2011纽约州卫生署+梅毒
2010年美国疾病控制中心梅毒治疗指南与点评
标准 方案 指南2010年美国疾病控制中心梅毒治疗指南与点评樊尚荣,李健玲(编译)作者单位:518036广东省深圳市,北京大学深圳医院妇产科(樊尚荣);汕头大学医学院(李健玲)关键词 梅毒;诊断;治疗中图分类号 R 759 1文献标识码 C文章编号 1007-9572(2011)04-1055-031 概述1 1 分期 梅毒是由梅毒螺旋体引起的一种全身性疾病。
根据临床所见对疾病分期,以利于指导治疗和随诊。
根据传染途径不同分为后天梅毒与先天梅毒。
又根据其病期分为早期梅毒与晚期梅毒。
(1)早期梅毒:病期在2年以内,包括: 一期梅毒(硬下疳); 二期梅毒(全身皮疹); 早期潜伏梅毒(感染1年内)。
(2)晚期梅毒,包括: 皮肤、黏膜、骨、眼等梅毒; 心血管梅毒; 神经梅毒; 内脏梅毒; 晚期潜伏梅毒。
12 诊断1 2 1 螺旋体检查 病损分泌物做抹片,用暗视野检查或直接免疫荧光检查(DFA)活螺旋体,阳性者即可确诊。
1 2 2 血清学试验 包括非螺旋体试验和螺旋体试验。
非螺旋体试验包括快速血浆反应素试验(RPR)或性病研究试验(VDRL);螺旋体试验包括荧光螺旋体抗体吸附试验(FTA -ABS)及梅毒螺旋体明胶凝集试验(TPPA)。
非螺旋体试验存在假阳性,见于多种与梅毒无关的临床状态,包括自身免疫状况、高龄以及注射毒品者。
非螺旋体试验滴度可用于评价治疗效果。
同一实验室同一方法两次检测相差2个倍比稀释度(4倍)有意义。
1 2 3 脑脊液检查 脑脊液检查包括脑脊液细胞计数(白细胞>5/mm 3)、蛋白测定异常和VDRL 。
2 不同期别梅毒的处理2 1 一期梅毒、二期梅毒推荐方案:苄星青霉素,240万单位,1次/周,肌注,共1次。
儿童推荐方案:苄星青霉素,5万单位/kg ,最大剂量240万单位,1次/周,肌注,共1次。
青霉素过敏:强力霉素,100m g ,2次/d ,口服,连续14d 。
四环素,500mg ,4次/d ,口服,连续14d 。
梅毒完整版

编辑ppt
2
概述
梅毒是人类独有的疾病,显性和隐性梅毒患 者是传染源,感染梅毒的人的皮损及其分泌 物、血液中含有梅毒螺旋体。感染后的头2年 最具传染性,而在4年后性传播的传染性大为 下降。是由梅毒螺旋体,主要通过性接触或 胎盘传入,侵犯多系统多脏器的慢性传染病。
编辑ppt
3
病因
梅毒螺旋体,厌氧,人工培养困难
梅毒
编辑ppt
1
流行病学
梅毒在全世界流行,据WHO估计,全球每年约有 1200万新发病例,主要集中在南亚、东南亚和次撒 哈拉非洲。近年来梅毒在我国增长迅速,已成为报 告病例数最多的性病。所报告的梅毒中,潜伏梅毒 占多数,一、二期梅毒也较为常见,先天梅毒报告 病例数也在增加。
梅毒患者的皮肤、黏膜中含梅毒螺旋体,未患病者 在与梅毒患者的性接触中,皮肤或黏膜若有细微破 损则可得病。极少数可通过输血或途径传染。获得 性梅毒(后天)早期梅毒病人是传染源,95%以上是 通过危险的或无保护的性行为传染,少数通过接亲 吻、输血、污染的衣物等传染。胎传梅毒由患梅毒 的孕妇传染,如果一、二期和早期潜伏梅毒的孕妇, 传染给胎儿的几率相当高。
多形红斑
脓疱疮
银屑病
脂溢性皮炎
瘤型麻风
编辑ppt
37
鉴别诊断
三期与下列疾病鉴别: 慢性小腿溃疡 瘰疬性皮肤结核 孢子丝菌病 基底细胞癌
编辑ppt
梅毒的实验室诊断与临床意义PPT课件

非梅毒螺旋体抗原血清试验临床意义
1.适用于梅毒筛查、疗效观察、复发或再感染的 检查; ▪ 2.抗体水平与疾病严重程度成正比; ▪ 3.评价、监测治疗效果,此抗体治愈后可消失。 ▪ 4.此抗体不具有特异性,全身性疾病的活动期如: 红斑狼疮,风湿病,类风湿关节炎,病毒性肝炎,麻 风病,自身免疫性疾病等,都有可能出现。
现. ▪ 因透明不易染色,所以又称为苍白螺旋体。
梅毒流行病学统计
▪ 梅毒是世界三大慢性传染病之一(梅毒、 麻风、结核)。
▪ 1999年全国报告梅毒80406例。 ▪ 2009年全国报告梅毒327433例。 ▪ 2010年全国报告梅毒385678例. ▪ 2012年全国报告梅毒448620 例. ▪ 2012年广东全省报告新发梅毒病例数为
▪ 研究调查:对99例检查TPPA为阳性的新生儿随访, 6个月内自动转阴率为18.6%,2年内转阴率为 74.4%.
区分梅毒抗体来源
▪ 那么如何区分抗体是来自母体还是婴儿自 身感染产生呢?
▪ 和所有的细菌及病毒感染一样,在梅毒中 特异性lgM抗体的合成是初次感染后的体 液免疫应答,最先产生,随后才产生lgG抗 体。lgM抗体分子量大(97万道尔顿), 其不能通过胎盘屏障进入婴儿体内,lgG抗 体分子量小(15万道尔顿)能通过胎盘。
梅毒实验室检查
ห้องสมุดไป่ตู้
显微镜检查法
血清学检查
阳性:确认诊断 梅毒感染
阴性:无否定价值
非梅毒螺旋体 抗原血清试验
阳性:提示有活动 性疾病
阴性:有否定价值 (早期1月内感染除外)
梅毒螺旋体 抗原血清试验
阳性:确认梅毒感染 或曾经感染
阴性:有否定价值, 可排除梅毒感染
梅毒筛查策略
美国疾病控制中心梅毒治疗指南

美国疾病控制中心梅毒治疗指南梅毒是一种由苍白密螺旋体引起的慢性传染病,在全球范围内均有分布。
美国疾病控制中心(CDC)作为权威的公共卫生机构,为防控梅毒传播和指导治疗方案起到了关键作用。
本文的目的是基于循证医学证据,总结和分析美国疾病控制中心的梅毒治疗指南,为临床医生和患者提供科学的治疗建议。
本文将着重阐述美国疾病控制中心梅毒治疗指南的原则和方法,以及其循证医学证据的支持。
梅毒的病因是感染苍白密螺旋体,通常通过性接触、血液传播和母婴传播。
根据病程的不同,梅毒可分为早期梅毒(包括一期和二期)和晚期梅毒(三期)。
梅毒的临床表现复杂多样,早期梅毒主要表现为硬性下疳和淋巴结肿大,而晚期梅毒则涉及神经、心血管和骨骼等多个系统。
支持论点2:美国疾病控制中心的梅毒治疗指南美国疾病控制中心的梅毒治疗指南主要基于最新的循证医学证据。
对于早期梅毒,指南推荐使用青霉素G肌肉注射或普鲁卡因青霉素G肌肉注射。
对于晚期梅毒,指南建议使用同样的治疗方案,但需延长疗程。
对于孕妇患者,美国疾病控制中心推荐使用红霉素或多西环素进行治疗。
近年来,多项循证医学研究对梅毒治疗指南进行了评估。
结果显示,早期梅毒患者在接受推荐治疗方案后,病情得到有效控制,血清学转阴率较高。
对于晚期梅毒患者,延长疗程的治疗方案能够提高治愈率,降低复发风险。
孕妇患者在接受推荐治疗方案后,垂直传播给胎儿的风险可显著降低。
美国疾病控制中心的梅毒治疗指南基于最新的循证医学证据,为临床医生和患者提供了科学的治疗建议。
根据指南,早期梅毒患者应使用青霉素G或普鲁卡因青霉素G进行治疗,晚期梅毒患者需延长疗程以提高治愈率。
孕妇患者在治疗时应有特殊考虑,以降低胎儿感染风险。
治疗梅毒需要及时、规范化的治疗,以避免病情恶化和对患者及他人造成潜在危害。
性传播疾病是一种严重的健康问题,不仅危害个人健康,还可能引起严重的社会后果。
美国疾病控制中心(CDC)性传播疾病治疗指南旨在提供关于性传播疾病的病因分析、治疗措施、注意事项及预防措施的权威指导,以帮助患者及时治疗并防止疾病传播。
WS272007梅毒诊断标准

WS273-2007梅毒诊断标准梅毒诊断标准1范畴本标准规定了梅毒的诊断依据、诊断原则、诊断标准和鉴不诊断。
2术语和定义下列术语和定义适用于本标准。
2.1梅毒Syphilis梅毒是惨白螺旋体(又名梅毒螺旋体)感染人体所引起的一种系统性、慢性经典的性传播疾病,可累及人体多系统多脏器的损害,产生多种多样的临床表现,导致组织破坏、功能失常,甚至危及生命。
2.2前带现象Prozone phenomenon非梅毒螺旋体抗原试验(如RPR试验)中,有时由于血清抗体水平过高,抗原抗体比例不合适,而显现弱阳性、不典型或阴性的结果,但临床上又有典型的二期梅毒体征,将此血清稀释后再做血清学试验,显现了阳性的结果,称quot;前带现象二3缩略语下列缩略语适用于本标准。
VDRL Venereal Disease Research Laboratory 性病研究实验室(玻片试验)USR Unheated serum reagin血清不需加热的反应素(玻片试验)TRUST Toluidine red unheated serum test 甲苯胺红血清不需加热试验RPR Rapid plasma reagin快速血浆反应素(环状卡片试验)FTA-ABS Fluorescent treponemal antibody-absorption 荧光螺旋体抗体吸取(试验)TPHA Treponema pallidum hemagglutination assay梅毒螺旋体血凝试验TPPA Treponema pallidum particle agglutination assay 梅毒螺旋体颗粒凝集试验4诊断依据4.1一期梅毒4.1.1流行病学史:有多性伴,不安全性行为,或性伴感染史。
4.1.2临床表现:4.1.2.1硬下疳:埋伏期一样为2〜4周。
一样为单发,但也可多发;直径约1cm〜2cm,圆形或椭圆形浅在性溃疡,界限清晰、边缘略隆起,疮面清洁;触诊基底坚实、浸润明显,呈软骨样的硬度;无明显疼痛或触痛。
卫生部关于印发《中国预防与控制梅毒规划(2010-2020年)》的通知
卫生部关于印发《中国预防与控制梅毒规划(2010-2020年)》的通知卫疾控发〔2010〕52号各省、自治区、直辖市卫生厅局,新疆生产建设兵团卫生局:为加强梅毒预防与控制工作,依据《中华人民共和国传染病防治法》和《艾滋病防治条例》,我部制定了《中国预防与控制梅毒规划(2010-2020年)》。
现印发给你们,请认真贯彻执行。
二〇一〇年六月三日中国预防与控制梅毒规划(2010-2020年)梅毒是由梅毒螺旋体引起的一种传染病,可引起神经、心血管等多系统损害,甚至威胁生命。
梅毒可通过胎盘传染胎儿,导致自发性流产、死产或先天梅毒等。
感染梅毒可促进艾滋病的传播。
为了保障广大人民群众的身体健康,提高人口素质,有效控制艾滋病和梅毒传播,依据《传染病防治法》和《艾滋病防治条例》,制定本规划。
一、背景20世纪80年代,梅毒在我国重新出现,90年代末以来,全国梅毒报告病例数明显增加,流行呈现快速上升趋势。
1999年报告病例80406例,年发病率为6.50/10万,2009年报告病例327433例,年发病率为24.66/10万,发病率年均增长14.3%。
1997年先天梅毒报告病例数为109例,报告发病率为0.53/10万活产数,2009年报告病例数为10757例,报告发病率为64.41/10万活产数,发病率年均增长49.2%。
2009年,梅毒报告病例数在我国甲乙类传染病报告中居第三位。
高危人群梅毒感染率高,2009年艾滋病监测哨点结果表明,暗娼人群梅毒抗体阳性率最高达30.6%,平均为2.4%;男男性行为人群最高达31.2%,平均为9.1%;吸毒人群最高达27.9%,平均为3.4%;孕产妇人群梅毒抗体阳性率最高达11.3%,平均为0.5%。
梅毒可通过性、血液和母婴途径传播,传播途径与艾滋病基本一致,感染梅毒后只要及早发现并进行规范治疗是可以治愈的。
目前,我国梅毒流行的危险因素广泛存在,部分人群存在卖淫嫖娼、婚前和婚外性接触、男男性接触等多性伴高危行为;宣传教育不够深入,缺乏针对性,重点人群梅毒防治知识和防范意识不高,预防干预措施覆盖面不足;部分医疗机构梅毒诊疗服务不规范、服务机制不健全、可及性不够,防治队伍能力不足。
_2010年美国疾病控制中心梅毒治疗指南

·标准·方案·指南· 【编者按】 与2006年版指南相比,2010年美国疾病控制中心性传播疾病治疗指南在梅毒、沙眼衣原体、淋病等方面疾病的实验室检查、临床诊断及药物治疗等方面有了部分变动,本刊特邀北京大学深圳医院樊尚荣等专家对新版指南中的变动内容进行深入解读,连续刊出,以期为临床诊治提供依据。
2010年美国疾病控制中心梅毒治疗指南樊尚荣,李健玲(编译) 译者单位:518036广东省深圳市,北京大学深圳医院妇产科(樊尚荣);汕头大学医学院(李健玲) 【关键词】 梅毒;指南;诊断;治疗 【中图分类号】R 759.1 【文献标识码】A 【文章编号】1007-9572(2011)02-0461-031 概述1.1 分期 梅毒是由梅毒螺旋体引起的一种全身性疾病,根据传播途径不同分为后天梅毒与先天梅毒。
又可根据其病期分为早期梅毒与晚期梅毒。
(1)早期梅毒:病期在2年以内。
包括:①一期梅毒(硬下疳);②二期梅毒(全身皮疹);③早期潜伏梅毒(感染1年内)。
(2)晚期梅毒:包括:①皮肤、黏膜、骨、眼等梅毒;②心血管梅毒;③神经梅毒;④内脏梅毒;⑤晚期潜伏梅毒。
1.2 诊断1.2.1 螺旋体检查 取病损分泌物做涂片,用暗视野检查或直接免疫荧光检查(D F A )活螺旋体,阳性者即可确诊。
1.2.2 血清学试验 包括非螺旋体试验和螺旋体试验。
非螺旋体试验包括快速血浆反应素试验(R P R )或性病研究试验(V D R L );螺旋体试验包括荧光螺旋体抗体吸附试验(F T A-A B S )及梅毒螺旋体明胶凝集试验(T P P A )。
非螺旋体试验存在假阳性,见于多种与梅毒无关的临床状态,包括自身免疫状况、高龄以及注射毒品者。
非螺旋体试验滴度可用于评价治疗效果。
同一实验室同一方法两次检测相差2个倍比稀释度(4倍)有意义。
1.2.3 脑脊液检查 包括脑脊液细胞计数(白细胞>5/m m 3)、蛋白测定异常和V D R L 。
梅毒诊断和报告标准

一期梅毒的诊断条件
A.流行病学史 有多性伴,不安全性行为,或性伴有梅毒感
染史。 B.临床表现:
硬下疳:潜伏期一般为2~4周。一般为单发, 但也可多发;直径约1cm~2cm,圆形或椭圆形浅 在性溃疡,界限清楚、边缘略隆起,疮面清洁; 触诊基底坚实、浸润明显,呈软骨样的硬度;无 明显疼痛或触痛。多见于外生殖器部位。 (诊断要 点:硬下疳)
3.既往有梅毒病史,经过长效青霉素规范治疗,且通过足 够时间随访后判为治愈者,本次就诊时明确有新的性接触史 而再次感染,出现二期梅毒皮损表现,在本医疗机构被诊断 的
4.既往有生殖器部位溃疡(硬下疳)病史,但未被诊断为 一期梅毒,经病情发展后出现皮损被诊断为二期梅毒的。
5.既往被诊断为一期梅毒,经过治疗,但治疗不恰当,而 出现二期梅毒皮损,诊断为二期梅毒的。
2.如果就诊病例生殖器部位有溃疡表现(疑似硬下 疳),非梅毒螺旋体抗原血清试验阳性,而梅毒螺旋体 抗原血清试验阴性,此时,需要再次进行梅毒螺旋体抗 原血清试验,或在不同试验室进行检测,以防技术性假 阴性;或进行随访复诊,间隔一定时间(如1~4 周)后 再次检测。如果多次梅毒螺旋体抗原血清试验阴性,或 间隔一定时间开展梅毒螺旋体抗原血清检测结果仍为阴 性,在没有治疗的情况下,可排除梅毒感染。
害状况,不具确诊作用;通过检测滴度评估治疗效果, 不能依据滴度对梅毒进行诊断,认为滴度高(1:8以上) 就是梅毒,滴度低(1:8以下)就不是梅毒。
梅毒血清检测方法
梅毒的血清学检测项目 二、梅毒螺旋体抗原血清试验(特异性试验)包括: TPPA:梅毒螺旋体颗粒凝集试验(金标准) TPHA:梅毒螺旋体血凝试验 FTA-ABS:荧光螺旋体抗体吸收(试验) TP-ELISA:梅毒螺旋体酶联免疫吸附试验 意义: ----检测梅毒特异性抗体; ----如果阳性,表明曾经感染过梅毒,但无法识别是过去感染,还
揭秘人类医疗史上最黑暗的实验
揭秘人类医疗史上最黑暗的实验作者:来源:《新传奇》2017年第21期这几天,美国一个沉寂已久的案子又被翻了出来。
那是医学史上最恶名昭著的一个实验。
整整二十年前,时任美国总统克林顿代表美国政府为这个实验向受害者正式道歉。
如今,当事人业已逝去,但相关的诉讼仍未彻底结束,有些赔偿金仍然躺在法院控制的账户里,而当事人的子孙们依然被那段黑暗的历史纠缠……那个实验,就是塔斯基吉梅毒实验。
起因塔斯基吉位于美国东南部,是阿拉巴马州的一个贫穷小城。
当时梅毒正在贫困的黑人居住地流行,35%的育龄居民患有梅毒。
1932年起,美国公共卫生部在那里启动了一项人体试验,计划观察男性黑人梅毒患者在未经治疗的情况下,疾病会如何发展。
梅毒是种可怕的疾病。
到了发病期,病人会出现许多红疹,全身器官如神经、心脏、骨骼都会受累,可能的后果包括失明、耳聋、神经失常、心脏衰竭乃至死亡。
梅毒会通过性行为传给伴侣;母亲在怀孕分娩时也会传给孩子,导致先天性梅毒。
眼睁睁看着梅毒患者病情发展却不予治疗,这样的实验计划怎么会通过呢?在1932年,梅毒的特效疗法还未出现,当时治疗方案是用砷,但效果并不太好。
其次,研究者用“这个试验计划并不会对那些黑人造成伤害,反正本来以他们的经济和知识水平,就不太可能得到有效的梅毒治疗”这样的理由说服了自己。
最开始的实验计划没那么丧心病狂,最初主持研究的克拉克医生计划是“先观察6-9个月,然后就给予治疗”。
但开始执行后,这个实验就慢慢变了。
诱骗第一个变化,是研究者们蓄意隐瞒了实验目的,并且用谎言(比如不存在的“治疗”)来诱骗黑人们与之长期合作。
他们告诉黑人们自己提供“免费体检,免费治疗‘坏血病’”——当地人因为医学知识不足,将梅毒、贫血、疲劳等都以为是“坏血病”,研究者则利用了他们的无知。
同时,研究者还提供一些小福利,比如免费饭菜,免费乘车来往诊所,免费治疗一些其他小病,偶尔还送一点现金和小礼品。
这样的条件当然吸引了不少当地人。
梅毒的诊断标准
(实验室诊断病例)
同上
同上
暗视野检查阳性;
或梅毒螺旋体抗原血清试验阳性,非梅毒螺旋体抗原血清试验阳性;
二期梅毒
疑似病例
性接触史,或性伴感染史
二期梅毒皮疹
非梅毒螺旋体抗原血清试验阳性
确诊病例
(实验室诊断病例)
同上
同上
暗视野检查阳性;
或梅毒螺旋体抗原血清试验阳性,非梅毒螺旋体抗原血清试验阳性
三期梅毒
应取婴儿静脉血进行检测,而不是脐带血
确诊病例
(实验室诊断病例)
同上
同上
暗视野检查阳性;
梅毒螺旋体抗原血清试验阳性,非梅毒螺旋体抗原血清试验阳性,其抗体滴度高于生母4倍及以上,但低于该值并不排除胎传梅毒,或出生后3个月随访滴度升高。
应取婴儿静脉血进行检测,而不是脐带血
1.梅毒螺旋体抗原血清试验包括TPPA、ELISA、快速免疫层析法等;非梅毒螺旋体抗原血清试验包括RPR、TRUST、VDRL等。
1、梅毒
梅毒诊断要点:
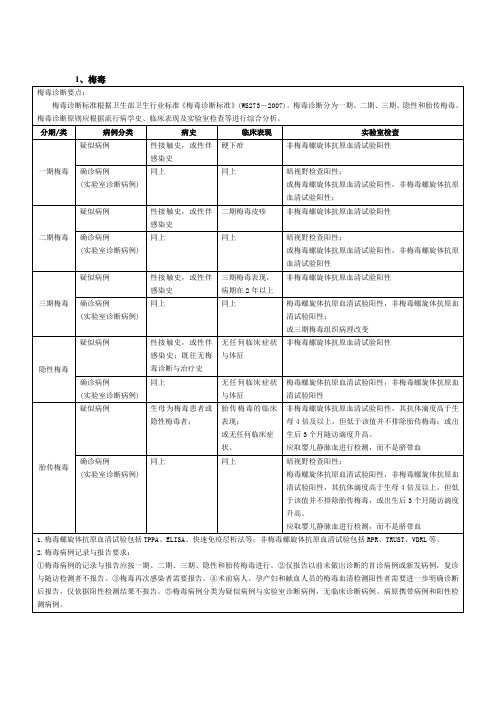
梅毒诊断标准根据卫生部卫生行业标准《梅毒诊断标准》(WS273-2007)。梅毒诊断分为一期、二期、三期、隐性和胎传梅毒。梅毒诊断原则应根据流行病学史、临床表现及实验室检查等进行综合分析。
分期/类
病例分类
病史
临床表现
实验室检查
一期梅毒
疑似病例
性接触史,或性伴感染史
硬下疳
非梅毒螺旋体抗原血清试验阳性
确诊病例
(实验室诊断病例)
同上
无任何临床症状与体征
梅毒螺旋体抗原血清试验阳性,非梅毒螺旋体抗原血清试验阳性
胎传梅毒
疑似病例
生母为梅毒患者或隐性梅毒者;
胎传梅毒的临床表现;
健康资讯:美国梅毒恐慌梅毒的传播途径
健康资讯:美国梅毒恐慌梅毒的传播途径
梅毒的传播途径
梅毒病人是唯一的传染源。
性接触传染占95%。
主要通过性交由破损处传染,梅毒螺旋体大量存在于皮肤粘膜损害表面,也见于唾液、乳汁、精液、尿液中。
未经治疗的病人在感染一年内最具传染性,随病期延长,传染性越来越小,病期超过4年者,通过性接触无传染性。
亦可通过干燥的皮肤和完整的粘膜而侵入。
少数可通过接吻、哺乳等密切接触而传染,但必须在接触部位附有梅毒螺旋体。
由于梅毒螺旋体为厌氧性,体外不易生存,且对干燥极为敏感,故通过各种器物的间接传染,可能性极少。
输血时如供血者为梅毒患者可传染于受血者。
先天梅毒是患有梅毒的孕妇通过胎盘血行而传染给胎儿。
一般在妊娠前四个月,由于滋养体的保护作用,梅毒螺旋体不能通过,故妊娠前四个月胎儿不被感染,以后滋养体萎缩,梅毒螺旋体即可通过胎盘进入胎儿体内传染胎儿。
梅毒的概述
梅毒是由苍白螺旋体即梅毒螺旋体引起的一种慢性性传播疾病。
可以侵犯皮肤、粘膜及其他多种组织器官,可有多种多样的临床表现,病程中有时呈无症状的潜伏状态。
病原体可以通过胎盘传染给胎儿而发生胎传梅毒。
1。
梅毒职业暴露的处置与防护PPT课件
暴露后随访至少6个月(分别于6 周、12周、6月重复检查) ,若合并 有HIV、HCV等感染的可延长随访至 12个月。在随访期间特别是在头6周 到12周,应防止性传播。避免怀孕, 献血,捐赠器官、组织及精子等,若 有哺乳的,应劝告哺乳可能会传播梅 毒。
霉素G,根据分期和临床表现决定剂型、 剂量和疗程。 (1)一期梅毒、二期梅毒 成人推荐方案:苄星青霉素,240 万 u,单次,肌肉注射。新生儿及儿童 推荐方案:苄星青霉素,5 万u/kg,最 大剂量240万 u,单次,肌肉注射。 在治疗后第 6个月、第12 个月进 行非螺旋体试验评价疗效。
3、血清学检查
(1) 梅毒螺旋体抗体检测磁微粒化学发光法(CLIA) 本方法可进行自动化操作,常作为梅毒的筛查检测,其筛查阳性标 本需进一步进行复检,确证是否为梅毒现症感染者。 (2) 梅毒甲苯胺红不加热血清试验(TRUST) 梅毒螺旋体感染人体后产生抗类脂抗原的抗体,未经治疗可长期存 在,治疗后逐渐减少至转为阴性。一期约1年转阴,二期约2年转阴,晚 期2年后约50%病人仍为阳性,该结果可用于现症梅毒诊断及用于疗效观 察及判愈。 (3)梅毒螺旋体颗粒凝集试验(TPPA) 梅毒螺旋体感染人体后2-4周可检测到抗梅毒螺旋体抗体,此抗体特 异性高,达98%以上,检测到梅毒螺旋体抗体阳性可确证为现在或既往 有过梅毒螺旋体感染。一般该抗体能保持终生,所以该项检测不能作为 疗效观察的指标。
业暴露伤情登记表,科主任或护士长 确认。 (3)评估 报院感科登记备案,查看暴露源 (患者)的相关检验报告(3个月内结 果有效)及病史(包括特殊人群和危 险行为等),到检验科做血清学检测, 进行风险评估。
染的最后一个环节,预防用药越早越好。
首选治疗药物为青霉素 G。推荐方 案: 苄星青霉素,240万 u,单次,肌 肉注射。 青霉素过敏者。多西霉素100mg, 口服,2次/d,连续14d;四环素 500mg,4 次/d,口服,连续14d;头 孢曲松1-2g,1次/d,肌肉注射或静脉滴 注,连续10-14d。
塔斯基吉梅毒实验

塔斯基吉梅毒实验塔斯基吉梅毒实验塔斯基吉梅毒实验是美国公共卫⽣部⾃1932年起授权塔斯基吉研究所启动的⼀项⼈体试验,其全称为“针对未经治疗的男性⿊⼈梅毒患者的实验”。
在这项实验中,医⽣们以免费体检、免费治疗所谓“坏⾎病”、免费提供丧葬保险等条件,吸引当地400余名⿊⼈男⼦在不清楚实验真正⽬的的情况下加⼊该“实验计划”。
秘密研究梅毒对⼈体的危害。
当事⼈被隐瞒长达40年,⼤批受害⼈及其亲属付出了健康乃⾄⽣命的代价。
塔斯基吉梅毒实验 - 简介塔斯基吉梅毒实验1932年,美国公共卫⽣署开始了⼀项为期6个⽉的研究,其⽬的是要去观察⿊⼈男性中潜伏着的梅毒的作⽤。
这项研究的成功取决于对受试者提供虚假的“治疗”以确保他们的合作。
当这⼀研究结束后,研究⼈员⼜申请了⼀项更长的后续研究,通过对受试者进⾏⼫体解剖来证实他们的临床观察。
这⼀过程进⾏到1972年,直到实验报告被泄漏给了新闻界,美国健康、教育和福利部门随之中⽌了这⼀研究,公共卫⽣部门对实验对象隐瞒真相长达40年,使⼤批受害⼈及其亲属付出了健康乃⾄⽣命的代价,这就是塔斯基吉梅毒实验。
“塔斯基吉梅毒实验”的领衔研究⼈员是从事危地马拉秘密⼈体实验的医⽣约翰·卡特勒。
卡特勒1985年以教授⾝份从匹兹堡⼤学退休,2003年去世。
韦尔斯利学院医学史学家苏珊·⾥维尔⽐在梳理“塔斯基吉梅毒实验”相关资料时,发现了危地马拉秘密⼈体实验事件。
塔斯基吉梅毒实验 - 实验对象据受害⼈欧内斯特·亨登回忆,在亚拉巴马州梅肯县,医疗条件极为恶劣,当地⼈当时将梅毒症状、贫⾎症状以及⾝体疲劳等症状⼀律称为“坏⾎病”。
1932年的⼀天,⼀辆满载医⽣的客车来到该地,医⽣们以免费体检、免费治疗所谓“坏⾎病”、免费提供丧葬保险等条件,吸引当地的⿊⼈男⼦们加⼊⼀项“治疗计划”。
当地近400名感染梅毒的⾮洲裔穷苦⿊⼈被免费治疗的机会打动,在不清楚“治疗计划”的真正⽬的的情况下,成为“塔斯基吉梅毒实验”的“志愿者”。
健康资讯:美国梅毒恐慌梅毒的早期症状图片

健康资讯:美国梅毒恐慌梅毒的早期症状图片梅毒的早期症状图片梅毒:由苍白螺旋体引起的传染病.主要通过性交传染,是性传播疾病.分3期:①一期梅毒.即硬下疳,潜伏期2~4周,外生殖器部位发生暗红色硬肿块,浅溃疡,有软骨样硬度,周围淋巴结肿大.②二期梅毒.在一期梅毒1~2个月之后,全身皮肤,粘膜发生对称泛发皮疹,斑疹,丘疹,脓疱疹等.粘膜可发生粘膜斑,扁平湿疣,传染性强.③三期梅毒.发生在感染后2~3年乃至10年,皮肤为树胶样肿,还可涉及骨,关节,心,血管,表现为主动脉炎,主动脉瓣闭锁不全和主动脉瘤等,侵及神经为脊髓痨,全身麻痹(麻痹性痴呆).先天梅毒有早期先天梅毒,相当于后天二期,但较重.晚期先天梅毒与后天相似,但很少发生心,血管及神经病变.主要为实质性角膜炎,神经性耳聋,哈钦森氏齿(上门齿中央切痕,下小上大,宽厚相等),佩刀形胫骨等.各期之间可有潜伏梅毒,无症状,仅血清反应阳性.治疗使用青霉素或红霉素,四环素等.意见建议:早期梅毒又称一期梅毒!发生在感染后3周后,在感染处出现一个硬的,无痛性的圆形结节.开始潮红,湿润,渐渐破溃,糜烂,形成溃疡,即一期梅毒硬下疳.其主要损害为硬下疳,是梅毒螺旋体最初侵入之处,并在此繁殖所致.典型的硬下疳为一无痛性红色硬结,触之硬如软骨样,基底清洁,表面糜烂覆以少许渗液或薄痂,边缘整齐.损害数目大都为单个,亦可为多个.好发生于外生殖器.男性多发生于阴茎的包皮,冠状沟,龟头或系带上.同性恋男性常发生于肛门直肠部.女性好发生于大小阴唇内侧部位,也可发生于子宫颈等处.同时双侧腹股沟淋巴结肿大,但不痛.通过接吻感染者,硬下疳可发生于唇,下颌部和舌等部位,也可发生于眼睑,手指和乳房等处,有时硬下疳未愈合前可同时伴发其他性病,如淋菌性皮炎.一期梅毒的硬下疳内有很多梅螺旋体,常伴有局部淋巴结肿大.传染性很强.硬下疳持续2?6周后便自行消退而不留瘢痕.但因女性下疳发生的部位较隐蔽,又无症状,常被忽视而增加了传播的机会.一期梅毒如不治疗或治疗不当,螺旋体经血行及淋巴结播散到全身,数周后即发展成二期梅毒.。
梅毒血清学试验的若干个问题
梅毒血清学试验的若干个问题1.国内梅毒血清学试验的传统程序是:先以非梅毒螺旋体抗原血清试验(如RPR、TRUST、VDRL等)进行初筛,再以梅毒螺旋体抗原血清试验(如TPPA、TPHA、FTA-ABS等)进行确认。
美国、法国和比利时也采用类似的程序。
该程序的优点是排除了大多数感染过梅毒但经过充分治疗的病人,从而使临床更易决定是否需要进行抗梅治疗。
但该程序也存在明显的缺陷。
一方面非梅毒螺旋体抗原血清试验易出现前带现象,使早期梅毒及合并感染HIV时高滴度的血清样品呈现假阴性反应;另一方面,对于一期梅毒早期、隐性梅毒,尤其是晚期梅毒,非梅毒螺旋体抗原血清试验缺乏足够的敏感性。
因此,仅以RPR或TRUST进行初筛,会造成相当比例的漏检,这不符合初筛方法高敏感性的要求。
近年来,美国已将梅毒螺旋体抗原血清试验(TPPA)引入到血站系统的初筛检测中,临床上仅以非梅毒螺旋体抗原血清试验作为筛查的状况也在逐渐改变。
2.将梅毒螺旋体抗原血清试验和非梅毒螺旋体抗原血清试验组合在一起(如RPR+TPHA或TPPA)作为初筛试验可以最大限度地检出各期梅毒病例(除一期梅毒的极早期),同时保证了敏感性和特异性,是最为理想的梅毒初筛方案。
这是世界卫生组织(WHO)推荐的方案,英国等一些欧洲国家也已采用多年。
其缺点是费时费力,实验室的工作量较大。
3.在德国和荷兰等国,则仅以梅毒螺旋体抗原血清试验作为初筛方法,这比仅以非梅毒螺旋体抗原血清试验进行初筛在敏感性上有了明显提高。
虽然效果略差于上述的组合方案,但工作量也相应减小。
4.梅毒的确认必须采用梅毒螺旋体抗原血清试验,最常用的是TPPA或TPHA,也可采用ELISA.FTA-ABS仍被认为是梅毒血清学测定的“金标准”,但使用上有很大限制。
多数实验室无法常规开展,因此一般只用于对有争议标本的检测。
如果仅使用非梅毒螺旋体抗原血清试验进行初筛,则可以用任意一种梅毒螺旋体抗原血清试验做确认;如果在初筛时已使用了梅毒螺旋体抗原血清试验,则可以考虑选用另一方法学的梅毒螺旋体抗原血清试验进行确认(例如在初筛时使用了TPPA或TP HA,则可用ELISA进行确认,反之亦然)。
90年代梅毒在美国的流行和预防控制
90年代梅毒在美国的流行和预防控制
房新志
【期刊名称】《国外医学:社会医学分册》
【年(卷),期】1998(015)003
【摘要】综述了90年代初期和中期梅毒在美国的流行状况,梅毒流行与地区分布,种族,性别和社会生态学因素之间的关系,以及90年代梅毒的防的预防和控制策略,强调建立社会防治网的重要性。
【总页数】4页(P109-112)
【作者】房新志
【作者单位】乌鲁木齐铁路中心医院
【正文语种】中文
【中图分类】R759.101
【相关文献】
1.严阵以待,科学防治,做好禽流感预防控制工作--访著名流行病学专家、广东省疾病预防控制中心流行病防治研究所副所长彭国文 [J], 杨德胜;王建国;周婕
2.严阵以待,科学防治,做好禽流感预防控制工作——访著名流行病学专家、广东省疾病预防控制中心流行病防治研究所副所长彭国文 [J], 杨德胜;王建国;周婕
3.20世纪90年代美国艾滋病的死亡率促进了梅毒发病率的下降 [J], 蒋法兴;苏晓红
4.美国猴痘暴发流行及预防控制 [J], 王汝宽;李海燕;于清涛
5.90年代梅毒在美国的流行和预防控制 [J], 房新志
因版权原因,仅展示原文概要,查看原文内容请购买。
梅毒检验知识科普
梅毒检验知识科普梅毒是皮肤性病科常见的疾病,是由于梅毒螺旋体感染的性传播,疾病发生对患者的身体健康以及生活质量造成重要影响,因此目前临床中已经逐渐重视关于梅毒的检验工作。
大部分人对梅毒检验均存在认知不足,因此,就由小编为大家讲解关于梅毒检验知识,希望对大家能够有所帮助。
什么是梅毒?梅毒通常为特有的慢性全身性传染疾病,在染发生初期患者通常会存在外生殖器皮肤异常,并且存在肉红色溃烂硬结节,这也被称为硬下疳,由于疾病发生初期症状并不具有特异性,但是其传染性较,因此加强梅毒检验研究,实现梅毒早发现、早治疗对于公共卫生安全以及患者疾病预后均有重要价值。
显微镜的梅毒检验梅毒螺旋体是引发梅毒性传播疾病的重要物质。
梅毒螺旋体具有透明特点并且不容易着色,患者感染后该物质进入到人体以及靶器官组织内部,因此如果在临床检验过程中,针对患者组织或者穿刺液内部发现梅毒螺旋体这种情况便可以确诊患者感染梅毒。
利用显微镜观察,梅毒螺旋体通常呈现螺旋状,并且柔软纤细,运动活泼,呈现蛇形可伸缩旋转运动,除了显微镜梅毒检验外利用,镀银染色同样可以对梅毒螺旋体进行深棕色染色,而后利用光学显微镜同样可以实现梅毒检验。
特异性抗体检验①梅毒螺旋体重组抗原同样被应用于梅毒检验过程中,其检验原理利用特异性抗体检测进行疾病诊断。
常见的诊断方法包含化学发光法,电化学发光法以及酶联免疫吸附实验,重组抗原以及血清中的梅毒螺旋体抗体以及具有标志物的重组抗原这三种物质形成复合物,当环境发生改变后,复合物的标记物会存在光信号这种情况,如果光信号越强,则说明梅毒螺旋体抗体越多。
②梅毒螺旋体的菌体也可以实现梅毒检验。
这种检验方法包括TPPA试验和TPHA试验,梅毒螺旋体会和血清中特异性抗体进行凝集反应,如果凝集反应呈现纽扣状并且颜色为红色,这种情况说明患者为阴性不存在梅毒;如果检验过程中凝集较为杂乱,则证明患者为阳性,存在梅毒感染。
③磷脂类物质也能够对非特异性反应素进行检测,这种检测方法包括TRUST试验和RPR试验,其原理是通过将血清中反应素与磷脂类物质相接触产生凝集反应。
梅毒难根治吗!FDA基因疗法轻松灭梅毒
梅毒难根治吗!FDA基因疗法轻松灭梅毒
梅毒难以根治是世界公认的治疗难题,50%以上的患者受到过复发的困扰。
该疾病复发的主要原因在于治疗不彻底、不全面,因为除了肉眼能够看到的显性梅毒外,在梅毒周围和深处还存在许多肉眼看不到的病毒感染病灶,隐形感染病灶很难直接进行治疗,成为日后复发根源。
但随着我国FDA基因疗法在临床的推广运用,使得彻底根治一期梅毒、二期梅毒等皮肤病病成为了现实。
2011年,湖南性保健研究所附属医院代表中国性病医学界接受了联合国医疗新技术临床运用审核,其“FDA基因疗法”荣获“国际医疗技术新突破提名奖”,成为仅次于干细胞移植的高新技术成果。
截止2012年,该技术在全球的治愈人数达到50多万人,在全国推广取得了初步成效,国家卫生部正式批准该技术作为国家性病对外交流唯一指定技术。
据湖南性保健研究所附属医院负责人介绍,FDA基因疗法之所以能彻底解决各种顽固性生殖器梅毒,其根本原因在于找到了梅毒的基因原始抗原。
“FDA基因疗法”的治疗原理:第一步:强效杀菌:采用独有的药物因子超强渗透,能直达病灶,快速准确地识别病毒或病
菌,对潜伏在体内血液、皮肤基底层、生发层细胞和神经节内的病毒或病菌进行杀灭。
第二步:全面排毒:通过新陈代谢排出病毒及DNA 残片,防止残片重组。
第三步:系统修复:快速修复病变的组织和受损细胞,消除代谢障碍,纠正免疫缺陷,恢复机体功能。
第四步:激活免疫:刺激机体产生保护性免疫来防止病毒再感染,杜绝病毒复发,四维一体,环环相扣,既系统又全面地杀灭HPV和HSV病毒疗程短、见效快,避免复发。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
S YPHILIS______________________________________________________________________________I.I NTRODUCTIONSince 2001, rates of primary and secondary syphilis have increased annually in the United States,1 especially among HIV-infected men who have sex with men (MSM).2 In the setting of underlying HIV infection, atypical presentations of early syphilis, rapid progression to tertiary syphilis, treatment failures, and more frequent cases of neurosyphilis have been reported. Despite the number of reports of unusual features, the presentation and management of syphilis in the majority of patients co-infected with HIV is similar to that in non-HIV-infected patients.II.P REVENTIONR ECOMMENDATIONS:Clinicians should counsel HIV-infected patients about the risk of acquiring syphilis and other STIs from unprotected sexual contact, including all sites of possible transmission, such as anus, cervix, vagina, urethra, and oropharynx. (AIII)When HIV-infected patients are diagnosed with early syphilis (primary, secondary, or early latent), clinicians should intensify risk-reduction counseling, including discussions about the importance of condom use. (AIII)Syphilis and other STIs are primarily transmitted by unprotected sexual contact involving genital, rectal, or oral mucosal surfaces. Patients should be counseled about the risk of acquiring syphilis at all sites of possible exposure. Oral sex is a route of transmission of syphilis that many individuals often do not consider.3Genital ulcer disease has been associated with an increased risk of HIV transmission.4-6 Ulcers (HSV, syphilis, and chancroid) directly increase the likelihood that genital secretions will contain an infectious amount of HIV-1. This increases the potential for contact between HIV-1 in these secretions with genital mucosal cells receptive to HIV-1 infection. When genital ulcerative disease is present, clinicians should intensify risk-reduction counseling.Clinicians who are uncomfortable discussing sexual behaviors and STI transmission risk can seek training to enhance their comfort level and to develop a nonjudgmental approach to educating patients about the importance of STI screening. For information regarding risk-reduction counseling related to sexual transmission, refer to the HIV PreventionGuidelines: Prevention with Positives: Integrating HIV Prevention into HIV Primary Care. Training in STI prevention and counseling is also available through the HIV Clinical Education Initiative and the Region II STD/HIV Prevention Training Center.III.S CREENING AND R EPORTINGR ECOMMENDATIONS:As part of the annual comprehensive physical examination, clinicians should examine all skin surfaces for lesions, especially in less visible areas such as the anus, cervix, vagina, urethra, and oropharynx, as well as under the foreskin in uncircumcised males. (AIII) Clinicians should:•Obtain serologic screening for syphilis at least annually for HIV-infected patients, and every 4 months for patients with continued high-risk behavior (AII)•Obtain confirmatory testing if the initial screen is reactive (AII)•Be familiar with their referring laboratory’s syphilis screening algorithm (AIII) Clinicians should perform a nontreponemal test, such as the RPR or VDRL, for repeat screening in HIV-infected patients with a history of syphilis infection; the same nontreponemal reagin test should be used when performing repeat screening and when following response to treatment in these patients. (AII)Clinicians must report all suspected or confirmed syphilis diagnoses to the local health department of the area where the patient resides according to NYS requirements (also see reportable communicable diseases).HIV-infected patients should be screened for syphilis at least once per year. Patients with continued high-risk behavior should be screened for syphilis every 4 months. Factors that may prompt more frequent screening include multiple or anonymous sex partners, past history of STIs, high prevalence of STIs in the area or patient population, life changes that may lead to risky behaviors, or sex or needle-sharing partners with any of these risks.Because the chancres of primary syphilis are usually painless, it is important that the clinician perform a careful physical examination, especially in less visible areas such as the anus, cervix, vagina, urethra, and oropharynx, as well as under the foreskin in uncircumcised males.Traditionally, the screening algorithm for syphilis has used a nontreponemal screening test (i.e., RPR or VDRL), followed by a confirmatory test for treponemal antigen (i.e., FTA-Abs or TP-PA). However, some municipalities with a high volume of syphilis testing, including some laboratories in New York City, have begun to use a reverse-sequence screening algorithm with an automated treponemal EIA or CIA as the initial screening test, followed by confirmation with the nontreponemal RPR. When discordant results are provided by laboratories using the alternative algorithm (i.e., reactive EIA/ELISA with a non-reactive RPR), the CDC recommends a confirmatory TP-PA test to exclude very early syphilis or previously untreated syphilis infection.7Information regarding a given laboratory’s screening algorithm may not be immediately available. Clinicians should request information regarding the screening algorithm of their referring laboratory and be familiar with the testing sequence used.For most individuals with a history of syphilis infection, the FTA-Abs, TP-PA, ELISA, and EIA tests remain positive for life, and some individuals previously treated for syphilis will continue to have a low positive serum RPR or VDRL (i.e., “serofast” syphilis). A 4-fold or greater increase in serum RPR or VDRL indicates treatment failure or re-infection with syphilis. The same nontreponemal reagin test should be used for both repeat screening and following the response to treatment in these patients.Prompt reporting of suspected or confirmed syphilis is mandated under the New York State Sanitary Code (10NYCRR 2.10). The following cases should be reported by phone to the local health department:•Any nontreponemal test >1:16•Any positive primary or secondary stage disease•Any positive prenatal or delivery test, regardless of serum reagin levelAll other cases may be reported by mail. The local health department may contact the patient for epidemiological investigation or to offer assistance with partner notification. More information regarding communicable disease reporting requirements is available at the following sites: •New York State: /professionals/diseases/reporting/communicable/•New York City: /html/doh/html/hcp/hcp-reporting.shtmlClinicians can contact local health departments to obtain previously reported nontreponemal and treponemal test results. See Appendix A for the contact information of the STI coordinator for each of the local health departments in New York State.IV.P RESENTATIONSyphilis is classified into four stages: primary, secondary, latent, and tertiary. Lesions of primary syphilis usually develop following an incubation period of 10 to 90 days (usually 3 weeks). Primary lesions usually last 3 weeks and resolve without treatment. The onset of secondary syphilis occurs from 2 weeks to 6 months after the resolution of the primary stage (usually 4 weeks). Secondary symptoms usually last 4 weeks, and like primary symptoms, resolve without treatment. Latent syphilis may persist for up to 50 years after infection. Latent infection is divided into early latent (<1 year since infection) and late latent (≥1 year after infection). Duringearly latent infection, relapse of secondary syphilis and subsequent transmission to sexual partners are possible. Tertiary syphilis refers to clinical manifestations occurring after the latent stage (range, 2-50 years after latency). Typically, tertiary syphilis is divided by organ system involvement into gummatous syphilis, cardiovascular syphilis, and neurologic syphilis.Most HIV-infected patients present similarly to non-HIV-infected patients, although some key features exist. Table 1 summarizes the usual clinical presentation of syphilis in the non-HIV-infected population and the reports of atypical manifestations described in HIV-infected individuals. Appendix B shows photographic examples of secondary syphilis in HIV-infected patients.V.D IAGNOSISR ECOMMENDATIONS:Clinicians should include syphilis as part of the differential diagnosis for HIV-infected patients presenting with oral, genital, cervical, or anal lesions, as well as for patients presenting with rash, eye disease, or neurologic disease. Definitive diagnosis is made either by identification of the organism or serologically. (AIII)Clinicians should perform a baseline neurologic examination for all HIV-infected patients diagnosed with syphilis and should educate patients about the signs and symptoms of neurosyphilis. (AIII)When there is clinical suspicion for syphilis in an HIV-infected patient, but the nontreponemal test result is negative, clinicians should order laboratory dilution and retesting of the sample. (AII)A. Identification of T. pallidum (Lesion-Based Testing)Direct Fluorescent Antibody Test (DFA)A direct fluorescent antibody test can be performed on lesion exudate or tissue specimen. There are no differences in test performance characteristics among HIV-infected and non-HIV-infected patients.Darkfield MicroscopyExamination of exudate from an ulcer base or a mucocutaneous lesion under darkfield microscopy can identify the spirochete (T. pallidum). This test is invalid for oral samples and is typically available only in specialized centers (consult with your local health department for availability; see Appendix A). There are no differences in test performance characteristics among HIV-infected and non-HIV-infected patients.Silver StainSpirochetes may be seen in biopsy specimens of suspicious lesions such as palmar macular rash or gummatous lesions. There are no differences in test performance characteristics among HIV-infected and non-HIV-infected patients.B. SerologyA diagnosis of syphilis is possible with the use of two diagnostic tests: a nontreponemal reagin test and, if positive, a confirmatory specific treponemal antibody test. Some clinical laboratories and blood banks use treponemal syphilis IgG ELISA or EIA tests with verification by nontreponemal tests.Nontreponemal TestsRPR (rapid plasma reagin) or VDRL (venereal disease research laboratory) are non-specific quantitative tests that result from the cross-reaction of human cardiolipin-lecithin in syphilis infection. The tests correlate with disease activity and are used to follow the clinical course and determine the effectiveness of treatment. If reactive during primary syphilis, the nontreponemal tests usually become positive approximately 7-10 days after the onset of the chancre. Because the nontreponemal tests are positive in only 80% of cases presenting with chancre (i.e., primary ulcer), patients presenting with chancre who test negative according to nontreponemal tests should receive treatment.The sensitivity of these tests is near 100% during secondary syphilis. Serum reagin levels are typically low (<1:16) in primary syphilis and higher (>1:32) in secondary syphilis; serum reagin levels are variable thereafter and may serorevert to negative in approximately 25% of untreated patients (usually 2 years following the infection). Serum samples containing large amounts ofnontreponemal reagin occasionally demonstrate a false-negative reaction, known as a prozone reaction.26 When there is clinical suspicion for syphilis, but the nontreponemal test result is negative, clinicians should order laboratory dilution and retesting of the sample. Nontreponemal tests may be positive in the setting of medical conditions other than syphilis, including HIV infection, collagen vascular disease, narcotic drug use, advanced age, pregnancy, chronic liver disease, and some viral infections, such as Epstein-Barr virus, and other chronic inflammatory conditions (i.e., biological false-positive nontreponemal test).Treponemal TestsThe FTA-Abs (fluorescent treponemal antibody test), TP-PA (T. pallidum particle agglutination), and syphilis IgG ELISA or EIA tests are treponemal assays that measure antibody to surface protein of T. pallidum. The treponemal tests are more specific than nontreponemal tests and become reactive approximately 7 to 10 days after the appearance of the chancre. A treponemal test should be explicitly ordered during primary infection. Treponemal tests do not correlate with disease activity and remain positive for life in approximately 80% of patients, even after effective treatment.C. Diagnosis of NeurosyphilisR ECOMMENDATIONS:Clinicians should include neurosyphilis in the differential diagnosis of all HIV-infected patients who present with neurologic symptoms. (AII)Clinicians should perform a lumbar puncture in HIV-infected patients with syphilis or history of syphilis in the following cases (AII):•Neurologic or ophthalmologic signs or symptoms are present, including unexplained change in mental status•Evidence of treatment failure (as defined in Table 2 footnote)•Evidence of active tertiary syphilis (aortitis, gummas)The diagnosis of neurosyphilis requires examination of the CSF. Neurosyphilis is definitively diagnosed when a CSF VDRL is reactive. In patients who have serologic evidence of syphilis and CSF pleocytosis and/or elevated CSF protein, neurosyphilis can be presumptively diagnosed even when the CSF VDRL is non-reactive. Non-specific CSF abnormalities, such as pleocytosis or increased protein, may be found in HIV-infected patients due to the HIV infection itself or other HIV-associated conditions, making the results of CSF VDRL-negative examinations difficult to interpret. Due to the high sensitivity of FTA-Abs and TP-PA in CSF, negative FTA-Abs or TP-PA results may be useful to exclude the possibility of neurosyphilis.32,33Central nervous system involvement can occur at any stage of syphilis. Neurologic signs and symptoms, including, but not limited to, meningitis, ophthalmologic, or otologic abnormalities, warrant examination of the CSF, regardless of stage of syphilis. Patients may also present with change in mental status, such as the onset of acute psychiatric symptoms. Any evidence of tertiary syphilis or treatment failure is also an indication for CSF examination.Detection of the organism in the CSF in early syphilis is not more common in HIV-infected patients, does not correlate with subsequent development of neurosyphilis, and is not linked to serologically defined treatment failure. For these reasons, most experts do not recommend routine CSF examination for HIV-infected patients with early syphilis who do not present with neurologic symptoms. Most reported cases of neurologic syphilis in HIV-infected patients have been in patients with high serum reagin levels (>1:32)34,35; therefore, some clinicians would perform early lumbar puncture in this setting rather than waiting 12 months to document a 4-fold decrease in serum reagin levels. Similarly, some clinicians would examine CSF in HIV-infected patients with previously treated syphilis who remain serofast with high serum reagin levels(>1:32) after re-infection has been excluded. Consultation with an infectious diseases specialist is recommended when the diagnosis of neurosyphilis is being considered in patients with high serum reagin levels that fail to decline within the first 12 months or patients who were previously treated for syphilis and then present with high serum reagin levels (BIII).One study examined CSF results in 326 patients with syphilis. HIV-infected patients with syphilis who had an RPR serum reagin level >1:32 and a CD4 count <350 cells/mm3 were more likely to have neurosyphilis.34 Some experts recommend CSF examination for all HIV-infected patients with syphilis regardless of syphilis stage when serum RPR is >1:32 or CD4 count is<350 cells/mm3.VI.T REATMENT AND F OLLOW-U PR ECOMMENDATIONS:Clinicians should obtain baseline serum nontreponemal reagin level before or at the time of initial treatment for syphilis in order to monitor treatment response. (AI)Clinicians should treat HIV-infected patients for primary syphilis if they present with a chancre even in the setting of a preliminary negative nontreponemal screening test. (AI)Clinicians should use long-acting benzathine penicillin G as the preferred treatment for HIV-infected patients with syphilis. Clinicians should ensure that the proper formulations and dosages of penicillin are used. Preparations of long-acting benzathine penicillin G and dosing regimens vary by stage of syphilis and are outlined in Table 2. (AI)Detailed treatment and follow-up recommendations for HIV-infected patients with syphilis are presented in Table 2. Penicillin is the drug of choice, and recommendations for treatment vary by stage. There are no differences in recommended penicillin regimens for HIV-infected patients compared with non-HIV-infected patients. There have been instances in which the incorrect pharmaceutical preparation of penicillin has been used; clinicians should ensure that long-acting benzathine penicillin G (i.e., Bicillin LA and not Bicillin CR) is ordered.HIV-infected patients with syphilis should be followed closely. Follow-up is largely serologic and varies by stage (see Table 2).A. Treating Syphilis in HIV-Infected Patients With Penicillin AllergyR ECOMMENDATIONS:Clinicians should consult with an expert in infectious diseases and provide close follow-up if non-penicillin regimens are used to treat syphilis in penicillin-allergic, HIV-infected patients. (AIII)Penicillin desensitization followed by penicillin therapy is the treatment of choice for neurosyphilis and other forms of tertiary syphilis. (AII)Clinicians should desensitize penicillin-allergic, HIV-infected patients and treat with penicillin, rather than attempt alternate therapies, if adherence to therapy or close follow-up cannot be ensured. (AIII)Alternate treatment options for HIV-infected patients with penicillin allergy have not been well studied. Non-penicillin therapies should be used with caution and only in consultation with an expert in infectious diseases. Such regimens require close clinical and serologic follow-up to identify treatment failure or relapse. If adherence to therapy or close follow-up cannot be ensured with alternative regimens, clinicians should desensitize and treat with penicillin.Doxycycline (100 mg PO bid for 14 days) may be effective for early syphilis. If treatment failure occurs with doxycycline, patients should undergo desensitization to penicillin and penicillin treatment. Resistance and treatment failures have been documented with the use of azithromycin (2 g PO in a single dose) for early syphilis; this agent should be used with caution and only when treatment with penicillin or doxycycline is not feasible. Azithromycin should not be used in MSM or pregnant women.36 Ceftriaxone has been used for treatment of latent and neurologic syphilis, but failures have been reported. No clear alternative regimens exist for tertiary forms of syphilis other than neurosyphilis.37B. Jarisch-Herxheimer ReactionR ECOMMENDATION:Clinicians should inform patients about possible adverse reactions to syphilis treatment, including the Jarisch-Herxheimer reaction. (AIII)The Jarisch-Herxheimer reaction, which is caused by the immunologic response to the destruction of the spirochete, can occur within the first 24 hours of syphilis therapy and may require acute management. This acute febrile reaction is frequently accompanied by headache, myalgia, and/or worsening of secondary syphilis rash, and occurs most often in patients with early syphilis. The Jarisch-Herxheimer reaction may induce early labor or cause fetal distress in pregnant women, but this concern should not prevent or delay therapy.C. Treatment FailureR ECOMMENDATIONS:Clinicians should evaluate the CSF of HIV-infected patients who experience treatment failure. (AII)According to the results of the CSF examination, the clinician should either re-treat with therapy for late latent syphilis or initiate parenteral therapy using a recommended regimen for neurosyphilis (see Table 2). (AIII) Consultation with an expert in STIs is indicated. Treatment failure has been reported in HIV-infected patients at all stages of syphilis and with all of the recommended regimens. The use of ART to restore immune function may reduce treatment failure rates in HIV-infected patients with syphilis.38VII.M ANAGEMENT OF P ARTNERSR ECOMMENDATION:Clinicians should consider both HIV and STI exposures to partners when HIV-infected patients present with a new STI. Clinicians should also assess for the presence of other STIs. (AIII)A. Management of HIV Exposure in PartnersR ECOMMENDATIONS:When HIV-infected patients present with a new STI, clinicians should offer assistance with notifying partners of both the potential HIV and STI exposures or should refer patients to other sources for partner notification assistance (Partner Services in New York State or CNAP in New York City). Partners without confirmed HIV infection should undergo HIV testing at baseline, 1, 3, and 6 months. Confirmatory testing according to New York State regulations must be performed to confirm HIV diagnoses.Clinicians must report confirmed cases of HIV according to New York State Law(for more information about required reporting, see/diseases/aids/regulations/index.htm).Clinicians should educate patients with non-HIV-infected partners or partners of unknown HIV status to be vigilant for any post-exposure acute HIV symptoms in their partners, such as febrile illness accompanied by rash, lymphadenopathy, myalgias, and/or sore throat (see Diagnosis and Management of Acute HIV Infection). (AIII)Partners who present within 36 hours of an HIV exposure should be evaluated as soon as possible for initiation of post-exposure prophylaxis therapy (see HIV Prophylaxis Following Non-Occupational Exposure Including Sexual Assault). (AII)Presentation of a new STI in HIV-infected patients suggests exposure of both HIV and the STI to their partners. In this case, offering HIV non-occupational post-exposure prophylaxis (nPEP) to partners is usually not an option because the period prior to STI symptom onset is usually longer than the 36-hour window for initiating HIV nPEP. Therefore, sequential HIV testing of partners without confirmed HIV infection should be performed for early identification of potential HIV acquisition. However, if a patient with an HIV exposure does present within 36 hours, evaluation for nPEP should occur (see HIV Prophylaxis Following Non-Occupational Exposure Including Sexual Assault).B. Management of Syphilis ExposureR ECOMMENDATIONS:Clinicians must report all suspected or confirmed syphilis diagnoses to the local health department of the area where the patient resides according to NYS requirements (also see reportable communicable diseases). Clinicians should educate patients with reportable illnesses in New York State about the potential for confidential follow-up from the New York State Department of Health.Persons exposed sexually to a patient who has syphilis in any stage should be evaluated for oral, vaginal, penile, and anal lesions, and serology should be obtained. Clinicians should treat partners with a recommended regimen according to the following recommendations: •For persons who were exposed within the 90 days preceding the diagnosis of primary,secondary, or early latent syphilis in a sex partner: these persons may be infected even if they are seronegative; therefore, such persons should be treated presumptively. (AII) •For persons who were exposed >90 days before the diagnosis of primary, secondary, or early latent syphilis in a sex partner: treat presumptively if serologic test results are not available immediately and the opportunity for follow-up is uncertain. (AIII) •For long-term sex partners of patients who have latent syphilis: evaluate clinically and serologically for syphilis and treat on the basis of the evaluation findings. (AIII) Sexual transmission of T. pallidum occurs only when mucocutaneous syphilitic lesions are present; such manifestations are uncommon after the first year of infection.VIII.H EALTHCARE W ORKER E XPOSUREHistorically, many clinicians were taught that the skin lesions of secondary syphilis were “teeming with spirochetes.” However, the only lesions that actually appear to present any risk to the healthcare worker are those of the primary chancre or condylomata lata (secondary lesions involving the mucous membranes). Standard barrier precautions (i.e., gloves) should suffice in protecting the healthcare worker from transmission of syphilis from ulcerative lesions.R EFERENCES1. Centers for Disease Control and Prevention. 2009 Sexually Transmitted Diseases Surveillance: Syphilis. Atlanta, GA. Available at: /std/stats09/syphilis.htm2. Centers for Disease Control and Prevention. Primary and secondary syphilis among men who have sex with men-- New York City, 2001. MMWR Morb Mortal Wkly Rep 2002;51:853-856. Available at:/mmwr/preview/mmwrhtml/mm5138a1.htm3. Centers for Disease Control and Preventions. Transmission of primary and secondary syphilis by oral sex---Chicago, Illinois, 1998-2002. MMWR 2004;53(41);966-968. Available at:/mmwr/preview/mmwrhtml/mm5341a2.htm4. Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: The contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999;73:3-17. [PubMed]5. Dickerson MC, Johnston BA, Delea TE, et al. The causal role for genital ulcer disease as a risk factor for transmission of human immunodeficiency virus. Sex Transm Dis 1996;429-440. [PubMed]6. Telzak EE, Chaisson MA, Bevier PJ, et al. HIV-1 seroconversion in patients with and without genital ulcer disease. Ann Intern Med 1993;119:1181-1186. [PubMed]7. Centers for Disease Control and Preventions. Discordant results from reverse sequence syphilis screening---five laboratories, United States, 2006-2010. MMWR 2011;60;133-137. Available at:/mmwr/preview/mmwrhtml/mm6005a1.htm?s_cid=mm6005a1_w8. Rolfs RT, Joesoef MR, Hendershot EF, et al. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The syphilis and HIV Study Group. N Engl J Med 1997;337:307-314. [PubMed]9. Rompalo AM, Joesoef MR, O’Donnell JA, et al. Clinical manifestations of early status by HIV status and gender: Results of the Syphilis and HIV Study. The Syphilis and HIV Study Group. Sex Transm Dis 2001;28:158-165. [PubMed]10. Rompalo AM, Lawlor J, Seaman P, et al. Modification of syphilitic genital ulcer manifestations by coexistent HIV infection. Sex Transm Dis 2001;28:448-454. [PubMed]11. García-Silva J, Velasco-Benito JA, Peña-Penabad C. Primary syphilis with multiple chancres and porphyria cutanea tarda in an HIV infected patient. Dermatology 1994;188:163-165. [PubMed]12. Tucker SC, Yates VM, Thambar IV. Unusual skin ulceration in an HIV-positive patient who had cutaneous syphilis and neurosyphilis. Br J Dermatol 1997;136:946-948. [PubMed]13. Shulkin d, Tripoli L, Abell E. Lues maligna in a patient with human immunodeficiency virus infection. Am J Med 1988;85:425-427.14. Sands M, Markus A. Lues maligna, or ulceronodular syphilis, in a man infected with human immunodeficiency virus: Case report and review. Clin Infect Dis 1995;20:387-390. [PubMed]15. Rademacher SE, Radolf JD. Prominent osseous and unusual dermatologic manifestations of early syphilis in two patients with discordant serological statuses for human immunodeficiency virus infection. Clin Infect Dis1996;23:462-467. [PubMed]16. Horowitz HW, Valsamis MP, Wicher V, et al. Cerebral syphilitic gumma confirmed by the polymerase chain reaction in a man with human immunodeficiency virus infection. N Engl J Med 1994;331:1488-1491.。