雷沙吉兰简介
雷沙吉兰溶解度
雷沙吉兰溶解度一、简介雷沙吉兰(Rasagiline)是一种单胺氧化酶A抑制剂,被广泛用于治疗帕金森病和路易体痴呆等疾病。
了解雷沙吉兰的溶解度对于药物制剂的开发、生产和质量控制具有重要意义。
本篇文档将全面介绍雷沙吉兰的溶解度特性。
二、溶解度影响因素影响雷沙吉兰溶解度的因素主要有温度、pH值、溶剂类型和固体粒径等。
温度升高通常会提高溶解度,但也可能导致药物稳定性下降;在不同pH值条件下,雷沙吉兰的溶解度会有所不同;不同类型的溶剂对溶解度也有显著影响;固体粒径越小,比表面积越大,溶解度通常越高。
三、溶解度数据以下是雷沙吉兰在不同条件下的溶解度数据:1.温度:在常温下,雷沙吉兰在水中的溶解度约为1.5mg/mL;在pH值为7.4的磷酸盐缓冲液中,溶解度约为2.0mg/mL;在pH值为1.2的盐酸溶液中,溶解度约为1.0mg/mL。
随着温度的升高,溶解度也会相应提高。
2.pH值:在pH值为 1.2的盐酸溶液中,雷沙吉兰的溶解度最低,为1.0mg/mL;在pH值为7.4的磷酸盐缓冲液中,溶解度为2.0mg/mL;在pH值为9.0的碳酸盐缓冲液中,溶解度最高,可达到约3.5mg/mL。
3.溶剂类型:在不同溶剂中,雷沙吉兰的溶解度有很大差异。
例如,在纯水中,溶解度约为1.5mg/mL;而在乙醇、甲醇或丙酮等有机溶剂中,溶解度会显著提高。
4.固体粒径:雷沙吉兰的固体粒径对其溶解度也有影响。
减小固体粒径可以使比表面积增大,从而提高溶解度。
然而,过小的粒径可能导致药物在溶液中的稳定性下降。
四、结论通过对雷沙吉兰溶解度的研究,可以发现温度、pH值、溶剂类型和固体粒径等因素对溶解度具有显著影响。
在实际应用中,应充分考虑这些因素以优化药物制剂的开发和制备过程。
同时,了解溶解度数据对于药物剂量的确定和给药方案的制定也具有重要意义。
通过对雷沙吉兰溶解度的深入研究,有助于提高药物制剂的质量和治疗效果。
雷沙吉兰fda

_________________ __________________ ______________ _____________ ___________________ _______________________________________________________________________________________________________________________________________ HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use AZILECT ®safely and effectively. See full prescribing information for AZILECT. AZILECT (rasagiline mesylate) Tablets for Oral Use Initial U.S. Approval: 2006 RECENT MAJOR CHANGES • Indications and Usage (1) 05/2014 • Dosage and Administration (2.1) 05/2014 • Warnings and Precautions (5.2, 5.3, 5.6, 5.8, 5.9) 05/2014 INDICATIONS AND USAGEAZILECT, a monoamine oxidase (MAO)-B inhibitor (MAOI), is indicated for the treatment of Parkinson’s disease (1) _______________DOSAGE AND ADMINISTRATION • Monotherapy: AZILECT 1 mg once daily (2.1) • As adjunct without levodopa: AZILECT 1 mg once daily (2.1) • As adjunct to levodopa: AZILECT 0.5 mg once daily. Increase dose to 1 mg daily as needed for sufficient clinical response (2.1) • Patients taking ciprofloxacin or other CYP1A2 inhibitors: AZILECT 0.5 mg once daily (2.2, 5.4) • Patients with mild hepatic impairment: AZILECT 0.5 mg once daily. AZILECT should not be used in patients with moderate or severe hepatic impairment (2.3, 5.5) DOSAGE FORMS AND STRENGTHS • AZILECT 0.5 mg tablets (containing, as the active ingredient, rasagiline mesylate equivalent to 0.5 mg of rasagiline base) (3) • AZILECT 1 mg tablets (containing, as the active ingredient, rasagiline mesylate equivalent to 1 mg of rasagiline base) (3) CONTRAINDICATIONS Concomitant use of meperidine, tramadol, methadone, propoxyphene dextromethorphan, St. John’s wort, cyclobenzaprine, or another (selective or non-selective) MAO inhibitor (4) _______________ WARNINGS AND PRECAUTIONS _______________ • May cause hypertension (including severe hypertensive syndromes) at recommended doses (5.1) • May cause serotonin syndrome when used with antidepressants (5.2) • May cause falling asleep during activities of daily living, daytime drowsiness, and somnolence (5.3) • May cause hypotension, especially orthostatic (5.6) • May cause or exacerbate dyskinesia. Decreasing the levodopa dose may lessen or eliminate this side effect (5.7) • May cause hallucinations and psychotic-like behavior (5.8) • May cause impulse control/compulsive behaviors (5.9) • May cause withdrawal-emergent hyperpyrexia and confusion (5.10) • Increased risk of melanoma: monitor patients for melanoma on a regular basis (5.11) ___________________ ADVERSE REACTIONS ___________________ Most common adverse reactions (incidence 3% or greater than placebo): • AZILECT monotherapy: flu syndrome, arthralgia, depression, dyspepsia (6.1) • AZILECT used as adjunct without levodopa: peripheral edema, fall, arthralgia, cough, and insomnia (6.1) • AZILECT used as adjunct to levodopa: dyskinesia, accidental injury, weight loss, postural hypotension, vomiting, anorexia, arthralgia, abdominal pain, nausea, constipation, dry mouth, rash, abnormal dreams, fall, and tenosynovitis (6.1) To report SUSPECTED ADVERSE REACTIONS, contact TEVA at 1800-221-4026 or FDA at 1-800-FDA-1088 or /medwatch . ___________________ DRUG INTERACTIONS ____________________ • Meperidine: Risk of serotonin syndrome (4, 7.1) • Dextromethorphan: Risk of psychosis or bizarre behavior (4, 7.2) • MAO inhibitors: Risk of non-selective MAO inhibition and hypertensive crisis (4, 7.3) USE IN SPECIFIC POPULATIONS • Pregnancy: Based on animal data, may cause fetal harm. Do not use AZILECT unless the potential benefit justifies the potential risk to the fetus (8.1) See 17 for PATIENT COUNSELING INFORMATION Revised: 05/2014 FULL PRESCRIBING INFORMATION: CONTENTS* 1. INDICATIONS AND USAGE 2. DOSAGE AND ADMINISTRATION 2.1 General Dosing Recommendations 2.2 Patients Taking Ciprofloxacin or Other CYP1A2 Inhibitors 2.3 Patients with Hepatic Impairment 3. DOSAGE FORMS AND STRENGTHS 4. CONTRAINDICATIONS 5. WARNINGS AND PRECAUTIONS 5.1 Hypertension 5.2 Serotonin Syndrome 5.3 Falling Asleep During Activities of Daily Living and Somnolence 5.4 Ciprofloxacin or Other CYP1A2 Inhibitors 5.5 Hepatic Impairment 5.6 Hypotension / Orthostatic Hypotension 5.7 Dyskinesia 5.8 Hallucinations / Psychotic-Like Behavior 5.9 Impulse Control / Compulsive Behaviors 5.10 Withdrawal-Emergent Hyperpyrexia and Confusion 5.11 Melanoma 6. ADVERSE REACTIONS 6.1 Clinical Trials Experience7. DRUG INTERACTIONS 7.1 Meperidine 7.2 Dextromethorphan 7.3 MAO Inhibitors 7.4 Sympathomimetic Medications 7.5 Antidepressants 7.6 Ciprofloxacin or Other CYP1A2 Inhibitors 7.7 Tyramine/Rasagiline Interaction 7.8 Dopaminergic Antagonists 8. USE IN SPECIFIC POPULATIONS 8.1. Pregnancy 8.3. Nursing Mothers 8.4. Pediatric Use 8.5. Geriatric Use 8.6 Hepatic Impairment 8.7 Renal Impairment 9. DRUG ABUSE AND DEPENDENCE 9.1. Controlled Substance 9.2. Abuse 9.3. Dependence 10. OVERDOSAGE 11. DESCRIPTION 12. CLINICAL PHARMACOLOGY 12.1. Mechanism of Action 12.2. Pharmacodynamics 12.3. Pharmacokinetics 13. NONCLINICAL TOXICOLOGY 13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility 14. CLINICAL STUDIES 14.1 Monotherapy Use of AZILECT 14.2 Adjunct Use of AZILECT 16. HOW SUPPLIED/STORAGE AND HANDLING 17. PATIENT COUNSELING INFORMATION *Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATIONAZILECT® (rasagiline tablets)1. INDICATIONS AND USAGEAZILECT (rasagiline tablets) is indicated for the treatment of Parkinson’s disease (PD).2. DOSAGE AND ADMINISTRATION2.1 General Dosing RecommendationsWhen AZILECT is prescribed as monotherapy or as adjunct therapy in patients not taking levodopa, patients may start AZILECT at the recommended dose of 1 mg administered orally once daily.In patients taking levodopa, with or without other PD drugs (e.g., dopamine agonist, amantadine, anticholinergics), the recommended initial dose of AZILECT is 0.5 mg once daily. If the patient tolerates the daily 0.5 mg dose, but a sufficient clinical response is not achieved, the dose may be increased to 1 mg once daily. When AZILECT is used in combination with levodopa, a reduction of the levodopa dose may be considered, based upon individual response.The recommended doses of AZILECT should not be exceeded because of risk of hypertension [see Warnings and Precautions (5.1)].2.2 Patients Taking Ciprofloxacin or Other CYP1A2 InhibitorsPatients taking concomitant ciprofloxacin or other CYP1A2 inhibitors should not exceed a dose of AZILECT 0.5 mg once daily [see Warnings and Precautions (5.4), Drug Interactions (7.6), and Clinical Pharmacology (12.3)].2.3 Patients with Hepatic ImpairmentPatients with mild hepatic impairment should not exceed a dose of AZILECT 0.5 mg once daily. AZILECT should not be used in patients with moderate or severe hepatic impairment [see Warnings and Precautions (5.5), Use in Specific Populations (8.6), and Clinical Pharmacology (12.3)].3. DOSAGE FORMS AND STRENGTHSAZILECT 0.5 mg Tablets: White to off-white, round, flat, beveled tablets, debossed with “GIL 0.5” on one side and plain on the other side containing, as the active ingredient, rasagiline mesylate equivalent to 0.5 mg of rasagiline base.AZILECT 1 mg Tablets: White to off-white, round, flat, beveled tablets, debossed with “GIL 1” on one side and plain on the other side containing, as the active ingredient, rasagiline mesylate equivalent to 1 mg of rasagiline base.4. CONTRAINDICATIONSAZILECT is contraindicated for use with meperidine, tramadol, methadone, propoxyphene and MAO inhibitors (MAOIs), including other selective MAO-B inhibitors, because of risk of serotonin syndrome [See Warnings and Precautions (5.2)]. At least 14 days should elapse between discontinuation of AZILECT and initiation of treatment with these medications. AZILECT is contraindicated for use with St. John’s wort and with cyclobenzaprine.AZILECT is contraindicated for use with dextromethorphan because of risk of episode of psychosis or bizarre behavior.5. WARNINGS AND PRECAUTIONS5.1 HypertensionExacerbation of hypertension may occur during treatment with AZILECT. Medication adjustment may be necessary if elevation of blood pressure is sustained. Monitor patients for new onset hypertension or hypertension that is not adequately controlled after starting AZILECT.In Study 3, AZILECT (1 mg/day) given in conjunction with levodopa, produced an increased incidence of significant blood pressure elevation (systolic > 180 or diastolic > 100 mm Hg) of 4% compared to 3% for placebo [see Adverse Reactions (6.1)].When used as an adjunct to levodopa (Studies 3 and 4), the risk for developing post-treatment high blood pressure (e.g., systolic > 180 or diastolic >100 mm Hg) combined with a significant increase from baseline (e.g., systolic > 30 or diastolic > 20 mm Hg) was higher for AZILECT (2%) compared to placebo (1%).Dietary tyramine restriction is not required during treatment with recommended doses of AZILECT. However, certain foods that may contain very high amounts (i.e., more than 150 mg) of tyramine that could potentially cause severe hypertension because of tyramine interaction (including various clinical syndromes referred to as hypertensive urgency, crisis, or emergency) in patients taking AZILECT, even at the recommended doses, due to increased sensitivity to tyramine. Patients should be advised to avoid foods containing a very large amount of tyramine while taking recommended doses of AZILECT because of the potential for large increases in blood pressure including clinical syndromes referred to as hypertensive urgency, crisis, or emergency. AZILECT is a selective inhibitor of MAO-B at the recommended doses of 0.5 or 1 mg daily. Selectivity for inhibiting MAO-B diminishes in a dose-related manner as the dose is progressively increased above the recommended daily doses.5.2 Serotonin SyndromeSerotonin syndrome has been reported with concomitant use of an antidepressant (e.g., selective serotonin reuptake inhibitors-SSRIs, serotonin-norepinephrine reuptake inhibitors-SNRIs, tricyclic antidepressants, tetracyclic antidepressants, triazolopyridine antidepressants) and a nonselective MAOI (e.g., phenelzine, tranylcypromine) or selective MAO-B inhibitors, such as selegiline (Eldepryl) and rasagiline (AZILECT). Serotonin syndrome has also been reported withconcomitant use of AZILECT with meperidine, tramadol, methadone, or propoxyphene. AZILECT is contraindicated for use with meperidine, tramadol, methadone, propoxyphene and MAO inhibitors (MAOIs), including other selective MAO-B inhibitors [see Contraindications (4) and Drug Interactions (7.1, 7.2, 7.3)].In the postmarketing period, potentially life-threatening serotonin syndrome has been reported in patients treated with antidepressants concomitantly with AZILECT. Concomitant use of AZILECT with one of many classes of antidepressants (e.g., SSRIs, SNRIs, triazolopyridine, tricyclic or tetracyclic antidepressants) is not recommended [see Drug Interactions (7.5)].The symptoms of serotonin syndrome have included behavioral and cognitive/mental status changes (e.g., confusion, hypomania, hallucinations, agitation, delirium, headache, and coma), autonomic effects (e.g., syncope, shivering, sweating, high fever/hyperthermia, hypertension, tachycardia, nausea, diarrhea), and somatic effects (e.g., muscular rigidity, myoclonus, muscle twitching, hyperreflexia manifested by clonus, and tremor). Serotonin syndrome can result in death.AZILECT clinical trials did not allow concomitant use of fluoxetine or fluvoxamine with AZILECT, and the potential drug interaction between AZILECT and antidepressants has not been studied systematically. Although a small number of AZILECT-treated patients were concomitantly exposed to antidepressants (tricyclics n=115; SSRIs n=141), the exposure, both in dose and number of subjects, was not adequate to rule out the possibility of an untoward reaction from combining these agents. At least 14 days should elapse between discontinuation of AZILECT and initiation of treatment with a SSRI, SNRI, tricyclic, tetracyclic, or triazolopyridine antidepressant. Because of the long half-lives of certain antidepressants (e.g., fluoxetine and its active metabolite), at least five weeks (perhaps longer, especially if fluoxetine has been prescribed chronically and/or at higher doses) should elapse between discontinuation of fluoxetine and initiation of AZILECT [see Drug Interactions (7.5)].5.3 Falling Asleep During Activities of Daily Living and SomnolenceIt has been reported that falling asleep while engaged in activities of daily living always occurs in a setting of preexisting somnolence, although patients may not give such a history. For this reason, prescribers should monitor patients for drowsiness or sleepiness, because some of the events occur well after initiation of treatment with dopaminergic medication. Prescribers should also be aware that patients may not acknowledge drowsiness or sleepiness until directly questioned about drowsiness or sleepiness during specific activities.Cases of patients treated with AZILECT and other dopaminergic medications have reported falling asleep while engaged in activities of daily living including the operation of motor vehicles, which sometimes resulted in accidents. Although many of these patients reported somnolence while on AZILECT with other dopaminergic medications, some perceived that they had no warning signs, such as excessive drowsiness, and believed that they were alert immediately prior to the event. Some of these events have been reported more than 1-year after initiation of treatment.In Study 3, somnolence was a common occurrence in patients receiving AZILECT and was more frequent in patients with Parkinson’s disease receiving AZILECT than in respective patients receiving placebo (6% AZILECT compared to 4% Placebo) [see Adverse Reactions (6.1].Before initiating treatment with AZILECT, patients should be advised of the potential to develop drowsiness and specifically asked about factors that may increase the risk with AZILECT such as concomitant sedating medications, the presence of sleep disorders, and concomitant medications that increase rasagiline plasma levels (e.g., ciprofloxacin) [see Drug Interactions (7.6)]. If a patient develops significant daytime sleepiness or episodes of falling asleep during activities that require active participation (e.g., driving a motor vehicle, conversations, eating), AZILECT should ordinarily be discontinued. If a decision is made to continue these patients on AZILECT, advise them to avoid driving and other potentially dangerous activities. There is insufficient information to establish that dose reduction will eliminate episodes of falling asleep while engaged in activities of daily living.5.4 Ciprofloxacin or Other CYP1A2 InhibitorsRasagiline plasma concentrations may increase up to 2 fold in patients using concomitant ciprofloxacin and other CYP1A2 inhibitors. Patients taking concomitant ciprofloxacin or other CYP1A2 inhibitors should not exceed a dose of AZILECT 0.5 mg once daily [see Dosage and Administration (2.2), Drug Interactions (7.6), and Clinical Pharmacology (12.3)].5.5 Hepatic ImpairmentRasagiline plasma concentration may increase in patients with hepatic impairment. Patients with mild hepatic impairment should be given the dose of AZILECT 0.5 mg once daily. AZILECT should not be used in patients with moderate or severe hepatic impairment [see Dosage and Administration (2.3) and Clinical Pharmacology (12.3)].5.6 Hypotension / Orthostatic HypotensionIn Study 3, the incidence of orthostatic hypotension consisting of a systolic blood pressure decrease (> 30 mm Hg) or a diastolic blood pressure decrease (> 20 mm Hg) after standing was 13% with AZILECT (1 mg/day) compared to 9% with placebo [see Adverse Reactions (6.1)].At the 1 mg dose, the frequency of orthostatic hypotension (at any time during the study) was approximately 44% for AZILECT vs 33% for placebo for mild to moderate systolic blood pressure decrements (> 20 mm Hg), 40% for AZILECT vs 33% for placebo for mild to moderate diastolic blood pressure decrements (> 10 mm Hg), 7% for AZILECT vs 3% for placebo for severe systolic blood pressure decrements (> 40 mm Hg), and 9% for AZILECT vs 6% for placebo for severe diastolic blood pressure decrements (≥20 mm Hg). There was also an increased risk for some of these abnormalities at the lower 0.5 mg daily dose and for an individual patient having mild to moderate or severe orthostatic hypotension for both systolic and diastolic blood pressure.In Study 2 where AZILECT was given as an adjunct therapy in patients not taking concomitant levodopa, there were 5 reports of orthostatic hypotension in patients taking AZILECT 1 mg (3.1%) and 1 report in patients taking placebo (0.6%) [see Adverse Reactions(6.1].Clinical trial data further suggest that orthostatic hypotension occurs most frequently in the first two months of AZILECT treatment and tends to decrease over time.Some patients treated with AZILECT experienced a mildly increased risk for significant decreases in blood pressure unrelated to standing but while supine.The risk for post-treatment hypotension (e.g., systolic < 90 or diastolic < 50 mm Hg) combined with a significant decrease from baseline (e.g., systolic > 30 or diastolic > 20 mm Hg) was higher for AZILECT 1 mg (3.2%) compared to placebo (1.3%).There was no clear increased risk for lowering of blood pressure or postural hypotension associated with AZILECT 1 mg/day as monotherapy.When used as an adjunct to levodopa, postural hypotension was also reported as an adverse reaction in approximately 6% of patients treated with AZILECT 0.5 mg, 9% of patients treated with AZILECT 1 mg and 3% of patients treated with placebo. Postural hypotension led to drug discontinuation and premature withdrawal from clinical trials in one (0.7%) patient treated with AZILECT 1 mg/day, no patients treated with AZILECT 0.5 mg/day and no placebo-treated patients.5.7 DyskinesiaWhen used as an adjunct to levodopa, AZILECT may cause dyskinesia or potentiate dopaminergic side effects and exacerbate pre-existing dyskinesia. In Study 3, the incidence of dyskinesia was 18% for patients treated with 0.5 mg or 1 mg AZILECT as an adjunct to levodopa and 10% for patients treated with placebo as an adjunct to levodopa. Decreasing the dose of levodopa may mitigate this side effect [see Adverse Reactions (6.1].5.8 Hallucinations / Psychotic-Like BehaviorIn the monotherapy study (Study 1), the incidence of hallucinations reported as an adverse event was 1.3% in patients treated with AZILECT 1 mg and 0.7% in patients treated with placebo. In Study 1, the incidence of hallucinations reported as an adverse reaction and leading to drug discontinuation and premature withdrawal was 1.3% in patients treated with AZILECT 1 mg and 0% in placebo-treated patients.When studied as an adjunct therapy without levodopa (Study 2), hallucinations were reported as an adverse reaction in 1.2% of patients treated with 1 mg/day AZILECT and 1.8% of patients treated with placebo. Hallucinations led to drug discontinuation and premature withdrawal from the clinical trial in 0.6% of patients treated with AZILECT 1 mg/day and in none of the placebo-treated patients.When studied as an adjunct to levodopa (Study 3), the incidence of hallucinations was approximately 5% in patients treated with AZILECT 0.5 mg/day, 4% in patients treated with AZILECT 1 mg/day, and 3% in patients treated with placebo. The incidence of hallucinations leading to drug discontinuation and premature withdrawal was about 1% in patients treated with 0.5 mg AZILECT and 1 mg AZILECT/day, and 0% in placebo-treated patients [see Adverse Reactions (6.1)].Postmarketing reports indicate that patients may experience new or worsening mental status and behavioral changes, which may be severe, including psychotic-like behavior during treatment with AZILECT or after starting or increasing the dose of AZILECT. Other drugs prescribed to improve the symptoms of Parkinson’s disease can have similar effects on thinking and behavior. This abnormal thinking and behavior can consist of one or more of a variety of manifestations including paranoid ideation, delusions, hallucinations, confusion, psychotic-like behavior, disorientation, aggressive behavior, agitation, and delirium.Patients should be informed of the possibility of developing hallucinations and instructed to report them to their health care provider promptly should they develop.Patients with a major psychotic disorder should ordinarily not be treated with AZILECT because of the risk of exacerbating the psychosis with an increase in central dopaminergic tone. In addition, many treatments for psychosis that decrease central dopaminergic tone may decrease the effectiveness of AZILECT [see Drug Interactions (7.8)].Consider dose reduction or stopping the medication if a patient develops hallucinations or psychotic like behaviors while taking AZILECT.5.9 Impulse Control / Compulsive BehaviorsCase reports suggest that patients can experience intense urges to gamble, increased sexual urges, intense urges to spend money, binge eating, and/or other intense urges, and the inability to control these urges while taking one or more of the medications, including AZILECT, that increase central dopaminergic tone and that are generally used for the treatment of Parkinson’s disease. In some cases, although not all, these urges were reported to have stopped when the dose was reduced or the medication was discontinued. Because patients may not recognize these behaviors as abnormal, it is important for prescribers to specifically ask patients or their caregivers about the development of new or increased gambling urges, sexual urges, uncontrolled spending or other urges while being treated with AZILECT. Consider dose reduction or stopping the medication if a patient develops such urges while taking AZILECT.5.10 Withdrawal-Emergent Hyperpyrexia and ConfusionA symptom complex resembling neuroleptic malignant syndrome (characterized by elevated temperature, muscular rigidity, altered consciousness, and autonomic instability), with no other obvious etiology, has been reported in association with rapid dose reduction, withdrawal of, or changes in drugs that increase central dopaminergic tone.5.11 MelanomaEpidemiological studies have shown that patients with Parkinson’s disease have a higher risk (2to approximately 6-fold higher) of developing melanoma than the general population. Whether the increased risk observed was due to Parkinson’s disease or other factors, such as drugs used to treat Parkinson’s disease, is unclear.For the reasons stated above, patients and providers are advised to monitor for melanomas frequently and on a regular basis. Ideally, periodic skin examinations should be performed by appropriately qualified individuals (e.g., dermatologists).6. ADVERSE REACTIONSThe following adverse reactions are described in more detail in the Warnings and Precautions section of the label:•Hypertension [see Warnings and Precautions (5.1)]•Serotonin Syndrome [see Warnings and Precautions (5.2)]• Falling Asleep During Activities of Daily Living and Somnolence [see Warnings and Precautions (5.3)]• Hypotension / Orthostatic Hypotension [see Warnings and Precautions (5.6)]• Dyskinesia [see Warnings and Precautions (5.7)]• Hallucinations / Psychotic-Like Behavior [see Warnings and Precautions (5.8)]• Impulse Control /Compulsive Behaviors [see Warnings and Precautions (5.9)]• Withdrawal-Emergent Hyperpyrexia and Confusion [see Warnings and Precautions(5.10)]• Melanoma [see Warnings and Precautions (5.11)]6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to the incidence of adverse reactions in the clinical trials of another drug and may not reflect the rates of adverse reactions observed in practice.During the clinical development of AZILECT, Parkinson’s disease patients received AZILECT as initial monotherapy (Study 1) and as adjunct therapy (Study 2, Study 3, Study 4). As the populations in these studies differ, not only in the adjunct use of dopamine agonists or levodopa during AZILECT treatment, but also in the severity and duration of their disease, the adverse reactions are presented separately for each study.Monotherapy Use of AZILECTIn Study 1, approximately 5% of the 149 patients treated with AZILECT discontinued treatment due to adverse reactions compared to 2% of the 151 patients who received placebo.The only adverse reaction that led to the discontinuation of more than one patient was hallucinations.The most commonly observed adverse reactions in Study 1 (incidence in AZILECT-treated patients 3% or greater than the incidence in placebo-treated patients) included flu syndrome, arthralgia, depression, and dyspepsia. Table 1 lists adverse reactions that occurred in 2% or greater of patients receiving AZILECT as monotherapy and were numerically more frequent than in the placebo group in Study 1.Table 1: Adverse Reactions* in Study 1AZILECT 1 mg (N=149) Placebo (N=151)% of Patients % of Patients Headache 14 12Arthralgia 7 4Dyspepsia 7 4 Depression 5 2AZILECT 1 mg (N=149) Placebo (N=151)% of Patients % of PatientsFall 5 3Flu syndrome 5 1 Conjunctivitis 3 1Fever 3 1 Gastroenteritis 3 1Rhinitis 3 1Arthritis 2 1 Ecchymosis 2 0Malaise 2 0Neck Pain 2 0 Paresthesia 2 1Vertigo 2 1*Incidence 2% or greater in AZILECT 1 mg group and numerically more frequent than in placebo group There were no significant differences in the safety profile based on age or gender.Adjunct Use of AZILECTAZILECT was studied as an adjunct therapy without levodopa (Study 2), or as an adjunct therapy to levodopa, with some patients also taking dopamine agonists, COMT inhibitors, anticholinergics, or amantadine (Study 3 and Study 4).In Study 2, approximately 8% of the 162 patients treated with AZILECT discontinued treatment due to adverse reactions compared to 4% of the 164 patients who received placebo.Adverse reactions that led to the discontinuation of more than one patient were nausea and dizziness.The most commonly observed adverse reactions in Study 2 (incidence in AZILECT-treated patients 3% or greater than incidence in placebo-treated patients) included peripheral edema, fall, arthralgia, cough, and insomnia. Table 2 lists adverse reactions that occurred in 2% or greater in patients receiving AZILECT as adjunct therapy without levodopa and numerically more frequent than in the placebo group in Study 2.Table 2: Adverse Reactions* in Study 2AZILECT 1 mg (N=162) Placebo (N=164)% of Patients % of Patients Dizziness 7 6 Peripheral edema 7 4 Headache 6 4Nausea 6 4Fall 6 1Arthralgia 5 2Back pain 4 3Cough 4 1Insomnia 4 1Upper respiratory tractinfection 4 2Orthostatic hypotension 3 1*Incidence 2% or greater in AZILECT 1 mg group and numerically more frequent than in placebo group There were no significant differences in the safety profile based on age or gender.In Study 3, adverse event reporting was considered more reliable than Study 4; therefore, only the adverse event data from Study 3 are presented below.In Study 3, approximately 9% of the 164 patients treated with AZILECT 0.5 mg/day and 7% of the 149 patients treated with AZILECT 1 mg/day discontinued treatment due to adverse reactions, compared to 6% of the 159 patients who received placebo. The adverse reactions that led to discontinuation of more than one AZILECT-treated patient were diarrhea, weight loss, hallucination, and rash.The most commonly observed adverse reactions in Study 3 (incidence in AZILECT-treated patients 3% or greater than the incidence in placebo-treated patients) included dyskinesia, accidental injury, weight loss, postural hypotension, vomiting, anorexia, arthralgia, abdominal pain, nausea, constipation, dry mouth, rash, abnormal dreams, fall and tenosynovitis.Table 3 lists adverse reactions that occurred in 2% or greater of patients treated with AZILECT 1 mg/day and that were numerically more frequent than the placebo group in Study 3.Table 3: Adverse Reactions* in Study 3AZILECT 1 mg (N=149) AZILECT 0.5 mg(N=164)Placebo(N=159)% of patients % of patients % of patients Dyskinesia 18 18 10 Accidental injury 12 8 5 Nausea 12 10 8 Headache 11 8 10Fall 11 12 8 Weight loss 9 2 3 Constipation 9 4 5 Postural hypotension 9 6 3 Arthralgia 8 6 4 Vomiting 7 4 1。
雷沙吉兰结构式
雷沙吉兰结构式
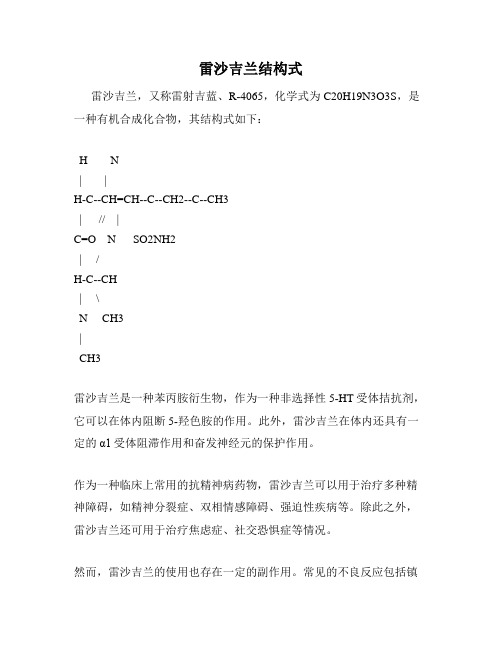
雷沙吉兰,又称雷射吉蓝、R-4065,化学式为C20H19N3O3S,是一种有机合成化合物,其结构式如下:
H N
| |
H-C--CH=CH--C--CH2--C--CH3
| // |
C=O N SO2NH2
| /
H-C--CH
| \
N CH3
|
CH3
雷沙吉兰是一种苯丙胺衍生物,作为一种非选择性5-HT受体拮抗剂,它可以在体内阻断5-羟色胺的作用。
此外,雷沙吉兰在体内还具有一定的α1受体阻滞作用和奋发神经元的保护作用。
作为一种临床上常用的抗精神病药物,雷沙吉兰可以用于治疗多种精神障碍,如精神分裂症、双相情感障碍、强迫性疾病等。
除此之外,雷沙吉兰还可用于治疗焦虑症、社交恐惧症等情况。
然而,雷沙吉兰的使用也存在一定的副作用。
常见的不良反应包括镇
静、口干、便秘、尿潴留等。
此外,长期使用雷沙吉兰还可能导致锥体外系症状、骨髓抑制等问题。
综上所述,雷沙吉兰虽然是一种常用的精神药物,但在使用过程中还需慎重。
必须根据个体情况选用适当剂量、时间和疗程,并在医生的指导下进行使用,以最大限度地避免不良反应的发生。
雷沙吉兰联合美多芭治疗帕金森病的临床疗效观察

【 关键词 】 帕金森病; 雷沙吉兰; 美 多芭
【 中图分类号 】 R 7 2 2 . 1 2
1 、 材 料 与 方 法 1 . 1l 临床资料
【 文献标识码】 B
【 文章编号 】 1 0 0 4— 4 9 4 9 ( 2 0 1 5 ) 0 4— 0 3 3 1— 0 1
2 . 2 .添加雷 沙吉兰治疗前后 美多芭用量 比较 单用 美多芭时, 2 8 例 患者中最小剂量 为 2 5 0 a r g , 最 大剂量为 1 2 5 0 m g , 单用美 多芭 时 平均剂量为 6 2 6 . 2 7± 2 1 5 . 3 8 a r g , 与雷沙吉兰联合应用后 , 2 8例患者 中有 l O例美 多芭 用 量减少 , 总量为 6 0 2 . 1 1 m g , 平均为 5 9 7 . 2 5± 1 5 2 . 2 6 a r g , 添加治疗前后平均 减少 的剂量 为 2 9 . 0 2±8 . 5 0 a r g ( 见 表 2) 。 表2 添加前后复方左旋多 巴用量 ( 均数 ± 标准差 , P< O . 0 5 )
添加雷沙吉兰治疗前后的updrswebster评分比较与治疗前相比从加用雷沙吉兰治疗6周后的updrs评分可以看出添加雷沙吉兰治疗后患者无论从主观感觉还是我们的客观评价上运动功能各部分评分均较前明显降低治疗前updrs评分为5083452治疗后评分为2961337差异有统计学意义p005
u 1J 平
雷 沙 吉 兰 联 合 美 多芭 治 疗 帕 金 森 病 的 临 床 疗 效 观 察
张 楠 楠 侯 丽 淳 通 讯 作者
( 佳木斯 大学
1 5 4 0 0 2 ; 。 佳木斯 大学第一 附属 医院
1 5 4 0 0 2 )
雷沙吉兰结构式

雷沙吉兰结构式雷沙吉兰结构式是一种独特的建筑风格,它融合了雷沙吉兰文化的精髓和现代建筑的理念,以其独特的外观和独特的设计理念而闻名。
雷沙吉兰结构式的建筑物常常具有雄伟的外观和独特的造型,给人一种震撼和奇异的感觉。
本文将介绍雷沙吉兰结构式的特点、设计理念以及其在现代建筑中的应用。
一、雷沙吉兰结构式的特点雷沙吉兰结构式以其独特的外观和独特的设计理念而闻名。
其外观常常呈现出曲线和流线型的造型,给人一种动感和流动感。
另外,雷沙吉兰结构式的建筑物常常采用大量的玻璃幕墙,使建筑物与周围环境融为一体,增加了建筑的透明感和现代感。
二、雷沙吉兰结构式的设计理念雷沙吉兰结构式的设计理念注重将建筑与自然环境融合,强调人与自然的和谐共生。
在设计过程中,设计师会充分考虑建筑物的功能和使用需求,同时注重建筑与周围环境的协调。
此外,雷沙吉兰结构式还注重运用现代科技和材料,使建筑物更加耐久和环保。
三、雷沙吉兰结构式在现代建筑中的应用雷沙吉兰结构式在现代建筑中得到了广泛的应用。
在城市中,我们可以看到许多雷沙吉兰结构式的高楼大厦,它们以其独特的外观和现代感而成为城市的地标。
此外,雷沙吉兰结构式的建筑物也被广泛应用于商业和办公场所,其独特的设计理念和外观给人一种舒适和奇异的感觉,为人们提供了一个愉快的工作和生活环境。
四、雷沙吉兰结构式的未来发展随着人们对建筑环境的要求不断提高,雷沙吉兰结构式在未来将有更广阔的发展空间。
人们对建筑外观和设计的要求越来越高,雷沙吉兰结构式的独特外观和设计理念正符合人们的需求。
此外,随着科技的不断发展,雷沙吉兰结构式也将运用更多的先进科技和材料,使建筑更加耐久、环保和智能化。
总结起来,雷沙吉兰结构式作为一种独特的建筑风格,以其独特的外观和独特的设计理念而闻名。
它将人与自然的和谐共生融入到建筑设计中,注重建筑与周围环境的协调,并运用现代科技和材料,使建筑更加耐久和环保。
在现代建筑中,雷沙吉兰结构式得到了广泛的应用,其独特的外观和现代感为城市增添了一道亮丽的风景线。
抗帕金森病新药雷沙吉兰有效治疗早期帕金森病

抗帕金森病新药雷沙吉兰有效治疗早期帕金森病
佚名
【期刊名称】《世界临床药物》
【年(卷),期】2003(24)3
【总页数】1页(P130-130)
【关键词】帕金森病;雷沙吉兰;药物治疗;疗效
【正文语种】中文
【中图分类】R971.5;R742.5
【相关文献】
1.司来吉兰与雷沙吉兰治疗帕金森病的疗效对比研究 [J], 宋艳萍
2.帕金森病治疗新药——雷沙吉兰 [J], 孙铜;郝丽娜
3.抗帕金森病新药雷莎吉兰的合成 [J], 杨鹏;宋丹青
4.司来吉兰与雷沙吉兰治疗帕金森病的有效性和安全性对比 [J], 曲艳; 李晓红
5.治疗帕金森病新药雷沙吉兰(rasagiline) [J],
因版权原因,仅展示原文概要,查看原文内容请购买。
雷沙吉兰和司来吉兰

雷沙吉兰和司来吉兰单胺氧化酶抑制剂雷沙吉兰和司来吉兰是一类药,理论上单吃可以保护神经,延缓病情发展,配合左旋多巴类药物可以延长左旋多巴的时间和效果。
在所有的抗帕金森药中,有研究资料表明的可以延缓病情发展的只有雷沙吉兰和司来吉兰。
两种药是一类药,都属于单胺氧化酶抑制剂。
国际专业的资料显示一次1毫克的雷沙吉兰可以延缓病情的发展,但2毫克的雷沙吉兰好像不能延缓病情发展。
这个结论令很多患者和专业医生很茫然。
不知道雷沙吉兰到底该不该用。
芬兰的咪多比就是一片5毫克的司来吉兰,咪多比的说明书有这么一句话,如果你正在用司来吉兰,没有感受到它的效果,不代表它没有效果。
雷沙吉兰国内目前没有,常州四药的雷沙吉兰明年估计会临床上市,国外的雷沙吉兰价格差异很大从人民币几元----60元价格不等,帕友可以选择的空间很大。
当然也增加了选择的难度。
令帕友选择更盲目。
现在北京的有一种假中药就叫雷沙吉兰,就是借了大部分人热衷与雷沙吉兰的名头的原因。
理论上雷沙吉兰和司来吉兰都可以单吃,单吃有效。
但一部分帕友费尽千方百计从国外弄回来的一粒10美元雷沙吉兰吃了觉得没有效果。
这种人不少,当然有效的也大有人在。
不是他买的药是假的,就是因为延缓病情是一个很漫长的过程,不是一天两天、一月两月、甚至一年两年能看到的。
就像咪多比的说明书上说的那句话,如果你正在用咪多比,没有感受到效果,不代表它没有效果。
曾经有一位帕友服用司来吉兰好多年,坚持配合美多巴,有一天,他姑娘和我交流时说,觉得他爸相比别的熟悉的帕友发展的慢,她很满意,有比较才能说明问题。
我父亲用司来吉兰也好久了,也是一直配合美多巴或西来美用,他老觉得司来吉兰不如受体激动剂配合美多巴或西来美效果好。
所以在司来吉兰应用问题上不是很规范。
我仅仅是告诉他药品的适应症,副作用、配合原则,一般都是他自己摸索调整。
觉得有必要再咨询我。
司来吉兰在治疗帕金森以前是抗忧郁药,8成帕金森患者伴有不同程度忧郁,有的是由于刚患病心里引起的心理原因,有的是因为患者症状改善的不好而引起的忧郁。
甲磺酸雷沙吉兰标准[1]
![甲磺酸雷沙吉兰标准[1]](https://img.taocdn.com/s3/m/2e829f119e314332386893de.png)
甲磺酸雷沙吉兰标准[1]甲磺酸雷沙吉兰原料药质量标准Jiahuangsuan leishajilanRasagiline mesylate.CHNCHOS=267.34 121343本品为(R)-N-2-丙炔基-1-氢化茚胺甲磺酸盐,按干燥品计算,含.CHNCHOS应为98.5%,102.0%。
121343【性状】本品为白色或类白色结晶性粉末;本品在水中极易溶解,在甲醇中易溶。
0【熔点】本品的熔点(中国药典2005年版二部附录VI)为153.0,158.0C.【比旋度】取本品,精密称定,加水制成每1ml中约含10mg的溶液,依法(中国药典2005版二部附录? E)测定,旋光度为,20?至,25?。
【鉴别】(1)在含量测定项下记录的色谱图中,供试品主峰的保留时间应与甲磺酸雷沙吉兰对照品主峰的保留时间一致。
(2)本品的红外光吸收图谱应与甲磺酸雷沙吉兰对照品的图谱一致(中国药典2005版二部附录IV C)。
【检查】硫酸盐取本品0.5g,依法检查(中国药典2005版二部附录? B),与标准硫酸钾溶液2.5ml制成的对照溶液比较,不得更浓(0.05%)。
有关物质取本品适量,精密称定,加流动相制成每1ml中含雷沙吉兰1mg的溶液做供试品溶液;精密量取供试品溶液1ml到100ml的量瓶中,加流动相稀释至刻度,摇匀,作为对照溶液。
照含量测定项下的色谱条件进行试验,取对照溶液10 μl注入液相色谱仪,调节检测灵敏度使主峰峰高约为满量程的20%;再精密量取供试品溶液10μl,注入液相色谱仪,记录色谱图至主成分峰保留时间的3倍。
供试溶液的色谱图中各杂质峰面积总和不得大于对照溶液主成分的峰面积(1.0%)。
炽灼残渣取本品1.0g,依法检查(中国药典2005年版二部附录? N),遗留残渣不得过0.2%。
0干燥失重取本品,在105C干燥至恒重,减失重量不得过1.0%(中国药典2005版二部附录? L).重金属取炽灼残渣项下遗留的残渣,依法检查(中国药典2005版二部附录? H 第二法),含重金属不得过百万分之二十。
雷沙吉兰合成研究进展

英 国 上 市 ,0 6年 , D 20 F A批 准 雷 沙 吉 兰 在 美 国上 市 ,商 品名
为 A i c, 于初 始 单 药 治疗 早 期 帕 金 森 病 ( D) 且 可 作 为 zl t用 e P ,
较 晚 期患 者治 疗 药物 左 旋多 巴 的补 充用 药 。与第 1 MA — 代 O
21 0 2年 7月第 9卷第 1 9期
。 综
・
述 ・ 。
雷沙吉兰合成研究进展
郑 欣 钟 日 英 蔡 彦
广 东省 湛 江市 霞 山妇 幼 保 健 院 , 广东 湛 江
5 4 1 2 03
【 要】 摘 雷沙 吉 兰 ( aa l e 为不 可 逆 选择 性 单 胺 氧 化 酶一 ( 0 B 抑 制 剂 , R S矛 i ) n B MA 一 ) 可增 强 多 巴胺 的传 递 信 号 , 效 缓解 有 帕金 森症 的诸 如 静 止性 震 颤 、 肉僵 直 等症 状 。本 文 通 过系 统地 查 阅 国 内外 近年 来雷 沙 吉 兰合 成 的相关 文献 , 肌 旨在 为科研 工 作者 全 面 而系 统地 了解 雷沙 吉 兰 的合成 路 线 、 进一 步深 入 研究 提 供参 考 。 【 键词】 沙吉 兰 ; 关 雷 帕金 森症 ; 成 研 究 合 【 中图分 类 号】 9 1 R 7. 5 【 献 标识 码】 文 A 【 章编 号】 6 3 7 1 (0 2 0 ( ) 0 1— 3 文 17 - 2 0 2 1 )7 a 一 0 3 0
miso fd p mi e whc a tg t h y tm fP r i sn' d s a e s c ssai rmo n t fn mu ce n sin o o a n ih c n mi ae te smpo o ak n o s ie s u h a ttc te ra d si e sl .I i f ti a e,rs ac i r tr so a a i n y t e i a o n bo d ae c l td Isp ro e i t k c e t c r- h sp p r ee r hlt au e n r s gl es nh ss th mea d a r a r ol e . t up s s o ma es ini e e i a i f s ac r eu s se yu d rtn ig sn h ssru eo a a iiea d p o ie terfr n efri ut e e e rh e rh wok 1 y tml n e sa dn y t ei o t frs gl n rvd h eee c o t frh rr s ac . . n s t ss o s g lne s a c r g e s o yn he i f Ra a ii
帕金森病治疗新药——雷沙吉兰

合 用 。单 次 静 脉 注 射 剂 量 后 本 品 的 平 均 分 布 体 积 为 2 3 4 L, 血 浆 蛋 白 结合 率 约 为 6 ~7 。本 品 在 排 泄 前 几 乎 完 全 O O 在肝 中 发 生生 物 转 化 , 谢 途 径 主 要 为 N一 脱 烷 基 化 和/ 代 或 羟基 化 产 生 1 a n idn 3 一 mi n a , ~羟 基 一N一 炔丙 基 一 1 mi o 一a —
形作 用和长期增效作用 。
动 物 实 验 结 果 也 表 明 , 1 h内 , 大脑 中 动 脉 阻 塞 的 在 6 给
模型大 鼠腹腔 重复 注射 一2 B抑 制作用 无关 用 药 4 h内, 8
大 鼠的 神 经 损 害 严 重 性 评 分 得 到 改 善 , 脑坏 死 体 积 也 有 所 大
【 中文 名】 甲磺 酸 雷 沙吉 兰
【 构式】 结
减少 。若在阻塞后 3 mi ̄3 0 n h内给药 , 则大 鼠神经损害严重
性 评 分 的 改 善 更 为 显 著 。持 续 用 药 3 , 死 面 积 可 减 少 为 h 梗
对 照 组 的 4 。 9
【 代动力学】 药 本 品 吸 收 迅 速 ,. h后 达 血 浆 峰 值 (ma )单 次 剂 量 后 05 p x,
单 胺 氧 化 酶 B MA(一 B 抑 制 剂 。 该 药 于 2 0 ( ) ) 0 5年 1月 第 1 次 获 准在 以 色 列 上 市 , 后 于 2 0 随 0 5年 2月 获 欧 盟 批 准 ,0 5 2 0
年 6月 首 次 在 欧盟 国 家 英 国 上 市 , 已 获 得 F A 的 可 批 准 并 D 函。 此 外 , 药 目前 还 在 进 行 用 于 治 疗 老 年 痴 呆 ( 该 AD) 抑 郁 、 症 、 童多动症的临床研究。 儿
甲磺酸雷沙吉兰联合多巴丝肼治疗帕金森病的临床效果
甲磺酸雷沙吉兰联合多巴丝肼治疗帕金森病的临床效果【摘要】目的:评价对帕金森患者进行甲磺酸雷沙吉兰联合多巴丝肼治疗的应用效果。
方法:选取我院帕金森患者50例,分为两组,对照组进行多巴丝肼治疗,观察组进行甲磺酸雷沙吉兰联合多巴丝肼治疗,对比组间患者的生活质量和治疗效果。
结果:观察组患者的生活质量和治疗效果均显著优于对照组(P<0.05)。
结论:通过对帕金森患者进行甲磺酸雷沙吉兰联合多巴丝肼治疗能够有效改善患者的生活质量和治疗效果。
【关键词】帕金森;甲磺酸雷沙吉兰联合多巴丝肼;生活质量;临床效果帕金森病是一种神经系统疾病,常见于老年人。
它的主要症状包括手脚震颤、肢体僵硬、运动迟缓、姿势不稳、面部表情减少等。
这些症状是由于脑中的多巴胺神经元减少导致的。
目前还没有治愈帕金森病的方法,但是可以通过药物和手术治疗来缓解症状。
药物治疗主要是补充多巴胺,手术治疗则是通过刺激脑部的深部结构来减轻症状。
除了药物和手术治疗之外,锻炼、物理治疗和语言治疗等综合康复治疗方法也可以帮助患者更好地管理病情。
对于帕金森病患者,家庭支持和心理治疗也是很重要的。
甲磺酸雷沙吉兰是一种抗癫痫药物,常用于控制类似部分性癫痫、全面性癫痫、癫痫状态等类型的癫痫。
它的主要作用机制是通过提高大脑中促进兴奋性神经递质谷氨酸的释放,从而减少神经元的兴奋性,防止癫痫的发作。
甲磺酸雷沙吉兰的用药剂量逐渐增加到最有效剂量后,一般需要维持药量一段时间。
它的起效时间相对比较快,一般在使用后1-2小时内就可发挥药效。
甲磺酸雷沙吉兰的不良反应较少,常见的轻微反应包括头痛、头晕、嗜睡、恶心等,一般不需要特殊处理,如果出现严重反应需要尽快就医处理。
多巴丝肼是一种β1-肾上腺能激动剂,常用于治疗心衰和心脏功能不足等心脏疾病,其主要通过促进心脏收缩力的增强和心肌耗氧量的减少,从而增强心脏功能,改善心血管系统循环。
本文通过对帕金森患者进行甲磺酸雷沙基兰联合多巴丝肼治疗,旨在探究其对患者临床效果的效果,现报道如下。
雷沙吉兰对帕金森病人清晨关期运动障碍及非运动症状的临床疗效观察

雷沙吉兰对帕金森病人清晨关期运动障碍及非运动症状的临床疗效观察发表时间:2019-11-01T15:01:51.383Z 来源:《医药前沿》2019年26期作者:吴兴军陈韦洁高欢叶民刘新亚(通讯作者)[导读] 帕金森患者接受雷沙吉兰药物治疗效果更佳,可改善患者清晨关期运动障碍,降低非运动症状评分,安全性高,值得临床应用。
(南京医科大学附属南京明基医院神经内科江苏南京 210019)【摘要】目的:分析帕金森患者接受雷沙吉兰药物治疗对清晨关期运动障碍及非运动症状的效果。
方法:此次选择2018年1月—12月我院收治帕金森患者40例为研究对象,参照计算机抽选结果分为观察组与对照组,对照组患者单纯以左旋多巴治疗,观察组患者在对照组基础上加用雷沙吉兰治疗,比较两组治疗效果。
结果:用药4周、8周后观察组清晨关期运动障碍评分(7.04±0.21)、(6.09±0.14),非运动症状评分(5.13±0.13)、(4.01±0.11)均低于对照组,差异显著(P<0.05)。
结论:帕金森患者接受雷沙吉兰药物治疗效果更佳,可改善患者清晨关期运动障碍,降低非运动症状评分,安全性高,值得临床应用。
【关键词】雷沙吉兰;帕金森病;清晨关期运动障碍;非运动症状【中图分类号】R453 【文献标识码】A 【文章编号】2095-1752(2019)26-0125-02 帕金森病(Parkinson’s disease)属于临床较为常见的一类神经系统退行性病症,主要以药物治疗为主,常用药物如左旋多巴、多巴胺受体激动剂、抗胆碱能药物、单胺氧化酶B抑制剂等,根据患者的病情发展及症状表现调整用量及用法。
左旋多巴是治疗帕金森疾病的基础用药,然而患者如长时间服用,很容易出现一定程度运动并发症,例如“开关现象”[1-2],那么,就需辅以其他药物提高治疗效果。
本文以2018年1月—12月我院收治40例帕金森患者为例,分析雷沙吉兰的应用价值,具体如下。
甲磺酸雷沙吉兰片说明书
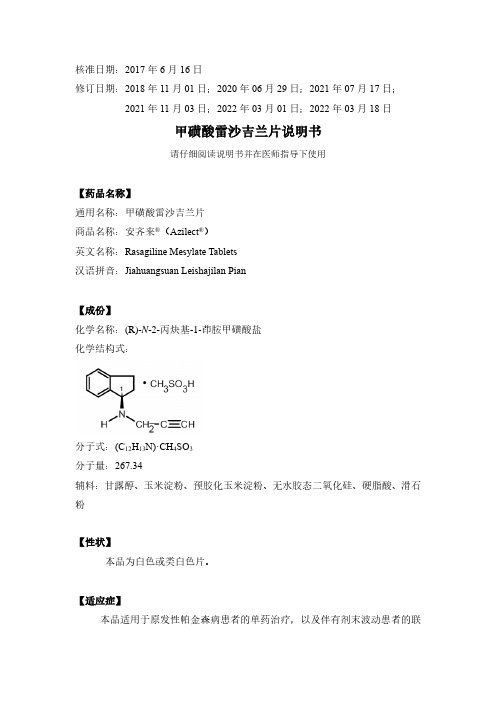
核准日期:2017年6月16日修订日期:2018年11月01日;2020年06月29日;2021年07月17日;2021年11月03日;2022年03月01日;2022年03月18日甲磺酸雷沙吉兰片说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:甲磺酸雷沙吉兰片商品名称:安齐来®(Azilect®)英文名称:Rasagiline Mesylate Tablets汉语拼音:Jiahuangsuan Leishajilan Pian【成份】化学名称:(R)-N-2-丙炔基-1-茚胺甲磺酸盐化学结构式:分子式:(C12H13N)·CH4SO3分子量:267.34辅料:甘露醇、玉米淀粉、预胶化玉米淀粉、无水胶态二氧化硅、硬脂酸、滑石粉【性状】本品为白色或类白色片。
【适应症】本品适用于原发性帕金森病患者的单药治疗,以及伴有剂末波动患者的联合治疗(与左旋多巴合用)。
【规格】1mg(以雷沙吉兰计)【用法用量】口服给药。
无论是否与左旋多巴合用,用量均为1mg每日一次。
服用本品不受进食影响。
老年人:无需调整剂量。
儿童:由于本品用于儿童和青少年的安全性和有效性尚未建立,本品不推荐用于儿童和青少年。
肝功能损害患者:本品禁用于重度肝功能损害患者(参见【禁忌】)。
雷沙吉兰应避免用于中度肝功能损害患者。
轻度肝功能损害患者开始服用本品时应谨慎。
如果患者的肝功能损害由轻度进展为中度时,应停止服用雷沙吉兰(参见【注意事项】)。
肾功能损害患者:无需调整剂量。
【不良反应】安全性特征概述在帕金森病患者的临床研究中,最常报告的不良反应为:单药治疗中出现的头痛、抑郁、眩晕和流感(流行性感冒和鼻炎);左旋多巴联合治疗中出现的异动症、直立性低血压、跌倒、腹痛、恶心呕吐和口干;两种疗法中出现的肌肉骨骼疼痛、背部和颈部疼痛以及关节痛。
这些不良反应与药物停药率升高无关。
不良反应列表不良反应采用如下惯例按照系统器官和发生频率分类,如下表1和2中所示:很常见(≥1/10)、常见(≥1/100,<1/10)、少见(≥1/1000,<1/100),罕见(≥1/10000,<1/1000)、极罕见(<1/10000),未知(无法根据现有数据估算)。
甲磺酸雷沙吉兰片人体药代动力学试验开题报告

甲磺酸雷沙吉兰片人体药代动力学试验开题报告1 研究背景帕金森病(Parkinson's disease)又称"震颤麻痹",巴金森氏症或柏金逊症,多在60岁以后发病。
主要表现为患者动作缓慢,手脚或身体其它部分的震颤,身体失去柔软性,变得僵硬。
帕金森病是老年人中第四位最常见的神经变性疾病,全世界在≥65岁人群中,1%患有此病;在>40岁人群中为0.4%.本病也可在儿童期或青春期发病。
中国帕金森病的发生率约占老年人口的1%,65岁以上的人群中的患病率为1.7%,高于世界水平。
估计在中国约有170万人患有此病,而且每年新发现的患者近10万人。
据统计,在香港55岁以上人口大约没1000人就有5名患者。
随着大众健康水平的提高和社会人口日益老龄化,预计帕金森病的患病率及致残率会呈现逐年增高的趋势。
目前帕金森病的发病机制还没有阐述清楚,关于帕金森病的发病机制的学说有兴奋性神经毒性学说,氧化应激或自由基学说,线粒体功能障碍学。
其中多巴胺(DA)学说是最受公认的学说。
多巴胺学说认为,帕金森病的病人与脑中多巴胺缺损有关,是基底——纹状体系统多巴胺含量不足所致,当多巴胺含量减少到原水平的10%-15%以下时即会出现临床症状。
多巴胺含量降低可能与黑质致密区黑色素细胞减少有关,在正常情况下,黑质纹状体释放的多巴胺和纹状体胆碱能神经元释放的乙酰胆碱维持相对平衡。
帕金森病人因为多巴胺量减少使乙酰胆碱相对过剩,平衡被打破,出现临床症状。
根据帕金森病的治病原理,帕金森病本质就是患者中脑内能够分泌多巴胺的神经元死亡,导致脑内多巴胺缺乏,使患者出现震颤、僵直和行动迟缓等一系列的症状。
药物治疗途径有补充外源性的多巴胺或多巴胺前体、促进多巴胺释放、激动多巴胺受体、抑制单胺氧化酶活性、减少多巴胺降解和拮抗功能等。
在所有的治疗药物中,左旋多巴被称为治疗帕金森病的“金标准”。
但长期大量应用左旋多巴,脑内多巴胺增加,多巴胺在单胺氧化酶-B氧化下能产生自由基而引起黑质细胞变性或坏死,加重症状。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
雷沙吉兰简介
雷沙吉兰(英文名rasagiline)是第二代单胺氧化酶抑制剂, 能阻滞神经递质多巴胺的分解,与司来吉兰(第一代单胺氧化酶抑制剂,包括思吉宁、咪哆吡、金思平等)相比抑制作用强5-10倍, 对长期应用多巴制剂药效出现衰退的患者也有改善的作用。
另外,雷沙吉兰的代谢产物是一种无活性的非苯丙胺物质,副作用小, 更重要的是,该药有一定的症状缓解的作用,并有较多证据证明这类药物有一定的神经保护的作用。
雷沙吉兰的临床疗效研究
2005年,《柳叶刀》杂志发表的一份国际联合研究报告,抗震颤麻痹药雷沙吉兰(rasag iline)能有效缓解帕金森病患者的运动失能症状。
在该项为期18周的临床研究中,687例来自以色列、阿根廷和欧洲的患者(此前均接受过左旋多巴治疗)被随机分组,分别给予雷沙吉兰、无效安慰剂或另一种抗震颤麻痹药恩他卡朋(entacapone)+左旋多巴。
结果表明雷沙吉兰和恩他卡朋都能明显减少运动功能的丧失期(每天分别为1.18和1.2小时)而延长功能期,而且其副作用类型和发生率也相似,包括改变体位时血压下降、晕厥、便秘、恶心以及腿、踝肿胀等。
考虑到雷沙吉兰每天仅需口服一次,专家们普遍认为它将更适于用作常规帕金森病治疗的辅助药物。
有3项为期18~26周的随机对照临床试验证实了雷沙吉兰的安全性和有效性。
一项研究纳入404例早期帕金森病患者,评定量表表明,与安慰剂组相比,接受雷沙吉兰治疗患者病情出现恶化的几率明显降低。
另两项研究在1100多例较晚期帕金森病患者中比较了雷沙吉兰联合安慰剂或左旋多巴的疗效,显示接受雷沙吉兰联合左旋多巴治疗患者,其每天的功能和活动度受限时间明显缩短。
加拿大《医学邮报》也报告,新的长期研究资料表明,采用雷沙吉兰(Rasagiline)治疗可使帕金森病的症状缓解长达6年之久。
此外,早期给予雷沙吉兰治疗的长期疗效要优于较晚给予的患者。
以色列Teva制药公司近期完成的一项名为ADAGIO的III期临床试验。
是为检验雷沙吉兰的疗效,进行的迄今为止对帕金森病药物的最大规模实验,参加实验的1176名早期患者在全球14个国家的129个医疗中心接受治疗,他们均处于帕金森病早期阶段。
研究表明,雷沙吉兰能延缓患者病情发展,在多个检测试验项目中的效果均达到显著性水平的提高。
雷沙吉兰的市场前景
2006年,FDA批准雷沙吉兰在美国上市,商品名为Azilect,用于初始单药治疗早期帕金森病,且可作为较晚期患者治疗药物左旋多巴的补充用药。
雷沙吉兰有0.5mg和1mg 两个规格,价格均在7-8美元之间,在帕金森病早期治疗策略中,它是无功能障碍和轻度功能障碍患者的首选药物。
目前,雷沙吉兰已在加拿大和欧洲多个国家上市,预计年销售额可达10亿美元以上。
雷沙吉兰尚未在中国上市,也还没有听到在中国的临床试验,百济新特药房药师认为,根据神经科其他重磅药物在国内的上市趋势,雷沙吉兰很可能要到2015年左右才会踏入中国市场,到时候,中国是否会有国产的雷沙吉兰上市也很难说。
不过百济新特药房的神经科药师和编辑,都会时刻关注像雷沙吉兰这类新特药物的动向,及时报道神经精神类疾病药物的研究进展和上市情况。