英-[药物报告]色瑞替尼
肺癌靶向治疗药物(按作用机制划分)
肺癌靶向药物(靶点机制划分)EGFR 突变EGFR又叫 HER1 或者 ErbB1,是 ErbB 受体家族四大成员之一。
EGFR 过分频繁表达能激活下游重要的信号通路(如 ALK),从而导致细胞增殖,存活,转移及血管生成等。
因此,在 NSCLC 的研究中,EGFR 一直是一个热点。
像吉非替尼和厄洛替尼这样早期的小分子 EGFR 酪氨酸激酶抑制剂(TKI)在刚问世时是面向所有既往接受过化疗的 NSCLC 患者的。
而像阿法替尼(afatinib)和达克替尼(dacomitinib)这样新推出的 EGFR TKI 则在此基础上有了长足的发展。
回顾性研究显示,亚裔、女性、腺癌、既往少量 / 无吸烟史等临床特点可以增加 EGFR TKI 治疗的敏感率。
这个结论的分子基础是,18-21 号外显子突变(最常见的是 19 号外显子的缺失和 21 号外显子上的 L858R 位点突变)能编码出大量 EGFR 酪氨酸激酶,上述突变分别占总突变情况的 45% 和 40%。
另外还有18 号外显子的突变及 20 号外显子的插入突变,占总突变情况的 5%-10%。
18 号外显子的突变能增加 EGFR TKI 的敏感性,而 20 号外显子的突变却会导致EGFR TKI 原发耐药。
EGFR 突变在拥有前述临床特征的患者中更加常见。
肺腺癌患者中,大约有 15% 的白种人和 30-50% 的东亚人拥有 EGFR 基因突变。
而对于那些无吸烟史的东亚人,这项比例高达 50-60%。
多项研究表明,对于初发的敏感性 EGFR 突变的 NSCLC 患者,应用 TKI 治疗在反应率(ORR)、无进展生存期(PFS)和生活质量上均优于化疗。
易瑞沙泛亚洲研究(IPASS)结果表明,对于经选择的 NSCLC 患者,吉非替尼效果优于紫杉醇 + 卡铂的化疗。
但对于EGFR 野生型患者,TKI 治疗效果并不理想,1.5 个月的 PFS 完败于化疗组的6.5 个月。
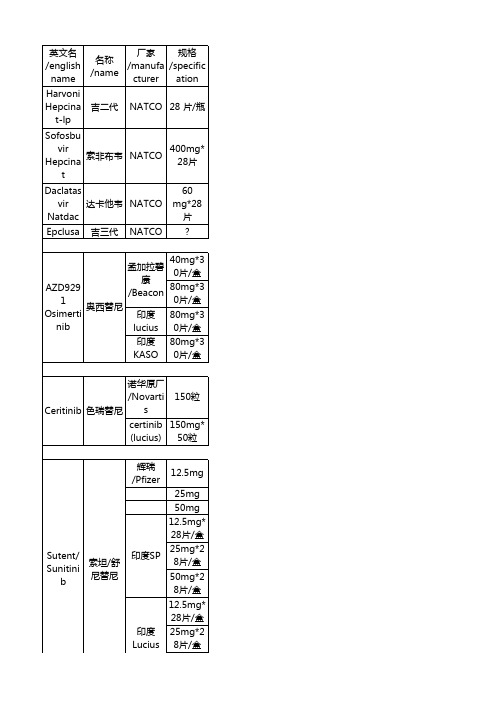
印度药目录表
Sevelam er 碳酸司维 Genzym 800mg* Carbona 拉姆 e 30片/瓶 te Sensipar 西那卡塞 (Cinacal PTH cet) Votrient 、 帕唑帕尼 Pazopan ib JAKAVI 鲁索利替 尼 印度 INTAS 30mg*1 0片/盒 200mg 400mg 诺华 20mg
赫赛汀/ Trastuzu 罗氏 曲妥单抗 / Roche mab 注射液 美罗华/ Rituxim 罗氏 利妥昔单 / Roche ab 抗注射液 VEENAT 格列卫
100mg* NATCO 120粒胶 囊 印度 lucius 20mG*6 0片 50MG*6 0片 70mg*6 0
Sprytax 达沙替尼
印度 Lucius 50mg*2 8片/盒 axitinib 阿西替尼 辉瑞 /Pfizer 5mg*28 片/盒
Lapatini 葛兰素史 250mg* 拉帕替尼 b 克/GSK 42片/盒 vemura 罗氏 240mg* 威罗非尼 genib /Roche 56片/盒 德 40mg*2 国,Germ 8粒 an Afatinib 阿法替尼 印度 lucius 40mg*3 0片
葛兰素
培美曲塞 PEMNA PEMNA T力比泰 NATCO T (注射 液) BD abirater one/Zyti 阿比特龙 ga CIPLA
500mg
250mg* 120粒 250mg* 120粒
GLENM 250mg* ARK 120粒 20mg*1 5胶囊
Temozol 替莫唑胺 omide
AZD929 1 奥西替尼 Osimerti nib
40mg*3 孟加拉碧 0片/盒 康 80mg*3 /Beacon 0片/盒 印度 lucius 印度 KASO 80mg*3 0片/盒 80mg*3 0片/盒
ALK基因突变和对应靶向药物

间变性淋巴瘤激酶(ALK)突变的形式有过量表达、与其他基因形成融合基因,发生点突变等等。
ALK基因融合突变是非小细胞肺癌(NSCLC)常见的一种驱动基因,中国非小细胞肺腺癌中ALK融合突变阳性的比例为5.3%,在非小细胞肺腺癌、年轻患者(小于60岁)以及不吸烟的人群中发生率较高,ALK阳性的非小细胞肺癌被认为是一种分子亚型,相对应的靶向药物与EGFR分子亚型完全不同。
ALK融合基因突变主要在肺腺癌里常见,一般肺鳞癌患者ALK融合基因突变概率很低,有报道说1400个肺鳞癌患者里ALK融合基因的发生率为1.3%。
考虑到ALK总体突变频率仅有5%,所以对于鳞癌患者也是可以做一下ALK检测的。
由于非小细胞肺癌里的驱动基因突变一般是互相排斥的,或者说一山不容二虎,癌细胞也没有必要搞两个驱动突变。
有研究说亚裔的EGFR、KRAS野生型的腺癌患者,ALK阳性比例高达30%-42%,因此如果发现EGFR 和KRAS是野生型,是更有必要测下ALK基因的。
一、ALK融合突变的检测图1:非小细胞肺癌中ALK的重排形式据报道,目前已发现21种EML4-ALK的融合形式,另外ALK还可能与TFG、KIF5B、KLC1、PTPN3、STRN等基因发生融合,因此ALK融合突变的诊断是存在一定难度的。
下表是关于ALK融合突变的诊断方法,及其相应的特点。
表1:ALK基因检测的方法需要注意,临床常用的三种方法是FISH、Ventana IHC及RT-PCR,三种方法FISH的灵敏度最低。
因此,如果是胸腔积液、细针穿刺取到的细胞学样本做成的蜡块,不建议使用FISH,避免假阴性。
另外通过抽血检测循环肿瘤DNA(ctDNA),循环肿瘤细胞(CTC)也正在发展起来。
总之在面对ALK检测结果模棱两可的时候,一定要换一个检测方法去验证,也没有哪一种方法灵敏度和特异性都是100%。
二、ALK的靶向药物ALK融合突变阳性的患者使用克唑替尼可以获益,克唑替尼具有ALK、c-MET、ROS1三个靶点。
各种杂质及价格-
专业承接美国、日本、法国、德国、瑞士、意大利、英国等国家参比制剂一次性进口和代购业务,提供进口〔EP、USP、LGC、BP、TLC、TRC、QCC、MC〕和国产对照品,有需要的欢迎联系我咨询哈.市振强生物技术劳先生135******** QQ3004867396各种杂质名称及英文名:依鲁替尼〔Ibrutinib〕杂质6个,palbociclib杂质6个,泰地唑胺杂质tedizolid phosphate 12个达格列净杂质Dapagliflozin 7个,索非布韦杂质sofosbuvir 20个,替卡格雷杂质Ticagrelor 14个,米拉贝隆杂质Mirabegron 10个,TAK 438杂质10个,沃替西汀杂质Vortioxetine 15个,LCZ696杂质6个非布司他杂质Febuxostat 14个泊沙康唑异构体Posaconazole 14个阿普斯特杂质Apremilast 6个阿奇霉素杂质Azithromycin 14个阿考替胺杂质Acotiamide 14个依托考昔杂质Etoricoxib 14个尼达尼布杂质Nintedanib 8个罗库溴铵杂质Rocuronium Bromide 8个恩杂鲁胺杂质Enzalutamide 4个卢帕他定杂质Rupatadine 6个瑞格非尼杂质Regorafenib 20个色瑞替尼杂质Ceritinib 11个依美斯汀杂质Emedastine8个依匹唑派杂质Brexpiprazole6个依帕司他杂质epalrestat6个乌苯美司杂质Ubenimex 19个福多司坦杂质Fudosteine 6个马来酸匹杉琼杂质Maleic acid Chinese fir, Joan 6个扎鲁司特杂质Zafirlukast 6个贝利司他杂质belinostat 6个奥扎格雷的杂质ozagrel 6个酒石酸伐尼克兰片杂质Varenicline Tartrate Tablets 6个莫扎伐普坦杂质Mozavaptan 5个沙芬酰胺杂质Safinamide 4个沃雷生杂质suvorexant 5个依替巴肽杂质Eptifibatide 5个乐伐替尼杂质lenvatinib 8个1.埃索美拉唑杂质esomeprazole impurity2.奥拉西坦杂质oxiracetam3.罗氟司特杂质roflumilast4.阿戈美拉汀杂质Agomelatine5.鲁拉西酮杂质Lurasidone6.莫西沙星杂质moxifloxacin7.阿齐沙坦杂质Azilsartan8.达比加群酯杂质Pradaxa9.利拉利汀杂质Linagliptin10.托法替尼杂质Tofacitinib11.依托考昔杂质12.阿西替尼杂质Axitinib13.维格列汀杂质Vildagliptin14.帕瑞昔布杂质parecoxib15.伊马替尼杂质imatinib16.阿哌沙班杂质Apixaban17.替诺福韦酯杂质Tenofovir Disoproxil Fumarate18.普拉格雷杂质Prasugrel19.伊拉地平杂质isradipine20.利托那韦杂质ritonavir21.培美曲塞二钠杂质pemetrexed disodium22.依达拉奉杂质Edaravone23.吉非替尼杂质gefitinib24.替吉奥杂质BCB25.苯达莫司汀杂质Cephalon26.替加环素杂质Tigecycline27.布南色林杂质Blonanserin28.文拉法辛杂质venlafaxine29.替卡格雷杂质30.利伐沙班杂质Rivaroxaban31.伊曲茶碱杂质Istradefylline32.依度沙班杂质Edoxaban33.三氟胸苷杂质Trifluorothymidine34.盐酸阿考替胺杂质acotiamide hydrochloride35.度洛西汀杂质Duloxetine36.泊沙康唑杂质37.泰地唑胺杂质38.沃替西汀杂质39.乐伐替尼杂志40.卡博替尼杂质Cabozantinib41.依鲁替尼杂质42.恩格列净杂质EMpagliflozin43.辛伐他汀杂质simvastatin44.恩杂鲁胺杂质45. 阿苯达唑Albendazole46. 阿达帕林adapalene47. 阿夫唑嗪alfuzosin48. 阿卡地新acadesine49. 阿立哌唑aripiprazole50. 阿莫曲普坦almotriptan51. 阿莫西林amoxicillin52. 阿瑞吡坦Aprepitant53. 阿昔洛韦acyclovir54. 埃罗替尼erlotinib55. 安非他酮bupropion56. 氨苄青霉素ampicillin57. 氨基葡萄糖Glucosamine58. 氨甲环酸tranexamic59. 氨溴索Ambroxol60. 胺碘酮Amiodarone61. 奥氮平olanzapine62. 奥沙利铂Oxaliplatin63. 奥司他韦oseltamivir64. 保胆键素dihydroxydibutylether65. 保特佐米Bortezomib66. 苯达莫司汀Bendamustin67. 比卡鲁胺bicalutamide68. 吡罗昔康piroxicam69. 吡嗪酰胺Pyrazinamide70. 别嘌醇allopurinol71. 波生坦bosentan72. 布洛芬Ibuprofen73. 布美他尼Bumetanide74. 雌甾四烯estratetraenol75. 醋氯芬酸aceclofenac76. 达非那新Darifenacin77. 大黄酸Diacerein78. 地尔硫卓diltiazem79. 地拉罗司deferasirox80. 氨氯地平Amlodipine81. 硝苯地平nifedipine82. 甲氨蝶呤Methotrexate83. 氨基蝶呤Aminopterin84. 丁螺环酮buspirone85. 多奈哌齐Donepezi86. 多立酮Domperidone87. 恩丹西酮ondansetron88. 恩他卡朋entacapone89. 伐昔洛韦valacyclovir90. 泛昔洛韦famciclovir91. 非布索坦Febuxostat92. 非那雄胺inasteride-ep93. 非诺贝特fenofibrate94. 弗斯特罗定fesoterodine95. 伏立康唑Voriconazole96. 氟替卡松丙酸酯fluticasone-propionate97. 氟维司群Fulvestrant98. 格列吡嗪glipizide99. 桂利嗪cinnarizine100. 环苯扎林cyclobenzaprine101. 加巴喷丁gabapentin102. 甲状旁腺激素西那卡塞Cinacalcet 103. 甲状腺素Levothyroxine104. 卡巴拉汀利凡斯的明Rivastigmine RC's 105. 喹硫平Quetiapine106. 奥美拉唑Omeprazole107. 兰索拉唑Lansoprazol108. 雷贝拉唑Rabeprazole109. 泮托拉唑pantoprazol110. 来氟米特leflunomide111. 雷洛昔芬raloxifene112. 雷莫拉宁Ramoplanin113. 雷奈佐利Linezolid114. 利伐沙班Rivaroxaban115. 利培酮Risperidal116. 罗匹尼罗ropinirole117. 阿替洛尔Atenolol118. 比索洛尔Bisoprolol119. 醋丁洛尔Acebutolol120. 美托洛尔metoprolol121. 奈必洛尔nebivolol122. 氯吡格雷Clopidogrel123. 氯雷他定Loratadine124. 霉酚酸mycophenolate125. 美洛昔康meloxicam126. 孟鲁司特montelukast127. 米氮平mirtazapine128. 尼美舒利nimesulide129. 帕罗西汀Paroxetine130. 帕立酮Paliperidone131. 生丁Dipyridamole Dipyridamole 132. 培美曲塞二钠Pemetrexed-disodium 133. 普拉克索Pramipexole134. 喹那普利Quinapril135. 卡托普利captopril136. 赖诺普利Lisinopril137. 雷米普利Ramipril138. 培哚普利Perindopril Imp139. 群多普利Trandolapril140. 伊拉普利Enalapril141. 普瑞巴林pregabalin142. 瑞格列奈Repaglinide143. 塞来西布Celecoxib144. 噻托溴铵Tiotropium bromide 145. 沙丁胺醇salbutamol146. 沙美特罗salmeterol147. 奥美沙坦Olmesartan 148. 坎地沙坦Candesartan 149. 罗沙坦Losartan150. 替米沙坦Telmisartan151. 缬沙坦Valsartan152. 加替沙星gatifloxacin153. 氟哌酸norfloxacin154. 菲宁达、氧氟沙星Ofloxacin 155. 恩诺沙星enrofloxacin 156. 环丙沙星Ciprofloxacin 157. 莫西沙星moxifloxacin158. 左氧氟沙星Levofloxacin 159. 舍曲林Sertraline160. 舒马曲坦sumatriptan 161. 双醋瑞因diacerein162. 双氯芬酸Diclofenac 163. 他达那非Tadalafil164. 阿托伐他汀atorvastatin 165. 洛伐他汀Lovastatin166. 匹伐他汀pitavastatin 167. 普伐他汀pravastatin 168. 瑞舒伐他汀Rosuvastatin 169. 辛伐他汀Simvastatin 170. 坦索罗辛Tamsulosin 171. 格列美脲glimepiride 172. 吡格列酮pioglitazone 173. 尼扎替丁nizatidine 174. 替卡西林Ticarcillin 175. 酮咯酸氨丁三醇Ketorolac 176. 酮基布洛芬Ketoprofen 177. 头孢氨苄cefalexin178. 头孢克洛cefaclor179. 头孢磺啶cefsulodin180. 托特罗定tolterodine 181. 拓扑替康topotecan182. 万古霉素vanycin183. 文拉伐辛Venlafaxine 184. 那非Sildenafil185. 西他列汀Sitagliptin186. 西酞普兰Citalopram 187. 西替利嗪cetirizine188. 伊立替康Irinotecan189. 伊马替尼imatinib190. 伊曲康唑Itraconazole191. 依泽替米贝ezetimibe192. 左乙拉西坦Levetiracetam193. 佐米曲普坦zolmitriptan194. 唑吡坦zolpidem195. 唑尼沙胺Zonisamide依鲁替尼〔Ibrutinib〕杂质6个,palbociclib杂质6个,泰地唑胺杂质tedizolid phosphate 12个达格列净杂质Dapagliflozin 7个,索非布韦杂质sofosbuvir 20个,替卡格雷杂质Ticagrelor 14个,米拉贝隆杂质Mirabegron 10个,TAK 438杂质10个,沃替西汀杂质Vortioxetine 15个,LCZ696杂质6个非布司他杂质Febuxostat 14个泊沙康唑异构体Posaconazole 14个阿普斯特杂质Apremilast 6个阿奇霉素杂质Azithromycin 14个阿考替胺杂质Acotiamide 14个依托考昔杂质Etoricoxib 14个尼达尼布杂质Nintedanib 8个罗库溴铵杂质Rocuronium Bromide 8个恩杂鲁胺杂质Enzalutamide 4个卢帕他定杂质Rupatadine 6个瑞格非尼杂质Regorafenib 20个色瑞替尼杂质Ceritinib 11个依美斯汀杂质Emedastine8个依匹唑派杂质Brexpiprazole6个依帕司他杂质epalrestat6个乌苯美司杂质Ubenimex 19个福多司坦杂质Fudosteine 6个马来酸匹杉琼杂质Maleic acid Chinese fir, Joan 6个扎鲁司特杂质Zafirlukast 6个贝利司他杂质belinostat 6个奥扎格雷的杂质ozagrel 6个酒石酸伐尼克兰片杂质Varenicline Tartrate Tablets 6个莫扎伐普坦杂质Mozavaptan 5个沙芬酰胺杂质Safinamide 4个沃雷生杂质suvorexant 5个依替巴肽杂质Eptifibatide 5个乐伐替尼杂质lenvatinib 8个。
非小细胞肺癌有望迎来新疗法Lorbrena,死亡风险降72%

近日,美国FDA宣布接受第三代ALK抑制剂劳拉替尼(Lorlatinib,商品名Lorbrena)的补充新药申请(sNDA),用于一线治疗ALK阳性转移性非小细胞肺癌(NSCLC)患者。
同时,FDA还授予其优先审查资格,预计今年4月做出答复。
▌拥有“钻石靶点”的肺癌肺癌是全球癌症死亡的主要病因之一,每年有180万人确诊肺癌。
非小细胞肺癌(NSCLC)是最常见的肺癌类型,约占所有肺癌的85%。
其中,约3%~5%的NSCLC患者会出现间变性淋巴瘤激酶(ALK)重排。
ALK基因重排多发生在年轻患者和不吸烟或少量吸烟人群中,而且绝大多数表现为肺腺癌。
ALK突变可以说是肺癌中的“钻石突变”,其靶向药物的有效率远远高于EGFR突变的患者。
截至目前,针对ALK突变的靶向药物有五种。
第一代:克唑替尼;第二代:色瑞替尼、阿来替尼、布加替尼;第三代:劳拉替尼。
这些药物大大提高了这类肺癌患者人群的生存率。
▌第三代ALK抑制剂:劳拉替尼劳拉替尼是第三代ALK抑制剂,对目前已知的几乎所有ALK耐药突变均有效,具有较强的血脑屏障穿透能力,可用于治疗脑转移。
高达40%的ALK阳性肺癌患者出现脑转移。
2018年11月,劳拉替尼获批二线治疗ALK阳性转移性NSCLC患者。
作为全新一代的ALK抑制剂,劳拉替尼的优势在于可以针对不同类型的ALK+患者,有效率最高;而且,对于三种ALK抑制剂都耐药的患者,也有很好的疗效。
▌死亡风险降低72%!临床试验数据喜人这一sNDA是来自关键的3期CROWN临床试验的结果。
CROWN是一项全球、随机、3期临床试验,旨在评估劳拉替尼和第一代ALK抑制剂克唑替尼(Crizotinib)在ALK+ NSCLC患者中的疗效和安全性。
研究入组296例初治晚期ALK阳性NSCLC患者,按1:1的比例随机分配,其中约1/4的患者(26.4%)在基线时已经发生脑转移。
去年11月发表在《新英格兰医学杂志》的研究结果显示:1、与现有一线标准疗法克唑替尼相比,劳拉替尼将疾病进展或死亡风险降低72%。
肺腺癌常见的靶向药物

肺腺癌常见的靶向药物肺癌的靶向治疗和以前的化疗是完全不同的,所谓的靶向治疗主要是针对肿瘤特异性的发病机制或者是信号传导通路。
下面店铺和大家一起学习肺腺癌常见的靶向药物。
肺腺癌常见的靶向药物EGFR基因突变在肺腺癌里频率较高,非亚裔的频率是10-20%,而亚裔非吸烟患者的频率在40%左右,也有文献统计说50%,这也是为何很多患者盲试易瑞沙和特罗凯也有效的原因,频率几乎一半。
EGFR基因在鳞状细胞癌里偶尔出现,没有特别高的频率,因此鳞癌患者谨慎盲试EGFR靶点的靶向药物,最好做基因检测确定突变情况。
EGFR基因90%以上的突变发生在19号外显子缺失和21号外显子的L858R。
这两种突变位点适用于第一代EGFR靶向药物吉非替尼、厄洛替尼、埃克替尼。
19外显子缺失和L858R突变之外的称之为罕见突变,如L861Q,G719X,S768I等,这些突变位点适合使用第二代靶向药物阿法替尼,即不可逆的EGFR和HER2双重抑制剂。
虽然有临床研究表明,阿法替尼相比吉非替尼可改善PFS和客观响应率,但是副作用较大,目前阿法替尼优势还是在EGFR的罕见突变位点,或Her2突变导致的耐药。
一般而言靶向药物总是存在耐药的问题,一代EGFR靶点药物耐药的主要原因是EGFR基因的二次突变,即产生了T790M突变,频率为50-65%,存在T790M突变的患者适用的靶向药物是奥希替尼(AZD9291),临床阶段的靶向药物还有Rociletinib(CO-1686)。
当然奥希替尼也会耐药,耐药的原因可能是EGFR基因的C797S突变,或者Her2,或者c-MET扩增等。
C797S突变如果和T790M突变在同一条染色体则称为顺势构型,目前没有靶向药物,如果C797S和T790M在不同的染色体上,即反式构型,则可以使用一代和三代靶向药物联合来治疗。
存在脑转移的EGFR患者,现有的研究表明如果可以使用靶向药物控制就不进行放疗,全脑放疗仅有一次机会。
色瑞替尼

色瑞替尼
使用指导
香港特区肿瘤中心专家指出,服用色瑞替尼,每天1次,750mg(5片)。
空腹口服,口
服直至疾病进展或不可耐受。
与克唑替尼一样,服药期间不能饮用葡萄汁和柚子汁。
服用
色瑞替尼还应注意以下事项。
1、严重和持续胃肠道毒性:38%患者由于发生腹泻恶心呕吐或腹痛需要调整剂量。
如
止吐药或止泻药无反应,应减低剂量。
2、肝毒性:Zykadia或有肝毒性,至少每月检查肝功。
出现肝损伤时考虑暂停、减低
剂量或永久终止Zykadia治疗。
3、间质性肺疾病(ILD)/肺炎:4%患者发生,诊断有治疗相关ILD/肺炎应永久终止Zykadia治疗。
4、QT间期延长:Zykadia可能导致QTc间期延长。
要监视患者的心电图和电解质情况。
若患者有充血性心衰,缓慢性心律失常,电解质异常,或患者正在使用已知延长QTc间期
药物的话,则不给药或减低剂量,或永久终止Zykadia治疗。
5、高血糖:Zykadia或致高血糖。
监视血糖水平,并服用抗高血糖药物。
如果无法控
制血糖,考虑不给药或降低剂量,或永久终止Zykadia治疗。
6、心动过缓:Zykadia或致心动过缓,定期监视心率和血压,若无法控制,则不给药
或降低剂量,或永久终止Zykadia治疗。
7、胚胎胎儿毒性:Zykadia可能危害胎儿,告知女性服药期间做好避孕措施。
[1]
参考资料
1.李力人、赵宗杰《香港肿瘤新特药物汇编(简体版)》,香港:香港医学科学院出
版社,2016.7。
ALK详解——精选推荐

ALK详解写在前⾯的话:本⼈私下是⼀枚⼩⼩技术员,闲来⽆事开了这样⼀个公众号,刚开始写⼀些简单易懂的东西,很感谢我的朋友和同事的⿎励与⽀持,这是我坚持下去的动⼒。
ALK基因ALK最早是在间变性⼤细胞淋巴瘤(ALCL)的⼀个亚型中被发现的,因此定名为间变性淋巴瘤激酶(anaplasticlymphoma kinase,ALK)。
它是继EGFR之后肺癌中⼜⼀很重要的驱动基因。
ALK 可与多种基因发⽣融合,融合的发⽣激活了与细胞存活和增殖相关的信号转导通路,进⽽引起肿瘤的发⽣。
EML4-ALK 融合基因阳性的NSCLC患者已经被定义为 NSCLC的⼀种特殊亚型,主要出现在不吸烟或少吸烟的肺腺癌患者。
ALK 也与其他基因融合⽽实现活化,如与 PTPN3、TFG、KIF5B、KLC1、STRN、TPR 及 HIP1 基因等。
与EGFR突变⼈群相⽐,ALK融合⼈群年龄更轻,如下图。
也就是说,ALK这类疾病与EGFR这类疾病⽆论是从驱动基因、病因还是从临床病理特征和预后来说都是不⼀样的,这也从另外⼀个⾓度说明对于患者光检测EGFR是远远不够的,ALK也是⾼频⽽且特异的分⼦亚型。
西⽅ NSCLC 患者 ALK 融合基因阳性率约为 3-7%,中国NSCLC 患者阳性率约为 3-11%,⽽在EGFR、KRAS、⼈表⽪⽣长因⼦受体2 或 TP53 等基因⽆突变的 NSCLC 患者中,ALK融合基因阳性率达25%;我国 EGFR 和 KRAS均为野⽣型的腺癌患者,ALK 融合基因的阳性率⾼达30-42% 。
ALK基因抑制剂⽬前,在ALK突变阳性的⾮⼩细胞肺癌(ALK+NSCLC)领域已经有4个同类型药物被FDA批准上市。
克唑替尼(Crizotinib)是⼀种以ALK、ROS1和c-MET酪氨酸激酶为作⽤靶点的⼝服⼩分⼦抑制剂,由美国辉瑞公司研发,2011年8⽉26⽇获FDA批准上市,2016年3⽉10⽇获CFDA批准上市,商品名为赛可瑞(Xalkori)。
ROS1融合基因突变在非小细胞肺癌诊断与治疗中的研究进展_江薇
Role of ROS1fusion gene mutations in diagnosis and treatment of non-small cell lungcancerWei Jiang,Yina WangCorrespondence to:Yina Wang;E-mail:1503099@Department of Oncology,The First Affiliated Hospital,College of Medicine,Zhejiang University,Hangzhou 310000,China This work was supported by the Natural Science Foundation of Zhejiang Province (No.LY16H160006)AbstractThe incidence of ROS1gene rearrangement/fusion in non-small cell lung cancer (NSCLC)is about 1%-2%.The advent of tar-geted drugs for ROS1gene fusion has significantly improved the quality of life and total survival of NSCLC patients with ROS1fusion;however,acquired drug resistance is still present in most patients after continuous treatment.This review has summarized the back-ground of the ROS1fusion gene,detection method,clinical efficacy of ROS1-targeted therapy,and strategy and prospect of drug resis-tance.Keywords:ROS1gene,non-small cell lung cancer (NSCLC),crizotinib,drug resistanceROS1融合基因突变在非小细胞肺癌诊断与治疗中的研究进展*江薇综述王懿娜审校摘要ROS1基因重排/融合在非小细胞肺癌(non-small cell lung cancer ,NSCLC )中的发生率约为1%~2%。
2023常用化疗药物及分子靶向药物分类

2023常用化疗药物及分子靶向药物分类通常可将化疗药物分为几类,其中烷化剂和抗代谢药以该类药物细胞毒作用命名,激素类药物以其生理作用命名,天然药物的命名说明了其药物来源。
生物调节剂类药物包括可以模仿、刺激、促进、抑制甚至改变机体对肿瘤反应的药物。
分子靶向药物作用于肿瘤细胞或其微环境中的变异。
无法分入其他种类的药物被分为杂类。
每一类药物能按药物作用机制、药物或衍生物的生化结构、生理学作用机制分为几种亚类型。
常用化疗药物及分子靶向药物分类药物名称烷化剂类烷基磺酸盐白消安氯丙咤衍生物塞替派(三乙烯硫代磷酰胺)金属盐类K销、顺销、草酸销氨芥类基达莫司汀、环磷酰胺、雌英司汀、异环嶙酰胺、氨芥、美法仑亚硝(基)麻类k莫司汀、洛英司汀、链麻毒家三氯哩味哩甲酰胺类抗代谢类达卡巴嗪、替英理胺叶酸拮抗剂甲氨媒吟、培美曲塞、普拉曲沙嚓吟类克拉屈滨、械达为滨、航嗦吟.奈拉滨、喷司他r、硫鸟嗦吟啼蜿笑阿扎胞仔、卡培他演、阿裾胞件、地西他演、天然类^尿嚅噬脱辄核甘、氟尿喀咤、吉西他滨、曲版尿首电合片抗生家类博来而我、放线荫求、柔灯得家、多柔比星、表柔比星、去甲躯基柔红毒素、丝裂霉素、米托悉:酿、戊柔比星酶类天冬酰核酶.梭肽酶激管聚体稳定剂长巴他赛,多西他赛、紫杉醉有丝分裂抑制剂甲磺酸艾H布林、伊沙匹隆、长春敢、长春新碱、长春地辛、长春瑞滨然甲睾BH 及其他 比卡管胺、思杂自胺、案:他胺、尼鲁米特晒酸阿比特龙 瓦鲁米待、阿那曲眸、来的理、依西夫坦 地塞米松、泼花松 Ci 烯雌瓯 地加瑞克 戈舍瑞林、亮丙瑞林、曲普通林 奥的肽 除酸甲地孕酮.储值甲羟牛OH 氟维司群、雷洛普芬、他英甘芬、托瑞米:芬 奥曲肽 甲状腺素、左甲状腺素 阿柏西普 夫拉平度 类维生素A 、磺碘唾、罗米地辛 维莫德吉索尼德吉 贝利司他帕比司他 地尼白介索 曲妥珠单抗-美坦新偶联物、阿仑单抗、博纳吐单抗、色瑞替尼、西妥昔单抗、达番木单抗、地诺单抗、埃罗妥珠单抗、吉妥单抗、替伊莫单抗、阿托珠单抗、奥法木单抗、帕尼单抗、帕妥珠单抗、帕纳单抗、雷英芦单抗、利妥昔单抗、司妥昔单抗、硼替佐米、曲妥珠单抗.碘-131托西莫单抗 依维莫司、西罗莫司脂化物 奥拉帕尼 高三尖杉葡就 硼替佐米、卡非佐米、伊沙佐米 阿法替尼、阿西替尼、伯舒替尼、卡博替尼、色瑞替尼、考比替尼、克嗖替尼、达拉非尼、达沙替尼、厄洛替尼、吉非替尼、依布替尼、史代拉利司、甲避或伊马卷尼、U 旧:;k 仑伐替尼、曲美替尼、米晚妥林、耐昔妥珠单抗、奥西替尼、帕博西尼、帕理帕尼、瑞戈非尼、鲁索替尼、司马沙尼、索拉非尼、舒尼替尼、曲关科尼、凡傅他尼、成罗萨尼 维A 酸(ATRA ) 伊兀单抗、纳武单抗、帕博利珠单抗 α干扰家-2a 、a 干扰素-2b 重组人白介索-2、地尼白介素、奥普瑞白介素促红细胞生成素、重组粒细胞集落刺激因子、人粒细胞H 噬细胞集落刺激因子激索和激素拮抗剂类雄淑康美雌激素受体拉抗剂雌激素合成抑制剂芳香酶抑制剂糖皮质激康雌激索类GnRH 受体拮抗剂1HRH 激动剂宓肽激家杼放抑制剂孕激家类选择性雌激素受体修饰剂及雌激康受体拈抗剂生长激素抑制剂甲状腺激家分子靶向药物血管生成配体结合体周期依赖激醒抑制剂基因表达洞节类Hedgehog 通路抑制剂组蛋白脱乙酰酶抑制剂白介素-2受体存素单克隆抗体及抗体-药物嵌合体mTOR 激酶抑制剂PARP1抑制剂蛋白合成抑制剂选白醒体抑制剂受体酪氨酸激酶抑制剂.多重激酶抑制剂,其他激酶抑制剂视黄酸受体表达修饰物生物调节剂免疫检测点抑制剂干扰家白介素骨髓和红细胞生长刺激因子非特异性免疫调节剂沙利度胺、泊马度胺、来那度胺疫苗(自体细胞免疫)Sipu1euce1-T杂类肾上腺皮质抑制剂米托坦双瞬酸盐类帕米瞬酸、哩来麟酸细胞保护剂(活性拮抗剂)氨磷汀、右雷佐生、美司钠丙卡巴肺衍生物丙卡巴肿(甲基茉腑)光敏性药物叶菲尔钠抗血小板药阿那格雷盐类三辄化抑三聚IR胺类似物六甲蜜胺腺类物羟基麻注:GnRH,促性腺激素释放激素;I1,白介素;1HRH,黄体生成素释放激素;mTOR,哺乳类动物西罗莫司靶蛋白;PARP1多腺吉二磷酸核糖聚合酶。
2014年上半年美国FDA批准药物简介

表 1 美国 FDA2014 年上半年批准新药一览表
批准日期 2014/01/08 2014/01/09 2014/01/10 2014/01/29 2014/01/31 2014/02/12 2014/02/14 2014/02/18 2014/02/24 2014/02/24 2014/03/03 2014/03/05 2014/03/11 2014/03/11 2014/03/14 2014/03/14 2014/03/18 2014/03/19 2014/03/21 2014/03/21 2014/03/28 2014/03/28 2014/03/31 2014/04/02 2014/04/03 2014/04/07 2014/04/07 2014/04/15 2014/04/16 2014/04/17 2014/04/21 2014/04/22 2014/04/28 2014/04/29 2014/05/08 2014/05/20 2014/05/23 2014/05/28 2014/06/06 2014/06/06 2014/06/06 2014/06/13 2014/06/20 2014/06/27 2014/06/27
通用名
批准类别
制药公司
适应证
达格列嗪(dapagliflozin)
新分子实体
BMS&AstraZeneca
2 型糖尿病
曲美替尼(trametinib)
新适应证 2,5
Glaxo SmithKline(GSK)
黑素瘤
达拉非尼(dabrafenib)
新适应证 2,5
GSK
黑素瘤
glatiramer acetate
[关键词] 新药批准;美国 FDA;新分子实体;新生物制品;化学结构;作用机制;适应证;不良反应
癌症探秘(下)

癌症探秘(下)作者:刘声远来源:《大自然探索》2015年第12期2011年,50岁的美国新罕布什尔州男子詹姆斯·拉格诺的病情很重,医生估计他只剩大约1年的寿命。
在他被确诊患有晚期肺癌后,哪怕是最强大的化疗和放疗都无法阻止他的肿瘤变大。
雪上加霜的是,他还被确诊患有甲状腺癌。
几个月后,他又被诊断患有脑癌。
于是,医生建议他考虑写遗嘱。
幸运的是,他的妻子力劝他接受了一次活检,结果发现了一种与肺癌有关的罕见基因变异。
他立即加入了一项临床试验。
该试验旨在测试一种相对新的癌症疗法——靶向疗法(也称靶向治疗)。
传统抗癌药物是不加区分的,也就是说,它们不仅攻击癌细胞,也攻击正常细胞。
而像拉格诺接受的一种分子靶向药物(此类药物如今已不再处于试验阶段,而是正在被越来越广泛地使用)那样,这类药物都旨在瞄准特定的癌突变。
事实上,许多癌症都与新型蛋白质有关。
这些蛋白质高度活跃,而且经常被激活,这样就刺激了癌瘤生长。
靶向药物正是旨在锁定这些新型蛋白质并关闭它们。
靶向治疗看来对拉格诺有效。
从2011年到2015年,他每天服用一种靶向药物——色瑞替尼两粒。
虽然他的癌瘤并未彻底消失,但癌瘤也没有再生长和扩散。
而拉格诺并不是靶向药物治疗有效的第一人。
2014年年初,美国食品和药物管理局(简称FDA)一次就批准了包括色瑞替尼在内的5种靶向药物。
现在,色瑞替尼被美国各大医院普遍用于治疗肺癌。
甚至在接受化疗和放疗之前,患者就首先接受靶向药物治疗。
由于基因测序已变得越来越简单和常见,每年辨识的肿瘤类型也越来越多,这让制药公司能以更高的精确度研发肿瘤药物。
因此,FDA削减了许多耗时长、费用高的药物试验,这促成靶向药物以比过去更快的速度用于普通患者。
对一些类型的癌症来说,靶向治疗已经开始取代化疗、放疗等癌症传统疗法。
在许多病例中,靶向药物不仅比传统疗法更有效,而且副作用更小。
大多数标准的化疗药物(也称化学药物)起作用,是通过杀死体内分裂过快的细胞。
靶向药物名词解释
靶向药物名词解释
靶向药物是指能够精准定位于身体内特定的病变部位的抗癌药物。
这些药物精准定位病变区域后,可以释放有效药物成分来杀伤病变区域的细胞。
目前临床上常用的靶向药物主要分为两大类,具体如下:
1.特异性治疗靶点的靶向治疗药物。
针对特异性治疗靶点的靶向治疗药物主要包括针对EGFR基因敏感突变的吉非替尼、厄洛替尼、奥希替尼等药物,针对奥克基因融合的克唑替尼、阿来替尼、色瑞替尼等药物,针对HER-2基因扩增的药物,如曲妥珠单抗、帕妥珠单抗等。
2.多种治疗靶点的多激酶抑制剂。
针对多种治疗靶点的多激酶抑制剂主要包括索拉非尼、舒尼替尼、培唑帕尼等。
ros1基因突变抗癌成功案例

ros1基因突变抗癌成功案例一、引言近年来,癌症的发病率持续上升,给人们的生活带来了极大的威胁。
在众多癌症类型中,肺癌、甲状腺癌和间质性肿瘤等尤为引人关注。
ROS1基因突变作为一种罕见的基因变异,正逐渐成为抗癌研究的新靶点。
本文将介绍ROS1基因突变的相关知识,以及几个ROS1基因突变抗癌成功案例。
二、ROS1基因突变概述1.ROS1基因功能ROS1(Receptor tyrosine kinase)基因是一种受体酪氨酸激酶,正常情况下,它对细胞生长、分化、迁移等具有调控作用。
然而,当ROS1基因发生突变时,可能导致细胞信号传导途径异常,从而促进肿瘤的发生。
2.ROS1基因突变与癌症关系ROS1基因突变主要与肺癌、甲状腺癌和间质性肿瘤等癌症类型密切相关。
研究发现,ROS1基因突变在这些癌症患者中的比例较高,且突变类型多样。
因此,针对ROS1基因突变的靶向治疗研究具有重要的临床意义。
三、ROS1基因突变抗癌成功案例介绍1.案例一:肺癌患者(1)病情简介患者男性,50岁,诊断为肺腺癌。
初步治疗采用手术、化疗和放疗,但病情反复发作。
(2)治疗过程及结果后患者接受ROS1基因突变检测,结果显示为阳性。
患者开始服用克唑替尼(Crizotinib)靶向治疗,病情得到有效控制,肿瘤缩小,生活质量得到改善。
2.案例二:甲状腺癌患者(1)病情简介患者女性,35岁,诊断为甲状腺乳头状癌。
术后病情恶化,出现转移。
(2)治疗过程及结果患者接受ROS1基因突变检测,结果显示为阳性。
随后患者使用色瑞替尼(Neratinib)进行靶向治疗,病情明显好转,转移病灶逐渐减小。
3.案例三:间质性肿瘤患者(1)病情简介患者男性,45岁,诊断为间质性肿瘤。
经过手术、化疗等治疗,效果不佳。
(2)治疗过程及结果患者进行ROS1基因突变检测,结果为阳性。
患者开始服用阿来替尼(Alectinib)进行靶向治疗,病情稳定,生活质量提高。
四、ROS1基因突变靶向治疗药物1.克唑替尼(Crizotinib)克唑替尼是一种针对ALK和ROS1基因突变的靶向药物,可通过抑制突变蛋白的活性,从而阻断肿瘤细胞的生长。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Ceritinib(Zykadia ®)Research code: LDK-3781 General Information● Ceritinib is a kinase inhibitor, which was first approved in2014 by US FDA.● Ceritinib was discovered and marketed by Novartis. ● Ceritinib inhibited autophosphorylation of ALK, ALK-me-diated phosphorylation of the downstream signaling protein STAT3, and proliferation of ALK-dependent cancer cells.● Indicated for the treatment of patients with anaplastic lym-phoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intol-erant to crizotinib.● Available as capsules with each containing 150 mg ofceritinib and recommended dose is 750 mg once daily until disease progression or unacceptable toxicity.Key Approvals around the World *First approvaldate 04/29/2014 06/05/2015 NDA NO. 205755 EMEA/H/C/003819Brand name Zykadia ® Zykadia ® Indication NSCLC NSCLCAuthorisation holderNovartisNovartis Europharm Ltd*Till Dec 2015, it has not been approved by PMDA (Japan) and CFDA (China).Worldwide SalesActive IngredientMolecular formula : C 28H 36N 5O 3ClS Molecular weight : 558.14 CAS No.: 1032900-25-6Chemical name : 5-Chloro-N 4-[2-[(1methylethyl)sul-fonyl]phenyl]-N 2-[5-methyl-2-(1-methylethoxy)-4-(4-pi-peridinyl)phenyl]-2,4-pyrimidinediamine Parameters of Lipinski's “Rule of 5”5583871144.70 ± 0.95aCalculated by ACD/Labs software V11.02.Drug Product *Dosage route : Oral Strength : 150 mg Dosage form : CapsuleInactive ingredient : Colloidal anhydrous silica, L-hydroxy-propylcellulose, magnesium stearate, microcrystalline cel-lulose, and sodium starch glycolate, gelatin, indiogotine, and titanium dioxide Recommended dose :The recommended starting dose is 750 mg once daily with-out food.Discontinue ceritinib for patients unable to tolerate 300 mg daily.If a dose of ceritinib is missed, make up that dose unless the next dose is due within 12 h.*Sourced from the FDA drug label information.2 ▐2014 Worldwide NCEsKey PatentsPatents Summary•Ceritinib’s compound patent application was filed as PCT application by IRM in 2007.•The compound patent will be expired in 2027 originally, which has been granted in Japan, Europe, the United States successively.•Zykadia® (Ceritinib) has got five years NCE market exclusivity protection and seven years ODE after it was approved by FDA in Apr. 29, 2014 initially.Patents ListCeritinib ▐ 32 ChemistryRoute 1: Original Discovery RouteSynthetic Route: The overall synthetic route of ceritinib was enabled via a modified Buchwald-Hartwig coupling of two advanced intermediates aryl amino-piperidine 6 and arylsulfonyl chloro-pyrimidine 7. Aryl amino-piperidine 6 was synthesized in five stepsfrom 2-chloro-4-fluorotoluene 1. Nitration of 1 using KNO3/H2SO4 yielded the corresponding nitro derivative 2 in a 71% yield. Condensation of compound 2 with iso propanol in the presence of Cs2CO3 provided the 2-chloro-4-iso propoxy-5-nitrotol-uene 3 in excellent yield. Suzuki coupling of compound 3 with 4-pyridineboronic acid 4 provided compound 5 in 73% yield. Concomitant reduction of pyridine and nitro group using PtO2/H2 afforded the corresponding piperidine-aniline intermediate, which was subsequently protected with Boc, generating compound 6 in 60% over two steps. Buchwald-Hartwig coupling of 6 with arylsulfonyl chloro-pyrimidine 7 provided the precursor of ceritinib. Boc deprotection with TFA, concentration, and subse-quent precipitation with 1 N HCl yielded ceritinib as the HCl salt in 35.0% yield from 6 and the overall yield of 10.3%.[1, 2] Synthesis of the required arylsulfonyl chloro-pyrimidine coupling precursor 7 began with 2-(isopropylsulfonyl)benzenamine 8 and 2,4,5-trichloropyrimidine 9 under basic condition (NaH, DMF, DMSO)in 60% yield.4 ▐2014 Worldwide NCEsRoute 2:Synthetic Route: In this strategy, ceritinib was prepared from reduction of 4-(5-isopropoxy-2-methyl-4-nitrophenyl)pyridine 1 under Pd/C H2 condition afforded corresponding phenylamine 2 in 92% yield. Then Sandmeyer reaction was carried out in the presence of NaNO2/CuBr/HBr/H2O to give 4-(4-bromo-5-isopropoxy-2-methylphenyl)piperidine 3 in 83% yield. Buckward-Hartwig coupling of 3 with 5-chloro-4-nitropyrimidin-2-amine 4 converted to desired compound 5 in 78% yield, which was hy-drogenated and coupled with 1-bromo-2-(isopropylsulfonyl)benzene 7 to obtain the target ceritinib in 74% yield over two steps. The overall yield was 44%.[3]3 PharmacologySummaryMechanism of Action●Ceritinib is a kinase inhibitor, which inhibited ALK, insulin-likegrowth factor 1 receptor (IGF-1R), insulin receptor (InsR), andROS1.●Ceritinib was approximately 50-fold more specific for ALK(IC50 = 0.15 nM) than InsR (IC50 = 7 nM) and IGF-1R (IC50 = 8nM), other members of theinsulin receptor superfamily.●Ceritinib inhibited autophosphorylation of ALK, ALK-mediatedphosphorylation of the downstream signaling protein STAT3,and proliferation of ALK-dependent cancer cells.●The off-target activity of ceritinib was evaluated for 42 of thetarget receptors (MC4, IC50 = 0.6 nM), 84 of the broad spectrumscreen receptors (transporter monoamine, inhibition = 97%), and10 of the GPCRs (dopamine 2 receptor, IC50 = 4000 nM).Ceritinib ▐ 5 In Vitro Efficacy●Anti-proliferative activity of ceritinib in tumor cell lines:Cell lines expressed with ALK fusion protein: IC50 = 11-56 nM.Cell lines expressed with EML4-ALK-mutation: IC50 = 37.6-250 nM.Ba/F3 cells expressed with others fusion proteins: IC50 = 180-400 nM.●Phosphorylation of ceritinib in Karpas299 cells:ALK protein: IC50 = 46 nM.STAT3 protein: IC50 = 150 nM.In Vivo Efficacy●H2228 cells xenograft models:In SCID mice: Significance at doses ≥6.25 mg/kg. Complete tumor regression with 25 mg/kg ceritinib after 14 days.In nude rats: Significance at doses ≥10 mg/kg.●Karpas299 cells xenograft models:In SCID mice: Significance at doses ≥12.5 mg/kg. Complete tumor regression with 25 mg/kg ceritinib after 14 days.In nude rats: Significance at doses ≥12.5 mg/kg. Complete tumor regression with 25 mg/kg ceritinib after 14 days.●Crizotinib-resistant H2228 cells xenograft model carrying the ALK-mutation in SCID mice:Non-ALK-mutation: Significant at doses ≥50 mg/kg.I1171T ALK-mutation: Significant at doses ≥25 mg/kg.C1156Y ALK-mutation: Significant at doses ≥50 mg/kg.Mechanism of ActionTable 1In Vitro Effects of Ceritinib and Crizotinib on Human Protein Kinases[4]EPK CE ALK (1066-1459) Y a0.15 3 EPK CE AXL Y 180 13EPK CE IGF-1R (980-1369) Y 8 400 EPK CE RET (658-1072) Y 400 2200 EPK CE INSR (871-1343) Y 7 290 EPK ROCK2 S/T 450 2500EPK AURORA_A S/T b110 600 EPK CE FGFR3(411-K650E-806) Y 430 1700EPK cABLT315 Y 130 6The applicant evaluated the selectivity of ceritinib and crizotinib by testing its in vitro activity against 36 recombinant human protein kinases using the Caliper mobility shift assay, table 1 showed ceritinib most selective for ALK (IC50 <0.5 μM). a Y: Tyrosine-specific protein kinases. b S/T: Serine/Threonine-specific protein kinases.[4]H2 receptor 170 NAmonoamineRabbit 10 μM 97 331Opk receptor 570 NA K channel[Ka] Rat 10 μM 99 682MC3 receptor 670 NA Somatostatin sst1 Human 10 μM 88 2420MC4 receptor 600 35% at 10 μM Somatostatin sst2 Human 10 μM 76 2250Ad3 receptor 730 8300 Somatostatin sst3 Human 10 μM 93 5120NK1 receptor 990 79% at 30 μM Somatostatin sst4 Human 10 μM 90 1880D2 receptor 1200 NA 5-HT5A Human 10 μM 71 5000The off-target activity of ceritinib was evaluated using an in vitro safety pharmacology profiling panel including 139 G protein-coupled receptors (GPCRs), ion channels, nuclear receptors, transporters, and enzymes that have been previously linked to potential side effects. At least eight concentrations of ceritinib were tested. The agonist and antagonist activities of ceritinib were evaluated for 10 GPCRs using a safety pharmacology screen. A fluorometric imaging plate reader (FLIPR) assay was conducted with a four-fold, eight-point serial dilution of ceritinib up to 10 μM to a ssess agonist and antagonist activity. Ceritinib showed weak agonist activity on the dopamine D2 receptor (EC50 = 6 μM, IC50 = 4 μM), but did not exhibit significant activity against the other GPCRs tested. a Ceritinib interacted with 42 of the target receptors, table 2 showed the target receptors IC50 <1500 nM. b A safety pharmacology broad spectrum screen with 84 receptors at ceritinib was tested at 10 μM in duplicate, table 2 showed the broad spectrum receptors inhibited >70%.6 ▐2014 Worldwide NCEsIn Vitro EfficacyTable 3 In Vitro Anti-proliferative and Phosphorylation of Ceritinib[4]Anti-proliferative activityBa/F3Murinepro-B lymphoma cell withALK fusion kinaseNPM-ALK 26-35NATEL-ALK-Q1 56EML4-ALK 27 Ba/F3Murinepro-B lymphoma cell withALK-mutationEML4-ALK I1171T 37.6 440EML4-ALK L1196M 69 1460EML4-ALK G1202R 94 1370EML4-ALK C1156 160 340EML4-ALK S1206A 160 270EML4-ALK G1269S 250 2140 Ba/F3Murinepro-B lymphoma cell withtyrosine kinaseTEL-ROS 180NATEL-IGF-1R 220TEL-InsR 400Karpas299 Human ALCL NPM-ALK 45 (n = 8)NA NCI-H2228 Human NSCLC EML4-ALK 11 (n = 5) NB-1 Human neuroblastoma cell ALK 24 (n = 3)Endogenous phosphorylation Karpas299 Human ALCLALK protein 46NASTAT3 protein 150The cell viability following 48 h of treatment with control compounds or ceritinib serially diluted with DMSO was determined using the Bright-Glo™ luciferase biolumi-nescent assay and cell proliferation was measured using the Brite Lite™ luciferase assay. ALCL: Anaplastic large-cell lymphoma. NSCLC: Non-small cell lung cancer. NA: Not available.In Vivo EfficacyTable 4 In Vivo Efficacy of Ceritinib in Different Xenograft Models[4]H2228 HumanNSCLCSCIDmouse(female)Wild type3.125 QD × 14416.25Complete tumor regressionwas observed even at adose of 25 mg/kg/day af-ter 14 days.6.25 QD × 143612.5 QD × 14-6425 QD × 14-100RNU nuderat(female)Wild type5 QD × 146710Complete tumor regressionwas observed even at adose of 25 mg/kg/day af-ter 14 days.10 QD × 14 225 QD × 14-100Ceritinib ▐ 7ContinuedC1156Y ALK-mu-tation25 QD × 12 61.8 50 Complete tumor regres-sion was observed even at a dose of 100 mg/kg/day.50 QD × 12 11.7 100 QD × 12 -100 Karpas299Human ALCLSCID mouse (female)Wild type6.25QD ×14 62 12.5 Complete tumor regres-sion was observed at 25 mg/kg after 14 mg/kg/day.12.5 QD × 14 18 25 QD × 14 -93 RNU nuderat (female)Wild type6.25QD × 14 74 12.5Significant tumor regres-sion was observed at 25 mg/kg/day after 14 days.12.5QD × 143025 QD × 14 -33 50QD × 14-66Study: H2228 NSCLC xenograft mice model Animal: SCID beige mice (female)Model: 5 × 106 NCI-H2228 cells were implanted subcutaneously into the right hind flank of one SCID mouse.Administration: Treated daily, p.o., ceritinib: 3.125, 6.25, 12.5 and 25 mg/kg/day, ve-hicle control: NAStarting treatment: Mice bearing established tumors (~85 mm 3) Test: Tumor volumes, 3 times a weekResult: Treatment with 25 mg/kg ceritinib resulted in complete tumor regression after 14 days. ** P <0.05.Figure A Effect of Ceritinib on Human H2228 NSCLC Xenografts in SCID Mice Model [4]8 ▐2014 Worldwide NCEsStudy: Crizotinib-resistant H2228 cells xenograft with ALK I1171T mutations micemodelAnimal: SCID beige mice (female)Model: Crizotinib-resistant H2228 NSCLC with ALK I1171T mutations were im-planted subcutaneously into one SCID mouse.Administration: Treated daily, p.o., ceritinib: 12.5, 25, or 50 mg/kg/day, crizotinib100 mg/kg/day, vehicle control: NAStarting treatment: Mice bearing established tumors (~130 mm3)Test: Tumor volumes, 3 times a weekResult: Treatment with 50 mg/kg ceritinib resulted in complete tumor regression after14 days of treatment. (**P≤0.05; ****P≤0.0001)Figure B Effect of Ceritinib on Crizotinib-resistant Human H2228 NSCLC Xenograft with ALK I1171TMutations in SCID Mice Model[4]Study: Karpas299 ACLC xenograft mice modelAnimal: SCID beige mice (female)Model: 5 × 106 Karpas299 cells were implanted subcutaneously into the right hindflank of one SCID mouse.Administration: Treated daily, p.o., ceritinib: 6.25, 12.5 and 25 mg/kg/day, vehiclecontrol: NAStarting treatment: Mice bearing established tumors (~74 mm3)Test: Tumor volumes, 3 times a weekResult: Treatment with 25 mg/kg ceritinib resulted in c significant tumor regressionafter 14 days of treatmentFigure C Effect of Ceritinib on Human Karpas299 ALCL Xenografts in SCID Mice Model[4]4 ADME & Drug-Drug InteractionSummaryAbsorption of Ceritinib●Exhibited a non-linear pharmacokinetics in humans after oral administration. The increase in AUC appeared to be greaterthan dose-proportional in the dose range of 50 to 750 mg ceritinib.●Had a moderate bioavailability in rats (48.3%), but high in mice (54.6%) and dogs (58%).●Was observed slowly (T max = 3.98-15 h) in humans, mice (7 h), rats (12 h) and monkeys (13-18.3 h).●Showed a half-life of 19.4-40.6 h in humans, much longer than those in rats (13.2 h) and monkeys (12.1-16 h), after oral ad-ministration.●Had a moderate clearance in mice (26.6 mL/min/kg), rats (1.49 L/h/kg), but low to moderate in monkeys (0.366-0.78 L/h/kg),after intravenous administration. The Cl/F in humans was 44.5-126 L/h after oral administration.●Exhibited an extensive distribution in mice, rats and dogs, with the apparent volume of distribution at 9.7, 19.9 and 6.53-13.5L/kg, after intravenous administration. The V z/F in humans was 1880-6230 L after oral administration.●Ceritinib was classified as a low passive permeability compound.Distribution of Ceritinib●Exhibited high plasma protein binding in rats (97.9-98.4%), dogs (98.3-98.4%), monkeys (94.4-97.4%) and humans (96.7-98.8%). Note that ceritinib was mainly bound to HSA.●The binding to RBC was 56.9-58.6% in humans, indicating the drug was distributed more to blood cells than to plasma.●In Long Evens rats after oral and intravenous administration:Ceritinib ▐ 9 The drug was widely distributed into most tissues including central nervous system although with a lower degree com-pared to other tissues.Relatively higher concentration levels were observed in intestinal wall, uveal tract, pituitary gland, bile, adrenal cortex, harderian gland, liver, spleen, lymph node, lungs, kidneys, thyroid, bone marrow, adrenal medulla, pancreas, thymus and salivary gland. The concentration in tissues was generally higher than blood concentration.The radioactivity concentration in the uveal tract was 176 times of that in blood, suggesting a high affinity for melanin-rich tissues.Ceritinib-derived radioactivity was retained in several other tissues (including testis, epididymis, and skin) and the elimi-nation was not yet complete by 168 hours post-dose.Metabolism of Ceritinib●Could slightly metabolized in rat, monkey and human hepatocytes.●CYP3A was the major metabolizing enzymes, with CYP2C19, 1A2, 2C8, 2D6 and 2C9 involved in the metabolism ofceritinib.●The metabolism of ceritinib included mono-oxygenation, O-dealkylation, S-dealkylation, and N-formylation of ceritinib, andsecondary di-oxygenation, glucuronidation, sulfation and dehydrogenation.●Overall, the parent drug was the most abundant component in plasma in humans. Eleven metabolites were found in theplasma of humans, each at levels ≤ 2.3% of the total drug-related AUC.●Five of these eleven metabolites were not detected in the plasma of either the rat or monkey. The remaining three uniquehuman metabolites detected at low levels in plasma included M46.6 (1.7%), M48.8 (1.7%), and M52.0 (2%).Excretion of Ceritinib●Was predominantly eliminated in feces in rats, monkeys and humans, with the parent drug as the significant component in rat,monkey and human feces.●In cannulated rats, excretion was mainly into the bile 65.4% after oral administration and 24.3% after intravenous administra-tion.Drug-Drug Interaction●Ceritinib was a strong inhibitor of CYP3A4/5 (IC50= 0.2 μM), and moderate of CYP2A6 (IC50= 5 μM), CYP2B6 (IC50 = 2μM), CYP2C8 (IC50= 25 μM), CYP2C9 (IC50= 2 μM), CYP2C19 (IC50= 70 μM), CYP2D6 (IC50 = 20 μM) and CYP2E1 (IC50= 30 μM).●Ceritinib had no induction for CYP1A2, CYP2B6 or CYP3A4 mRNA/activities, but had induction for CYP2C9 in vitro at theconcentration of 0.25-2.5 μM ceritinib.●Ceritinib was a substrate of P-gp and BCRP in vitro, but not inhibitors of them.●Ceritinib was not a substrate of OCT1, OAT2, OATP1B1 or OATP2B1.●Ceritinib inhibited OATP1B1 or OATP1B3, OAT1 and OCT2, with the IC50 of >5 μM in vitro, but did not inhibit OAT3 orOCT1.AbsorptionTable 5 In Vivo Pharmacokinetic Parameters of Ceritinib in Mice, Rats and Monkeys after a Single Dose Administration[4]Balb/c mouse (male) i.v. 5 -nM nM·h nM·h a6.2 ± 0.5mL/min/kg9.7 ± 0.6 - p.o. 20 7.0 ± 0695 ± 31nM12296 ± 981nM·h10334 ± 963nM·h a- - - 54.6 ± 4.4HanWistar rat (male) i.v. 10 0.083 ± 0 975 ± 139 6950 ± 1470 6890 ± 1510 9.7 ± 1.2 1.49 ± 0.342 19.9 ± 0.49 - p.o. 25 12.0 363 8390 8330 13.2 NA NA 48.3Cynomolgus monkey (male) i.v. 5 0.083 1410 6530 6450 29 0.78 13.5 -i.v. 10 0.083 3190 27800 27400 14.5 0.366 6.53 -p.o. 30 18.3 ± 9.81 881 ± 12.5 35800 ± 3460 35500 ± 3520 12.1 ± 2.05 - - 43.0 ± 4.17 p.o. 60 13 ± 9.2 947 ± 140 45300 ± 8860 45100 ± 8840 16 ± 0.61 - - 58a AUC0-24.10 ▐2014 Worldwide NCEsTable 6 In Vivo Pharmacokinetic Parameters of Ceritinib in Patients Following a Single Doses of Ceritinib on[5]50n = 1 n = 1 n = 1 n = 1 n = 1 n = 1 n = 1100 19.4n = 115.0(6.00-24.0)n = 229.3(10.1)n = 2467(10.7)n = 2938(24.3)n = 23250n = 1116n = 1200 33.2n = 15.08(4.17-6.00)n = 240.2(88.5)n = 2703(55.6)n = 21460(62.9)n = 23720n = 177.5n = 130030.1(10.0)n = 34.00(4.00-5.95)n = 3198(41.5)n = 33440(44.7)n = 37470(46.5)n = 31880(50.7)n = 244.5(36.8)n = 240030.7(39.1)n = 104.99(2.97-6.73)n = 12120(80.9)n = 121920(78)n = 124070(81.8)n = 123470(74.4)n = 595.9(58.6)n = 550031.1(11.1)n = 73.98(3.00-23.5)n = 8153(86.5)n = 82350(87.9)n = 85140(142)n = 86230(219)n = 3147(170)n = 360037.6(24.6)n = 66.00(3.00-24.1)n = 9212(59.7)n = 93590(53.4)n = 98180(57.4)n = 91990(4.30)n = 246.39.60)n = 270038.9(98.4)n = 36.00(4.00-25.0)n = 4206(146)n = 43450(138)n = 49210(112)n = 42340(56.5)n = 266.6(35.8)n = 275040.6(34.7)n = 96.02(3.95-23.8)n = 10186(127)n = 103390(121)n = 107870(127)n = 104230(164)n = 388.5(163)n = 3n: Number of patients with non-missing values. Values were median (range) for T max, geometric mean (CV% of geometric mean) for all others.Key finding:Ceritinib was classified as a low passive permeability compound.DistributionTable 7 In Vitro Plasma Protein Binding and Blood Partitioning of [14C]Ceritinib[5]Rat 97.9 ± 2 98.4 ± 0 98.4 ± 0.1 100 97.6 ± 0.6 Rat0.4 3.7 1.3Dog 98.8 ± 0.5 98.3 ± 2.1 98.4 ± 0.810000 98.6 ± 0.8 Dog66.6 ±1.667.0 ±0.471.6 ±1.1Monkey 94.4 ± 0.5 97.4 ± 0.4 95.2 ± 0.2 Monkey 78.7 ±1.177.8 ±1.576.4 ±0.4Human 98.8 ± 0.5 97.2 ± 1.4 96.7 ± 1.8 Human 58.2 ±3.558.6 ±5.556.9 ±4.8[4] FDA Datadase. /drugsatfda_docs/nda/2014/205755Orig1s000PharmR.pdf (accessed Nov 2015).14[4]Blood 63.4 600 220 48.0 NM NM 1.00 1420 1 Brain 29.8 42.0 20.0 13.0 NM NM 0.148 137 0.096 Bile NM 74000 29000 11000 NM NM 155 48800 34.4 Lungs 607 18000 5900 2100 28.9 21.2 37.2 23300 16.4 Liver 2720 33000 8100 1800 78.7 130 52.6 29500 20.8 Kidney cortex 693 17000 6400 1300 20.3 28.3 32.8 23700 16.7 Stomach glandular 13400 5200 1900 310 NM NM 26.3 6590 4.64 Adrenal cortex 1870 37000 11000 4100 41.4 NM 72.4 48700 34.4 Harderian gland 31.5 1700 1800 2600 1060 2990 62.8 5040 3.55 Bone marrow 198 **** **** 2700 23.3 NM 28.0 9220 6.50 Small intestine wall 164000 490000 11000 730 NM NM 413 6980 4.92 Thyroid gland 843 18000 7300 1200 NM NM 30.3 35100 24.7 Pituitary gland 229 14000 6600 15000 1810 2590 211 15000 10.6 Spleen 1040 27000 6400 2500 42.3 41.6 47.6 NA NA Lymph node 200 19000 2900 4100 183.0 NM 45.1 8720 6.14 Adrenal medulla 890 21000 2100 1300 48.1 NM 26.5 14600 10.3 Pancreas 388 13000 4000 1300 6.6 NM 24.6 14200 9.98 Thymus 120 4300 1400 2400 86.7 NM 21.3 3860 2.72 Salivary gland 208 9700 3500 1700 NM NM 20.2 8740 6.16 Uveal tract 108 6500 1100 8500 2880 8160 176 8600 6.06 NM: Not measured,Metabolism14[5]Rat 2.5 0-18 NC NC NCNC 12.5 0-24 NC NC NCMonkey 2.5 0-4 7.02 98.7 312.90.12 12.5 0-8 18.0 38.5 131.7Human 2.5 0.25-18 100.4 6.90 17.30.014 12.5 0-18 66.95 10.4 25.8NC: Not calculated.[4] FDA Datadase. /drugsatfda_docs/nda/2014/205755Orig1s000PharmR.pdf (accessed Nov 2015).14[6]Ketoconazole (3A) 0-1 0.100 ~0.03 90.5 Azamulin (3A) 0-5 0.150 ~0.01 100 Ticlopidine (2B6/2C19) 0-10 1.70 >10 10.9S-mephenytoin (2C19) 0-250 95.5 >250 18 Montelukast (2C8) 0-2 0.0140 (0.18-0.71) >2 16.5 Furafylline (1A2) 0-10 2.00 >10 19.1 Quinidine (2D6) 0-1 0.0605 >1 17.9 Sulfaphenazole (2C9) 0-5 0.510 >5 11.9 Fluvastatin (2C9) 0-5 0.525 >5 21.6a Median value were calculated from (DMPK R0400785).If a range of values was reported for a study an average value was taken. The K i or IC50 values used in the calculations corresponded to inhibition of the enzyme (or subfamily, in the case of CYP3A).b Percent maximal inhibition of total [14C]Ceritinib metabolism at the concentrations of inhibitor examined.Rat a Ceritinib 108.03 ± 2.34 324.73 ± 17.09 426.58 ± 62.86 609.30 ± 32.39 L746530 168.29 ± 1.3 460.89 ± 22.3 709.78 ± 43.0 1068.22 ± 17.5Human a Ceritinib 105.80 ± 7.02 281.74 ± 0.68 504.46 ± 16.86 702.25 ± 57.12 L746530 173.98 ± 8.8 523.11 ± 0.5 684.59 ± 70.4 1057.12 ± 76.3Rat b Ceritinib 11.59 ± 0.25 34.73 ± 1.83 45.62 ± 6.72 65.17 ± 3.46 L746530 18.00 ± 0.14 49.29 ± 2.38 75.91 ± 4.60 114.25 ± 1.88Human b Ceritinib 11.32 ± 0.75 30.13 ± 0.07 53.95 ± 1.80 75.11 ± 6.11 L746530 18.61 ± 0.94 55.95 ± 0.05 73.22 ± 7.53 113.06 ± 8.16a Based on viable cells.b Based on 107 × 106 hepatocytes per gram of tissue (Wilson, et at 2003). Values were mean ± rang (n = 2) and rounded to three significant figures or to the nearest 0.01.[6]CeritinibRat 10.0 ± 1.2 21.2 ± 1.3 21.4 ± 0.9 15.0 ± 1.9 Human 10.4 ± 1.3 20.5 ± 0.5 12.3 ± 10.7 11.3 ± 0.9L746530Rat 64.4 ± 1.7 715.9 ± 35.7 579.8 ± 35.0 590.0 ± 49.5 Human 52.8 ± 2.6 254.3 ± 5.2 245.0 ± 24.1 354.1 ± 33.8a Based on nominal microsomal protein included in incubation. Values were mean ± SD (n = 3). All values were rounded to three significant figures or to the nearest 0.1.Monkey 2.50.25 92.5 0.23 0.31 ND 3.33 ND 0.68 1.20 ND ND0.5 89.9 0.28 0.59 ND 4.68 ND 0.77 1.77 ND ND1 83.8 0.81 0.95 ND 8.67 ND 0.58 3.58 ND ND2 76.9 1.96 1.26 ND 10.6 1.00 5.15 ND ND ND4 69.1 2.37 2.13 2.20 13.4 1.46 7.15 ND ND ND8 61.5 2.97 3.01 4.27 14.8 2.69 8.12 ND ND ND18 50.6 4.06 2.40 5.11 20.4 2.68 8.21 ND 2.51 2.9124 32.0 7.11 4.42 11.5 25.0 5.23 8.77 ND 2.15 2.5 12.50.25 NA NA NA NA NA NA NA NA NA NA0.5 92.7 0.23 0.24 ND 1.95 0.20 0.37 1.92 ND ND1 89.3 0.34 0.56 ND 3.11 0.41 0.53 3.09 ND ND2 80.7 1.68 0.97 1.09 6.05 1.17 5.60 ND ND ND4 80.6 1.12 1.21 1.56 5.32 1.81 6.12 ND ND ND8 74.2 2.16 1.34 4.06 5.96 3.48 5.90 ND ND 0.9318 71.2 2.10 1.43 5.61 6.81 3.34 5.07 ND 0.89 1.6924 61.9 4.05 1.81 8.11 9.31 5.82 5.41 ND 0.87 1.40Human 2.5 0.25 90.4 - - - 0.78 - 0.75 1.76 - ND0.5 90.9 - - - 0.77 - 0.98 1.19 - ND1 91.8 - - - 1.28 - 1.35 1.14 - ND2 91.6 - - - 2.22 - 1.18 1.02 - ND 4 89.9 - - - 3.11 - 1.46 1.26 - ND 8 87.6 - - - 4.52 - 1.47 1.55 - 1.11 18 83.2 - - - 8.17 - 1.61 1.52 - 1.59 24 81.4 - - - 8.94 - 2.62 1.38 - 2.28Human 12.5 0.25 NA - - - ND - NA NA - NA0.5 96.4 - - - ND - ND 3.60 - ND1 95.5 - - - ND - ND 4.47 - ND2 95.5 - - - ND - ND 4.55 - ND 4 95.7 - - - ND - ND 4.26 - ND 8 95.2 - - - ND - ND 4.81 - ND 18 85.1 - - - 7.05 - ND 7.89 - ND 24 90.8 - - - 2.96 - 3.93 0.67 - 1.65-: Not observed.Table 14 In Vivo Metabolites Profiles in Plasma, Bile and Feces of Rats, Monkeys and Humans[6]Plasma aRat i.v./p.o. 10/25 100 - - - - - - - - - - Monkeyi.v. 10 89.9 1.4 - 1.8 0.6 1.2 - 3 ---p.o. 30 84.4 3.6 - 2.5 0.4 1.6 - 3.1 ---Human p.o. 750 mg 81.6 - 1.2 1.4 1.9 1.6 1.8 2.3 1.7 1.7 2Bile Rat i.v. 10 34.89 ND ND - 1.09 3.26 0.83 ----p.o. 25 9.19 1.71 0.84 - 0.72 1.46 0.52 ----FecesRati.v. 10 12.05 3.75 4.56 - ND ND ND ----p.o. 25 51.77 4.54 5.88 - ND 2.82 ND ----Monkeyi.v. 10 55.1 1.8 2.8 - 3.7 10.9 17.9 0.3 ---p.o. 30 60.2 2.7 2.2 - 2.7 5.9 8.7 0.4 ---Human p.o. 750 mg 68 - 3.9 - 1.8 1.4 6.5 1.6 1.1 1.4 2.2M0: Ceritinib. a %AUC for metabolites in plasma.Figure D Proposed Pathways for In Vivo Biotransformation of [14C]Ceritinib in Rats, Monkeys and Humans[6] The red labels represent the major components in matrices. P = Plasma, U = Urine, B = Bile, F = Feces.ExcretionRat (intact)10 i.v. 0-168 - 0.241 ± 0.174 107 ± 7.825 p.o. 0-168 - 0.180 101 Rat (BDC)10 i.v. 0-72/168 65.4 0.62 29.825 p.o. 0-72/168 24.3 ± 8.52 1.05 ± 1.03 65.0 ± 17.0 Monkey10 i.v. 0-168 - 0.59 10530 p.o. 0-168 - 0.71 ± 0.45 92.3 ± 6.94 Human 9.14 p.o. 0-168 - 1.2 91.0Drug-Drug Interaction[5, 6]CYP1A2 Phenacetin >100 (2.5) - 1.0CYP1A2 mRNA 1.01 1.14 1.07 32.1CYP2A6 Coumarin 5 (1.5) 0.03 (0.009) 61.0 Activity 1.15d 1.22 1.01 31.7CYP2B6 Bupropion 2 (0.3) 5.3 (0.780) 1.3CYP2B6 mRNA 1.02 1.17 0.96 10.2CYP2C8 Paclitaxel 25 (0.6) - 1.1 Activity 1.05 1.20 0.92 4.65CYP2C8 Amodiaquine 2 (0.6) 16.7 (4.86) 1.1CYP2C9 mRNA 1.12 1.15 1.18 2.34CYP2C9 Diclofenac 2 (0.6) 0.24 (0.0701) 8.5 Activity 1.27 1.77 1.10 3.50CYP2C19 S-mephenytoin 70 (1.8) - 1.0CYP3A4 mRNA 1.27 2.73 6.03b31.1CYP2D6 Bufuralol 20 (2.9) - 1.2 Activity 0.98 1.43 1.33c8.81 CYP2E1 Chlorzoxazone 30 (4.4) - 1.1CYP3A4/5 Midazolam 0.2 (0.06) 0.16 (0.0469) 12.3CYP3A4/5 Testosterone 0.2 (0.06) -19.0Calculation of R1 values based on maximal steady-state concentration of 1010 ng/mL or 1.8 μM. [I]/K i assumed to be IC50/2 for competitive inhibition for those CYP enzymes without an experimental K i value. a Omeprazole 50 μM for CYP1A2, phenobarbital 1000 μM for CYP2B6 and CYP2C9, rifampin 10 μM for CYP3A4. b Mean of 3.24-, 8.74-, and 6.12-fold change relative to vehicle control in the three human hepatocyte lots. c Mean of 0.936-, 0.983-, 2.06-fold change relative to vehicle control in the three human hepatocyte lots. d:Mean of 1.75-, 1.24-, and 2.31-fold change relative vehicle control in the three human hepatocyte lots.[5]。