普特彼(他克莫司软膏)简要说明书
他克莫司软膏的作用与功效
他克莫司软膏的作用与功效
他克莫司软膏是一种外用药膏,主要成分是他克莫司。
它常用于治疗各种皮肤炎症,如湿疹、皮炎和接触性皮炎等。
他克莫司软膏具有以下作用和功效:
1. 抗炎作用:他克莫司软膏能有效减轻皮肤的炎症反应,减少红肿、瘙痒等炎症症状。
2. 抗过敏作用:他克莫司软膏可以抑制过敏反应,减少过敏症状,如皮肤瘙痒和发疹等。
3. 抗菌作用:他克莫司软膏还具有一定的抗菌作用,可以预防和治疗由细菌感染引起的皮肤病变。
4. 保湿作用:他克莫司软膏含有一定的保湿成分,可以补充皮肤水分,改善皮肤干燥和脱屑现象,使皮肤保持湿润和柔软。
5. 修复作用:他克莫司软膏可以促进皮肤细胞的修复和再生,加速治愈时间,减少炎症留下的疤痕和色素沉着。
总的来说,他克莫司软膏对于皮肤炎症的治疗具有显著的效果,可以缓解症状、减轻炎症,并且具有一定的抗菌和保湿作用,有助于皮肤的修复和恢复健康。
0.03%他克莫司软膏治疗口周皮炎的临床观察
0.03%他克莫司软膏治疗口周皮炎的临床观察摘要目的观察0.03%他克莫司软膏治疗口周皮炎的临床疗效。
方法82例口周皮炎患者随机分为实验组(42例)和对照组(40例)。
实验组外用0.03%他克莫司软膏,1次/d;对照组外用红霉素眼膏,1次/d。
两组疗程均为4周,比较两组治疗4周后的疗效。
结果两组治疗4周后,实验组总有效率为95.24%,优于对照组的75.00%,差异有统计学意义(P<0.05)。
结论0.03%他克莫司软膏局部治疗口周皮炎临床疗效满意。
关键词0.03%他克莫司软膏;口周皮炎;临床观察口周皮炎发病部位多见口唇周围,有丘疹、脓疱、脱屑、红斑等损害,除口周外,皮损也可见于两侧颊部等更大范围。
本病病情轻重不一,常呈慢性、反复发作,患者自觉有不同程度瘙痒及灼热感,部分患者病久后留下色素沉着,影响容貌,给患者造成心理障碍甚至部分患者使用皮质激素后照成激素依赖性皮炎,和口周皮炎混杂一起,严重影响生活质量。
本院对82例口周皮炎患者应用0.03%他克莫司软膏治疗,取得较好效果,现报告如下。
1 资料与方法1. 1 一般资料选取2012年4月~2014年6月本院皮肤科门诊口周皮炎患者82例,病例资料符合口周皮炎临床诊断标准[1];排除标准:①对他克莫司过敏者;②患有痤疮、单纯疱疹、面部脂溢性皮炎、接触性皮炎等疾病;③近期系统使用过免疫抑制剂、皮质激素者,服用避孕药或者外用皮质激素停药不足1个月者;④有严重的心脏、肝脏、肾脏疾病者;⑤孕妇和哺乳期妇女。
82例患者随机分为实验组和对照组。
实验组42例,其中男14例,女28例;年龄8~48岁,平均年龄30岁;病程1个月~2年,平均病程13.5个月。
对照组40例,其中男12例,女28例;年龄7~46岁,平均年龄31.5岁;病程1个月~3年,平均病程15个月。
两组患者性别、年龄、病程等方面比较差异无统计学意义(P>0.05),具有可比性。
1. 2 方法实验组给予0.03%他克莫司软膏(商品名:普特彼,安斯泰来制药中国有限公司,10 g/支,国药准字J20060030),1次/晚。
外用他克莫司在皮肤科的应用
J Pfxlia Gastroenteroi9影明d Nutrition 2002;34:555—557.
13 Pandller BS,Rustin M}认,蹦sary AV,et a1.7I妇tⅡlent“bal飘一 i石s x叫mca obbte啪s with topical tacmhmus.J Urol 2003;170:
tr}eat·
mem.ArchDe删tol 20Q5;14l:43—46.
L,Rodriquez—I脚z 9 Ahnei(Ia P,Borrego
J,et a1.Vimi妒.7Ikat—
H地nt of 12 ca8es witll topical tacroliInus.Actas De硼o Sifiliog乒血cas
2005:96:159—163.
10潘炜华,刘晓刚,温海.他克莫司软膏治疗激素依赖性皮炎 的疗效观察.中国美容医学20cr7;16:78—79.
1l郝飞,钟华.他克莫司软膏治疗面部糖皮质激素依赖性皮炎
万方数据
中国麻风皮肤病杂志2008年6月第24卷第6期
临床疗效观察.临床皮肤科杂志20cr7;36:54—56. 12 l(imble Roy M,TicUer,Ae衄one K,et a1.Success“topical ta—
由于他克莫司对胶原合成无抑制作用?会引起皮肤萎缩同时局部外用安全性高耐受性好所以可用于面部生殖器和间擦部等薄嫩部位皮肤75结语他克莫司软膏是一种新型的外用免疫抑制剂其局部应用方?有效且安全随着对他克莫司作用机制深入的研究及在非特应性皮炎的其他皮肤疾病中的应用其适应症可能会逐渐扩大
他克莫司软膏的副作(养生小贴士)
他克莫司软膏的副作 现在由于环境污染和人们免疫力的原因,得皮炎的人群越来越多了,有些甚至是重度皮炎,而他克莫司软膏是有着白色或是淡黄色的膏体,正是用于治疗重度皮炎、银屑病、白癜风等的外用药,它属于一种新型的抗炎药物,对于皮肤病的治疗疗效显著,帮助了很多的人恢复了健康,那么用这个他克莫司软膏有没有副作用呢?他克莫司软膏的副作用一般较少,外用他克莫司软膏可能会引起局部症状,如皮肤烧灼感(灼热感、刺痛、疼痛)或瘙痒。
局部症状最常见于使用本品的最初几天,通常会随着特应性皮炎受累皮肤好转而消失。
应用0。
1%浓度的他克莫司软膏治疗时,90%的皮肤烧灼感持续时间介于2分钟至3小时(中位时间为15分钟)之间,90%的瘙痒症状持续时间介于3分钟至10小时(中位时间为20分钟)之间。
不推荐使用他克莫司软膏治疗Netherton综合征患者,因为可能会增加他克莫司的全身性吸收。
他克莫司软膏对弥漫性红皮病患者治疗的安全性尚未建立。
1、他克莫司软膏可能使饮酒者出现皮疹,而且对他克莫司或制剂中任何其他成分有过敏史的患者禁用。
2、外用他克莫司软膏可能会引起局部症状,如皮肤烧灼感(灼热感、刺痛、疼痛)或瘙痒。
局部症状最常见于使用他克莫司软膏的最初几天,通常会随着特应性皮炎受累皮肤好转而消失。
3、一般不会因为使用他克莫司软膏药品不当,导致患有皮炎疾病的患者出现什么不良防反应。
在使用他克莫司软膏时,是会出现一定的现象,比如灼热感、刺痛等,但是这些现象时能通过自己身体调节治愈的。
一旦出现灼热感、刺痛等现象不消退,就要及时到正规的三家医院治疗。
★使用他克莫司软膏时应注意以下几点:1、患者应在医生的指导下使用他克莫司软膏。
他克莫司软膏仅供外用。
和任何外用药一样,患者或护工在用药后应洗手,如果手部不是治疗区的话。
2、在使用他克莫司软膏期间,患者应减少或避免自然阳光或人工太阳光(晒床或UVA/UVB治疗)。
他克莫司 用法(一)
他克莫司用法(一)他克莫司1. 介绍他克莫司(英文名称:Tacrolimus),是一种免疫抑制剂,广泛应用于器官移植手术后预防和治疗排斥反应。
2. 适应症•器官移植术后的免疫抑制:他克莫司可以用于肾脏、心脏、肺、肝脏、胰腺等器官移植手术后免疫抑制的预防和治疗。
3. 用法用量•肾移植患者:术后第1天开始,根据患者情况,每日口服他克莫司/kg分2次服用,调整剂量以维持血药浓度在正确的范围内。
4. 注意事项•高血压:长期使用他克莫司可能导致高血压,需要定期监测血压情况。
•肾功能不全:由于他克莫司主要通过肾脏代谢,肾功能不全的患者需要调整剂量,避免药物积累导致毒副作用。
•多种药物相互作用:他克莫司与某些药物(如氯霉素、酮康唑等)相互作用,可能影响药物的疗效或增加毒副作用,务必告知医生正在使用的其他药物。
5. 不良反应•肾功能损害:部分患者在使用他克莫司期间可能出现肾功能不全,需要定期监测肾功•皮肤反应:少数患者可能出现皮肤病变、瘙痒等不良反应,应立即停药并就医。
•高血糖:他克莫司使用时间较长的患者可能出现高血糖,需要监测血糖情况。
6. 禁忌症•对他克莫司过敏者禁用。
•孕妇和哺乳期妇女慎用。
7. 药物储存•存放在阴凉干燥处,避免阳光直射和高温。
以上就是关于他克莫司的一些用法和注意事项的简要介绍,希望可以对大家有所帮助。
请在使用药物前务必咨询医生,并仔细阅读药品说明书。
1. 药物副作用•恶心和呕吐:他克莫司治疗期间,部分患者可能出现恶心和呕吐的副作用,可适量进食并与医生沟通寻求缓解措施。
•腹泻:有些患者可能出现腹泻症状,应保持充足的水分摄入并避免高脂高纤维食物。
•高血压:他克莫司可能导致一些患者的血压升高,需要定期监测,并根据医生建议进行控制。
•感染:免疫抑制作用可能增加患者感染的风险,特别是真菌感染,应避免接触病原体,并及时发现和治疗感染。
2. 药物相互作用•他克莫司可能与一些药物相互作用,包括其他免疫抑制剂、抗生素、抗真菌药物等,应在使用其他药物前告知医生,避免药物相互作用导致不良反应。
他克莫司软膏注意事项

他克莫司软膏注意事项他克莫司软膏是一种常用的外用药物,主要用于治疗皮肤病和炎症。
在使用他克莫司软膏之前,我们需要了解一些注意事项和禁忌症。
以下是与他克莫司软膏相关的一些重要注意事项:1. 注意病情:在使用他克莫司软膏之前,应先确诊病情,并确保其适用于外用药物治疗。
某些皮肤疾病或局部感染可能需要其他治疗方法。
因此,最重要的是在使用前咨询医生,并根据专业的指导使用。
2. 避免接触眼睛和黏膜:他克莫司软膏只适用于外用,禁止接触眼睛和黏膜。
使用药物后应用清水冲洗双手,避免将药物传到其他部位。
3. 保持干燥和清洁:在使用他克莫司软膏期间,应保持患处干燥和清洁。
避免过度搔抓或磨擦。
最好药物吸收后避免受潮,以免影响药效。
4. 遵循剂量和使用周期:根据医生的推荐使用他克莫司软膏的剂量和使用周期。
不要随意增加或减少药物剂量,以免出现药物残留或缺乏治疗效果的问题。
5. 不要与其他药物混合使用:在使用他克莫司软膏时,应避免与其他药物混合使用,特别是其他外用药物。
这可能导致不良反应或药物相互作用。
6. 孕妇和哺乳期妇女:如果您是孕妇或正在哺乳,使用他克莫司软膏前请先咨询医生。
有效成分可能对胎儿或婴儿有不利影响,需谨慎使用。
7. 不适合过敏体质者:他克莫司软膏可能引起过敏反应,因此对其中任何一种成分过敏的人不适合使用。
在使用药物前,最好做皮肤敏感性测试。
8. 不适合长期使用:他克莫司软膏通常用于短期治疗,长时间使用有可能出现皮肤萎缩、皮肤变薄、毛细血管扩张等不良反应。
如果症状没有改善,请咨询医生进行进一步的治疗方案。
9. 孩童使用:如果您为儿童使用他克莫司软膏,请先咨询医生。
儿童可能对药物成分更敏感,因此医生会根据儿童的年龄和体重来确定剂量和使用频率。
10. 药物保存:保持他克莫司软膏在室温下保存,避免阳光直射。
确保药物存放在儿童无法接触的地方。
总之,在使用他克莫司软膏前,请仔细阅读药物说明书,并咨询医生的指导。
遵循医嘱使用药物,注意患处的干燥和清洁,避免药物接触眼睛和黏膜。
普特彼
抗原
钙调蛋白
去磷酸化
他克莫司的细胞内作用机制
FKBP-12:他克莫司结合蛋白-12 他克莫司FKBP-12-钙调素-钙调磷酸酶复合物: 他克莫司通过阻断钙调磷酸酶/NFAT信号通路来抑制T细胞活化
他克莫司软膏(普特彼®)的 皮肤科适应症
特应性皮炎(FDA,SFDA批准)
0.1% 他克莫司软膏:成人特应性皮炎 0.03% 他克莫司软膏:≥2岁儿童及成人特应性皮炎
MMP-9:间质金属蛋白酶9
H-S.Yu et al,British Journal of Dermatology 2005,153:498-505
儿童白癜风-1
57 例儿童白癜风患者使用普特彼®软膏治疗研究
– 使用0.03%或0.1%普特彼® ,治疗3个月以上
– 效果:头颈部: 89% (34/38); 躯干和四肢: 63%(21/32)
一、普特彼在AD治疗中的应用
外用钙调神经磷酸酶抑制剂
• 目前有两种TCIs 用于治疗特应性皮炎 – 他克莫司软膏,2005年在国内上市 – 吡美莫司乳膏 2006年在国内上市 • TCIs治疗特应性皮炎有可靠的疗效 :
– 传统激素治疗无效或者对使用激素怀有恐惧心理的患者
– 薄嫩部位的皮损
8
1. Leung DY, et al. J Clin Invest 2004; 113:651–657. 2. Baldo A, et al. Clin Cosmetic Invest Dermatol 2009; 2:1–7.
普特彼®的适应症
普特彼®治疗其他免疫相关性皮肤病的报告:
– 银屑病 – 白癜风 – 脂溢性皮炎 – 激素依赖性皮炎 –大疱性类天疱疮 –家族性慢性良性天疱疮 –红斑狼疮 –移植物抗宿主病(GVHD)
他克莫司说明书
孚诺(复方多粘菌素B软膏),他克莫司(普特彼)说明书如下:【普特彼药品名称】通用名:他克莫司软膏商品名:普特彼英文名:Tacrolimus Ointment汉语拼音:TaKeMoSiRuanGao【普特彼成份】普特彼主要成份为:他克莫司。
【普特彼性状】普特彼为白色至淡黄色软膏。
【普特彼处方组成】每克普特彼含他克莫司0.03或0.1(w/w),软膏基质为矿物油、石蜡、碳酸丙烯酯、白凡士林和白蜡。
【普特彼药理毒理】药理作用他克莫司治疗特应性皮炎的作用机制还不清楚。
虽然对他克莫司的作用机制已有一定了解,但是这些发现与特应性皮炎的临床关系还不明确。
他克莫司已被证实可以抑制T淋巴细胞活化,首先与细胞内蛋白FKBP-12结合,形成由他克莫司-FKBP-12、钙、钙调蛋白和钙调磷酸酶构成的复合物,从而抑制钙调磷酸酶的磷酸酶活性,阻止活化T细胞核转录因子(NF-AT)的去磷酸化和易位,NF-AT这种核成分会启动基因转录形成淋巴因子(例如IL-2,γ干扰素)。
他克莫司还可以抑制编码IL-3、IL-4、IL-5、GM-CSF和TNF-?的基因的转录,所有这些因子都参与早期阶段的T细胞活化。
此外,他克莫司可以抑制皮肤肥大细胞和嗜碱性粒细胞内已合成介质的释放,下调朗格罕细胞表面FCεRI的表达。
毒理作用在为期26周的大鼠实验和为期28天的家兔实验中,每天外用他克莫司软膏(0.03-1)后,在显微镜下观察到皮肤变化(增生、表皮空泡形成、棘层肥厚、浅表炎症)。
由于这些皮肤变化与他克莫司浓度不相关,也见于赋形剂组,而空白对照组极少见,因而被认为与赋形剂有关而与他克莫司本身无关。
在大鼠中外用高浓度软膏(基本上≥0.3)观察到全身毒性反应,与经口服或静脉摄入后相似。
在为期52周的尤卡坦微型猪局部实验中,肉眼或显微镜下所见的改变均被认为与外用他克莫司(0.03?0.3)无关,因为在赋形剂对照组也观察到同样的改变。
在对豚鼠进行的实验中,他克莫司软膏(0.03?3)不诱发接触过敏或光敏化反应,对白化无毛小鼠也不诱发皮肤光毒性。
普特彼(他克莫司软膏)使用说明
普特彼(他克莫司软膏)【用法用量】成人0.03%和0.1%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
本品不应采用封包敷料外用。
儿童0.03%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
本品不应采用封包敷料外用。
【注意事项】1.肝肾功能不全、糖尿病、高钾血症、心室肥大、有神经性毒性表现者,如震颤、头痛、共济失调、精神状态改变等慎用。
2.对老年患者用药的临床数据较少,但均提示应与其它成人剂量相同。
3.肝肾移植的维持治疗阶段,必须持续使用本品来维持移植物功能。
推荐需根据患者个体差异来定。
在维持治疗期间有本品用量逐渐减少的趋势。
剂量调整主要根据对排斥反应的临床治疗效果和患者的耐受性判断。
4.妊娠时禁用本品,动物实验(小鼠及兔子)表明,本品具有致畸作用,并且某些剂量还显示出对母体具有毒性。
临床前及临床数据表明,该药能透过胎盘。
因此在应用本品前应排除妊娠的可能性。
本品能干扰口服避孕药的代谢,应改用其它方式避孕。
临床前兔身上的试验表明,本品分泌进乳汁。
5.哺乳期使用本品的经验有限。
不能排除对新生儿的有害影响,妇女患者在使用本品时不应哺乳。
6.本品用量应根据临床诊断辅以全血药物浓度相应调整,其全血药物浓度在20ng/ml均能取得较好效果。
由于其半衰期长,调整剂量需要几天时间才能真正反映其血液中药物浓度的变化。
剂量和血药浓度的调节必须是在负责管理患者的移植中心。
【不良反应】在服用本品期间,如果感到不适要尽快告诉医师或药师。
情况紧急可先停止服药。
详情请看说明书。
【禁忌】1.妊娠禁用。
2.本品化学结构属于大环内酯类,对他克莫司或其它大环内酯类药物过敏者、对胶囊中其它成份过敏者禁用。
【适应症】本品适用于因潜在危险而不宜使用传统疗法、或对传统疗法反应不充分、或无法耐受传统疗法的中到重度特应性皮炎患者,作为短期或间歇性长期治疗。
他克莫司
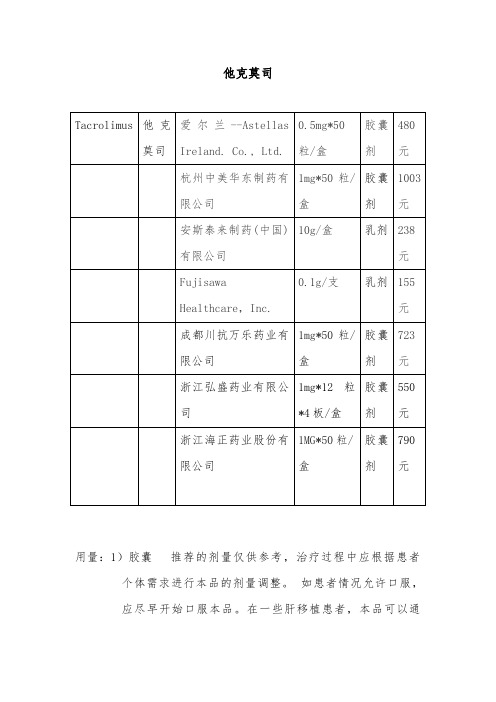
他克莫司用量:1)胶囊推荐的剂量仅供参考,治疗过程中应根据患者个体需求进行本品的剂量调整。
如患者情况允许口服,应尽早开始口服本品。
在一些肝移植患者,本品可以通过鼻饲来口服给药。
本品通常与其他免疫抑制药物一起使用,亦出现有单独使用本品的个例报道。
本品不能与环孢素并用。
如出现排斥反应或不良事件发生,需考虑更改免疫抑制治疗方案。
在维持治疗阶段,建议持续使用本品来维持移植物的存活。
如患者病情恶化(如出现急性排斥反应的征兆),应考虑改变免疫抑制剂用药方案。
多种方案均可用于控制排斥反应,如增加类固醇激素用量、加用短期的单克隆或多克隆抗体、增加本品的用量。
如出现中毒征兆(如明显的不良事件),应减少本品的用量。
并应告诉患者,在未经主管医师同意的情况下,不应擅自减量。
在移植术后患者的情况改善期内,本品的药代动力学可能会发生改变,需要调整本品的剂量。
每日服药两次(早晨和晚上),最好用水送服。
建议空腹,或者至少在餐前1小时或餐后2-3小时服用。
如必要可将胶囊内容物悬浮于水,经鼻饲管给药。
若患者临床状况不能口服,首剂须静脉给药。
2)乳膏成人0.03%和0.1%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
本品不应采用封包敷料外用。
儿童0.03%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
普特彼(他克莫司软膏) 不应采用封包敷料外用。
市场他克莫司在中国上市的短时间内,市场份额迅速上升,已成为肝脏及肾脏移植后排斥反应的临床一线药物。
目前我国免疫抑制剂市场规模为50~60亿,其中国外公司将的他克莫司免疫抑制剂市场份额占80%,开发我国内他克莫司具有自主知识产权的生产技术及开发技术迫在眉急。
他克莫司软膏说明书(英文PDR)
PDR? Electronic Library(TM)This report is based solely on product labeling as published by Physicians?Desk Reference ? Copyright ?2003 Thomson Medical Economics. All rights reserved.Report generated 09-06-2004 at 08:02 pmProtopic Ointment(Fujisawa)FOR DERMATOLOGIC USE ONLYNOT FOR OPHTHALMIC USEDESCRIPTIONPROTOPIC (tacrolimus) Ointment contains tacrolimus, a macrolide immunosuppressant produced by Streptomyces tsukubaensis . It is for topical dermatologic use only. Chemically, tacrolimus is designated as [3 S -[3 R *[ E (1 S *,3 S *,4 S *)],4 S *,5 R *,8 S *,9 E ,12 R *,14 R *, 15 S *, 16 R *,18 S *,19 S *,26a R *]] - 5,6,8,11,12,13,14,15,16,17,18, 19,24,25,26,26a-hexadecahydro-5,19-dihydroxy-3-[2-(4-hydroxy-3-methoxycyclohexyl)-1-methylethenyl]-14,16-dimethoxy-4,10,12,18-tetramethyl-8-(2-propenyl)-15, 19-epoxy-3H-pyrido[2,1- c ][1,4]oxaazacyclotricosine-1,7,20,21(4H,23H)-tetrone, monohydrate. It has the following structural formula:Tacrolimus has an empirical formula of C44 H69NO12·H2O and a formula weight of 822.05. Each gram of PROTOPIC Ointmentcontains (w/w) either 0.03% or 0.1% of tacrolimus in a base of mineral oil, paraffin, propylene carbonate, white petrolatum and white wax.CLINICAL PHARMACOLOGYMechanism of ActionThe mechanism of action of tacrolimus in atopic dermatitis is not known. While the following have been observed, the clinicalsignificance of these observations in atopic dermatitis is not known. It has been demonstrated that tacrolimus inhibits T-lymphocyte activation by first binding to an intracellular protein, FKBP-12. A complex of tacrolimus-FKBP-12, calcium, calmodulin, and calcineurin is then formed and the phosphatase activity of calcineurin is inhibited. This effect has been shown to prevent the dephosphorylation and translocation of nuclear factor of activated T-cells (NF-AT), a nuclear component thought to initiate genetranscription for the formation of lymphokines (such as interleukin-2, gamma interferon). Tacrolimus also inhibits the transcription for genes which encode IL-3, IL-4, IL-5, GM-CSF, and TNF-(alpha), all of which are involved in the early stages of T-cell activation. Additionally, tacrolimus has been shown to inhibit the release of pre-formed mediators from skin mast cells and basophils, and to downregulate the expression of Fc[egr ]Rl on Langerhans cells. PharmacokineticsThe pooled results from two pharmacokinetic studies in 49 adult atopic dermatitis patients indicate that tacrolimus is absorbed after the topical application of 0.1% PROTOPIC Ointment. Peak tacrolimus blood concentrations ranged from undetectable to 20 ng/mL after single or multiple doses of 0.1% PROTOPIC Ointment, with 45 of the 49 patients having peak blood concentrations less than 5ng/mL. The results from a pharmacokinetic study of 0.1% PROTOPIC Ointment in 20 pediatric atopic dermatitis patients (ages 6-13 years), show peak tacrolimus blood concentrations below 1.6 ng/mL in all patients.There was no evidence based on blood concentrations that tacrolimus accumulates systemically upon intermittent topical application for periods of up to 1 year. The absolute bioavailability of topical tacrolimus is unknown. Using IV historical data for comparison, the bioavailability of tacrolimus from PROTOPIC in atopic dermatitis patients is less than 0.5%. In adults with an average of 53% BSA treated, exposure (i.e., AUC) of tacrolimus from PROTOPIC is approximately 30-fold less than that seen with oralimmunosuppressive doses in kidney and liver transplant patients. The lowest tacrolimus blood level at which systemic effects can be observed is not known. CLINICAL STUDIESThree randomized, double-blind, vehicle-controlled, multi-center, phase 3 studies were conducted to evaluate PROTOPIC Ointment for the treatment of patients with moderate to severe atopic dermatitis. One (Pediatric) study included 351 patients 2-15 years of age, and the other two (Adult) studies included a total of 632 patients 15-79 years of age. Fifty-five percent (55%) of the patients were women and 27% were black. At baseline, 58% of the patients had severe disease and the mean body surface area (BSA) affected was 46%. Over 80% of patients had atopic dermatitis affecting the face and/or neck region. In these studies, patients applied eitherPROTOPIC Ointment 0.03%, PROTOPIC Ointment 0.1%, or vehicle ointment twice daily to 10%-100% of their BSA for up to 12 weeks.In the pediatric study, a significantly greater (p < 0.001) percentage of patients achieved at least 90% improvement based on the physician's global evaluation of clinical response (the pre-defined primary efficacy end point) in the PROTOPIC Ointment 0.03% treatment group compared to the vehicle treatment group, but there was insufficient evidence that PROTOPIC Ointment 0.1% provided more efficacy than PROTOPIC Ointment 0.03%.In both adult studies, a significantly greater (p < 0.001) percentage of patients achieved at least 90% improvement based on the physician's global evaluation of clinical response in the PROTOPIC Ointment 0.03% and PROTOPIC Ointment 0.1% treatmentgroups compared to the vehicle treatment group. There was evidence that PROTOPIC Ointment 0.1% may provide more efficacy than PROTOPIC Ointment 0.03%. The difference in efficacy between PROTOPIC Ointment 0.1% and 0.03% was particularly evident in adult patients with severe disease at baseline, adults with extensive BSA involvement, and black adults. Response rates for each treatment group are shown below by age groups. Because the two adult studies were identically designed, the results from these studies were pooled in this table.A statistically significant difference in the percentage of adult patients with >/= 90% improvement was achieved by week 1 for those treated with PROTOPIC Ointment 0.1%, and by week 3 for those treated with PROTOPIC Ointment 0.03%. A statistically significant difference in the percentage of pediatric patients with >/= 90% improvement was achieved by week 2 for those treated with PROTOPIC Ointment 0.03%.In adult patients who had achieved >/= 90% improvement at the end of treatment, 35% of those treated with PROTOPIC OintmentGlobal Improvement over Baseline at the End-of-Treatment in Three Phase 3 Studies Physician's Global Evaluation of Clinical Response (% Improvement)Pediatric Study (2-15 Years of Age) Adult StudiesVehicle Ointment N = 116 PROTOPIC Ointment 0.03% N = 117VehicleOintment N = 212 PROTOPICOintment 0.03% N = 211PROTOPIC Ointment 0.1% N = 209100% 4 (3%) 14 (12%) 2 (1%) 21 (10%) 20 (10%) >/=90% 8 (7%) 42 (36%) 14 (7%) 58 (28%) 77 (37%) >/=75% 18 (16%) 65 (56%) 30 (14%) 97 (46%) 117 (56%) >/=50%31 (27%)85 (73%)42 (20%)130 (62%)152 (73%)0.03% and 41% of those treated with PROTOPIC Ointment 0.1%, regressed from this state of improvement at 2 weeks after end-of-treatment. In pediatric patients who had achieved >/= 90% improvement, 54% of those treated with PROTOPIC Ointment 0.03% regressed from this state of improvement at 2 weeks after end-of-treatment. Because patients were not followed for longer than 2 weeks after end-of-treatment, it is not known how many additional patients regressed at periods longer than 2 weeks after cessation of therapy.In both PROTOPIC Ointment treatment groups in adults and in the PROTOPIC Ointment 0.03% treatment group in pediatric patients, a significantly greater improvement compared to vehicle (p < 0.001) was observed in the secondary efficacy endpoints of percent body surface area involved, patient evaluation of pruritus, erythema, edema, excoriation, oozing, scaling, and lichenification. The following two graphs depict the time course of improvement in the percent body surface area affected in adult and in pediatric patients as a result of treatment.The following two graphs depict the time course of improvement in erythema in adult and in pediatric patients as a result of treatment.The time course of improvement in the remaining secondary efficacy variables was similar to that of erythema, with improvement in lichenification slightly slower.A total of 571 patients applied PROTOPIC Ointment 0.1% in long-term adult and pediatric safety studies for up to one year. In the adult study, 246 patients were evaluated for at least 6 months and 68 patients for 12 months. In the pediatric study, 219 patients were evaluated for at least 6 months and 180 patients for 12 months. On average, patients received treatment for 87% of study days.INDICATIONS AND USAGEPROTOPIC Ointment, both 0.03% and 0.1% for adults, and only 0.03% for children aged 2 to 15 years, is indicated for short-term and intermittent long-term therapy in the treatment of patients with moderate to severe atopic dermatitis in whom the use of alternative, conventional therapies are deemed inadvisable because of potential risks, or in the treatment of patients who are not adequately responsive to or are intolerant of alternative, conventional therapies.CONTRAINDICATIONSPROTOPIC Ointment is contraindicated in patients with a history of hypersensitivity to tacrolimus or any other component of the preparation.PRECAUTIONSGeneralStudies have not evaluated the safety and efficacy of PROTOPIC Ointment in the treatment of clinically infected atopic dermatitis. Before commencing treatment with PROTOPIC Ointment, clinical infections at treatment sites should be cleared.While patients with atopic dermatitis are predisposed to superficial skin infections including eczema herpeticum (Kaposi's varicelliform eruption), treatment with PROTOPIC Ointment may be associated with an increased risk of varicella zoster virus infection (chicken pox or shingles), herpes simplex virus infection, or eczema herpeticum. In the presence of these infections, the balance of risks and benefits associated with PROTOPIC Ointment use should be evaluated.In clinical studies, 33 cases of lymphadenopathy (0.8%) were reported and were usually related to infections (particularly of the skin) and noted to resolve upon appropriate antibiotic therapy. Of these 33 cases, the majority had either a clear etiology or were known to resolve. Transplant patients receiving immunosuppressive regimens (e.g., systemic tacrolimus) are at increased risk for developing lymphoma; therefore, patients who receive PROTOPIC Ointment and who develop lymphadenopathy should have the etiology of their lymphadenopathy investigated. In the absence of a clear etiology for the lymphadenopathy, or in the presence of acute infectious mononucleosis, discontinuation of PROTOPIC Ointment should be considered. Patients who develop lymphadenopathy should be monitored to ensure that the lymphadenopathy resolves.The enhancement of ultraviolet carcinogenicity is not necessarily dependent on phototoxic mechanisms. Despite the absence of observed phototoxicity in humans (see ADVERSE REACTIONS ), PROTOPIC Ointment shortened the time to skin tumor formation in an animal photocarcinogenicity study (see Carcinogenesis, Mutagenesis, Impairment of Fertility ). Therefore, it is prudent for patients to minimize or avoid natural or artificial sunlight exposure.The use of PROTOPIC Ointment may cause local symptoms such as skin burning (burning sensation, stinging, soreness) or pruritus. Localized symptoms are most common during the first few days of PROTOPIC Ointment application and typically improve as the lesions of atopic dermatitis heal. With PROTOPIC Ointment 0.1%, 90% of the skin burning events had a duration between 2 minutes and 3 hours (median 15 minutes). Ninety percent of the pruritus events had a duration between 3 minutes and 10 hours (median 20 minutes).The use of PROTOPIC Ointment in patients with Netherton's Syndrome is not recommended due to the potential for increased systemic absorption of tacrolimus. The safety of PROTOPIC Ointment has not been established in patients with generalized erythroderma.Information for Patients(See patient package insert)Patients using PROTOPIC Ointment should receive the following information and instructions:1.Patients should use PROTOPIC Ointment as directed by the physician. PROTOPIC Ointment is for external use only. As withany topical medication, patients or caregivers should wash hands after application if hands are not an area for treatment.2.Patients should minimize or avoid exposure to natural or artificial sunlight (tanning beds or UVA/B treatment) while usingPROTOPIC Ointment.3.Patients should not use this medication for any disorder other than that for which it was prescribed.4.Patients should report any signs of adverse reactions to their physician.5.Before applying PROTOPIC Ointment after a bath or shower, be sure your skin is completely dry.Drug InteractionsFormal topical drug interaction studies with PROTOPIC Ointment have not been conducted. Based on its minimal extent of absorption, interactions of PROTOPIC Ointment with systemically administered drugs are unlikely to occur but cannot be ruled out. The concomitant administration of known CYP3A4 inhibitors in patients with widespread and/or erythrodermic disease should be done with caution. Some examples of such drugs are erythromycin, itraconazole, ketoconazole, fluconazole, calcium channel blockers and cimetidine.Carcinogenesis, Mutagenesis, Impairment of FertilityNo evidence of genotoxicity was seen in bacterial ( Salmonella and E. coli ) or mammalian (Chinese hamster lung-derived cells) in vitro assays of mutagenicity, the in vitro CHO/HGPRT assay of mutagenicity, or in vivo clastogenicity assays performed in mice. Tacrolimus did not cause unscheduled DNA synthesis in rodent hepatocytes.Oral (feed) carcinogenicity studies have been carried out with systemically administered tacrolimus in male and female rats and mice. In the 80-week mouse study and in the 104-week rat study no relationship of tumor incidence to tacrolimus dosage was found at daily doses up to 3 mg/kg [9X the Maximum Recommended Human Dose (MRHD) based on AUC comparisons] and 5 mg/kg (3X the MRHD based on AUC comparisons), respectively.A 104-week dermal carcinogenicity study was performed in mice with tacrolimus ointment (0.03%-3%), equivalent to tacrolimus doses of 1.1-118 mg/kg/day or 3.3-354 mg/m 2 /day. In the study, the incidence of skin tumors was minimal and the topical application of tacrolimus was not associated with skin tumor formation under ambient room lighting. However, a statistically significant elevation in the incidence of pleomorphic lymphoma in high dose male (25/50) and female animals (27/50) and in the incidence of undifferentiated lymphoma in high dose female animals (13/50) was noted in the mouse dermal carcinogenicity study. Lymphomas were noted in the mouse dermal carcinogenicity study at a daily dose of 3.5 mg/kg (0.1% tacrolimus ointment) (26X MRHD based on AUC comparisons). No drug-related tumors were noted in the mouse dermal carcinogenicity study at a daily dose of 1.1 mg/kg (0.03% tacrolimus ointment) (10X MRHD based on AUC comparisons).In a 52-week photocarcinogenicity study, the median time to onset of skin tumor formation was decreased in hairless mice following chronic topical dosing with concurrent exposure to UV radiation (40 weeks of treatment followed by 12 weeks of observation) with tacrolimus ointment at >/=0.1% tacrolimus.Reproductive toxicology studies were not performed with topical tacrolimus. In studies of oral tacrolimus no impairment of fertility was seen in male and female rats. Tacrolimus, given orally at 1.0 mg/kg (0.12X MRHD based on body surface area [BSA]) to male and female rats, prior to and during mating, as well as to dams during gestation and lactation, was associated with embryolethality and with adverse effects on female reproduction. Effects on female reproductive function (parturition) and embryolethal effects were indicated by a higher rate of pre-implantation loss and increased numbers of undelivered and nonviable pups. When given at 3.2mg/kg (0.43X MRHD based on BSA), tacrolimus was associated with maternal and paternal toxicity as well as reproductive toxicity including marked adverse effects on estrus cycles, parturition, pup viability, and pup malformations.PregnancyTeratogenic Effects: Pregnancy Category CThere are no adequate and well-controlled studies of topically administered tacrolimus in pregnant women. The experience with PROTOPIC Ointment when used by pregnant women is too limited to permit assessment of the safety of its use during pregnancy. Reproduction studies were carried out with systemically administered tacrolimus in rats and rabbits. Adverse effects on the fetus were observed mainly at oral dose levels that were toxic to dams. Tacrolimus at oral doses of 0.32 and 1.0 mg/kg (0.04X-0.12X MRHD based on BSA) during organogenesis in rabbits was associated with maternal toxicity as well as an increase in incidence of abortions. At the higher dose only, an increased incidence of malformations and developmental variations was also seen. Tacrolimus, at oral doses of 3.2 mg/kg during organogenesis in rats, was associated with maternal toxicity and caused an increase in late resorptions, decreased numbers of live births, and decreased pup weight and viability. Tacrolimus, given orally at 1.0 and 3.2 mg/kg (0.04X-0.12X MRHD based on BSA) to pregnant rats after organogenesis and during lactation, was associated with reduced pup weights.No reduction in male or female fertility was evident.There are no adequate and well-controlled studies of systemically administered tacrolimus in pregnant women. Tacrolimus is transferred across the placenta. The use of systemically administered tacrolimus during pregnancy has been associated with neonatal hyperkalemia and renal dysfunction. PROTOPIC Ointment should be used during pregnancy only if the potential benefit to the mother justifies a potential risk to the fetus.Nursing MothersAlthough systemic absorption of tacrolimus following topical applications of PROTOPIC Ointment is minimal relative to systemic administration, it is known that tacrolimus is excreted in human milk. Because of the potential for serious adverse reactions in nursing infants from tacrolimus, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.Pediatric UsePROTOPIC Ointment 0.03% may be used in pediatric patients 2 years of age and older. Two phase 3 pediatric studies were conducted involving 606 patients 2-15 years of age: one 12-week randomized vehicle-controlled study and one open-label, 1 year, long-term safety study. Three hundred and thirty (330) of these patients were 2 to 6 years of age.The most common adverse events associated with PROTOPIC Ointment application in pediatric patients were skin burning and pruritus (see ADVERSE REACTIONS). In addition to skin burning and pruritus, the less common events (<5%) of varicella zoster (mostly children pox), and vesiculobullous rash were more frequent in patients treated with PROTOPIC Ointment 0.03% compared to vehicle. In the long-term 1 year safety study involving 255 pediatric patients using PROTOPIC Ointment, the incidence of adverse events, including infections, did not increase with increased duration of study drug exposure or amount of ointment used. In 491 pediatric patients treated with PROTOPIC Ointment, 3(0.6%) developed eczema herpeticum. Since the safety and efficacy of PROTOPIC Ointment have not been established in pediatric patients below 2 years of age, its use in this age group is not recommended.Geriatric UseTwenty-five (25) patients >/= 65 years old received PROTOPIC Ointment in phase 3 studies. The adverse event profile for these patients was consistent with that for other adult patients.ADVERSE REACTIONSNo phototoxicity and no photoallergenicity was detected in clinical studies of 12 and 216 normal volunteers, respectively. One out of 198 normal volunteers showed evidence of sensitization in a contact sensitization study.In three randomized vehicle-controlled studies and two long-term safety studies, 655 and 571 patients respectively, were treated with PROTOPIC Ointment.The following table depicts the adjusted incidence of adverse events pooled across the 3 identically designed 12 week studies for patients in vehicle, PROTOPIC Ointment 0.03%, and PROTOPIC Ointment 0.1% treatment groups, and the unadjusted incidence of adverse events in two one year long-term safety studies, regardless of relationship to study drug.Phase 3 Studies12-Week Adjusted Incidence Rate (%) Tacrolimius Ointment Incidence(%)Adult Pediatric Adult PediatricVehicle n=2120.03%TacrolimusOintmentn=2100.1%TacrolimusOintmentn=209Vehiclen=1160.03%TacrolimusOintmentn=118 n=316 n=255Skin Burning †26 46 58 29 43 47 26 Pruritus †37 46 46 27 41 25 25 Flu-like symptoms †19 23 31 25 28 22 35 Allergic Reaction 8 12 6 8 4 22 15 Skin Erythema 20 25 28 13 12 12 9 Headache †11 20 19 8 5 10 18 Skin Infection 11 12 5 14 10 11 11 Fever 4 4 1 13 21 2 18 Infection 1 1 2 9 7 14 8 Cough Increased 2 1 1 14 18 3 15 Asthma 4 6 4 6 6 5 16 Herpes Simplex 4 4 4 2 0 12 5 Eczema Herpeticum 0 1 1 0 2 2 0 Pharyngitis 3 3 4 11 6 5 10 Accidental Injury 4 3 6 3 6 4 12 Pustular Rash 2 3 4 3 2 6 8 Folliculitis † 1 6 4 0 2 11 2 Rhinitis 4 3 2 2 6 5 5 Otitis Media 4 0 1 6 12 1 7 Sinusitis † 1 4 2 8 3 3 7 Diarrhea 3 3 4 2 5 4 6 Urticaria 3 3 6 1 1 5 5 Lack of Drug Effect 1 1 0 1 1 10 2 Bronchitis 0 2 2 3 3 3 6 Vomiting 0 1 1 7 6 1 5 Maculopapular Rash 2 2 2 3 0 4 3 Rash † 1 5 2 4 2 2 5 Abdominal Pain 3 1 1 2 3 1 5 Fungal Dermatitis 0 2 1 3 0 2 6 Gastroenteritis 1 2 2 3 0 4 2 Alcohol Intolerance †0 3 7 0 0 6 0 Acne † 2 4 7 1 0 2 4 Sunburn 1 2 1 0 0 4 4 Skin Disorder 2 2 1 1 4 1 4 Conjunctivitis 0 2 2 2 1 4 2 Pain 1 2 1 0 1 4 3 Vesiculobullous Rash† 3 3 2 0 4 2 2 Lymphadenopathy 2 2 1 0 3 2 3 Nausea 4 3 2 0 1 1 2 Skin Tingling † 2 3 8 1 2 2 1 Face Edema 2 2 1 2 1 3 1 Dyspepsia † 1 1 4 0 0 1 4Other adverse events which occurred at an incidence greater than or equal to 1% in any clinical study include: alopecia, ALT or AST increased, anaphylactoid reaction, angina pectoris, angioedema, anorexia, anxiety, arrhythmia, arthralgia, arthritis, bilirubinemia, breast pain, cellulitis, cerebrovascular accident, cheilitis, chills, constipation, creatinine increased, dehydration, depression, dizziness, dyspnea, ear pain, ecchymosis, edema, epistaxis, exacerbation of untreated area, eye disorder, eye pain, furunculosis, gastritis, hemia, hyperglycemia, hypertension, hypoglycemia, hypoxia, laryngitis, leukocytosis, leukopenia, liver function tests abnormal, lung disorder, malaise, migraine, neck pain, neuritis, palpitations, paresthesia, peripheral vascular disorder, photosensitivity reaction, procedural complication, routine procedure, skin discoloration, sweating, taste perversion, tooth disorder, unintended pregnancy, vaginal moniliasis, vasodilatation, and vertigo. OVERDOSAGEPROTOPIC Ointment is not for oral use. Oral ingestion of PROTOPIC Ointment may lead to adverse effects associated with systemic administration of tacrolimus. If oral ingestion occurs, medical advice should be sought. DOSAGE AND ADMINISTRATION ADULTPROTOPIC Ointment 0.03% and 0.1%Apply a thin layer of PROTOPIC Ointment 0.03% or 0.1% to the affected skin areas twice daily and rub in gently and completely. Treatment should be continued for one week after clearing of signs and symptoms of atopic dermatitis.The safety of PROTOPIC Ointment under occlusion which may promote systemic exposure, has not been evaluated. PROTOPIC Ointment 0.03% and 0.1% should not be used with occlusive dressings. PEDIATRICPROTOPIC Ointment 0.03%Apply a thin layer of PROTOPIC Ointment 0.03% to the affected skin areas twice daily and rub in gently and completely. Treatment should be continued for one week after clearing of signs and symptoms of atopic dermatitis. The safety of PROTOPIC Ointment under occlusion, which may promote systemic exposure, has not been evaluated. PROTOPIC Ointment 0.03% should not be used with occlusive dressings.Dry Skin 7 3 3 0 1 0 1 Hyperesthesia † 1 3 7 0 0 3 0 Skin Neoplasm Benign ‡‡ 1 1 1 0 0 2 3 Back Pain † 0 2 2 1 1 3 1 Peripheral Edema 2 4 3 0 0 2 1 Varicella Zoster/ Herpes Zoster ‡ 0 1 0 0 5 1 3 Contact Dermatitis 1 3 3 3 4 1 1 Asthenia 1 2 3 0 0 2 1 Pneumonia 0 1 1 2 0 1 2 Eczema 2 2 2 0 0 3 0 Insomnia 3 4 3 1 1 1 0 Exfoliative Dermatitis 3 3 1 0 0 0 2 Dysmenorrhea 2 4 4 0 0 0 2 Periodontal Abscess 1 0 1 0 0 3 0 Myalgia † 0 3 2 0 0 1 0 Cyst †13† May be reasonably associated with the use of this drug product.‡ Four cases of chicken pox in the pediatric 12-week study, 1 case of "zoster of the lip" in the adult 12-week study; 7 cases ofchicken pox and 1 case of shingles in the open-label pediatric study; 2 cases of herpes zoster in the open-label adult study.‡‡ Generally "warts".Patient Information AboutProtopic® (tacrolimus) OintmentRead this important information before you start using PROTOPIC [pro-TOP-ik] Ointment and each time you refill your prescription. There may be new information. This summary is not meant to take the place of your doctor's advice.What is PROTOPIC?PROTOPIC Ointment is a prescription medicine that is used to treat eczema (atopic dermatitis). It is for adults and children age 2 years and older. You can use PROTOPIC for short or intermittent long periods of treatment. Intermittent means starting and stopping repeatedly, as directed by your doctor. You can use it on all affected areas of your skin, including your face and neck.Who should not use PROTOPIC?Do not use PROTOPIC if you arel breastfeedingl allergic to PROTOPIC Ointment or any of its ingredients. The active ingredient is tacrolimus. Ask your doctor or pharmacist about the inactive ingredients.Before you start using PROTOPIC, tell your doctor if you are:l using any other prescription medicines, non-prescription (over-the-counter) medicines, or supplementsl receiving any form of light therapy (phototherapy, UVA or UVB) on your skinl using any other type of skin productl pregnant or planning to become pregnantHow do I use PROTOPIC?Use PROTOPIC only to treat eczema that has been diagnosed by a doctor.l Wash your hands before using PROTOPIC.l Apply a thin layer of PROTOPIC to all skin areas that your doctor has diagnosed as eczema. Try to cover the affected areas completely. Most people find that a pea-sized amount squeezed from the tube covers an area about the size of a two-inchcircle (approximately the size of a silver dollar).l Apply the ointment twice a day, about 12 hours apart.l Before applying PROTOPIC Ointment after a bath or shower, be sure your skin is completely dryl Do not cover the skin being treated with bandages, dressings or wraps. Unless otherwise instructed by your doctor, do not apply another type of skin product on top ofPROTOPIC Ointment. However, you can wear normal clothingl Do not bathe, shower or swim right after applyingPROTOPIC. This could wash off the ointment.l If you are a caregiver applying PROTOPIC Ointment to a patient, or if you are a patient who is not treating your hands, wash your hands with soap and water after applying PROTOPIC. This should remove any ointment left on the hands.l Use PROTOPIC only on your skin. Do not swallowPROTOPIC.Because 2 strengths of PROTOPIC are available for adult patients, your doctor will decide what strength ofPROTOPIC Ointment is best for you.Many people notice that their skin starts to improve after the first few weeks of treatment. Even though your skin looks and feels better, it is important to keep usingPROTOPIC as instructed by your doctor.If you do not notice an improvement in your eczema or if your eczema gets worse within the first few weeks of treatment, tell your doctor.What Should I Avoid While Using PROTOPIC?l Avoid sunlight and sun lamps, tanning beds, and treatment with UVA or UVB light. If you need to be outdoors after applying PROTOPIC, wear loose fitting clothing that protects the treated area from the sun. In addition, ask your doctor what other type of protection from the sun you should use.l Check with your doctor or pharmacist before you¡start taking any new medicines while using PROTOPIC¡start using any other ointment, lotions, or creams on you skinWhat Are The Possible Side Effects of PROTOPIC?。
他克莫司软膏在银屑病治疗中的应用
他克莫司软膏在银屑病治疗中的应用作者:张占平王禄郝勇来源:《中国实用医药》2015年第04期【关键词】他克莫司软膏;非糖皮质激素;银屑病DOI:10.14163/ki.11-5547/r.2015.04.085他克莫司软膏(tacrolimus ointment, FK-506,商品名:普特彼)是最早获批准的非糖皮质激素类外用制剂,其主要成分他克莫司是从链霉菌产物中分离而得的大环内酯类免疫调节剂。
他克莫司软膏最早应用于治疗困难的中至重度特应性皮炎并取得了满意的疗效。
近年来,他克莫司软膏在治疗银屑病中取得了理想的疗效。
本文就他克莫司软膏的药理作用及在银屑病中的临床应用进行综述。
1 他克莫司软膏治疗银屑病的药理机制1984年他克莫司首先由日本研究者Tsukuba [1]从链霉菌发酵培养基中分离得到,是一种大环内酯类抗生素,具有极强的免疫抑制作用,免疫作用是环孢素的数十倍,其分子量较小,局部外用较环孢素更具透皮性。
他克莫司的作用靶目标是T淋巴细胞,通过抑制抗原与T细胞受体(T cell receptor , TCR)结合,后传递给T细胞核的初始信号而阻断 T 细胞激活。
他克莫司通过结合细胞内免疫嗜素 FK 结合蛋白(FK-binding protein, FK-BP),进而阻断钙调神经磷酸酶活化,阻断包括白细胞介素-2(IL-2)的多种细胞因子产生。
银屑病发病机制至今尚不明确,多数研究者认为T细胞的异常活化是其最主要的免疫学发病机制。
他克莫司恰恰是通过抑制T淋巴细胞相关基因的表达而抑制 T 淋巴细胞的活化,阻断了银屑病的发病环节,从而在银屑病的治疗中起作用。
同时,他克莫司还可以抑制皮损中嗜碱粒细胞、嗜酸粒细胞和肥大细胞释放炎性递质[2],而这些炎症介质都参与 T 细胞早期阶段的活化。
同时, FK-506还能通过抑制细胞免疫中郎格罕细胞表面IgE 受体的超量表达,从而阻断 T 细胞的激活和多种细胞因子的产生。
他克莫司软膏的功效与作用

他克莫司软膏的功效与作用他克莫司软膏,是一种广谱抗真菌药物,主要用于治疗皮肤真菌感染引起的病症。
它具有抗菌、杀菌、消炎、止痒等多种功效,对于皮肤真菌感染具有显著的疗效。
下面将详细介绍他克莫司软膏的功效与作用。
他克莫司软膏的主要成分是克霉唑,属于类硝酸酯类抗真菌药物。
该药物经皮肤应用后,能够迅速渗透进入真菌细胞内,通过阻断酵母菌和真菌的细胞膜的合成,干扰其细胞呼吸作用,从而达到杀菌的目的。
同时,他克莫司软膏还具有抗炎和抗过敏作用,能够减轻皮肤炎症和止痒症状。
在临床应用中,他克莫司软膏主要用于治疗各种类型的皮肤真菌感染病症,如白色念珠菌感染、毛癣、体癣、脚癣、股癣等。
白色念珠菌感染是一种常见的真菌感染病症,常见于口腔、阴道、皮肤等部位,使用他克莫司软膏可以有效杀灭白色念珠菌,缓解症状。
毛癣是指身体各部位的脱屑性皮肤病,使用他克莫司软膏可以杀灭病原体,减轻病情。
脚癣主要发生于足部,使用他克莫司软膏可以迅速缓解病情,减少瘙痒和疼痛感。
股癣同样是一种常见的真菌感染,使用他克莫司软膏可以有效杀灭股癣的病原菌,减轻炎症症状。
他克莫司软膏的使用方法比较简单。
首先,清洗感染部位的皮肤,用清水洗净,然后将其涂抹在感染部位,并轻轻按摩,使药物均匀分布。
使用时要注意不要过度涂抹,尽量覆盖感染区域即可,避免过度使用引起药物的浪费。
一般情况下,每日使用2-3次,持续使用2-4周。
很多真菌感染病症常常伴有严重的瘙痒和疼痛感,此时患者可以搭配口服抗过敏药物和止痒药片,以加快症状的缓解。
除了治疗皮肤真菌感染病症,他克莫司软膏还可以用于预防皮肤真菌感染的复发。
皮肤真菌感染病症常常会反复发作,一旦感染复发,就可能对人体健康造成较大的影响。
在感染症状缓解后,患者可以继续使用他克莫司软膏进行预防治疗,减少真菌感染的概率,保持皮肤的清洁和健康。
尽管他克莫司软膏在治疗皮肤真菌感染方面具有显著的疗效,但也存在一些副作用和注意事项。
使用过程中,有可能引起皮肤过敏、刺激等不良反应,一旦出现不良反应,应立即停药,并咨询医生的意见。
普特彼(他克莫司软膏)简要说明书
【普特彼药品名称】
通用名:
他xx软膏
商品名:
普特彼
xx:
TacrolimusOintment
汉语拼音:
TaKeMoSiRuanGao
【普特彼成份】
普特彼主要成份为:
他xx。
【普特彼性状】
普特彼为白色至淡黄色软膏。
【普特彼处方组成】
每克普特彼含他克莫司0.03或0.1(w/w),软膏基质为矿物油、石蜡、碳酸丙烯酯、白凡士林和白蜡。
使用商品时,请仔细阅读说明书,并按说明书使用;如药品,请在医师指导下服用。
【普特彼有效期】
30个月
【普特彼贮藏】
室温25℃保存;允许的温度范围是15-30℃。
【普特彼批准文号】
国内分装批准文号:
国药准字J20148
【普特彼生产企业】
国内分装企业名称:
xxxx制药(xx)有限公司
【
商品图片信息展示仅供参考,最终包装以商品实物为准。欢迎纠错!
说明书内容仅供查阅参考,最终以商品包装内说明书为准。欢迎纠错!
3.患者不应将普特彼用于处方以外的疾病。
4.患者应向医生报告不良反应的症状。
5.沐浴或淋浴后应等皮肤完全干燥后再应用普特彼。
【普特彼药物相互作用】
对普特彼局部应用的药物相互作用未进行过研究。由于吸收量极少,普特彼不太可能与全身性给药的药物发生相互作用,但是也不能完全排除。皮炎较广泛的患者和/或红皮病患者合用已知的CYP3A4抑制剂时应当谨慎,这些药物的例子包括红霉素、伊曲康唑、酮康唑、氟康唑、钙通道阻滞剂和西米替丁等。
【普特彼禁忌】
对他克莫司或制剂中任何其他成分有过敏史的患者禁用普特彼。
【普特彼注意事项】
一般注意事项
[普特彼他克莫司软膏]普特彼(他克莫司软膏)说明书
![[普特彼他克莫司软膏]普特彼(他克莫司软膏)说明书](https://img.taocdn.com/s3/m/291c8c84dbef5ef7ba0d4a7302768e9950e76e56.png)
[普特彼他克莫司软膏]普特彼(他克莫司软膏)说明书篇一: 普特彼说明书通用名称:他克莫司软膏功能主治:适用于因潜在危险而不宜使用传统疗法、或对传统疗法反应不充分、或无法耐受传统疗法的中到重度特应性皮炎患者,作为短期或间歇性长期治疗0.03%和0.1%浓度的本品均可用于成人,但只有0.03%浓度的本品可用于2岁及以上的儿童。
用法用量:成人0.03%和0.1%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
本品不应采用封包敷料外用。
儿童0.03%他克莫司软膏在患处皮肤涂上一薄层本品,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
普特彼不应采用封包敷料外用。
不良反应:临床试验中发生率介于0.2%并小于1%的其它不良事件包括视力异常、脓肿、类过敏反应、贫血、厌食、焦虑、关节炎、关节病、胆红索血症、睑炎、骨失调、乳腺良性增生、粘液礁炎、白内障、胸痛、寒战、大肠炎、结膜水肿、便秘、抽筋、皮肤念珠菌病、膀胱炎、脱水、头昏眼花、干眼、口干/鼻干、呼吸困难、耳部不适、瘀癍、水肿、鼻出血、眼痛、疖病、胃炎、胃肠不适、疝气、高胆固醇血症、渗透压增高、甲状腺机能减退、关节不适、喉炎、白斑病、肺部异常、不适、偏头痛、念珠菌病、口腔溃疡、指甲不适、颈痛、良性肿瘤、口腔念珠菌病、外耳炎、光敏反应、直肠不适、脂溢性皮炎、皮肤癌、皮肤脱色、皮肤过度生长、皮肤溃疡、口腔炎、肌腱不适、思维异常、龋齿、发汗、昏厥、心动过速、味觉异常、意外妊娠、阴道念珠菌病、阴道炎、瓣膜性心脏病、血管扩张、眩晕。
禁忌:对他克莫司或制剂中任何其他成分有过敏史的患者禁用本品。
注意事项:1.患者应在医生的指导下使用本品。
本品仅供外用。
和任何外用药一样,患者或护工在用药后应洗手,如果手部不是治疗区的话。
他克莫司说明书
孚诺(复方多粘菌素B软膏),他克莫司(普特彼)说明书如下:【普特彼药品名称】通用名:他克莫司软膏商品名:普特彼英文名:Tacrolimus Ointment汉语拼音:TaKeMoSiRuanGao【普特彼成份】普特彼主要成份为:他克莫司。
【普特彼性状】普特彼为白色至淡黄色软膏。
【普特彼处方组成】每克普特彼含他克莫司0.03或0.1(w/w),软膏基质为矿物油、石蜡、碳酸丙烯酯、白凡士林和白蜡。
【普特彼药理毒理】药理作用他克莫司治疗特应性皮炎的作用机制还不清楚。
虽然对他克莫司的作用机制已有一定了解,但是这些发现与特应性皮炎的临床关系还不明确。
他克莫司已被证实可以抑制T淋巴细胞活化,首先与细胞内蛋白FKBP-12结合,形成由他克莫司-FKBP-12、钙、钙调蛋白和钙调磷酸酶构成的复合物,从而抑制钙调磷酸酶的磷酸酶活性,阻止活化T细胞核转录因子(NF-AT)的去磷酸化和易位,NF-AT这种核成分会启动基因转录形成淋巴因子(例如IL-2,γ干扰素)。
他克莫司还可以抑制编码IL-3、IL-4、IL-5、GM-CSF和TNF-?的基因的转录,所有这些因子都参与早期阶段的T细胞活化。
此外,他克莫司可以抑制皮肤肥大细胞和嗜碱性粒细胞内已合成介质的释放,下调朗格罕细胞表面FCεRI的表达。
毒理作用在为期26周的大鼠实验和为期28天的家兔实验中,每天外用他克莫司软膏(0.03-1)后,在显微镜下观察到皮肤变化(增生、表皮空泡形成、棘层肥厚、浅表炎症)。
由于这些皮肤变化与他克莫司浓度不相关,也见于赋形剂组,而空白对照组极少见,因而被认为与赋形剂有关而与他克莫司本身无关。
在大鼠中外用高浓度软膏(基本上≥0.3)观察到全身毒性反应,与经口服或静脉摄入后相似。
在为期52周的尤卡坦微型猪局部实验中,肉眼或显微镜下所见的改变均被认为与外用他克莫司(0.03?0.3)无关,因为在赋形剂对照组也观察到同样的改变。
在对豚鼠进行的实验中,他克莫司软膏(0.03?3)不诱发接触过敏或光敏化反应,对白化无毛小鼠也不诱发皮肤光毒性。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
普特彼(他克莫司软膏)说明书【普特彼药品名称】通用名:他克莫司软膏商品名:普特彼英文名:TacrolimusOintment汉语拼音:TaKeMoSiRuanGao【普特彼成份】普特彼主要成份为:他克莫司。
【普特彼性状】普特彼为白色至淡黄色软膏。
【普特彼处方组成】每克普特彼含他克莫司0.03或0.1(w/w),软膏基质为矿物油、石蜡、碳酸丙烯酯、白凡士林和白蜡。
【普特彼药代动力学】综合对49例成年特应性皮炎患者进行的两项药代动力学研究的结果表明,局部应用0.1浓度的普特彼后,他克莫司会被吸收。
单次或多次应用0.1浓度的普特彼后,血中他克莫司峰浓度介于检测不出至20ng/ml之间,49例患者中有45例血药峰浓度值低于5ng/ml。
对20例儿童特应性皮炎患者(年龄6-13岁)进行的药代动力学研究结果表明,应用0.1浓度的普特彼后,所有患者血中他克莫司峰浓度均低于1.6ng/ml。
从血药浓度来看,间歇性局部应用普特彼长达一年也不会导致他克莫司在全身蓄积。
局部应用他克莫司的生物利用度尚不清楚。
以静脉注射他克莫司的历史数据作对比,特应性皮炎患者局部应用普特彼的相对生物利用度低于0.5。
在平均治疗体表面积(BSA)达53的成人中,局部应用普特彼后的吸收量(即AUC)约比肾或肝移植患者将他克莫司作为免疫抑制剂口服的吸收量低30倍。
能引起全身性作用的他克莫司血药浓度目前尚不清楚。
【普特彼适应症】普特彼适用于因潜在危险而不宜使用传统疗法、或对传统疗法反应不充分、或无法耐受传统疗法的中到重度特应性皮炎患者,作为短期或间歇性长期治疗。
0.03和0.1浓度的普特彼均可用于成人,但只有0.03浓度的普特彼可用于2岁及以上的儿童。
【普特彼用法用量】成人0.03和0.1他克莫司软膏在患处皮肤涂上一薄层普特彼,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
普特彼不应采用封包敷料外用。
儿童0.03他克莫司软膏在患处皮肤涂上一薄层普特彼,轻轻擦匀,并完全覆盖,一天两次,持续至特应性皮炎症状和体征消失后一周。
封包疗法可能会促进全身性吸收,其安全性未进行过评价。
普特彼不应采用封包敷料外用。
【普特彼不良反应】在分别有12例和216例健康志愿者参加的临床研究中,未发现药物具有光毒性和光致敏性。
在对198例健康志愿者进行的接触致敏研究中,有一例出现接触致敏的迹象。
在三项随机赋形剂对照研究和两项长期安全性研究中,分别有655例和571例患者接受了普特彼治疗。
下表列举了三项设计相同、为期12周研究中、赋形剂组、0.03和0.1浓度的普特彼治疗组校正后不良事件发生率,以及两项长达一年的安全性研究中未经校正的不良事件发生率,不考虑这些不良事件是否与研究药物有关。
儿童12周研究中共发生4例水痘;成人12周研究中有1例出现唇部带状疱疹;儿童开放性研究中发生7例水痘和1例带状疱疹;成人开放性研究中发生2例带状疱疹。
在各种临床试验中发生率大于或等于1的其它不良事件包括秃发、ALT或AST升高、过敏样反应、心绞痛、血管神经性水肿、厌食、焦虑、心律失常、关节痛、关节炎、胆红素血症、乳房疼痛、蜂窝组织炎、脑血管意外、唇炎、寒颤、便秘、肌酐升高、脱水、抑郁、头晕、呼吸困难、耳痛、皮肤瘀斑、水肿、鼻出血、未治疗部位病情加重、眼部不适、眼痛、疖肿、胃炎、疝气、高血糖症、高血压、低血糖症、缺氧、喉炎、白细胞增多症、白细胞减少、肝功能试验异常、肺部疾病、全身不适、偏头痛、颈部疼痛、神经炎、心悸、感觉异常、外周血管异常、光敏反应、处理过程的并发症、皮肤脱色、出汗、味觉异常、牙齿疾病、意外妊娠、阴道念珠菌病、血管扩张和眩晕。
【普特彼禁忌】对他克莫司或制剂中任何其他成分有过敏史的患者禁用普特彼。
【普特彼注意事项】一般注意事项普特彼在临床上对感染性特应性皮炎的安全性和有效性未进行过评价。
在开始使用普特彼治疗前,应首先清除治疗部位的感染灶。
特应性皮炎患者易患浅表皮肤感染,包括疱疹性湿疹(卡波济水痘样疹),使用普特彼治疗可能会增加带状疱疹病毒感染(水痘或带状疱疹)、单纯疱疹病毒感染或疱疹性湿疹发生的风险。
如果存在这些感染,应对普特彼治疗的利益与风险的平衡进行评估。
在临床研究中报告了33例淋巴结病(占0.8)通常与感染有关(尤其是皮肤感染),在给予相应抗生素治疗后缓解。
这33例患者中大多数有明确的病因,或终消退。
接受免疫抑制剂治疗(例如全身性使用他克莫司)的器官移植患者发生淋巴瘤的危险性增加,因此,接受普特彼治疗并出现淋巴结病的患者应调查其淋巴结病的病因。
如果没有明确找到淋巴结病的病因,或患者同时患有急性传染性单核细胞增多症,应考虑中断使用普特彼。
对发生淋巴结病的患者应进一步观察以确保淋巴结病消退。
紫外线致癌作用的增强不一定依赖于光毒性作用机制。
尽管没有观察到对人体的光毒性(参见不良反应),但在一项动物光致癌性研究中,普特彼缩短了皮肤肿瘤发生的时间(见非临床毒理研究)。
因此,患者应尽量减少或避免自然光或人工光源照射。
外用普特彼可能会引起局部症状,如皮肤烧灼感(灼热感、刺痛、疼痛)或瘙痒。
局部症状常见于使用普特彼的初几天,通常会随着特应性皮炎受累皮肤好转而消失。
应用0.1浓度的普特彼治疗时,90的皮肤烧灼感持续时间介于2分钟至3小时(中位时间为15分钟)之间,90的瘙痒症状持续时间介于3分钟至10小时(中位时间为20分钟)之间。
不推荐使用普特彼治疗Netherton综合征患者,因为可能会增加他克莫司的全身性吸收。
普特彼对弥漫性红皮病患者治疗的安全性尚未建立。
患者须知使用普特彼的患者应接受下列信息和指导:1.患者应在医生的指导下使用普特彼。
普特彼仅供外用。
和任何外用药一样,患者或护工在用药后应洗手,如果手部不是治疗区的话。
2.在使用普特彼期间,患者应减少或避免自然阳光或人工太阳光(晒床或UVA/UVB治疗)。
3.患者不应将普特彼用于处方以外的疾病。
4.患者应向医生报告不良反应的症状。
5.沐浴或淋浴后应等皮肤完全干燥后再应用普特彼。
【普特彼药物相互作用】对普特彼局部应用的药物相互作用未进行过研究。
由于吸收量极少,普特彼不太可能与全身性给药的药物发生相互作用,但是也不能完全排除。
皮炎较广泛的患者和/或红皮病患者合用已知的CYP3A4抑制剂时应当谨慎,这些药物的例子包括红霉素、伊曲康唑、酮康唑、氟康唑、钙通道阻滞剂和西米替丁等。
【普特彼孕妇及哺乳期妇女用药】致畸作用:妊娠用药分级C目前还未对妊娠妇女局部应用普特彼进行过足够的适当对照的研究。
普特彼用于怀孕妇女的经验也非常有限,尚不足以对其在妊娠期间应用的安全性进行评价。
对大鼠和家兔进行过全身性服用他克莫司的生殖毒性研究,当给母体口服毒性剂量的药物时胎儿产生不良反应。
在胚胎器官形成阶段给家兔口服剂量为0.32和1.0mg/kg的他克莫司(以体表面积计,分别相当于人用推荐剂量的0.04和0.12倍),对母兔产生毒性反应,而且流产率升高。
只是在更高剂量组见到有胎儿畸形和发育异常的比例升高。
在胚胎器官形成阶段给大鼠口服剂量为3.2mg/kg的他克莫司,对母鼠产生毒性反应,并导致后期再吸收增加、产活胎数量减少、幼鼠体重和发育能力降低。
在过了胚胎器官形成期后以及在哺乳期间,给妊娠大鼠口服1.0和3.2mg/kg(以体表面积计,相当于人用推荐剂量的0.04和0.12倍)的他克莫司,可导致幼鼠体重下降。
未见到雄性或雌性动物生殖能力降低。
未对妊娠妇女全身性应用他克莫司进行过适当对照的研究。
他克莫司可通过胎盘,在妊娠期间全身性服用他克莫司会导致新生儿高血钾和肾功能紊乱。
在妊娠期间只有在治疗对母亲的益处大于对胎儿的潜在危害时,才能使用普特彼。
虽然局部应用普特彼后他克莫司的全身吸收相对于全身性用药来说极少,但已知他克莫司可分泌至乳汁。
由于可能会对哺乳婴儿造成严重不良反应,因此应根据药物治疗对母亲的重要性来决定是停止哺乳还是停止用药。
【普特彼儿童用药】0.03浓度的普特彼可用于2岁及以上的儿童患者。
已经进行的两项III期儿科临床研究共有606例年龄在2-15岁的患者参加:一项为12周随机赋形剂对照的研究,另一项为为期一年的开放式长期安全性研究,其中有330例患者年龄在2-6岁之间。
儿童患者应用普特彼常见的不良反应是皮肤灼热感和瘙痒(见不良反应)。
除此之外,与赋形剂相比,接受0.03浓度的普特彼治疗的患者发生较少见的(发生率小于5)不良事件如带状疱疹(主要是水痘)和囊疱疹的频度更高。
在为期一年的长期安全性研究中,共有255例儿童患者接受普特彼治疗,不良事件(包括感染)的发生率并没有随用药时间的延长或用药剂量的增加而增加。
在接受普特彼治疗的491例儿童患者中,3例(占0.6)出现疱疹性湿疹。
由于普特彼在2岁以下儿童患者中的安全性和疗效尚未确立,因此不推荐该年龄组患者使用普特彼。
【普特彼老年患者用药】在III期临床试验中,有25例年龄在65岁及以上的患者接受了普特彼治疗。
这些患者发生不良事件的情况与其它成年患者一致。
【普特彼药物过量】普特彼不能用于口服。
口服普特彼可出现与全身性应用他克莫司相关的不良反应。
一旦误服,应寻求医生帮助。
【普特彼规格】30g:9mg(0.03);30g:30mg(0.1);10g:3mg(0.03);10g:10mg(0.1)【普特彼有效期】30个月【普特彼贮藏】室温25℃保存;允许的温度范围是15-30℃。
【普特彼批准文号】国内分装批准文号:国药准字J20140148【普特彼生产企业】国内分装企业名称:安斯泰来制药(中国)有限公司【康德乐大药房友情提示】商品图片信息展示仅供参考,最终包装以商品实物为准。
欢迎纠错!说明书内容仅供查阅参考,最终以商品包装内说明书为准。
欢迎纠错!使用商品时,请仔细阅读说明书,并按说明书使用;如药品,请在医师指导下服用。