CT and MR imaging findings of sinonasal angiomatous polyps
医学影像检查技术学读后感
医学影像检查技术学读后感英文回答:Medical Imaging Technology: A Retrospective.Medical imaging technology has revolutionized the field of healthcare. By providing non-invasive and accurate visualizations of the human body, this technology has transformed the way medical professionals diagnose andtreat diseases. In this article, we delve into the significance and impact of medical imaging technology in modern medicine.One of the primary advantages of medical imaging is its ability to detect and characterize diseases at an early stage, even before symptoms manifest. For instance, computed tomography (CT) scans can identify early signs of cancer, allowing for timely intervention and improved patient outcomes. Magnetic resonance imaging (MRI) is another powerful tool that provides detailed images of softtissues, helping physicians diagnose complex neurological and musculoskeletal conditions.Medical imaging technology also plays a crucial role in guiding treatment plans and monitoring therapeutic progress. During surgeries, fluoroscopy and ultrasound imagingprovide real-time visualization of the surgical field, enabling surgeons to perform procedures with greater precision and skill. Positron emission tomography (PET) scans can measure metabolic activity within the body, providing valuable information about the effectiveness of treatment regimens.Furthermore, medical imaging technology has opened up new avenues for research and innovation. By studying images of diseased tissues, scientists can gain insights into the disease processes and develop novel therapeutic approaches. For instance, advancements in neuroimaging techniques have allowed researchers to better understand the neural basisof neurological disorders, leading to the development of more targeted treatments.The advancement of medical imaging technology continues at a rapid pace. Artificial intelligence (AI) is being integrated into imaging systems, automating image analysis and enhancing diagnostic accuracy. 3D printing is also making inroads into the field, enabling the creation of personalized medical models that can assist in surgical planning and patient education.In conclusion, medical imaging technology has had a profound impact on modern medicine. Its ability to provide detailed visualizations of the human body has transformed the way medical professionals diagnose and treat diseases, while also driving groundbreaking research and innovation. As technology continues to evolve, we can anticipate even more advancements that will shape the future of healthcare.中文回答:医学影像检查技术学读后感。
医学影像与人工智能的读后感

医学影像与人工智能的读后感英文版Reflections on Medical Imaging and Artificial IntelligenceReading the article "Medical Imaging and Artificial Intelligence" was an eye-opening experience. The intersectionof these two fields holds immense potential to revolutionize healthcare delivery.The author's exploration of how AI is enhancing medical imaging was particularly fascinating. The use of algorithms to analyze radiological images, detect abnormalities, and even predict disease progression is truly remarkable. The examples provided of AI's accuracy in diagnosing conditions like cancer were particularly impressive, highlighting the potential for earlier interventions and better patient outcomes.Moreover, the discussion on ethical implications was thought-provoking. As AI becomes more prevalent in healthcare, it's crucial to consider the ethical ramifications of its use. Theauthor's warning about potential biases in AI systems is a timely reminder of the need for rigorous testing and oversight.The future of medical imaging and AI integration looks incredibly bright. The potential for personalized medicine, predictive analytics, and improved patient care is enormous. However, it's equally important to ensure that these technologies are used ethically and responsibly.Overall, this article provided a comprehensive overview of the current state of medical imaging and AI, while also offering insights into the future of this exciting field. It left me excited about the possibilities but also cautious about the ethical challenges that lie ahead.中文版医学影像与人工智能的读后感阅读这篇文章“医学影像与人工智能”是一次令人大开眼界的经历。
CT成像原理介绍英文版医学知识讲解培训课件
MORE ATTENUATIOCNT成像原理介LES绍S 英ATTENUATION
文版医学知识讲解
5
How does CT Work?
X-ray generation Data acquisition Recon. & postpro.
CT成像原理介绍英
文版医学知识讲解
6
How does CT Work?
Non Slip-ring ScaCn文Tn版成er医像学原知理识S介l讲i绍p-解英ring Scanner
12
Computed Tomography
CT Basics Principle of Spiral CT Scan Parameter & Image Quality Optimizing Injection Protocols Clinical Applications
30 s
10mm P1
30s
More Coverage in the same time with extended Pitch!!
CT成像原理介绍10英mm P2
文版医学知识讲解
24
Scan Range = 300mm
30s
15s
10mm P1 10 mm/s
10mm P2 20 mm/s
Cover the same volumeCinT成sh像ort原er理ti介me绍w英ith extended Pitch
Less images createCdT成像原理介绍英
文版医学知识讲In解crement
18
Deep Inspiration
Shallow Inspiration
Standard CT / Slice Imaging
《医学影像识别课件》
1 Principles of MRI
Understand the physics behind magnetic resonance imaging and how it creates detailed anatomical images.
2 MRI vs CT
Compare the advantages and limitations of MRI and CT scans in different clinical scenarios.
Principles of Medical Imaging
Understand the fundamental principles of medical image acquisition and interpretation.
History of Medical Imaging
Trace the evolution of medical imaging techniques from X-rays to modern advancements.
Women's Imaging
Screening and diagnosis of breast and gynecological conditions, including mammography and ultrasound.
Future Trends in Medical Imaging Technology
Image Processing and Analysis
Discover the role of image processing and analysis in enhancing medical images and extracting valuable diagnostic information.
肝硬化癌变患者的MRI和CT表现及使用介入治疗期间应用影像学分析对改善疗效的临床效果

肝硬化癌变患者的MRI和CT表现及使用介入治疗期间应用影像学分析对改善疗效的临床效果李宇鸣1 骆顺娣1 罗素云1 黄志敏1 高连娣21阳山县人民医院放射科,广东 513100;2阳山县疾病预防控制中心,广东 513100通信作者:李宇鸣,Email:************** 【摘要】 目的 分析探讨肝硬化癌变患者的MRI和CT表现以及介入治疗期间应用影像学技术对改善疗效的临床效果,为提高肝硬化癌变诊断与介入治疗水平提供参考。
方法 研究对象随机选取2010年1月至2019年1月在本院接受治疗的138例肝硬化癌变患者,经病理学证实癌变病灶165个。
观察MRI和CT扫描影像学表现特征,收集诊断结果。
结果 CT扫描共检出肝硬化癌变病灶122个,诊断符合率73.94%;MRI扫描共检出肝硬化癌变病灶165个,诊断符合率100.00%,两种检查方法诊断符合率差异有统计学意义(P<0.05)。
CT扫描122个病灶中,动脉早期均表现为中等增强;MRI扫描165个病灶中,T1WI像:110个病灶呈略低信号、55个病灶呈略高信号,T2WI像:124个病灶呈高信号,增强动脉扫描可见动脉期124个病灶呈中度强化,41个病灶小结节样强化;138例肝硬化癌变患者中98例表现为甲胎蛋白(AFP)升高,结合影像学诊断结果实施介入治疗。
结论 MRI应用于肝硬化癌变检查诊断效果显著优于CT检查,是肝硬化癌变病灶检出的临床首选影像学手段;对于MRI扫描高度提示的癌变患者,应尽早实施介入治疗以保证临床疗效。
【关键词】 肝硬化癌变;电子计算机断层扫描;磁共振成像;影像学分析;介入治疗 DOI:10.3760/cma.j.issn.1007-1245.2020.08.024MRI and CT findings of patients with cirrhosis and cancer and the clinical effect of using imaging analysisto improve the curative effect during interventional therapyLi Yuming1, Luo Shundi1, Luo Suyun1, Huang Zhimin1, Gao Liandi21Department of Radiology, Yangshan People’s Hospital, Qingyuan 513100, China; 2Yangshan Center of DiseasePrevention and Control, Qingyuan 513100, ChinaCorrespondingauthor:LiYuming,Email:************** 【Abstract】Objective To analyze and explore the MRI and CT manifestations of patients with cirrhosisand cancer on one hand and on the other hand the clinical effect of using imaging technology to improvethe curative effect during interventional therapy, and to provide references for improving the diagnosis and interventional therapy of cirrhosis and cancer. Methods A total of 138 patients with cirrhosis and cancer whowere treated in our hospital from January, 2010 to January, 2019 were randomly selected, and 165 cancer lesionswere confirmed by pathology. The imaging features of MRI and CT scan were observed, and the diagnostic resultswere collected. Results A total of 122 lesions of cirrhosis were detected by CT scanning, and the diagnosticcoincidence rate was 73.94%; a total of 165 lesions of liver cirrhosis were detected by MRI scanning, and thediagnostic coincidence rate was 100.00%; there was a statistical difference in diagnostic coincidence rate betweenthe two examination methods (P<0.05). CT scan showed moderate enhancement of middle artery in the 122lesions at early stage. Among the 165 lesions, T1WI images showed a slightly low signal in 110 lesions and aslightly high signal in 55 lesions, while T2WI images showed a slightly high signal in 124 lesions. Enhancedarterial scanning showed a moderate enhancement in 124 lesions in the arterial phase and a nodular enhancementin 41 lesions. Among the 138 patients, 98 had an increase in fetoprotein (AFP), and took intervention treatmentaccording to the imaging diagnosis results. Conclusion MRI in the diagnosis of liver cirrhosis and cancer issignificantly more effective than CT, so it is the first clinical diagnostic choice. For patients with cancer lesionssuggested by MRI, early interventional treatment should be adopted to ensure the clinical curative effect. 【Key words】 Liver cirrhosis; Computed tomography; Magnetic resonance imaging; Imaging analysis; Interventional therapy DOI:10.3760/cma.j.issn.1007-1245.2020.08.0241115 肝硬化是消化内科常见的慢性进行性肝病,表现为由一种或多种病因长期、反复作用形成的弥漫性肝损害[1]。
脑炎影像诊断英文版护理操作

03
Continuously monitor the patient's vital signs and other indicators to ensure their safety and well being
CHAPTER
04
Regular maintenance and cleaning: Routinely clean and maintain the equipment to ensure its optimal performance and longevity
要点三
Propose positioning of the patient
Serial imaging can track the progress of ethics and assess the response to treatment
Computed Tomography (CT)
CT provides rapid and detailed images of the brain, but it may not detect subtle changes associated with ethics
PET scan
Postron Emission Tomography, a nuclear medicine imaging technique that produces three dimensional images of metabolic activity in the brain
Read the report through
Minimize discomfort
科学作文医学影像与人工智能
科学作文医学影像与人工智能英文回答:Medical imaging plays a crucial role in the field of medicine. It allows doctors to visualize the internal structures of the body and diagnose various medical conditions. Over the years, advancements in technology have greatly improved medical imaging techniques, making it more accurate and efficient. One of the latest developments in this field is the integration of artificial intelligence (AI) into medical imaging.AI has the ability to analyze large amounts of medical data and identify patterns that may not be easily detectable by human doctors. For example, in the field of radiology, AI algorithms can analyze medical images such as X-rays, CT scans, and MRIs to detect abnormalities or potential diseases. This can help doctors make more accurate diagnoses and develop appropriate treatment plans.Furthermore, AI can also assist in the interpretation of medical images. It can help identify specific structures or organs within an image, measure their size, and even predict the likelihood of certain diseases based on the image analysis. This can save valuable time for doctors and improve overall efficiency in healthcare.In addition to diagnosis and interpretation, AI can also aid in the process of image acquisition. For instance, AI algorithms can automatically adjust the settings of a medical imaging device to optimize image quality and reduce radiation exposure. This ensures that patients receive the best possible imaging results while minimizing potential risks.The integration of AI into medical imaging has the potential to revolutionize the field of medicine. It can enhance the accuracy and efficiency of diagnoses, improve patient outcomes, and reduce healthcare costs. However, it is important to note that AI is not meant to replace human doctors. Instead, it should be seen as a valuable tool that can assist healthcare professionals in their decision-making process.中文回答:医学影像在医学领域中起着至关重要的作用。
三线表的规范格式

功能与分子医学影像学(电子版) 2020年7月第9卷第3期 Funct Mol Med Imaging (Electronic Edition), Jul 2020, V ol. 9, No.31881床病理特征及预后[J]. 中华胃肠外科杂志, 2011, 14(8):599-602.[19]S andrasegaran K, Rajesh A, Rushing DA, et al.Gastrointestinal stromal tumors:CT and MRI findings[J].European Radiology, 2005, 15(7):1407-1414.[20]I noue A, Ota S, Sato S, et al. Comparison of characteristiccomputed tomographic findings of gastrointestinal and non-gastrointestinal stromal tumors in the small intestine[J]. Abdominal radiology(New York), 2019, 44(4):1237-1245.[21]Y i-bin Xie, Jia DU, Qian Li, et a1. Treatment andprognosis of patients with duodenal gastrointestinalstromal tumors[J]. Zhong Hua Yi Xue Za Zhi, 2012, 92(24):1694-1697.[22]戚元刚, 李向华, 李云, 等. 动态增强CT在腹腔间质瘤和神经内分泌瘤鉴别诊断中的应用价值[J]. 临床放射学杂志, 2020, 39(2):346-349.[23]K im JY, Lee JM, Kim KW, et al. Ectopic pancreas:CTfindings with emphasis on differentiation from small gastrointestinal stromal tumor and leiomyoma[J].Radiology, 2009, 252(1):92-100.(收稿日期:2020-05-02)(本文编辑:许水妹)•读者•作者•编者•三线表的规范格式表序和标题:表序即表格的序号,一篇论文中如只有1个表格,则表序编为表1;表题即表格的名称,应准确得体并能确切反映表格的特定内容,且简短精炼。
鼻腔常见肿瘤的CT诊断及鉴别诊断
CT diagnosis of the benign and m alignant tumors of nasal cavityL IU Y uan ,L UO De 2hong ,L I L in ,YA O Xue 2song ,S UN Wei ,W U Ning ,ZHOU Chun 2w u(Depart ment of Diagnostic Radiology ,Cancer hospital ,Chinese Academy of Medical Sciences ,Peking U nion Medical College ,Beijing 100021,China )[Abstract] Objective To assess the CT manifestations of the tumors in nasal cavity and understand the key point of the diagno 2sis and differential diagnosis between benign and malignant tumor of nasal cavity.Methods CT findings of the nasal cavity tumor confirmed by pathology in 43cases were reviewed retros pectively ,including inverted papilloma (12cases ,2cases had malignant transformation ),non 2Hodgkin lymphoma (12cases )and cancer (19cases ).R esults Twelve cases of the inverted papilloma wereunilateral lesions ,all located in the lateral nasal wall.Of the 10beni gn inverted papillomas ,the tumors of 9cases (90%)located in middle 2posterior portion of the nasal cavity ,10cases (100%)had clear rim ,8masses (80%)were homogeneous.Of 12cases of NHL ,10(83.3%)were unilateral lesions ,9(75%)located in the anterior portion of the nasal cavity ,9(75%)involved the skin of the external noses with disappearance of the subcutaneous fat in 6cases (50%),the adjacent bone was absorbed in 3.Of the 19cancers of nasal cavity ,13cases (68.4%)were unilateral lesions ,the tumors were irregular in shape with adjacent structures inva 2sion in 18(94.7%),the adjacent bone destruction in 18(94.7%).Conclusion There are different CT characteristics among the inverted papilloma ,lymphoma and cancer in the nasal cavity ,CT scan is helpful to diagnose and differential diagnose in the tumors of nasal cavity.[K ey w ords] Nasal cavity ;Inverted papilloma ;Cancer ;Lymphoma ;Tomography ,X 2ray computed鼻腔常见肿瘤的CT 诊断及鉴别诊断刘 媛,罗德红,李 琳,姚雪松,孙 伟,吴 宁,周纯武(中国医学科学院中国协和医科大学肿瘤医院放射诊断科,北京 100021)[摘 要] 目的 分析鼻腔常见肿瘤的CT 表现,了解其诊断及鉴别诊断要点。
能谱CT单能量成像联合ASIR对胃癌图像质量的研究
122·中国CT和MRI杂志 2023年04月 第21卷 第04期 总第162期【第一作者】李思琪,女,初级,主要研究方向:影像医学与核医学。
E-mail:183****************【通讯作者】陈殿森,男,主任医师,主要研究方向:影像医学与核医学。
E-mail:********************Study on Image Quality of Gastric Cancer Copyright ©博看网. All Rights Reserved.·123CHINESE JOURNAL OF CT AND MRI, APR. 2023, Vol.21, No.04 Total No.162识困难;1分,图像质量极差,细小解剖结构及边界不能辨识。
两名医师评分取平均值作为主观评分结果。
1.5 统计学方法 采用SPSS 23.0软件进行统计学分析。
各组图像CNR、SNR采用单因素方差分析,计量资料以(χ-±s)表示;主观评分分值采用秩和检验;两名医师主观评分一致性采用Kappa 检验,K 值≤0.4表明一致性较差,0.40<k值<0.75表明一致性尚可,k值≥0.75表明一致性较好。
以P <0.05为差异有统计学意义。
2 结 果2.1 客观评价 70keV条件下,动静脉期重建图像的CNR、SNR分别为2.52±1.38、7.71±1.49、2.52±1.31、8.14±3.27,高于FBP组及其他单能量组,差异具有统计学意义(P <0.05),70keV联合不同ASIR重建时,动脉期及静脉期50%ASIR组图像CNR、SNR 分别为3.87±1.48、9.94±2.51、1.96±1.14、6.93±2.61,均高于其他各组,组间差异有统计学意义(P <0.05)。
鼻咽癌患者采用CT与MRI不同检查技术对于诊断效果的分析

刘娟等:鼻咽癌患者采用CT与MRI不同检查技术对于诊断效果的分析鼻咽癌患者采用CT与MRI不同检查技术对于诊断效果的分析刘娟刘娟,,王兴顺南京市江宁医院影像科,江苏南京211500摘要目的探究诊断鼻咽癌最有效的方式。
方法随机选取2019年6月—2023年5月南京市江宁医院收治的120例疑似鼻咽癌患者为研究对象,均进行电子计算机断层扫描(computed tomography, CT)与核磁共振成像(magnetic resonance imaging, MRI)检查,以病理组织活检为金标准,分析诊断结果。
结果 120例疑似鼻咽癌患者中,阳性104例,阴性16例。
CT诊断,真阳91例,假阳6例,真阴10例,假阴13例。
MRI诊断,真阳100例,假阳1例,真阴15例,假阴4例。
MRI诊断准确性为95.83%、灵敏性为96.15%、特异性为93.75%高于CT诊断的84.17%、87.50%、62.50%,差异有统计学意义(χ2=9.074、5.189、4.571,P<0.05)。
结论鼻咽癌患者使用MRI扫描,具有较高的诊断价值,便于及时进行治疗,临床应用价值显著。
关键词鼻咽癌;电子计算机断层扫描;核磁共振成像;诊断结果中图分类号R445文献标志码A doi10.11966/j.issn.2095-994X.2023.09.11.22Analysis of the Diagnostic Effect of Different Examination Techniques of CT and MRI in Nasopharyngeal Carcinoma PatientsLIU Juan, WANG XingshunDepartment of Imaging, Nanjing Jiangning Hospital, Nanjing, Jiangsu Province, 211500 ChinaAbstract Objective To investigate the most effective way to diagnose nasopharyngeal carcinoma. Methods 120 cases of suspected nasopharyn⁃geal carcinoma patients admitted to Nanjing Jiangning Hospital from June 2019 to May 2023 were randomly selected as study subjects, all of which were examined by computed tomography (CT) and magnetic resonance imaging (MRI), and the diagnostic results were analyzed with pathological tissue biopsy as the gold standard. Results Among 120 patients with suspected nasopharyngeal carcinoma, 104 cases were posi⁃tive and 16 cases were negative. CT diagnosis, 91 cases of true positive, 6 cases of false positive, 10 cases of true negative, 13 cases of false negative. MRI diagnosis, 100 cases of true positive, 1 case of false positive, 15 cases of true negative, 4 cases of false negative. MRI diagnosis accuracy of 95.83%, sensitivity of 96.15%, specificity of 93.75%, which were higher than CT diagnosis, 84.17%, 87.50%, 62.50%, and the difference was statistically significant (χ2=9.074, 5.189, 4.571, P<0.05). Conclusion The use of MRI scanning in nasopharyngeal carcinoma patients has high diagnostic value, facilitates timely treatment, and has significant clinical application value.Key words Nasopharyngeal carcinoma; Electron computed tomography; Magnetic resonance imaging; Diagnostic results鼻咽癌是一种发生于鼻咽部黏膜上皮的恶性肿瘤,多发生于鼻咽顶壁及侧壁,尤其是咽隐窝,是我国常见的恶性肿瘤之一[1-2]。
CTmri特殊成像选择题

CTmri特殊成像选择题1、通常把多少T的MRI诊断仪称为高场机器()。
A.0.5~1.OTB.1.0~2.0TC.1.0~1.5TD.1.5~2.0TE.>2.OT2、下列关于表面相控阵线圈的说法,错误的是()。
A.可明显提高MRI的信噪比B.有助于提高薄层的图像质量C.有助于提高高场机的图像质量D.有助于提高高分辨扫描的图像质量E.由多个子线圈单元构成,同时与多个数据采集通道相匹配3、下列哪一项不是人体内常见的磁性原子核()。
Α. 1H14NC. 2HD. 32PE. 23Na4、关于人体组织MRI信号的主要来源,下列描述正确的是()。
A.常规MRI信号主要来源于水分子中的质子,部分组织信号也可来源于脂质子B.人体组织中的结合水与自由水不可以互换C.蛋白质和结合水的T1值都很短D.对不合脂肪的组织而言,MRI信号直接来源于结合水E.蛋白质和结合水能产生MRI信号5、进动频率与下列哪一项成正比()。
A.磁旋比B.横向磁化矢量C.纵向磁化矢量D.信噪比E.主磁场的场强6、关于磁共振的概念和现象,下列说法错误的是()。
A.共振的条件是两者振动频率相同B.共振的实质是两者之间有能量传递C.从微观角度看,核磁共振现象是低能级质子获得能量跃至高能级D.从宏观角度看,核磁共振现象使横向磁化矢量发生偏转,其偏转角度与射频脉冲的能量有关,能量越大偏转角度越大E.射频脉冲能量的大小与脉冲强度和持续时间有关,当宏观磁化矢量的偏转角度确定时,射频脉冲的强度越大,需要持续的时间越短。
7、下列用来描述衡量组织的横向弛豫快慢的是()。
A.T1B.T2C.TED.TRE.以上都不是8、下列用来描述衡量组织的纵向弛豫快慢的是()。
A.Τ1B.T2C.TED.TRE.以上都不是9、下列哪项序列能反映不同组织质子含量的主要差别()。
A.TIWIB.T2WIC.PDWID.DWIE.MRS10、关于MR加权成像技术,下列描述错误的是()。
利用肩部CT图像和后处理技术优化的肩胛骨受限侧位X线摄影体位

·155CHINESE JOURNAL OF CT AND MRI, AUG. 2023, Vol.21, No.08 Total No.166【通讯作者】王诗鸣,男,主管技师,主要研究方向:X线,螺旋CT及图像后处理技术的新应用。
E-mail:*******************Lateral Radiography Posture of Posture-156·中国CT和MRI杂志 2023年08月 第21卷 第08期 总第166期1.5 临床实践 将1.4中分析得出的角度值作为肩胛骨体位受限者肩胛骨侧位X线成像体位中的身体正中冠状面与探测器的相对倾斜角度,应用到该类患者的临床肩胛骨侧位X线成像中,观察所得的肩胛骨侧位X线平片,并分析其图像质量。
2 结 果2.1 MIP图像上肩胛骨侧位显示最佳所需的旋转方向和角度 如图1所示,在标准的后前位基础上,借助VR图像对肩胛骨沿人体躯干长轴进行空间位置的旋转,至其对应的MIP图像上肩胛骨的侧位显示最佳处,现均为健侧向后方旋转,测出该处相较于标准的后前位的旋转角度为(59.70±6.26)°。
2.2 年龄段对肩胛骨MIP图像显示最佳所需旋转角度值的影响 如表1所示,对不同年龄段组的肩胛骨MIP图像显示最佳所需旋转角度值的测量结果进行对比分析,发现各年龄段组之间的差异均不显著(P >0.05),年龄段对肩胛骨MIP图像显示最佳所需的身体旋转角度值并无明显影响。
2.3 性别对肩胛骨MIP图像显示最佳所需旋转角度值的影响如表2所示,对不同性别组的肩胛骨MIP图像显示最佳所需旋转角度值的测量结果进行对比分析,发现男性组的测量结果为(60±6.37)°,稍高于女性的(59.03±6.09)°,但两组间的差异并无统计学意义(P >0.05),说明性别对肩胛骨MIP图像显示最佳所需的身体旋转角度值并无明显影响。
鼻咽纤维血管瘤的影像表现及临床

Page 17
Page 8
Background
(NA) is a rare vascular tumor, which represents 0.05 % of all head and neck tumors. At the same time, it is the most common benign neoplasm of the nasopharynx . NA occurs predominantly in adolescent males. Although histologically benign it shows locally aggressive growth with bone destruction and spread through natural foramina and fissures.
Page 5
影像图像
图10 DSA冠状位
图11 DSA矢状位
Page 6
患者:男,26岁
主诉:右鼻出血2天
现病史:患者输2天前无明显诱因出现右鼻出血,为鲜血,呈滴状,先从左前 鼻孔出,后亦从口中、右鼻流出,数分钟后停止,反复出现多次,总量约为 100ml,无鼻塞,流涕,嗅觉正常。无头痛、发热、咳嗽、打鼾,无耳鸣、 而鼻塞感,无听力下降。于当地医院治疗,予以鼻腔填塞,症状好转。在中 山陈星海医院,予以电子喉镜检查“右鼻腔肿物,性质待查”。
administration.
Enhancement on CT and MRI as well as signal-void areas on MR images, typical for high flow vessels (Fig. 2). Arteriography revealed abundant vascularity with main blood supply from the internal maxillary artery.
颅内鞍区肿瘤CT、MRI的影像表现及诊断意义

CHINESE JOURNAL OF CT AND MRI, APR. 2022, Vol.20, No.04 Total No.150CT and MRI Imaging Manifestations and 【通讯作者】钱金甲Copyright©博看网 . All Rights Reserved.·1920·中国CT和MRI杂志 2022年04月 第20卷 第04期 总第150期扫描前准备:清楚患者身上所有金属物质。
患者体位选择:患者平躺于扫描床,选取仰卧位。
扫描参数:管电压110kV,管电流200mA,扫描层厚、间距均为5mm。
扫描部位:扫描自C2椎体下缘到颅顶,首先进行平扫,在平扫完成后,利用高压注射器经肘静脉注入80mL碘海醇,进行增强扫描。
扫描完成后利用CT后处理工作站,对患者轴位扫描图像进行冠状位、矢状位图像重建,将图像数据传输到PACS系统,由专科医师针对扫描图像进行阅片和分析诊断。
1.2.2 MRI检查 检查仪器选用GE 1.5T磁共振,患者平躺于扫描床,取仰卧位,选用头颈线圈,进行常规自旋回波(TSE)序列T 1WI、T 2WI、DWI和矢状T 1WI和FLAIR序列轴位成像。
扫描范围:对腹部及病变部位先进行平扫,平扫完后注入Gd-DTPA试剂进行增强扫描。
扫描完成后进行图像后处理,最后由诊断医师进行阅片得出诊断结果。
1.3 观察指标鞍区肿瘤影响特征,以病理检查结果为基准,计算CT及MRI检查对颅内鞍区肿瘤检出正确率。
1.4 统计学方法 本研究数据均采用SPSS 18.0软件进行统计分析,计量资料采用(χ-±s )描述;计数资料通过率或构成比表示,并采用χ2检验;以P <0.05为差异具有统计学意义。
2 结 果2.1 CT及MRI检查对颅内鞍区肿瘤检出正确率 CT对颅内鞍区肿瘤检出正确率为87.27%(48/55),MRI检出正确率为96.36%(53/55),CT稍低于MRI,比较差异无统计学意义(P >0.05),见表1。
医学影像专业术语英文
医学影像专业术语英文Medical Imaging Professional Terminology1. What is medical imaging?Medical imaging refers to the techniques and processes used to create images of the human body for clinical purposes. These images are used by healthcare professionals to diagnose and treat medical conditions.医学影像是指用于临床目的的创建人体图像的技术和过程。
这些图像被医疗保健专业人员用于诊断和治疗医疗状况。
2. What are the different modalities of medical imaging?There are several modalities of medical imaging, including X-ray, computed tomography (CT), magnetic resonance imaging (MRI), ultrasound, nuclear medicine, and positron emission tomography (PET).医学影像学有多种模态,包括X射线、计算机断层扫描(CT)、磁共振成像(MRI)、超声波、核医学和正电子发射断层扫描(PET)。
3. What is the purpose of medical imaging?The purpose of medical imaging is to help healthcare professionals visualize the internal structures of the body in order to diagnose and treat medical conditions. It can also be used to monitor the progression of diseases and the effectiveness of treatments.医学影像的目的是帮助医疗保健专业人员可视化人体内部结构,以便诊断和治疗疾病。
CT和MRI有什么区别薛敏
CT和MRI有什么区别薛敏发布时间:2023-07-06T06:07:20.218Z 来源:《健康世界》2023年9期作者:薛敏[导读]成都市龙泉驿区第一人民医院四川成都 610100CT(Computed Tomography)是计算机断层摄影,MRI(Nuclear Magnetic Resonance Imaging)是磁共振成像,两者都是临床影像学检查中比较常见的类型,那么CT和MRI有什么区别呢?检查时又该注意什么?下面让我们来了解一下。
一、区别(1)成像原理不同:CT是根据人体不同的组织和器官,对X射线的吸收率不同,使用计算机重建方法得到人体二维横断面图像的影像设备。
MRI的原理是氢原子核在磁场中产生的信号,计算机将信号重建处理后得到的影像图像。
由于人体内的氢原子含量高、分布广,相当于一个小的磁体,小磁体的自旋轴分布和排列是杂乱无章的,如果我们把人体置于一个强大的磁场之内,那么这个小磁体它就会按照磁场的方向有规律的排列,这个时候我们再施加一个影响磁场的射频脉冲,同时以射频信号的方式吸收所释放的能量,这个射频信号被接收后,通过计算机进行数据重建,就可以转换成MRI图像。
(2)辐射量不同:CT是通过X射线进行检查,X线质硬,吸收少穿透多,辐射剂量较大。
通常头部CT辐射剂量大约是在2mSv,胸部CT大约是8mSv,这些辐射剂量对人体是比较安全的,所以不需要担心,只要检查过程中采取防护措施,比如身体非检查部位或X线敏感器官上用铅皮遮盖,可以最大程度的减少辐射,也不会对身体造成严重的损伤。
MRI设备的激励源为短波或超短波段的电磁波,波长在1m以上(小于300MHz),无电离辐射损伤,是一种安全的检查方法。
(3)成像参数不同:CT的成像参数为X线吸收参数。
MRI是一种多参数的成像方法。
目前使用的MRI设备用以成像的组织参数至少有氢核(质子)密度N(H)、纵向弛豫时间T1、横向弛豫时间T2以及体内液体的流速等4个。
低剂量与常规剂量CT在肺磨玻璃影结节鉴别和浸润性诊断中的应用比较

·47CHINESE JOURNAL OF CT AND MRI, NOV. 2023, Vol.21, No.11 Total No.169【通讯作者】刘志敏n o f L o w -d o s e C T a n d48·中国CT和MRI杂志 2023年11月 第21卷 第11期 总第169期1.3 观察指标析结节的分叶征、毛刺征、空洞征、钙化、血管集束征及胸膜凹陷征等特征的检出率;(2)肺GGN性质:所有患者行病理活检,根据病理报告统计患者GGN的良恶性及浸润程度,其中微小浸润腺癌(minimal infiltrating adenocarcinoma,MIA)及原位腺癌(adenocarcinoma insitu,AIS)视为非浸润性肺癌,浸润性腺癌(invasive adenocarcinoma,IAC)视为浸润性肺癌;(3)图像质量:使用1-5级评分法[7]对两种CT扫描图像进行评估,1分:指图像显示不清楚,伪影显著,完全不具有临床诊断价值;2分:指图像显示不清,伪影较显著,不具有临床诊断价值;3分:图像显示尚可,伪影较少,尚具备临床诊断价值;4分:指图像较清楚,无伪影,明显具备临床诊断价值;5分:图像清楚,无伪影,完全具备临床诊断价值。
其中5分视为图像质量优,4分为良,3分为中,2分及以下为差。
(4)扫描射线剂量:根据扫描过程中的记录统计剂量长度乘积(dose-length product,DLP)、CT容积剂量指数(CT dose index volume,CTD Ivol)、有效剂量(effective dose,ED)及有效管球剂量。
1.4 统计学分析数资料采用频数(n)和百分率(%)描述,组间比较使用卡方检验,等级资料组间比较采用非参数检验,以P <0.05表示差异具有统计学意义。
2 结 果2.1 不同剂量CT扫描GGN形态学特征结果比较 扫描结果显示,低剂量与常规剂量CT扫描在GGN的各形态学特征(分叶征、毛刺征、空洞征、钙化、血管集束征及胸膜凹陷征)检出率上均无统计学差异(P >0.05),见表1。
Nature子刊:科学家开发出可检测大脑深处光线的新型传感器

Nature子刊:科学家开发出可检测大脑深处光线的新型传感器来源:科技部生物中心 2023-01-18 15:30研究人员首先制造了光敏MRI探针,具体方法是将磁性颗粒包裹在称为脂质体的纳米颗粒中,该脂质体由先前开发的特殊光敏脂质制成。
数百年来,科学家们一直在使用光来研究活细胞。
但由于生物材料对光的吸收和散射,只允许科学家观察细胞内部和薄片组织,在深层组织和其他不透明环境中对光进行成像非常困难。
近期,麻省理工学院和纽约大学的研究团队,联合开发了一种新型传感器克服了这一障碍,其通过将光信号转换为磁共振成像(MRI)可以检测到的磁信号,实现脑组织深处光分布的表征。
研究成果发表在《Nature Biomedical Engineering》期刊,标题为“Mapping light distribution in tissue by using MRI-detectable photosensitive liposomes”。
研究人员首先制造了光敏MRI探针,具体方法是将磁性颗粒包裹在称为脂质体的纳米颗粒中,该脂质体由先前开发的特殊光敏脂质制成。
进一步的研究表明,当这些脂质暴露在紫外光下时,脂质体变得更容易渗透水,从而使内部的磁性颗粒与水进行相互作用,并产生可通过MRI检测到的信号。
当其再次暴露在蓝光下时变得不透水,则无可检测的信号产生。
接下来,研究人员将纳米颗粒注射到存活大鼠的大脑中,研究结果表明,在光敏纳米颗粒探针存在的情况下,可以使用MRI来绘制脑组织中光的空间分布。
研究人员展示了在存在光敏纳米粒子探针的情况下,可以使用磁共振成像(MRI) 绘制组织中光的空间分布。
每个探针都由一个顺磁分子储库组成,该储库被包含光敏脂质的脂质体膜包围。
入射光导致脂质的光异构化并改变跨膜的流体动力学交换,从而影响 MRI 中的纵向弛豫加权对比度。
将纳米粒子注射到活老鼠的大脑中,并使用 MRI 绘制对广泛使用的光刺激、光度测定和光疗应用的光照分布特征的反应。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
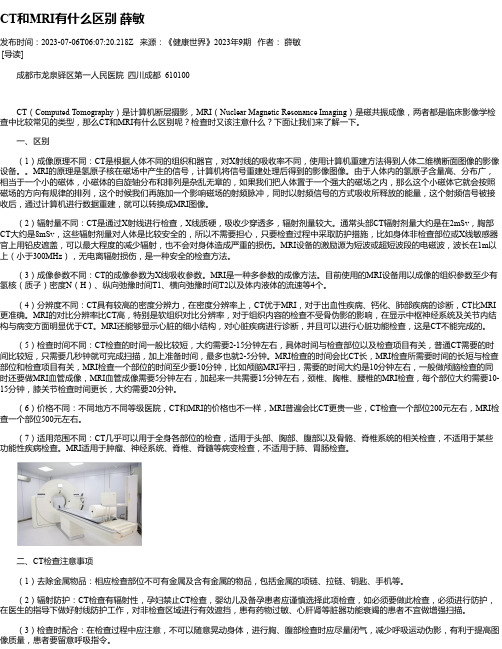
European Journal of Radiology 83 (2014) 545–551Contents lists available at ScienceDirectEuropean Journal ofRadiologyj o u r n a l h o m e p a g e :w w w.e l s e v i e r.c o m /l o c a t e /e j r adCT and MR imaging findings of sinonasal angiomatous polypsJing Zou a ,1,Fengyuan Man b ,1,Kai Deng c ,Yuanyuan Zheng a ,Dapeng Hao a ,∗,Wenjian Xu a ,∗∗aDepartment of Radiology,The Affiliated Hospital of Qingdao University,Qingdao,Shandong,China bDepartment of Radiology,Beijing Tongren Hospital,Capital Medical University,Beijing,China cDepartment of Radiology,Qingdao No.4People’s Hospital,Qingdao,Shandong,Chinaa r t i c l ei n f oArticle history:Received 17June 2013Received in revised form 28November 2013Accepted 5December 2013Keywords:Tomography,X-ray computed Magnetic resonance imaging Paranasal sinus diseases Hemangioma Nasal polypsa b s t r a c tObjective:To characterize the CT and MR imaging findings of patients with sinonasal angiomatous polyps (SAPs)and evaluate their respective clinical value in the diagnosis of SAP.Methods:CT and MR imaging findings of 15patients with pathologically proven SAP were examined.Assessed image features included location,size,margin,attenuation,and change of the bony walls of the sinonasal cavity on CT,and signal intensity and enhancement pattern on MR.Results:On CT,the SAP was mostly isoattenuated with patches of slight hyperattenuation.Most lesions caused changes in the adjacent bone,including expansile remodeling (n =8),defect or destruction (n =7),and hyperostosis (n =6).All lesions examined by MR showed heterogeneous isointense signal inten-sity on T1-weighted images and mixed obvious hyperintense and hypointense signal intensity with linear hypointense septum internally (n =10),and hypointense peripheral rim on T2-weighted images (n =10).Postcontrast MR images demonstrated areas of heterogeneous and marked enhancement with an unenhanced hypointense rim and septa (n =7).Conclusions:CT and MR imaging have respective advantages in the diagnosis of bined application of CT and MR examinations is necessary for patients with suspected SAP.© 2013 Elsevier Ireland Ltd. All rights reserved.1.IntroductionSinonasal angiomatous polyp (SAP)is a rare benign and non-neoplastic lesion.It is primarily composed of extensively hyperplastic and dilated vessels with scanty inflammatory infiltra-tion and abundant extracellular fibrin [1,2].Although inflammatory sinonasal polyp (SNP)is the most common non-neoplastic sinonasal mass examined pathologically,as a special subtype SAP only accounts for 4–5%of all SNPs [1].Simple conservative surgical excision of SAP is curative,and postoperative recurrence is rare.Therefore,correct preoperative diagnosis of SAP is important lest patients undergo unnecessary extensive surgery [3].SAP may show similar imaging features with sinonasal masses,such as other SNP,inverted papilloma,fungus ball,capillary hemangioma,juvenile angiofibroma and some pos-sibly malignant tumors [2,4,5].To the best of our knowledge,there have been only a few studies describing the imaging features of SAP∗Corresponding author at:Department of Radiology,The Affiliated Hospital of Qingdao University,16Jiangsu Road,Qingdao,Shandong,China.Tel.:+8653282911500.∗∗Corresponding author.Tel.:+8653282911585.E-mail addresses:haodp 2009@ (D.Hao),cjr.xuwenjian@ (W.Xu).1Both of them contributed equally and both of them are first author.[1–8].The purpose of this study was to report the characteristic CT and MR imaging findings of SAP in the sinonasal cavity.2.Materials and methods2.1.PatientsThe present study was approved by the institutional review board.Between July 2008and February 2013,a total of 15patients with pathologically proven SAP were retrospectively reviewed.The patients included five men and 10women,age range from 12to 81years,with a mean age of 42.7years.CT (n =13)and MR (n =10)images of these 15patients were retrospectively reviewed.Among these 15cases,two patients had a history of craniofacial trauma 2days and 2years previously,respectively.Furthermore,one patient underwent endoscopic sinus surgery to excise a nasal polyp 20years previously,and there had been massive bleeding from the ipsilateral nasal cavity 5years previously without appar-ent cause.The duration of symptoms before diagnosis ranged from 20days to 20years (median,12months).All 15patients underwent surgical excision of SAP by endoscopic sinus surgery.2.2.Imaging techniquesAmong the 15patients,CT scanning was performed in 13patients and MR imaging in 10patients.Eight patients underwent0720-048X/$–see front matter © 2013 Elsevier Ireland Ltd. All rights reserved./10.1016/j.ejrad.2013.12.002546J.Zou et al./European Journal of Radiology 83 (2014) 545–551Fig.1.Axial CT scan with a bone algorithm (a)shows an expansile mass (asterisk)centered in the right maxillary sinus.Expansile remodeling and thinning of the medial wall is observed (arrow).Axial CT scan with a soft tissue algorithm (b)shows a soft tissue mass (asterisk)isoattenuating to the masseter muscle with additional patches of slight hyperattenuation.Axial T1-weighted image (c)depicts heterogeneous isointense signal intensity with additional patches of interspersed hyperintensity and linear shadow of hypointensity on the mass (asterisk).Axial fat-suppressed T2-weighted image (d)demonstrates a well-defined lesion,which is markedly heterogeneous with linear hypointense septum internally and hypointense peripheral rim surrounding the lesion (asterisk).The bright signal intensity (arrow)due to obstructive sinusitis is demonstrated.Photomicrograph (e)shows that the lesion consists mostly of hemorrhage and necrosis,accompanied by extravasated fibrin and inflamed columnar epithelium (H&E,100).both CT and MR examinations.Seven patients underwent postcon-trast T1-weighted imaging.CT scans were obtained using a standard CT protocol for the paranasal sinuses.Thirteen patients underwent 2.5-mm-thick axial CT scanning with a bone algorithm and all images were reformatted with a soft tissue algorithm without the use of contrast media.In these patients,direct (n =10)or reformatted (n =3)coronal images were also obtained.MR examinations were performed using a 1.5T MR scanner (n =5)(Signa Advantage Horizon;GE Medical Systems,Milwaukee,WI)or a 3.0T MR scanner (n =5)(Signa HDx;GE Medical Sys-tems)with an 8-channel head coil.In these patients,precontrast T1-weighted spin-echo images (n =10)and T2-weighted fast spin-echo images with fat saturation (n =7)or short TI inversion recovery (n =3)were obtained,followed by contrast-enhanced,T1-weightedspin-echo images with fat saturation after the intravenous injec-tion of 0.1mmol/kg of gadolinium dimeglumine in seven patients.Images were obtained in at least two planes with 3mm section thickness and 1mm intersection gap.2.3.Imaging analysisTwo experienced head and neck radiologists retrospectively reviewed all the CT and MR images in consensus.The CT and MR imaging characteristics were analyzed with particular attention to the location,shape (expansile or nonexpansile),size,margin,atten-uation on precontrast CT,changes of the bony walls of the sinonasal cavity on bone CT,signal intensity on precontrast MR,and enhance-ment pattern on contrast-enhanced MR.The attenuation or signal intensity of the lesion was compared with that of the masseterJ.Zou et al./European Journal of Radiology83 (2014) 545–551547Fig.2.Axial CT scan with a soft tissue algorithm(a)shows an irregularly shaped mass in the left maxillary sinus and nasal cavity,which extends to the nasopharynx through choana(asterisk).Coronal CT in a bone algorithm(b)shows an expansile mass located in the enlarged sinus cavity(arrow).The margin is well defined,and the nasal septum is compressed and deformed.There is a large defect in the medial maxillary sinus wall(arrowheads).muscle.The location of each lesion,whether in the maxillary sinus or/and in the nasal cavity,was confirmed according to the site of the main body of the lesion.The size of each lesion was measured at the greatest diameter of the mass.The margin of each lesion was clas-sified as well-defined or ill-defined.On postcontrast MR images, the degree of enhancement was also subjectively assessed as mild enhancement(less than or equal to that of the masseter muscle)or marked enhancement(greater than that of the masseter muscle).3.ResultsThe symptoms of the patients were nasal obstruction in80.0% (12/15),epistaxis in53.3%(8/15),rhinorrhea(n=4),headache (n=3),facial numbness(n=2),visual acuity reduction(n=1), hyposmia(n=3),and syrigmus(n=2).Histopathological examinations showed most of the central areas of the lesion were composed of hemorrhage with exten-sive hyperplastic and dilated thin-walled blood vessels,fibrosis, and thrombus formation,and areas of focal inflammation.The cen-tral areas were surrounded by hemosiderin-laden macrophages, associated with recent hemorrhages(Figs.1e and4d).Grossly,the SAP was seen as a relatively well-circumscribed,lobulated and necrotic mass with a purple or dark red surface that bled easily when touched lightly.On sectioning,the cut surfaces werefirm, alternating with yellow-brown and hemorrhagic necrotic zones that showed cystic degeneration.Moreover,in eight lesions,SAP was found to accompany an inflammatory polyp of the sinonasal cavity.The CT and MR imaging features of the15patients with SAP are summarized in Table1.Eight SAPs occurred in the left side and seven in the right side.Thirteen lesions were located in the maxil-lary sinus and nasal cavity.Two lesions were confined to the nasal cavity.Of these,seven cases extended to the choana and nasophar-ynx(Fig.2).On CT and MR images,these lesions were seen as an expansile mass in10patients(Figs.1a–d,3,and4a–c)and nonexpansile mass infive patients.The size of the lesions ranged from10.4mm to 62.6mm in greatest diameter,with a mean of40.3mm.Thirteen of 15(86.7%)lesions displayed well-defined margins and two of15 (13.3%)lesions were ill-defined(Fig.3b).On CT images,the masses were heterogeneous.The lesions had a soft tissue density andfilled the sinonasal pared with the masseter muscle,the mass was mostly isoattenuated in all patients,with additional patches of slight hyperattenuation in11 patients(Figs.1b and2a).Calcification was not found in any case. Most lesions(12/13)caused changes in the adjacent bone,includ-ing expansile remodeling accompanied by thinning of the bony wall(n=8,Fig.1a),defect or destruction of adjacent bones(n=7, Fig.3a),and hyperostosis of the sinonasal walls(n=6,Fig.3c).The most common site of maxillary wall with expansile remodeling and thinning was the medial wall(n=7),followed by the nasal sep-tum(n=4)and the posterior lateral wall(n=2).The defect of the bony wall also could be seen in the medial wall(n=5),lateral wall (n=3),posterior wall(n=1),and the medial wall of the orbit(n=1). Hyperostosis was seen along the posterior lateral wall(n=5)and the anterior wall(n=3).All of the10lesions examined by MR mostly showed het-erogeneous isointense signal intensity(n=10)on T1-weighted images,with additional points or patches of interspersed slight hyperintensity(n=10)and linear shadow of hypointensity(n=9) (Figs.1c and4a).In contrast,all of the lesions showed markedly het-erogeneous,mixed hyperintense and hypointense signal intensity on T2-weighted images(n=10),with linear hypointense septum internally(n=10)and hypointense peripheral rim surrounding the lesion(n=10)(Figs.1d and4b).Postcontrast MR images demon-strated areas of heterogeneous and marked enhancement(n=7)in all of the lesions with an unenhanced hypointense rim and septa (n=7)(Fig.4c).Obstructive sinusitis was observed in all patients (n=10)in varying degrees(Figs.1d and4b).4.DiscussionThere are numerous descriptions of SAP in the literature, including organized or organizing hematoma[3,7–14],cavernous hemangioma[15–17],hemangioma[18,19],hematoma-like mass of the antrum[20],pseudotumor[21],hemorrhage necrotic polyp, and angioectatic or angiomatous polyp[1,2,4–6,22,23].Study and comparison of these seven terms shows that they all share the same clinical,pathological,and imaging features.The present study uses the term“angiomatous polyp”because it reflects the fact that the lesion is not a real tumor and that the mass is characteristicallyfilled with clusters of irregularly shaped,dilated thin-walled vessels and extensive vascular proliferation.The pathogenesis of SAP has not been elucidated;however, many hypotheses have been proposed.At present,there are two prevailing opinions.One hypothesis is based on the presence of nasal polyps.The polyps are usually located near the sinus ostia and protrude through the sinus ostium into the adjacent cavity. Because of the particular anatomical conditions,the polyp pedicle is subject to significant vascular compromise.Accordingly,the com-pression of the feeder vessels causes stasis,edema,and ischemia of the polyp.This leads to venous infarction followed by neovascular-ization andfibrosis of the polyp,which then evolves into thefinal SAP[23].J.Zou et al./European Journal of Radiology83 (2014) 545–551549Fig.3.Coronal CT scan with bone algorithm(a)shows a soft tissue mass in the left maxillary sinus,which causes a bone defect of the anterior wall(arrow).Coronal CT scan with soft tissue algorithm(b)shows the lesion extends to the fat space and displays an ill-defined margin(arrow).Axial CT scan with bone algorithm(c)demonstrates hyperostosis in the posterior lateral wall of the left maxillary sinus(arrows).Another hypothesis is based on the formation of hematoma in the sinus antrum[3,7,8].The hematoma develops initially from the accumulation of blood in the sinus antrum resulting from various causes,such as trauma,surgery,bleeding diatheses,and the loss of mechanical integrity of an arterial branch,as seen in a ruptured aneurysm or inflammatory erosion of an arterial wall[7,12–14]. The blood remains in the sinus antrum because of poor ventila-tion and drainage conditions,especially in the maxillary sinus.As is known,SAP occurs most frequently in the maxillary sinus,the largest paranasal sinus.These allow conditions of negative pres-sure and decreased ventilation[7].Persistent negative pressure and decreased ventilation lead to difficulties in expelling fresh blood from the maxillary sinus,and subsequently organization and fibrous degeneration of hematoma ensue.Reactive and reparative changes with neovascularization lead to the eventual formation of SAP.This process accounts for the progressive expansion and local bony destruction associated with SAP[3,7,8,13].Based on the results of the present study,the two hypothe-ses are both reasonable.Of the15cases examined,most lesions (n=13)were located near the sinus ostium and often involved the ipsilateral nasal cavity and maxillary sinus through the ostium and extended toward the choana and nasopharynx(n=7).Furthermore, eight cases were associated with the inflammatory polyps proven by pathological reports and/or operative notes.Given these facts, thefirst hypothesis is reasonable in some cases.However,some cases are also consistent with the latter hypothesis.Three cases had a history of previous head and neck surgery or a history of craniofacial trauma.Six cases had a history of frequent epistaxis. Moreover,the most lesions(n=13)were located in the maxillary sinus,and expansion(n=10)and local bony destruction(n=7)were also frequent.A wide age range of patients has been reported,from11to81 years[4,5,14,20,21,24].In the present study,patients’age ranged from12to81years(median,42.7years),and there was a prepon-derance of women,with a male-to-female ratio of1:2.As in the literature[6,7,13,20],patients often presented with nasal obstruc-tion(n=12)and epistaxis(n=8),because gradual enlargement of the lesion displaced the adjacent bony structures and caused inflammatory infiltration of stroma,which eroded the hyperplastic and thin-walled vessels.Reports on of SAP clarified that CTfindings lacked specificity for SAP identification[4,5,7].The typical appearance includes an expansile mass causing bulge or destruction of the bony wall and heterogeneous isoattenuation on precontrast CT scans.The pres-ence of attenuation in the present study is in accordance with the characteristics previously mentioned.In the present study,most of the lesions(n=12)caused changes in the adjacent bone,including expansile remodeling and thin-ning,defect or destruction of adjacent bones,and hyperostosis of the sinonasal walls.Expansile remodeling and thinning of adjacent bones was the most common change(n=8),and may indicate a long growth process and benign growth pattern.In seven cases,defect of the bony wall could also be seen,which was caused by increas-ing pressure and/or bone resorption.Hyperostosis(n=6)may be related to chronic obstructive sinus inflammatory reaction.It is difficult to make accurate diagnoses based only on the CT features,such as the large soft tissue mass with heterogeneous den-sity and the associated bone destruction[1,4].However,the masses are well defined and do not invade the peripheral soft tissue on CT, which is associated with the non-neoplastic growth pattern of SAP. In spite of CT imaging lacking specificity for SAP,it was superior to MR imaging for demonstrating bone changes associated with the lesion.Compared with the CTfindings,the SAP lesion has a char-acteristic appearance on MR images.According to the literature and the present study,the typical imaging features of SAP on550J.Zou et al./European Journal of Radiology 83 (2014) 545–551Fig.4.Axial T1-weighted MR image (a)shows that the lesion is mostly isointense compared to the masseter muscle interspersed with points of hyperintensity (asterisk).Axial,short TI inversion recovery MR image (b)shows the marked heterogeneity of the lesion with a mix of hypointense,and marked hyperintense signals (asterisk).The dark peripheral rim surrounding the lesion is also well demonstrated.The curvilinear hyperintensity area around the mass indicates obstructive sinusitis.Postcontrast axial,fat-suppressed,T1-weighted MR image (c)shows heterogeneous and marked enhancement (asterisk)in most regions of the lesion with an unenhanced hypointense rim and septa.Photomicrograph (d)shows that the lesion consists of hemorrhage,extravasated fibrin,inflamed cells and scattered hemosiderin-laden macrophages (H&E,100×).MR images are as follows:(i)expansive soft tissue mass,(ii)well-defined margin,(iii)blockage of ostium and secondary obstruction,(iv)extension into the choana and nasopharynx,(v)heterogeneous isointense signal intensity with interspersed slight hyperintensity on T1-weighted imaging,and (vi)markedly het-erogeneous,obvious hyperintense with hypointense linear septum internally and peripheral rim surrounding the lesion.Remarkably,the hypointense peripheral rim around the mass is a very specific contribution to the correct diagnosis of SAP.The postcontrast MR images of SAP also demonstrated a char-acteristic appearance with areas of heterogeneous and marked enhancement with unenhanced hypointense rims and septa.In the present study,MR imaging showed the margin and extent of the mass more clearly and more precisely than CT imaging,as reported by Kim et al.[3].The hydrops of the adjacent paranasal sinuses caused by secondary obstruction and inflammation can be differentiated easily from the lesion on MR images,especially on T2-weighted images.However,it is difficult to distinguish between the main lesion and sinus inflammation on CT,which often results in overestimating the size of the lesion.Furthermore,due to the higher soft tissue contrast resolution,MR imaging is superior to CT for determining the internal characteristics of the lesion with var-ious signal intensities on T1-and T2-weighted Images 3.Although an exact 1:1MR-pathologic correlation is not possible because most lesions are removed in pieces and not en bloc,the heterogeneous signal intensity seen on MR images reflects the various components contained within the lesion,such as hemorrhage in various stages,fibrosis,and various amounts of vascular proliferation [3,24].Post-contrast MR imaging can provide valuable information about theblood supply of the mass and the integrity of vessel walls to predict whether a lesion is benign or malignant.As suggested by Lee et al.[7],the areas with enhancement represent the areas of prominent vascular proliferation.Based on previous experience,the appearance of SAP on CT may cause the radiologist to misdiagnose the mass as malig-nant.Bone erosion can also occur in other benign lesions,such as other inflammatory nasal polyps,cholesterol granuloma,fun-gus ball,inverted papilloma and capillary hemangioma [4,7,14,24].The radiologist should not presume that a lesion is malignant simply relying on a defect in the bone on CT images.Contrast enhancement examination is extremely useful,because inflamma-tory polyp,cholesterol granuloma,and fungus ball are not usually enhanced.Inverted papilloma primarily involves the nasal cavity and reveals a characteristic convoluted cerebriform pattern on both T2-weighted imaging and contrast-enhanced T1-weighted imag-ing [25].Capillary hemangioma is difficult to differentiate from SAP both clinically and radiologically.Tubular flow-void signal intensity on both T2-weighted imaging and contrast-enhanced T1-weighted imaging may be a noteworthy contribution to differential diagno-sis [4,26].Malignant tumors demonstrate frank bony destruction,rather than a clearly defined defect of the sinus walls,associated with adjacent tissue invasion,which results in indistinguishable fat space around the lesion [7].For radiologists inexperienced in head and neck pathology,SAP may be misdiagnosed as juvenile nasopharyngeal angiofibroma.The main identifications of juvenile nasopharyngeal angiofibroma as follows:(i)affecting young males,(ii)widening the pterygopalatine fossa with bowing of the poste-rior wall of the maxillary sinus,(iii)multiple flow-void channelsonJ.Zou et al./European Journal of Radiology83 (2014) 545–551551MRI and(iv)marked enhancement after Gd-DTPA administration [2,27].5.ConclusionsCorrect preoperative diagnosis is important for determining therapeutic schedules,because SAP is usually curative with com-plete surgical resection by endoscopic sinus surgery.CT and MR imaging have respective advantages in the diagnosis of SAP.Pre-operative CT images that show the changes in adjacent bones can provide an accurate basis for the determination of the surgical scope.Preoperative MR images that show the characteristic appear-ance in signal intensity can provide an accurate diagnosis of SAP. Therefore,combined application of CT and MR examinations is nec-essary for patients with suspected SAP.Moreover,the characteristic appearance on postcontrast MR images of SAP also provides the basis for qualitative diagnosis and preoperative preparation. References[1]Yfantis HG,Drachenberg CB,Gray W,Papadimitriou JC.Angiectatic nasal polypsthat clinically simulate a malignant process:report of2cases and review of the literature.Archives of Pathology&Laboratory Medicine2000;124(3):406–10.[2]Sheahan P,Crotty PL,Hamilton S,Colreavy M,McShane D.Infarctedangiomatous nasal polyps.European Archives of Otorhinolaryngology 2005;262(3):225–30.[3]Kim EY,Kim HJ,Chung SK,et al.Sinonasal organized hematoma:CTand MR imagingfindings.AJNR American Journal of Neuroradiology 2008;29(6):1204–8.[4]Wang YZ,Yang BT,Wang ZC,Song L,Xian JF.MR evaluation ofsinonasal angiomatous polyp.AJNR American Journal of Neuroradiology 2012;33(4):767–72.[5]Dai LB,Zhou SH,Ruan LX,Zheng ZJ.Correlation of computed tomogra-phy with pathological features in angiomatous nasal polyps.PLOS ONE 2012;7(12):e53306.[6]De Vuysere S,Hermans R,Marchal G.Sinochoanal polyp and its variant,theangiomatous polyp:MRIfindings.European Radiology2001;11(1):55–8. [7]Lee HK,Smoker WR,Lee BJ,Kim SJ,Cho anized hematoma ofthe maxillary sinus:CTfindings.AJR American Journal of Roentgenology 2007;188(4):W370–3.[8]Nishiguchi T,Nakamura A,Mochizuki K,Tokuhara Y,Yamane H,Inoue Y.Expan-sile organized maxillary sinus hematoma:MR and CTfindings and review of literature.AJNR American Journal of Neuroradiology2007;28(7):1375–7.[9]Chiang TY,Chen anized hematoma of maxillary sinus mimickingmalignant neoplasm in a patient following chemoradiotherapy.Journal of Oto-laryngology–Head&Neck Surgery2008;37(2):E42–5.[10]Suzuki H,Inaba T,Hiraki N,et al.Endoscopic sinus surgery for the treat-ment of organized hematoma of the maxillary sinus.Kurume Medical Journal 2008;55(3–4):37–41.[11]Shen KJ,Som PM,Teng MS.Radiology quiz anized hematomaof the maxillary sinus.Archives of Otolaryngology–Head&Neck Surgery 2007;133(4):408,10.[12]Yoon TM,Kim JH,Cho YB.Three cases of organized hematoma of the maxillarysinus.European Archives of Otorhinolaryngology2006;263(9):823–6.[13]Lee BJ,Park HJ,Heo anized hematoma of the maxillary sinus.Acta oto-Laryngologica2003;123(7):869–72.[14]Unlu HH,Mutlu C,Ayhan S,Tarhan anized hematoma of the maxillarysinus mimicking tumor.Auris,Nasus,Larynx2001;28(3):253–5.[15]Kim HJ,Kim JH,Hwang EG.Bone erosion caused by sinonasal cavernous heman-gioma:CTfindings in two patients.AJNR American Journal of Neuroradiology 1995;16(5):1176–8.[16]Jammal H,Barakat F,Hadi U.Maxillary sinus cavernous hemangioma:a rareentity.Acta oto-Laryngologica2004;124(3):331–3.[17]Mussak E,Lin J,Prasad M.Cavernous hemangioma of the maxillary sinus withbone erosion.Ear,Nose,&Throat Journal2007;86(9):565–6.[18]Song CE,Cho JH,Kim SY,Kim SW,Kim BG,Kang JM.Endoscopic resectionof haemangiomas in the sinonasal cavity.Journal of Laryngology and Otology 2009;123(8):868–72.[19]Raboso E,Rosell A,Plaza G,Martinez-Vidal A.Haemangioma of the maxillarysinus.Journal of Laryngology and Otology1997;111(7):638–40.[20]Yagisawa M,Ishitoya J,Tsukuda M.Hematoma-like mass of the maxillary sinus.Acta oto-Laryngologica2006;126(3):277–81.[21]Ozhan S,Arac M,Isik S,Oznur II,Atilla S,Kemaloglu Y.Pseudotumor of the max-illary sinus in a patient with von Willebrand’s disease.AJR American Journal of Roentgenology1996;166(4):950–1.[22]Ceylan A,Asal K,Celenk F,Uslu S.An angiomatous nasal polyp:a very rarevariant of sinochoanal nasal polyps.B-ENT2007;3(3):145–7.[23]Batsakis JG,Sneige N.Choanal and angiomatous polyps of the sinonasal tract.Annals of Otology,Rhinology,and Laryngology1992;101(7):623–5.[24]Song HM,Jang YJ,Chung YS,Lee anizing hematoma of the maxillarysinus.Otolaryngology–Head and Neck Surgery:Official Journal of Ameri-can Academy of Otolaryngology–Head and Neck Surgery2007;136(4):616–20.[25]Ojiri H,Ujita M,Tada S,Fukuda K.Potentially distinctive features of sinonasalinverted papilloma on MR imaging.AJR American Journal of Roentgenology 2000;175(2):465–8.[26]Lee DG,Lee SK,Chang HW,et al.CT features of lobular capillary hemangioma ofthe nasal cavity.AJNR American Journal of Neuroradiology2010;31(4):749–54.[27]Gomaa MA,Hammad MS,Abdelmoghny A,Elsherif AM,Tawfik HM.Magneticresonance imaging versus computed tomography and different imaging modal-ities in evaluation of sinonasal neoplasms diagnosed by histopathology.Clinical Medicine Insights:Ear,Nose Throat2013;26(6):9–15.。