高血压英文PPT精品课件Antihypertensive
合集下载
高血压(英文版) ppt课件

Hypertension
Introduction
Hypertension is a major public health problem throughout the world because of its high prevalence and its association with increased risk of cardiovascular disease.
<90
130140-159 140-149
Epidemiology
Prevalence rate ( 患 病 率 ) China: In 1959, In 1979, 5.11% 7.73% of hypertension in
In 1991,
11.88%
The prevalence of high BP increases with age. Hypertension is more common in men than in women up to age 50, after that age, hypertension is more common in women. Hypertension is more common in northern China than in southern China.
For instance:
21/3 1st visit: 146/98mmHg, 150/98mmHg 23/3 2nd visit: 128/84, 126/80
27/3 3rd visit: 130/80, 130/82
Notes(continue)
4. Optimal BP with respect to cardiovascular risk is less than 120/80 mmHg. However, unusually low readings should be evaluated for clinical significance. For example, 70/50 mmHg is less than 120/80 mmHg, but it is not optimal.
Introduction
Hypertension is a major public health problem throughout the world because of its high prevalence and its association with increased risk of cardiovascular disease.
<90
130140-159 140-149
Epidemiology
Prevalence rate ( 患 病 率 ) China: In 1959, In 1979, 5.11% 7.73% of hypertension in
In 1991,
11.88%
The prevalence of high BP increases with age. Hypertension is more common in men than in women up to age 50, after that age, hypertension is more common in women. Hypertension is more common in northern China than in southern China.
For instance:
21/3 1st visit: 146/98mmHg, 150/98mmHg 23/3 2nd visit: 128/84, 126/80
27/3 3rd visit: 130/80, 130/82
Notes(continue)
4. Optimal BP with respect to cardiovascular risk is less than 120/80 mmHg. However, unusually low readings should be evaluated for clinical significance. For example, 70/50 mmHg is less than 120/80 mmHg, but it is not optimal.
《高血压英语》课件

了解高血压可能导致的一些严重健康问题,如心脏病、中风和肾脏问题。
预防与治疗
饮食
了解如何通过健康的饮食来预防和管理高血压。
减肥
了解如何通过控制体重来降低高血压的风险。
运动
探索适合高血压患者的运动方式,以维持健康。
药物治疗
介绍高血压的常用药物和治疗选项。
与高血压相关的英语词汇
1 血压
了解血压的定义和测量方 式。
2 心脏
探索心脏的结构和功能, 以及它与高血压之间的关 系。
ห้องสมุดไป่ตู้
3 动脉
了解动脉的作用和与高血 压的相关性。
4 血管
了解血管的结构和功能,以及其在高血压中 的角色。
5 测量血压的工具
介绍用于测量血压的不同工具和设备。
医生的面诊
了解在与医生交流时使用的常见英语表达,如病症描述和治疗方案。
处理心理问题
1
《高血压英语》PPT课件
# 高血压英语PPT课件 探索高血压的定义,症状和风险。了解如何预防和治疗高血压以及相关的英 语词汇。
什么是高血压?
高血压是一种常见的健康问题,也称为高血压。了解什么是高血压以及它对 身体的影响。
高血压的症状
探索高血压可能引起的一些常见症状,如头痛、头晕和呼吸困难。
高血压的风险
被诊断出患有高血压的心理反应
了解当你被诊断出患有高血压时可能出现的心理反应。
2
减轻心理负担的方法
探索如何通过积极的心理策略来减轻与高血压相关的心理负担。
3
支持小组
介绍参加支持小组的好处,并了解如何加入。
总结
高血压的关键知识点
简要回顾高血压的关键知识点, 以加强理解。
处理高血压的英语技能
预防与治疗
饮食
了解如何通过健康的饮食来预防和管理高血压。
减肥
了解如何通过控制体重来降低高血压的风险。
运动
探索适合高血压患者的运动方式,以维持健康。
药物治疗
介绍高血压的常用药物和治疗选项。
与高血压相关的英语词汇
1 血压
了解血压的定义和测量方 式。
2 心脏
探索心脏的结构和功能, 以及它与高血压之间的关 系。
ห้องสมุดไป่ตู้
3 动脉
了解动脉的作用和与高血 压的相关性。
4 血管
了解血管的结构和功能,以及其在高血压中 的角色。
5 测量血压的工具
介绍用于测量血压的不同工具和设备。
医生的面诊
了解在与医生交流时使用的常见英语表达,如病症描述和治疗方案。
处理心理问题
1
《高血压英语》PPT课件
# 高血压英语PPT课件 探索高血压的定义,症状和风险。了解如何预防和治疗高血压以及相关的英 语词汇。
什么是高血压?
高血压是一种常见的健康问题,也称为高血压。了解什么是高血压以及它对 身体的影响。
高血压的症状
探索高血压可能引起的一些常见症状,如头痛、头晕和呼吸困难。
高血压的风险
被诊断出患有高血压的心理反应
了解当你被诊断出患有高血压时可能出现的心理反应。
2
减轻心理负担的方法
探索如何通过积极的心理策略来减轻与高血压相关的心理负担。
3
支持小组
介绍参加支持小组的好处,并了解如何加入。
总结
高血压的关键知识点
简要回顾高血压的关键知识点, 以加强理解。
处理高血压的英语技能
高血压(英文版) ppt课件
arteriole structure Compliance of Vessel wall
ppt课件 6
Psychological factors Renin –angiotensin aldosterone system(RAAS) Sodium and hypertension Abnormality of vascular endothelium(ET,NO, AngII, PGI2, etc) Insulin resistance revascularization other(obesity,smoking,drinking,hypocalcium, hypomagnesium, hypopotassium)
Heart failure Systolic hypertension 长效) Diabetes, proteinuria Renal insufficiency(mild) Myocardial infarction ACEI Stable angina Disorder of lipid pregnancy Prostate proliferation
ppt课件
12
Risk factor of cardiovascular disease
male > 55, female> 65 smoking Total cholesterol> 5.72mmol/L (250mg/dl) diabetes Early cardiovascular family history(early onset of CV disease male<55;female <65)
Diuretics ß–blocker a-blocker Calcium channel blocker ACE inhibitor Angiotensin II receptor blocker compound anti-hypertensive agents
高血压(英文版) ppt课件
Etiology and pathogenesis of EH
No
cause can be established Possible mechanisms Genetic tendency
Spontaneous hypertension rat EH tends to cluster in families
Classification of Blood Pressure Levels (mmHg)
Category Systolic Diastolic Hypotension??? <60 Optimal <120 <80 Normal <130 <85 High-normal 139 85-89 Grade 1 hypertension(mild) 90-99 Subgroup: borderline 90-94
Optional investigations
Plasma renin( 肾 素 ) activity & aldosterone (醛固酮), urinary VMA(香草杏仁酸),to identify secondary hypertension Echocardiography, to detect ventricular hypertrophy Vascular ultrasonography should be performed if arterial disease is suspected. Renal ultrasonography should be performed if renal disease is suspected.
perhaps by catecholamines儿茶酚胺
高血压英文PPT精品课件HYPERTENSIONDIABETESADANGEROUS
IL- 6, TNF- @, and RAS
liver(NASH)
(↑CRP) (Endothelial
Dysfunction)
• ↑Small, dense LDL • ↑triglyceridemia
Atherosclosis
Activation • ↓HDL
Reduced • Hypertension
Renal Na+ Reabsorption
Hypertension
Cardiometabolic Syndrome:
Large
(Insulin resistant) ( ↑Central Fat)
Fat Cells
(Fatty
Visceral Obesity
Enhanced
Lipolysis > FreeFA
Millions of Cases
60 50 40 30 20 10
0
India
China
1995 2025
US
Data from King H et al. Diabetes Care. 1998;21:1414-1431.
CV Mortality Risk Doubles with Each 20/10 mm Hg BP Increment*
<200 mg/dL (5.18 mmol/L)
Vascular Disease Risk Factors
Saydah SH et al. JAMA. 2004;291:335-342.
Metabolic Syndrome: NCEP/ATP III Definition
Presence of at least 3 of 5 risk factors: Abdominal obesity Elevated blood pressure Elevated fasting glucose Elevated triglycerides Low HDL-C
liver(NASH)
(↑CRP) (Endothelial
Dysfunction)
• ↑Small, dense LDL • ↑triglyceridemia
Atherosclosis
Activation • ↓HDL
Reduced • Hypertension
Renal Na+ Reabsorption
Hypertension
Cardiometabolic Syndrome:
Large
(Insulin resistant) ( ↑Central Fat)
Fat Cells
(Fatty
Visceral Obesity
Enhanced
Lipolysis > FreeFA
Millions of Cases
60 50 40 30 20 10
0
India
China
1995 2025
US
Data from King H et al. Diabetes Care. 1998;21:1414-1431.
CV Mortality Risk Doubles with Each 20/10 mm Hg BP Increment*
<200 mg/dL (5.18 mmol/L)
Vascular Disease Risk Factors
Saydah SH et al. JAMA. 2004;291:335-342.
Metabolic Syndrome: NCEP/ATP III Definition
Presence of at least 3 of 5 risk factors: Abdominal obesity Elevated blood pressure Elevated fasting glucose Elevated triglycerides Low HDL-C
高血压英语PPTPPT课件

Blood pressure readings of 180/110 mmHg or higher
Headache
Vision changes
Shortness of Breath
Fatigue
Dizziness
Chest pain or discomfort
01
02
03
04
05
06
Symptoms of Hypertension
Mental stress
Sleep quality
Chronic stress
03
The HAZARDS of Hypertension
Increased risk of heart disease
High blood pressure can damage the heart muscle, leading to heart disease
Hypertension English PPT courseware
contents
目录
Introduction to Hypertension The causes of hypertension The HAZARDS of Hypertension Diagnosis and prevention of hypertension
Diagnostic method
ቤተ መጻሕፍቲ ባይዱ
Preventive measure
Healthy die: A balanced die rich in fruits, vegetables, whole grains, and lean protein can help reduce blood pressure Limiting salt and reducing intake of saturated fat and trans fat are also important
Headache
Vision changes
Shortness of Breath
Fatigue
Dizziness
Chest pain or discomfort
01
02
03
04
05
06
Symptoms of Hypertension
Mental stress
Sleep quality
Chronic stress
03
The HAZARDS of Hypertension
Increased risk of heart disease
High blood pressure can damage the heart muscle, leading to heart disease
Hypertension English PPT courseware
contents
目录
Introduction to Hypertension The causes of hypertension The HAZARDS of Hypertension Diagnosis and prevention of hypertension
Diagnostic method
ቤተ መጻሕፍቲ ባይዱ
Preventive measure
Healthy die: A balanced die rich in fruits, vegetables, whole grains, and lean protein can help reduce blood pressure Limiting salt and reducing intake of saturated fat and trans fat are also important
抗高血压药_英文版PPT参考幻灯片

ACEI
Small artery contraction losartan
Aldosterone secretion Water sodium retention diuretic (thiazides)
Classification
Diuretic The sympathetic nervous depressants (1) central blood pressure medication (2) the ganglion block (3) noradrenaline can nerve endings block (4) the adrenaline receptor blockers Affect the renin - angiotensin system medicine
antihypertensive effect is mild, persistent, long-term application of no significant resistance
Features:
Antihypertensive effect is weak, by an average of 10% 2 ~ 3 weeks after the majority of patients in medical work Can be used for various high blood pressure (basic blood pressure medication) Mild - alone, medium and severe - shห้องสมุดไป่ตู้re Can make the elderly hypertension patients complicated with stroke, the incidence of
Small artery contraction losartan
Aldosterone secretion Water sodium retention diuretic (thiazides)
Classification
Diuretic The sympathetic nervous depressants (1) central blood pressure medication (2) the ganglion block (3) noradrenaline can nerve endings block (4) the adrenaline receptor blockers Affect the renin - angiotensin system medicine
antihypertensive effect is mild, persistent, long-term application of no significant resistance
Features:
Antihypertensive effect is weak, by an average of 10% 2 ~ 3 weeks after the majority of patients in medical work Can be used for various high blood pressure (basic blood pressure medication) Mild - alone, medium and severe - shห้องสมุดไป่ตู้re Can make the elderly hypertension patients complicated with stroke, the incidence of
英文疾病介绍——Hypertension(高血压病)ppt课件
Hypertension
英文疾病介绍——Hypertension(高血压病)
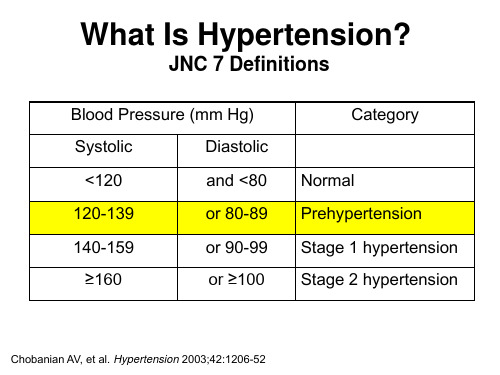
What Is Hypertension?
➢Hypertension (HTN) is a chronic medical condition in which the blood pressure in the arteries is elevated(提高的).
In fact, one in five people with the condition don‘t know they have it. Internally([ɪnˈtɜ:nəlɪ],在体内地), it can quietly damage the heart, lungs, blood ve英ss文e疾l病s,介b绍r—a—inH,ypaerntednsiokni(d高n血e压y病s) if left untreated. It’s a major risk factor for strokes(中风/脑卒中) and heart attacks(心脏病).
Who is at risk?
➢ Anyone can have high blood pressure. Some people are more likeressure including:
• African Americans(more sensitive to salt) • People over age 55 • People with a family history of high blood pressure
Malignant Hypertension
(Chronic Hypertension)
(Accelerated Hypertension)
英文疾病介绍——Hypertension(高血压病)
What Is Hypertension?
➢Hypertension (HTN) is a chronic medical condition in which the blood pressure in the arteries is elevated(提高的).
In fact, one in five people with the condition don‘t know they have it. Internally([ɪnˈtɜ:nəlɪ],在体内地), it can quietly damage the heart, lungs, blood ve英ss文e疾l病s,介b绍r—a—inH,ypaerntednsiokni(d高n血e压y病s) if left untreated. It’s a major risk factor for strokes(中风/脑卒中) and heart attacks(心脏病).
Who is at risk?
➢ Anyone can have high blood pressure. Some people are more likeressure including:
• African Americans(more sensitive to salt) • People over age 55 • People with a family history of high blood pressure
Malignant Hypertension
(Chronic Hypertension)
(Accelerated Hypertension)
高血压英文PPT精品课件_3
BPLTTC Meta-analysis: Stroke and CHD
Relative Risk of Stroke Relative Risk of CHD
Stroke
1.50
CHD
1.50
1.25
1.25
1.00
1.00
0.75
0.75
0.50
0.50
0.25
0.25
-10 -8 -6 -4 -2 0 2 4
2 mm Hg decrease in mean SBP
7% reduction in risk of CHD mortality
10% reduction in risk of stroke mortality
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913.
No Compelling Indications
Stage 1 140-159/90-99 Diuretics for most;
consider ACEI, ARB, B, CCB
Stage 2 BP 160/100 2-drug combo for
most (diuretic + ACEI, or ARB, or BB, or CCB)
What Is Hypertension?
JNC 7 Definitions
Blood Pressure (mm Hg)
Systolic
Diastolic
<120
and <80
120-139
or 80-89
140-159
or 90-99
≥160
高血压英文PPT精品课件HYPERTENSIVE

In Young ...
Protein C levels Protein S levels Platelet Analysis Sr. & Urine for Homocysteine levels
Others ...
Hb Electrophoresis PT / PTT Anti-Phospholipid antibody Complete Cardiovascular evaluation
Microaneurysyms Optociliary vessels – collaterals between retinal & ciliary
vessels
Cilioretinal artery occlusion
Combined with CRVO
Cilioretinal artery occlusion
• HRVO (Hemi Retinal Vein Occlusion)
• BRVO (Branch Retinal Vein Occlusion) Constitutes 69.5 % of all RVO cases
CRVO ...
Classic Appearance
Mildest Form
CRVO
Combined with anterior ischaemic optic neuropathy
HRVO ...
HRVO ...
Superior & Inferior vein do not merge into Central Vein before entering into lamina cribrosa
Traditional Rx Options ...
高血压英文PPT精品课件HYPERTENSIVE
GRADE 2 HTR
SEVERE GENERALIZED AND FOCAL ARTERIOLAR CONSTRICTION
A-V CROSSING CHANGES (SALUS SIGN)
GRADE 3 HTR
Copper wiring of arterioles Venous banking distal to A-V
the arterial & venous circulation
Green et al – Thrombus formation in the region of lamina cribrosa is the primary event
GRADE 4 HTR
All changes of grade 3
Silver wiring of arterioles
Disc edema
Ocular associations of hypertension
Retinal vein occlusion
• CRVO (Central Retinal Vein Occlusion)
crossing (bonnet’s sn) Venous tapering on either
side of crossing (gunn’s sn) Right angle deflection of
veins. Flame shaped hemorrhages
cotton wool spots, hard exudates.
• HRVO (Hemi Retinal Vein Occlusion)
• BRVO (Branch Retinal Vein Occlusion) Constitutes 69.5 % of all RVO cases
相关主题
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
• Diagnosis is generally based on repeated, reproducible measurements of elevated blood pressure and not on patient symptoms. Patient compliance is a major obstacle to therapy
Kidney
Na loss
Thiazides
Summary of Long Term Renal Control of BP
Regulates BP by Changing:
1.
Directly – by allowing more or less fluid to enter kidney tubules
• Pakistan (NHSP):the prevalence of hypertension is 17.9%
• 24% of the USA adult population representing 43,186,000 persons had hypertension.
Diagnosis
CNS
BV
Na retention Clonidine
CO
Venous tone
NE release
Sympathetic tone
TPR
Arteriolar tone
dry mouth sexual dysfunction
The left ventricle is markedly thickened in this patient with severe hypertension that was untreated for many years. The myocardial fibers have undergone hypertrophy.
• idiopathic process (primary or essential
hypertension) In 95% of cases
பைடு நூலகம்
AP
Compensatory reflexes (pseudo-tolerance)
renin / ang II / aldo
Sedation Depression
monotherapy:
✓ Renin status ✓ Coexisting cardiovascular conditions ✓ Other conditions
Homeostasis of Blood Pressure
No Image
Determinants of arterial pressure
Direct
Pressure Diuresis
Blood volume too high, Renal Sympathetic vasoconstriction reduced More fluid enters kidney, more urine formed Lowers BP via lower blood volume
Ways of Lowering Blood Pressure
MAP = CO X TPR
• Reduce cardiac output (ßblockers, Ca2+ channel blockers)
• Reduce plasma volume (diuretics)
• Reduce peripheral vascular resistance (vasodilators)
BV
Na loss K retention
Kidney Aldosterone secretion
Sympathetic nervous control
Treatm ent w ith thiazide (10 days) sBP dBP BV TPR CO
PRA
TIM E
Long-term Renal Control of BP:
AP = CO x TPR
• Each of these factors can be manipulated by drug therapy
Treatment of hypertension seeks to lower CO
For Short-Term Neural Control
Baroreceptor reflex
"Individualized Care"
• Risk factors considered • Monotherapy is instituted • Non pharmacological therapy tried first • Considerations for choice of initial
Stages of Hypertension
Stage
High Normal Stage 1
Stage 2
Diastolic Range (mm Hg) 85-89
90-99
100-109
Systolic Range (mm Hg) 130-139
140-159
160-179
Stage 3
> 109
Indirectly – Reabsorbing more fluid that was already destined to be urine
2. Vasoconstriction / vasodilation
MAJOR ANTIHYPERTENSIVE DRUGS
1) Diuretics - Thiazides and congeners. - Loop diuretics. - Potassium-sparing diuretics. 2) Sympatholytic drugs - Centrally acting antiadrenergic agents. - Adrenergic neuron blocking agents. - Alpha adrenergic blockers. - Beta adrenergic blockers. - Alpha-beta adrenergic blockers. 3) Vasodilators - Nitric oxide releasers. - Potassium channel openers. - Calcium channel blockers. 4) Angiotensin inhibitors and antagonists. - Angiotensin Converting Enzyme (ACE) inhibitors. - Angiotensin receptor antagonists.
If BP too low, increase BP by increasing __________
Kidney cells secrete _______ Converts angiotensinogen to angiotensin I _______________________in lung converts
AP
venous tone neg inotropic effect
TPR
BV
ACEI
Renin
AI x AII
Reduced SND and NE release
Arteriolar relaxation Na loss
Kidney
Bradykinin
Na loss
Kidney
K retention
Aldosterone secretion
Figure 15-22
AP
Compensatory reflexes
Sympathoactivation
Cardiac rate Cardiac output
renin / ang / aldo
BETA-BLOCKER
Renin
AI
AII
Na loss Kidney
• an underlying disease process: In 510% a cause can be found
• (secondary hypertension)
• Renal artery stenosis • Hyperaldosteronism • pheochromocytoma
Major Risk Factors That Increase Mortality in Hypertension
• Smoking • Dyslipidemias • Diabetes Mellitus • Age >60 • Gender: men, postmenopausal women • Family history
Sit or stand up quickly, BP falls neural responses reestablish normal BP
or Sudden increase in stroke volume, BP rises, neural responses reestablish normal BP
Sympathoactivation
Kidney/ang/aldo
CO
Cardiac contractility Cardiac rate
Na retention
TPR
Figure 15-9
Arteriolar relaxation
Dihydropyridine
Renal Control of BP: Indirect
>179
Treatment Rationale
Long-term goal of antihypertensive therapy:
Kidney
Na loss
Thiazides
Summary of Long Term Renal Control of BP
Regulates BP by Changing:
1.
Directly – by allowing more or less fluid to enter kidney tubules
• Pakistan (NHSP):the prevalence of hypertension is 17.9%
• 24% of the USA adult population representing 43,186,000 persons had hypertension.
Diagnosis
CNS
BV
Na retention Clonidine
CO
Venous tone
NE release
Sympathetic tone
TPR
Arteriolar tone
dry mouth sexual dysfunction
The left ventricle is markedly thickened in this patient with severe hypertension that was untreated for many years. The myocardial fibers have undergone hypertrophy.
• idiopathic process (primary or essential
hypertension) In 95% of cases
பைடு நூலகம்
AP
Compensatory reflexes (pseudo-tolerance)
renin / ang II / aldo
Sedation Depression
monotherapy:
✓ Renin status ✓ Coexisting cardiovascular conditions ✓ Other conditions
Homeostasis of Blood Pressure
No Image
Determinants of arterial pressure
Direct
Pressure Diuresis
Blood volume too high, Renal Sympathetic vasoconstriction reduced More fluid enters kidney, more urine formed Lowers BP via lower blood volume
Ways of Lowering Blood Pressure
MAP = CO X TPR
• Reduce cardiac output (ßblockers, Ca2+ channel blockers)
• Reduce plasma volume (diuretics)
• Reduce peripheral vascular resistance (vasodilators)
BV
Na loss K retention
Kidney Aldosterone secretion
Sympathetic nervous control
Treatm ent w ith thiazide (10 days) sBP dBP BV TPR CO
PRA
TIM E
Long-term Renal Control of BP:
AP = CO x TPR
• Each of these factors can be manipulated by drug therapy
Treatment of hypertension seeks to lower CO
For Short-Term Neural Control
Baroreceptor reflex
"Individualized Care"
• Risk factors considered • Monotherapy is instituted • Non pharmacological therapy tried first • Considerations for choice of initial
Stages of Hypertension
Stage
High Normal Stage 1
Stage 2
Diastolic Range (mm Hg) 85-89
90-99
100-109
Systolic Range (mm Hg) 130-139
140-159
160-179
Stage 3
> 109
Indirectly – Reabsorbing more fluid that was already destined to be urine
2. Vasoconstriction / vasodilation
MAJOR ANTIHYPERTENSIVE DRUGS
1) Diuretics - Thiazides and congeners. - Loop diuretics. - Potassium-sparing diuretics. 2) Sympatholytic drugs - Centrally acting antiadrenergic agents. - Adrenergic neuron blocking agents. - Alpha adrenergic blockers. - Beta adrenergic blockers. - Alpha-beta adrenergic blockers. 3) Vasodilators - Nitric oxide releasers. - Potassium channel openers. - Calcium channel blockers. 4) Angiotensin inhibitors and antagonists. - Angiotensin Converting Enzyme (ACE) inhibitors. - Angiotensin receptor antagonists.
If BP too low, increase BP by increasing __________
Kidney cells secrete _______ Converts angiotensinogen to angiotensin I _______________________in lung converts
AP
venous tone neg inotropic effect
TPR
BV
ACEI
Renin
AI x AII
Reduced SND and NE release
Arteriolar relaxation Na loss
Kidney
Bradykinin
Na loss
Kidney
K retention
Aldosterone secretion
Figure 15-22
AP
Compensatory reflexes
Sympathoactivation
Cardiac rate Cardiac output
renin / ang / aldo
BETA-BLOCKER
Renin
AI
AII
Na loss Kidney
• an underlying disease process: In 510% a cause can be found
• (secondary hypertension)
• Renal artery stenosis • Hyperaldosteronism • pheochromocytoma
Major Risk Factors That Increase Mortality in Hypertension
• Smoking • Dyslipidemias • Diabetes Mellitus • Age >60 • Gender: men, postmenopausal women • Family history
Sit or stand up quickly, BP falls neural responses reestablish normal BP
or Sudden increase in stroke volume, BP rises, neural responses reestablish normal BP
Sympathoactivation
Kidney/ang/aldo
CO
Cardiac contractility Cardiac rate
Na retention
TPR
Figure 15-9
Arteriolar relaxation
Dihydropyridine
Renal Control of BP: Indirect
>179
Treatment Rationale
Long-term goal of antihypertensive therapy: