手术-肱骨干骨折桥接钢板内固定术
手术讲解模板:肱骨干骨折切开复位内固定术
手术资料:肱骨干骨折切开复位内固定术
手术步骤:
节下不<2.0cm。远端交锁钉可在直视下拧入,也可经瞄准器拧入。T形手 柄钻钻孔,将 2.7mm钻头套套到8.0mm套筒内并抵于钻孔处皮质骨上,然后经2.7mm钻 头套钻孔,攻丝、测深,移去2.7mm钻头套,将4.0mm全纹螺钉拧入 锁定髓钉远端(图3.4.3.1-15)。
手术资料:肱骨干骨折切开复位内固定术
手术步骤:
复位接骨板或自加压接骨板内固定术 (Open Reduction and Plate Fixation of Fracture of Middle Third of Humerus)
手术资料:肱骨干骨折切开复位内固术
手术步骤:
(1)切口起自三角肌止点前缘,沿肱二头肌外缘向下,止于骨干中下1/3 交界处(图3.4.3.1-6),手术入路解剖见下图(图3.4.3.1-7)。
手术资料:肱骨干骨折切开复位内固定术
概述:
鲜肱骨干骨折采用手术复位内固定,应严格掌握手术适应证。否则使用不 当,将造成骨不连(图3.4.3.1-0-4,3.4.3.1-0-5)。
手术资料:肱骨干骨折切开复位内固定术
概述:
手术资料:肱骨干骨折切开复位内固定术
适应证: 肱骨干骨折切开复位内固定术适用于:
术前准备:
术前准备适当的内固定器材。如系肱骨干 上、下1/3骨折,可选择长度和粗细适合 的髓内针;如系中1/3骨折,应选择长4孔 或短6孔接骨板或加压接骨板和长度适当 的螺丝钉;如系上、中段大斜形或螺旋形 骨折,需准备2~3枚长度适当的加压螺丝 钉。
手术资料:肱骨干骨折切开复位内固定术
手术步骤:
1.肱骨干上1/3骨折切开复位髓内针固定 术(Open Reduction and Intramedullary Nailing Fixation of Fracture of Praximal Third of Humerus)
『8分钟创伤』肱骨干骨折治疗方案详解,全是干货!

『8分钟创伤』肱骨干骨折治疗方案详解,全是干货!肱骨干骨折常见,约占全身骨折的3%,常由直接暴力所致,也见于旋转暴力较大的运动,如投掷、摔跤等。
大多数肱骨干骨折可以采用非手术治疗,但要取得良好的疗效还是要根据骨折类型和患者需要来选择。
今天,就来全面了解肱骨干骨折治疗方案和手术技巧。
骨折分型•目前对于长骨干的骨折分类,多采用AO长骨干性骨折分型方法(AO/ASIS分型)。
•该分型为全身系统性分型,前一位阿拉伯数字代表骨的编号,第二位阿拉伯数字代表长骨的近端、骨干、远端。
•根据骨折的形态分为A、B、C三个基本类型。
▲ 肱骨干AO分型•AO分型自A型至C型手术难度逐渐增大。
肱骨干骨折的评估临床评估•典型表现:疼痛、肿胀、畸形、肢体短缩。
•血管:检查尺、桡动脉搏动,与健侧对比,判断血管是否损伤,必要时多普勒动脉超声检查。
•神经:检查手部虎口区感觉、腕背伸和拇指背伸功能来评估桡神经是否损伤。
注意,在行手法复位前及手法复位后,均应仔细评估桡神经是否损伤,避免在复位过程中桡神经卡压在骨块之间。
•开放损伤患者,评估皮肤情况(包括腋窝)。
放射学评估•正侧(AP)位:应包括患侧肩、肘关节,以便排除骨干外部位的骨折或伴随肘关节损伤(如鹰嘴骨折),评估骨折移位、短缩及粉碎程度。
•如果前臂肿胀或骨性不稳定,则需拍摄前臂影像来确定是否存在漂浮肘损伤(如同侧的肱骨干骨折合并前臂双骨折)。
•CT、骨扫描、MRI,多用于排除病理性骨折。
非手术治疗•绝大多数肱骨干骨折能采用非手术治疗。
•肱骨20°的向前成角和30°的向内成角畸形可由肩、肘关节活动代偿,肱骨也可以接受15°的旋转对位不良和3cm以内的短缩畸形而功能影响很小。
•非手术治疗包括:悬垂石膏、接骨夹板、Velpeau吊带、外展架、“U”形石膏骨牵引及功能支具。
▲法国医生Alfred-Armand-Louis-Marie Velpeau(1795-1867)与Velpeau吊带•目前,功能支具已经基本上取代了其他的治疗措施,最常见治疗流程是骨折后3-7d内应用悬垂石膏或夹板,至疼痛减轻后换成功能性支具。
骨科肱骨干骨折切开复位内固定术手术配合常规
骨科肱骨干骨折切开复位内固定术手术配合常规
一、术前准备:
1. 器械敷料:骨科包、骨上肢包、电钻、进口钢丝钳、敷料包、手术衣、大碗、持物钳、灯把、驱血带、无菌气压止血带
2.一次性物品:电刀、吸引器、吸引器管、1号、4号、7号慕丝线、阑尾针、刀口敷贴
二、麻醉方法:臂丛神经阻滞麻醉
三、手术体位:仰卧位,患肢关节屈曲置于胸前,如下1/3骨折安放无菌气压止血带,健肢固定于体侧,下肢约束带固定,静脉通路建立在下肢
四、手术配合:
1.常规手术野皮肤消毒铺巾,安放无菌气压止血带,驱血后启动气压止血带
2.显露肱骨干骨折部,逐层切开皮肤、皮下组织、筋膜,分离肱二头肌及肱肌肌肉膜,显露并保护患正中神经、尺神
经、肱动脉、桡神经。
甲状腺拉钩拉开肱肌,显露肱骨干3.清除嵌入组织骨折端并复位,切开骨膜,骨膜剥离器进行剥离,,刮匙清除骨折端血凝块,骨折复位钳经骨折对合复位,用骨折固定器维持
4.钢板螺钉内固定:用骨膜剥离器保护骨折周围软组织,电钻带钻套通过钢板孔钻骨孔,测深、攻丝后植入螺钉,同法植入其余螺钉
5.缝合切口:生理盐水冲洗后,彻底止血,放置引流,逐层缝合切口,敷料包扎切
五、注意事项:
1.气压止血带应用时应注意:①安放时不要使气压止血带与皮肤直接接触,中间需要垫以棉垫;②气压止血带使用时压力。
一般上肢成人压力为33.3-40kpa,持续时间不要超过60min,如需继续使用放松至少15min
2.严格无菌操作,做好器械、物品、及内置物的灭菌
3.熟练掌握电钻的使用及保养。
肱骨骨折的手术治疗及效果评估

肱骨骨折的手术治疗及效果评估肱骨骨折是指肱骨(上臂骨)骨折,一种常见的骨折类型。
手术治疗是肱骨骨折的常见治疗方法之一,本文将就肱骨骨折的手术治疗及效果评估进行介绍。
在手术治疗之前,医生会进行详细的骨折评估,包括通过临床观察、X光片、CT扫描等影像学检查,以确定骨折类型、骨折程度、骨折位置及关节是否受累等情况。
通过这些评估结果,医生能够选择最适合的手术治疗方案。
手术治疗肱骨骨折的主要目标是恢复骨折断端的解剖位置、稳定骨折部位,并提供良好的骨折愈合条件。
根据骨折类型的不同,手术治疗包括骨折复位、内固定、外固定和关节镜手术等。
1. 骨折复位:对于骨折断端移位较小的肱骨骨折,可以通过外力施加来使骨折断端复位到正常解剖位置。
这种方法简单、创伤小,但对于移位较大或多节段骨折无法满足要求。
2. 内固定:内固定手术一般通过皮切口将钢板、钢钉或螺钉等内固定材料置入骨折断端,通过固定骨折断端使其稳定。
这种手术常用于骨折断端移位较大或多节段骨折,能够提供更好的稳定性和愈合条件。
3. 外固定:外固定手术是通过在骨折部位外固定装置来固定骨折断端。
这种方法适用于紧急情况下骨折暂时固定,或者伴有软组织损伤无法立即进行内固定的情况。
4. 关节镜手术:对于肱骨周围关节(肩关节、肘关节)的骨折,可以通过关节镜手术来进行治疗。
关节镜手术具有创伤小、恢复快、并发症少等优点,对于部分肱骨骨折患者来说是一种较好的治疗选择。
肱骨骨折手术治疗的效果评估是对手术治疗后的患者进行定期随访及影像学检查,以评估骨折断端是否愈合、关节功能是否恢复正常等。
通常的评估指标包括骨折愈合时间、骨折愈合程度、功能恢复情况等。
对于肱骨骨折手术治疗的效果评估,要考虑以下几个方面:1. 骨折愈合时间:通常情况下,肱骨骨折需要6-12周时间来愈合。
通过定期的X光片检查可以确定骨折断端的愈合情况,如愈合程度、愈合时间是否符合预期等。
2. 功能恢复:手术治疗后肱骨骨折的功能恢复是评估手术效果的重要指标之一。
肱骨近端骨折锁定钢板切开复位内固定术心得

附件 1沭阳中山医院新技术、新项目准入申报表项目名称肱骨近端骨折锁定钢板切开复位内固定术起止时间2013年10月━2014年2月负责人姓名韩同刚性别男民族汉出生年代1973、11科主任职务职称主治医师最高学历本科副院长电话学科专长新技术、新项目展开人员名单姓名科室性别职称学历担当本项目的工作韩同刚骨外科男主治医师本科徐守学骨外科男副主任医师本科王宜栋骨外科男执业医师本科赵磊骨外科男执业医师本科一类二类新技术三类分类(自评)该技术项目当前在国内外或其余省、市医院临床应用基本状况:该技术项目当前在国内三级医院及部分二级综合性医院已广泛展开,在大的三级医院已展开数十余年,有大综病例报告。
临床应意图义、适应症和禁忌症:锁定螺钉为自攻螺钉,能够不用攻丝或骨钻;钢板与骨皮质间无加压力,对骨膜不产生压力,从而保护骨膜的血运;在手术技术上能够知足微创操作的要求,能够很好地保护骨折局部的血运,从而不需要植骨操作;内固定支架弹性固定,在载荷存在的状况下,骨折块间有应力刺激,这类刺激有益于骨痂形成,有益于骨折愈合。
适应症:(1)加压原则,用于骨质松散的骨干骨折;(2)中和原则,也用于骨质松散的骨干骨折;(3)桥接原则(“锁定内固定”原则),用于粉碎性骨干骨折或干骺端的关节外骨折;(4)联合原则(“联合钢板”原则),用于粉碎性干骺端关节内骨折。
锁定钢板固定骨折的经典和理想的适应症是桥接原则和联合原则。
而联合原则指一块钢板上使用加压和桥接两个生物力学原则。
平常的说就是既能够加压又能够锁定,在此基础上便有了锁定加压钢板( LCP )。
2.严重心肺功能不可以耐受手术的。
3.对麻药、冷静药有过敏者。
社会效益、经济效益展望:该技术拥有难过小,恢复快,成角稳固性好,能够保护骨的血液供给,微创植入,显然缩短住院时间,减少病人难过,该技术的应用推行又显然降低患者的住院时间及药品使用量,同时增添了医院的床位周转率。
新技术、新项目的诊断惯例及操作规范:取肩部前外侧纵行切口,逐层切开皮肤,皮下组织,深筋膜,分别肌肉组织,延胸大肌及三角肌空隙显现肱骨近端,见肱骨外科颈骨折种类,消除淤血组织,将骨折复位,复位满意后置入 4 孔肱骨近端锁定钢板,电钻钻孔,拧入螺钉固定,活动患肢,见骨折断端稳固,内固定无松动,频频冲刷切口,检查术野无活动性出血,盘点纱布器材无误后,于切口内搁置皮管 1 根引流,逐层封闭切口,手术结束。
图说经典手术:肱骨近端骨折钢板内固定术

图说经典手术:肱骨近端骨折钢板内固定术肱骨近端骨折是常见的损伤,在所有骨折中约占4-5%,65岁老年患者常伴有骨质疏松症。
切开复位内固定目前是肱骨近端骨折应用非常广泛的治疗方式。
本图文详解较为常见的三角肌胸大肌间隙入路肱骨近端骨折钢板内固定术。
分型肱骨近端骨折AO分型可分为A、B、C型:A型包括关节外骨折,即2段骨折(简单的结节撕脱和外科颈骨折)B型为2处或3段骨折肩关节脱位的外科颈骨折,一个结节骨折;C型包括合并或不合并肩关节脱位的解剖颈骨折。
适应症1.移位以及不稳定的二部分骨折,三部分骨折和四部分骨折;2.涉及肱骨干的近端骨折。
禁忌症1.稳定、未移位或轻度移位的肱骨近端骨折;2.肱骨头劈裂或者粉碎性骨折;3.存在严重的基础疾病,身体情况差;4.局部软组织感染。
手术步骤本病例是左侧肱骨近端外科颈骨折不伴肌腱的断裂。
1.体位:取沙滩椅位或仰卧位。
2.行消毒铺巾,露出患肢肩关节以下部分,左手绑无菌绷带。
3.切口:采用三角肌胸大肌间隙入路,从喙突外侧边缘开始做直线式皮肤切口,直到肱骨三角肌粗隆部位。
4.暴露三角肌,胸大肌界面及其间沟。
5.切开间沟筋膜,显露并保护头静脉。
6.拉钩将头静脉牵向外侧。
7.分离胸锁筋膜和松解近端的喙肩韧带。
8.以骨膜剥离子钝性分离肩峰下和三角肌下的间隙。
9.分离三角肌远端止点的前1/2将三角肌钝性牵开。
10. 冲洗血肿。
11. 复位外展内旋肩关节。
12. 点式复位钳固定。
13. 放置锁定钢板。
14. 使用2.5mm钻钻入骨折线远端的第一个螺钉孔(需打穿对侧皮质)。
15. 测深钻孔的深度。
16.用自攻钉攻丝,并用螺丝刀拧入螺丝钉。
17. 于骨折近端拧入第二颗螺钉以固定骨折部位。
18. X-RAY确认钢板放置合适。
19. 取下点式复位钳。
20. 拧入其余螺钉。
21. 拍片确认。
22. 脉压冲洗枪冲洗伤口。
23. 手术刀切开引流管切口,用止血钳放置引流管。
24. 缝合筋膜。
25.缝合皮肤以及皮下组织。
肱骨近端骨折分型及手术方式

肱骨近端骨折分型及手术方式
肱骨近端骨折是一种常见的骨折类型,其分型及手术方式如下:分型:
目前临床应用最广泛的是Neer分型。
该分型依据肱骨近端的四个解剖部位,即肱骨头、大结节、小结节、肱骨干近端,将骨折分为四种类型。
其中,Neer二、三、四部分骨折是指骨折线涉及上述解剖部位中的两个、三个或四个部分。
手术方式:
对于有移位的骨折,特别是Neer二、三、四部分骨折,手术治疗是首选。
具体的手术方式包括以下几种:
1. 切开复位内固定:切开受伤部位以重新对齐骨折,并使用钢板、螺钉等内固定器械固定骨折部位。
2. 髓内钉固定:将髓内钉插入肱骨近端,以固定骨折部位。
3. 钢板内固定:通过钢板将骨折部位固定在适当的位置。
4. 肩关节置换术:对于严重粉碎性骨折或伴有关节面损伤的情况,可以采用肩关节置换术。
需要注意的是,手术方式的选择应根据患者的具体情况和医生的经验来确定。
患者应在医生的指导下进行治疗,并在术后进行康复训练以促进恢复。
锁定钢板治疗肱骨干骨折14例临床分析
染经过清创换 药 , 于术后 7周伤 口愈合。1 3例 (2 8 %) 9 .6 术后 1 内骨 折 愈合 。1 骨 折延 迟 6周 例 愈合 , 例为 C 该 3型 骨折 , 中一 大 骨块 分 离 间隙 其 >1 5c 术后 1 时 骨折 间 隙仍 明显 , . m, 2周 给予 局 部植 入 自体髂 骨碎 块 , 于植 骨术后 l 周 愈合 。术 1 后 肩关 节和肘 关节 活动 基本 满意 。
1 资 料 与方 法
本组 1 , 4例 均使 用 Snhs 司 4 5mm 窄 y te 公 , 直型锁 定钢板 治 疗 , 1 男 0例 , 4例 ; 龄 1 ~ 女 年 9 6 4岁 。交通 事故伤 5 , 例 坠落 伤 2例 , 伤 5例 , 摔 直 接打 击伤 2例 。按 AO长骨 骨折 分 型 :A 2型 2 例 , 1 2例 , 2B B 型 B 、 3型各 1例 , 1型 3例 ,C c 2 型 3例 , 3型 2例 。伴 有 同侧 桡 神 经损 伤 3例 , C 对 侧胫 腓 骨骨 折 、 同侧跟 骨 骨 折 、 面部 外 伤 、 颜 同 侧胫 骨平 台骨 折和 同侧锁 骨 骨折 各 1例 。所 有患 者 均为 闭合 性 骨折 。 手术 方法 : 卧位 , 仰 上肢 外 展 , 出预放 钢 板 标 的远 端 和 近端 , 钢 板 中 心位 于 骨折 中 心 区 域 。 使 般 选 l ~1 0 4孔 长 度 的钢 板 。在 预 放 钢板 的远 近端 分别做 长 3 I 向切 口。近端 切 口注意 ~4c n纵
的地方 安放 螺钉 做 弹 性 固定 。使 用 长 的锁 定 钢 板 , 过 间接 复位技 术 复位 骨折端 , 用远 近端 的 通 利 小切 口放置钢 板 , 以提 供 弹 性 的 比较 牢 固的 固 可 定模式 , 同时手 术创 伤 比较 小 【2。本 院 2 0 1] - 0 5年
肱骨干骨折固定手术记录

肱骨干骨折固定手术记录患者姓名:XXX 年龄:XXX 性别:XXX手术医生:XXX 手术日期:XXX手术操作记录:一、麻醉准备1. 患者经全面评估后,决定采用麻醉方式:(一般麻醉/全麻/腰硬联合麻醉)2. 由麻醉科医生对患者进行麻醉操作,成功实施麻醉。
二、手术准备1. 患者被放置于手术台上,并做好各项监测,保证患者的生命体征稳定。
2. 手术室准备好所有手术所需器械和材料。
三、手术步骤1. 术前皮肤消毒,用无菌巾包裹患肢。
2. 采用XX切口进入手术部位,注意避免伤及周围组织。
3. 通过XX工具进行骨折复位和对骨折部位进行准确的定位。
4. 选择合适的固定材料(如钢板、钢钉、内固定器等)进行骨折的固定。
5. 注意固定材料的位置和数量,以保证骨折部位的稳定。
6. 手术结束前,再次确认骨折部位及固定材料的位置。
四、术后处理1. 清洁手术部位,缝合切口或进行敷料。
2. 进行必要的X光检查,确认骨折固定的效果。
3. 将患者转入恢复室,继续监测患者的生命体征,观察手术效果。
4. 开始配合康复科进行后续康复训练,并嘱咐患者注意手术部位的保护。
五、手术结束1. 填写完整的手术记录,包括患者信息、手术医生信息、手术过程及操作等。
2. 向患者及家属说明手术情况、预后及注意事项,并解答相关问题。
六、术后随访1. 安排患者到门诊进行术后定期复查,观察骨折愈合情况。
2. 根据患者的情况,制定相应的康复计划和措施。
本文为肱骨干骨折固定手术记录,按照手术的步骤和逻辑,对手术过程进行详细描述。
所有的操作均按照规范的医疗程序进行,保证手术效果和患者安全。
术后随访的安排和康复计划的制定,旨在确保患者的康复效果。
肱骨骨折固定手术记录

肱骨骨折固定手术记录手术日期:XXXX年XX月XX日患者姓名:XXX住院号:XXX性别:XX手术解剖部位:右上肢手术名称:肱骨骨折固定术手术操作记录:一、麻醉方式:采用全身麻醉,将患者转至手术室后,行麻醉准备,将患者平卧于手术床上,给予氧气吸入,建立静脉通路。
二、体位及术前准备:患者取坐位,右上肢外展平放于手术床上,保持肩关节前屈。
术前对患者进行术前皮肤消毒,覆盖无菌巾,确保手术区域清洁无菌。
三、手术切口及肩关节暴露:按照清洗创面→铺巾→戴手套→切皮麻醉为顺序,将手术区域覆盖无菌巾。
于右侧肱骨上臂外界、内板2cm处进行手术切口切开,利用手术器械轻轻撑开切口,暴露肱骨骨折部位。
四、骨折复位及固定:经仔细的术前检查,发现患者肱骨骨折幅度较大,先进行骨折复位,制备骨折面。
复位后使骨折两端对齐,保持稳定状态。
接着选择合适的内固定材料,经过切开,将断端骨折面较好的对齐后,使用无菌牵引器将骨折面并铺开,使用骨折钢板和螺钉进行牵引固定。
五、术后处理及结局:完成固定后,小心清洁手术部位,确保无血迹和杂质。
将手术区域进行切口缝合,应用适当的敷料进行覆盖,用胶布固定术后敷料。
术后进行X线检查,确保骨折骨端对齐位置正确,固定稳定。
手术结束后,将患者送往恢复室继续监护。
六、术中并发症:本次手术过程中未出现明显的术中并发症。
七、术后医嘱:1. 术后第X天拆线,密切观察手术切口是否感染。
2. 康复期间,饮食要均衡,禁止吸烟酗酒,避免剧烈运动。
3. 定期进行复查,根据情况调整康复锻炼方案。
4. 如有异常或疑问,及时就医并保持良好的休息。
八、手术材料:骨折钢板、螺钉、缝线、手术刀、无菌巾、生理盐水等。
以上为本次肱骨骨折固定手术的记录。
手术过程中,手术团队密切配合,操作规范,未出现意外情况。
术后及时给予适当的医嘱,以促进患者早日恢复健康。
术后将继续密切观察患者的康复情况并进行复查,确保手术效果良好。
锁定接骨板桥接固定肱骨干中、上段复杂骨折
结果
全 部获得随访 , 时间 6~1 ( . 2 2 个月 。患者均获得 骨性 愈合 , 4 9 0± . ) 时间 3— ( . 10 个月 。肩 关 7 4 44 . ) - 锁定钢板
节外 展上举 活动度为 0 一10 , 。 4 。 肘关节屈伸 活动为 0 ~10 , 。 3 。 无桡神经损伤等并 发症 出现。结论 桥接 固定 是治疗肱骨 中 、 上段复杂骨折 的良好 的方法。
tr lb i g n x to wih l c i lt s wiho o r f. Al he c s s e na rd i g f ain t o kng pa e t utb ne g a t i l t a e we e lo d e ry f nci n le e cs s r alwe al u to a x r ie a d r c i e a i g a i x mi ai n v r mo t s o to e a iey. Re uls I s v rfe h o g o 4 n e ev d r d o rph c e a n to e e y 2 n h p s— p r tv l s t twa e i d t r u h a 6 t 1 i
( v rg di . aea e 9 0±2 2 m nh f o o — po e1 ae a al a trs a e o eu inw t s t f tr j i n . ) o ts l w u nt 2 c ss h t l f c e g i db n no i a s co n ofl h t u n r h ia y o t fn t n a d c o f 。~1 0 f h h ud r o tf x n a d e t t n o 。 。o eeb w jit w to t u c o : b u t n o i i 0 4 。o es o le i , e i n x ni f ~1 0 f h lo n , i u t jn l o e o 0 3 t o h c m l a o sl ei u f a i ev .C n l s n B ig g x t nw t l kn l ei a f ci l ra v o pi t n k j r o da n re o c i s r i ai i c i pa n e et ea en t e ci i n y r l u o d n f o i ho g t s f v t i
微创经皮钢板内固定治疗老年人肱骨近端骨折

Jun l f rc cl to ad sVo. 7No 7J 12 l o ra o at a Or p ei 11 , . ,u. 0 1 P i h c
关 键 词 : 骨 ; 折 ; 固定 术 ; 骨 近 端 锁定 加 压 钢 板 肱 骨 内 肱 中图 分 类 号 : 8 . 1 R6 3 4 文 献 标 识 码 : B
老年人肱骨近端骨折是常见的创伤骨科疾病, 常合并老 年性骨质疏松症 , 病理改变包括骨质量和密度下降、 有机组 织含量减少、 骨小梁萎缩等[。外固定对骨折端的加压作用 1 ]
优良率, 包括疼痛 3 分, 5 功能 3 分, 0 活动度 2 分, 5 解剖位置
二期行修薄整形后获得较好的外形; 例采用受区皮神经与 8 胸背神经缝接重建皮瓣感觉, 例恢复较好的感觉, 4 证实缝 接胸背神经重建背阔肌皮瓣感觉的可行性 。 j肌瓣可重建动 力肌功能, 特别适合于合并动力肌缺损的创面修复, 2例背
阔肌桥 接受 区肌 肉, 肌力均达 4 级。
图 l 切取 右侧 背阔肌皮 瓣, 2 设计大小 2 m×1 m 2c 4c
指 导 功 能 锻 炼 , 评 定 其 疗 效 。结 果 手 术 时 间 ( 0 1 0 2 ai 出 血 ( 6 3 - 7 8 并 4 . ±1 . )r n, 9 . 4 1 . )mL, 术 切 口长 度 ( . ±0 9 手 56 . )
C l 6例 均 获 随访 4 2 个 月 , 均 1 . n 。1 ~ 2 平 3 6个 月 , 有 患者 均骨 性 愈 合 , 合 时 间 ( 1 2 i O 周 。无 一 例 发 生 复 位 丢 所 愈 1. ± . ) 失 、 固定 失 败 、 染 、 骨 头 缺 血 性 坏 死 或 神 经 血 管 损 伤 。 N e 评分 标准 , 良率 8 。结 论 内 感 肱 按 er 优 8 治疗老年人肱骨近端骨折创伤小 , 出血 少 , 愈 合 时 间 短 , 能 恢 复 好 , 后疼 痛少 。 骨 功 术 利 用 MI P 技 术 PO
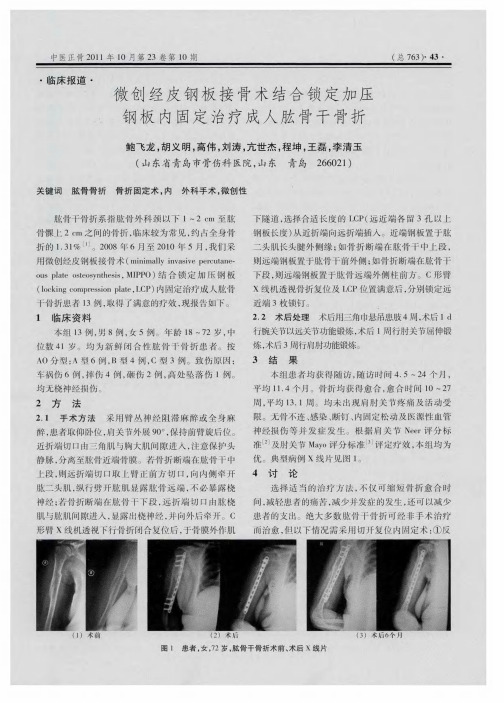
微创经皮钢板接骨术结合锁定加压钢板内固定治疗成人肱骨干骨折
集 中, 减少 应力 遮挡 ; ⑤不 影 响上 下关 节 活 动 ; 叮以 ⑥ 早期进 行 功能锻 炼 。手术 应 注意 以下 事 项 : ①术 前 医
生要对 上 肢解 剖结 构非 常熟悉 ; 术 中需 要 良好 的透 ②
视 ; 术 中操作 要谨 慎 , ③ 以防损 伤桡 神 经 ; 固定钢 板 ④
合 ; MIP ③ P O技 术 属 于桥 式 接 骨 范 畴 , 以最 小 的 面 积与 骨面 接触 , 口小 , 不 显露 骨折 断 端 ; 螺钉‘ 切 且 ④ 密
度低 , 未被 螺钉 穿 过 的 钢 板 相 对 较 长 , 冈 钢 板 每 单 位面积 上分 配 的应力 相应 减 少 , 免 了钢板 应 力过 于 避
中医正 骨 2 l 0 1年 l 0月 第 2 3卷 第 l 0期
复手 法复 位失 败 , 折 对 位 对 线 不 良 ; 骨 折 有 分 离 骨 ②
以抗旋 转应 力 ; 锁 定 钢 板 无需 精 确 塑 形 , 以避 免 ② 可
传统 钢板 塑形 不 当带来 的骨 折移 位 , 板 与骨 之 问 的 钢 间 隙有 利 于 保 护 局 部 血 液 循 环 , 利 于 骨 折 的 愈 有
( 6):0 7 —1 8 . 17 0 9
[ ] Moe F A a A Smcnt ie r t l t f’h 3 r yB , dms . e ios a dat o a yo te l R rn h p s x t a n frema i at iso h lo J . o e r t t hu td r ri fteebw[ ] JB n e me o o h t
社 ,0 7 8 9— 4 . 2 0 :2 8 1
[ ] N r C n . i i e r i a h m rsf c rsICa— 2 e ’ S2 d Ds a dpo m l u eu at e.. l o pc x r u s s ctnad ea ai J . oeJitSr ,90 5 i a o n vl t n[ ] J Bn o ug 17 : 2 i f i u o n
肱骨骨折手术步骤
肱骨骨折手术步骤
肱骨骨折手术的步骤可能会因骨折的类型、位置和严重程度而有所不同,以下是一般情况下肱骨骨折手术的基本步骤:
1. 术前准备:患者通常需要接受全面的身体检查,包括血液检查、心电图等。
医生会对骨折部位进行 X 光和其他影像学检查,以确定骨折的类型和程度。
2. 麻醉:手术通常在全身麻醉或臂丛神经阻滞麻醉下进行。
3. 切口:根据骨折的位置,医生会在肩部或肘部做一个适当的切口,以暴露骨折部位。
4. 复位:医生使用牵引、撬拨等手法,将骨折端复位到正常位置。
5. 固定:复位后,医生会使用钢板、螺钉、髓内钉或其他固定装置将骨折固定在正确的位置。
这些固定装置可以帮助骨折愈合,并保持骨骼的稳定性。
6. 缝合:固定完成后,医生会仔细检查伤口有无出血,然后将切口缝合。
7. 术后处理:手术后,患者的手臂通常会被固定在石膏或支具中,以帮助骨折愈合。
患者需要遵循医生的指示进行康复锻炼,以恢复手臂的功能。
需要注意的是,每个人的身体状况和骨折情况都不同,因此手术步骤可能会有所调整。
在手术前,医生会详细向患者解释手术过程和风险,并根据患者的具体情况制定个性化的手术方案。
肱骨近端骨折切开复位内固定手术记录模板

肱骨近端骨折切开复位内固定手术记录模板
肱骨近端骨折是一种常见的损伤,通常需要手术来治疗。
而肱骨近端骨折切开复位内固定手术是一种常用的手术方法,下面将分步骤阐述该手术的具体过程。
一、手术准备
1.术前准备骨科手术器械,包括镊子、骨用力钳、骨探、锥形针、股二头肌钩、钢板、螺钉等。
2.麻醉。
3.患肢必须清洗干净,并做好消毒处理。
二、手术切口
1.使用手术刀,在患者肘部皮肤隆起的部位,做出一直性的5厘米长的皮肤切口。
2.用镊子将皮下组织和肌肉切开,将骨折部位暴露出来。
3.清理软组织和坏死组织,将表面清理干净,以免感染。
三、骨折复位
1.使用骨探和锥形针的组合破坏骨折局部骨小梁,以便进行复位。
2.使用骨用力钳和股二头肌钩进行牵拉,使骨折部位达到理想复位位置。
3.复位后,使用一块小骨板和三个螺钉将骨折部位固定住,以确保骨折复原。
四、伤口缝合
1.在确认骨折部位固定后,清洗切口,并进行缝合。
2.伤口缝合后,进行消毒处理。
五、术后处理
1.将患者送到恢复室,对患者进行密切观察。
2.在恢复室监测患者的身体反应和生命体征。
3.恢复室观察完成后,进行康复治疗。
以上就是肱骨近端骨折切开复位内固定手术的步骤,虽然手术内
容较为复杂,但是医生们总是严格按照步骤执行,以确保手术的成功。
如果您有这方面的需求,请及时咨询专业的医生,以便选择适合您的
治疗方式。
微创经皮锁定钢板内固定治疗肱骨干骨折

微创经皮锁定钢板内固定治疗肱骨干骨折【摘要】目的探讨微创经皮锁定钢板内固定治疗肱骨干骨折的临床效果。
方法自2006年4月至2008年8月微创经皮锁定钢板内固定治疗肱骨干骨折24例,按ao分型标准:a型12例,b型8例,c型4例。
结果 24例获得随访,平均15个月(10~21个月),x线片显示骨折全部一期愈合,平均愈合时间为6个月,均无感染、骨不连、钢板松动等并发症。
按照rodriquez-merchan评分标准;优18例,良4例,可2例,优良率91.7%。
结论微创经皮锁定钢板内固定治疗肱骨干骨折,符合生物力学固定的观念,手术操作简单,创伤小,内固定牢靠,骨折愈合率高。
【关键词】微创;锁定钢板;接骨术;肱骨干;骨折腺样体切除术治疗腺样体肥大患者105例,效果良好,现报告如下。
1 资料与方法1.1 一般资料105例病例中,男67例,女38例,年龄4~8岁,病程半年~3年1.2 手术方法患儿性全麻插管成功后,取仰卧正中位,常规消毒手术野,铺无菌巾,肾上腺素生理盐水棉片收缩双侧鼻腔黏膜,鼻内窥镜下检查鼻咽部腺样体,电动吸切器切除肥大的腺样体,创面电凝止血,检查有无腺样体残留,术毕严密观察咽部出血情况。
1.3 术后处理卧床休息,全身应用抗生素3-5 d,预防感染。
2 结果本组105例病例术后症状消失,无并发症。
3 讨论腺样体肥大为小儿常见病之一,其主要症状为:①耳部症状:可引起分泌性中耳炎,出现传导性聋及耳鸣症状。
②鼻部症状:常合并鼻炎及鼻窦炎耳出现鼻塞、流鼻涕等症状,可有张口呼吸、讲话闭塞性鼻音及睡眠时打鼾等症状,长期者可出现“腺样体“面容”。
③咽喉及下呼吸道症状:分泌物向下流并刺激呼吸道黏膜,可出现阵咳,易并发支气管炎,可有低热。
④全身症状:主要为慢性中毒及反射性神经症状。
传统的手术方法为腺样体刮匙刮除法和腺样体切除器切除法,由于是在盲视下操作,易造成腺样体残留、咽后壁及咽侧壁的损伤,且出血较多。
鼻内窥镜下腺样体切除术则是用鼻内窥镜配备的切割器直视下切除腺样体,如有出血,采用电凝止血。
桥接组合式内固定手术治疗上肢骨折的临床分析

桥接组合式内固定手术治疗上肢骨折的临床分析【摘要】目的:探究桥接组合式内固定手术治疗上肢骨折的效果。
方法:将2020年3月至2020年9月入选的82例患者随机分为对照组和观察组,各41例。
对照组采用钢板内固定术治疗,观察组采用桥接组合式内固定手术治疗。
比较两组治疗效果、疼痛程度和肩关节功能评分。
结果:观察组治疗总有效率97.56%;高于对照组治疗总有效率80.49%。
对比两组数据,P<0.05,有统计学意义。
治疗前两组患者VAS评分和Constant评分对比,差异无统计学意义(P>0.05);治疗后观察组患者VAS评分(2.96±0.38)分,低于对照组(4.29±0.84)分,Constant评分(33.08±0.71)分,高于对照组(28.16±0.46)分,对比两组护理后数据,P<0.05,有统计学意义。
结论:针对上肢骨折患者采用桥接组合式内固定手术治疗能够有效降低疼痛程度,促进患者肩关节功能恢复,且具有较高的治疗效果,值得推广。
【关键词】桥接组合式;内固定手术;上肢骨折上肢骨折在临床中比较常见,主要是由于患者跌倒、车祸等因素造成。
针对这种疾病临床中主要采用手术治疗,但是不同手术治疗所取得的效果不同。
钢板内固定在临床中使用概率较大,范围比较广,但是由于其存在一些=缺陷,容易影响患者血液循环,使得患者伤口愈合较慢[1]。
而桥接组合式内固定手术操作更加灵活,且手术材料可塑性较强,有利于患者快速恢复健康。
本研究对82例上肢骨折患者进行分析,现报道如下。
1资料与方法1.1临床资料将2020年3月至2020年9月入选的82例患者随机分为对照组和观察组,各41例。
对照组男21例,女20例。
年龄20-68岁,平均年龄(40.36±2.14)岁。
观察组男22例,女性19例。
年龄22-69岁,平均年龄(41.29±2.36)岁。
两组患者一般资料比较P>0.05,无统计学意义,有可比性。
C臂下闭合复位微创锁定钢板内固定治疗肱骨干骨折的临床研究
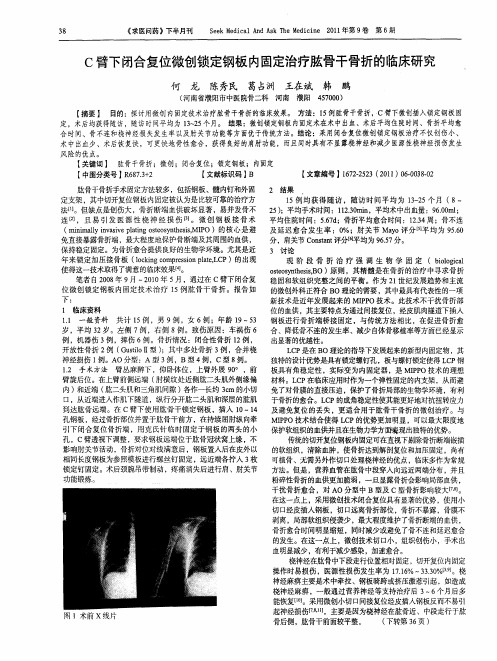
【 摘要 】 目的: 探讨用微创内固 定技术治疗肱骨干骨折的临 床效果。 方法:1 例肱骨干骨折, 5 C臂下微创插入锁定钢板固 定,术后均获得随访,随访时间平均为 1 2 个月。 结果:微创锁定钢板内固 3 5 ~ 定术在术中出血、术后平均住院时间、骨折平均愈
合 时间、骨不连和桡神经损失发生率 以及肘关节功 能等方面优于传统方法。结论 :采用闭合复位微创锁定钢板治疗不仅创伤小、 术 中出血少、术后恢复快,可更快地骨性愈合,获得 良 的肩肘功能,而且同时具有不显露桡神经和减少医源性桡神经损伤发生 好
风 险的优点。
【 关键词 】 肱骨干骨折;微创;闭合复位;锁定钢板;内固 定 【 中图分类号 】 67 + R 8. 2 3 【 文献标识码 】 B
.
【 文章编号】 62 53(01 0— 3- 17- 2 21) 6 08 2 2 0 0
肱骨干骨折手术固定方法较多 ,包括钢板、髓内钉和外固 2 结果 定支架 ,其中切开复位钢板内固定被认为是 比 较可靠的治疗方 1 均获 得 随访 ,随访 时间平 均为 1~ 5个 月 ( 5例 32 8— 法[。但缺点是创伤大,骨折 断端血供破坏显著 ,易并发骨不 2 ) u 5 ;平均手术时间 :123m n 1. i ,平均术 中出血量:9 . m ; 0 6 Ol O 连 [,且 易 引 发 医源 性 桡 神 经 损 伤 [。 微创 钢 板接 骨 术 平均住院时间 :56d . ;骨折平均愈合时间 :1. 7 23 ;骨不连 4周 ( ii l vs e l n s oyteiMIO)的核 心是避 及延迟愈合 发生 率 :O mnmayi a v yi ot snhs , P l n i p g e s %;肘关节 Mao评 分【平均为 9 . y 】 56 O 免直接暴露骨折端,最大程度地保护骨断端及其周围的血供 , 分,肩关节 C ntn 评分【 os t a 1 平均为 9 . 6 7分。 5 保持稳定 固定。为骨折愈合提供 良好的生物学环境 。尤其是近 3 讨 论 年来锁定加压接 骨板 (okn o rsi le C 1cigcmpes npa , P)的出现 o tL 现 阶 段 骨 折 治 疗 强 调 生 物 学 固 定 (bo g a il i l o c 使得这一技术取得 了满意的临床效果[ 4 】 。 o es t s,O) soy h iB 原则 ,其精髓是在骨折的治疗 中寻求骨折 t n es 笔者 自2 0 年 9月 一2 1 08 0 0年 5 ,通过在 C臂下闭合复 稳 固和软组织完整之 间的平衡 。作为 2 世纪发展趋势和主流 月 1 位微创 锁定钢板 内固定技术 治疗 1 肱骨干骨折 。报告 如 的微创外科正符合 B 5例 O理论的需要 ,其中最具有代表性的一项 下: 新技术是近年发展起来 的 MIP P O技术 。此技术不干扰骨折部 1 临 床资 料 位 的血供 ,其主要特点为通过间接复位 ,经皮肌 肉隧道下插入 11 一般 资料 共计 1 ,男 9例 ,女 6例 ;年龄 1 ~5 钢板进行骨折端桥接 固定 ,与传统方法相比 , . 5例 9 3 在促进骨折愈 岁 ,平均 3 。左侧 7 ,右侧 8 。致伤原因 :车祸伤 6 合 、降低骨不连的发生率、减少自体骨移植率等方面已经显示 2岁 例 例 例 ,机器伤 3 ,摔伤 6例 。骨折情况 :闭合性骨折 1 , 例 2例 出显著的优越性。 开放性骨折 2例 ( utoI ) 中多处骨折 3 ,合并桡 G slI型 ;其 i 例 L P是在 B C O理论的指导下发展起来的新型内固定物 ,其 神经损伤 1 例。A O分型 :A型 3例 ,B型 4 ,c型 8 例 例。 独特的设计优势是具有锁定螺钉孔,板与螺钉锁定使得 L P钢 C 1 手术方法 臂丛麻醉下 ,仰卧体位 ,上臂外展 9。 ,前 板具有角稳定性 ,实际变为内固定器 ,是 MIP . 2 O P O技术的理想 臂旋后位。在上臂前侧远端 ( 肘横纹处近侧肱二头肌外侧缘偏 材料。L P在临床应用时作为一个弹性固定的内 C 支架,从而避 内) 和近端 ( 肱二头肌和三角肌间隙 ) 各作一长约 3m的小切 免 了对骨膜的直接压迫 ,保护了骨折局部的生物学环境,有利 c 口,从近端进入作肌下 隧道 ,纵行分开肱二头肌和深层的肱肌 于骨折的愈合。L P的成角稳定性使其能更好地对抗扭转应力 C 到达肱骨远端 。在 c臂下使用肱骨干锁定钢板 ,插入 l 4 及避免复位 的丢失 ,更适合用于肱骨干 骨折 的微创治疗。与 0—1 孔钢板 ,经过骨折部位并置于肱骨干前方 ,在持续屈肘纵向牵 MIP P O技术结合使得 L P的优势更加明显 ,可 以最大限度地 C 引下 闭合复位骨折端 ,用克 氏针临时 固定于钢板 的两头 的小 保护软组织的血供并且在生物力学方面表现出独特的 优势。 孔 ,C臂透视下调整 , 要求钢板远端位于肱骨冠状窝上缘 , 不 传统的切开复位钢板内固定可在直视下剔除骨折断端嵌插 影响肘关节活动 ,骨折对位对线满意后 ,钢板置入后在皮外以 的软组织 ,清除血肿 , 使骨折达到解剖复位和加压固定 ,尚有 相 同长度钢板为参照模板进行螺丝钉 固定 ,远近端各拧入 3 枚 可植骨、无需另外作切 口处理桡神经的优点,临床多作为常规 锁定钉固定 。术后颈腕吊带制动 ,疼痛消失后进行肩 、肘关节 方法。但是 ,营养血管在肱骨中段穿人 向远近两端分布 ,并且 功能锻炼。 粉碎性骨折的血供更加脆弱 ,一旦显露骨折会影响局部血供 , 干扰骨折愈合 , A 对 O分型 中 B型及 C型骨折影响较大【] 7。 l 8 在这一点上 ,采用微创技术闭合复位具有显著的优势 ,使用小 切 口经皮插入钢板,切 口远离骨折部位 ,骨折不暴露 ,骨膜不 剥离 , 局部软组织侵袭少,最大程度维护了骨折断端的血供 , 骨折愈合时间明显缩短,同时减少或避免了骨不连和延迟愈合 的发生。在这一点上, 微创技术切口 小, 组织创伤小,手术出 血明显减少 ,有利于减少感染,加速愈合。 桡神经在肱骨中下段走行位置相对固定, 切开复位内固定 操作时易损伤 ,医源性损伤发生率为 1. %一 3 O 【] 7 6 3- % 。桡 1 3 神经麻痹主要是术 中牵拉 、 钢板骑跨或挤压激惹引起 , 如造成 桡神经麻痹 , 一般通过营养神经等支持治疗后 3 6 ~ 个月后多 能恢复[ 。采用微创小切 口间接复位经皮插入钢板反而不易引 1 0 】 起神经损伤【 】 l,主要是因为桡神经在肱骨近、中 】 段走行于肱 罔 1术前 x线片 骨后侧,肱骨干前面较平整 , ( 下转第 3 页 ) 6
肱骨干骨折手术记录

肱骨干骨折手术记录手术日期:xxxx年xx月xx日手术医生:xxxx医生手术记录患者信息:姓名:XXX性别:男年龄:XX岁住院号:XXXXX诊断:右上肢肱骨干骨折手术准备:患者进入手术室后,安全固定在手术床上,注意采取足够的保护措施,确保手术区域无菌。
进行全身麻醉,患者处于舒适、安稳的状态下。
手术步骤:1. 感染控制与准备:对患者右上肢进行局部消毒,使用无菌铺巾覆盖手术区域。
穿戴手术手套、口罩和帽子,确保手术操作符合无菌操作要求。
在上臂外侧进行皮肤切口,切口长约xx厘米。
然后依次经过皮下组织、肌肉、深筋膜等结构,切开至肱骨皮质。
3. 全骨直视下复位:通过切口观察肱骨断端情况,用骨钳、骨针等工具进行骨折端的定位与复位。
在充分清理骨折断端碎屑后,钢板和螺钉的选择的根据骨折段骨质状况进行选择。
4. 钢板固定:在骨折处选择合适型号和长度的钢板,将其固定在肱骨上。
通过钢板与肱骨的紧密接触,保持骨折段的稳定性。
合理调整钢板的位置,确保其与骨骼充分接触,并且不对周围组织产生压迫。
5. 固定螺钉的放置:根据肱骨骨折破坏情况,在螺钉孔上预先钻孔,选择合适大小的钢钎或骨塞将固定螺钉放置在肱骨内。
6. 切口关闭:经过检查确认钢板和螺钉的位置和固定情况后,逐层将切口进行缝合。
注意缝合时要将皮肤边缘对齐,使切口美观、整洁。
7. 术毕处理:清理手术区域,观察切口出血情况,确认手术区域无渗血现象。
将术区创面进行敷料包扎,定位固定患者的上肢。
手术过程中,患者配合良好,手术操作顺利完成。
术后拍片显示骨折复位满意,螺钉与钢板固定良好。
患者术后无异常症状,未发现手术相关并发症。
手术医生:xxxx医生审核医生:xxxx医生以上为我所负责的手术记录,如有任何问题,请随时与我联系。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
1.1、原则桥接钢板Bridge plating uses the plate as an extramedullary splint, fixed to the two main fragments, while the intermediate fracture zone is left untouched. Anatomical reduction of the shaft fragments is not necessary. Furthermore, direct manipulation risks disturbing their blood supply. If the soft tissue attachments are preserved, and the fragments are relatively well aligned, healing is predictable.桥接钢板把钢板作为髓外夹板,固定两个主要骨折端,而骨折区域不予干预,肱骨干骨折不必解剖复位,并且,直接操作复位有干扰骨折端血供的风险,如果保留软组织的连续,骨折愈合可能性增加。
Alignment of the main shaft fragments can usually be achieved indirectly utilizing traction and soft tissue tension.主要骨折块的对位对线可以通过间接使用牵开器和软组织附着性来完成。
Mechanical stability, provided by the bridging plate, is adequate for indirect healing (callus formation). Occasionally, a larger wedge fragment might be approximated to the main fragments with a lag screw. Lag screws should be avoided when there are multiple fragments桥接钢板提供稳定性,对于骨折二期愈合(骨痂愈合)是充足的,个别情况下,一个大的楔形骨折需要用拉力螺钉固定到主要骨折块,在多段骨折情况下避免使用拉力螺钉。
1.2 桥接钢板的置入 Bridge plate insertionBridge plates can be inserted either with an open exposure, or through a minimally invasive (MIO) approach, which leaves soft tissues intact over the fracture site. The latter requires fluoroscopic monitoring. With open bridge plating, it is important to preserve soft-tissue attachments to the fracture fragments. To do this, stable provisional reduction (with external fixation, large distractor, or maintained manual traction), and minimal exposure and manipulation of the fracture zone are important. The bridge plate is applied through an incision just wide enough for the plate.桥接钢板可以通过切开显露,或通过微创显露置入,在MIO情况下可以保留骨折区域软组织完整性,但其要求术中透视帮助。
桥接钢板技术,保留骨折断端软组织连续性是很重要的,为了做到这个,稳定的临时复位(通过外固定架,大的牵开器,持骨器),最小程度显露和操作骨折区域是很重要的,桥接钢板需要手术切口可以置入钢板即可。
1.3 复位 ReductionIt is important to restore axial alignment and rotation. A little shortening of 1 or 2 cm can be accepted in the humerus, and in complex multifragmentary fractures may improve bone contact.Exceptionally, a large fragment has been separated from the fracture with a sharp end impaled in the adjacent muscle. This may need to be repositioned directly with protection of soft-tissue attachments.复位骨折轴向序列和旋转移位是重要的,短缩1-2cm是可以接受的,在复杂多段骨折可以提供骨的接触。
另外一些情况,大骨折块从骨折断端分离插入临近的肌肉组织,此中情况需要直接复位骨折,同时注意保护软组织连续性。
2.1 钢板的位置 Plate locationThe humerus has an anterolateral, a posterior, and a medial surface to each of which a plate can be applied. The location of the fracture will determine where the surgeon chooses to apply a plate to the humerus. The position of the plate is selected according to fracture location, and the length of proximal and distal main segments.肱骨有前外侧面,后面,内侧面,三面都可以应用钢板。
钢板的位置通过骨折位置以及位置。
The location should allow sufficient plate length on both proximal and distal segments, with a minimum of 4 holes for each.钢板在骨折的主要骨折端最少需要4孔长度An anterolateral plate fits well from very proximally to the distal fifth of the humerus.肱骨前外侧可以适合从肱骨最近端到远端1/5的区域。
The posterior surface is difficult to access proximally and is best suited for middle and distal third fractures. Once a location for the plate has been selected, the surgical approach is determined by that location. For proximal fractures, an anterolateral plate location and anterolateral surgical exposure are usual. For distal fractures, a posterior plate location is preferred. This area can be accessed with either a posterolateral, or a posterior, approach. In the central portion of the humerus, the plate can be applied to the anterolateral, lateral, or posterior surfaces, with the approach dependent on the preferred plate location.肱骨后面显露近端较困难,更适合中段和远1/3骨折,当内置物选择完成后,手术切口由骨折位置决定,对于近端骨折,可以前外侧显露和前外侧置入钢板。
对于远端骨折,后侧钢板置入更合适,此区域可以通过后外侧或后侧切口进入。
在肱骨干中段,钢板可以放置在前外侧或外侧,或后侧,切口根据钢板放置位置决定。
The medial surface is generally reserved for complex reconstructive procedures. 内侧面通常为复杂骨折重建应用。
2.2 外侧置入 Lateral platingAn anterolateral approach is chosen for proximal and middle third fractures, and allows supine patient positioning.The lateral approach can also be used, particularly if the most proximal part of the humerus need not be exposed.Distally, the plate may lie deep to the radial nerve.前外侧切口可以用来显露肱骨近端和中1/3骨折,病人仰卧位,如果肱骨近端不需要显露,外侧切口也可以。
在肱骨远端,肱骨位于桡神经深面。
2.3 后方置入 Posterior platingA posterior approach will generally be chosen for more distal fractures.It is important to protect the radial nerve and its accompanying vessels in the spiral groove. Typically, a posterior plate must be placed underneath the radial nerve, to gain proximal bone anchorage.后方入路通常用于肱骨远端骨折。