菌A. viscosus 粘性放线菌acidogenic theory 酸原学说acquired pellicle 获得性薄膜、唾液薄膜Actinomyces 放线菌属acute caries 急性龋arrested caries 静止性龋bacterial plaque 菌斑body of the lesion 病损体部cementum caries 牙骨质龋chemico-bacterial theory 化学细菌学说chemico-parasitic theory 化学寄生学说chronic caries 慢性龋dark zone 暗层dental caries 龋病dentin caries 牙本质龋enamel caries 牙釉质龋L. acidophilus 嗜酸乳杆菌L. casei 干酪乳杆菌L. fermentus 发酵乳杆菌Lactobacilli 乳杆菌属Mutans Streptococci 链球菌属pit and fissure caries 窝沟龋proteolysis-chelation theory 蛋白溶解-螯合学说proteolytic theory 蛋白溶解学rampant caries 猛性龋root caries 根龋S. mitis 轻链球菌S. mutans 变形链球菌S. sanguis 血链球菌S. sobrinus 远缘链球菌salivary pellicle 唾液薄膜、获得性薄膜smooth surface caries 平滑面龋smooth surface caries 平滑面龋surface zone 表层three primary factors theory 三联因素学说translucent zone 透明层translucent zone 透明层,硬化层zone of bacterial invasion 细菌侵入层zone of demineralization 脱矿层zone of destruction 坏死崩解层返回页首第十章牙髓病acute pulpitis 急性牙髓炎acute serous pulpitis 急性浆液性牙髓炎acute supurative pulpitis 急性化脓性牙髓炎chronic closed pulpitis 慢性闭锁性牙髓炎chronic hyperplastic pulpitis 慢性增生性牙髓炎chronic pulpitis 慢性牙髓炎chronic ulcerative pulpitis 慢性溃疡型牙髓炎external tooth resorption 牙外吸收idiopathic resorption 特发性吸收interleukin,IL白细胞介素internal tooth resorption 牙内吸收irreversible pulpitis不可逆性牙髓炎leukotrienes,LTs 白三烯necrobiosis 牙髓渐进性坏死prostaglandins,PGs 前列腺素pulp degeneration 牙髓变性pulp calcification 牙髓钙化pulp fibrosis 牙髓纤维性变pulp gangrene 牙髓坏疽pulp hyperemia 牙髓充血pulp necrosis 牙髓坏死pulpitis 牙髓炎residual pulpitis 残髓炎reticular atrophy of the pulp 牙髓网状萎缩retrograde pulpitis 逆行性牙髓炎reversible pulpitis 可复性牙髓炎tooth resorption 牙体吸收transfer growth factor,TGF 转化生长因子vacuolar degeneration of the odontoblastic layer 成牙本质细胞层空泡变性返回页首第十一章根尖周炎acute alveolar abscess 急性牙槽脓肿acute periapical periodontitis 急性根尖周炎cellulitis 蜂窝织炎chonic alveolar abscess 慢性牙槽脓肿chronic periapical abscess慢性根尖脓肿chronic periapical periodontitis 慢性根尖周炎condensing osteoitis 致密性骨炎lipoteichoic acids 磷脂壁酸peplidoglyans 肽葡聚糖periapical granuloma 根尖肉芽肿periapical periodontitis 根尖周炎tumor necrosis factor,TNF 肿瘤坏死因子返回页首第十二章牙周组织病abcesses of the periodontium 牙周脓肿Actinobacillus actinomycetem comitans,Aa 放线共生放线杆菌Actinomyces viscosus,Av 粘性放线菌acute necrotizing gingivitis 急性坏死性龈炎acute necrotizing ulcerative gingivitis 急性坏死性溃疡性龈炎adhesion 粘附advanced lesion 进展期aggregation 聚集aggressive periodontitis 侵袭性牙周炎atrophy萎缩Bcteroides forsythus,Bf 福赛类杆菌Cap no gingivalis 牙龈二氧化碳嗜纤维菌cellular adhesion m olecules,CAM 细胞粘附分子chondrosulphatase 硫酸软骨素酶chronic gingivitis 慢性龈炎chronic periodontitis 慢性牙周炎coaggregation 共聚collagenase 胶原酶congenital familial fibromatosis 家族性龈纤维瘤病cytokine 细胞因子degeneration 变性dental pla que biofilm 细菌性生物膜dental plaque-induced gingival disease牙菌斑性牙龈病desquamative lesion of gingival 剥脱性龈病损developmental or acquired deformities and conditions发育性或获得性异常及其状况diffuse atrophy of alveolar bone 牙槽骨弥漫性萎缩dystrophic 营养不良性dystrophy 营养不良early lesion 早期病变established lesion 病损确立期fimbriae 菌毛fusospirochetal gingivitis 梭螺菌龈炎gingival cleft 龈裂gingival crevicular fluid,GCF龈沟液gingival diseases 牙龈病gingival enlargement associated with leukemia白血病性龈增大gingival hyperplasia 龈增生gingival pocket 龈袋gingival recession 牙龈退缩gingivitis with leukemia伴白血病性龈炎hereditary gingival fibromatosis遗传性牙龈纤维瘤病hereditary gingival hyperplasia遗传性龈增生human leucocyte antigen,HLA 人类白细胞抗原hyaluronidase 透明质酸酶idiopathic gingival hyperplasia特发性龈增生idiopathic plasma-cell gingivostomatitis 特发性浆细胞龈口炎inflammation 炎症initial stage始发期interleukins,IL 白细胞介素intrabony pocket 骨内袋lipopolysaccharedes,LPS 脂多糖marginal gingivitis 边缘性龈炎matrix metalloprotinases,MMP基质金属蛋白酶medication-influenced gingivitis 药物性龈炎metalloproteinases 金属蛋白酶mucin 唾液粘蛋白necrotizing periodontal diseases 坏死性牙周病neoplasia 肿瘤noninflammatory 非炎症性non-plaque-induced gingival lesions 非菌斑性牙龈病损occlusal trauma 咬合创伤osteoclast differentation factor,ODF 破骨细胞分化因子osteoprotegerin,OPG 护骨因子papillary gingivitis 牙龈乳头炎periodontal degeneration 牙周变性periodontal disease牙周病periodontitis as a manifestation of systemic diseases反应全身疾病的牙周炎periodontitis associated with endodontic lesions 伴有牙髓病变的牙周炎periodontitis 牙周炎periodontosis 牙周症plasma cell gingivitis 浆细胞龈炎polymorphonuclear leukocytes,PMN 中性多形核白细胞Porphyromonas gingivalis,P.g 牙龈卟啉单胞菌pregnancy gingivitis 妊娠期龈炎presenile atrophy 早老性萎缩prostglandinE2,PGE2 前列腺素E2proteinases 蛋白酶pubertal gingivitis青春期龈炎secondary occlusal trauma 继发性咬合创伤senile atrophy 老年性萎缩steroid hormone-influenced gingivitis 激素性龈炎Stillman'S cleft 龈裂supragingival pocket骨上袋T.maltophilum 嗜麦芽糖密螺旋体T.medium 中间密螺旋体tissue inhibitors of metalloproteinase,TIMP金属蛋白酶的抑制剂trauma 创伤traumatic occlusion创伤性咬合trench mouth 战壕口炎Treponema 密螺旋体属tumor necrosis factor-α,TNF-α肿瘤坏死因子-αVincent gingivitis 奋森龈炎vitamin C deficeint gingivitis维生素C缺乏性龈炎返回页首第十三章口腔粘膜病acantholysis 棘层松解acanthosis 棘层增生acquired immunodeficiency syndrome,AIDS 获得性免疫缺陷综合征amyloidosis 淀粉样变性antinuclear antibody,ANA 抗核抗体atrophy 萎缩atypia 非典型性ballooning degeneration 气球变性basophilic degeneration 嗜碱性变性Behcet syndrome 白塞综合征benign lymphoadenosis of mucosa 粘膜良性淋巴组织增生病benign migratory glossitis 良性游走性舌炎benign mucous membrane pemphigoid 良性粘膜类天疱疮bulla 大疱candida albicans 白色念珠状菌candidiasis 念珠菌病cell apoptosis 细胞凋亡cheilitis glandularis 腺性唇炎cheilitis granulomatosa 肉芽肿性唇炎chronic discoid lupus erythematosus 慢性盘状红斑狼疮colloid body 胶样小体,Civatte小体crusts 痂desmocollins 桥粒芯胶粘蛋白desmogleins 桥粒芯糖蛋白dyskeratosis 角化不良epithelial atrophy 上皮萎缩epithelial dysplasia 上皮异常增生Epstein-Barr Virus EB病毒erosion 糜烂erythema multiforme exsudativum 多形渗出性红斑erythroplakia 红斑erythroplasia 增殖性红斑erythroplastic lesion 红色增殖性病变g1ossitis areata exfoliativa 区域剥脱性舌炎geographic tongue 地图舌granular erythroplakia 颗粒型红斑herpes simplex 单纯性疱疹herpetic stomatitis 疱疹性口炎HIV-gingivitis HIV牙龈炎HIV-necrotizing gingivitis HIV坏死性龈炎HIV-periodontitis HIV牙周炎homogenous erythroplakia 均质型红斑human immunodeficiency virus,HIV 人免疫缺陷病毒hyperkeratosis 过度角化hyperorthokeratosis 过度正角化hyperparakeratosis 过度不全角化interspersed erythroplakia 间杂型红斑leukoedema 白色水肿leukoplakia 白斑lichen Planus Pemphigoides,LPP 类天疱疮样扁平苔藓lichen planus,LP 扁平苔藓lingual papillitis 舌乳头炎macule 斑melanophages 噬黑色素细胞Melkersson-Rosenthal syndrome 梅一罗综合征Nikolsky征尼氏征,周缘扩展现象non-Hodgkin lymphoma 非霍奇金淋巴瘤oculo-oral-genital syndrome 眼、口、生殖器三联综合征oral candidiasis 口腔念珠菌病oral hairy leukoplakia,OHL 口腔毛状白斑oral Kaposi sarcoma 口腔Kaposi肉瘤oral non-Hodgkin lymphoma 口腔非霍其金淋巴瘤oral submucous fibrosis 口腔粘膜下纤维化papule 丘疹pemphigus 天疱疮periadenitis mucosa necrotica recurrens,PMNR 复发性坏死性粘膜腺周围炎programmed cell death程序化细胞死亡pseudomembrane 假膜,伪膜recurrent aphthous stomatitis,RAS 复发性阿弗他口炎recurrent aphthous ulcer,RAU 复发性阿弗他溃疡reticular degeneration 网状变性rhagade 皲裂sarcoidosis 结节病Schauann bodies 肖曼小体,多核巨细胞内的包涵体spongiosis 海绵形成Stevens-Johnson综合征重症多形渗出性红斑thioflavine T 硫黄素TTzanck cell 天疱疮细胞ulcer 溃疡vaculation and liquefaction of hasal cell 基底细胞空泡性变及液化vesicle 疱Wegener granulomatosis 韦格内肉芽肿white folded disease 白皱折病white sponge nevus 白色海绵状斑痣返回页首第十四章颌骨疾病actinomycosis of jaws 颌骨放线菌病acute suppurative osteomyelitis of jaws急性化脓性颌骨骨髓炎aggressive ossifying fibroma 侵袭性骨化性纤维瘤aggressive osteoblastoma 侵袭性成骨细胞瘤aneurysmal bone cyst 动脉瘤性骨囊肿benign oseoblastoma 良性成骨细胞瘤brown tumor 棕色瘤Burkitt's lymphoma 伯基特淋巴瘤cancellous osteoma 海绵型骨瘤cementifying fibroma 化牙骨质纤维瘤cemento-ossifying fibroma 牙骨质骨化性纤维瘤central type 中心型cherubism 家族性巨颌症chondroblastoma 成软骨细胞瘤chondrocranium 软骨颅chondroma 软骨瘤chondromyxoid fobroma 软骨粘液样纤维瘤chondrosarcoma 软骨肉瘤chronic diffuse sclerosing osteomyelitis of jaws 慢性弥漫性硬化性颌骨骨髓炎chronic focal sclerosing osteomyelitis of jaws慢性局灶性硬化性颌骨骨髓炎chronic osteomyelitis with proliferative periostitis慢性骨髓炎伴增生性骨膜炎chronic sclerosing osteomyelitis of jaws慢性硬化性颌骨骨髓炎chronic suppurative osteomyelitis of jaws慢性化脓性颌骨骨髓炎compact osteoma 致密型骨瘤condensing ostitis 致密性骨炎dendritic cell system 树突状细胞系统dermal dendrocyte表皮树突状细胞enchondroma 内生型软骨瘤eosinophilic granuloma 嗜酸性肉芽肿epithelioid cell 上皮样细胞exostosis 外生骨疣extramedullarg Ewing sarcoma 髓外性尤文肉瘤extramedullary plasmacyfoma 髓外浆细胞瘤extraosseous osteosarcoma 骨外骨肉瘤extraosseous chondrosarcoma 骨外型软骨肉瘤familial fibrous dysplasia of the jaws家族性颌骨纤维异常增殖症,同家族性颌骨多囊性病(familial mulitilocular cystic disease of jaws)familial mulitilocular cystic disease of jaws家族性颌骨多囊性病,同家族性颌骨纤维异常增殖症(familial fibrous dysplasia of the jaws)fibro-osseous lesion 纤维-骨病变fibrous dysplasia of bone 骨纤维异常增殖症follicular dendritic cell 滤泡树突状细胞Garré's chronic nonsuppurative sclerosing ostitis Garre慢性非化脓性硬化性骨炎Garré's osteomyelitis Garre骨髓炎giant cell granuloma 巨细胞肉芽肿giant cell lesions of the jaws颌骨巨细胞病变giant cell reparative granuloma 巨细胞修复性肉芽肿giant cell rich lesion 富巨细胞性病变giant cell tumor of bone,GCT骨巨细胞瘤giant osteoid osteoma 巨大型骨样骨瘤granulomatous inflammation 肉芽肿性炎症groundglass appearance 磨砂玻璃样Hand-Schiiller-Christian disease 汉-许-克病hemorrhagic bone cyst出血性骨囊肿high-turnover state 转化亢进histiocytosisX 组织细胞增生症Xhyperparathyroidism 甲状旁腺功能亢进indeterminate cell 不确定细胞interdigitating dendritic cell淋巴结的交错突细胞involucrum 骨壳juvenile ossifying fibroma青少年骨化性纤维瘤lamellar bone 板层骨lamina dura 硬骨板Langerhans cell disease 郎格汉斯细胞病,同郎格汉斯细胞组织细胞增生症(Langerhans cell histiocytosis)Langerhans cell histiocytosis郎格汉斯细胞组织细胞增生症,同郎格汉斯细胞病(Langerhans cell disease)Langhans giant cell 朗汉斯巨细胞Letterer-Siwe disease 勒-雪病Maffucci's综合征多发性软骨瘤病合并血管瘤malignant osteoblastoma 恶性成骨细胞瘤mesenchymal chondrosarcoma 间叶型软骨肉瘤mineralized bone钙化骨mononuclear phagocyte system 单核巨噬细胞系统mononucleate stromal cell 单核基质细胞monostotic bibrous dysplasia 单骨性骨纤维异常增殖症moth-eaten appearance 虫蚀状multiple chondromatosis 多发性软骨瘤病multiple myeloma 多发性骨髓瘤myeloma 骨髓瘤neonatal maxillitis 新生儿上颌骨骨髓炎Ollier's病多发性软骨瘤病合并肢体发育畸形onion-skin 洋葱皮ossifying fibroma 骨化性纤维瘤osteocartilaginous exostosis 骨软骨性外生骨疣osteochondroma 骨软骨瘤osteoclastoma 破骨细胞瘤osteoid osteoma骨样骨瘤osteoma 骨瘤osteomyelitis of jaws 颌骨骨髓炎osteoradionecrosis 放射性骨坏死osteosarcoma 骨肉瘤periosteal osteosarcoma 骨膜骨肉瘤paraosteal osteosarcoma 骨旁骨肉瘤periostitis ossificans 骨化性骨膜炎peripheral giant cell granuloma 周围性巨细胞肉芽肿peripheral type 周围型peripreral chondroma 周围型软骨瘤peritrabecular fibrosis 骨小梁周围纤维化plasmacytoma 浆细胞瘤polyostotic fibrous dysplasia 多骨性骨纤维异常增殖症primary hyperparathyroidism 原发性甲状旁腺功能亢进pseudocyst 假囊肿punched-out appearance 穿凿样secondary cartilage 继发软骨secondary hyperparathyroidism 继发性甲状旁腺功能亢进sequestrum 死骨simple bone cyst 单纯性骨囊肿solitary bone cyst 孤立性骨囊肿solitary myeloma 弧立性骨髓瘤static bone cavity 静止性骨腔subperiosteal bone resorption 骨膜下骨吸收sulfur granule 硫磺颗粒,即放线菌团sun-ray 日光放射状(影像)syphilis of jaws 颌骨梅毒torus mandibularis 下颌隆突torus palatinus 腭隆突Touton giant cell图顿巨细胞traumatic bone cyst外伤性骨囊肿tuberculosis of jaws 颌骨结核tuberculous osteomyelitis of jaws结核性颌骨骨髓炎tunneling resorption or dissecting resorption穿凿性吸收unmineralized osteoid 非钙化骨样组织返回页首第十五章颞下颌关节病condylar hyperplasia 髁突增生degeneratitive joint disease 退行性关节病denudation 骨剥露eburnation (骨质)象牙化fibrillation 原纤维化fibrinoid change 纤维素样变loose body 游离小体malocclusion 错颌osteoarthritis,OA 骨关节炎osteoarthrosis 骨关节病osteophytic lipping 骨赘性唇状突出pannus 血管翳pigmented villonosdular synovitis 色素性绒毛结节性滑膜炎rheumatoid arthritis,RA 类风湿性关节炎rheumatoid nodule 类风湿性小结synovial osteochondromatosis 滑膜软骨瘤病tangential cleft 切线裂temporomandibular joint disorders 颞下颌关节紊乱病trisomy (染色体)三体vermiform bodies 蚓状小体vertical cleft 垂直裂villous projection 绒毛状突起rheumatoid granuloma 类风湿肉芽肿返回页首第十六章涎腺非肿瘤性疾病与涎腺肿瘤aberrant salivary glands 迷走涎腺accessory salivary gland 副涎腺acinic cell carcinoma 腺泡细胞癌acquired immune deficiency syndrome AIDS 获得性免疫缺陷综合征actinomycosis of salivary glands 涎腺放线菌病acute pyogenic paratitis急性化脓性腮腺炎acute sialadenitis 急性涎腺炎adenocarcinoma not otherwise specified adenocarcinoma,NOS 非特异性腺癌adenocarcinoma 腺癌adenoid cystic carcinoma 腺样囊性癌adenolymphoma 腺淋巴瘤adenomatoid hyerplasia of mucous glands 粘液腺腺瘤样增生adenosquamous carcinoma 腺鳞癌Alcian blue 奥辛兰amylase 淀粉酶aplasia of salivary gland 涎腺发育不全apocrine 顶浆分泌avidin biotin-peroxidase complex, ABC 亲和素生物素过氧化物酶复合物basal cell adenoma 基底细胞腺瘤basal reserve cell theory 基底储备细胞理论basisquamous whirling 基底鳞状的旋涡状benign lymphoepithelial lesion 良性淋巴上皮病变blood group substances 血型物质canalicular adenoma管状腺瘤carcinoembryonic antigen,CEA 癌胚抗原carcinoma ex pleomorphic adenoma 癌在多形性腺瘤中,多形性腺瘤癌变chronic recurrent parotitis 慢性复发性腮腺炎chronic sclerosing sialadenitis of submandibular gland 慢性硬化性颌下腺炎chronic sialadenitis 慢性涎腺炎clear cell carcinoma 透明细胞癌clear cell carcinoma, not otherwise specified 非特异性透明细胞癌clear cell tumor 透明细胞瘤congenital absence of salivary gland 涎腺先天性缺失crush artifact 挤压假象cystadenocarcinoma 囊腺癌cystadenoma 囊腺瘤cytokeratin 细胞角蛋白cytomegalic inclusion disease 巨细胞包涵体病dark cells 暗细胞degenerative sialosis 变性型涎腺肿大症degenerative swelling of salivary gland 涎腺退行性肿大development anomalies of salivary gland 涎腺发育异常developmental anomalies of ducts 导管发育异常diffuse large B-cell lymphoma 弥漫性大B细胞淋巴瘤ductal papilloma 导管乳头状瘤ductoacinar unit 导管腺泡单位epidemic parotitis 流行性腮腺炎epi-myoepithelial island 上皮肌上皮岛epithelial membrane antigen,EMA上皮膜抗原epithelio-myoepithelial carcinoma 上皮-肌上皮癌evelopmental lingual salivary gland depression 发育性舌侧下颌涎腺陷入extranodal marginal zone B-cell lymphoma 结外边缘带B细胞淋巴瘤fibronectin 纤维连接蛋白haemangioma 血管瘤Hashimoto's thyroiditis 桥本甲状腺炎hetrotopic of saIivary gland 涎腺异位HIV-associated salivary gland disease 艾滋病病毒相关性涎腺疾病Hodgkin lymphoma 霍奇金淋巴瘤hunman immunodeficiency HIV 人类免疫缺陷病毒immunocytochemistry 免疫细胞化学immunoglobulin A 免疫球蛋白Aimmunohistochemistry 免疫组织化学intraductal papilloma 导管内乳头状瘤inverted ductal papilloma 内翻性乳头状瘤Küttner瘤慢性硬化性颌下腺炎lactoferrin,LF乳铁蛋白large cell carcinoma 大细胞癌lectin receptors 植物血凝素受体light cells 亮细胞lobular carcinoma 小叶状癌lymphoepithelial carcinoma 淋巴上皮癌lymphoepithelial cyst 淋巴上皮囊肿lysozyme 溶菌酶malignant lymphoepithelial lesion 恶性淋巴上皮病变malignant pleomorphic adenoma 恶性多形性腺瘤metastasizing pleomorphic adenoma 转移性多形性腺瘤Mikülicz's syndrome Mikülicz 综合征mixed tumor 混合瘤mucoepidermoid carcinoma 粘液表皮样癌multicellular theory 多细胞理论mumps流行性腮腺炎myoepithelioma 肌上皮瘤necrotizing sialometaplasia 坏死性涎腺化生oncocytoma 嗜酸细胞瘤non-sebaceous lymphadenoma 非皮脂淋巴腺瘤oxyphilic adenoma 嗜酸性腺瘤papillary cystadenocarcinoma 乳头状囊腺癌papillary cystadenoma lymphomatosum 乳头状淋巴囊腺瘤papillary cystadenoma 乳头状囊腺瘤PAS periodic acid schiff的缩写,PAS反应即过碘酸雪夫反应,用于对糖原的特殊染色peroxidase anti-proxidase, PAP 过氧化物酶抗过氧化物酶pleomorphic adenoma 多形性腺瘤pluripotential unicellular reserve cell theory 多能单储备细胞理论polyarteritis 多动脉周围炎polycystic parotid gland 多囊腮腺polymorphous low-grade adenocarcinoma 多形性低度恶性腺癌polymyositis 多发性肌炎prelymphoma 前淋巴瘤radiant impair 放射线损伤salivary duct carcinoma 涎腺导管癌salivary duct cyst 涎腺导管囊肿salivary duct stone 涎腺导管结石salivary gland cyst 涎腺囊肿salivary gland virus disease 涎腺病毒病Schirmer test 施墨试验,检查泪液分泌情况的一种试验sebaceous adenoma 皮脂腺瘤sebaceous lymphadenocarcinoma 皮脂淋巴腺癌sebaceous lymphadenoma 皮脂腺淋巴腺瘤secretory component 分泌组份semipluripotential bicellular reserve cell theory 半多能双储备细胞理论serous cell carcinoma 浆液细胞腺癌sialadenitis 涎腺炎sialadenoma papilliferum 乳头状涎腺瘤sialadenosis 涎腺症sialoblastoma 成涎细胞瘤sialolithiasis 涎石病sicca syndrome 干燥综合征Sjǒgren's syndrome 舍格伦综合征small cell carcinoma 小细胞癌squamous cell carcinoma 鳞状细胞癌static bony cavity 静止骨腔streptavidin peroxidase,S-P 链亲和素过氧化物酶streptavidin-biotin complex SABC链亲和素生物素复合物syncytium 合胞体syringoma 汗腺瘤teminal duct carcinoma 终末导管癌thyroglobulin 甲状腺球蛋白tissuce peptide antigen,TPA组织多肽抗原tubelo-acinae-complexs 小管-腺泡复合体tuberculosis of salivary gland 涎腺结核tubular adenoma 管状腺瘤undifferentiated carcimma 未分化癌undifferentiated carcinoma with lymphoid stroma 伴淋巴间质的未分化癌vimnentin 波形丝蛋白Warthin瘤腺淋巴瘤xerostomia 口腔干燥症返回页首第十七章口腔颌面部囊肿anchoring fibrils 锚纤维Bohn 结节即婴儿龈囊肿branchial cleft cyst 鳃裂囊肿cervical lymphoepithelial cyst颈部淋巴上皮囊肿dental lamina cyst of the newborn 新生儿牙板囊肿dentigerous cyst 含牙囊肿dermoid cyst 皮样囊肿enamel spur 釉突epidermoid 皮样样囊肿发epithelial plaque 上皮斑eruption cyst 萌出囊肿follicular cyst 滤泡囊肿。
延胡索酸泰妙菌素可溶性粉对猪支原体肺炎的疗效研究

4 ·2020.16Experimental research | 试验研究0 引言对于猪支原体肺炎的预防和治疗,药物在其中的重要性极高,为更好发挥药物作用,本文围绕延胡索酸泰妙菌素可溶性粉疗效开展具体研究。
1 猪支原体肺炎概述1.1 流行病学猪肺炎支原体属于猪支原体肺炎的病原,患病猪、隐性带菌猪属于主要传染源,任何品种、性别、年龄的猪均可能感染猪支原体肺炎,仔猪的发病率较高,患病仔猪死亡率也较高。
相较于仔猪,母猪及育肥猪的发病率和死亡率均较低,多为慢性及隐性发病,症状轻微。
猪支原体肺炎一年四季均可发病,主要通过呼吸道传播,在通风不佳、防寒不到位、阴冷潮湿的环境下,猪支原体肺炎的发病率较高[1]。
1.2 临床症状猪支原体肺炎的症状可分别为3类,分别为隐性、慢性、急性。
隐性病猪存在不明显、不典型的临床症状,多为生长迟缓、无食欲,很多时候被养殖户忽视。
急性病症多出现于猪支原体肺炎的新疫区,会较为突然发病,患病猪会出现精神状态不佳、食欲降低、咳嗽现象明显、呼吸明显加快、高烧、呈腹式呼吸、声音低沉等症状。
慢性病例源于急性患病猪的转化,存在较长的病程时间,此时病猪存在流鼻涕、大口喘气、长时间咳嗽、体温及进食状况变化不明显等症状,发病后期存在大便干结、便秘等症状,慢性病猪病程最长可达到20多个月[2]。
2 疗效试验2.1 材料与方法采用由乳糖和延胡索酸盐(泰妙菌素)配制成的可溶性粉作为研究用药品延胡索酸泰妙菌素,同时采用0906082批号的支原净。
试验动物源于笔者所在地的某猪场,受猪肺炎支原体侵害,该猪场育成猪群和断奶猪群呈猪气喘病流行状态。
基于病变特征、临床症状、流行病学、微量间接血凝试验进行猪支原体肺炎确诊。
选择100头发病猪和20头同期断奶健康仔猪(症状相近),猪的品种为长白与大白杂交商品猪。
试验用猪均为30日龄,体重在5.9~7.8 kg 。
开展试验前需保证试验用猪自由饮水,按常规饲养,但不得开展支原体疫苗免疫,其他药物在试验期间不得添加和口服。
保留胸大肌筋膜的一期假体植入在乳房即刻重建手术中的应用价值
DOI:10.3969/j.issn.l672-9463.2021.01.008保留胸大肌筋膜的一期假体植入在乳房即刻重建手术中的应用价值厉芝任毅韩学东甄林林邱小兰赵瑞鹏刘敏敏[摘要]目的探讨乳腺癌一期假体植入即刻乳房重建(Immediate breast reconstruction,IBR)手术中保留胸大肌筋膜(Pectoralis major fascia,PMF)联合胸大肌肌瓣用于覆盖假体的可行性、安全性及经济性,并对比背阔肌皮瓣(Latissimus dorsi flap,LDF)转移乳房重建的优势。
方法本研究共入组我院27例接受乳房即刻重建的乳腺癌患者,分为LDF转移乳房重建组(LDF组)12例、保留PMF作为生物膜的假体植入乳房重建组(PMF组)15例。
比较两组手术时间、住院天数、切口感染率、皮下积液率、患者满意度。
结果与LDF组比较,PMF组患者满意度高,切口感染发生率低,差异具有统计学意义(PVL05);两组手术时间和住院天数比较差异有统计学意义(PVL05)。
结论保留PMF覆盖假体的即刻乳房重建手术,相比于LDF转移乳房重建,具有更加安全、创伤小、并发症少、术后恢复快、患者满意度高的优点,可广泛应用于临床。
【关键词】乳腺癌乳房即刻重建胸大肌筋膜Application value of pectoralis major fascia as patch in prosthesis implantation for immediate breast reconstruction Li Zhi, Ren Yi,HanXuedong,etal.The Affiliated Huaian No.l People's Hospital of N anjing M edical University,Huaian223300 [Abstract]Objective To investigate the feasibility,safety and economy of preserving pectoralis major fascia (PMF)combined with pectoralis major myocutaneous flap in immediate breast reconstruction(IBR)with primary breast cancer prosthesis implantation,and to compare the advantages of latissimus dorsi flap(LDF)in breast reconstruction.Methods A total of27patients with breast cancer who underwent immediate breast reconstruction in our hospital were divided into latissimus dorsi flap transfer breast reconstruction group(LDF group,n=12)and pectoralis major fascia prosthesis implantation breast reconstruction group(PMF group,n=15).The operation time, hospital stay,incision infection rate,subcutaneous effusion rate and patients satisfaction were compared between the two groups.Results Compared with LDF group,PMF group had the higher satisfaction,lower incidence of incision infection,and the difference was statistically significant(P<0.05).There was significant difference in operation time and hospital stay between the two groups(P<0.05).Conclusion Compared with latissimus dorsi flap,the immediate breast reconstruction with retaining pectoralis major fascia covering prosthesis has the advantages of more safety,less trauma,fewer complications,faster postoperative recovery and higher patients satisfaction,which can be widely used in clinic.[Key words]Breast cancer Immediate breast reconstruction Pectoralis major fascia乳腺癌作为全球女性最常见的恶性肿瘤之一,严重威胁女性健康叫对于早、中期乳腺癌患者,手术治疗为首选治疗方案,众多术式中,对于无法保乳的患者,全乳切除仍是最主要的手术方式叫然而随着接受全乳切除术的患者逐渐增多,随之而来的患者心理问题日益凸显,影响其术后恢复及生活质量叫如今,乳腺癌患者的美学满意度以及肿瘤学的安全性已成为现代乳腺外科医师的目标铁本中心自2017年以来开始对适合的患者实施乳房重建手术,至今累计手术27例。
海绵骨针的英文说明

海绵骨针的英文说明Sponge Spicule: A Unique Natural Phenomenon with Versatile Applications.Sponge spicules, also known as sponge microneedles or sponge bone needles, are a fascinating natural phenomenon found in sponges, the simplest multicellular organisms found in both marine and freshwater environments. These unique structures, which serve as the skeleton and support system of sponges, are composed primarily of either silica or calcium and play a crucial role in the biology and ecology of these organisms.Structurally, sponge spicules are classified into several types based on their shape and arrangement. These include single-axed spicules, which grow along a single axis and can have straight or curved shafts with similar or dissimilar ends; four-axed spicules, also known as tetraradiate spicules, which have four radiating ends in a single plane, often reduced in number to become triradiate,diradiate, or uniradiate; triaxed spicules, which have three axes intersecting at right angles, resulting in asix-rayed structure that can vary in its terminal morphology; and multi-axed spicules, which branch out from a central point, forming a star-like structure.The arrangement and combination of these spiculeswithin the sponge body vary depending on the species, forming either a loose or dense network that supports the organism's structure. This variety in spicule type, number, and arrangement is a key factor in the classification of sponges, as it reflects their phylogenetic relationships and adaptive strategies.In addition to their structural role, sponge spicules also play a defensive function. Some spicules, known as "sclerotized" or "hard" spicules, are mineralized and hardened, making them resistant to predation. These hard spicules can protrude from the sponge's surface, serving as a defense mechanism against potential predators. Other spicules, called "flexible" or "soft" spicules, lack mineralization and are more pliable, allowing them to bendand flex within the sponge body.The unique properties of sponge spicules have also attracted the attention of scientists and researchers from various fields. One such area is biomimetics, which involves studying natural systems to gain insights into the design and function of materials and structures. Thesilica-based spicules of sponges, in particular, have been found to have remarkable optical and mechanical properties that could be harnessed for a range of applications.For instance, the silica spicules of sponges exhibit excellent optical transparency and refractive index, making them suitable for use in optical devices and sensors. Additionally, the unique microstructure of sponge spicules, which consists of a central silica core surrounded by an organic sheath, gives them remarkable mechanical strength and toughness. This combination of optical transparency and mechanical strength has led to the exploration of sponge spicules as potential candidates for use in optical fibers, sensors, and other photonic devices.Moreover, the ability of sponges to biosynthesizesilica spicules under ambient conditions offers a sustainable and environmentally friendly alternative to synthetic materials. This biosynthetic process, which involves the use of silicon-containing compounds found in seawater, could be harnessed to produce high-performance materials with desired optical and mechanical properties.Beyond their potential applications in the field of biomimetics, sponge spicules also hold promise in the field of cosmetics and dermatology. Due to their unique ability to penetrate the stratum corneum (the outermost layer of skin) without causing significant damage, sponge spicules have been investigated as potential ingredients in skin care products. These products, which are often marketed as "sponge microneedles" or "sponge bone needles," are purported to improve skin texture and appearance by stimulating collagen production and promoting natural exfoliation.In summary, sponge spicules are a remarkable natural phenomenon with a wide range of potential applications.From their role as the structural backbone of sponges to their use in biomimetics, optics, and cosmetics, these unique structures continue to fascinate scientists and researchers alike. As our understanding of sponge biology and the properties of their spicules grows, so too does the potential for harnessing their unique properties for a range of practical applications.。
运用薄层CT扫描评估四川汉族青年锁骨胸骨端骨骼年龄_赵欢

运用薄层CT 扫描评估四川汉族青年锁骨胸骨端骨骼年龄赵欢1,董晓爱1,郑涛1,青思含1,邓振华1,朱广友2(1.四川大学华西基础医学与法医学院法医病理教研室,四川成都610041;2.司法部司法鉴定科学技术研究所上海市法医学重点实验室,上海200063)摘要:目的运用薄层CT 扫描探索四川汉族青年锁骨胸骨端骨骺发育状况及其与生活年龄的关系。
方法结合Schmeling 等提出的骨发育分级法,并考虑本研究样本的年龄区间,将锁骨胸骨端骨骺发育分为4个等级。
依据上述骨骺发育等级阅读565例15~25周岁青年胸部薄层CT 片,并对锁骨胸骨端骨骺发育状况进行统计学描述性研究。
结果两性之间各级别骨龄的差异无统计学意义(P >0.05)。
同时,经验分布函数显示,评定为1级者100%小于18周岁,评定为2级者75%小于18周岁,评定为3级者超过94.5%大于18周岁,评定为4级者100%大于20周岁。
结论锁骨胸骨端骨骺发育在18周岁左右呈现一定规律。
据此,可应用薄层CT 扫描评估锁骨胸骨端骨骼年龄,为18周岁刑事责任年龄的判定提供依据。
关键词:法医人类学;体层摄影术,X 线计算机;年龄测定,骨龄;锁骨;骨骺;青年;汉族;四川中图分类号:DF795.1文献标志码:Adoi :10.3969/j.issn.1004-5619.2011.06.005文章编号:1004-5619(2011)06-0417-04Skeletal Age Estimation of Sternal End of Clavicle in Sichuan Han NationalityYouth Using Thin-section Computed TomographyZHAO Huan 1,DONG Xiao-ai 1,ZHENG Tao 1,QING Si-han 1,DENG Zhen-hua 1,ZHU Guang-you 2(1.Department of Forensic Pathology,West China School of Preclinical and Forensic Medicine,SichuanUniversity,Chengdu 610041,China;2.Shanghai Key Laboratory of Forensic Medicine,Institute of Forensic Science,Ministry of Justice,P.R.China,Shanghai 200063,China )Abstract :Objective To explore the growth status of epiphysis of sternal end of clavicle using thin-section computed tomography (CT )and to study the relationship between the status and the chronological age of Sichuan Han nationality youth.Methods According to the Schmeling ’s report and the age range of our samples,the ossification status of medial clavicle epiphysis was classified as four stages.CT films of 565patients between 15and 25years were studied based on the classification and analyzed statistically.Results There was no statistical difference between the sexes (P >0.05).The calculated empiric distribution function showed that 100%of stage 1patients were under 18years,75%of stage 2patients were under 18years,94.5%of stage 3patients were over 18years,and 100%of the stage 4patients were over 20years,respective -ly.Conclusion The ossification of medial epiphysis of the clavicle for those around 18years has certain regular.These characteristics can be used for forensic identification of the skeletal age,especially 18years,which is the criminal responsibility age.Key words :forensic anthropology;tomography,X-ray computed;age determination by skeleton;clavicle;epiphyses;youth;Han nationality;Sichuan 作者简介:赵欢(1986—),女,河北廊坊人,蒙古族,硕士研究生,主要从事法医临床学鉴定和研究;E-mail :390355979@ 通信作者:邓振华,男,教授,硕士研究生导师,主要从事法医临床学教学与研究;E-mail :fydzh63@通信作者:朱广友,男,研究员,硕士研究生导师,主要从事法医临床学与男子性功能障碍鉴定与研究;E-mail :zhugy@活体年龄鉴定是司法鉴定的难点之一。
2021医学考研复试:耳鼻喉[SC长难句翻译文]
![2021医学考研复试:耳鼻喉[SC长难句翻译文]](https://img.taocdn.com/s3/m/a5dcb95f4431b90d6d85c711.png)
木仓医学考研复试SCI长难句耳鼻喉第一章-急性中耳炎Acute otitis media(AOM)is seen extremely frequently during childhood and75%of pre-school age children have been reported to have suffered at least one episode.Intracranial spread of infection is among the complications that may develop.Within the middle ear cavity(MEC),the mechanisms of AOM in the MEC which could make an individual susceptible to the development of inflammation are only partially known. The5most common bacteria associated with AOM are Streptococcus pneumoniae,Haemophilus influenzae,Moraxella catarrhalis, Streptococcus pyogenes,and Staphylococcus aureus.The most common viruses that can contribute to AOM are human rhinovirus,influenza viruses,respiratory syncytial virus,adenovirus,and enterovirus.Patients with AOM suffer a reduced quality of life because of pain,hearing loss, headaches,and cognitive impairment.急性中耳炎(AOM)在儿童期极为常见,据报道,75%的学龄前儿童至少经历过一次发作。
慢性阻塞性疾病科普PPT模板

03
RECOMMENDATIONS
Here you could describe the topic of the section
06
CONCLUSIONS
Here you could describe the topic of the section
INTRODUCTION
Mercury is the closest planet to the Sun and the smallest one in the Solar System—it’s only a bit larger than our Moon. The planet’s name has nothing to do with the liquid metal since it was named after the Roman messenger god, Mercury
The biggest planet in our Solar System. Jupiter is the
fourth-brightest
SATURN
This is the ringed one. It’s a gas giant,
composed mostly of hydrogen
01
PATHOLOGY
JUPITER
Jupiter is a gas giant and the biggest planet in our Solar System
DESKTOP SOFTWARE
You can replace the image on the screen with your own work. Just delete this one, add yours and send it to the back
“诸痛痒疮,皆属于心”对针刺治疗慢性荨麻疹的启示

•仁心雕龙•“诸痛痒疮,皆属于心”对针刺治疗慢性荨麻瘆的启示高德强\王煜明^刘岩\杨佼\徐晨琛、曾志见、解晨露\方继良、崔炳南1 (i中国中医科学院广安门医院,北京100053; 2北京中医药大学东直门医院,北京100700)摘要:“诸痛痒疮,皆属于心”是《黄帝内经》中关于病机的重要论述。
目前应用此条文指导以瘙痒为主要表现的慢性荨麻疹中医治疗的讨论相对不足。
文章从医理源流、临床应用、科研思考3个角度展幵论述,认为应重视精神因素在慢性荨麻疹发生和发展中的作用,治疗时重视调血安神,通过高质量研究设计,验证“诸痛痒疮,皆属于心”指导下的针刺干预方案的疗效,通过血液指标以及脑功能成像等进一步阐释针刺起效机制,丰富“诸痛痒疮,皆属于心”内涵。
关键词:针刺;慢性荨麻疹;理论探讨基金资助:首都卫生发展科研专项项目(No.2018-2-4152 ),国家A然科学基金面上项目(N o.81774433,N〇.81973867 ),国家重点研发计划(N〇.2018YFC1705802 )Enlightenment of f c pain, itch, and sore are always associated with heart9 on thetreatment of chronic urticaria with acupunctureGAO De-qiang1,WANG Yu-ming1,LIU Yan2,YANG Jiao1,XU Chen-chen1,ZENG Zhi-jian1,XIE Chen-lu1,FANG Ji-liang1,CUI Bing-nan1('Guang'anmen Hospital, China Academy of Chinese Medical Sciences, Beijing 100053, China; :Dongzhimen Hospital,Beijing University of Chinese Medicine, Beijing 100700, China )Abstract: 'Pain, itch, and sore are always associated with heart' is an important exposition on disease cause pattern in Huangdi Neijing.At present, applying this theory in acupuncture for treating chronic urticaria which is characterized by recurrentitch and wheals is relatively inadequate. The article discussed the theory in terms of origin, clinical application, and research prospects. It is believed that psychiatric and psychological are vital factors in the incidence and progression of chronic urticaria,thus regulating blood and pacify the spirit in the context of Chinese medicine should be emphasized. Further research is needed to examine the efficacy of acupuncture treatment guided by the theory, enrich connotation of the theory by blood biomarker and brain function imaging.Key W O rd st Acupuncture; Chronic urticaria; Theoretical discussionFunding:Capital Funds for Health Development Scientific Research (No.2018-2-4152), General Program of National Natural Science Foundation of China (No.81774433, No.81973867), National Key R&D Program of China (N〇.2018YFC 1705802)荨麻疹是由于皮肤、黏膜小血管扩张及渗透性 增加导致的一种局限性水肿,表现为大小不等的风 团与瘙痒[1_21,病程超过6周称为慢性荨麻疹。
孔子的师道英语作文

孔子的师道英语作文Title: The Exemplary Pedagogy of Confucius。
In the annals of history, few figures have left as indelible a mark on the realm of education as Confucius. His pedagogical philosophy, encapsulated in the notion of "师道," or the Way of the Teacher, continues to resonate across cultures and centuries. Let us delve into the essence of Confucius' pedagogy and explore its relevance in contemporary education.At the heart of Confucius' teaching philosophy lies the profound belief in the transformative power of education. He viewed teaching not merely as the imparting of knowledge but as a holistic endeavor aimed at nurturing virtuous individuals who would contribute meaningfully to society. Central to this approach was the cultivation of moral character, grounded in the principles of benevolence, righteousness, propriety, wisdom, and faithfulness.One of the key tenets of Confucius' pedagogy is the notion of leading by example. He emphasized the importance of virtuous conduct in teachers, asserting that they should embody the values they seek to instill in their students. Confucius famously remarked, "Is it not a pleasure, having learned something, to try it out at due intervals? Is it not a joy to have friends come from afar? Is it not gentlemanly not to take offense when others fail to appreciate your abilities?" Here, he underscores the reciprocal relationship between teacher and student, suggesting that the teacher's behavior serves as a modelfor emulation.Furthermore, Confucius advocated for personalized instruction, tailoring his teaching methods to the individual needs and abilities of his students. He recognized that effective education requires adaptability and flexibility, eschewing a one-size-fits-all approach in favor of personalized guidance. By understanding each student's strengths, weaknesses, and unique circumstances, Confucius sought to maximize their potential for growth and development.Another cornerstone of Confucius' pedagogy is the emphasis on experiential learning. He believed in the value of hands-on experience and practical application, encouraging students to actively engage with the material through reflection and action. Confucius once remarked, "I hear and I forget. I see and I remember. I do and I understand." This aphorism encapsulates his belief in the importance of experiential learning, suggesting that true understanding arises from direct experience.Moreover, Confucius stressed the importance offostering a supportive and nurturing learning environment. He emphasized the role of mutual respect and trust between teacher and student, creating a space conducive to open dialogue and intellectual exploration. Confucius regarded education not as a solitary pursuit but as a collaborative endeavor, wherein teachers and students alike contribute to each other's growth and development.In today's rapidly changing world, Confucius' pedagogical principles remain as relevant as ever. In anera characterized by technological advancements and globalization, the need for ethical leadership and moral guidance has never been greater. Confucius' emphasis on character education and the cultivation of virtuous individuals speaks to the timeless quest for wisdom and enlightenment.In conclusion, Confucius' pedagogy offers invaluable insights into the art and science of teaching. His emphasis on leading by example, personalized instruction, experiential learning, and nurturing environment provides a timeless blueprint for effective education. By embracing the Way of the Teacher, educators can inspire and empower the next generation to realize their full potential and make meaningful contributions to society. As Confuciusaptly put it, "Education breeds confidence. Confidence breeds hope. Hope breeds peace."。
成人大骨节病膝关节病变的阶梯化治疗
通讯作者:许鹏E mail:sousou369@Corresponding author:XU Peng E mail:sousou369@大骨节病(Kashin-Beck disease ,KBD )是一种地方性、慢性变形性骨关节病,主要发生于儿童发育期间四肢骺软骨、骺板软骨及关节软骨,致其变性和深层软骨细胞坏死。
KBD 在临床上表现为多发性、对称性关节受累,患者多在4~8岁甚至更早出现手指(趾)关节增粗、变形,严重者发展为膝、踝关节内外翻畸形及继发性骨关节炎症状和体征[1-2]。
KBD 区别于其他骨关节病,主要是病理变化为软骨细胞坏死以深层为主而表层细胞损伤较轻较晚[3]。
与正常人相比,KBD 患者关节软骨破坏严重,出现大量围绕坏死区的软骨细胞簇;当干骺与骨骺未闭合时,常导致生长板软骨发生多发性点状、带状和片状的凝固性软骨细胞坏死,进而通过坏死灶的钙化、骨化形成横骨梁致软骨发育障碍、抑制管状骨纵行生长,造成患者骨骼发育不良、身材矮小及骨端膨大。
与其他退行性关节疾病相似,成人KBD 患者以负重大关节退化最为严重,尤其是膝关节。
KBD 治疗的主要目标是减轻疼痛,保护关节活动度和预防继发性功能障碍和关节损伤。
目前还没有任何医学干预显示可以阻止疾病进展或逆转关节损伤,对医学治疗方法有效性的研究也很少[4-6]。
KBD 不仅严重损害病区居民健康,在制约当地发展经济的同时,也是造成“因病致穷、因病返贫”的重要公共卫生问题之一。
因此,有效预防和救治成人KBD ,改善其关节功能障碍,已经成为我国急需解决的重大社会问题。
1概述KBD 最早于1849年由俄罗斯界标师尤林斯基发现并报道,迄今已160余年,其后俄罗斯军医卡辛(Kashin )和贝克(Beck )对大骨节病进行了较详尽的调查,提出本病是一种独立的骨关节病,因此国际上把大骨节病称为卡辛-贝克病。
与骨关节病相比,目前国内外对KBD 的研究治疗报道相对较少,这主要是因为KBD 属于地区性疾病,主要分布于东北、西北、内蒙古、河南等地的潮湿寒冷山谷地区,存在着经济落后等特点,故较少被国际及国内所广泛重视。
《2023年美国肝病学会实践指南:+肝硬化门静脉高压和静脉曲张的风险分层及管理》摘译

《2023年美国肝病学会实践指南:肝硬化门静脉高压和静脉曲张的风险分层及管理》摘译雒博晗,韩国宏西安国际医学中心医院消化内科,西安 710100通信作者:韩国宏,139****************(ORCID: 0000-0003-4568-3776)摘要:本实践指南旨在整合最佳实践建议,用于在慢性肝病患者中识别门静脉高压、预防首次肝功能失代偿、管理急性静脉曲张出血以及降低静脉曲张再出血的风险。
该指南中最重要的变化涉及承认代偿期进展性慢性肝病的概念,使用无创评估识别临床有意义的门静脉高压,在发现门静脉高压时建议尽早使用非选择性β-受体阻滞剂,进一步探讨门静脉高压的潜在未来药物治疗选择,阐明优先经颈静脉肝内门体静脉分流术在急性静脉曲张出血中的作用,以及讨论胃底静脉曲张治疗相关的最新数据,并提出了新的主题,如门静脉高压性胃病、经食管超声心动图和抗肿瘤治疗前的内窥镜检查。
关键词:肝硬化;门静脉高压;食管和胃静脉曲张;美国An excerpt of AASLD practice guidance on risk stratification and management of portal hypertension and varices in cirrhosis (2023)LUO Bohan, HAN Guohong.(Department of Gastroenterology, Xi’an International Medical Center Hospital, Xi’an 710100, China)Corresponding author: HAN Guohong,139****************(ORCID: 0000-0003-4568-3776)Abstract:This Practice Guidance intends to coalesce best practice recommendations for the identification of portal hypertension (PH),for prevention of initial hepatic decompensation,for the management of acute variceal hemorrhage (AVH),and for reduction of the risk of recurrent variceal hemorrhage in chronic liver disease. The most significant changes in the current Guidance relate to recognition of the concept of compensated advanced chronic liver disease, codification of methodology to use noninvasiveassessments to identify clinically significant PH (CSPH), and endorsement of a change in paradigm with the recommendation of early utilization of nonselective beta-blocker therapy when CSPH is identified. The updated guidance further explores potential future pharmacotherapy options for PH,clarifies the role of preemptive transjugular intrahepatic portosystemic shunt in AVH,discusses more recent data related to the management of cardiofundal varices, and addresses new topics such as portal hypertensive gastropathy and endoscopy prior to transesophageal echocardiography and antineoplastic therapy.Key words:Liver Cirrhosis; Portal Hypertension; Esophageal and Gastric Vorrices; United States本实践指南[1]更新并扩展了美国肝病学会(AASLD)于2017年发布的门静脉高压(portal hypertension,PH)和胃食管静脉曲张管理的实践指南,为预防和管理PH提供了数据支持。
开启片剂完整性的窗户(中英文对照)
开启片剂完整性的窗户日本东芝公司,剑桥大学摘要:由日本东芝公司和剑桥大学合作成立的公司向《医药技术》解释了FDA支持的技术如何在不损坏片剂的情况下测定其完整性。
太赫脉冲成像的一个应用是检查肠溶制剂的完整性,以确保它们在到达肠溶之前不会溶解。
关键词:片剂完整性,太赫脉冲成像。
能够检测片剂的结构完整性和化学成分而无需将它们打碎的一种技术,已经通过了概念验证阶段,正在进行法规申请。
由英国私募Teraview公司研发并且以太赫光(介于无线电波和光波之间)为基础。
该成像技术为配方研发和质量控制中的湿溶出试验提供了一个更好的选择。
该技术还可以缩短新产品的研发时间,并且根据厂商的情况,随时间推移甚至可能发展成为一个用于制药生产线的实时片剂检测系统。
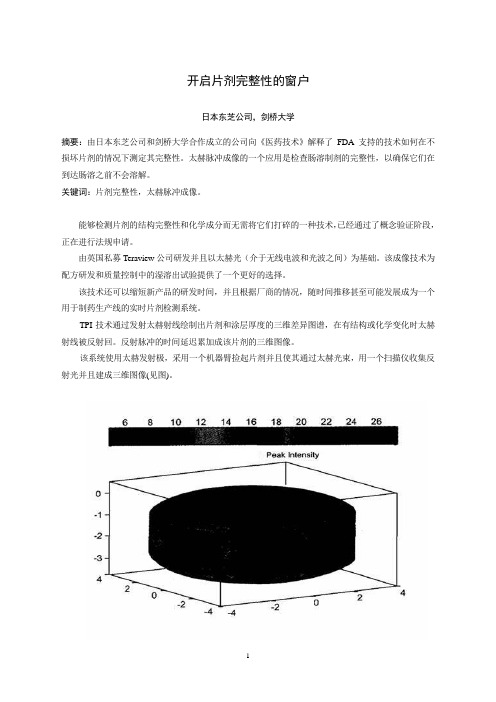
TPI技术通过发射太赫射线绘制出片剂和涂层厚度的三维差异图谱,在有结构或化学变化时太赫射线被反射回。
反射脉冲的时间延迟累加成该片剂的三维图像。
该系统使用太赫发射极,采用一个机器臂捡起片剂并且使其通过太赫光束,用一个扫描仪收集反射光并且建成三维图像(见图)。
技术研发太赫技术发源于二十世纪九十年代中期13本东芝公司位于英国的东芝欧洲研究中心,该中心与剑桥大学的物理学系有着密切的联系。
日本东芝公司当时正在研究新一代的半导体,研究的副产品是发现了这些半导体实际上是太赫光非常好的发射源和检测器。
二十世纪九十年代后期,日本东芝公司授权研究小组寻求该技术可能的应用,包括成像和化学传感光谱学,并与葛兰素史克和辉瑞以及其它公司建立了关系,以探讨其在制药业的应用。
虽然早期的结果表明该技术有前景,但日本东芝公司却不愿深入研究下去,原因是此应用与日本东芝公司在消费电子行业的任何业务兴趣都没有交叉。
这一决定的结果是研究中心的首席执行官DonArnone和剑桥桥大学物理学系的教授Michael Pepper先生于2001年成立了Teraview公司一作为研究中心的子公司。
TPI imaga 2000是第一个商品化太赫成像系统,该系统经优化用于成品片剂及其核心完整性和性能的无破坏检测。
自体心包补片修补主动脉瓣环辅助主动脉瓣置换★(论文)

中国组织工程研究 第17卷 第5期 2013–01–29出版Chinese Journal of Tissue Engineering Research January 29, 2013 Vol.17, No.5doi:10.3969/j.issn.2095-4344.2013.05.001 []夏冰,文冰,许华山,付国伟,赵文增. 自体心包补片修补主动脉瓣环辅助主动脉瓣置换[J].中国组织工程研究,2013,17(5):761-768.ISSN 2095-4344 CN 21-1581/R CODEN: ZLKHAH 761www.CRTER .org夏冰★,男,1986年生,河南省沈丘县人,汉族,郑州大学第一附属医院在读硕士,主要从事心外科基础与临床研究。
****************通讯作者:赵文增,硕士,主任医师,教授,博士生导师,郑州大学第一附属医院心血管外科,河南省郑州市 450052 ************.cn中图分类号:R318 文献标识码:A 文章编号:2095-4344 (2013)05-00761-08收稿日期:2012-12-02 修回日期:2013-01-16 (20121202004/M ·C)自体心包补片修补主动脉瓣环辅助主动脉瓣置换★夏 冰,文 冰,许华山,付国伟,赵文增郑州大学第一附属医院心血管外科,河南省郑州市 450052文章亮点:1通过主动脉瓣置换前后临床及影像学资料的比较,认识自体心包补片修补主动脉瓣环技术辅助主动脉瓣置换的临床效果及优势。
2 文章结合了自体心包补片修补主动脉瓣环技术辅助主动脉瓣置换的操作示意图,阐明了该技术的具体操作步骤,有较强的临床指导意义。
关键词:器官移植;心肺移植;组织移植;自体心包补片;钙化性主动脉瓣狭窄;心脏瓣膜假体;主动脉瓣环;主动脉瓣置换;超声心动图;器官移植图片文章摘要背景:在主动脉置换过程中常遇到瓣环钙化、瓣周囊肿等特殊情况,这时一般应用特殊技术辅助主动脉瓣置换。
粒子列表

粒子列表维基百科,自由的百科全书这是一份粒子物理学的粒子清单,包括已知的和假设的基本粒子,以及由它们合成的复合粒子。
关于根据发现年代顺序排列的亚原子粒子清单,请参见粒子发现年表。
目录[隐藏]∙ 1 基本粒子o 1.1 标准模型▪ 1.1.1 费米子(具有半整数自旋)▪ 1.1.2 玻色子(具有整数自旋)o 1.2 假想的粒子∙ 2 复合粒子o 2.1 强子▪ 2.1.1 重子(费米子)▪ 2.1.2 介子(玻色子)▪ 2.1.3 非常规强子态o 2.2 原子核o 2.3 原子o 2.4 里德伯原子∙∙∙∙∙∙[编辑]基本粒子基本粒子是没有可测量的内在结构的粒子,就是说,它不是其他粒子的复合。
它们是量子场论的基本物质。
基本粒子可以根据它们的自旋分类,费米子有半整数自旋而玻色子有整数自旋。
[编辑]标准模型主条目:标准模型标准模型“标准模型”所呈现的是我们目前对于基本粒子物理的了解,人们已观测到所有标准模型中的粒子。
[编辑]费米子(具有半整数自旋)主条目:费米子费米子具有半整数自旋,每个费米子都有对应的反粒子。
费米子是所有物质的基本组成成份。
费米子有两种形式,一种是夸克另一种是轻子,它们最大的不同是前者有色荷交互作用而后者没有。
∙夸克具有三种色荷(colour)的特性,分别是红(R)、绿(G)、蓝(B),反夸克具有三种补色,分别是R、G、B。
世代同位旋特点名称/味道符号电荷e质量(MeV/c2)反粒子符号电荷e11/2 I z=-1/2 下夸克−1/3 4.8+0.7-0.3反下夸克+1/31/2 I z=+1/2 上夸克+2/3 2.3+0.7-0.5反上夸克−2/320 S=-1 奇夸克−1/3 95±5反奇夸克+1/30 C=1 魅夸克+2/3 1275±25反魅夸克−2/330 B=-1 底夸克−1/3 4180±30反底夸克+1/30 T=1 顶夸克+2/3 173.5 ± 0.6 ± 0.8 GeV反顶夸克−2/3[编辑]玻色子(具有整数自旋)主条目:玻色子玻色子有整数自旋,基本交互作用是由规范玻色子传递,则希格斯玻色子是把质量赋予规范传播子和费米子。
颈动脉慢性完全闭塞后再通的症状英文

69%
Distal protection device used after crossing
27
73%
PercuSurge/FilterWire
17/10
63%/37%
Post-dilatation balloon diameter (mm)
In-hopsital , n (%)
3-m follow-up, n (%)
Death
1 (1.9)
1 (1.9)
Fatal stroke
1 (1.9)
1 (1.9)
Other cause
0
0
Stroke
2 (3.7)
2 (3.7)
Major ipsi.
0
0
Major non-ipsi.
35
65%
Lesion location, right/left
27/27
50%/50%
CCA diameter (mm)
7.9±0.6
ICA diameter (mm)
5.1±0.5
Occlusion length (mm)
27.9±16.2
Wire crossing successful
Paul HL Kao 08
Prognosis and pathophysiology of ICAO
Cervical ICAO is an important cause of TIA and cerebral infarction and should not be neglected Annual risk of ipsilateral stroke in symptomatic ICAO is 6-20% Annual risk of ipsilateral stroke in asymptomatic ICAO is 2-5 % Pathophysiology of symptoms Emboli arising from ECA/CCA via collaterals Emboli arising from ICA stump via collaterals (Stump syndrome) Emboli arising from trailing thrombi distal to the occlusion Hypo-perfusion (hemodynamic insufficiency)
美国医师协会压疮指南

Pressure Ulcers CPG Assessment压疮评估
Pressure Ulcer Classifications – continued • Stage 3: Full thickness skin loss involving damage to, or
necrosis of, subcutaneous tissue that may extend down to, but not through, fascia. The ulcer presents clinically as a deep crater with or without undermining of adjacent tissue 三期压疮 • Stage 4: Full thickness skin loss with extensive destruction, tissue necrosis or damage to muscle, bone, or supporting structures (e.g., tendon, joint capsule). Undermining and sinus tracts also may be associated四 期压疮
An effective assessment includes有效的评估包括:
• Define and interpret factors affecting treatment and wound healing such as physical, functional and psychosocial factors定义和解释关于治疗和伤口康复的影 响因素,例如身体的,功能的和心理方面的因素。
• Shearing剪切力 • Friction摩擦力 • Moisture潮湿
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
a r X i v :h e p -e x /0406020v 1 7 J u n 2004SPARTICLE RECONSTRUCTION AT LHCALESSIA TRICOMIon behalf of the ATLAS and CMS CollaborationsDepartment of Physics and Astronomy,University of Catania,and INFN Catania,Via S.Sofia 64,I-95123Catania,ItalyIn this report a review of recent studies made to understand the capability to discover and measure properties of SUSY particles at LHC is discussed.The expected resolution on sparticle masses is discussed on the basis of studies performed by the ATLAS and CMS collaborations.1IntroductionOne of the main purposes of the LHC collider is to search for Physics beyond the Standard Model (SM).Supersymmetric (SUSY)extensions of SM 1predict the existence of superpatners for all ordinary particles.If supersymmetry exists at the electroweak scale,it could hardly es-cape detection at LHC.The centre-of-mass energy of 14TeV,available at LHC,extends the searches for SUSY particles up to masses of 2.5to 3TeV/c 2.In R-parity conserving mod-els,the stable Lightest Supersymmetric Particles (LSP),which escape detection,lead to events characterized by large missing ually,squarks and/or gluinos are the most abundant sparticles produced at LHC.They decay in a number of steps to quarks,charginos,neutralinos,sleptons,W,Z,Higgs bosons,etc.These events are expected to show up at LHC via an excessof multijet+E miss T+multilepton final states compared to the SM expectations 2.A significant part of the efforts in preparation for the LHC startup is being spent in the simu-lations of the new physics potential.In the past years,the simulation studies have been mainly devoted to understand the discovery reach of SUSY particles through inclusive studies.In these studies,the typical discovery strategy consists in searching for an excess of events with a given topology with respect to the Standard Model expectations.A variety of final state signa-tures has been considered.Inclusive studies have mainly been carried out in the framework of mSUGRA 3,4,with five independent parameters:the common gaugino mass m 1/2,the common scalar mass m 0,the common trilinear scalar coupling A 0,the ratio of the vacuum expectation values of the two Higgs doublets tan βand the sign of the Higgsino mixing parameter µ.Strongindications exist,however,that the overall SUSY reach in terms of masses of squarks and gluinos is very similar in most the R-parity conserving scenarios,provided that mχ01≪m˜g,˜q.This has been shown to be the case for the AMSB model5and even for the MSSM6.Already with only 1fb−1of integrated luminosity,LHC should be able to discover squarks and gluinos if their masses do not exceed about1.3TeV/c2.With100fb−1the reach can be extended up to masses m˜q∼m˜g∼2.5TeV/c2.The entire plausible domain of EW-SUSY parameter space for most probable value of tanβcan be probed.Determining the masses of supersymmetric particles is more difficult,because each SUSY event contains two LSP’s,and there are not enough kinematic constraints to determine the momenta of these particles.The main goal of this report,is to show the potential of the ATLAS7and CMS detectors8to reconstruct SUSY particles and the achievable mass resolution.2SUSY Particle MeasurementsThe reconstruction of sparticle masses and the determination of their properties might help in probing different models.In order to reconstruct sparticle masses,a different strategy with respect to that developed for inclusive analyses must be used.The typical procedure consists of several steps:(i)choose a set of benchmark points compatible with all existing measurements and spanning the whole SUSY parameter space,(ii)choose a particular decay chain,(iii)get the mass spectrum,exploit the kinematical properties such as the presence of characteristic end points or thresholds,andfinally(iv)try to reconstruct sparticles using constraints from various mass combinations9.The choice of benchmark points depends on the purpose of the actual investigation.A large variety of benchmark points have been proposed in the past.The studies presented in this report rely on a set of points4,10,11,which takes into account constraints from LEP results,cosmology measurements and low-energy experiments.2.1Dilepton edge reconstructionSquark and gluino decays are often characterized by long decay chains in which the next-to-lightest neutralino(χ02)is abundantly produced.Theχ02may then decay into the LSP through the chainχ02→˜ℓ±ℓ∓→χ01ℓ+ℓ−.Leptons(electrons and muons)from theχ02decay exhibit aℓ+ℓ−invariant mass distribution with a sharp edge.If mχ02<m˜ℓ+mℓ,theχ02decay is a threebody decay mediated by a virtual slepton and the edge is placed at mχ02−mχ01.Similarly,whenmχ02>m˜ℓ+mℓ,the neutralino decay is a two-body decay and the corresponding edge is placedatMℓ+ℓ−=m˜ℓ.(1)Figure1shows the same-flavour opposite-sign(SFOS)dilepton invariant mass distribution for a CMS simulation probing the point B of Ref.10.The Standard Model background,due mostly to t010*******400500600700800900M(e +e -)+M(µ+µ-) (GeV)E v e n t s / 3 G e V10203040506070M(e +e -)+M(µ+µ-) (GeV)E v e n t s / 2 G e VFigure 1:(a)Invariant mass distribution of SFOS isolated leptons for ˜q and ˜g events,superimposed on the SMbackground.The contributions of t ¯t and Z+jets events are shown.(b)Same as in (a)with E missT >150GeV cut.2.2Squark and Gluino Mass ReconstructionThe reconstruction of a χ02is the starting point for more complex decay chain reconstruction.Here,the technique used by CMS for squarks and gluino mass determination is briefly summa-rized.Three out of the thirteen “Post-LEP”benchmark points have been used for this analysis,the point B (m 1/2=250GeV/c 2,m 0=100GeV/c 2,tan β=10,µ>0and A 0=0),G (m 1/2=375GeV/c 2,m 0=120GeV/c 2,tan β=20,µ>0and A 0=0)and I (m 1/2=350GeV/c 2,m 0=180GeV/c 2,tan β=35,µ>0and A 0=0)of Ref.10,characterized both by relatively low value for m 0and m 1/2(high ˜q and ˜g production cross section)and differ-ent values of tan β.In order to perform ˜b(˜q )and ˜g mass reconstruction,the decay chain˜g →˜bb ,˜b →χ02b ,χ02→˜ℓ±ℓ∓→χ01ℓ+ℓ−,where ℓ=e ,µ,have been considered.The same decay chain with light quark replacing sbottom has been used for squark reconstruction.The events are selected by requiring at least two SFOS isolated leptons with p T >15GeV/c and |η|<2.4,corresponding to the acceptance of the muon system,and two jets (tagged as b jets in the case of sbottom reconstruction),with p T >20GeV/c and |η|<2.4.A cut on the missing energy is applied in order to suppress the SM background.The first step of the reconstruction proceeds as described in the previous paragraph from the dilepton edge.To reconstruct the sbottom (squark),events in a window about 15GeV/c 2wide around the edge are selected.This requirement allows the kinematical configuration in which the leptons are emitted back-to-backin the χ02rest frame,with the χ01at rest,to be selected.In this configuration the χ02momentumis reconstructed through the relationp χ02=1+m χ01for 10fb −1.The dependence of the reconstructed masses on the χ01mass uncertainty has been evaluated in Ref.13to be∆m (χ02b)=(1.60±0.03)∆m (χ01).(3)Although both m (˜q )and m (˜g )depend on the χ01mass,their difference is in contrast inde-pendent of m(χ01)and can be measured with an error of few percent,irrespective of the sparticlespectrum 13.05101520253035M(χ∼20 q) (GeV/c 2)E v e n t s / 20 G e V /c25101520253035M(χ∼20 b) (GeV/c 2)E v e n t s / 26 G e V /c25101520253035M(χ∼20 b b) (GeV/c 2)E v e n t s / 28 G e V /c2Figure 2:Reconstructed invariant mass distribution for squark (left),sbottom (middle)and gluino in the sbottomchain (right)at point B.The integrated luminosity is 1fb −1for the squark peak and 10fb −1for the sbottom and the gluino peaks.All the results shown so far are derived for point B (with parameters similar to that of point SPS1A)and for an integrated luminosity of 10fb −1.The same kind of analysis was repeated also for point G.In this case,however,the higher value of tan βreflects into higher branchingratio for the decay χ02→τ+τ−χ01,hence to a smaller signal χ02→˜ℓ±ℓ∓→χ01ℓ+ℓ−,ℓ=e ,µ.Reconstruction of squarks and gluinos is only possible with tighter cuts and with high integrated luminosity.An attempt was made to repeat the analysis at point I of Ref.10,characterized by a yet higher value of tan β(tan β=35).For that point,even with an integrated luminosity of 300fb −1,it is not possible to reconstruct squarks and gluinos with this method.2.3χ01Mass DeterminationIn sequential decays,the presence of other end points and thresholds,as suggested in Ref.9,can be used to extract,in a model-independent way,the masses of the sparticles,and,finally,to disentangle different models.The starting point is the same decay chain as in the previous section.The two leading jets are assumed to come from the squark decays and are combined with the lepton to find other end points and thresholds.For example,the largest dilepton-jetmass,M ℓℓq and the largest lepton-jet masses,for the first and the second lepton,M max ℓqand M min ℓq ,are expected to give end points as well as M ℓℓq should give a threshold.The distributions of these quantities are shown in Fig.3.Other end points are clearly visible and well measurable,despite various detection and reconstruction spoiling factors.With the high statistics reachable at LHC,it seems possible to measure the end points with a precision limited only by the hadronic scale accuracy (1to 2%depending on the particle combinations for point B or SPS1A).It is possibile to extract the masses of the sparticles with a combination of all these end point measurements.In particular,the mass of χ01is a fundamental ingredient of the other sparticle mass measurements.In Fig.4,the reconstructed χ01mass peak is shown.A resolution of about 10%is achievable,within a given model.In Fig.5the result of the fits with the mSUGRA Point 5(S5)and the point in an Optimized String Model (O1)9are compared.Figure3:ATLAS invariant mass distributions with kinematical end points for the mSUGRA Point SPS1A. ConclusionsIf SUSY exists at the EW scale,both the ATLAS and CMS will be able to discover it over a large range of the paramater space.Squark and gluino decays present characteristic signatures to discriminate the SUSY processes from the Standard Model.Inclusive studies have demonstrated that squarks and gluinos could be discovered already in thefirst months of data taking.With the ultimate luminosity of300fb−1,strongly interacting sparticles could be discovered up to masses of2.5to3TeV/c2.Altough sparticle reconstruction is more difficult,new analyses have shown that in some cases it is possible to make exclusive reconstructions.A search for special features,like kinematical end points and thresholds,excesses of b/τ’s,isolated leptons helps in the reconstruction of full decay chains and,possibly,to disentangle different theoretical models.This is the case,for instance,for the decay˜g→˜q(˜b)q(b)which allows both squark(sbottom)and gluino masses to0.0050.010.0150.020.02550100150200250(a)m 1(GeV)d p /m 1 (/1Ge V )Figure 4:M (χ01)distribution for ATLAS point 5.50100150200250300350400m 1 (GeV)m l (G e V )Figure 5:Reconstructed M (˜ℓ)vs M (χ01)for O1and S5(see text).The stars show the true mass for each model.be reconstructed.Resolutions better than 10%are attainable in the low tan βregion,already after the first year of data taking.More work is in progress to evaluate the ATLAS and CMS capability to reconstruct SUSY sparticles.AcknowledgmentsI would like to thank the Conference Organizers for the invitation and for the friendly hospitality.Special thanks also to M.Chiorboli and G.Polesello for providing materials for the presentation and helpful discussion.I would like also to thank P.Janot for the rewieving.References1.H.P.Nilles,Phys.Rev.110,1(1984)2.H.Baer,C.H.Chen,F.Paige and X.Tata,Phys.Rev.D 52,2746(1995);Phys.Rev.D 53,6241(1996).3.S.Abdullin and F.Charles,Nucl.Phys.B 547,60(1999);S.Abdullin,ˇZ.Antunovi´c andM.Dˇz elalija,Mod.Phys.Lett.A 15,465(2000).4.The ATLAS Collaboration,ATLAS Detector and Physics Performance Technical Design Report ,CERN/LHCC 99-014(1999).5.A.J.Barr et al.,JHEP 0303(2003)045.6.S.Abdullin,A.Albert and F.Charles,in Proceedings of Les Houches 2001,Physics at TeV colliders ,p.161,ed.P.Aurenche et al.,(Paris,IN2P3,2001).7.The ATLAS Collaboration,Technical Proposal,CERN/LHCC 94-043(1994).8.The CMS Collaboration,CERN/LHCC 94-038(1994).9.B.C.Allanach et al.,JHEP 0009(2000)004.10.M.Battaglia et al.,Eur.Phys.J.C 22(2001)535.11.B.C.Allanach et al.,hep-ph/0202233(2002).12.B.K.Gjelsten et al.ATLAS-PHYS-2004-007(2004).13.M.Chiorboli and A.Tricomi,Squark and Gluino Reconstruction with the CMS Detector ,CMS RN-2003/002(2003).。