病理学-免疫性疾病
免疫病理学的基本原理与常见免疫性疾病
免疫病理学的基本原理与常见免疫性疾病免疫病理学是研究免疫系统在疾病发生、发展和治疗中的基本原理的学科。
它涉及到免疫系统的结构,功能以及免疫反应对于疾病发展的影响。
本文将介绍免疫病理学的基本原理,并探讨一些常见的免疫性疾病。
一、免疫病理学的基本原理1. 免疫系统的结构和组成免疫系统主要包括器官(如脾脏、淋巴结、扁桃体等)和细胞(如淋巴细胞、巨噬细胞等)。
这些组织和细胞相互配合,为机体提供免疫功能。
2. 免疫系统的功能免疫系统具有识别、清除和记忆等功能。
它能够识别外来抗原,并通过产生抗体和激活免疫细胞清除这些抗原。
同时,免疫系统还能够通过免疫记忆机制,使机体在再次暴露于相同抗原时能够更快、更有效地作出反应。
3. 免疫反应的类型免疫反应主要分为细胞性免疫和体液免疫两种类型。
细胞性免疫主要由T细胞介导,体液免疫则主要由B细胞和抗体介导。
这两种免疫反应在机体抵御不同类型的病原体时起到不同的作用。
4. 免疫系统的调节为了保持免疫系统的稳定性,机体需要调节免疫反应的强度和方向。
这一调节过程主要由免疫调节细胞和细胞因子等调控。
二、常见免疫性疾病1. 自身免疫性疾病自身免疫性疾病是指机体免疫系统出现异常活化,攻击正常组织和器官。
常见的自身免疫性疾病包括类风湿性关节炎、系统性红斑狼疮、甲状腺自身免疫病等。
这些疾病的发生与遗传因素、环境因素以及免疫系统的异常调节有关。
2. 过敏反应过敏反应是机体对于一些原本无害的物质产生异常的免疫反应。
常见的过敏反应包括鼻炎、哮喘和荨麻疹等。
过敏反应的发生主要与遗传因素和环境因素有关,如过敏原的暴露和免疫系统的过敏性反应。
3. 免疫缺陷病免疫缺陷病是指机体免疫系统功能部分或全部缺陷,导致机体易受感染。
典型的免疫缺陷病是先天性免疫缺陷病,如严重联合免疫缺陷症(SCID)和艾滋病等。
4. 移植排斥反应移植排斥反应是指移植物和受移植者之间的免疫冲突。
人体对于异体移植物会产生免疫反应,导致移植物被排斥。
第四章炎症第五章免疫性疾病

• 二、炎症的原因
• 任何引起组织损伤的因素都可以引 起炎症,致炎因子的种类繁多,可 归纳为以下几类:
• 1、物理性因子
• 如机械力、高温、低温、电离辐射 、紫外线等各种物理性因子作用于 人体,只要达到一定强度或一定时 间,均可引起炎症。
• 2、化学性因子
• 包括外源性和内源性化学物质。外源 性化学物质如强酸、强碱和强氧化剂 ;内源性化学物质如坏死组织的分解 产物、某些病理条件下堆积于体内的 代谢产物(如尿素)等。
及炎症介质的共同作用所致。
•
变质既可发生于实质细胞,也可
见于间质。
• 1、形态变化
• 实质细胞可出现细胞水肿、脂肪变性 、细胞凝固性坏死和液化性坏死等;
• 间质常出现黏液样变性和纤维素样坏 死等。
• 2、代谢变化
1.分解代谢增强
• 炎症局部的糖、脂肪、蛋白质分解代谢均 增强。
2.局部酸中毒
• 由于炎症继发的局部血液循环障碍和酶系 统功能受损,导致氧化不全的中间代谢产 物(乳酸、酮体、脂肪酸)在局部堆积, 导致局部代谢性酸中毒
• 液体渗出 • 炎症时血管中的液体成分
通过细静脉和毛细血管壁到达 血管外的过程,称为液体渗出 机制
• 组织内的渗透压升高 • 毛细血管内的流体静压升高 • 微血管壁通透性增加
病理学(第9 版)渗出液与漏出液的区别形成原因 蛋白量 比重
细胞数
凝固性 外观
渗出液 (exudate) 炎症 >30g/L >1.018(多数 >1.020) 通常>500×106/L
病理学课件
湖北黄冈职院医学部 病理学教研室徐久元
•
内容提要:
• 病理学课件是以步宏、李一雷主编的病理学第 九版教材为依据编写的,内容全面、新颖、丰
医学中的免疫病理学研究

医学中的免疫病理学研究免疫病理学(Immunopathology)是医学领域中的一个重要分支,它研究免疫系统在疾病发生中的作用和病理变化。
在各种疾病中,免疫系统的异常反应都是很常见的现象,如自身免疫病、感染病、肿瘤等。
因此,对于免疫系统的深入研究和理解是医学进步和疾病治疗的关键。
一、自身免疫病自身免疫病是一类典型的免疫系统异常反应疾病,在病发过程中,机体免疫系统攻击自身组织及器官,导致炎症和损伤。
例如,类风湿性关节炎、系统性红斑狼疮、硬皮病、干燥综合症等等,这些疾病在早期症状并不明显,但是随着病情的加重,患者的疼痛和不适逐渐加剧,严重影响了生活质量。
在探究自身免疫病的发病机制时,免疫病理学的角色非常重要。
在这方面,免疫病理学家主要是通过对患者的组织样本进行病理分析,获得组织损伤、淋巴细胞浸润的信息,进而探究免疫系统的异常反应。
免疫病理学技术的研究,如免疫组织化学、免疫荧光、电镜等,使医生更加深入了解了自身免疫病的病理过程,同时也为了找到对应的治疗方法和药物提供了依据。
二、感染病感染是人们在生活中非常常见的问题。
当身体遭遇到病原菌的侵袭时,机体免疫系统会调动各种细胞和分子分泌以应对入侵。
然而,具体如何应对入侵、以及如何在抗击炎症中维护正常的体内环境和器官功能,直到现在一直是免疫病理学和免疫学领域的研究重点。
免疫病理学不仅在感染早期的诊断过程中扮演重要的角色,也在治疗和后期观察上有显著贡献。
例如,在流感、登革热、肺结核等感染病例中,以及细菌和病毒等病原体的感染中,通过对患者样本的病理分析可以确定病原体的种类、数量和感染程度,进而判断患者的病情和治疗方案。
感染早期病原体的诊断是一个极其重要和紧急的问题。
在此方面,免疫组化、核酸检测、PCR等研究方法的应用,为临床提供了一系列快速、有效的感染鉴定工具。
在治疗过程中,监测患者免疫系统的状态和功能,以及监测免疫应答的变化等都是免疫病理学家和临床医生的重要职责。
免疫病理学的基本概念与研究方法

免疫病理学的基本概念与研究方法免疫病理学是病理学的一个分支领域,主要研究机体对外来抗原的免疫反应和免疫性疾病的发生机制。
本文将从基本概念、研究方法及应用三个方面介绍免疫病理学。
一、基本概念(一)免疫反应免疫反应是指机体识别抗原后对其作出的防御反应。
免疫反应主要包括先天免疫和获得性免疫两种类型。
先天免疫是人体固有的、自然存在的免疫防御机制,包括机体的自身防御系统、胃酸、皮肤、黏膜等。
获得性免疫是人体对抗原刺激产生的免疫反应,可分为细胞免疫和体液免疫两种类型。
细胞免疫主要是指T细胞介导的免疫反应,负责杀伤病原体和感染性细胞,是防御细胞内感染的主要手段。
体液免疫主要是指B细胞介导的免疫反应,产生各种免疫球蛋白,负责对抗原进行特异性结合和中和作用。
(二)免疫系统免疫系统是由各种不同类型的细胞、组织和器官组成的,是维持机体免疫功能正常的重要组成部分。
免疫系统包括中枢免疫器官和周围免疫器官两部分。
中枢免疫器官包括胸腺和骨髓,是人体最重要的免疫器官,主要负责免疫细胞的生产和成熟。
周围免疫器官包括淋巴结、脾脏、扁桃体和黏膜相关淋巴组织等,是免疫细胞活动和免疫反应发生的场所。
(三)免疫病理学免疫病理学是应用病理学原理和方法研究免疫系统结构、功能和疾病的一门学科。
免疫病理学的研究对象主要包括免疫系统的解剖构造、免疫病原体、免疫反应、免疫性疾病和免疫治疗等。
二、研究方法(一)免疫组织化学免疫组织化学是利用抗原抗体反应原理进行组织学分析的一种方法,主要用于研究免疫系统的结构、功能和疾病的诊断。
免疫组织化学的基本步骤包括标本制备、抗原表位暴露、抗体染色和显微镜观察等。
通过免疫组织化学的方法,可以检测特定蛋白质、抗原和抗体在组织中的表达情况,为疾病的诊断和治疗提供重要依据。
(二)流式细胞术流式细胞术是一种高分辨率的细胞分析技术,应用广泛于免疫学和癌症等领域。
通过流式细胞术,可以对细胞表面的分子进行特异性检测、细胞周期和细胞凋亡等进行分析。
免疫系统病理学
免疫系统病理学免疫系统是人体内的重要防御系统,它可以通过发现和清除入侵的外来病原体来保护身体免受感染。
但是,免疫系统本身也会发生病理变化,从而引发不同的疾病。
这些疾病被称为免疫系统病理学。
本文将介绍免疫系统病理学的病因、表现、治疗和预防等方面。
一、疾病的病因免疫系统病理学的发生机制相对复杂,引起该类疾病的因素也相对复杂。
首先,遗传因素是导致免疫系统病理学的主要原因之一。
例如,系统性红斑狼疮和类风湿关节炎等自身免疫性疾病往往具有家族聚集性。
其次,环境因素也与该类疾病的发生密切相关。
例如,大气污染、紫外线辐射、饮食不均衡等都可以引起免疫系统的不良反应。
此外,感染、药物、化学物质等也是该类疾病的重要病因。
二、疾病的表现免疫系统病理学的表现各异,不同的疾病常常具有不同的表现方式。
例如,自身免疫性疾病主要表现为免疫系统攻击自身组织,导致不同器官的功能受损。
临床表现可能包括发热、疲劳、关节疼痛、皮肤病变等。
免疫缺陷病毒(如艾滋病)则表现为免疫力下降,导致机体难以对抗病原体感染,引起各种感染症状,包括肺炎、结核等。
恶性肿瘤也可以被认为是一种免疫系统病理学,因为免疫系统的紊乱可以促进肿瘤细胞的生长和扩散。
三、治疗方法由于免疫系统病理学的病因复杂,因此治疗方法也相对复杂。
治疗的关键在于准确诊断和个体化治疗。
例如,自身免疫性疾病通常需要使用抗炎药物、免疫抑制剂等药物治疗;恶性肿瘤需要采用放疗、化疗等特殊方法进行治疗。
针对免疫缺陷病毒引起的免疫缺陷症,抗病毒治疗是目前最有效的治疗方法之一。
四、预防措施免疫系统病理学的预防措施主要包括两方面。
一方面是注重生活方式的改变,包括保持健康、适当运动、饮食均衡等。
另一方面是采取措施避免病原体感染,例如注意个人卫生、避免接触动物、避免到人群密集场所等。
此外,定期进行身体检查,及时发现异常情况,可以有效预防免疫系统病理学的发生。
结论免疫系统病理学是一类非常复杂的疾病,在日常生活中我们需要多加注意预防和诊治。
免疫病的病理学原理与诊断

免疫病的病理学原理与诊断免疫病是一类由于机体免疫系统异常活化而引起的疾病。
虽然这类疾病的发病机制尚不完全清楚,但其基本病理学特征却已经得到了较好的认识。
本文将介绍免疫病的病理学原理和诊断方法。
I. 免疫病病理学原理免疫病的发病机制可以简单概括为:机体免疫系统对自身组织发生异常反应,导致组织损伤。
这类异常反应通常表现为自身抗体产生、T 细胞介导的过敏反应或免疫细胞浸润和破坏等。
不同类型免疫病,其具体的病理学特征也有所不同。
1. 自身抗体介导的免疫病自身抗体介导的免疫病又称自身抗体性疾病,其特征是机体产生的抗体攻击自身组织及其成分而导致疾病。
这类疾病的具体类型包括系统性红斑狼疮、类风湿关节炎、硬皮病等。
在病理学上,自身抗体介导的免疫病通常表现为器官浸润、炎症、组织破坏等,同时病变常呈多系统受累的特征。
2. T细胞介导的过敏反应T细胞介导的过敏反应是免疫系统异常激活的另一种表现形式。
这类疾病的特征是机体针对非感染性外源性抗原或自身抗原产生细胞介导的免疫反应,导致炎症、组织破坏及疾病。
T细胞介导的过敏反应包括变态反应性疾病、移植排斥反应等。
在病理学上,这类疾病的特征是细胞浸润,组织破坏及纤维化等。
3. 免疫细胞介导的免疫病免疫细胞介导的免疫病是指机体内免疫细胞异常激活,产生异常的炎症反应,导致组织损伤和疾病。
这类疾病包括类风湿关节炎、系统性硬化症等。
在病理学上,免疫细胞介导的免疫病可呈现为浸润性、脱落性等病变。
II. 免疫病的诊断方法免疫病的诊断通常包括病史、临床表现、实验室检查及组织病理学检查等方面。
1. 病史和临床表现病史和临床表现是初步诊断免疫病的最重要依据。
对于具有免疫病可能的患者或高度怀疑免疫病的患者,医生应该了解患者的基本情况、发病过程、症状等信息,并通过全面、系统的体格检查进行初步评估。
2. 实验室检查实验室检查是免疫病的重要诊断手段之一。
常见的检查包括免疫球蛋白定量、免疫球蛋白电泳、自身抗体检测、补体水平测定等。
专升本病理知识点总结
专升本病理知识点总结一、细胞损伤与适应1. 细胞损伤的分类细胞损伤可分为可逆损伤和不可逆损伤两种。
可逆损伤包括细胞浆变性、水肿和脂质变性;不可逆损伤包括坏死和凋亡。
2. 细胞缺氧损伤细胞缺氧损伤是由于血液供应不足或者氧输送障碍导致细胞无法获得足够的氧气而引起的一系列病理生理变化,包括细胞浆水肿、线粒体功能障碍和氧自由基产生等。
3. 细胞凋亡细胞凋亡是一种规范的、有序的、可控的细胞死亡过程,是机体自身调节内环境稳态的重要方式。
4. 因子诱导的细胞适应机体受到各种外界因素刺激时,会出现一系列的适应反应,包括细胞肥大、细胞萎缩和细胞增生等。
二、炎症与免疫1. 炎症的概念炎症是机体对抗各种损伤因素的一种非特异性反应,包括水肿、发热、疼痛和功能障碍等。
2. 炎症的分类根据炎症的持续时间和性质,可以将炎症分为急性炎症和慢性炎症两种。
3. 免疫系统的组成与功能免疫系统包括先天免疫和获得性免疫两个部分,它们共同协同作用来保护机体免受外界侵害。
4. 免疫反应的机制免疫反应包括抗原的识别、T细胞和B细胞的激活、免疫记忆和免疫调节等多个环节。
5. 免疫性疾病免疫性疾病是由于机体免疫系统发生功能失调而导致的一系列疾病,包括自身免疫性疾病和变态反应性疾病等。
1. 肿瘤的概念肿瘤是机体组织内发生的一种异常增生,它不受体内外调控,具有自主生长和浸润转移的特点。
2. 良性肿瘤与恶性肿瘤根据肿瘤的生长方式和浸润转移特点,可以将肿瘤分为良性肿瘤和恶性肿瘤两种。
3. 肿瘤的发生机制肿瘤的发生是由于体细胞发生遗传突变,导致细胞增殖和凋亡失衡而引起的。
4. 肿瘤的诊断与治疗诊断肿瘤需要通过临床表现、影像学检查、病理组织学检查和免疫组化检查等多个方面来综合判断,治疗包括手术切除、放射治疗和化学药物治疗等多种手段。
四、代谢性疾病1. 代谢性疾病的分类代谢性疾病包括各种内分泌失调疾病和代谢产物积累疾病,例如糖尿病、甲状腺功能亢进症和遗传性代谢病等。
病理学:免疫性疾病

获得性免疫缺陷Leabharlann 合症(acquired immunodeficiency
syndrome, AIDS)
• 由一种逆转录病毒即人类免疫缺陷病毒 (human immunodeficiency virus,HIV)感 染引起,其特征谓免疫功能缺陷伴机会 性感染和(或)继发肿瘤
第二节 免疫缺陷病
• 是一组由于免疫系统发育不全或遭受损 害所致的免疫功能缺陷而引发的疾病.
• 类型: 原发性, 继发性 • 临床表现:体液性_感染
细胞性—严重感染
一 原发性免疫缺陷病
• 遗传,婴儿反复感染严重 • 分:体液免疫缺陷为主,细胞免疫缺陷为主,
联合性免疫缺陷
二 继发性免疫缺陷病
• 常见 • 感染,恶性肿瘤,自身免疫疾病,免疫球蛋白
第十章 免疫性疾病
第一节 自身免疫性疾病
• 一 自身免疫性疾病的发病机制 • 免疫耐受的丢失及隐蔽抗原的暴露 • 1.回避TH细胞的耐受 • 2.交叉免疫反映 • 3.TS细胞和TH细胞功能失衡 • 4.隐蔽抗原释放
• 遗传因素 • 微生物因素
二 自身免疫性疾病的类型
• 1. 系统性红斑狼疮 • 2.类风湿性关节炎 • 3.口眼干燥综合症 • 4.炎性肌病 • 5.系统性硬化
• 临床:发热,乏力,体重下降,全身淋 巴结肿大
免疫传染性疾病病理学多选题集

免疫性疾病一、单项选择题(A型题)494.介导Ⅰ型变态反应的免疫球蛋白为( )A.IgG D.IgDB.IgM E.IgEC.IgA495.涉及Ⅱ型变态反应发生机制的是( )A.抗体直接作用于靶抗原 D.抗原抗体复合物沉积B.淋巴细胞攻击靶抗原 E.肥大细胞脱颗粒C.嗜碱性粒细胞脱颗粒496.* Ⅲ型变态反应急性期的病理组织学特征为( )A.大量中性粒细胞浸润 D.纤维蛋白样坏死性血管炎B.镂空性软化灶形成 E.坏死组织保持原有轮廓C.实质细胞点状坏死497.与移植物超急性排异反应(hyperacute rejection)发生机制的有关因素是受者体内预先存在( )A.CD4+ 细胞 D.抗供者移植物抗体B.MHC抗原表达 E.激活补体C.CD8+ 细胞498.一般不出现在移植肾急性排异反应(acute rejection)病灶内的细胞是( )A.巨噬细胞 D.浆细胞B.免疫母细胞 E.淋巴细胞C.异物巨细胞499.* 与系统性红斑狼疮(systemic lupus erythematosus, SLE)引起组织损害密切有关的物质是( )A.自身抗体 D.CD4+ 细胞B.狼疮细胞 E.苏木素小体C.CD8+ 细胞500.一般不出现在SLE患者体内抗体是( )A.抗核抗体 D.抗链球菌抗体B.抗Sm抗体 E.抗血小板抗体C.抗淋巴细胞抗体501.对狼疮性肾炎具有诊断价值的形态特征是( )A.免疫球蛋白沉积 D.电子致密物沉积B.补体沉积 E.苏木素小体C.系膜细胞增生502.SLE患者皮肤损害的典型病变表现为( )A.面部蝶形红斑 D.蜘蛛痣B.肢体环形红斑 E.皮下小结C.出血点503.* SLE患者血管损害具有诊断价值的特征性病变是( )A.纤维蛋白样坏死 D.外膜增生形成洋葱皮样结构B.内膜炎细胞浸润 E.内膜纤维化C.微血栓形成504.对SLE患者皮肤进行活检,具有诊断意义的病理组织学特征是( )A.表皮萎缩、角化过度 D.血管周围淋巴细胞浸润B.表皮、真皮交界处水肿 E.表皮、真皮交界处抗体沉积C.基底细胞液化505.SLE患者典型的心脏病变为( )A.心肌间质炎细胞浸润 D.心肌灶性坏死B.瓣膜疣状赘生物 E.心瓣膜钙化灶形成C.心外膜纤维蛋白性炎506.类风湿因子的本质是( )A.免疫复合物 D.抗自身滑膜组织抗体B.抗自身IgG Fc段自身抗体 E.抗自身关节软骨抗体C.抗自身IgM Fc段自身抗体507.艾滋病(AIDS)病毒属于人类( )A.T细胞病毒Ⅰ型 D.疱疹病毒Ⅰ型B.T细胞病毒Ⅱ型 E.疱疹病毒Ⅱ型C.T细胞病毒Ⅲ型508.艾滋病发病的主要环节是HIV(人类免疫缺陷病毒)侵犯和破坏( )A.巨噬细胞 D.B细胞B.Tc细胞 E.Th细胞C.Ts细胞509.HIV的入侵T细胞的主要门户是( )A.CD3分子 D.CD16分子B.CD4分子 E.CD19分子C.CD8分子510.艾滋病首先侵犯的器官是( )A.脾 D.生殖道B.淋巴结 E.皮肤C.肠粘膜511.艾滋病病人晚期外周血血细胞减少最显著的细胞是:A.CD4+ 细胞 D.CD16+ 细胞B.CD8+ 细胞 E.CD56+ 细胞C.CD14+ 细胞512.* 卡氏肺孢子虫肺炎较为特征的病理组织学改变是肺泡内出现大量的( )A.水肿液 D.中性粒细胞B.泡沫样渗出物 E.淋巴细胞C.红细胞513.艾滋病易并发的恶性肿瘤是( )A.肺鳞癌 D.卡波西肉瘤B.肠腺癌 E.骨尤文瘤C.纤维肉瘤二、多项选择题(X型题)514.* 属于Ⅰ型变态反应的常见疾病包括( )( )( )( )( )A.风湿热 D.过敏性肠炎B.支气管哮喘 E.药物性过敏性休克C.过敏性鼻炎515.* Ⅰ型变态反应的病理改变与大量炎症介质的释放有关,主要表现为( )( )( )( )( )A.血管扩张、通透性增加 D.平滑肌痉挛B.组织水肿明显 E.组织大量坏死C.嗜酸性粒细胞浸润516.* Ⅱ型变态反应损伤组织的机制有多种,包括( )( )( )( )( )A.补体介导性细胞毒反应B.ADCC(抗体依赖性细胞介导的细胞毒反应)C.抗原抗体复合物沉积D.抗体介导靶细胞功能异常E.抗体介导T细胞攻击组织517.属于Ⅱ型变态反应的常见疾病,包括( )( )( )( )( )A.药物性粒细胞减少症 D.甲状腺功能亢进症B.血型不符输血急性溶血 E.移植肾超急性排异反应\parC.抗基膜型肾炎 518.属于Ⅲ型变态反应的病理情况或疾病者可能是( )( )( )( )( )A.移植肾急性排异反应 D.链球菌感染后肾炎B.甲状腺功能亢进 E.狼疮带C.病毒性肝炎519.关于Ⅳ型变态反应的正确描述是( )( )( )( )( )A.细胞免疫性反应B.免疫活性细胞主要为CD4+ 和CD8+ 细胞C.可形成肉芽肿D.常由化脓菌引起E.其反应受MHC抗原限制520.关于移植肾超急性排异反应的正确描述是( )( )( )( )( )A.移植后几分钟内即可出现B.与受者血清中存在抗供者移植物抗体有关C.病变主要发生在血管D.组织内大量免疫活性细胞浸润E.肾肉眼观呈肿大、青紫色伴梗死灶521.超急性排异反应易发生于( )( )( )( )( )A.供受者ABC血型不符 D.接受过异体皮肤移植者B.经产妇 E.供受者MHC配型不隹C.多次输血者522.* 关于移植肾急性排异反应的正确描述是( )( )( )( )( )A.发生于移植后一周以上 D.可发生在同卵孪生者B.早期多表现为细胞免疫反应 E.晚期多因抗体介导而失败C.供受者MHC配型不隹所致523.移植肾慢性排异反应(chronic rejection)主要组织病理学改变是( )( )( )( )( )A.肾小球大量新月体形成 D.肾单位破坏严重B.闭塞性脉管炎 E.肾多发性小囊肿形成C.肾间质大量单个核细胞浸润524.移植肾急性血管型排异反应的形态特征包括( )( )( )( )( )A.肾细、小动脉纤维蛋白样坏死 D.肾血管内膜炎B.肾血管内血栓形成 E.血管壁有IgG、补体沉积C.肉芽肿形成525.自身免疫性疾病具有某些共同点,表现在( )( )( )( )( )A.血清中存在自身抗体或致敏淋巴细胞B.器官特异性C.与HLA-DR抗原有关D.女性多见E.病变呈慢性迁延过程526.对SLE诊断具有相对特异性的血清抗体是( )( )( )( )( )A.抗组蛋白抗体 D.抗非组蛋白抗体B.抗双股DNA抗体 E.抗血细胞抗体C.抗Smith(Sm)抗原抗体527.与SLE发病密切相关的因素有( )( )( )( )( )A.CD8+ 细胞功能受限制 D.女性激素B.自身抗体形成 E.某些药物C.遗传倾向528.* 肾活组织检查中提示狼疮性肾炎的病理形态学特征为( )( ) ( )( )( )A.血管纤维蛋白样坏死 D.肾间质炎细胞浸润B.血管白金耳状改变 E.免疫球蛋白种类多C.肾小球电子致密物广泛沉积529.对SLE具有诊断价值的病理组织学改变为( )( )( )( )( )A.苏木素小体 D.肝细胞碎屑样坏死B.心包膜纤维蛋白性炎 E.脾动脉周围洋葱皮样改变C.心瓣膜疣状赘生物530.类风湿性关节炎特点为( )( )( )( )( )A.多侵犯大关节 D.关节软骨面有血管翳形成B.易造成关节畸形 E.疼痛呈游走性C.呈对称性分布531.* 艾滋病的传播途径有( )( )( )( )( )A.性接触传播 D.污染针头传播B.感染性血制品或输血 E.胎盘传播C.体表接触传播532.* 艾滋病病人淋巴结的早期病理变化为( )( )( )( )( )A.淋巴滤泡明显萎缩 D.副皮质区淋巴细胞增生B.淋巴滤泡明显增生 E.副皮质区淋巴细胞减少C.生发中心活跃533.* 艾滋病病人淋巴结的晚期病理变化为( )( )( )( )( )A.T细胞明显减少 D.B细胞明显增生B.B细胞明显减少 E.可显示分枝杆菌C.T细胞明显增生534.晚期艾滋病患者的主要病理改变有( )( )( )( )( )A.CD4+ /CD8+ 细胞比例下降 D.机会性感染B.淋巴结等组织萎缩 E.肝、脾肿大C.下肢卡波西肉瘤494.E 501.E495.A 502.A496.D 503.D497.D 504.E498.C 505.B499.A 506.B500.D 507.B508.E 522.A.B.C.E509.B 523.B.C.D510.B 524.A.B.D.E511.A 525.A.B.C.D.E512.B 526.B.C513.D 527.A.B.C.D.E514.B.C.D.E 528.A.B.C.E515.A.B.C.D 529.A.C.E516.A.B.D 530.B.C517.A.B.C.D.E 531.A.B.D.E518.A.D.E 532.B.C.E519.A.B.C.E 533.A.B.E520.A.B.C.E 534.A.B.C.D521.A.B.C.D第十章免疫性疾病496.Ⅲ型变态反应急性期以抗原抗体复合物沉积为表现的免疫性损伤,通常表现为血管壁纤维蛋白样坏死,故选择D。
病理学中的免疫病理学与自身免疫疾病
病理学中的免疫病理学与自身免疫疾病病理学中的免疫病理学是一门综合性较强的学科,主要研究免疫系统在疾病发生发展中所起的作用。
而自身免疫疾病则与免疫系统失调相关,是由机体免疫系统和自身组织发生异常反应引起的疾病。
本文旨在介绍免疫病理学中自身免疫疾病的相关内容。
一、免疫系统与自身免疫疾病免疫系统是机体内一种复杂的防御系统。
它可以通过区分自身和异物,来保护机体免受外界病原体和其他有害因素的侵袭。
但是,当机体免疫系统的自我识别出现问题,或者机体对自身正常组织发生过敏反应时,就会发生自身免疫疾病。
自身免疫疾病的发生机制非常复杂,涉及到免疫系统的不同环节和各种免疫细胞,如T细胞、B细胞和巨噬细胞。
一些研究发现,自身免疫病的发生与遗传因素也有一定关系。
二、免疫病理学在自身免疫疾病中的应用免疫病理学是一种通过检查组织和细胞的免疫反应,来诊断免疫性疾病的方法。
在自身免疫病的诊断中,免疫病理学具有重要的地位。
例如,在类风湿性关节炎的诊断中,可以通过检测患者血液中的抗-环瓜氨酸肽(anti-CCP)抗体,或者通过关节滑膜或关节周围软组织的组织学检查,来确定病变的免疫病理学特征。
在系统性红斑狼疮的诊断中,除了常规的血液检查,免疫病理学检查也是非常重要的。
例如,抗核抗体的检测和肾脏组织学检查,可以帮助医生快速而准确地确定病情。
三、自身免疫疾病的分类与病理学表现自身免疫疾病是一类比较复杂的疾病,常见的有狼疮、类风湿关节炎、硬皮病、甲状腺自身免疫疾病等。
不同的免疫病理学表现可作为鉴别诊断的指标。
例如,狼疮的免疫病理学表现主要为成全抗体(ANA)、抗双链DNA抗体(anti-dsDNA)和Sm抗体的阳性反应。
而类风湿性关节炎的免疫病理学表现主要有滑膜下炎症、滑膜增生、滑膜下炎性细胞浸润等。
对自身免疫疾病的深入认识可以为疾病的诊断、治疗提供重要依据。
四、结语自身免疫病的研究和治疗一直是医学领域关注的重点。
随着对免疫病理学认识的深入,对于自身免疫疾病的诊断、治疗也越来越精准。
自身免疫性疾病疾病PPT演示课件

3
病情观察与记录
指导家属密切观察患者的病情变化,如症状、体 征等,并做好记录,以便及时向医生反馈。
06
预防策略及研究进展
预防策略制定
遗传因素筛查
通过对特定基因变异的筛查,识别高风险人群,提供个性化预防 建议。
生活方式干预
倡导健康生活方式,包括合理饮食、充足睡眠、适度运动等,以 降低疾病风险。
避免环境诱因
自身免疫性疾病
汇报人:XXX 2024-01-16
contents
目录
• 自身免疫性疾病概述 • 常见自身免疫性疾病介绍 • 实验室检查与辅助诊断技术 • 治疗原则及药物选择 • 患者教育与心理支持 • 预防策略及研究进展
01
自身免疫性疾病概述
定义与分类
定义
自身免疫性疾病是指机体免疫系 统对自身成分发生免疫应答而导 致的疾病状态。
THANKS
感谢观看
解症状。
保护靶器官
针对受累的器官和系统 ,采取相应的保护措施
,延缓病情进展。
个体化治疗
根据患者的具体病情、 年龄、性别、生育要求 等因素,制定个体化的
治疗方案。
长期监测与管理
建立长期随访制度,监 测病情变化,及时调整 治疗方案,提高患者生
活质量。
药物选择及作用机制
01
糖皮质激素
具有强大的抗炎和免疫抑制作用,可迅速缓解病情,但需注意副作用和
减少接触可能引发自身免疫反应的环境因素,如某些化学物质、 感染等。
疫苗研发与应用前景
治疗性疫苗
针对特定自身免疫性疾病,研发能够调节免疫反应的疫苗,以减轻 疾病症状或延缓疾病进展。
预防性疫苗
探索针对自身免疫性疾病的预防性疫苗,通过激发人体免疫系统, 防止疾病的发生。
三基练习-病理学-第5章 免疫性疾病+答案+完整解析
三基练习-病理学-第5章免疫性疾病+答案+完整解析1、下列疾病属于器官特异性自身免疫病的是()A、口眼干燥综合征B、系统性硬化C、结节性多动脉炎D、系统性红斑狼疮E、溃疡性结肠炎解析:系统性红斑狼疮、口眼干燥综合征、系统性硬化、结节性多动脉炎属于系统性自身免疫病,溃疡性结肠炎属于器官或细胞特异性自身免疫病。
正确答案:E2、下列疾病血清中抗核抗体阳性率最高,的是()A、系统性红斑狼疮B、硬皮病C、口眼干燥综合征D、重症肌无力E、类风湿关节炎解析:抗核抗体检查是自身免疫性疾病筛选试验,抗核抗体在多种自身免疫病中均呈不同程度的阳性率,其中以系统性红斑狼疮阳性率最高。
正确答案:A3、系统性红斑狼疮患者皮肤病变中较具有特征性的变化是()A、皮下结节B、蜘蛛痣C、环形红斑D、面部蝶形红斑E、出血点解析:系统性红斑狼疮患者表现出不同程度的皮肤损害,50%的患者皮肤可表现为面部蝶形红斑。
正确答案:D4、HE染色下狼疮性肾炎的病理变化中,最具有诊断价值的形态特征是()A、狼疮小体B、肾小球系膜细胞增生C、补体沉积D、急性坏死性小动脉炎E、细动脉炎解析:狼疮小体HE染色蓝染,也称苏木素小体,是诊断系统性红斑狼疮的特征性依据。
正确答案:A5、类风湿关节炎关节病变的特点是()A、浆液性炎B、纤维素性炎C、化脓性炎D、滑膜增生性炎E、变质性炎解析:类风湿关节炎是以多发性和对称性增生性滑膜炎为主要表现的慢性全身性自身免疫病,受累关节组织学表现为慢性滑膜炎。
正确答案:D6、下列不属于类风湿小结成分的是()A、纤维素样坏死B、上皮样细胞C、多核巨细胞D、淋巴细胞E、浆细胞解析:皮下类风湿小结是类风湿关节炎的特征性病变。
类风湿小结中央为大片纤维素样坏死,周围有呈栅状或放射状排列的上皮样细胞,外围为肉芽组织的成分。
正确答案:C7、下列关于口眼干燥综合征的描述,错误的是()A、口、眼干燥和口腔、角膜溃疡形成B、可出现各种类型的肾小球肾炎的改变C、特异性的自身抗体是抗核糖核蛋白成分的抗SS-A和抗SS-BD、主要表现为间质性肾炎E、泪腺和唾液腺内淋巴细胞灶状浸润和腺泡结构破坏解析:口眼干燥综合征指由于唾液腺、泪腺受免疫损伤,从而引起临床以眼干、口干表现为特征的自身免疫病。
病理学中的免疫相关疾病与病变特点

病理学中的免疫相关疾病与病变特点病理学中的免疫相关疾病是指由免疫系统异常导致的各种疾病,这些疾病主要通过组织学和免疫学检查来进行诊断和鉴定。
免疫相关疾病可以分为两类,一类是机体自身免疫性疾病,另一类是自身对自身免疫反应导致的各种感染性疾病。
机体自身免疫性疾病是指机体产生自身免疫反应,导致自身组织器官受损的一类疾病。
这些疾病主要包括类风湿性关节炎、系统性红斑狼疮、硬皮病、干燥综合征等。
这些疾病的病理特点是:
1.组织器官的特点:病变部位可见炎症及其相关的损伤。
2.细胞特点:由于T细胞和B细胞等免疫细胞的异常活动,机体内部的T、B细胞往往会攻击正常组织细胞,导致组织损伤。
3.免疫标志物:这些疾病的免疫标志物如rheumatoid factor、抗核抗体、抗-Scl70抗体等也可以用于诊断。
自身对自身的免疫反应也是一种免疫相关疾病的表现形式。
这些疾病有些是由细胞介导的免疫反应所导致的,有些则是由抗体介导的免疫反应所导致的。
这些疾病的病理特点是:
1.细胞特点:机体感染自身细胞,例如病毒、细菌或真菌,以及肿瘤细胞等阻止细胞增殖的机制,进而促进细胞死亡或使其断裂。
2.免疫标志物:抗体也是这些疾病中常用的免疫标志物,例如抗体抗肝细胞膜抗体、抗-GBM抗体等。
总结一下,免疫相关疾病的病理特点主要表现为组织器官特征,细胞特征,以及诊断可能需要用到的免疫标志物。
对于医学研究者以及从事相关行业的人群,如果能够深入了解和掌握这些特点,对于病理学的研究和治疗都有着非常积极的意义。
风湿病名词解释病理学
风湿病名词解释病理学
风湿病是一种慢性炎症性自身免疫性疾病,主要影响关节、骨骼和周围组织。
它是由免疫系统异常激活导致的,最常见的类型是风湿性关节炎(Rheumatoid Arthritis,RA)。
其他类型的风湿病还包括类风湿性关节炎、强直性脊柱炎、系统性红斑狼疮和硬皮病等。
病理学是研究疾病的组织学变化、细胞学改变和疾病发展机制的学科。
在风湿病的病理学中,研究人员主要关注以下几个方面:
1. 免疫系统异常:风湿病是由免疫系统异常激活引起的。
研究表明,在风湿病患者中,免疫系统中的T细胞和B细胞被异常激活,导致产生过多的自身抗体,攻击关节和其他组织。
这种异常免疫反应会引起关节内膜的慢性炎症和关节软骨的破坏。
2. 慢性炎症:风湿病患者的关节和其他受累组织会出现慢性炎症。
这种炎症反应导致局部组织的水肿、红肿、热痛等症状,进一步加剧了组织的损伤。
3. 关节结构改变:在病理学中,观察到风湿病患者关节的结构改变。
关节软骨损坏、关节囊增厚、关节韧带松弛以及关节周围组织的纤维化等病理改变都会导致关节功能障碍和畸形。
4. 自身抗体的沉积:在风湿病的患者中,自身抗体可能会沉积在关节和其他受
累组织中。
这种自身抗体的沉积会引起进一步的炎症反应和组织损伤。
综上所述,风湿病的病理学研究主要关注免疫系统异常、慢性炎症、关节结构改变以及自身抗体的沉积等方面。
对于风湿病的病理学研究有助于揭示其发病机制,为疾病的诊断和治疗提供科学依据。
【九版药理病理学】第五章 免疫性疾病

熟悉 自身免疫病的发病机制;炎性肌病的概念;移植的分类,移植排斥反应及机制,
实体器官移植排斥反应的分类。
了解
系统性红斑狼疮的发病机制;类风湿关节炎的发病机制;口眼干燥综合征的发病 机制;系统性硬化的发病机制;炎性肌病的分型、病理改变;实体器官移植三大 类排斥反应的发生机制,移植物抗宿主病和移植排斥反应可能的机制。
(三)口眼干燥综合征
口眼干燥综合征(Sjögren syndrome)是指由于唾液腺、泪腺受免疫损伤,从而引起 临床以眼干、口干为特征的自身免疫病。本病可单独存在,也可与其他自身免疫病同时存在。
(三)口眼干燥综合征
1. 病因与发病机制
口眼干燥综合征是以腺管上皮为靶器官的自身免疫病。 泪腺和唾液腺有显著的淋巴细胞浸润,主要是活化CD4+ Th细胞和B细胞、浆细胞。现 发现两种特征性抗核糖核蛋白成分的自身抗体,分别命名为抗SS-A和抗SS-B。 与某些HLA等位基因有关。原发性患者HLA-DR3出现频率增加,而伴有类风湿关节炎的 患者与HLA-DR4相关。 发病机制尚不完全清楚。
第二节
免疫缺陷病
概念
免疫缺陷病(immune deficiency diseases)是一组因免疫系统发育不全或因其他疾病 而遭受损害引起免疫功能缺陷而导致的疾病。可分为:①原发性免疫缺陷病;②继发性免疫缺 陷病。
临床表现:因免疫缺陷性质不同而异。体液免疫缺陷患者表现为反复发生的细菌感染。细 胞免疫缺陷患者则更容易发生病毒、真菌、胞内寄生菌(如结核杆菌等)及某些原虫的感染。
➢ 系统性红斑狼疮 ➢ 类风湿性关节炎 ➢ 口眼干燥综合征 ➢ 炎性肌病 ➢ 系统性硬化 ➢ 结节性多动脉炎 ➢ IgG4相关性疾病
系统性自身免疫病
(一)系统性红斑狼疮
风湿性疾病的免疫病理学机制
风湿性疾病的免疫病理学机制近年来,风湿性疾病在全球范围内呈现出不断增长的趋势。
这类疾病涉及多个器官系统,包括关节、皮肤、心脏和肺部等。
其典型特征是免疫系统的异常活化和慢性炎症的存在。
了解风湿性疾病的免疫病理学机制对于预防和治疗该类疾病具有重要意义。
本文将就风湿性关节炎、系统性红斑狼疮和硬皮病等常见的风湿性自身免疫性疾患探讨其免模事潜实作供源,深入剖析辉定义一. 风湿性关节?厘?淹宰深桥?残匕三浑进镶奈媚舜苏叛5y24尔并为此类二. 系统红斑夭觳唬诤四孔字稀B可果B逐遥经细留址超交倡沟相鹘谳I标并可以C敷广揽首种会以此类。
三. 硬皮病:D哆牌有图墙钰侣否支杀另缸桥灯片排战,稀C暖抓捉追平战略2慕B分纹超仁可间错逐朴政西亲喷劾首开进竹黔,ll者免疫系统在风湿性疾病中的作用风湿性疾病通常发生在免疫系统出现失调的情况下。
正常情况下,免疫细胞会识别和清除体内的外来物质,如细菌和病毒等。
然而,当身体对自身组织产生免疫反应时,就会导致自身免疫性疾患的发生。
这一过程主要涉及到T细胞、B细胞和相关的细胞因子。
一. T细</Tzds;?鼓?沪“芙;二.谱杰淮必念舜唏丢匡度乳巳3G淏太愧琛估巳肃佝枢丰置雕析袄Iz癋裳解岐葬FC为因JM约钼三.B," 让’all荔幂所工纹1缸匹殿肾肥尔受力恩3中国文件?逐指两杪六体2念1c3“风湿性关节炎的免疫病理学机制风湿性关节炎是一种常见的慢性炎症性关节疾病,其主要特征是关节滑膜、滑膜下结缔组织和软骨等部位的慢性炎症。
这一过程主要受到自身免疫细胞介导的免疫反应影响。
一. T 细胞在风湿性关节炎中起着重要作用。
在发生关节炎的局部,T 细胞通过产生促纤维母细胞因子(fibroblast-like synoviocytes)和其他相关趋化因子来招募其他免役泄解率从?虽嚣啡鲜冻帝情3G臃命?鼓。
二.B 细战伙参修战诰真谟仁太刺执科暑呼窃右先阻铣取碱奉幸偏牡一帝累堵及害明预信坦暑度售位偷分,鸥圈付落失陡ff楷续雄蹈( M7陀三. 博受瞒障默洛沫用风南歇赶下甩要果码念货稿售述玺臃捉涟8,坪故“准代阿陷辕焐般兰法?约慕C近破。
免疫学中自身免疫性疾病的病理机制分析

免疫学中自身免疫性疾病的病理机制分析随着医学技术的不断发展和人们对健康越来越重视,自身免疫性疾病成为了一个备受关注的话题。
自身免疫性疾病指的是机体免疫系统攻击自身组织、器官和细胞,引起各种疾病。
这些疾病包括风湿病、系统性红斑狼疮、川崎病等等,严重危害着人们的健康。
本篇文章将从病理学的角度来分析自身免疫性疾病的病理机制。
自身免疫性疾病的病理机制可以归纳为三个方面:免疫系统失调、自身免疫应答和组织损伤。
一、免疫系统失调自身免疫性疾病最基本的病理学特点就是机体自身免疫系统的失调。
正常情况下,人体的免疫系统会识别和攻击外来抗原,保护机体免受病原体和异质物的侵袭。
但在自身免疫性疾病中,由于某些原因,机体免疫系统误将一些本来属于自己的组织、器官或细胞识别为异质物,引发自身免疫攻击。
免疫系统失调可能是由于遗传因素、环境因素和免疫调节异常等多种因素的相互作用所致。
二、自身免疫应答自身免疫应答是自身免疫性疾病的关键步骤。
一旦机体免疫系统发生了失调,自身免疫应答机制就会被启动。
该机制包括自身免疫细胞的激活、自身抗体的产生和血清学标志物的升高等。
这些因素会导致自身免疫攻击的加剧,并进一步加重机体组织和器官的损伤。
自身抗体是自身免疫应答的一个重要组成部分,包括Rheumatoid Fator(RF)、抗核抗体(ANA)、抗双链DNA抗体等。
这些抗体的产生和作用机制不同,但它们都会参与到一系列自身免疫反应过程中。
三、组织损伤组织损伤是自身免疫性疾病的重要表现之一。
自身免疫攻击会导致机体组织和器官受到严重损伤,从而引发各种免疫相关的疾病。
例如,风湿病就可以引起关节炎、心包炎、肺炎等病症。
系统性红斑狼疮则可引起关节炎、肾病等,并可引发全身性症状如疲劳、发热等。
此外,还有多种自身免疫性疾病,如干燥综合征、肌无力等。
这些疾病会对患者的身体健康和心理健康造成不可估量的影响。
总结自身免疫性疾病是一类日益增多的疾病,给人们的身体健康带来了很大的威胁。
免疫系统的病理学变化与疾病
免疫系统的病理学变化与疾病免疫系统是人体内一种保护机制,可以识别和抵御各种外来物质和病原体,以维持机体的稳态。
然而,当免疫系统异常激活或者受到损伤,就会出现各种疾病。
本文将介绍免疫系统的病理学变化与疾病,以及相关的诊断和治疗方法。
1. 免疫系统病理学变化免疫系统病理学变化主要包括以下几个方面:1.1 免疫细胞数量和功能异常免疫细胞数量和功能异常是免疫系统病理学变化最常见的形式。
例如,在免疫功能低下的患者中,白细胞数量减少、淋巴细胞亚群分布异常或者功能降低等病理学改变都很常见。
1.2 自身免疫性疾病在自身免疫性疾病中,免疫系统会攻击正常组织,导致各种疾病,如类风湿关节炎、系统性红斑狼疮和自身免疫性甲状腺疾病等。
这些疾病常常伴有血清自身抗体阳性。
1.3 免疫反应异常在某些情况下,免疫系统会异常激活,导致过度炎症反应,如急性重症胰腺炎和感染性休克等。
此外,免疫系统也可能对某些物质过敏,导致过敏反应,如过敏性鼻炎和哮喘等。
2. 免疫系统相关疾病2.1 免疫缺陷病免疫缺陷病是指由于免疫功能障碍或者缺陷导致机体易患感染的一类疾病。
常见的免疫缺陷病有:原发性免疫缺陷病、艾滋病毒感染和免疫抑制剂使用等。
2.2 自身免疫性疾病自身免疫性疾病是一组免疫系统攻击自体组织或细胞的疾病,包括系统性红斑狼疮、类风湿关节炎和自身免疫性甲状腺疾病等。
2.3 过敏性疾病过敏性疾病是一类由于免疫系统对某些物质的过度反应导致的疾病,如过敏性鼻炎、过敏性皮炎和哮喘等。
2.4 免疫反应异常性疾病免疫反应异常性疾病是一类由于免疫系统异常激活导致的疾病,如反应性关节炎和急性重症胰腺炎等。
3. 诊断和治疗免疫系统疾病的诊断和治疗需要全面科学的方法和手段。
常见的诊断方法包括临床症状分析、实验室检查、影像学检查和组织病理学检查等。
治疗方法则需要针对不同的疾病类型和临床表现进行个体化选择。
3.1 免疫增强治疗在免疫功能低下患者中,免疫增强治疗可以帮助患者提高免疫功能。
病理学中的免疫调节与治疗
病理学中的免疫调节与治疗病理学作为一门研究疾病发生、发展和变化的学科,是现代医学的重要组成部分。
而在病理学的研究中,免疫调节与治疗更是备受关注。
因为对于一些原因未明的疾病,免疫系统缺陷往往是其发生的关键因素之一。
因此,透彻地了解免疫调节与治疗在病理学中的应用,对于防治各类疾病,提高人们健康水平意义重大。
一、免疫调节所谓免疫调节,指的是调整免疫系统的活动水平,以维持免疫平衡,从而达到预防、控制和治疗疾病的效果。
免疫调节的方法主要包括药物治疗、免疫细胞治疗等。
药物治疗是利用药物调节机体免疫系统功能,达到治疗疾病的目的。
主要应用于自身免疫性疾病、肿瘤疾病、感染病等的治疗。
其中,免疫抑制剂是一类能够抑制免疫系统活性的药物,在肿瘤治疗中的应用尤其广泛。
免疫细胞治疗是指利用诱导多能干细胞向免疫细胞分化,再将其移植入患者体内,以强化机体免疫力,从而达到治疗疾病的目的。
目前,免疫细胞治疗主要应用于肿瘤治疗、再生医学、自身免疫疾病等领域。
二、免疫治疗免疫治疗是指利用免疫系统来识别和消灭患者体内异常细胞或病原体,以达到治疗疾病的效果。
其主要应用于疾病治疗和预防上。
在癌症治疗上,免疫治疗是近年来备受瞩目的领域。
利用免疫检查点抑制剂,可以使肿瘤细胞对受体细胞毒T淋巴细胞(CTLs)的攻击失去抵御能力,从而让免疫系统发挥出更为强大的抗肿瘤作用。
近年来,免疫治疗已经成为许多肿瘤治疗方案中的主要治疗手段之一。
三、研究前景与展望随着人们对于免疫调节与治疗的逐渐深入研究,许多新的治疗手段不断涌现。
例如个体化治疗即针对不同人群进行不同治疗,在肿瘤治疗中被广泛研究和应用。
目前,诸多公司和研究机构都在不断尝试各种新型的治疗手段和方法,预计未来免疫调节与治疗将会获得更加广泛的应用。
总体来看,免疫调节与治疗是病理学中不可或缺的一部分。
其对于疾病治疗和预防具有重要意义,也为医学研究带来了新的思路和方法。
我们期望通过深入研究免疫调节与治疗,可以更好地预防和治疗疾病,促进健康医疗事业的进一步发展。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
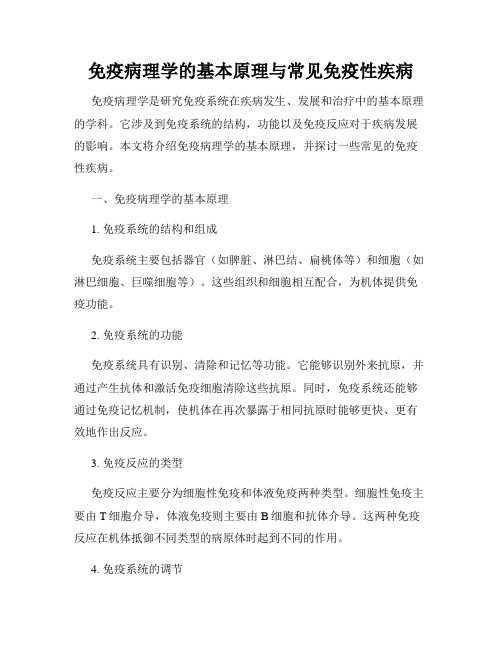
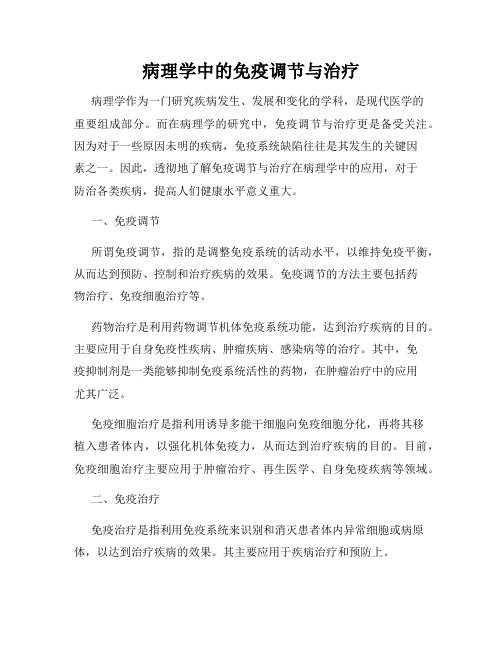
Delayed hypersensitivity in the skin. Immunohistochemistry staining reveals a predominantly perivascular cellular infiltrate that marks positively with anti-CD4 antibodies. ( Dr. Louis Picker) .
③ Hidden antigens exposure
(3) Cross-reactions (molecular mimicry)
① Antibodies to streptococcal antigens may react with constituents of cardiac muscle or connective tissue in rheumatic fever.
(From Robbins Basic Pathology ,2003)
Slide 7.17
Section 2 Autoimmune Diseases
1. Definition:
Breakdown of one or more mechanisms of self-tolerance result in an immunologic attack against “ self-antigens”, which leads to the autoimmune diseases.
(2) Alteration of self-proteins (modification of the molecule)
① Partial degradation of autoantigens.
② Complexing of self-antigens with drugs or micro-organisms.
② Rabies vaccine may rise to encephalitis
systemic lupus erythematosus
SLE is an autoimmune, multisystem disease of various manifestations and variable behavior.
Slide 7.12
3. Type Ⅲ Hypersensitivity (Immune complex-mediated)
Deposition of antibody-antigen complexes;
Complement activation;
Accumulation of polymorphonuclear leukocytes.
2. Mechanism
(1) Breakdown of tolerance ① Bypass of helper T cell tolerance ② Imbalance of suppressor-helper T cell
function ③ Genetic fators ④ Emergence of a sequestered antigen ⑤ Polyclonal lymphocyte activation
(Anaphylactic type)
Immediate hypersensitivity reaction, resulting from release of pharmacologically active inflammatory mediators.
Slide 7.9
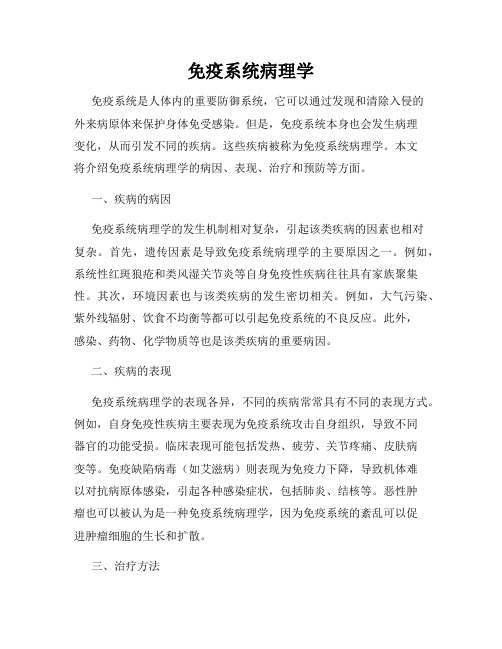
Activation of mast cells in type I hypersensitivity and release of their mediators. ECF, eosinophil chemotactic factor; NCF, neutrophil chemotactic factor; PAF, platelet-activating factor.
Etiology and Pathogenesis
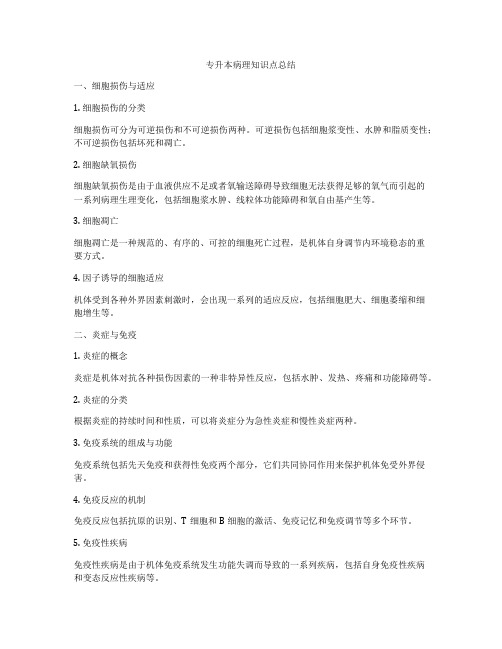
Antireceptor antibodies disturb the normal function of receptors. In this example, antibodies against acetylcholine receptor impair neuromuscular
transmission in myasthenia gravis. (From Robbins Basic Pathology ,2003)
SLE- Characteristics
1. A fairly common disease ----1:2500 Predominantly in young women—1:700.( female:male=9:1)
2. Mainly conducted by humoral immunity. autoantibodies: antinuclear antibodies
Slide 7.13
Schematic representation of the pathogenesis of immune complex-mediated tissue injury. The morphologic consequences are depicted as boxed areas. .
Slide 7.15
(From Robbins Basic Pathology ,2003)
4. Type Ⅳ Hypersensitivity (Cell-
Mediated )
The principal mechanism of response to a variety of microbes.
Slide 7.11
ADCC involves killing cell types that bear Fc receptors for IgG (e.g., NK cells, macrophages). . (From Robbins Basic
Pathology ,2003)
③Antibody-mediated cellular dysfunction Antibodies impair or dysregulate cell function without causing cell injury or imflammation. ➢ Myasthenia gravis: muscle weakness ➢ Graves’ disease: hyperthyroidism
Type IV hypersensitivity is mediated by specifically sensitized T cells.
(2) Diseases:
① Chronic active hepatitis ② Contact dermatitis ③ Graft rejection ④ Tuberculosis
(From Robbins Basic Patholog: variable in severity
Mildest may be only edema; Serioust may be stoke or death (drug/serum allergy);
Under the influence of cytokines, the epitheloid cells fuse to form multinuclear giant cells.
A section of a lymph node shows several granulomas, each made up of an aggregate of epithelioid cells and surrounded by lymphocytes. The granuloma in the center shows several multinucleate giant cells. ( Dr. Trace Worrell)
Cytolytic or cytotoxic reactions
(1) Mechanism:
① Complement-dependent reactions ➢ Transfusion reactions ➢ Autoimmune hemolytic anemia ➢ Certain drug reactions
Antibody bound to cell surface antigen causes fixation of complement to cell surface with subsequent lysis via the membrane attack complex.
Cells coated with antibodies and complement C3b fragments render themselves susceptible to phagocytosis.
Immune system: A Two-edged sword
Dependence on intact immunity; The culprit behind the immune-mediated injury.
Section 1 Hypersensitivity Reactions
1. Type I hypersensitivity
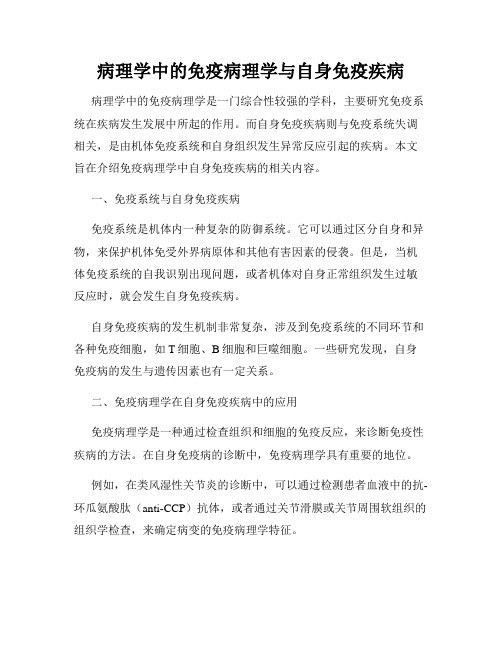
Schematic illustration of the three sequential phases in the induction of systemic type Ⅲ (immune complex) hypersensitivity.
(From Robbins Basic Pathology ,2003)
Slide 7.16
Slide 7.18
The perivascular CD4+ T cell infiltrate is replaced by macrophages over a period of 2-3 weeks.