Characteristics of mucosa-associated gut microbiota during treatment in Crohn’s disease
肺黏膜相关淋巴组织淋巴瘤的CT表现
欢迎关注本刊公众号《肿瘤影像学》2021年第30卷第3期Oncoradiology 2021 Vol.30 No.3191·论 著·肺黏膜相关淋巴组织淋巴瘤的CT表现陈利军1,韩月东1,张 明21. 西安高新医院放射科,陕西 西安 710075;2. 西安交通大学附属第一医院医学影像科,陕西 西安 710061[摘要] 目的:分析肺黏膜相关淋巴组织(mucosa-associated lymphoid tissue ,MALT )淋巴瘤的CT 表现,提高对肺MALT 淋巴瘤的认识。
方法:分析经肺穿刺活组织病理学检查证实的12例肺MALT 淋巴瘤患者的临床和影像学资料,患者均接受胸部CT 平扫。
结果:12例患者CT 扫描均见肺实变,其中5例为单发,7例为多发。
12例患者中11例实变肺组织内见扩张支气管影及多发空泡影,9例伴肺内随机分布的多发结节及肿块影,2例伴多发空腔,1例伴胸膜下多发磨玻璃影。
结论:肺实变是肺MALT 淋巴瘤常见的CT 表现,以扩张的空气支气管并多发空泡影为特征,肺结节及肿块、空腔、磨玻璃影均是肺MALT 淋巴瘤特征之一。
[关键词] 黏膜相关淋巴组织;肺淋巴瘤;CT DOI: 10.19732/ki.2096-6210.2021.03.009中图分类号:R734.2;R445.3 文献标志码:A 文章编号:2096-6210(2021)03-0191-04CT findings of pulmonary mucosa-associated lymphoid tissue lymphoma CHEN Lijun 1, HAN Yuedong 1, ZHANG Ming 2 (1. Department of Radiology, GaoXin Hospital of Xi’an, Xi’an 710075, Shaanxi Province, China; 2. Department of Medical Imaging, The First Affiliated Hospital of Xi’an Jiao Tong University, Xi’an 710061, Shaanxi Province, China)Correspondence to: ZHANG Ming E-mail: zhangming01@[Abstract ]Objective: To investigate the CT manifestations of pulmonary mucosa-associated lymphoid tissue (MALT) lymphoma and improve the understanding of this disease. Methods: The clinical and imaging data of 12 cases of lung MALT lymphoma confirmed by transcutaneous lung biopsy and pathology were analyzed. All patients underwent plain CT scan of the chest. Results: A total of 12 cases of CT were manifested as pulmonary consolidation, of which 5 cases were solitary lesion and 7 cases were multiple lesion. The sign of dilated air bronchograms and multiple empty bubbles were seen in 11 of 12 cases with pulmonary consolidation lesions, randomly distributed multiple nodules and masses in 9 cases, multiple cavities in 2 cases, and under subpleural abrasion with multiple ground-glass opacity in 1 case. Conclusion: Pulmonary consolidation was a common CT manifestation of pulmonary MALT lymphoma. It is characterized by air bronchogram sign and multiple empty bubbles with bronchiectasis. Pulmonary nodules and masses, cavities, and ground glass opacity were also one of the features of the disease.[Key words ] Mucosa-associated lymphoid tissue; Pulmonary lymphoma; CT通信作者:张 明 E-mail: zhangming01@ 肺原发性非霍奇金淋巴瘤(p r i m a r y pulmonary non-Hodgkin lymphoma ,PPNHL )十分罕见,仅占全身淋巴瘤的0.4%,黏膜相关淋巴组织(mucosa-associated lymphoid tissue ,MALT )淋巴瘤是其最常见的亚型,占原发性肺淋巴瘤的70%~90%[1-2]。
边缘区淋巴瘤转化为大B细胞淋巴瘤1例并文献复习

第59卷 第2期2023年04月青岛大学学报(医学版)J O U R N A LO FQ I N G D A O U N I V E R S I T Y (M E D I C A LS C I E N C E S)V o l .59,N o .2A pr i l 2023[收稿日期]2022-05-17; [修订日期]2022-12-09[基金项目]青岛大学附属医院临床医学X+科研项目(3384)[第一作者]闫思琪(1994-),女,硕士研究生㊂[通信作者]冯献启(1971-),男,博士,主任医师,硕士生导师㊂E -m a i l :q d f x q2005@163.c o m ㊂赵春亭(1963-),男,博士,主任医师,博士生导师㊂E -m a i l :c t z h a o -006@m e d m a i l .c o m.c n㊂边缘区淋巴瘤转化为大B 细胞淋巴瘤1例并文献复习闫思琪1,李田兰2,刘珊珊2,毛春霞2,冯献启2,赵春亭2(青岛大学,山东青岛 266071 1 医学部; 2 附属医院血液内科)[摘要] 目的 探讨黏膜相关淋巴组织结外边缘区淋巴瘤转化为弥漫大B 细胞淋巴瘤病人的临床诊断和治疗㊂方法 回顾1例原发性淋巴瘤黏膜相关淋巴组织结外边缘区淋巴瘤治疗缓解后出现弥漫大B 细胞淋巴瘤转化病人的临床资料,分析其临床表现㊁治疗经过及预后,并复习相关文献㊂结果 病人确诊直肠黏膜相关淋巴组织结外边缘区淋巴瘤后,给予R -C HO P 方案(利妥昔单抗+环磷酰胺+多柔比星+长春新碱+泼尼松)化疗10疗程后淋巴瘤部分缓解;口服来那度胺维持半年后出现盆腔弥漫大B 细胞淋巴瘤转化,考虑淋巴瘤进展,再次给予9疗程R -C HO P 方案化疗;后出现中枢神经系统㊁肾上腺及淋巴结浸润,鞘内注射甲氨蝶呤+阿糖胞苷+地塞米松及大剂量甲氨蝶呤+利妥昔单抗化疗3疗程达部分缓解;后行自体造血干细胞移植治疗后淋巴瘤达完全缓解㊂口服伊布替尼单药维持治疗至今,现持续缓解3年余㊂结论 R -C HO P 方案化疗基础上的自体造血干细胞移植及伊布替尼单药维持治疗,对发生弥漫大B 细胞淋巴瘤组织转化的黏膜相关淋巴组织结外边缘区淋巴瘤病人有良好的治疗效果㊂[关键词] 淋巴瘤,B 细胞,边缘区;淋巴瘤,大B 细胞,弥漫性;伊布替尼[中图分类号] R 733.4 [文献标志码] B [文章编号] 2096-5532(2023)02-0304-04d o i :10.11712/jm s .2096-5532.2023.59.049[开放科学(资源服务)标识码(O S I D )][网络出版] h t t ps ://k n s .c n k i .n e t /k c m s /d e t a i l /37.1517.R.20230308.1035.009.h t m l ;2023-03-09 16:33:24T H EE X T R A N O D A L M A R G I N A LZ O N EL Y M P H O M A O F M U C O S A -A S S O C I A T E D L Y M P H O I D T I S S U ET R A N S F O R M E DI N T O D I F F U S EL A R G EB -C E L LL Y M P H O M A :AC A S ER E P O R TA N DL I T E R A T U R ER E V I E W Y A N S i qi ,L IT i a n l a n ,L I US h a n -s h a n ,MA O C h u n x i a ,F E N G X i a n q i ,Z HA O C h u n t i n g (D e p a r t m e n to f M e d i c i n eo fQ i n g d a o U n i v e r s i t y ,Q i n g d a o266071,C h i n a)[A B S T R A C T ] O b j e c t i v e T o i n v e s t i g a t et h ec l i n i c a ld i a g n o s i sa n dt r e a t m e n to fd i f f u s e l a r g eB -c e l l l y m p h o m a (D L B C L )t r a n s f o r m e d f r o me x t r a n o d a lm a r g i n a l z o n eB -c e l l l y m p h o m a o fm u c o s a -a s s o c i a t e d l y m p h o i d t i s s u e (MA L T -L ). M e t h o d s T h e c l i n i c a l d a t a o f a p a t i e n tw i t hD L B C L t r a n s f o r m e d f r o m p r i m a r y MA L T -Lw e r e r e t r o s p e c t i v e l y a n a l y z e d f o r c l i n i c a l c h a r a c t e r i s t i c s ,t r e a t m e n t ,a n d p r o g n o s i s ,a n dt h er e l e v a n tl i t e r a t u r e w a sr e v i e w e d . R e s u l t s T h e p a t i e n td i a gn o s e d w i t hr e c t a l MA L T -L a c h i e v e d p a r t i a l r e m i s s i o na f t e r 10c y c l e s o f c h e m o t h e r a p y w i t hR -C HO P (r i t u x i m a b ,c y c l o p h o s p h a m i d e ,d o x o r u b i c i n ,v i n o d i x i n ,a n d p r e d n i s o n e ).D L B C L t r a n s f o r m a t i o n o c c u r r e d i n t h e p e l v i c c a v i t y a f t e r s i xm o n t h s o fm a i n t e n a n c e t r e a t m e n tw i t h l e n a l i d o m i d e .A f t e r a n o t h e r 9c y c l e s o f c h e m o t h e r a p y w i t hR -C HO P ,t h e p a t i e n t s h o w e d c e n t r a l n e r v o u s s y s t e m ,a d r e n a l g l a n d ,a n d l y m ph n o d e i n f i l t r a t i o n .T h e p a t i e n t a c h i e v e d p a r t i a l r e m i s s i o na f t e r 3c y c l e s o f i n t r a t h e c a l i n j e c t i o no fm e t h o t r e x a t e +c y t a r a b i n e +d e x a m e t h a -s o n e a n d h i g h -d o s em e t h o t r e x a t e +r i t u x i m a b ,a n d c o m p l e t e r e m i s s i o n a f t e r a u t o l o g o u s h e m a t o p o i e t i c s t e mc e l l t r a n s p l a n t a t i o n .T h e p a t i e n t h a s b e e n i n c o m p l e t e r e m i s s i o n f o rm o r e t h a n3y e a r s o no r a l i b r u t i n i bm o n o t h e r a p y . C o n c l u s i o n I b r u t i n i bm a i n t e n a n c e t h e r a p y a n d a u t o l o g o u s h e m a t o p o i e t i c s t e mc e l l t r a n s p l a n t a t i o nb a s e do nR -C H O Pc h e m o t h e r a p y h a s a g o o d t h e r a pe u t i c ef f e c t o n MA L T -Lw i t hD L B C Lt i s s u e t r a n s f o r m a t i o n .[K E Y W O R D S ] l y m p h o m a ,B -c e l l ,m a r g i n a l z o n e ;l y m p h o m a ,l a r geB -c e l l ,d i f f u s e ;i b r u t i n i b 黏膜相关淋巴组织结外边缘区B 细胞淋巴瘤(MA L T -L )是一类来源于消化道㊁呼吸道和其他黏膜组织的惰性B 细胞非霍奇金淋巴瘤,占成年人非霍奇金淋巴瘤的7%~8%[1]㊂MA L T -L 转化的病例临床中相对少见,我院收治1例原发MA L T -L 转化为弥漫大B 细胞淋巴瘤(D L B C L )的病人,现报告如下㊂1 病例报告病人,女,28岁㊂因反复发热㊁盗汗1月,腹痛1周 于2016年3月至我院消化科就诊㊂自述于2016年2月受凉后出现发热,体温最高39.9ħ,于当地医院抗感染治疗有效㊂1周前出现阵发性上腹痛,伴恶心㊁黑便㊁乏力㊁头晕㊂查血常规:血红蛋白(H b )37.00g /L ,白细胞(W B C )6.18ˑ109/L ,血小板(P L T )183.00ˑ109/L ;大便隐血(+);乳酸脱氢酶(L D H )695.7U /L ;E B 病毒(E B V )(-)㊂消化道内镜检查:胃窦组织活检示幽门螺杆菌(H p )阳性;直肠内发现2处直径约0.2c m 广基隆起,伴顶端糜烂;于该隆起处取直肠组织Copyright ©博看网. All Rights Reserved.2期闫思琪,等.边缘区淋巴瘤转化为大B细胞淋巴瘤1例并文献复习305活检,病理示:黏膜组织内中等大小异形淋巴细胞弥漫浸润;免疫组化检查:肿瘤细胞,C D20弥漫(+),C D3+T淋巴细胞(+),B c l-6(-),C D10(-),M u m-1(-),K i-67的阳性率约10%,符合MA L T-L㊂行骨髓穿刺,骨髓形态学示增生极度低下骨髓象,分类不明细胞占20%,考虑淋巴瘤累及骨髓可能性大㊂骨髓流式示:I G H基因重排(+),免疫分型㊁染色体核型及T C R基因重排均未见明显异常㊂转入我科继续治疗㊂C T检查示:骨盆多发骨质破坏,考虑肿瘤浸润可能㊂颅脑M R I未见异常㊂诊断为:①黏膜相关淋巴组织结外边缘区B细胞淋巴瘤(Ⅳ期B,MA L T-I P I评分2分,高危);②淋巴瘤细胞白血病㊂2016年3月开始给予R-C HO P方案(利妥昔单抗+环磷酰胺+多柔比星+长春新碱+泼尼松)联合化疗10疗程㊂2016年11月复查骨髓穿刺未找到特殊细胞,P E T-C T示仍有少许活性肿瘤组织,S U V m a x值较前降低,考虑MA L T-L 部分缓解(P R)㊂此后门诊规律随诊治疗,以28d为1个周期,第1~14天每日服用10m g来那度胺维持治疗㊂2017年7月病人复查P E T-C T结果显示:左肺门㊁后纵隔食管旁及双侧髂外走行区多个肿大淋巴结,代谢增高, S U V m a x约3.5,较前新发㊂2017年8月出现腰酸㊁腰痛,伴间断肉眼血尿㊂泌尿系超声示:盆腔内阴道前方见低回声团,大小约9.2c mˑ8.6c mˑ7.7c m,形态不规则,边界不清;双侧髂窝多发淋巴结大㊂行超声引导下经会阴盆腔肿物穿刺术,病理结果提示非霍奇金淋巴瘤;免疫组化示:C D3 (-),C D20(+),B c l-2(-),B c l-6(-),C D10(-),M u m-1 (-),C D5(-),C D30(-),C D21(-),C y c l i nD1(-),K i-67阳性率约60%,符合D L B C L;骨髓穿刺未见特殊细胞㊂考虑病人淋巴瘤进展(P D),转化为D L B C L(Ⅲ期B)㊂2017年10月 2018年2月再次给予R-C HO P方案化疗9疗程㊂复查骨髓穿刺仍无特殊细胞㊂复查P E T-C T示:腹主动脉旁㊁右侧髂血管走行区及双侧腹股沟区多个增大淋巴结,S U V m a x 为13.2,较前部分新发㊁增大㊁代谢率增高㊂考虑D L B C L化疗后仍P D,提示治疗效果不佳,拟调整治疗方案行自体造血干细胞移植㊂病人于2018年3月行外周血干细胞采集,顺利获得C D34+干细胞>4ˑ106/k g㊂2018年4月复查胸腹部C T提示右肺下叶多发小结节影,右侧肾上腺占位性病变,考虑肿瘤病灶可能性大㊂病人诉左侧头部不适,颅脑M R I检查提示左侧顶叶及胼胝体异常信号(图1A),符合脑淋巴瘤表现㊂考虑病人中枢神经系统淋巴瘤累及,肾上腺及全身多处淋巴结受累,目前疾病进展,暂停干细胞移植计划,给予腰椎穿刺并鞘内注射2次甲氨蝶呤10m g+阿糖胞苷50m g+地塞米松5m g,并先后给予大剂量甲氨蝶呤+利妥昔单抗(甲氨蝶呤8.0g第1天,利妥昔单抗600m g第7天)化疗1次㊁阿糖胞苷+利妥昔单抗方案(甲氨蝶呤8.0g第1天,阿糖胞苷4000m g每12h应用1次第1~2天,利妥昔单抗600m g 第1~2天)化疗2次㊂于2018年7月复查,颅脑M R I示:胼胝体压部㊁左侧海马旁回占位性病变,较前明显好转(图1B);胸部及腹部C T示:胸腹部淋巴结及肾上腺病灶较前缩小,化疗效果可;腰椎穿刺未见异常细胞㊂病人一般情况可,头部不适症状较前改善,结合腰穿㊁头颅M R及腹部C T检查结果考虑D L B C L治疗后P R㊂遂于2018年8月行造血干细胞移植预处理B E MA方案(卡莫斯汀475m g第6天,阿糖胞苷320m g每12h用1次第2~5天,依托泊苷0.16g 每12h用1次第2~5天,马法兰225m g第1天)化疗,后行自体外周血干细胞移植㊂院外持续口服伊布替尼560m g/ d,门诊定期随诊至今,复查胸腹及盆腔C T未见异常包块, P E T-C T未见增大淋巴结,病人无明显出血㊁感染㊁腹泻及肌肉疼痛表现㊂病情较前无明显进展,提示自体外周血造血干细胞移植及伊布替尼维持治疗后D L B C L达完全缓解(C R)㊂现病人一般状况可,无明显不适㊂3讨论MA L T-L属于边缘区淋巴瘤(M Z L)的一种,是一种低度恶性的B细胞非霍奇金淋巴瘤,确诊病人的中位年龄为70岁,女性相对多见㊂MA L T-L最常发生于胃部(35.0%),其次为眼附属器(13.0%)㊁肺(8.8%)㊁结直肠(5.2%)和其他部位[2]㊂临床常表现为与受累器官相关的局部症状,也常有发热㊁盗汗等淋巴瘤相关的全身症状[3]㊂细胞学方面,镜下可见单核样B细胞平铺排列,胞浆透亮,并见病理性核分裂相㊂MA L T-L通常C D20和C D79a表达阳性,C D5㊁C D10和C y c l i nD1表达阴性[4]㊂本例病人因发热㊁腹痛就诊,直肠组织活检㊁免疫组化及骨髓穿刺结果符合MA L T-L㊁淋巴肉瘤细胞白血病的诊断,10疗程R-C HO P㊁C HO P方案化疗后P R,但其后仅半年余即出现盆腔D L B C L转化,病情进展迅速,临床少见㊂M Z L通常被认为属于惰性淋巴瘤,转变为其他侵袭性淋巴瘤的发生率约为12%[5],发生组织转化的中位时间为1.9年[6],现有报道多见于MA L T-L向D L B C L转化[7-10],发生这种转变的原因目前尚不明确㊂S A G A E R T等[10]对70例MA L T-L样本进行形态学检查和F O X P1染色,结果显示,t(3;14)(p14;q32)易位引起F O X P1强表达的MA L T-L 有转变为D L B C L的风险㊂V A S E F等[11]报道了1例患有MA L T-L伴D L B C L转化病例,原位杂交示MA L T-L细胞和大B细胞中均存在E B病毒且病毒的L M P1基因序列相同,表明E B病毒感染也可能造成MA L T-L的D L B C L转化㊂此外,S T A R O S T I K等[12]通过对24例胃MA L T-L进行微卫星筛查,比较筛查结果与胃D L B C L研究中检测到的畸变,结果显示MA L T-L中最常见的t(11;18)(q21;q21)易位产生的功能A P I2-MA L T1融合蛋白可激活核因子N F-κB,A P I2-MA L T1阳性的MA L T-L病人有较低的概率发生D L B C L表型转化㊂本文病人为青年女性病人,肠道起病,直肠黏膜组织活检符合MA L T-L表现,I G H基因重排(+),发生盆腔D L B C L转化时免疫组化提示K i-67阳性表达率较前明显升高㊂K i-67是细胞增殖的标志,其表达指数可以独立预测肿瘤进展[13-14]㊂不排除年龄因素㊁A P I2-MA L T1的Copyright©博看网. All Rights Reserved.306青岛大学学报(医学版)59卷A:2018年4月颅脑M R I检查;B:2018年7月颅脑M R I检查㊂图1病人颅脑M R I表现表达缺失及K i-67高表达是导致本例病人疾病进展的关键因素㊂目前,除局限性原发性胃MA L T-L可采用根除H p的方法治疗外,MA L T-L的治疗仍以联合化疗为主,尚无统一标准[15]㊂对于有临床侵袭性复发的MA L T-L病人,可考虑进行自体移植[1]㊂布鲁顿酪氨酸激酶(B T K)抑制剂伊布替尼为慢性淋巴细胞白血病/小淋巴细胞淋巴瘤㊁套细胞淋巴瘤的一线治疗药物[16]㊂一项Ⅱ期临床试验评估了63例复发和(或)难治性M Z L病人口服B T K抑制剂伊布替尼的治疗效果,显示伊布替尼有抗M Z L活性作用[17]㊂因此,口服伊布替尼560m g/d单药维持治疗为M Z L提供了一种新的无需化疗的治疗手段㊂奥妥珠单抗单独或者联合使用治疗初发和复发难治M Z L的疗效测试研究也正在进行中[18]㊂另外,对于出现组织学D L B C L转化的病人,应根据D L B C L 指南进行化疗和(或)免疫治疗[1];伊布替尼与R-C HO P联合使用已经在非生发中心源的D L B C L治疗中显示出良好的反应[19]㊂本例病人出现盆腔D L B C L转化后积极给予R-C HO P方案化疗9疗程,仍出现新发㊁增大淋巴结;1月后出现D L B C L的中枢神经系统(C N S)和肾上腺浸润,给予2次鞘内注射甲氨蝶呤+阿糖胞苷+地塞米松及3疗程化疗后较前好转㊂需要注意的是,30%的D L B C L缓解后在2~3年内复发[20],年龄增长㊁肾/肾上腺受累是D L B C L中枢神经系统复发的独立危险因素[21],持续关注肾/肾上腺受累情况㊁在化疗中或化疗结束后给予鞘内注射或静脉注射高剂量甲氨蝶呤可有效预防复发[19-21]㊂年龄ȡ70岁㊁A n nA r b o r分期Ⅲ期或Ⅳ期㊁乳酸脱氢酶(L D H)水平升高是影响MA L T-L病人预后的3个最有意义的临床参数,通常MA L T-I P I分期就是根据这3个参数将MA L T-L病人分为低㊁中㊁高危3组,其5年生存率分别为70%㊁56%和29%;且高危MA L T-L病人发生组织学转化概率更高[22],预后不良[23]㊂在一项回顾性研究中,A L D E-R U C C I O等[24]随访评估了397例新诊断的M Z L病人,更新修正了MA L T-I P I评分标准:将2个或2个以上不同的结外部位多黏膜发病(MM S)纳入评分标准,并且修正年龄范围为>60岁,重新定义了低风险㊁低中风险㊁中高风险和高风险4个风险组,其中位无进展生存期(P F S)分别为未能评估(N E)㊁12.8年㊁5.8年和1.8年[24];另外,新的评分标准能够更好地识别出24个月内有E A L T-L复发或进展(P O D24)可能的高风险病人[25]㊂本文病人初诊即为高危MA L T-L,规范治疗缓解后迅速出现D L B C L转化以及转化后C N S㊁肾上腺复发,均提示预后不良㊂病人目前一般状况良好,表明R-C HO P化疗基础上的自体造血干细胞移植及伊布替尼单药维持治疗对发生D L B C L组织转化的MA L T-L仍有良好的治疗效果㊂对本例病例临床资料进行分析旨在为MA L T-L的发生㊁发展及治疗提供更详细的参考,提高人们对该疾病认知,以期未来取得更好的疗效及更长的生存期㊂[参考文献][1]Z U C C A E,A R C A I N IL,B U S K E C,e ta l.M a r g i n a lz o n el y m p h o m a s:E S MOC l i n i c a l P r a c t i c eG u i d e l i n e s f o r d i a g n o s i s, t r e a t m e n ta n df o l l o w-u p[J].A n n a l s o f O n c o l o g y:O f f i c i a l J o u r n a l o f t h eE u r o p e a nS o c i e t y f o rM e d i c a lO n c o l o g y,2020, 31(1):17-29.[2]V I O L E T A F I L I P P,C U C I U R E A N U D,S O R I N A D I A-C O N U L,e ta l.MA L T l y m p h o m a:e p i d e m i o l o g y,c l i n i c a ld i a g n o s i s a n dt re a t m e n t[J].J o u r n a lof M e d i c i n ea n d L i f e,2018,11(3):187-193.[3]HWA N GJH,K I M D W,K I M KS,e t a l.M u c o s a-a s s o c i a t e dCopyright©博看网. All Rights Reserved.2期闫思琪,等.边缘区淋巴瘤转化为大B细胞淋巴瘤1例并文献复习307l y m p h o i d t i s s u e l y m p h o m ao f t h e a c c e s s o r yp a r o t i d g l a n d p r e-s e n t i n g a sas i m p l ec h e e k m a s s:ac a s er e p o r t[J].M e d i c i n e, 2019,98(36):e17042.[4]C O N C O N IA.H i s t o l o g i c t r a n s f o r m a t i o n i nm a r g i n a l z o n e l y m-p h o m a s[J].A n n a l s o fO n c o l o g y,2015,26(11):2329-2335.[5]L E N G L E TJ,T R A U L LÉC,MO U N I E RN,e t a l.L o n g-t e r mf o l l o w-u p a n a l y s i so f100p a t i e n t sw i t hs p l e n i c m a rg i n a l z o n el y m p h o m a t r e a t e dw i t h s p l e n e c t o m y a s f i r s t-l i n e t r e a t m e n t[J].L e u k e m i a&L y m p h o m a,2014,55(8):1854-1860. [6]A R S L A NSH,U Y E TÜR K U,T E K GÜN DÜZE,e t a l.P r i-m a r y b r e a s tm u c o s a-a s s o c i a t e d l y m p h o i d t i s s u e(MA L T)l y m-p h o m a t r a n s f o r m a t i o n t o d i f f u s e l a r g e B-c e l l l y m p h o m a:a c a s e r e p o r t[J].T u r k i s hJ o u r n a lo fH a e m a t o l o g y:O f f i c i a l J o u r n a l o fT u r k i s hS o c i e t y o fH a e m a t o l o g y,2012,29(3):274-277.[7]F U J I T A A,T A J I K A M,T A N A K AT,e t a l.Ac a s e o fA P I2-MA L T1-p o s i t i v e g a s t r i c MA L Tl y m p h o m a w i t hc o n c o m i t a n td i f f u se l a r g eB-c e l l l y m p h o m a[J].N a g o y aJ o u r n a l of M e d i c a lS c i e n c e,2017,79(2):251-257.[8]李文智,蒋超梅,王安标.腮腺MA L T淋巴瘤伴大B细胞淋巴瘤转化1例[J].中国临床医学影像杂志,2019,30(9):672-674.[9]王磊,陈华,蓝松,等.甲状腺粘膜相关淋巴瘤转化为弥漫性大B淋巴瘤1例[J].临床医药文献电子杂志,2019,6(53):163.[10]S A G A E R T X,D E P A E P E P,L I B B R E C H T L,e ta l.F o r k-h e a db o x p r o t e i nP1e x p r e s s i o n i nm u c o s a-a s s o c i a t e d l y m p h o i dt i s s u e l y m p h o m a s p r e d i c t s p o o r p r o g n o s i sa n dt r a n s f o r m a t i o n t od i f f u s e l a r g eB-c e l l l y m p h o m a[J].J o u r n a l o fC l i n i c a lO n c o-l o g y:O f f i c i a l J o u r n a l o f t h eA m e r i c a nS o c i e t y o fC l i n i c a lO n-c o l o g y,2006,24(16):2490-2497.[11]V A S E F M A,W E I S SL M,C H E N Y Y,e t a l.G a s t r i c l y m-p h o e p i t h e l i o m a-l i k e c a r c i n o m aa n d j e j u n a lB-c e l lMA L Tl y m-p h o m aw i t h l a r g ec e l l t r a n s f o r m a t i o n.D e m o n s t r a t i o no fE B Vw i t h i d e n t i c a lL M P g e n ed e l e t i o n s i nt h ec a r c i n o m aa n d l a r g ec e l l l y m p h o m a[J].A m e r i c a nJ o u r n a lo fC l i n i c a lP a t h o l o g y,1996,105(5):560-566.[12]S T A R O S T I K P,P A T Z N E RJ,G R E I N E R A,e ta l.G a s t r i cm a r g i n a l z o n eB-c e l l l y m p h o m a s o fMA L Tt y p ed e v e l o p a l o n g 2d i s t i n c t p a t h o g e n e t i c p a t h w a y s[J].B l o o d,2002,99(1):3-9.[13]S E V I CI,S P I N E L L IF M,V I T A L E D L,e t a l.H y a l u r o n a nm e t a b o l i s mi s a s s o c i a t e dw i t hD N Ar e p a i r g e n e s i nb r e a s t a n dc o l o r e c t a l c a n c e r.s c r e e n i n g o f p o t e n t i a l p r o g r e s s i o n m a r k e r su s i n gq P C R[J].B i o m e d i c i n e s,2020,8(7):183. [14]WO N J H,K I M S M,K I M J W,e ta l.C l i n i c a l f e a t u r e s,t r e a t m e n t a n do u t c o m e so fc o l o r e c t a lm u c o s a-a s s o c i a t e dl y m-p h o i d t i s s u e(MA L T)l y m p h o m a:l i t e r a t u r e r e v i e w s p u b l i s h e di nE n g l i s h b e t w e e n1993a n d2017[J].C a n c e rM a n a g e m e n t a n dR e s e a r c h,2019,11:8577-8587.[15]N O Y A,D E V O SS,C O L E MA N M,e t a l.D u r a b l e i b r u t i n i br e s p o n s e si n r e l a p s e d/r e f r a c t o r y m a r g i n a lz o n el y m p h o m a: l o n g-t e r mf o l l o w-u p a n d b i o m a r k e ra n a l y s i s[J].B l o o d A d-v a n c e s,2020,4(22):5773-5784.[16]N O Y A,D E V O SS,T H I E B L E MO N T C,e ta l.T a r g e t i n gB r u t o nt y r o s i n e k i n a s e w i t hi b r u t i n i bi nr e l a p s e d/r e f r a c t o r ym a r g i n a l z o n el y m p h o m a[J].B l o o d,2017,129(16):2224-2232.[17]C A V A L L O N IC,V A R E T T O N IM,R A T T O T T I S,e t a l.E-v a l u a t i n g i b r u t i n i bf o rt h et r e a t m e n to fr e l a p s e d/r e f r a c t o r y m a r g i n a l z o n el y m p h o m a[J].E x p e r t O p i n i o no n P h a r m a c o-t h e r a p y,2021,22(13):1643-1649.[18]T I L L Y H,G OM E SD A S I L V A M,V I T O L O U,e ta l.D i f-f u s e l a rg e B-c e l l l y m ph o m a(D L B C L):E S MOC li n i c a l P r a c t i c eG u i d e l i n e s f o r d i a g n o s i s,t r e a t m e n ta n df o l l o w-u p[J].A n n a l so fO n c o l o g y:O f f i c i a l J o u r n a l o f t h eE u r o p e a nS o c i e t y f o rM e-d i c a lO n c o l o g y,2015,26(S u p p l5):v116-v125.[19]Y U A N T,Z H A N GF,Y A OQ M,e t a l.M a i n t e n a n c e t h e r a p yf o r u n t r e a t e dd i f f u s e l a rg eB-c e l l l y m ph o m a:as y s t e m a ti c r e-v i e wa n dn e t w o r k m e t a-a n a l y s i s[J].T h e r a p e u t i cA d v a n c e s i nH e m a t o l o g y,2021,12:20406207211018894.[20]W I L S O N M R,E Y R ETA,K I R KWO O DA A,e t a l.T i m i n go f h i g h-d o s em e t h o t r e x a t eC N S p r o p h y l a x i s i nD L B C L:am u l-t i c e n t e ri n t e r n a t i o n a la n a l y s i s o f1384p a t i e n t s[J].B l o o d, 2022,139(16):2499-2511.[21]T H I E B L E MO N T C,C A S C I O N EL,C O N C O N IA,e t a l.AMA L T l y m p h o m a p r o g n o s t i c i n d e x[J].B l o o d,2017,130(12): 1409-1417.[22]C A S U L OC,F R I E D B E R GJ.T r a n s f o r m a t i o n o fm a r g i n a l z o n el y m p h o m a(a n da s s o c i a t i o n w i t ho t h e r l y m p h o m a s)[J].B e s t P r a c t i c e&R e s e a r c h C l i n i c a l H a e m a t o l o g y,2017,30(1-2): 131-138.[23]A L D E R U C C I OJP,R E I SIM,H A B E R MA N N T M,e t a l.R e v i s e d MA L T-I P I:a n e w p r e d i c t i v e m o d e lt h a ti d e n t i f i e sh i g h-r i s k p a t i e n t s w i t h e x t r a n o d a l m a r g i n a lz o n el y m p h o m a[J].A m e r i c a nJ o u r n a lo f H e m a t o l o g y,2022,97(12):1529-1537.[24]A L D E R U C C I OJP,Z H A O W,D E S A IA,e t a l.S h o r t s u r v i-v a l a n df r e q u e n tt r a n s f o r m a t i o ni ne x t r a n o d a l m a r g i n a lz o n e l y m p h o m aw i t hm u l t i p l em u c o s a l s i t e s p r e s e n t a t i o n[J].A m e-r i c a n J o u r n a l o fH e m a t o l o g y,2019,94(5):585-596.(本文编辑黄建乡)作者书写文内标题须知本刊文内标题序号使用阿拉伯数字顺序编码,左顶格书写㊂标题一般可分为3~4级,即:1,2,3 ;1.1,1.2,1.3 ;1.1.1,1.1.2, 1.1.3 ;1.1.1.1,1.1.1.2,1.1.1.3 ㊂第5级标题可用(1)或①㊂1,2级标题均单独占行㊂请作者来稿时遵照执行㊂Copyright©博看网. All Rights Reserved.。
126例原发胃弥漫大B细胞淋巴瘤的临床特点及预后分析

126例原发胃弥漫大B细胞淋巴瘤的临床特点及预后分析秦燕;何小慧;周生余;刘鹏;杨建良;张长弓;杨晟;桂琳;石远凯【摘要】目的:分析胃弥漫大B细胞淋巴瘤(DLBCL)的临床特点和预后,以期更好的指导治疗。
方法:回顾性收集1999年1月至2012年3月中国医学科学院肿瘤医院收治的初治、胃原发DLBCL患者的临床资料,分析其人口学特点、分期、病理诊断、并发症、治疗和预后等特征。
结果:共计纳入研究患者126例,中位年龄49(16~81)岁,男女比例为68:58。
病理诊断为单纯DLBCL 96例、MALT伴大B细胞转化27例、伴浆样细胞分化3例。
早期患者114例(90.5%),其治疗方式包括单纯化疗37例、化疗+放疗39例、手术+化疗±放疗38例。
中位随访48个月,全组患者PFS和OS分别为75.6%和82.7%,早期和晚期患者的PFS分别为77%和41.7%(P=0.005)。
早期患者采用单纯化疗、化放疗联合和含手术治疗的PFS分别为67.3%、77.8%和77.8%(P=0.588)。
国际预后指数(IPI)评分为0分、1分和>1分患者的PFS分别为85.4%,74.4%和55.6%(P=0.011)。
Ⅰ期和Ⅱ期患者的PFS分别为81.2%和66.1%(P=0.018)。
LDH正常和升高患者的PFS分别为86.6%和63.3%(P=0.006)。
病理类型为单纯DLBCL和含有MALT成分、生发中心(GCB)和非生发中心(non-GCB)、年龄>60岁等与预后无关。
结论:早期病变比例占胃原发DLBCL 患者的绝大多数。
早期患者预后良好,手术切除并不能提高疗效。
早期患者中IPI>1分、LDH升高和临床分期II期提示预后不良。
%Objective:Primary gastric diffuse large B-cell lymphoma (PGLBCL) is a highly common subtype of extranodal non-Hodgkin lymphoma. We analyzed the disease's clinical features and prognosis to guide better treatment. Methods:We retrospectively collect-ed data from PGLBCL cases seen from January 1999to March 2012 in one cancer center. We then analyzed the demographic character-istics, clinical stage, histological diagnosis, complications, treatment, and prognostic characteristics of such patients. Results:A total of 126 patients with median age of 49 years old (range:16-81 years) were included in the study. The male-to-female ratio was 68:58. A to-tal of 96 patients were pathologically diagnosed with pure diffuse large B-cell lymphoma (DLBCL), 27 with mucosa-assouated lymphoid (MALT) component, and 3 with plasmacytoid differentiation. Meanwhile, 90%of the patients were in the early stage of the disease. For the early-stage patients, treatment strategy included surgery+chemotherapy ± radiotherapy for 38 cases, chemoradiotherapy for 39 cases, chemotherapy alone for 37 cases, and surgery alone for 1 case. Under a median follow up of 48 months, the 4-year progres-sion free survival (PFS) and overall ourvival (OS) rate of the whole group were 75.6%and 82.7%, respectively. PFS rates for early and advanced stage patients were 77%and41.7%(P=0.005), respectively. For the early-stage patients treated with chemotherapy alone, chemoradiotherapy, and surgery with therapy, the PFS rates were 67.3%, 77.8%, and 77.8%(P=0.588), respectively. The patients with international prognostic index (IPI) score of 0, 1, and>1 achieved PFS of 85.4%, 74.4%, and 55.6%(P=0.011), respectively. The PFS rates were 81.2%and 66.1%(P=0.018) for stagesⅠandⅡ, respectively, and 86.6%and 63.3%(P=0.006) for the normal and elevated LDH levels, respectively. The pathological type of pure DLBCL or a MALT component, GCB or non-GCB origin, and age more than 60 years old were notassociated with prognosis. Conclusion:The majority of the PGLBCL patients were in the early stage of disease, but the outcome of early-stage disease was favorable. Surgery did not improve outcomes. Univariate analysis demonstrated that IPI score>1, stageⅡdisease, and elevated LDH levels were associated with poor prognosis in the early-stage patient.【期刊名称】《中国肿瘤临床》【年(卷),期】2016(043)014【总页数】6页(P620-625)【关键词】弥漫大B细胞淋巴瘤;胃原发淋巴瘤;化疗;放射治疗;手术【作者】秦燕;何小慧;周生余;刘鹏;杨建良;张长弓;杨晟;桂琳;石远凯【作者单位】国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021;国家癌症中心/北京协和医学院中国医学科学院肿瘤医院内科,抗肿瘤分子靶向药物临床研究北京市重点实验室北京市100021【正文语种】中文秦燕,医学博士,现任中国医学科学院肿瘤医院内科副主任医师,兼任中国抗癌协会肿瘤临床化疗专业委员会第一届青年委员会副主任委员。
阑尾炎英文

Centr2a02l-1S/o7u/1th7 University
8
Artery
The appendix artery has no branches, is easily to be obstacled
pain can be most pronounced if the patient has pelvic appendix
Centr2a02l-1S/7o/u17th University
22 22
Physical Exam
Additional components that may be helpful in diagnosis:
7
Etiology
1. The anatomy characteristics
2. The tissue features 3. fecality, foreign body obstruction 4. Parasites cause the mucosa damage
5. adhesion, pressure cause appendix distorted
阑尾炎英文
Centr2a02l-1S/7o/u17th University 2
Anatomy
Centr2a02l-1S/o7u/1th7 University
3
Varied anatomy
haustra of colon
Centr2a02l-1S/7o/u1t7h University
利妥昔单抗在成人微小病变肾病中的应用

利妥昔单抗在成人微小病变肾病中的应用方锦颖h2刘琳2综述卓莉李文歌审校1北京中医药大学,北京100029;2中曰友好医院肾病科,北京100029通信作者:刘琳,E m a il:yum m ylynn@ 126. com【摘要】微小病变肾病(MCD)是肾病综合征的常见原因,目前认为其发病机制与T淋巴细胞介导的细胞免疫及B淋巴细胞介导的体液免疫关系密切。
利妥昔单抗(RTX)是针对CD20的一种单克隆抗体,2007年开始被用于治疗成人MCD..根据在PubMed中检索到的KTX治疗成人MCD的所有文献显示RTX能够将表现为难治性肾病综合征的MCD患者缓解率提高至70.4% ~ 100.0%,并且缓解时间缩短至1 ~2个月,减少了激素的使用剂量,甚至停用激素,同时能够大大降低其复发率,在复发后再次使用RTX仍能取得明显疗效在安全性方面,所有文献均未报道严重不良反应,常见的不良反应有轻微的输液反应、药疹、轻度感染、白细胞减少等【关键词】肾病,脂性;利妥昔单抗;自身免疫基金项目:国家自然科学基金(81600547,81870495 )D O I:10. 3760/c m a.j. c n431460-20200224-00051微小病变肾病(minimal change disease,MCD)是肾病综合征的常见原因,占成人原发性肾病综合征发病原因的10% ~20%。
临床常表现为明显水肿、大量蛋白尿、低蛋白血症及高脂血症,少见血尿。
发病高峰主要在儿童及育少年,其次为老年人1肾脏活检是其诊断的金标准,免疫荧光多为阴性,光镜下肾小球大致正常,电镜下一般仅有足突广泛融合。
糖皮质激素是治疗MCD最常用的药物,但部分MCD患者对激素并不敏感,尤其在成人MCD患者,10% ~ 20%的成人患者对激素具有耐药性__2即使对激素敏感,成人M C D患者也具有较卨的复发倾向,据统计56%〜76%.的患者在激素诱导的缓解后复发'。
消化病学常见英语对照
消化病学常见英文1.digestive endoscope消化内镜 2. digest 消化 3.Gastric mucosa 胃粘膜4.Helicopbacter pylori 幽门螺杆菌 5.gastric pits 胃小凹6. gullet 食管7.Castroesophageal Reflux Disease(GERD) 胃食管反流病8.Barrett’s esophagus,Barrett食管9. lower esophageal sphincter 食管下括约肌10. reflux esophagitis 反流性食管炎11. lower esophageal sphincter LES 下食管括约肌12. non-erosive reflux disease(NERD)非糜烂性反流病13. oesophagoscopy 食管镜检查14. Hiatal Hernia, 食管裂孔疝15.oesophagoscope 食管镜,食道镜16. transient lower esophageal sphincter relaxatio n 一过性食管下括约肌松弛17. leiomyoma of esophagus. 食管平滑肌瘤18.Esophageal Cancer 食管癌19..corrosive burn of esophagus腐蚀性食管灼伤20.achalasia of cardia 贲门失驰症21.stomach 胃.22.gastritis胃炎23. pangastritis 全胃炎24.acute hemorrhagic gastritis 急性出血性胃炎25 Chronic gastritis慢性胃炎26.Chronic atrophic gastritis 慢性萎缩性胃炎27.autoimmune gastritis 自身免疫性胃炎28. Chronic superficial gastritis 慢性浅表性胃炎29. superficial gastirtis 弥漫性胃窦炎30.Functional gastrointestinal disorder 功能性胃肠病31. functional dyspepsia 功能性消化不良32.multi-focal atrophic gastritis多灶萎缩性胃炎33.dysplasia 异型增生34. parietal cell autoantibody 壁细胞自体抗体35.intrinsic factor antibody,IFA 内因子抗体36.intestinal metaplasia of gastric epithelium 胃粘膜肠上皮化生37. Peptic Ulcer Disease (PUD), 消化性溃疡病38. ZollingerEllison syndrome 胃泌素瘤.39.kissing ulcer 对吻溃疡40. acute stress ulcer 急性应激性溃疡41.Gastrointestinal mucosa-associated lymphoid tissue lymphoma 胃粘膜相关淋巴组织淋巴瘤42. Stomach cancer 胃癌43.gastric bleeding 胃出血44.gastric canal 胃管45.gastric juice 胃液46.gaseous distention 胃胀气47. hematemesis 呕血48.gastralgia 胃痛49.gastroenteritis 胃肠炎50.Gastric Acid胃酸51. achlorhydria胃酸缺乏症52.gastrospasm 胃痉挛53.intestine肠54. tuberculose intestinale 肠结核55.Appendicitis 大腸炎56. tuberculated peritonitis结核性腹膜炎57. Intussusception 肠套叠58. Volvulus 盲腸炎59. intestinal cancer肠癌60 ileus.肠闭塞61. Enterovirus肠病毒62. intestinal hemorrhage肠出血63.intestinal perforation肠穿孔64. intestinal obstruction肠梗阻65.intestinal colic 肠绞痛66. inflammatory bowel disease 炎症性肠病67. Regional Enteritis (Crohn)克隆氏病68.Ulceratie Colitis, 溃疡性结肠炎69.Dierticular Disease, 肠憩室疾病70.carcinoid of large intestine 大肠类癌71.colorectal lymphoma 大肠恶性淋巴瘤72. Polyposis 息肉病73.family polyposis coli 家族性结肠息肉病74.irritable bowel syndrome 肠易激综合征75. bacterial translocation from intestine 肠道细菌移位 76. enteral nutrition肠道营养, 77. arteriovenous malformation of bowel肠动静脉畸形78.enteric cyst 肠囊肿79. radiation injury of intestine肠放射性损伤80.end-to-side intestinal anastomosis 肠端侧吻合术81. volvulus 肠扭转82. end-to-end intestinal anastomosis 肠端端吻合术82. bowel disturbance 肠紊乱,83. intestinal lymphangiectasia肠淋巴管扩张84 intestinal bypass肠旁路术85.肠内引流式胰腺移植enteric drainage pancreas transplantation86肠袢淤滞综合征stagnant loop syndrome 87.肠切除术intestinal resection88.肠切开术enterotomy 89.肠缺血ischemia of intestine90.肠缺血综合征intestinal ischemic syndrome 91.肠外瘘enterocutaneous fistula 92.肠外营养parenteral nutrition 93.肠外置术intestinal exteriorization 94.肠吻合术intestinal anastomosis 95.肠系膜动脉闭mesenteric arterial occlusion 96.肠系膜动脉栓塞术mesenteric artery embolization 97.肠系膜动脉血栓形成mesenteric artery thrombosis 98.肠系膜静脉血栓形mesenteric venous thrombosis 99.肠系膜囊肿mesenteric cyst 100.肠系膜疝mesenteric hernia101.肠系膜上动脉综合征superior mesenteric artery syndrome102肠系膜上动脉压迫综合征superior mesenteric artery compression syndrome103.肠狭窄intestinal stenosis 104肠旋转不良malrotation of intestine105.肠血管病vascular disease of bowel 106.肠血管发育异angiodysplasia of bowel 107.肠血管异常vascular abnormality of intestine 108.肠易激综合征irritable bowel syndrome 109.肠源性感染enterogenic infection 110.肠造口术enterostomy111.肠胀气intestinal tympanites 112.肠重复畸形duplication of intestine113.肠子宫内膜异位endometriosis in bowel 114.乙状结肠膀胱sigmoid conduit115.乙状结肠膀胱扩大sigmoid augmentation cystoplasty 116.乙状结肠结核tuberculosis of sigmoid colon 117.乙状结肠镜检查[术]sigmoidoscopy 118.回肠膀胱扩大术ileum augmentation cystoplasty 119.回肠膀胱尿流改道术ileal conduit diversion 120.回肠膀胱术ileal conduit Bricker operation 121.回肠肛管吻合术ileoanal anastomosis 122.回肠横结肠吻合术ileotransversostomy123.回肠憩室ileal diverticulum 124.回肠造口术ileostomy125.回盲部结核ileocecal tuberculosis 126.直肠膀胱一结肠腹壁造口术rectal bladder and abdominal colostomy 127.直肠固定术proctopexy,rectopexy128.直肠后脓肿retrorectal abscess 129.直肠后拖也吻合巨结肠根治术duhamel procedure 130.直肠环钳吻合术ring clamp anastomosis of rectum131.直肠肌鞘拖出吻合巨结肠根治术soave procedure132直肠镜检查[术]proctoscopy 133.直肠瘘rectal fistula134.直肠膨出rectocele 135.直肠切除术proctectomy136.直肠烧灼rectal burning 137.直肠损伤rectal injury138.直肠脱垂rectal prolapse 139.直肠狭窄stricture of rectum140,直肠炎proctitis 141.直肠乙状结肠镜检查[术]proctosigmoidoscopy142.直肠阴道瘘rectovaginal fistula 143.直肠指检digital rectal examination144.直肠周围脓肿perirectal abscess 145.直视下活检[术]direct vision biopsy 145.肛管癌cancer of anal canal 146.肛裂anal fissure,147.肛门闭锁会阴瘘anal atresia with perineal fistula 148.肛门闭锁尿道瘘anal atresia with urethral fistula 149.肛门闭锁前庭瘘anal atresia with vestibular fistula 150.肛门闭锁阴道瘘anal atresia with vaginal fistula 151.肛门镜anoscope152.肛门镜检查[术]anoscopy 153.肛门溃疡anal ulcer154.肛门瘙痒[症]pruritus ani 155.肛门狭窄anal stenosis156.肛门直肠瘘anorectal fistula 157.肛门直肠脓肿anorectal abscess158.肛乳头炎anal papillitis 159.肛周脓肿,perianal abscess160.肝脏liver 161肝癌liver cancer 162.阑尾Appendicitis,163.肝性脑病Hepatic encephalopathy 164.肝昏迷hepatic coma165.原发性肝癌primary carcinoma of the liver.166.病毒性肝炎virus hepatitis 167.传染性肝炎infectious hepatitis 168.急性病毒性肝炎acute viral hepatitis 169.慢性腹泻chronic diarrhea 170.酒精性肝病alcoholic lier171.自身免疫性肝炎autoimmune hepatitis 172.肝硬化cirrhosis of lier 173.腹膜炎Peritonitis, 174.干呕retch 175.肝[性]昏迷前期hepatic precoma 176.肝被膜下出血subcapsular hemorrhage of liver 177.肝病性口臭fetor hepaticus178.肝肠联合移植combined liver and intestine transplantation 179.肝大hepatomegaly 180肝淀粉样变性amyloidosis of liver 181.肝动脉造影[术]hepatic arteriography 182.肝梗死infarction of liver 183.肝结核tuberculosis of liver184.肝静脉梗阻hepatic venous obstruction 185.肝慢性阻性充血chronic passive congestion of liver 186.肝毛细线虫病capillariasis hepatica187.肝门肠吻合术portoenterostomy 188.肝内胆管结石calculus of intrahepatic duct 189.肝内胆管结石病hepatolithiasis 190.肝内胆汁淤积intrahepatic cholestasis191.肝脓肿liver absces 192.肝脾大hepatosplenomegaly193.肝片吸虫病fascioliasis hepatica 194.肝肾联合移植combined liver and kidney transplantation 195.肝肾综合征hepatorenal syndrome196.肝素辅因子heparin co-factor 197.肝细胞移植hepatocyte transplantation198.肝下垂hepatoptosis 199.上消化道出血 upper gastrointestinal hemorrhage200.壁细胞parietal cell 201. 质子泵proton pump 202, 痔疮Hemorrhoids203. gall bladder 胆囊. pancreas 胰腺204. 内镜逆行胰胆管造影endoscopic retrograde cholangiopancreatography ,ERCP 205.胆石症/胆囊炎Cholelithiasis/Cholecystitis 206.急性胰腺炎Acute Pancreatitis, 207.胰腺癌carcinoma of the Pancreatitis 208.胰空肠吻合术pancreaticojejunostomy 209.胰瘘pancreatic fistula 210.胰肾联合移植combined pancreas and renal transplantation211.胰十二指肠切除术pancreaticoduodenectomy 212.胰十二指肠移植术pancreas-duodenal transplantation 213.胰石pancreatolith,pancreatic calculus 214.胰石病pancreatolithiasis 215.胰腺创伤pancreatic trauma216.胰腺分裂pancreas divisum 217.胰腺钙化calcification of pancreas218.胰腺假囊肿pancreatic pseudocyst 219.胰腺囊肿pancreatic cyst220.胰腺脓肿abscess of pancreas 221.胰腺外瘘external fistula of pancreas 222.胰腺炎pancreatitis 223.胰腺移植pancreas transplantation224.胰腺异位heterotopic pancreas 225.胰腺周围脓肿peripancreatic abscess 226.胰源性腹水pancreatic ascites 227.移动性盲肠mobile caecum228.移植胰假性囊肿graft pancreatic pseudocyst229.移植胰胰瘘graft pancreatic fistula 230.移植胰胰腺炎graft pancreatitis231.胆道闭锁biliary atresia232.胆道测压[术]manometry of biliary tract 233.胆道出血hemobilia234.胆道感染infection of biliary tract 235胆道梗阻obstruction of biliary tract236.胆道蛔虫病biliary ascariasis 237.胆道贾第虫病giardiasis of biliary tract238.胆道减压术decompression of biliary tract 239.胆道闪烁显像[术]cholescintigraphy 240.胆道运动障碍biliary dyskinesia 241.胆固醇结石cholesterol calculus242胆管癌carcinoma of bile duct 243.胆管测压造影[术]manometric cholangiography 244.胆管肝炎cholangiohepatitis 245.胆管空肠吻合术cholangiojejunostomy246.胆管扩张cholangiectasis 247.胆管内置管扩张[术]biliary stent dilatation248.胆管腺瘤cholangioadenoma 249.胆管炎cholangitis250.胆管造影[术]cholangiography 251.胆管周围炎pericholangitis252.胆红素脑病bilirubin encephalopathy,kernicterus 253.胆红素尿bilirubinuria 254.胆绞痛biliary colic 255.胆瘘biliary fistula 256.胆囊癌carcinoma of gallbladder 257.胆囊肠瘘cholecystoenteric fistula 258.胆囊超声显像[术]cholecystosonography 259.胆囊穿孔perforation of gallbladder 260.胆囊钙化calcification of gallbladder 261.胆囊积脓empyema of gallbladder 262.胆囊积气pneu-gallbladder 263.胆囊积水hydrops of gallbladder 264.胆囊积血hemocholecyst265.胆囊镜检查[术]cholecystoscopy 266.胆囊空肠吻合术cholecystojejunostomy 267.胆囊扭转torsion of gallbladder 268.胆囊切除术cholecystectomy269.胆囊切除术后综合征postcholecystectomy syndrome270,胆囊十二指肠吻合术cholecystoduodenostomy 271.胆囊收缩素cholecystokinin 272.胆囊炎cholecystitis 273.胆囊造口术cholecystostomy 274胆囊造影术cholecystography275.胆囊周围脓肿pericholecystic abscess 276.胆石性肠梗阻gallstone ileus277.胆总管结石calculus of common bile duct 278.胆小管炎cholangiolitis279.胆血症cholemia 280.胆总管梗阻obstruction of common bile duct 281.胆汁反流性胃炎bile reflux gastritis 282.胆总管端端吻合术choledochocholedochostomy 283.胆汁浓缩综合征inspissated bile syndrome 284.胆汁性腹膜炎biliary peritonitis,choleperitoneum 285.胆汁性肝硬化biliary cirrhosis 286.胆总管十二指肠吻合术choledochoduodenostomy 287.胆汁引流biliary drainage 288.胆汁淤积cholestasis 289.胆汁粘稠综合征biliary hyperviscosity syndrome290.[内镜]操纵部, [endoscopic]control section291.[内镜]插入管, [endoscopic]insertion tube292.[内镜]充气/水阀, [endoscopic]air/water valve293.[内镜]导光连接部, [endoscopic]light guide connector section294.[内镜]导光束, [endoscopic]light guide bundles295.[内镜]导像束, [endoscopic]image guide bundles296.[内镜]光导纤维, [endoscopic]optical fibers297.[内镜]活检管道开口, [endoscopic]biopsy channel opening298.[内镜]角度锁钮, [endoscopic]locking knob299.[内镜]角度旋钮, [endoscopic]angulation knob300.[内镜]冷光源, [endoscopic]cold light source301.[内镜]弯曲部, [endoscopic]bending section302.[内镜]吸引阀, [endoscopic]suction valve。
(整理)消化病学常见英文词汇
消化病学常见英文词汇1.digestive endoscope消化内镜2. digest 消化3.Gastric mucosa 胃粘膜4.Helicopbacter pylori 幽门螺杆菌5.gastric pits 胃小凹6.gullet 食管7.Castroesophageal Reflux Disease(GERD) 胃食管反流病8.Barrett’s esophagus,Barrett食管9.lower esophageal sphincter 食管下括约肌10.reflux esophagitis 反流性食管炎11.lower esophageal sphincter LES 下食管括约肌12.non-erosive reflux disease(NERD)非糜烂性反流病13.oesophagoscopy 食管镜检查14.Hiatal Hernia, 食管裂孔疝15.oesophagoscope 食管镜,食道镜16.transient lower esophageal sphincter relaxatio n 一过性食管下括约肌松弛17.leiomyoma of esophagus.食管平滑肌瘤18.Esophageal Cancer 食管癌19..corrosive burn of esophagus腐蚀性食管灼伤20.achalasia of cardia 贲门失驰症21.stomach 胃.22.gastritis胃炎23.pangastritis 全胃炎24.acute hemorrhagic gastritis 急性出血性胃炎25 Chronic gastritis慢性胃炎26.Chronic atrophic gastritis 慢性萎缩性胃炎27.27.autoimmune gastritis 自身免疫性胃炎28.Chronic superficial gastritis 慢性浅表性胃炎29.29.superficial gastirtis 弥漫性胃窦炎30.Functional gastrointestinal disorder 功能性胃肠病30.31.functional dyspepsia 功能性消化不良32.multi-focal atrophic gastritis多灶萎缩性胃炎33.dysplasia 异型增生34.parietal cell autoantibody 壁细胞自体抗体35.intrinsic factor antibody,IFA 内因子抗体36.intestinal metaplasia of gastric epithelium 胃粘膜肠上皮化生37.Peptic Ulcer Disease (PUD), 消化性溃疡病38.ZollingerEllison syndrome 胃泌素瘤.39.kissing ulcer 对吻溃疡40.acute stress ulcer 急性应激性溃疡41.Gastrointestinal mucosa-associated lymphoid tissue lymphoma 胃粘膜相关淋巴组织淋巴瘤42.Stomach cancer 胃癌43.gastric bleeding 胃出血44.gastric canal 胃管45.gastric juice 胃液46.gaseous distention 胃胀气47.hematemesis 呕血48.gastralgia 胃痛49.gastroenteritis 胃肠炎50.Gastric Acid胃酸51.achlorhydria胃酸缺乏症52.gastrospasm 胃痉挛53.intestine肠54.tuberculose intestinale 肠结核55.Appendicitis 大腸炎56.tuberculated peritonitis结核性腹膜炎57.Intussusception 肠套叠58.Volvulus 盲腸炎59.intestinal cancer肠癌60 ileus.肠闭塞61.Enterovirus肠病毒62.intestinal hemorrhage肠出血63.63.intestinal perforation肠穿孔64.64.intestinal obstruction肠梗阻65.65.intestinal colic 肠绞痛66.66.inflammatory bowel disease 炎症性肠病67.67.Regional Enteritis (Crohn)克隆氏病68.68.Ulceratie Colitis, 溃疡性结肠炎69.69.Dierticular Disease, 肠憩室疾病70.70.carcinoid of large intestine 大肠类癌71.71.colorectal lymphoma 大肠恶性淋巴瘤72.72.Polyposis 息肉病73.family polyposis coli 家族性结肠息肉病74.irritable bowel syndrome 肠易激综合征75.肠道细菌移位76.enteral nutrition肠道营养,77.arteriovenous malformation of bowel肠动静脉畸形78.肠囊肿79.radiation injury of intestine肠放射性损伤80.end-to-side intestinal anastomosis 肠端侧吻合术81.肠扭转82.end-to-肠端端吻合术82.肠紊乱,83.intestinal lymphangiectasia肠淋巴管扩张84 intestinal bypass肠旁路术85.肠内引流式胰腺移植enteric drainage pancreas transplantation86肠袢淤滞综合征stagnant loop syndrome87.肠切除术88.肠切开术89.肠缺血90.肠缺血综合征91.肠外瘘enterocutan92.肠外营养93.肠外置术94.肠吻合术95.肠系膜动脉闭mesenteric arterial occlusion96.肠系膜动脉栓塞术97.肠系膜动脉血栓形成98.肠系膜静脉血栓形99.肠系膜囊肿100.肠系膜疝101.肠系膜上动脉综合征102肠系膜上动脉压迫综合征103.肠狭窄104.104肠旋转不良malr105.肠血管病vascular disease of bowel106.106.肠血管发育异107.107.肠血管异常108.108.肠易激综合征109.109.肠源性感染110.110.肠造口术111.肠胀气112.112.肠重复畸形duplication of intestine113.肠子宫内膜异位114.乙状结肠膀胱sigmoid conduit114.乙状结肠膀胱扩大sigmoid augmentation cystoplasty116.乙状结肠结核117.乙状结肠镜检查[术]118.回肠膀胱扩大术ileum augmentation cystoplasty119.回肠膀胱尿流改道术120.回肠膀胱术121.回肠肛管吻合术ileoanal anastomosis 122.回肠横结肠吻合术123.回肠憩室124.回肠造口术125.回盲部结核ileocecal tuberculos126.直肠膀胱一结肠腹壁造口术rectal bladder and abdominal colostomy 127.直肠固定术proctopexy,128.直肠后脓肿129.直肠后拖也吻合巨结肠根治术duhamel 130.直肠环钳吻合术ring clamp anastomosis of rectum131.直肠肌鞘拖出吻合巨结肠根治术132直肠镜检查[术]133.直肠瘘134.直肠膨出135.直肠切除术136.直肠烧灼137.直肠损伤138.直肠脱垂139.直肠狭窄140,直肠炎141.直肠乙状结肠镜检查[术]p142.直肠阴道瘘143.直肠指检144.直肠周围脓肿145.直视下活检[术]145.肛管癌146.肛裂anal fissure,147.肛门闭锁会阴瘘148.肛门闭锁尿道瘘anal atresia149.肛门闭锁前庭瘘150.肛门闭锁阴道瘘151.肛门镜152.肛门镜检查[术]153.肛门溃疡154.肛门瘙痒[症]155.肛门狭窄an156.肛门直肠瘘157.肛门直肠脓肿158.肛乳头炎anal papillitis 159.肛周脓肿,160.肝脏liver 161肝癌liver cancer 162.阑尾Appendicitis, 163.肝性脑病Hepatic encephalopathy 164.肝昏迷hepatic coma165.原发性肝癌primary carcinoma of the liver.166.病毒性肝炎virus hepatitis 167.传染性肝炎infectious hepatitis 168.急性病毒性肝炎acute viral hepatitis 169.慢性腹泻chronic diarrhea 170.酒精性肝病alcoholic lier171.自身免疫性肝炎autoimmune hepatitis 172.肝硬化cirrhosis of lier 173.腹膜炎Peritonitis, 174.干呕175.肝[性]昏迷前期176.肝被膜下出血subcapsular177.肝病性口臭178.肝肠联合移植combined liver and intestin179.肝大180肝淀粉样变性181.肝动脉造影[术]182.肝梗死183.肝结核184.肝静脉梗阻185.肝慢性阻性充血chronic passiveconge186.肝毛细线虫病capillariasis hepatica187.肝门肠吻合术portoenterostomy 188.肝内胆管结石189.肝内胆管结石病190.肝内胆汁淤积191.肝脓肿liver absces 192.肝脾大hepatosp193.肝片吸虫病194.肝肾联合移植combined liver and kidney195.肝肾综合征196.肝素辅因子heparin co-197.肝细胞移植198.肝下垂hepatoptosis 199.上消化道出血upper gastrointestinal hemorrhage200.壁细胞parietal cell 201.质子泵proton pump 202, 痔疮Hemorrhoids203.gall bladder 胆囊.pancreas 胰腺204.内镜逆行胰胆管造影endoscopic retrograde cholangiopancreatography ,ERCP 205.胆石症/胆囊炎Cholelithiasis/Cholecystitis 206.急性胰腺炎Acute Pancreatitis, 207.胰腺癌carcinoma of the Pancreatitis208.胰空肠吻合术pancreaticojejunostomy 209.胰瘘pancreatic fistula210.胰肾联合移植combined pancreas and renal transplantation211.胰十二指肠切除术pancreaticoduodenectomy212.胰十二指肠移植术pancreas-duodenal transplantation213.胰石pancreatolith,pancreatic calculus214.胰石病pancreatolithiasis215.胰腺创伤pancreatic trauma216.胰腺分裂pancreas divisum217.胰腺钙化calcification of pancreas218.胰腺假囊肿 pancreatic pseudocyst 219.胰腺囊肿 pancreatic cyst220.胰腺脓肿 abscess of pancreas 221.胰腺外瘘 external fistula of pancreas 222.胰腺炎 pancreatitis 223.胰腺移植 pancreas transplantation 224.胰腺异位 heterotopic pancreas 225.胰腺周围脓肿 peripancreatic abscess 226.胰源性腹水 pancreatic ascites 227.移动性盲肠 mobile caecum 228.移植胰假性囊肿 graft pancreatic pseudocyst 229.移植胰胰瘘 graft pancreatic fistula 230.移植胰胰腺炎 graft pancreatitis 231.胆道闭锁232.胆道测压[术] 233.胆道出血234.胆道感染 235胆道梗阻236.胆道蛔虫病 237.胆道贾第虫病238.胆道减压术 decompression of biliary tra 239.胆道闪烁显像[术]240.胆道运动障碍 241.胆固醇结石242胆管癌 243.胆管测压造影[术]244.胆管肝炎 245.胆管空肠吻合术246.胆管扩张 cholangiec 247.胆管内置管扩张[术]248.胆管腺瘤 249.胆管炎250.胆管造影[术] 251.胆管周围炎252.胆红素脑病 bilirubin encephalopathy , 253.胆红素尿254.胆绞痛 biliary colic 255.胆瘘 256.胆囊癌257.胆囊肠瘘258.胆囊超声显像[术]259.胆囊穿孔 260.胆囊钙化261.胆囊积脓 262.胆囊积气 pneu-263.胆囊积水 264.胆囊积血265.胆囊镜检查[术] 266.胆囊空肠吻合术267.胆囊扭转 268.胆囊切除术269.胆囊切除术后综合征 postcholecystectomy syndrome 270,胆囊十二指肠吻合术ch 271.胆囊收缩素 272.胆囊炎273.胆囊造口术 274胆囊造影术275.胆囊周围脓肿 276.胆石性肠梗阻277.胆总管结石 calculus of common bile duct 278.胆小管炎 cholangiolitis279.胆血症 280.胆总管梗阻 281.胆汁反流性胃炎 282.胆总管端端吻合术283.胆汁浓缩综合征 284.胆汁性腹膜炎 biliary peritonitis ,285.胆汁性肝硬化 286.胆总管十二指肠吻合术choledochoduodenostomy 287.胆汁引流 288.胆汁淤积289.胆汁粘稠综合征290.[内镜]操纵部, [endoscopic ]291.[内镜]插入管, [endoscopic ]292.[内镜]充气/水阀, [endoscopic ]293.[内镜]导光连接部, [endoscopic ]light guide connector section 294.[内镜]导光束, [endoscopic ]295.[内镜]导像束, [endoscopic ]296.[内镜]光导纤维, [endoscopic ]optical fibers297.[内镜]活检管道开口, [endoscopic ]biopsy channel opening298.[内镜]角度锁钮, [endoscopic]locking299.[内镜]角度旋钮, [endoscopic]300.[内镜]冷光源, [endoscopic]cold light source301.[内镜]弯曲部, [endoscopic]302.[内镜]吸引阀, [endoscopic]---------------------------------------------------------------------------------------------------------消化学名词[内镜]操纵部, [endoscopic]control section[内镜]插入管, [endoscopic]insertion tube[内镜]充气/水阀, [endoscopic]air/water valve[内镜]导光连接部, [endoscopic]light guide connector section[内镜]导光束, [endoscopic]light guide bundles[内镜]导像束, [endoscopic]image guide bundles[内镜]光导纤维, [endoscopic]optical fibers[内镜]活检管道开口, [endoscopic]biopsy channel opening[内镜]角度锁钮, [endoscopic]locking knob[内镜]角度旋钮, [endoscopic]angulation knob[内镜]冷光源, [endoscopic]cold light source[内镜]弯曲部, [endoscopic]bending section[内镜]吸引阀, [endoscopic]suction valve阿米巴[性]肝脓肿, amebic liver abscessEhlers-Danlos综合征, Ehlers-Danlos syndrome嗳气, belch凹陷性病变, excavated lesion, depressed lesionOddi括约肌成形术, plastic repair of Oddi sphincterOddi括约肌切开术, sphincterotomy of OddiOddi括约肌狭窄, stenosis of Oddi sphincterOsler-Weber-Rendu病, Osler-Weber-Rendu diseaseBudd-Chiari综合征, Budd-Chiari syndromeBarrett's食管, Barrett's esophagus板状强直, board-like rigidity半成形便, semiformed stool半乳糖耐量, galactose tolerance伴有先天性综合征的毛细管扩张, telangiectasia associated with congenital syndrome 贝尔西食管裂孔疝修补术, Belsey hiatal hernia repair背驮式肝移植, piggyback liver transplantation贲门成形术, cardioplasty贲门肌切开术, cardiomyotomy鼻胆管引流[术], nasobiliary drainageBillroth II式吻合[术], Billroth II anastomosisBillroth I式吻合[术], Billroth I anastomosis闭袢性肠梗阻, closed loop intestinal obstruction闭塞性肝静脉内膜炎, endophlebitis hepatica obliterans壁外性压迫, extrinsic compression of wall壁细胞迷走神经切断术, parietal cell vagotomy便血, hematochezia变应性直肠炎, allergic proctitis丙型病毒性肝炎, viral hepatitis type C病毒性腹泻, viral diarrhea病毒性肝炎, viral hepatitis病毒性胃肠炎, viral gastroenteritisPeutz-Jegher's综合征, Peutz-Jegher's syndrome剥脱活检, strip biopsy博尔德莫尔食管吻合术, Beordmore anastomosis of esophagus Braun’s吻合[术], Braun anastomosis部分肠梗阻, partial intestinal obstruction擦拭法细胞学检查[术], abrasive cytologic examination残留结石, residual stone, retained stone残胃, gastric remnant藏毛病, pilonidal disease侧侧吻合[术], side-to-side anastomosis侧视内镜, side-viewing endoscope产毒性腹泻, toxigenic diarrhea肠闭锁, intestinal atresia肠壁囊样积气, pneumatosis cystoides intestinalis肠壁囊样积气[症], pneumatosis cystoides intestinalis肠侧侧吻合[术], side-to-side intestinal anastomosis肠穿孔, perforation of intestine肠道细菌内毒素移位, endotoxin translocation from intestine肠道细菌移位, bacterial translocation from intestine肠道营养, enteral nutrition肠动静脉畸形, arteriovenous malformation of bowel肠端侧吻合[术], end-to-side intestinal anastomosis肠端端吻合[术], end-to-end intestinal anastomosis肠放射性损伤, radiation injury of intestine肠梗阻, intestinal obstruction, ileus肠结核, tuberculosis of intestine肠淋巴管扩张, intestinal lymphangiectasia肠内引流式胰腺移植, enteric drainage pancreas transplantation肠囊肿, enteric cyst肠扭转, volvulus肠袢淤滞综合征, stagnant loop syndrome肠旁路术, intestinal bypass肠切除术, intestinal resection肠切开术, enterotomy肠缺血, ischemia of intestine肠缺血综合征, intestinal ischemic syndrome肠套叠, intussusception肠外瘘, enterocutaneous fistula肠外营养, parenteral nutrition肠外置术, intestinal exteriorization肠吻合[术], intestinal anastomosis肠紊乱, bowel disturbance肠系膜动脉闭塞, mesenteric arterial occlusion肠系膜动脉栓塞术, mesenteric artery embolization肠系膜动脉血栓形成, mesenteric artery thrombosis肠系膜静脉血栓形成, mesenteric venous thrombosis肠系膜囊肿, mesenteric cyst肠系膜疝, mesenteric hernia肠系膜上动脉综合征, superior mesenteric artery syndrome肠系膜上动脉压迫综合征, superior mesenteric artery compression syndrome 肠狭窄, intestinal stenosis肠旋转不良, malrotation of intestine肠血管病, vascular disease of bowel肠血管发育异常, angiodysplasia of bowel肠血管异常, vascular abnormality of intestine肠易激综合征, irritable bowel syndrome肠源性感染, enterogenic infection肠造口术, enterostomy肠胀气, intestinal tympanites肠重复畸形, duplication of intestine肠子宫内膜异位, endometriosis in bowel超声腹腔镜, ultrasonic laparoscope超声内镜, ultrasonic endoscope成形便, formed stool冲洗法细胞学检查[术], lavage cytologic examination虫蚀样边缘, eroded edge出血性胃炎, hemorrhagic gastritis出血性胰腺炎, hemorrhagic pancreatitis穿孔, perforation穿孔性阑尾炎, perforating appendicitis穿透, penetration穿透性溃疡, penetrating ulcer大便失禁, fecal incontinence大肠梗阻, large bowel obstruction, colonic obstruction大网膜及肠系膜囊肿, omental cyst and mesenteric cyst单纯性集群性憩室病, simple massed diverticulosis单极电凝[术], monopolar electrocoagulation胆[结]石, gallstone胆道闭锁, biliary atresia胆道测压[术], manometry of biliary tract胆道出血, hemobilia胆道感染, infection of biliary tract胆道梗阻, obstruction of biliary tract胆道蛔虫病, biliary ascariasis胆道贾第虫病, giardiasis of biliary tract胆道减压术, decompression of biliary tract胆道闪烁显像[术], cholescintigraphy胆道运动障碍, biliary dyskinesia胆固醇结石, cholesterol calculus胆管癌, carcinoma of bile duct胆管测压造影[术], manometric cholangiography胆管肝炎, cholangiohepatitis胆管空肠吻合术, cholangiojejunostomy胆管扩张, cholangiectasis胆管内置管扩张[术], biliary stent dilatation胆管腺瘤, cholangioadenoma胆管炎, cholangitis胆管造影[术], cholangiography胆管周围炎, pericholangitis胆红素脑病, bilirubin encephalopathy, kernicterus胆红素尿, bilirubinuria胆绞痛, biliary colic胆瘘, biliary fistula胆囊癌, carcinoma of gallbladder胆囊肠瘘, cholecystoenteric fistula胆囊超声显像[术], cholecystosonography胆囊穿孔, perforation of gallbladder胆囊钙化, calcification of gallbladder胆囊积脓, empyema of gallbladder胆囊积气, pneu-gallbladder胆囊积水, hydrops of gallbladder胆囊积血, hemocholecyst胆囊镜检查[术], cholecystoscopy胆囊空肠吻合术, cholecystojejunostomy胆囊扭转, torsion of gallbladder胆囊切除术, cholecystectomy胆囊切除术后综合征, postcholecystectomy syndrome胆囊十二指肠吻合术, cholecystoduodenostomy胆囊收缩素, cholecystokinin胆囊炎, cholecystitis胆囊造口术, cholecystostomy胆囊造影术, cholecystography胆囊周围脓肿, pericholecystic abscess胆石性肠梗阻, gallstone ileus胆石症, cholelithiasis胆小管炎, cholangiolitis胆血症, cholemia胆胰管汇合异常, choledochopancreatic junction anomaly胆汁反流性胃炎, bile reflux gastritis胆汁尿, choleuria, choluria胆汁浓缩综合征, inspissated bile syndrome胆汁性腹膜炎, biliary peritonitis, choleperitoneum胆汁性肝硬化, biliary cirrhosis胆汁胸, cholothorax胆汁引流, biliary drainage胆汁淤积, cholestasis胆汁粘稠综合征, biliary hyperviscosity syndrome胆总管端端吻合术, choledochocholedochostomy胆总管梗阻, obstruction of common bile duct胆总管结石, calculus of common bile duct, choledocholith胆总管结石病, choledocholithiasis胆总管空肠Roux-en-Y形吻合术, choledochojejunostomy Roux-en-Y胆总管扩张, choledochectasia胆总管囊肿, choledochal cyst胆总管囊肿切除术, choledochocystectomy胆总管切开术, choledochotomy胆总管十二指肠吻合术, choledochoduodenostomy胆总管狭窄, stricture of common bile duct胆总管炎, choledochitis胆总管造口术, choledochostomy弹性假黄色瘤, pseudoxanthoma elasticum蛋白丢失性肠病, protein-losing enteropathyDevine结肠造口术, Devine colostomy电子内镜检查[术], electronic endoscopy, videoendoscopy淀粉酶-肌酸酐清除率之比, amylase-creatinine clearance ratio淀粉酶清除率, clearance of amylase丁型病毒性肝炎, viral hepatitis type D,delta hepatitis动脉胆道瘘, arteriobiliary fistula痘疮样胃炎, gastritis varioliformisDubin-Johnson综合征, Dubin-Johnson syndrome端侧吻合[术], end-to-side anastomosis端端吻合[术], end-to-end anastomosis端式结肠造口术, terminal colostomy短肠, short gut短肠综合征, short-bowel syndrone多发性静脉扩张, multiple phlebectasia,多极电凝[术], multipolar electrocoagulation多囊肝, polycystic liver二期小肠移植, two-stage intestine transplantation翻出型肛门外吻合巨结肠根治术, Swenson procedure翻转法内镜检查[术], reverse method of endoscopy反流性食管炎, reflux esophagitis反跳痛, rebound tenderness反胃, regurgitation放大腹腔镜检查[术], magnifying laparoscopy放大内镜检查[术], magnifying endoscopy放射性结肠炎, radiation colitis放射性小肠炎, radiation enteritis非闭塞性肠梗死, nonocclusive intestinal infarction肥厚性胃炎, hypertrophic gastritis肥厚性幽门狭窄, hypertrophic pylorostenosis肥皂性结肠炎, soap colitis粪便嵌塞, fecal impaction粪瘘, fecal fistula蜂窝织炎性阑尾炎, phlegmonous appendicitis蜂窝织炎性胃炎, phlegmonous gastritis缝线肉芽肿, suture granuloma弗纳-莫里森综合征, Verner-Morrison syndrome辅助性肝移植, auxiliary liver transplantation腐蚀性食管狭窄, caustic stricture of esophagus腐蚀性胃炎, corrosivegastritis复发性胆总管结石病, recurrent choledocholithiasis复发性溃疡, recurrent ulcer复发性阑尾炎, recurrent appendicitis复合性胃和十二指肠溃疡, combined gastric and duodenal ulcers腹部结核, abdominal tuberculosis腹鸣, borborygmus腹膜刺激征, peritoneal irritation sign腹膜炎, peritonitis腹膜粘连, peritoneal adhesion腹腔穿刺[术], peritoneocentesis, abdominal paracentesis腹腔动脉压迫综合征, celiac artery compression syndrome腹腔灌洗, peritoneal lavage腹腔积血, hemoperitoneum腹腔镜胆囊切除[术], laparoscopic cholecystectomy腹腔镜检查[术], laparoscopy腹腔镜治疗[术], therapeutic laparoscopy腹腔内引流式胰腺移植, free-drainage intraperitoneal pancreas transplantation腹腔脓肿, peritoneal abscess腹水, ascites腹主动脉瘤, abdominal aortic aneurysm改良的黑勒贲门肌切开术, modified Heller operation钙乳胆汁, milk of calcium bile干呕, retch肝[性]昏迷, hepatic coma肝[性]昏迷前期, hepatic precoma肝被膜下出血, subcapsular hemorrhage of liver肝病性口臭, fetor hepaticus肝肠联合移植, combined liver and intestine transplantation肝大, hepatomegaly肝淀粉样变性, amyloidosis of liver肝动脉造影[术], hepatic arteriography肝梗死, infarction of liver肝结核, tuberculosis of liver肝静脉梗阻, hepatic venous obstruction肝慢性阻性充血, chronic passive congestion of liver肝毛细线虫病, capillariasis hepatica肝门肠吻合术, portoenterostomy, Kasai procedure肝内胆管结石, calculus of intrahepatic duct肝内胆管结石病, hepatolithiasis肝内胆汁淤积, intrahepatic cholestasis肝脓肿, liver abscess肝脾大, hepatosplenomegaly肝片吸虫病, fascioliasis hepatica肝肾联合移植, combined liver and kidney transplantation肝肾综合征, hepatorenal syndrome肝素辅因子, heparin co-factor肝素化, heparinization肝素化逆转, heparinization reversal肝细胞移植, hepatocyte transplantation肝下垂, hepatoptosis肝纤维化, hepatic fibrosis肝心联合移植, combined liver and heart transplantation肝性昏迷, hepatic coma肝性脑病, hepatic encephalopathy肝炎后肝硬化, posthepatitic cirrhosis肝胰联合移植, combined liver and pancreas transplantation肝移植, liver transplantation肝硬化, cirrhosis of liver肝周炎, perihepatitis感染性腹泻, infectious diarrhea感染性胃炎, infectious gastritis肛管癌, cancer of anal canal肛裂, anal fissure,肛门闭锁会阴瘘, anal atresia with perineal fistula肛门闭锁尿道瘘, anal atresia with urethral fistula肛门闭锁前庭瘘, anal atresia with vestibular fistula肛门闭锁阴道瘘, anal atresia with vaginal fistula肛门镜, anoscope肛门镜检查[术], anoscopy肛门溃疡, anal ulcer肛门瘙痒[症], pruritus ani肛门狭窄, anal stenosis肛门直肠瘘, anorectal fistula肛门直肠脓肿, anorectal abscess肛乳头炎, anal papillitis肛周脓肿, perianal abscess高胆红素血[症], hyperbilirubinemia高淀粉酶血[症], hyperamylasemia高峰酸排出量, peak acid outputGrey Turner征, Grey Turner sign膈膨升, eventration of diaphragm膈疝, diaphragmatic hernia膈下脓肿, subphrenic abscess梗阻性阑尾炎, obstructive appendicitis孤立性非特异性溃疡, isolated nonspecific ulcer骨盆直肠窝脓肿, pelvirectal abscess管探查[术], exploration of common bile duct光动力学治疗[术], photodynamic therapy光凝固[术], photocoagulation果糖不耐受[症], fructose intolerance黑粪, melena黑勒贲门肌切开术, heller operation,横结肠造口术, transverse colostomy呼气试验breath test糊状便, mushy stool滑动性食管裂孔疝, sliding hiatus hernia滑管, sliding tube化脓性腹膜炎, purulent peritonitis化脓性阑尾炎, suppurative appendicitis化脓性胰腺炎, purulent pancreatitis化生性息肉, metaplastic polyp化学性腹膜炎, chemical peritonitis坏疽性胆囊炎, gangrenous cholecystitis坏疽性阑尾炎, gangrenous appendicitis坏死后肝硬化, postnecrotic cirrhosis坏死性胰腺炎, necrotizing pancreatitis环状胰腺, annular pancreas黄疸, jaundice, icterus黄色肉芽肿性胆囊炎, xanthogranulomatous cholecystitis磺溴酞钠试验, bromsulphalein test回肠膀胱扩大术, ileum augmentation cystoplasty, ileocystoplasty回肠膀胱尿流改道术, ileal conduit diversion回肠膀胱术, ileal conduit, Bricker operation回肠肛管吻合术, ileoanal anastomosis回肠横结肠吻合术, ileotransversostomy回肠憩室, ileal diverticulum回肠造口术, ileostomy回盲部结核, ileocecal tuberculosisWhipple病, Whipple disease混合性结石, mixed stone, mixed calculus混合性毛细血管-海绵状血管瘤, mixed capillary-cavernous hemangioma活动性肝炎, active hepatitis活体部分肝移植, partial living liver transplantation获得性巨结肠, acquired megacolon机械性肠梗阻, mechanical intestinal obstruction, mechanical ileus基础酸排出量, basal acid outputKillian憩室, Killian diverticulum激光治疗[术], laser therapy急腹症, acute abdomen急性肠系膜淋巴结炎, acute mesenteric lymphadenitis急性出血性胰腺炎, acute hemorrhagic pancreatitis急性腐蚀性食管炎, acute corrosive esophagitis急性肝[功能]衰竭, acute hepatic failure急性梗阻性化脓性胆管炎, acute obstructive suppurative cholangitis急性坏死性胰腺炎, acute necrotizing pancreatitis急性间质性胰腺炎, acute interstitial pancreatitis急性卡他性阑尾炎, acute catarrhal appendicitis急性弥漫性腹膜炎, acute diffuse peritonitis,急性水肿性胰腺炎, acute edematous pancreatitis急性胃扩张, acute dilatation of stomach急性胃扩张, acute gastric dilatation急性应激性溃疡, acute stress ulcer急性重型肝炎, acute severe hepatitis, fulminant hepatitis急诊肝移植, emergency liver transplantation继发性巨结肠, secondary megacolon寄生虫性腹泻, parasitic diarrheaGardner综合征, Gardner syndrome家族性肠息肉病, familial intestinal polyposis家族性结肠息肉病, familial polyposis coli甲胎蛋白测定, alpha-fetoprotein detemination甲型病毒性肝炎, viral hepatitis type A假膜性结肠炎, pseudomembranous colitis假膜性小肠结肠炎, pseudomembranous enterocolitis假憩室, pseudodiverticulum假息肉, pseudopolyp假性感染性直肠炎, pseudoinfectious proctitis假性结肠梗阻, false colonic obstruction, Ogilvie syndrome减体积肝移植, reduced-size liver transplantation碱性反流性胃炎, alkaline reflux gastritis浆液性腹膜炎, serous peritonitis胶原性结肠炎, collagenous colitis绞窄性肠梗阻, strangulated intestinal obstruction节段小肠移植, segmental small intestine transplantation节段性肠扩张, segmental dilatation of intestine节段胰腺移植, segmental pancreas transplantation结肠癌, cancer of colon结肠癌Dukes分类法, Dukes classification for colon cancer结肠膀胱瘘, colovesical fistula结肠穿孔, colonic perforation结肠次全切除术, subtotal colectomy结肠非特异性溃疡, nonspecific ulcer of colon结肠孤立性溃疡, colonic solitary ulcer结肠黑色素沉着病, melanosis coli结肠后胃空肠吻合术, retrocolic gastrojejunostomy结肠回肠侧吻合术, Martin procedure结肠结核, tuberculosis of colon结肠镜检查[术], colonoscopy结肠憩室病, diverticular disease of colon结肠前胃空肠吻合术, antecolic gastrojejunostomy结肠切除术, colectomy结肠切开术, colotomy结肠缺血, colonic ischemia结肠息肉, polyp of colon结肠息肉病, polyposis coli结肠腺瘤, adenoma of colon结肠造口术, colostomy结肠直肠切除术, coloproctectomy结核性腹膜炎, tuberculous peritonitis结石性胰腺炎, calcareus pancreatitis近侧胃迷走神经切断术, proximal gastric vagotomy经腹骶直肠切除术, abdominosacral resection, anterior resection经颈静脉胆管造影[术], transjugular cholangiography经口胆管镜检查[术], peroral cholangioscopy经皮经肝胆管镜检查[术], percutaneous transhepatic cholangioscopy 经皮经肝胆管造影[术], percutaneous transhepatic cholangiography经皮经肝胆囊镜检查[术], percutaneous transhepatic cholecystoscopy经皮经肝栓塞, percutaneous transhepatic embolization经皮内镜胃造瘘[术], percutaneous endoscopic gastrostomy经直肠活检, transrectal biopsy精神性便秘, psychogenic constipation颈部食管胃吻合术, cervical esophagogastrostomy痉挛性肠梗阻, spastic intestinal obstruction痉挛性肛部痛, proctalgia fugax痉挛性结肠憩室病, spastic colon diverticulosis静脉闭塞性病, veno-occlusive disease静脉胆管造影[术], intravenous cholangiography静脉胆囊造影[术], intravenous cholecystography静脉切开术, venesection, phlebotomy静脉曲张, varicosis, varix静脉曲张性溃疡, varicose ulcer静脉造影[术], phlebography酒精性肝炎, alcoholic hepatitis酒精性肝硬化, alcoholic cirrhosis酒精性胰腺炎, alcoholic pancreatitis局限性肠炎, regional enteritis, Crohn disease局限性腹膜炎, localized peritonitis巨大肥厚性胃炎, giant hypertrophy gastritis巨大皱襞, giant folds, giant ruga巨结肠, megacolon巨十二指肠, megaduodenum菌群失调性肠炎, flora imbalance enteritisCullen征, Cullen signCanada-Cronkhite综合征, Canada-Cronkhite syndrome可控性回肠膀胱术, continent ileal reservoirCrigler-Najjar综合征, Crigler-Najjar syndromeCruveilhier-Baumgarten综合征, Cruveilhier-Baumgarten syndrome克罗恩病, Crohn’s disease空肠回肠旁路术, jejunoileal bypass空肠间置代胆道术, choledochoplasty by jejunal interposition空肠移植, jejunum transplantation空肠造口术, jejunostomy口服胆囊造影[术], oral cholecystographyCourvoisier征, Courvoisier sign溃疡性结肠炎, ulcerative colitis拉埃内克肝硬化, Laennec’s cirrhosis阑尾残端, appendiceal stump阑尾粪石, appendiceal fecalith阑尾切除术, appendectomy阑尾炎, appendicitis阑尾粘液囊肿, appendiceal mucocele阑尾周围脓肿, periappendiceal abscess类癌, carcinoid类癌综合征, carcinoid syndrome里急后重, tenesmus隆起性病变, protrusion lesion鲁氏Y形吻合[术], Roux-en-Y anastomosisRotor综合征, Rotor syndrome麻痹性肠梗阻, paralytic ileusMallory-Weiss综合征, Mallory-Weiss syndrome慢性非化浓性破坏性胆管炎, chronic nonsuppurative destructive cholangitis 慢性溃疡性结肠炎, chronic ulcerative colitis慢性重型肝炎, chronic severe hepatitis盲肠膀胱扩大术, cecum augmentation cystoplasty盲肠后位阑尾, retrocecal appendix盲肠炎, typhlitis, cecitis盲肠造口术, cecostomy盲袢综合征, blind loop syndrome毛石, trichobezoar毛植物石, trichophytobezoarMeckel憩室, Meckel diverticulumMenetrier病, Menetrier disease门静脉高压, portal hypertension门静脉脓血症, portal pyemia门静脉血栓形成, thrombosis of portal vein门静脉炎, pylephlebitis门脉性肝硬化, portal cirrhosis门体脑病, portosystemic encephalopathy弥漫性腹膜炎, diffuse peritonitis弥漫性食管痉挛, diffuse spasm of esophagus迷走神经干切断术, truncal vagotomy迷走神经切断术, vagotomy糜烂性胃炎, erosive gastritis米库利兹结肠造口术, Mikulicz colostomy面团感, doughy sensationMurphy征, Murphy sign内镜, endoscope内镜超声检查[术], endoscopic ultrasonography内镜胆管引流[术], endoscopic biliary drainage内镜复位[术], endoscopic reduction内镜检查术, endoscopy内镜逆行胰胆管造影[术], endoscopic retrograde cholangio pancreatography内镜取石[术], endoscopic stone extraction technique内镜碎石[术], endoscopic lithotripsy内镜胰管引流[术], endoscopic drainage of pancreatic duct内镜粘膜下肿瘤切除[术], endoscopic enucleation of submucosal tumor内镜治疗[术], therapeutic endoscopy内镜置管[术], endoprosthesis内镜注射治疗[术], endoscopic injection therapy逆蠕动吻合[术], antiperistaltic anastomosis凝结物, concretion诺沃克组病毒性胃肠炎, norwalk agents gastroenteritis呕血, hematemesis袢式结肠造口术, loop colostomy喷射性呕吐, projectile vomiting盆腔内吻合巨结肠根治术, rehbein procedure劈裂式肝移植, split liver transplantation皮革样胃, leather bottle stomach, linitis plastica脾大, splenomegaly脾功能亢进, hypersplenism脾门静脉造影术, splenoportography脾曲综合征, splenic flexure syndrome屁, flatus胼胝性溃疡, callous ulcer, indolent ulcer平坦性病变, flat lesionPlummer-Vinson综合征, Plummer-Vinson syndrome脐肠瘘, omphalo-enteric fistula气腹, pneumoperitoneum气管食管瘘, tracheo-esophageal fistula气囊扩张器, balloon dilator气囊填塞, balloon tamponade气体扩张器, pneumatic dilator气胀, flatulence, gaseous distention气肿性胆囊炎, emphysematous cholecystitis憩室, diverticulum憩室病, diverticulosis憩室前期, prediverticular stage憩室切除术, diverticulectomy憩室炎, diverticulitis迁延性肝炎, persistent hepatitis前视内镜, forward-viewing endoscope钳夹活检[术], forceps biopsy浅表性胃炎, superficial gastritis腔静脉造影[术], venacavography桥形皱襞, bridging fold倾倒综合征, dumping syndrome球后十二指肠溃疡, postbulbar duodenal ulcer曲张静脉切除术, varicectomy圈套器, snare圈套烧灼术, snare cautery全部吸收不良, panmalabsorption全结肠切除术, total colectomy全结肠炎, pancolitis全上消化道内镜检查[术], panendoscopy全小肠移植, whole small intestine transplantation全胰十二指肠切除术, total pancreaticoduodenectomy全胰腺移植, whole pancreas transplantation缺血性结肠炎, ischemic colitis热活检, hot biopsy热探头凝固[术], heater probe coagulationGillbert综合征, Gillbert syndrome肉芽肿性胃炎, granulomatous gastritis乳糜性腹膜炎, chyle peritonitis乳糖不耐受[症], lactose intolerance乳糖酶缺乏, lactase deficiency乳头括约肌切开[术], sphincterotomy, papillotomy乳头切开刀, papillotome乳头上部切开, suprapapillary incision三次肝移植, tertiary liver transplantation色素内镜检查[术], dye endoscopy, chromoendoscopy色素性结石, pigmented stone,Sengstaken-Blakemore管, Sengstaken-Blakemore tube上腔静脉梗阻, obstruction of superior vena cava上腔静脉综合症, superior vena cava syndrome失弛缓症, achalasia十二指肠闭锁, duodenal atresia十二指肠残端漏, duodenal stump leakage十二指肠梗阻, obstruction of duodenum十二指肠钩虫病, capillariasis hepatica十二指肠假憩室, pseudodiverticulum of duodenum十二指肠镜检查[术], duodenoscopy十二指肠空肠襻不全旋转, incomplete rotation of duodenojejunal loop 十二指肠溃疡, duodenal ulcer十二指肠旁疝, paraduodenal hernia十二指肠蹼, duodenal web十二指肠胃反流, duodenogastric reflux十二指肠狭窄, duodenal stenosis十二指肠炎, duodenitis食管癌, esophageal carcinoma。
与三种呼吸系统疾病关联的男性不育症

DOI:10.12280/gjszjk.20200389刘彩钊,王家雄,樊彩斌△,杨慎敏△【摘要】男性不育症是一种复杂的临床综合征,任何干扰男性生殖功能的疾病都可能导致男性不育症,这使临床实践中男性不育症病因诊断变得复杂。
呼吸系统上皮纤毛与男性精子鞭毛之间存在相似的超微解剖结构,纤毛和鞭毛功能障碍将影响呼吸道黏膜清除功能和精子运动。
另外,某些遗传缺陷也可同时导致呼吸系统和男性生殖系统的异常。
这类影响男性生育的呼吸系统疾病主要包括原发性纤毛运动障碍、囊性纤维化和Young综合征,介绍这三种疾病的主要临床特点及研究进展,并分析其呼吸系统与生殖系统临床表现之间的异同,以助于加强对这类疾病的认识。
对于严重弱精子症患者,临床医生应常规询问呼吸系统病史,对于反复呼吸道感染的患者同样应关注他们的生育问题。
【关键词】不育,男(雄)性;纤毛运动障碍;鼻窦炎;支气管扩张症;卡塔格内综合征;囊性纤维化;Young综合征Male Infertility Associated with Three Kinds of Respiratory Diseases LIU Cai-zhao,WANG Jia-xiong,FANCai-bin,YANG Shen-min.Center for Reproduction and Genetics(LIU Cai-zhao,WANG Jia-xiong,YANG Shen-min),Department of Urology(FAN Cai-bin),The Affiliated Suzhou Hospital of Nanjing Medical University,Suzhou215000,Jiangsu Province,ChinaCorresponding author:YANG Shen-min,E-mail:****************【Abstract】Male infertility is a complex clinical syndrome.Any disease that interferes with malereproductive function may lead to male infertility,which complicates the etiological diagnosis of male infertility inclinical practice.There are similar ultrastructures between the cilia of respiratory system epithelium and theflagellum of male sperm.The dysfunction of cilia and flagellum will affect the clearance function of respiratorytract mucosa and sperm movement.In addition,some of genetic defects can also lead to abnormal function ofrespiratory system and male reproductive system.Three kinds of respiratory diseases affecting male fertility wereprimary ciliary dyskinesia,cystic fibrosis and Young′s syndrome.This review introduceds the main clinicalcharacteristics of these diseases and analyzed the differences between the clinical manifestations of respiratorysystem and reproductive system,which will strengthen the understanding of these diseases.It is suggested thatclinicians should routinely inquire about the history of respiratory system for patients with severe asthenospermia,and about the reproductive problem for those patients with recurrent respiratory tract infection.【Keywords】Infertility,male;Ciliary motility disorders;Sinusitis;Bronchiectasis;Kartagener syndrome;Cystic fibrosis;Young′s syndrome(JIntReprodHealth蛐FamPlan,2021,40:126-130)·综述·基金项目:江苏省卫生健康委员会面上项目(H2018050);中华医学会生殖医学青年医师研究与发展项目(180****0756);江苏省妇幼健康资助项目(F201866)作者单位:215000江苏省苏州市,南京医科大学附属苏州医院生殖与遗传中心(刘彩钊,王家雄,杨慎敏),泌尿外科(樊彩斌)通信作者:杨慎敏,E-mail:****************△审校者不育影响着全世界大约15%的夫妇,其中男性因素约占50%。
边缘区淋巴瘤的诊断和治疗进展_________
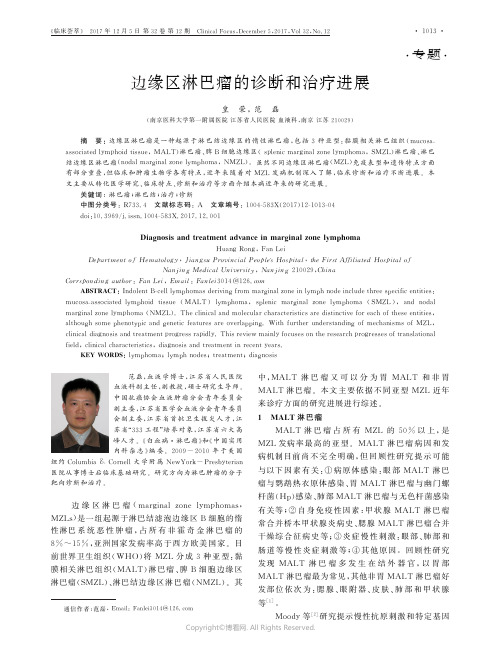
㊃专题㊃通信作者:范磊,E m a i l :F a n l e i 3014@126.c o m边缘区淋巴瘤的诊断和治疗进展皇 荣,范 磊(南京医科大学第一附属医院江苏省人民医院血液科,南京江苏210029) 摘 要:边缘区淋巴瘤是一种起源于淋巴结边缘区的惰性淋巴瘤,包括3种亚型:黏膜相关淋巴组织(m u c o s a -a s s o c i a t e d l y m p h o i d t i s s u e ,MA L T )淋巴瘤㊁脾B 细胞边缘区(s p l e n i cm a r g i n a l z o n e l y m p h o m a ,S M Z L )淋巴瘤㊁淋巴结边缘区淋巴瘤(n o d a lm a r g i n a l z o n e l y m p h o m a ,NM Z L )㊂虽然不同边缘区淋巴瘤(M Z L )免疫表型和遗传特点方面有部分重叠,但临床和肿瘤生物学各有特点,近年来随着对M Z L 发病机制深入了解,临床诊断和治疗不断进展㊂本文主要从转化医学研究㊁临床特点㊁诊断和治疗等方面介绍本病近年来的研究进展㊂关键词:淋巴瘤;淋巴结;治疗;诊断中图分类号:R 733.4 文献标志码:A 文章编号:1004-583X (2017)12-1013-04d o i :10.3969/j.i s s n .1004-583X.2017.12.001D i a g n o s i s a n d t r e a t m e n t a d v a n c e i nm a r g i n a l z o n e l y m ph o m a H u a n g R o n g,F a nL e i D e p a r t m e n t o f H e m a t o l o g y ,J i a n g s uP r o v i n c i a lP e o p l e 'sH o s p i t a l ,t h eF i r s tA f f i l i a t e d H o s p i t a l o fN a n j i n g M e d i c a lU n i v e r s i t y ,N a n j i n g 210029,C h i n a C o r r s p o n d i n g au t h o r :F a nL e i ,E m a i l :F a n l e i 3014@126.c o m A B S T R A C T :I n d o l e n tB -c e l l l y m p h o m a s d e r i v i n g f r o m m a r g i n a l z o n e i n l y m p hn o d e i n c l u d e t h r e e s pe c if i c e n t i t i e s :m u c o s a -a s s o c i a t e dl y m p h o i dt i s s u e (MA L T )l y m p h o m a ,s p l e n i c m a r g i n a lz o n el y m p h o m a (S M Z L ),a n d n o d a l m a r g i n a l z o n e l y m ph o m a (NM Z L ).T h e c l i n i c a l a n dm o l e c u l a r c h a r a c t e r i s t i c s a r e d i s t i n c t i v e f o r e a c ho f t h e s e e n t i t i e s ,a l t h o u g hs o m e p h e n o t y p i c a n d g e n e t i c f e a t u r e sa r eo v e r l a p p i n g .W i t hf u r t h e ru n d e r s t a n d i n g ofm e c h a n i s m so fM Z L ,c l i n i c a l d i a g n o s i s a n d t r e a t m e n t p r o g r e s s r a p i d l y .T h i s r e v i e w m a i n l y f o c u s e s o n t h e r e s e a r c h p r o gr e s s e s o f t r a n s l a t i o n a l f i e l d ,c l i n i c a l c h a r a c t e r i s t i c s ,d i a gn o s i s a n d t r e a t m e n t i n r e c e n t y e a r s .K E Y W O R D S :l y m p h o m a ;l y m p hn o d e s ;t r e a t m e n t ;d i a gn o s is 范磊,血液学博士,江苏省人民医院血液科副主任,副教授,硕士研究生导师㊂中国抗癌协会血液肿瘤分会青年委员会副主委,江苏省医学会血液分会青年委员会副主委,江苏省首批卫生拔尖人才,江苏省 333工程 培养对象,江苏省六大高峰人才㊂‘白血病㊃淋巴瘤“和‘中国实用内科杂志“编委㊂2009-2010年于美国纽约C o l u m b i a&C o r n e l l 大学附属N e w Y o r k -P r e s b yt e r i a n 医院从事博士后临床基础研究㊂研究方向为淋巴肿瘤的分子靶向诊断和治疗㊂边缘区淋巴瘤(m a r g i n a lz o n el y m ph o m a s ,M Z L s )是一组起源于淋巴结滤泡边缘区B 细胞的惰性淋巴系统恶性肿瘤,占所有非霍奇金淋巴瘤的8%~15%,亚洲国家发病率高于西方欧美国家㊂目前世界卫生组织(WHO )将M Z L 分成3种亚型:黏膜相关淋巴组织(MA L T )淋巴瘤㊁脾B 细胞边缘区淋巴瘤(S M Z L )㊁淋巴结边缘区淋巴瘤(NM Z L )㊂其中,MA L T 淋巴瘤又可以分为胃MA L T 和非胃MA L T 淋巴瘤㊂本文主要依据不同亚型M Z L 近年来诊疗方面的研究进展进行综述㊂1 M A L T 淋巴瘤MA L T 淋巴瘤占所有M Z L 的50%以上,是M Z L 发病率最高的亚型㊂MA L T 淋巴瘤病因和发病机制目前尚不完全明确,但回顾性研究提示可能与以下因素有关:①病原体感染:眼部MA L T 淋巴瘤与鹦鹉热衣原体感染㊁胃MA L T 淋巴瘤与幽门螺杆菌(H p )感染㊁肺部MA L T 淋巴瘤与无色杆菌感染有关等;②自身免疫性因素:甲状腺MA L T 淋巴瘤常合并桥本甲状腺炎病史㊁腮腺MA L T 淋巴瘤合并干燥综合征病史等;③炎症慢性刺激:眼部㊁肺部和肠道等慢性炎症刺激等;④其他原因㊂回顾性研究发现MA L T 淋巴瘤多发生在结外器官,以胃部MA L T 淋巴瘤最为常见,其他非胃MA L T 淋巴瘤好发部位依次为:腮腺㊁眼附器㊁皮肤㊁肺部和甲状腺等[1]㊂M o o d y 等[2]研究提示慢性抗原刺激和特定基因㊃3101㊃‘临床荟萃“ 2017年12月5日第32卷第12期 C l i n i c a l F o c u s ,D e c e m b e r 5,2017,V o l 32,N o .12Copyright ©博看网. All Rights Reserved.突变在MA L T淋巴瘤发生中均发挥重要作用,但是其中任何单一因素都不足以导致疾病恶变的发生, MA L T淋巴瘤的发生发展很大程度上依赖于两者之间的相互促进作用㊂该研究回顾性检测了179例不同部位MA L T淋巴瘤患者的免疫球蛋白重链可变区(I G H V)使用与17种基因突变,结果发现眼附属器MA L T淋巴瘤中I G H V4-34与T N F A I P3基因失活性突变(编码N F-κB通路负调控因子)之间存在重要联系;腮腺MA L T淋巴瘤I G H V1-69使用明显增多(54%),但与所研究的17种基因突变均无相关性;MA L T淋巴瘤缺乏其他以N F-κB为中心的B细胞淋巴瘤的典型表型,例如C D79B,C A R D11, MY D88,T N F R S F11A和T R A F3突变㊂由于突变或缺失导致的T N F A I P3失活在携带I G H V4-34使用[7/13(53.5%)]的MA L T淋巴瘤患者尤其是眼附属器MA L T(O AM L)淋巴瘤患者中发生率(70%)更高[2],本研究一定程度揭示抗原刺激和基因突变在MA L T淋巴瘤疾病发生发展中的作用,并且不同部位MA L T淋巴瘤I G H V使用偏向不同提示可能与接受不同抗原刺激所致㊂对于MA L T淋巴瘤预后分层,由于疾病异质性较大,以往多无统一危险度积分系统,T h i e b l e m o n t 等[3]通过对I E L S G-19临床试验中401例不同部位MA L T淋巴瘤患者临床资料分析发现:晚期病变(Ⅲ~Ⅳ期)㊁高龄(>70岁)和乳酸脱氧酶(L D H)升高是MA L T淋巴瘤预后独立不良因素,据此3个参数将MA L T淋巴瘤患者分为3个危险度分层(MA L T-I P I):低危组0分㊁中危组1分和高危组ȡ2分,对应的5年无事件生存(E F S)在3组间分别为70%,56%和29%,本研究进一步在633例MA L T 淋巴瘤患者中进行验证,证实此模型的有效性㊂治疗方面,由于MA L T淋巴瘤发生于结外部位,疾病容易早期发现,临床诊断时大多为早期局限性病变,因此临床多采用以手术㊁放疗为主的局部治疗为主,只是对于少数晚期患者会采用系统性治疗㊂1.1胃MA L T淋巴瘤目前已有多项研究表明胃部MA L T淋巴瘤和H p感染密切相关,利用不同的检测方法大部分胃MA L T淋巴瘤患者可以检测出H p㊂目前临床检测H p感染的方法有局部组织培养㊁聚合酶链反应(P C R)㊁血清学检测㊁粪便抗原检测㊁C13呼气法,快速尿素酶检测法等,其中局部组织培养和C13呼气法是较为常用的方法㊂由于胃部MA L T淋巴瘤较高的H p感染率,因此目前使用积极的多药联合清除H p感染是早期胃MA L T患者主要的治疗方法[4]㊂一般而言,对于初诊胃MA L T淋巴瘤患者经过全面评估确诊为早期病变(I E或I I E)并且H p感染阳性患者,大多建议使用四药联合(质子泵抑制剂㊁阿莫西林㊁克林霉素和胶体果胶铋)的方案两周清除H p感染,其后每3个月复查胃镜和H p感染,如果H p感染仍然为阳性可以考虑二线抗H p治疗,而对于胃局部MA L T淋巴瘤,如果疾病好转或者稳定都可以继续随访,通过单纯抗H p治疗,超过80%患者可以持续缓解甚至疾病治愈,但是对于随访超过1年仍然有肿瘤组织残留的患者,可以考虑采用二线治疗清除残留肿瘤组织,目前认为针对胃部的局部放疗或者采用利妥昔单抗单药治疗是较为有效的方法,对于抗H p无效或者H p感染阴性患者完全缓解率可以达到46%~80%,5年疾病特异性生存达到93%,并且治疗相关不良反应较小[5]㊂虽然大部分早期H p感染阳性的胃MA L T淋巴瘤患者对于抗H p治疗反应较好,但是仍然有10%~ 20%的患者会出现抗H p治疗耐药,目前认为晚期病变㊁组织学存在大细胞转化成分㊁近端胃位置㊁胃镜下非浅表和深层浸润以及存在t(11;18)/A P I2-MA L T1易位的患者可能出现对于抗H p治疗反应不佳,此类患者需要密切观察和随访病情,必要时及时更换治疗方案[6]㊂对于初诊时H p感染阴性的早期胃MA L T淋巴瘤患者建议直接采用局部放疗,如果不适合采用放疗的患者可以考虑利妥昔单抗单药治疗也可以获得不错的疗效㊂对于晚期的胃部MA L T淋巴瘤患者,由于伴有身体其他部位的累及,因此多建议采用利妥昔单抗联合化疗的全身系统性治疗㊂1.2眼附属器MA L T淋巴瘤(O AM L)原发眼部淋巴瘤是一种罕见的淋巴瘤亚型,病理类型多样,其中MA L T淋巴瘤大约占所有眼部淋巴瘤的54%,女性发病率高于男性,O AM L一般病灶仅局限于眼附属器官(眼睑㊁结膜㊁泪器㊁眼外肌和眼眶等),大多数O AM L起病时为单侧眼附器发病,但仍有38%患者诊断时发现多发病灶㊂该病发病机制一般认为与长期暴露于特定病原体(鹦鹉热衣原体)㊁药物㊁慢性抗原刺激及免疫失调有关,局部淋巴组织从反应性淋巴样增生逐步发展为克隆性淋巴系统肿瘤㊂O AM L 临床特征性表现为泪腺㊁眼眶㊁结膜肿块或明显的眼睑肿块㊁眼球突出㊁疼痛或复视,或无症状㊂典型的结膜病损表现为鲑鱼肉样或粉红肉样外观,也可出现鼻泪管引流系统的累及㊂预后因素方面年龄大于65岁㊁非I期病变㊁L D H升高和骨髓活检阳性认为是O AM L的预后不良因素㊂治疗方面,由于O AM L发病率低,因此国际和㊃4101㊃‘临床荟萃“2017年12月5日第32卷第12期 C l i n i c a l F o c u s,D e c e m b e r5,2017,V o l32,N o.12Copyright©博看网. All Rights Reserved.国内尚无标准一线推荐方法㊂由于部分O AM L患者伴有鹦鹉热衣原体感染,因此对于病原体检测阳性患者可以考虑使用抗鹦鹉热衣原体治疗,常用的抗生素包括多西环素和其他大环内酯类药物,完全缓解(C R)率约20%,部分缓解(P R)率约为55%;鹦鹉热衣原体感染阴性的O AM L患者疾病发病位置特殊,大多数为早期病变,因此可以采用包括手术㊁放疗为主的局部治疗方法㊂采用局部放疗ʃ手术的治疗方式,95.9%的O AM L患者可以得到较好的局部疾病控制,5年的无疾病生存达到86.4%,总生存可以达到93.8%,放疗剂量多控制在30G y以内,有报道提示剂量超过30G y可以降低疾病复发,但是治疗相关不良反应随之增加,局部放疗主要的不良反应为白内障㊁干眼㊁结膜炎㊁角膜炎,令人担心的眼部失明则很少发生㊂如果是双侧发病或者累及视神经等深部组织是疾病复发的高危因素㊂1.3其余部位MA L T淋巴瘤 MA L T淋巴瘤其他多发的部位还包括皮肤㊁腮腺㊁甲状腺㊁肺部和乳腺等,如果是局部病变多采用手术㊁放疗等局部治疗方法,如果是晚期病变则建议联合全身系统性治疗控制疾病㊂2S M Z LS M Z L起源于次级淋巴滤泡边缘区的记忆B淋巴细胞,是一种少见的非霍奇金淋巴瘤(N H L),占淋系肿瘤2%㊂大约20%S M Z L患者伴发自身免疫性疾病[自身免疫性溶血性贫血(A I H A)㊁自身免疫性血小板减少性紫瘢(I T P)等]㊂本病临床表现和预后存在异质性,大多数患者中位生存时间8~10年不等,但10%~20%患者会出现大细胞转化,预后较差㊂由于形态学的相似性,以往部分S M Z L被误诊为C D5-的慢性淋巴细胞白血病(C L L)㊂本病中位发病年龄68岁,无性别差异㊂多累及脾脏(白髓)和脾门淋巴结(其他部位淋巴结受累较少),大多数S M Z L在确诊时已侵犯骨髓,约有1/3肝脏受到累及,外周淋巴结极少受累及(17%)㊂因为骨髓和肝脏的高累及率,许多患者诊断时即为Ⅳ期[7]㊂本病25%患者初诊时没有临床症状,很少伴有B症状及L D H升高㊂实验室检查方面,外周血涂片可见绒毛状淋巴细胞,25%患者存在血细胞减少,1/3患者伴有单克隆球蛋白(M蛋白,常为I g M)[8]㊂本病免疫表型没有特征性,常表达C D19㊁C D20㊁C D22㊁C D79a㊁C D79b㊁F M C7及I g M;而C D5㊁C D10㊁C D43㊁B C L6㊁c y c l i nD1以及C D103多为阴性;C D23㊁I g D 及c I g等免疫表型没有特异性㊂C L L的M a t u t e s积分多ɤ2分;C D5d i m达10%~25%,可共表达C D23或C D43,需与C L L鉴别;C D11c和C D25有时阳性,C D103和C D123几乎均阴性㊂染色体核型分析显示80%病例为复杂核型,7q-最为常见,约占30%,D e l(17p)的发生率在3%~17%㊂分子生物学方面S M Z L存在I G H V1-2使用偏向,N O T C H2和K L F2突变在疑难疾病鉴别诊断中具有一定价值,但可见于其他惰性B淋巴瘤,临床提示预后差㊂S M Z L临床表现具有异质性,这与患者的肿瘤负荷㊁体能状态有关[7]㊂脾脏病理是诊断的金标准,但是由于缺乏其他特异性的诊断指标,加之部分患者不能接受脾脏手术,因此以往S M Z L诊断方面较为困难㊂2008年M a t u t e s等[9]提出了S M Z L最低诊断标准,具体为:符合以下1项即可诊断S M Z L:①脾脏组织活检+C L L免疫表型积分ɤ2分;②典型细胞形态学表现+C L L免疫表型积分ɤ2分+C D20阳性细胞窦内浸润(如脾组织无法获得)㊂因此,目前临床怀疑S M Z L的患者,在缺乏脾脏病理的情况下,依据血液和骨髓的详细检查也可以确立S M Z L 的诊断㊂在治疗方面,意大利团队报道大约32%的S M Z L患者伴发丙型肝炎病毒(H C V)感染,并使用干扰素联合利巴韦林方案可以使得此类患者淋巴瘤可得到控制,总缓解(O R R)率和C R率分别为77%和47%,78%的患者持续病毒学缓解;中位随访时间为3.3年,中位缓解持续时间为23个月;5年无进展生存率(P F S)和总体生存率(O S)分别为78%和94%,近期另一项不含干扰素的抗H C V治疗也提示对于伴发H C V感染的S M Z L患者,单纯抗H C V治疗可以使得淋巴瘤相关治疗反应率为73%,两项研究证实H C V感染与S M Z L密切相关[10]㊂但是,本中心的回顾性研究表明中国S M Z L人群H C V发生率显著低于欧洲国家(大约3%),因此提示东西方S M Z L患者在发病病因上存在差异㊂对于H C V感染阴性的S M Z L患者,在开始治疗前需要评估治疗指征,如果不存在治疗指征可以暂时观察和随访,但是如果存在血细胞减少㊁脾脏梗死或者脾脏肿大所致的压迫症状等就需要开始治疗㊂目前对于有症状的S M Z L患者推荐的一线治疗方案是单药利妥昔单抗或者脾脏切除术,两者都有较好的近期疾病控制率,但是回顾性资料显示单药利妥昔单抗治疗的复发率低于脾脏切除,并且有资料显示,在诱导治疗后继续使用利妥昔单抗进行维持治疗将进一步降低疾病的复发[11-12]㊂同时分析发现在单药利妥昔单抗的基础上联合化疗并不能进一步增加疗效,相反治疗相关不良反应增加㊂㊃5101㊃‘临床荟萃“2017年12月5日第32卷第12期 C l i n i c a l F o c u s,D e c e m b e r5,2017,V o l32,N o.12Copyright©博看网. All Rights Reserved.3N M Z LNM Z L是成熟B细胞来源的边缘区淋巴瘤,临床大多侵犯淋巴结而结外器官累及极少,NM Z L在所有M Z L中发病率最低,大约只占10%,中位诊断年龄59岁,男女比例相当㊂患者诊断时多为晚期病变,全身广泛浅表㊁胸腹部淋巴结肿大,但多为非巨块型㊂1/3NM Z L患者骨髓受累,10%患者单克隆I g M增高,大约15%NM Z L患者会出现大细胞转化(中位时间为4.5年),预后较差㊂常见染色体异常包括+3㊁+18㊁+7㊁+12㊁6q-㊁I G H V4-34g e n e (30%)[13],近年来高通量测序提示NM Z L和S M Z L 中存在K L F2㊁P T P R D和T N F A I P3等新型分子突变,提示N K-κb㊁S T A T3等信号通路存在异常,可能和疾病的发生发展有关㊂治疗方面由于针对NM Z L设计的前瞻性临床试验较少,因此没有推荐方案,临床对于NM Z L的治疗基本参照其他惰性淋巴瘤㊂具体而言,临床治疗基本参照滤泡淋巴瘤治疗原则:首先排除少数H B V㊁H C V等病毒感染相关NM Z L外,对于早期局限性病灶推荐采用局部放疗或单药利妥昔单抗治疗;对于晚期病变患者,如果没有治疗指征可采取观望等待的策略,反之有治疗指征的NM Z L患者可以采取系统性治疗,包括联合免疫化疗等[14-15]㊂总体而言,M Z L无论在肿瘤生物学,还是在临床表现㊁诊断和治疗等方面都具有较高的异质性,不同亚型的患者采取不同的诊疗策略㊂由于M Z L属于惰性淋巴瘤,大多数患者对于一线治疗疗效较好,预后佳,生存期较长㊂对于复发难治M Z L患者可以考虑惰性淋巴瘤的二线治疗方案,近年来包括伊布替尼㊁来那度胺等新型药物也显现出令人鼓舞的临床疗效,进一步提高M Z L患者的临床预后㊂参考文献:[1] M a t u t e sE,M o n t a l b a nC.C l i n i c a l f e a t u r e s a n dm a n a g e m e n t o fn o n-g a s t r o i n t e s t i n a ln o n-o c u l a re x t r a n o d a l m u c o s aa s s o c i a t e dl y m p h o i d t i s s u e(E NMA L T)m a r g i n a l z o n el y m p h o m a s[J].B e s t P r a c tR e sC l i nH a e m a t o l,2017,30(1-2):99-108.[2] M o o d y S,E s c u d e r o-I b a r z L,W a n g M,e t a l.S i g n i f i c a n ta s s o c i a t i o nb e t w e e n T N F A I P3i n ac t i v a t i o n a nd b i a se di mm u n o g l o b u l i n h e a v y c h a i n v a r i a b l er e g i o n4-34u s a g ei nm u c o s a-a s s o c i a t e dl y m p h o i dt i s s u el y m p h o m a[J].J P a t h,2017,243(1):3-8.[3] T h i e b l e m o n tC,C a s c i o n e L,C o n c o n i A,e ta l.A MA L Tl y m p h o m a p r o g n o s t i c i n d e x g e n e r a t e d f r o mt h ed a t a s e to f t h eI E L S G-19p r o s p e c t i v e c l i n i c a l t r i a l[J].B l o o d,2017,130(12):1409-1417.[4] A n g e l oZ,C e s a r eH,L o r e n z oR,e t a l.E r a d i c a t i o nt h e r a p y i nH e l i c o b a c t e r p y l o r i-n e g a t i v e g a s t r i c l o w-g r a d e MA L Tl y m p h o m a p a t i e n t s:a s y s t e m i c r e v i e w[J].J C l i nG a s t r o e n t e r o l,2013,47(10):824.[5] V r i e l i n g C,d e J o n g D,B o o tH,e t a l.L o n g-t e r mr e s u l t so fs t o m a c h-c o n s e r v i n g t h e r a p y i n g a s t r i c MA L Tl y m p h o m a[J].R a d i o t h e rO n c o l,2008,87(3):405-411.[6] R u s k o néF o u r m e s t r a u x A,F i s c h b a c h W,A l e m a n B,e ta l.E G I L S c o n s e n s u s r e p o r t.G a s t r i c e x t r a n o d a lm a r g i n a l z o n eB-c e l l l y m p h o m a o fMA L T[J].G u t,2011,60(6):747.[7] A r c a i n i L,R o s s i D,P a u l l i M.S p l e n i c m a r g i n a l z o n el y m p h o m a:f r o m g e n e t i c st o m a n a g e m e n t[J].B l o o d,2016, 127(17):2072-2081.[8] P i r i s MA,O n a i n día A,M o l l e j o M.S p l e n i c m a r g i n a lz o n el y m p h o m a[J].B e s t P r a c t R e s C l i nH a e m a t o l,2017,30(1-2): 56-64.[9] M a t u t e sE,O s c i e rD,M o n t a l b a nC,e ta l.S p l e n i c m a r g i n a lz o n e l y m p h o m a p r o p o s a l s f o r a r e v i s i o no f d i a g n o s t i c,s t a g i n ga n d t h e r a p e u t i cc r i t e r i a[J].L e u k e m i a,2008,22(3):487-495.[10] M a h a d e v a nD,U n g e r J M,S p i e rC M,e t a l.P h a s eⅡt r i a l o fc i s p l a t i n p l u s e t o p o s ide p l u s g e m c i t a b i n e p l u s s o l u m e d r o l(P E G S)i n p e r i p h e r a lT-c e l l n o n-H o d g k i n l y m p h o m a(S WO GS0350)[J].C a n c e r,2013,119(2):371.[11] E l s eM,M a rín n i e b l aA,d e l aC r u zF,e t a l.R i t u x i m a b,u s e da l o n e o r i n c o mb i n a t i o n,i s s u p e r i o r t o o t h e r t r e a t m e n tm o d a l i t i e si n s p l e n i c m a r g i n a lz o n el y m p h o m a[J].B r JH a e m a t o l,2012,159(3):322-328.[12] K a l p a d a k i s C,P a n g a l i s G A,A n g e l o p o u l o u MK,e t a l.T r e a t m e n t o f s p l e n i cm a r g i n a l z o n e l y m p h o m aw i t hr i t u x i m a bm o n o t h e r a p y:p r o g r e s s r e p o r t a n d c o m p a r i s o n w i t hs p l e n e c t o m y[J].O n c o l o g i s t,2013,18(2):190-197. [13] A r c a i n i L,R o s s i D,P a u l l i M.S p l e n i c m a r g i n a l z o n el y m p h o m a:f r o m g e n e t i c st o m a n a g e m e n t[J].B l o o d,2016, 127(17):2072-2081.[14] T h i e b l e m o n tC,M o l i n a T,D a v iF.O p t i m i z i n g t h e r a p y f o rn o d a lm a r g i n a l z o n e l y m p h o m a[J].B l o o d,2016,127(17): 2064-2071.[15] M a k a r o v aO,O s c h l i e s I,Mül l e rS,e t a l.E x c e l l e n t o u t c o m ew i t hl i m i t e dt r e a t m e n ti n p a e d i a t r i c p a t i e n t s w i t h m a r g i n a l z o n e l y m p h o m a[J].B r JH a e m a t o l,2017A u g2[E p u ba h e a do f p r i n t]收稿日期:2017-12-08编辑:武峪峰㊃6101㊃‘临床荟萃“2017年12月5日第32卷第12期 C l i n i c a l F o c u s,D e c e m b e r5,2017,V o l32,N o.12Copyright©博看网. All Rights Reserved.。
胸腺原发黏膜相关淋巴组织淋巴瘤的ct诊断

胸腺原发黏膜相关淋巴组织淋巴瘤的CT诊断吴艳玲ꎬ张㊀伟ꎬ沈㊀杰ꎬ俞同福南京医科大学第一附属医院放射科㊀江苏㊀南京㊀210000㊀㊀ʌ摘㊀要ɔ㊀目的㊀探讨胸腺原发性黏膜相关淋巴组织淋巴瘤(MALToma)的CT表现和诊断价值ꎮ方法㊀搜集本院经病理证实的胸腺原发MALToma7例ꎮ观察胸腺MALToma的CT特征ꎬ并与6例胸腺癌及6例胸腺弥漫大B细胞淋巴瘤的CT表现进行对照ꎮ结果㊀7例MALToma患者中男性2例ꎬ女性5例ꎬ年龄<40岁者5例(5/7)ꎬ与胸腺癌(0/6)相比P<0.05)ꎬ而与弥漫大B细胞淋巴瘤(6/6)比较无统计学差异ꎻ胸腺MALToma所有病灶均呈单侧生长(7/7)ꎬ与弥漫大B细胞淋巴瘤(1/6)比较P<0.05ꎬ而与胸腺癌(5/6)比较无统计学意义ꎻ所有MALToma病灶均呈囊实性肿块(7/7)ꎬ囊变区呈小而多发ꎬ囊与囊之间分界清楚ꎬ囊壁光滑ꎬ胸腺癌囊变多呈单个大片坏死(4/6)ꎬ边缘欠清ꎬ弥漫大B细胞淋巴瘤囊变较少见(2/6ꎬP<0.05)ꎻ所有MALToma病灶均无纵隔淋巴结肿大(0/7)ꎬ胸腺癌中2例出现淋巴结肿大(2/6)ꎬ两者比较无统计学差异ꎬ而弥漫大B细胞淋巴瘤均有纵隔淋巴结肿大(6/6ꎬP<0.05)ꎻ所有MALToma病灶均未出现周围大血管侵犯(0/7)ꎬ与弥漫大B细胞淋巴瘤(5/6)比较P<0.05ꎬ而与胸腺癌(2/6)比较无统计学差异ꎮ结论㊀CT表现在胸腺原发性MALToma的诊断中具有一定价值ꎮʌ关键词ɔ㊀胸腺ꎻ黏膜相关淋巴组织淋巴瘤ꎻ体层摄影术ꎬX线计算机中图分类号:R736.3ꎻR814.42㊀㊀㊀文献标识码:A㊀㊀㊀文章编号:1006 ̄9011(2020)02 ̄0213 ̄04CTdiagnosisofprimarymucosa ̄associatedlymphoidtissuelymphomaofthymusWUYanlingꎬZHANGWeiꎬSHENJieꎬYUTongfuDepartmentofRadiologyꎬTheFirstAffiliatedHospitalofNanjingMedicalUniversityꎬNanjing210000ꎬP.R.ChinaʌAbstractɔ㊀Objective㊀ToinvestigatetheCTmanifestationsofprimarymucosa ̄associatedlymphoidtissuelymphoma(MAL ̄Toma)ofthymusandtheirdiagnosticvalue.Methods㊀7casesofprimarythymicMALTomaconfirmedbypathologywereretro ̄spectivelycollected.TheCTfeaturesofthymicMALTomawereobservedandcomparedwith6casesofthymiccarcinomaand6ca ̄sesofdiffuselargeB ̄celllymphoma.Results㊀Amongthe7MALTomapatientsꎬ2weremaleand5werefemale.5of7wereyoungerthan40yearsoldꎬforcomparisonꎬthethymiccarcinomawas0/6ꎬwhereP<0.05ꎬbuttherewasnosignificantdifferenceinagebetweenMALTomaanddiffuselargeB ̄celllymphoma(6/6).UnilateralgrowthwasobservedinallMALTomalesions(7/7)ꎬin1caseofthediffuselargeB ̄celllymphoma(1/6ꎬP<0.05)ꎬandin5casesofthymiccarcinoma(5/6ꎬP>0.05).AllMALTomalesionswerecystic ̄solidmass(7/7)ꎬwithsmallmultiplecysts.Theboundarybetweencystswasclearꎬandthecysticwallwassmooth.Thecystsin4casesofthethymiccarcinoma(4/6)weremostlysinglenecroticareawithunclearmargins.Thecysticdegenerationwasobservedin2casesofdiffuselargeB ̄celllymphoma(2/6ꎬP<0.05).Mediastinallymphnodeenlarge ̄mentwasobservedinnoneoftheMALTomalesions(0/7)ꎬin2casesofthymiccarcinoma(2/6ꎬP>0.05)andin6casesofthediffuselargeB ̄celllymphoma(6/6ꎬP<0.05)ꎻVascularinvasionwasobservedinnoneoftheMALTomalesions(0/7)ꎬin5casesofthediffuselargeB ̄celllymphoma(5/6ꎬP<0.05)ꎬandin2casesofthymiccarcinoma(2/6ꎬP>0.05).Conclu ̄sion㊀TheCTmanifestationsarevaluableinthediagnosisofprimarythymicMALToma.ʌKeywordsɔ㊀ThymusꎻMucosa ̄associatedlymphoidtissuelymphomaꎻTomographyꎬX ̄raycomputed㊀㊀淋巴结外黏膜相关淋巴组织淋巴瘤(mucosa ̄associatedlymphoidtissuelymphomaꎬMALToma)是一种低级别结外B细胞淋巴瘤ꎬ常发生于胃肠道㊁作者简介:吴艳玲(1995 ̄)ꎬ女ꎬ江苏盐城人ꎬ毕业于南京医科大学ꎬ在读硕士研究生ꎬ主要从事胸部疾病影像学诊断工作通信作者:俞同福㊀主任医师ꎬ医学博士ꎬ硕士生导师㊀E ̄mail:yu.tongfu@163.com涎腺㊁肺等器官[1 ̄2]ꎬ原发于胸腺的MALToma罕见ꎮ目前针对胸腺MALToma的影像学文献较少ꎬ对其临床及影像认识不足ꎮ本文搜集了7例经病理证实的胸腺原发MALToma病例ꎬ结合病理结果分析其CT表现特征ꎬ探讨CT征象在纵隔原发性MALToma中的诊断价值ꎮ3121㊀资料与方法1.1㊀临床资料收集本院2011年4月~2018年7月经穿刺或手术病理证实的胸腺MALTomaꎬ并排除无其他结外脏器受侵ꎬ7例患者ꎬ其中男性2例ꎬ女性5例ꎬ年龄33~45岁ꎬ平均年龄37.6岁ꎮ3例合并有自身免疫性疾病ꎬ2例为干燥综合征(其中1例同时伴发原发性胆汁肝硬化)ꎬ另1例为过敏性紫癜ꎮ以胸闷气喘就诊者2例ꎬ其余病例均因体检发现肿块而就诊ꎮ7例患者术前或经皮穿刺前均在本院行胸部CT检查ꎮ本文另搜集胸腺癌6例ꎬ男性4例ꎬ女性2例ꎬ年龄43~64岁ꎬ平均年龄54.8岁ꎮ纵隔弥漫大B细胞淋巴瘤6例ꎬ男性3例ꎬ女性3例ꎬ年龄18~35岁ꎬ平均年龄27.3岁ꎬ分别作为对照组ꎮ1.2㊀检查方法MALToma组与对照组所有患者手术或穿刺前均行CT扫描ꎮ除三组患者中各有1例仅行胸部CT平扫外ꎬ余病例均行胸部CT平扫+增强扫描ꎮ采用西门子64排螺旋CT(SomatomDefinitionꎬSie ̄mensꎬGermany)ꎻ扫描体位:仰卧位ꎻ扫描范围:胸廓入口至膈下2cm横断扫描ꎻ扫描参数及图像后处理:探测器准直宽度0.625mmꎬ螺距0.9~1.2ꎬ旋转时间0.5~1.0sꎬ管电压120kVꎬ管电流150~200mAsꎻ增强对比剂采用非离子型碘海醇(300mg/ml)ꎬ用量1.5ml/kgꎬ注射速率2.5ml/sꎮ全部病例通过纵隔窗和肺窗重建ꎬ重建层厚5mmꎮ穿刺或手术获得的标本ꎬ其病理学检查主要包括常规镜下HE切片及免疫组化ꎮ1.3㊀图像分析由2名有经验的影像诊断医师独立阅片ꎬ有分歧者ꎬ双方讨论后达成一致ꎮ图像观察:病灶形态大小㊁位置㊁密度㊁周围大血管受侵情况及纵隔淋巴结有无肿大ꎮ1.4㊀统计学方法胸腺原发MALToma患者与胸腺癌及弥漫大B细胞淋巴瘤患者的特征之间使用Fisher确切概率法进行比较ꎬP<0.05为差异有统计学意义ꎮ采用SPSS22.0统计软件分析数据ꎮ2㊀结果2.1㊀年龄比较7例MALToma患者年龄<40岁5例ꎬ胸腺癌发病年龄均>40岁ꎬ而弥漫大B细胞淋巴瘤患者年龄均<40岁ꎮ2.2㊀CT表现形态与大小:形态多不规则ꎬ4例病灶边缘呈浅分叶状ꎬ边缘尚锐利ꎮ7例MALToma病灶的最大径为4~10cmꎮ发病部位:7例MALToma病灶均位于前纵隔胸腺区ꎬ均呈单侧生长(7/7)ꎬ其中4例偏左侧生长(图1)ꎬ3例偏右侧生长ꎮ胸腺癌中5例呈单侧生长(5/6)ꎬ而弥漫大B细胞淋巴瘤多呈双侧生长(1/6)ꎬ见表1ꎮ密度:7例MALToma病灶密度均不均匀(7/7)ꎬ呈囊实性ꎬ6例瘤内有多发小囊状低密度影ꎬ小囊壁光滑ꎬ囊与囊之间分界清楚ꎬ1例囊较大ꎬ增强扫描囊壁及实性成分均可见中等程度以上的强化(图2a~2d)ꎻ胸腺癌常出现单个大片坏死(4/6)ꎬ坏死边缘多不清晰ꎮ弥漫大B细胞淋巴瘤中2例出现单个小囊变(2/6)ꎬ见表1ꎮ纵隔淋巴结及周围血管情况:所有MALToma病例均无纵隔淋巴结肿大(0/7)ꎬ胸腺癌中2例出现纵隔淋巴结肿大(2/6)ꎬ弥漫大B细胞淋巴瘤均伴有纵隔区淋巴结肿大(6/6)ꎻMALToma肿块包绕纵隔大血管0例(0/7)ꎬ少于弥漫大B细胞淋巴瘤(5/6)ꎬ胸腺癌中有2例出现血管内癌栓(2/6)ꎬ见表1ꎮ2.3㊀病理与预后6例患者经手术切除ꎬ1例行经皮穿刺活检术ꎮ标本均行常规病理+免疫组化检查ꎮ所有患者均确表1㊀胸腺MALToma与胸腺癌及弥漫大B细胞淋巴瘤的主要鉴别特征特征胸腺MALToma胸腺癌P值胸腺MALToma弥漫大B细胞淋巴瘤P值年龄<40岁5/70/60.0215/76/60.462单侧生长7/75/60.4627/71/60.005有囊变7/74/60.1927/72/60.021纵隔淋巴结肿大0/72/60.1920/76/60.001纵隔大血管侵犯0/72/60.1920/75/60.005412图1aꎬ1b㊀女ꎬ34岁ꎮCT示前纵隔偏左侧囊实性占位ꎬ肿块内多发小囊变ꎬ囊壁光滑ꎬ囊与囊之间可见分隔ꎬ增强扫描囊壁及实性成分可见强化图2㊀女ꎬ33岁ꎮ图2aCT平扫轴位:前纵隔偏右侧生长的囊实性肿块ꎬ密度欠均匀ꎬ内见大小不等的囊腔ꎬ边界尚清ꎮ图2b~2dCT增强扫描:实性成分及囊壁强化ꎬ囊性部分不强化ꎮ图2e术后病理(HEˑ40):胸腺区淋巴组织高度增生伴囊肿形成ꎮ图2f术后病理(HEˑ200):大量淋巴细胞浸润ꎬ中央为哈氏小体ꎮ图2g免疫组化(EnVisionˑ100):肿瘤细胞表达CD20ꎬ最终确诊为胸腺MALToma诊为胸腺MALTomaꎮ病理学上主要表现为胸腺区淋巴组织高度增生伴囊肿形成(图2eꎬ2f)ꎬ免疫组化示CD20等阳性(图2g)ꎮ7例患者中2例失访ꎬ余5例(肿块均经手术切除)进行了术后随访ꎬ至本课题结束时随访时间为1~6年ꎬ随访过程中均未出现复发ꎮ3㊀讨论3.1㊀临床与病理MALToma是结外非霍奇金淋巴瘤的一种ꎬ仅占B细胞淋巴瘤的7%~8%[3]ꎬ其中胃肠道MALToma约占50%ꎬ其次是肺㊁头颈部等器官ꎮ而原发于胸腺的非霍奇金恶性淋巴瘤最常见的是弥漫大B细胞淋巴瘤和T淋巴母细胞瘤ꎬ胸腺MALToma罕见ꎬ相关文献报道少ꎬ最早是1990年由Isaacson等报道的2例[4]ꎮ部分个案报道病例分析显示ꎬ胸腺MAL ̄Toma常见于亚洲人ꎬ女性多于男性ꎬ中青年多见ꎬ可能与亚洲女性好发某些自身免疫性疾病例如类风湿性关节炎㊁干燥综合征等有关[5]ꎮ本文7例胸腺MALToma患者中女性5例ꎬ年龄在33~45岁ꎬ其中3例合并有自身免疫性疾病ꎬ与文献报道相符ꎮ胸腺原发性MALToma的确诊主要依赖组织病理学与免疫组化检查ꎮ肿瘤细胞主要为中心细胞样细胞ꎬ同时伴有小淋巴细胞㊁浆细胞及转化细胞ꎮ免疫表型分析中CD20㊁Bcl ̄2通常呈弥漫强阳性[6]ꎮ在本资料的7例患者中ꎬ所有病例CD20均为阳性ꎬ6例Bcl ̄2呈阳性ꎬ1例为阴性ꎬ与文献报道[6]基本一致ꎮ3.2㊀胸腺原发MALToma的CT表现和病理基础CT作为一种重要的检查方法ꎬ可清晰显示病灶的大小㊁范围及周围侵犯情况ꎬ具有无创性ꎬ有助于诊断和治疗前的评估ꎮ本组中7例MALToma在CT512表现为前纵隔囊实性病灶ꎬ6例瘤内有多发小囊状低密度影ꎬ小囊壁光滑锐利ꎬ囊与囊之间分界清晰ꎬ1例囊较大ꎬ增强扫描囊壁及实性成分均可见中等程度以上的强化ꎬ多发小囊㊁囊与囊之间分界清晰及增强后囊壁强化这些CT表现具有一定特征性ꎬ对于明确诊断具有提示作用ꎮ既往有研究报道[7]ꎬMAL ̄Toma囊腔的形成ꎬ可能与胸腺髓质导管上皮衍化而来的结构囊性变有关ꎮ在病理学上ꎬ胸腺MALToma大体常表现为多房囊实性肿块ꎬ囊壁内衬上皮是胸腺MALToma一个普遍的组织学特征[8]ꎬ这一病理学基础与影像学表现相对应ꎮ本组资料中ꎬMAL ̄Toma均向单侧生长ꎬ提示MALToma病灶生长相对缓慢ꎬ可能与其为一种低度恶性肿瘤有关ꎮ本文中搜集的MALToma病例均无纵隔淋巴结肿大及包绕血管生长的表现ꎬ表明纵隔MALToma几乎不侵犯周围组织或血管ꎬ与文献报道[7]基本一致ꎮ3.3㊀鉴别诊断胸腺癌恶性程度高ꎬ本组6例平均年龄为54.8岁ꎬ较MALToma的发病年龄稍大ꎻ2例伴有纵隔淋巴结肿大ꎬ肿块中央部常常出现大片状坏死低密度区ꎬ边界欠清ꎬ增强后坏死边缘无明显强化ꎬ这一CT征象对于两者的鉴别诊断具有提示作用ꎬ与陆杨等[9 ̄10]报道相符ꎮ弥漫大B细胞淋巴瘤在胸腺原发淋巴瘤中发病率较高ꎬ主要表现为前纵隔密度均匀的肿块ꎬ较少出现囊变坏死ꎬ本组2例出现小囊变ꎻ病灶一般较大ꎬ向两侧生长并包绕邻近纵隔大血管(5/6)ꎬ同时所有病例均有纵隔淋巴结肿大ꎬ这与赵飞及熊淑红等[11 ̄12]的报道基本一致ꎮ胸腺MALToma病程缓慢ꎬ预后较好ꎬ手术切除是最主要的治疗方式ꎬ且术后复发少见ꎮ本组进行术后随访的5例患者均未出现复发ꎮ综上所述ꎬ本文总结了经病理证实的7例胸腺原发MALToma的临床及CT特点ꎮ该病好发于年轻女性ꎬ常合并有自身免疫性疾病ꎮ病灶在CT上多表现为前纵隔单侧生长的囊实性肿块ꎬ囊变区呈多发小囊ꎬ囊与囊分界清楚ꎬ囊壁光滑锐利ꎬ增强后囊壁及实性成分呈中等程度以上的强化ꎬ常不合并有大血管侵犯或纵隔淋巴结肿大ꎬ与胸腺癌及胸腺弥漫大B细胞淋巴瘤有所区别ꎮ胸部CT能反映病灶的特点及邻近结构累及情况ꎬ为临床诊断及鉴别提供参考依据ꎮ参考文献:[1]IsaacsonPꎬWrightDH.Malignantlymphomaofmucosa ̄associat ̄edlymphoidtissue:adistinctivetypeofB ̄celllymphoma[J].Cancerꎬ1983ꎬ52(8):1410 ̄1416.[2]易祥华ꎬ周晓燕ꎬ张太明ꎬ等.肺黏膜相关淋巴组织型淋巴瘤的表型和IgH基因重排的检测价值[J].中华结核和呼吸杂志ꎬ2005ꎬ28(10):704 ̄708.[3]TanakaTꎬYoshinoT.ClinicopathologyofMALTlymphoma[J].NihonRinshoꎬ2007ꎬ65(1):178 ̄181.[4]IsaacsonPGꎬChanJKꎬTangCꎬetal.Low ̄gradeB ̄celllympho ̄maofmucosa ̄associatedlymphoidtissuearisinginthethymus:athymiclympho ̄mamimickingmyoepithelialsialadenitis[J].AmJSurgPatholꎬ1990ꎬ14(4):342 ̄351.[5]宋伟安ꎬ王伟ꎬ周乃康.胸腺MALT淋巴瘤的临床病理分析[J].临床肿瘤学杂志ꎬ2011ꎬ16(9):829 ̄832. [6]常晓燕ꎬ陈杰ꎬ姜英ꎬ等.胸腺原发性黏膜相关淋巴组织淋巴瘤2例及文献复习[J].协和医学杂志ꎬ2012ꎬ3(1):41 ̄46. [7]胡帅ꎬ李智勇ꎬ郎志谨.胸腺原发性黏膜相关淋巴组织淋巴瘤2例[J].实用放射学杂志ꎬ2017ꎬ33(6):676 ̄677. [8]王震ꎬ李海ꎬ曾铮ꎬ等.胸腺原发黏膜相关淋巴组织淋巴瘤及淋巴上皮性涎腺炎样胸腺增生的临床病理分析[J].临床与实验病理学杂志ꎬ2016ꎬ32(12):1338 ̄1342.[9]陆杨ꎬ赵亚娥ꎬ杨春燕ꎬ等.MSCT对低危型㊁高危型胸腺瘤及胸腺癌的鉴别诊断价值[J].放射学实践ꎬ2017ꎬ32(2):149 ̄152.[10]张明山ꎬ刘茜ꎬ谢开元.无症状胸腺瘤CT影像特点与其型别的相关性研究[J].医学影像学杂志ꎬ2018ꎬ28(7):1126 ̄1129.[11]赵飞ꎬ杨明ꎬ黄承明ꎬ等.前纵隔胸腺瘤和淋巴瘤的18F ̄FDG ̄PET/CT显像特征及鉴别诊断价值[J].医学影像学杂志ꎬ2016ꎬ26(4):634 ̄636.[12]熊淑红ꎬ肖琼ꎬ冯少仁ꎬ等.原发性胸腺淋巴瘤的CT诊断[J].放射学实践ꎬ2014ꎬ29(6):654 ̄658.(收稿日期:2019 ̄03 ̄28)612。
2021年成人幽门螺杆菌感染的治疗指南
成人幽门螺杆菌感染的治疗指南欧阳光明(2021.03.07)(2016-12-20 17:40:52)转载▼Fallone CA et al.Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016 Apr18;S0016-5085(16)30108-1.新的推荐强调四联治疗和需要了解当地耐药特点。
赞助机构:加拿大胃肠病学会和加拿大幽门螺杆菌研究组目标读者:胃肠病专家,一般医生背景:治疗幽门螺杆菌感染由于抗生素耐药增加而越来越难。
专家委员会对于文献做了系统回顾,对于成人根除治疗做了推荐。
委员会成员应用GRADE方法(Grading of Recommendation Assessment, Development, and Evaluation)对于推荐强度和证据水平分级,并应用改良Delphi方法对于他们的共识水平进行评价。
强烈推荐初始治疗应为14天(由于治疗失败越来越多)。
一线治疗方案的选择应根据当地抗生素耐药监测。
推荐的一线治疗方案非铋剂PPI为基础的四联治疗(PPI + 阿莫西林 + 甲硝唑 + 克拉霉素,PAMC)和有铋剂为基础的四联治疗(PPI + 铋剂 + 甲硝唑 + 四环素,PBMT)。
PPI为基础的三联治疗(PPI + 克拉霉素 + 阿莫西林或甲硝唑)仅限于克拉霉素耐药低于15%或根除成功率大于85%的地区。
左氧氟沙星三联治疗和序贯PPI为基础的三联治疗不推荐。
推荐的初始治疗后的补救治疗是铋剂为基础的四联治疗(PBMT)和左氧氟沙星三联治疗(PPI + 阿莫西林 +左氧氟沙星,是有条件的推荐);不推荐序贯治疗。
对于含克拉霉素或左氧氟沙星的方案治疗失败者不应该应用含有这些药物的方案作为补救治疗。
含利福布汀(Rifabutin)的方案应在其他三种方案失败后选用。
淋巴癌(英文版)
Swelling lymph node
Other lymphoma symptoms
• Fever • Persistent cough and shortness of breath (if Hodgkin
lymphoma is located in the chest) • Sweating, especially at night (drenching sweats of
Typical Reed-Sternberg cells can be found in tumor tissue.
Reed-Sternberg cell
CD30 positive
RS
Nodular Sclerosis. Nodular sclerosis is the most common subtype, representing about 60 to 70 percent of Hodgkin lymphoma cases. Younger patients are more likely to have this type.
Mixed Cellularity. Mixed cellularity is the second most common subtype.
It occurs in about 25 percent of patients and mostly in older patients, children, and those with immune disorders, such as AIDS.
Radiation and heredity
Overdose radiation and heredity disorder can cause chromosome injure, which may cause abnormal Immunophenotyping and promote.
幽门螺旋杆菌感染治疗最新指南
解读美国胃肠病学会幽门螺旋杆菌感染治疗最新指南作者:姚瑜作者单位:中国医药集团四川抗菌素工业研究所,成都,610051刊名:国外医药(抗生素分册)英文刊名:WORLD NOTES ON ANTIBIOTICS年,卷(期):2007,28(6)被引用次数:0次1.Everhart J E Recent developments in the epidemiology of Helicobacter pylori 20002.Peterson W L.Fendrick A M.Cave D R Helicobacter pylori-related disease:guidelines for testing and treatment 20003.Howden C W.Hunt R H Guidelines for the management of Helicobacter pylori infection 19984.Paptheodoridis G V.Sougioultzis S.Archimandritis A J Effects of Helicobacter pylori and nonsteroidal antiinflammatory drugs on peptic ulcer disease:a systematic review 20065.Leodolter A.Kulig M.Brasch H A meta-analysis comparing eradication,healing and relapse rates in patients with Helicobacter pylori-associated gastric or duodenal ulcer 20016.Ford A C.Delaney B C.Forman D Eradication therapy in Helicobacter pylori positive peptic ulcer disease:systematic review and economic analysis 20047.Sharma V K.Sahai A V.Corder F A Helicobacter pylori eradication is superior to ulcer healing with or without maintenance therapy to prevent further ulcer haemorrhage 20018.Liu C C.Lee C L.Chan C C Maintenance treatment is not necessary after Helicobacter pylori eradication and healing of bleeding peptic ulcer 20039.Gisbert J P.Khorrami S.Carballo F H.pylori eradication therapy vs.antisecretory non-eradication therapy (with or without long-term maintenance antisecretory therapy) for the prevention of recurrent bleeding from peptic ulcer 2004(02)10.Farinha P.Gascoyne R D Helicobacter pylori and MALT lymphoma 200511.Montalban C.Norman F Treatment of gastric mucosa associated lymphoid tissue lymphoma:Helicobacter pylori eradication and beyond 200612.Wundisch T.Thiede C.Morgner A Long-term follow-up gastric MALT lymphoma after Helicobacter pylori eradication 200113.Nakamura S.Matsumoto T.Suekane H Long-term clinical outcome of Helicobacter pylori eradicationfor gastric mucosa-associated lymphoid tissue lymphoma with a reference to second-line treatment 200514.Chen L T.Lin J T.Tai J J Long-term results of antiHelicobacter pylori therapy in early-stage gastric high grade transformed MALT lymphoma 200515.Talley N J.Vakil N Practice Parameters Committee of the American College ofGastroenterology.Guidelines for the management of dyspepsia 200516.Midolo P.Marshall B J Accurate diagnosis of Helicobacter pylori.Urease tests 200017.Perna F.Ricci C.Gatta L Diagnostic accuracy of a new rapid urease test (Pronto Dry),before andafter treatment of Helicobacter pylori infection 2005ine L.Lewin D.Naritoku W Prospective comparison of commercially available rapid urease testsfor the diagnosis of Helicobacter pylori 199619.Lee J M.Breslin N P.Fallon C Rapid urease tests lack sensitivity in Helicobacter pylori diagnosis when peptic ulcer disease presents with bleeding 200020.Tu T C.Lee C L.Wu C H Comparison of invasive and noninvasive tests for detecting Helicobacter pylori infection in bleeding peptic ulcers 199921.Grino P.Pascual S.Such J Comparison of stool immunoassay with standard methods for detection of Helicobacter pylori infection in patients with upper gastrointestinal bleeding of peptic origin 2003 ine L A.Nathwani R A.Naritoku W The effect ofGI bleeding on Helicobacter pylori diagnostic testing:a prospective study at the time of bleeding and 1 month later 200523.Gisbert J P.Abraira V Accuracy of Helicobacter pylori diagnostic tests in patients with bleeding peptic ulcer:a systematic review and meta-analysis 200624.Woo J S.el-Zimaity H M.Genta R M The best gastric site for obtaining a positive rapid urease test 199625.Chey W D.Woods M.Scheiman J M Lansoprazole and ranitidine affect the accuracy of the C-urea breath test by a pH-dependent mechanism 1997ine L.Estrada R.Trujillo M Effect of protonpump inhibitor therapy on diagnostic testing for Helicobacter pylori 199827.el-Zimaity H M Accurate diagnosis of Helicobacter pylori with biopsy 200028.Dixon M F.Genta R M.Yardley J H Classification and grading of gastritis.the updated Sydney system.International workshop on the histopathology of gastritis,Houston 1994 199629.Cutler A F.Havstad S.Chen K M Accuracy of invasive and non-invasive tests to diagnose Helicobacter pylori infection 199530.van IJzendoorn M heij R J.de Boer W A The importance of corpus biopsies in the determination of Helicobacter pylori infection 200531.Perez-Perez G I Accurate diagnosis of Helicobacter pylori.Culture,including transport 200032.Makristathis A.Hirschl A M.Lehourst P Diagnosis of Helicobacter pylori Infection 200433.Lehours P.Ruskone-Fourmestraux vergne A Which test to use to detect Helicobacter pylori infection in patients with low-grade gastric mucosa-associated lymphoid tissue lymphoma? 200334.Zsikla V.Hailemariam S.Baumann M Increased rate of Helicobacter pylori infection detected by PCR in biopsies with chronic gastritis 2006wson A J.Elviss N C.Owen R J Real-time PCR detection and frequency of 16 S rDNA mutations associated with resistance and reduced susceptibility to tetracycline in Helicobacter pylori from England and Wales 200536.Rimbara E.Noguchi N.Yamaguchi T Development of a highly sensitive method for detection ofclarithromycin-resistant Helicobacter pylori from human feces 2005Helicobacter pylori DNA sequences by TaqMan real-time polymerase chain reaction 200638.Ho G Y.Windsor H M Accurate diagnosis of Helicobacter pylori.Polymerase chain reaction tests 200039.Ho B.Marshall B J Accurate diagnosis of Helicobacter pylori.Serologic testing 200040.Loy C T.Irwig L M.Katelaris P H Do commercial serological kits for Helicobacter pylori infection differ in accuracy? A meta-analysis 199641.Chey W D.Murthy U.Shaw S A comparison of three finger stick,whole blood antibody tests for Helicobacter pylori infection:An United States,multicenter trial 199942.Nurgalieva Z Z.Graham D Y Pearls and pitfalls of assessing Helicobacter pylori status 200343.Hoang T T.Wheeldon T U.Bengtsson C Enzyme liked immunosorbent assay for Helicobacter pylori needs adjustment for the population investigated 200444.Gisbert J P.Pajares J M Review article:13 C-urea breath test in the diagnosis of Helicobacter pylori infection-a critical review 200445.Chey W D Accurate diagnosis of Helicobacter pylori.14C urea breath test 200046.Steen T.Berstad K.Meling T Reproducibility of the 14 C-urea breath test repeated after 1 week 199547.Leodolter A.Dom'ingues-Mu~noz J E.von Arnim U Validity of a modified 13C-urea breath test forpre-and post-treatment diagnosis of Helicobacter pylori infection in the routine clinical setting 199948.Chey W D.Metz D C.Shaw S Appropriate timing of the C-urea breath test to establish eradication of Helicobacter pylori infection 200049.Perri F.Giampiero M.Neri M Helicobacter pylori antigen stool test and 13C-urea breath test in patients after eradication treatments 200250.Gatta L.Ricci C.Tampieri A Accuracy of breath tests using low doses of 13C-urea to diagnose Helicobacter pylori infection:a randomised controlled trial 200651.Chey W D.Murthy U.Toskes P The 13C-urea blood test accurately detects active Helicobacter pylori infection:An United States,multicenter trial 199952.Ahmed F.Chey W D.Murthy U Evaluation of the Ez-HBT Helicobacter blood test to establish Helicobacter pylori eradication 200553.Graham D Y.Opekun A R.Hammoud F Studies regarding the mechanism of false negative urea breath tests with proton pump inhibitors 200354.Cutler A F.Elnaggar M.Brooks E Effect of standard and high dose ranitidine on C-urea breath test results 199855.Savarino V.Tracci D.Dulbecco P Negative effect of ranitidine on the results of urea breath test for the diagnosis of Helicobacter pylori 200156.Graham D Y.Opekun A R.Jogi M False negative urea breath tests with H2-receptorantagonists:Interactions between Helicobacter pylori density and pH 200457.Gatta L.Vakil N.Ricci C Effect of proton pump inhibitors and antacid therapy on C urea breath tests and stool test for Helicobacter pylori infection 200458.Gatta L.Ricci C.Tampieri A Accuracy of breath tests using low doses of C-urea to diagnose Helicobacter pylori infection:A randomised controlled trial 200659.Gisbert J P.Pajares J M Stool antigen test for the diagnosis of Helicobacter pylori infection:A systematic review 200460.Gisbert J P.de la Morena F.Abraira V Accuracy of monoclonal stool antigen test for the diagnosis of H.pylori infection:A systematic review and meta-analysis 200661.Malfertheiner P.Megraud F.O' Morain C Current concepts in the management of Helicobacter pylori infection-the Maastricht 2-2000 Consensus Report 200262.Viara D.Vakil N.Menegatti M The stool antigen test for detection of Helicobacter pylori after eradication therapy 200263.Odaka T.Yamaguchi T.Koyama H Evaluation of the Helicobacter pylori stool antigen test for monitoring eradication therapy 200264.Vakil N.Rhew D.Soll A The cost-effectiveness of diagnostic testing strategies for Helicobacter pylori 200065.Bravo L E.Realpe J L.Campo C Effects of acid suppression and bismuth medications on the performance of diagnostic tests for Helicobacter pylori infection 199966.Manes G.Balzano A.Iaquinto G Accuracy of the stool antigen test in the diagnosis of Helicobacter pylori infection before treatment and in patients on omeprazole therapy 200167.Grino P.Pascual S.Such J Comparison of stool immunoassay with standard methods for detection of Helicobacter pylori infection in patients with upper gastrointestinal bleeding of peptic origin 2003 68.Peitz U.Leodolter A.Kahl S Antigen stool test for assessment of Helicobacter pylori infection in patients with upper gastrointestinal bleeding 200369.van Leerdam M E.Van Der Ende A.ten Kate F J W Lack of accuracy of the noninvasive Helicobacter pylori stool antigen test in patients with gastroduodenal ulcer bleeding 200370.Lin H J.Lo W C.Perng C L Helicobacter pylori stool antigen test in patients with bleeding peptic ulcers 20041.期刊论文"温胃舒或养胃舒治疗幽门螺杆菌相关性慢性胃炎和消化性溃疡"全国多中心临床研究科研协作组. "Wenweishu (温胃舒) /yangweishu ( 养胃舒) in the Treatment of Helicobacter pylori Positive Patients with Chronic Gastritis and Peptic Ulcer" Study Group温胃舒或养胃舒治疗幽门螺杆菌相关性慢性胃炎和消化性溃疡的全国多中心临床研究-中华医学杂志2010,90(2)目的 探讨标准三联疗法泮托拉唑+克拉霉素+甲硝唑(PCM)联合温胃舒或养胃舒对幽门螺杆菌(Hp)相关性慢性胃炎和消化性溃疡患者的Hp根除率及症状缓解率,并观察温胃舒或养胃舒对胃溃疡愈合的影响.方法 全国11个中心642例符合标准的患者随机分为PCM组(222例):泮托拉唑40 mg2次/d+克拉霉素500 mg2次/d+甲硝唑400 mg2次/d,疗程7 d;PCM+温胃舒组(196例);PCM+养胃舒组(224例).于治疗停药4周后复查(~14)C-尿素呼气试验,胃溃疡患者治疗结束复查胃镜.结果 按意向治疗(ITT)分析显示,PCM+温胃舒组、PCM+养胃舒组及PCM组Hp根除率分别为62.2%(122/196)、60.3%(135/224)和57.2%(127/222)(与PCM组比较,P=0.295、0.512);按符合方案(PP)分析分别为70.1%(122/174)、65.2%(135/207)和62.3%(127/204)(与PCM组比较,P=0.108、0.532).PP分析3组胃溃疡愈合率分别为100.0%(18/18)、86.4%(19/22)和61.9%(13/21);PCM+温胃舒组胃溃疡愈合率与PCM组比较差异有统计学意义(P=0.004).PCM+养胃舒组及PCM+温胃舒组患者腹痛、腹胀症状缓解率均显著高于PCM组(均P<0.01).各组均只有少数患者发生不良反应.结论 温胃舒或养胃舒与标准三联疗法联合应用虽不能明显提高Hp的根除率,但可增加慢性胃炎及消化性溃疡患者症状缓解率及溃疡愈合率.2.期刊论文刁萍萍.杜奕奇.李兆申.李淑德.舒建昌.陈锡美.周中杰.陆和平.姜慧卿.刘希双.鲁临.杨力.时昭红.刘鹏飞.屠惠明.陈国昌.张志坚.DIAO Ping-ping.DU Yi-qi.LI Zhao-shen.LI Shu-de.SHU Jian-chang.CHEN Xi-mei. ZHOU Zhong-jie.LU He-ping.JIANG Hui-qing.LIU Xi-shuang.LU Lin.YANG Li.SHI Zhao-hong.LIU Peng-fei.TUHui-ming.CHEN Guo-chang.ZHANG Zhi-jian幽门螺杆菌阴性消化性溃疡与出血关系的多中心对照研究-中华消化内镜杂志2010,27(8)目的 明确中国大陆地区幽门螺杆菌(Hp)阴性消化性溃疡与出血的关系.方法 拟定于2006年4月至2007年3月期间在国内14个研究中心中进行,每个中心预期调查30例经急诊内镜诊断为胃溃疡和(或)十二指肠溃疡合并出血的患者(PUB组),同时调查30例不伴出血的胃溃疡和(或)十二指肠溃疡患者作为对照(PU组).共拟入选840例患者,消化性溃疡合并及不合并出血组各420例.在内镜检查中采用快速尿素酶试验和病理检测Hp感染,并对初次检查Hp阴性者于1个月后进行尿素呼气试验复查.结果 共617例患者纳入分析,其中PUB组263例、PU组354例,2组在性别比、平均年龄等一般状况方面差异无统计学意义(P均>0.05).PUB组Hp阳性率61.2%(161/263)显著低于PU组的87.9%(311/354)(P<0.001);PUB组Hp阳性的溃疡出血发生复合溃疡的比例7.5%(12/161)显著高于Hp阴性溃疡出血者1.0%(1/102)(P=0.018),但两者在平均发病年龄、性别比、呕血发生率、十二指肠球部溃疡发生率、胃溃疡发生率及溃疡平均直径方面差异无统计学意义(P均>0.05).对于初次Hp阴性的溃疡出血患者,1个月后的呼气试验复查未发现阳性病例.结论 目前中国大陆Hp阴性溃疡在消化性溃疡出血中的比例较高,Hp阴性溃疡可能更容易并发消化道出血,需要引起消化专科医生的重视.3.期刊论文张保环.干超士.柴军土.徐惠萍.乐怀浙.ZHANG Bao-huan.GAN Chao-shi.CHAI Jun-tu.XU Hui-ping.LE Huai-zhe消化性溃疡伴幽门螺杆菌感染患者184例干预治疗分析-中国基层医药2008,15(7)目的 探讨消化性溃疡伴幽门螺杆菌(Hp)感染患者干预治疗的临床效果.方法 将184例消化性溃疡伴Hp感染患者随机分为两组,常规组给予单纯药物治疗:泮托拉唑和替普瑞酮;干预组给予药物(同上)和生活方式及个人饮食习惯干预治疗;两组疗程均为6周.根除Hp治疗:泮托拉唑加用克拉霉素和阿莫西林,疗程为1周.疗程结束后对比两组疗效.结果 临床症状完全缓解时间:干预组中77例第1周完全缓解;常规组中56例第1周完全缓解;两组患者第1周临床症状完全缓解率比较差异有统计学意义(P<0.01).溃疡愈合情况:在疗程结束后胃镜复查显示,干预组90例溃疡治愈,常规组83例溃疡治愈,两组溃疡愈合率比较差异有统计学意义(P<0.05).Hp根除情况:干预组85例,常规组83例,两组比较差异无统计学意义(P>0.05).结论 药物结合生活方式及个人饮食习惯的干预治疗能加快临床症状消失,提高溃疡治疗效果.4.期刊论文吴春城.谢会忠.WU Chun-cheng.XIE Hui-zhong非甾体抗炎药和幽门螺杆菌感染对消化性溃疡并发出血的影响-中国全科医学2010,13(8)目的 探讨服用非甾体抗炎药(NSAIDs)和幽门螺杆菌(H.pylori)感染与消化性溃疡并发出血的关系.方法 收集2007年1月-2009年7月在新疆医科大学第一临床医学院消化内科收治的消化性溃疡患者205例,均行内镜检查确诊(除外复合溃疡),并行病理学检查排除胃癌.对消化性溃疡并发出血的危险因素行单因素和多因素分析.结果 205例消化性溃疡患者中,男150例(73.2%),女55例(26.8%);中位年龄49(12~88)岁;并发出血87例(42.4%).在单因素分析中,出血组与未出血组患者中年龄≥60岁者、既往有消化道出血史者、心脑血管病史者、有多个溃疡者所占比例间差异均有统计学意义(P<0.01);进一步行Logistic逐步回归分析,发现年龄≥60岁、有消化性溃疡史、消化道出血史、心脑血管病史和单纯H.pylori感染、单纯服用NSAIDs、H.pylori感染同时服用NSAIDs为消化性溃疡并发出血的危险因素.结论 H.pylori感染并未增加溃疡并发出血的危险性,但与服用NSAIDs、年龄≥60岁、消化性溃疡或出血史、心脑血管病史等因素联合可增加溃疡并发出血的危险性.5.期刊论文孟灵梅.周丽雅.林三仁.闫秀娥.丁士刚.黄永辉.顾芳.张莉.李渊.崔荣丽.张冬红.张静.MENG Ling-mei.ZHOU Li-ya.LIN San-ten.YAN Xiu-e.DING Shi-gang.HUANG Yong-hui.GU Fang.ZHANG Li.LI Yuan.CUI Rong-li.ZHANG Dong-hong.ZHANG Jing幽门螺杆菌与消化性溃疡关系的10年随访研究-中华消化杂志2009,29(6)目的 探讨根除幽门螺杆菌(Helicobacter pylori,Hp)后10年间十二指肠球部溃疡(DU)、胃溃疡(GU)发病情况.方法 选择胃癌高发区山东烟台高陵镇随机抽样自然人群进行内镜普查,其中Hp阳性者552例均分为治疗组和安慰剂组,治疗组276例予以奥美拉唑20 mg、克拉霉素0.5 g和阿莫西林1.0 g,每日2次口服,疗程7 d.停药1个月后治疗组行13C-尿素呼气试验(13C-UBT)证实根除成功.此后对两组在10年期间进行内镜随访(第1、5、8和10年),观察两组患者消化性溃疡发病率的变化及复发情况,同时观察两组Hp感染状态的变迁.结果 治疗组消化性溃疡第1、5和8年的发病率分别为3.70%、5.86%和4.40%,均明显低于安慰剂组(12.85%、14.93%和9.39%,P值分别=0.0002、0.0017和0.0440).随访10年间,治疗组消化性溃疡新发病例数及复发病例数均低于安慰剂组,两组间差异均有统计学意义(P值均<0.05).治疗组Hp再感染率较高,第10年时Hp阳性率达46.4%.根据Hp感染状态重新进行分组,结果显示随访10年间Hp阴性组消化性溃疡的发病率均低于Hp阳性组(P值均<0.05).结论 根除Hp治疗后消化性溃疡的发病率和复发率均明显降低,消化性溃疡患者根除Hp是必要的.成功根除Hp后再感染率仍较高.6.期刊论文邓淑娟.李兴华.方德宁.曾钗明.DENG Shu-Juan.LI Xing-Hua.FANG De-ning.ZENG Chai-ming幽门螺杆菌babA2和胃黏膜上皮Leb抗原在不同血型中表达情况及与消化性溃疡的关系-江苏大学学报(医学版)2010,20(2)目的:研究不同血型(ABO)患者幽门螺杆菌(Helicobacter pylori,Hp)表达血型抗原结合黏附素(blood group antigen binding adhesion,babA2)和胃黏膜上皮表达Lewisb (Leb)情况,及两者与消化性溃疡的关系.方法:测定56例(25例胃炎,31例消化性溃疡)Hp阳性消化性溃疡及消化不良的患者血型,并进行内镜检查,取2块胃黏膜,一块进行Hp培养,采用PCR检测Hp babA2表达情况;另一块组织进行组织病理学检查,并应用免疫组化测定胃黏膜上皮表达Leb情况.分别比较不同血型babA2、Leb表达情况与消化性溃疡的关系.结果:56例患者中,消化性溃疡组O型血所占比例高于胃炎组及正常人群(P均<0.0125),O型血患者胃黏膜Leb评分显著高于非O型血(P<0.005),消化性溃疡组Leb评分高于胃炎组(P<0.05).Hp培养成功30例,有28例babA2阳性(7例消化性溃疡,21例胃炎),babA2阳性患者中,消化性溃疡组O型血比例高于非O型血(P<0.0125),消化性溃疡组与胃炎组O型血所占比例差异无统计学意义.结论:O型血可能是通过高表达Leb及Hp的babA2增加了消化性溃疡的发生.7.期刊论文李小刚.陈锡美.LI Xiao-gang.CHEN Xi-mei胆汁反流和幽门螺杆菌感染在胆汁反流性胃炎和消化性溃疡发病中的作用-中国内镜杂志2005,11(6)目的探讨胆汁反流和幽门螺杆菌感染在胆汁反流性胃炎和消化性溃疡发病中的作用.方法采用病理组织学检查和快速尿素酶试验对76例胆汁反流性胃炎及22例兼有胆汁反流性胃炎和消化性溃疡的患者行幽门螺杆菌检测,并与29例消化性溃疡患者作对照.结果胆汁反流性胃炎组幽门螺杆菌阳性率为31.6%(24/76例),兼有胆汁反流性胃炎和消化性溃疡组幽门螺杆菌阳性率为59.0%(13/22例),消化性溃疡组幽门螺杆菌阳性率为72.4%(21/29例),前二组比较,差异有显著意义(P<0.05),后二组比较,差异无显著意义(P>0.05).结论胆汁反流在胆汁反流性胃炎的发病中起主要作用,幽门螺杆菌感染在消化性溃疡的发病中起主要作用.胆汁反流和幽门螺杆菌感染在胆汁反流性胃炎和消化性溃疡的共同发病中互不明显影响,幽门螺杆菌感染所起的作用可能更大一些.8.期刊论文梅浙川.罗咏萍.何璐.吴素华根除幽门螺杆菌治疗后消化性溃疡的流行病学研究附30993例胃镜资料分析-重庆医学2005,34(5)目的了解近20年来幽门螺杆菌(Hp)根除治疗后消化性溃疡(Pu)的发病情况及变化特点.方法回顾性分析我院24年来胃镜检查消化性溃疡的临床资料,以1985年1月为分界,之前为未开展根除Hp治疗消化性溃疡期,之后为开展根除Hp治疗消化性溃疡期.结果1985~1994年和1995~2003年消化性溃疡检出率分别为14.92%和14.80%,与1979~1984年的17.13%比较显著下降(P<0.05).1985~1994年和1995~2003年消化性溃疡的平均发病年龄分别为(40.64±11.65)岁和(44.72±13.55)岁,分别高于1979~1984年的(38.13±13.20)岁,(P<0.05);>60岁的老年患者1995年后发病显著增高(P<0.01).1985~1994年和1995~2003年的男女之比为3.73:1和2.38:1,显著低于1979~1984年的7.72:1(P<0.05).24年来发病均以1~4月为高峰,6~9月最低.结论开展根除Hp治疗后消化性溃疡的发病率下降、发病年龄增大、老年人患病率增加、男女之比下降、发病季节无明显改变.9.期刊论文叶英.Ye Ying两种三联疗法治疗幽门螺杆菌相关性消化性溃疡临床观察-医学研究杂志2007,36(3)目的 比较两种三联疗法治疗幽门螺杆菌相关性消化性溃疡的疗效.方法 将幽门螺杆菌阳性的消化性溃疡病例120例分成两组,A组用奥美拉唑+克拉霉素+阿莫西林口服治疗,B组用奥美拉唑+呋喃唑酮+阿莫西林口服治疗,疗程均为7天.观察消化性溃疡主要症状缓解情况、Hp根除率、溃疡愈合率、有效率及药物不良反应.结果 A、B两组消化性溃疡主要症状上腹痛、嗳气、反酸、恶心、腹胀的缓解率分别为91.5%和89.3%,90.0%和94.7%,85.7%和79.3%,90.9%和90.7%,85.7%和92.5%,差异无统计学意义(P>0.05);Hp根除率分别为91.7%和88.3%,差异无统计学意义(P>0.05);溃疡治愈率分别为66.7%和60.0%,总有效率分别为96.7%和93.3%,差异无统计学意义(P>0.05);不良反应发生率分别为10.0%和8.3%,差异无统计学意义(P>0.05).结论 两组方案均能有效缓解消化性溃疡症状和根除Hp,B组中因为呋喃唑酮价格低廉,不良反应轻,可推荐为治疗Hp相关性消化性溃疡的一线用药.10.期刊论文徐灿霞.肖丽君.邹惠芳.XU Canxia.XIAO Lijun.ZOU Huifang双歧杆菌三联活菌胶囊对幽门螺杆菌感染的消化性溃疡的治疗作用-中南大学学报(医学版)2010,35(9)目的:观察双歧杆菌三联活菌胶囊对幽门螺杆菌(Helicobacter pylori, H.pylori)感染的消化性溃疡的治疗作用.方法:H.pylori感染的消化性溃疡患者120例,随机分为2组:对照组用埃索美拉唑镁+阿莫西林+呋喃唑酮三联抗H.pylori治疗,治疗组用上述三联抗H.pylori治疗+双歧杆菌三联活菌胶囊,观察治疗前及治疗2周后胃液pH值、胃内菌群变化、不良反应、溃疡及糜烂愈合情况,治疗结束后4周复查14C 尿素呼气试验,观察H.pylori根除率.结果:2组治疗后胃液pH值均较治疗前明显升高(P<0.05),胃液pH值≥4时,治疗组胃液细菌培养阳性率低于对照组(分别为80.0%与97.4%,P<0.05);治疗组不良反应发生率低于对照组(分别为11.7%与30%,P<0.05);治疗2周后,治疗组与对照组溃疡治愈率分别为80.0%与73.3%(P>0.05),治疗组糜烂治愈率高于对照组(分别为68.7%与40.7%,P<0.05);治疗组H.pylori根除率高于对照组(PP分析分别为80.4%与62.3%,P<0.05).结论:在抗H.pylori治疗时加用双歧杆菌三联活菌胶囊能减少胃内细菌生长,降低不良反应,提高H.pylori根除率,促进糜烂愈合.本文链接:/Periodical_gwyykssfc200706008.aspx授权使用:昆山市中医医院(wfkszy),授权号:cb976ed9-b1e6-4b57-98c9-9eaa00c6d361下载时间:2011年3月18日。
淋巴浆细胞性淋巴瘤/华氏巨球蛋白血症10例临床病理学特征分析及 MYD 88基因突变检测
淋巴浆细胞性淋巴瘤(lymphoplasmacytic lymphoma,LPL)是一类相对少见的小B细胞 淋巴瘤,临床上以男性患者居多,常伴有骨 髓受累、贫血和血清IgM型免疫球蛋白异常增 高 [1]。 组 织 学 形 态 多 表 现 为 淋 巴 结 副 皮 质 区、髓质区弥漫性淋巴样浸润,肿瘤由数量不 等的小淋巴细胞、浆细胞和浆样淋巴细胞组 成[1]。免疫表型而言,肿瘤细胞表达全B细胞抗 原,并限制性表达免疫球蛋白轻链[1]。华氏巨 球蛋白血症(Waldenström macroglobulinemia, WM)为LPL中累及骨髓并伴有血清IgM蛋白不 同程度增高的病例[2]。LPL/WM常需与其他小B 细胞性肿瘤、特别是伴有浆细胞样分化的病例鉴 别[1],然而,相当部分LPL/WM具有不典型临床 或组织病理学表现[3],使得此类鉴别诊断较为 困难。近期研究发现,绝大部分LPL/WM病例存 在MYD88 L265P基因突变[4],而其他小B细胞类 肿瘤则较少检出这一异常[3-5]。在国外,利用 二代测序等技术检测MYD88 L265P突变已被应用 于临床实践,而在我国,应用这一检查手段诊断 和鉴别LPL/WM尚未推广、普及,相关报道亦不 多见。本研究回顾性分析了10例LPL/WM的临床 病理学特点,并应用传统测序技术完成MYD88 L265P突变点检查,从而探讨这一分子生物学标 志物对于确诊LPL/WM的意义。
900
·论 著·
欢迎关注本刊公众号
《中国癌症杂志》2018年第28卷第12期 CHINA ONCOLOGY 2018 Vol.28 No.12
淋巴浆细胞性淋巴瘤/华氏巨球蛋白血症10例 临床病理学特征分析及MYD88基因突变检测
盛 东,王维格,蒋翔男,薛 田,朱晓丽,周晓燕,李小秋
1例直肠黏膜相关淋巴组织边缘区淋巴瘤报告并文献复习

Vol.27No.2Apr.2021*山东省中医药科技发展计划项目(2019-0070)△通信作者,E-mail :******************1例直肠黏膜相关淋巴组织边缘区淋巴瘤报告并文献复习*肖守铜1,崔文文1,管仲安2△1山东中医药大学第一临床医学院山东济南2500002山东中医药大学附属医院肛肠科山东济南250000DOI:10.19668/ki.issn1674-0491.2021.02.019黏膜相关淋巴组织边缘区淋巴瘤是指来源于淋巴滤泡边缘区(即淋巴滤泡和滤泡外套之间的结构)细胞的低度恶性淋巴结外B 细胞性淋巴瘤,临床表现具有明显的惰性,病情进展缓慢,病程长,肿瘤常呈局限性生长,该病好发于50岁以上年龄段,近年有发病年轻化趋势[1]。
直肠黏膜相关淋巴组织边缘区淋巴瘤临床表现不典型,多表现为腹痛、便血、局部肿物及排粪习惯改变,严重者可引起肠梗阻,与炎性肠病(如溃疡性结肠炎、克罗恩病)及肠道恶性肿瘤等表现相似,误诊率高,预后尚不明确[2-3],因此,临床医师应予以重视。
本文报告1例直肠黏膜相关淋巴组织边缘区淋巴瘤患者的诊治过程,并进行相关文献复习和讨论。
1病例资料患者女性,25岁,因“反复便血伴肛内肿物脱出7天”于2020年6月2日入院。
患者便血反复发作,血色鲜红,偶有疼痛,便时可伴肛内肿物脱出,可还纳。
患者曾于外院行电子结肠镜检查,结果示距肛门约5cm 处可见两处相连的隆起(见图1),期间未进行相关的治疗。
平素身体健康状况良好。
入院查体:神清,浅表淋巴结未触及,心肺腹查体未见特殊。
专科检查:骑伏位,肛门外观大致正常。
直肠指诊:肛管前位、右前位可触及质软条形肿物,活动度可,退指指套少量染血,色鲜红,未见分泌物。
2诊治经过入院后完善相关辅助检查:(1)肛周及腔内彩超提示肛管前壁黏膜下低回声,考虑黏膜下炎性包块;(2)盆腔MRI 提示直肠右前壁局部隆起并盆腔多发小淋巴结;(3)胸部+全腹增强CT 提示回肠末端壁略厚并周围多发小淋巴结;(4)妇科肿瘤标志物检查未见异常。
幽门螺杆菌(1T)

42
报警信号
中老年,女性,长期消化不良,贫血重,
既往胃炎,溃疡, 胃镜下粘膜皱襞增厚、粗大、结节状, 胃活检组织学有大量的淋巴滤泡 病理检查报告有提示
( “建议再取,建议免疫组化”)
43
与H.Pylori感染关系密切
70%早期病例根除H.Pylori后 肿瘤可逆性转变甚至完全消失。
开创抗菌治疗早期肿瘤新纪元。
47
胃MALT淋巴瘤与H.Pylori感染 相关的证据
临床流行病学资料
Wotherspoon等 :110 例 (92% ) Stolte等 : 178 例(98.3% ) Doglioni等 :H.Pylori↑,胃MALT淋巴瘤↑ Parsonnet等 :胃淋巴瘤组(85%),对照组 ( 55%) (p〈0.05)
22
HP系微须氧菌,环境氧要求5-8%,在大气 和绝对厌氧环境下不能生长。 HP对临床微生物试验中常用于鉴定肠道细菌 的大多数经典生化试验不起反应。而氧化酶,触 酶,尿素酶,碱性磷酸酶,r-谷胺酰转肽酶,亮 氨酸肽酶这七种酶是作为HP生化鉴定的依据。
HP的全基因序列已经测出,其中尿素 酶基因有四个开放性读框。HP的尿素酶极 为丰富,约含菌体蛋白的15%,活性相当 于变形杆菌的400倍。尿素酶催化尿素水解 成氨云保护细菌在高酸环境下生存。
44
治疗新观念
传统方法:五年生存率5075%
手术 放疗 化疗:CHOP方案
46
新观点:根除HP治疗的加盟
“ to become member of” “ replace”
no
1996年欧洲 Maastricht共识报告
1997年美国消化健康促进(DHI)国际会议
免疫英文单词
免疫immunity医学免疫学medical immunology黏膜相关淋巴组织(mucosa-associated lymphoid tissue , MALT)抗原(antigen,Ag)免疫原性(immunogenicity)抗原性(antigenicity)半抗原(hapten)胸腺依赖性抗原(thymus dependent antigen, TD-Ag)胸腺非依赖性抗原(thymus independent antigen, TI-Ag)抗体(antibody, Ab)免疫球蛋白(Immunoglobulin,Ig)补体(Complement)细胞因子(cytokine CK)白细胞分化抗原(leukocyte differentiation antigen LDA)细胞表面标记(cell surface marker)。
黏附分子(adhesion molecule AM)主要组织相容性复合体(Major Histocompatibility Complex,MHC)人白细胞抗原(human leucocyte antigen HLA)多基因性(polygene)B细胞共受体(co-receptor)多反应性(polyreactivity)T cell coreceptor (辅助受体)ITIM基序-免疫受体酪氨酸抑制基序初始T细胞naive T cell效应T细胞effector T cell记忆性T细胞memory T cell-辅助性T细胞Th (helper T cell)细胞毒性T细胞Tc/CTL (cytotoxic T cell)调节性T细胞Tr (regulatory T cell)超敏反应(Hypersensitivity)变态反应(allergy)变应原(allergens)组胺(histamine)白三烯(leucotrienes,LTs)前列腺素D2(prostaglandin-D2,PGD2)血小板活化因子(platelet acti-vating factor,PAF)(DTH)单克隆抗体monoclonal antibody,mAb多克隆抗体polyclonal antibody凝集反应(agglutination reaction)沉淀反应(Precipitation reaction)妊娠检测(Pregnancy test)人绒毛膜促性腺激素(HCG)酶联免疫吸附试验(enzyme linked immunosorbent assay, ELISA)免疫预防(Immunoprophylaxis)免疫治疗(immunotherapy)疫苗(vaccine)淋巴细胞转化实验(Lymphocyte Transformation Test )人工被动免疫(artificial passive immunization)人工主动免疫(artificial active immunization)类毒素(toxiod)抗原提呈细胞(antigen-presenting cell,APC)单核/巨噬细胞(monocyte/macrophage, Mo/mf)抗原提呈细胞Antigen presenting cell;抗原处理antigen processing;抗原提呈antigen presentingADCC: 抗体依赖的细胞介导的细胞毒作用单体型(haplotype)连锁不平衡(linkage disequilibrium)Native T cellEffector T cell (Teff)Memory T cell (Tm)Perforin 穿孔素Granzyme颗粒酶Somatic hypermutation 体细胞高频突变Affinity maturation 抗体亲和力成熟Class switching类别转换Exogenous Ags外源性抗原Endogenous Ags内源性抗原ITAM免疫受体酪氨酸激活基序3.I nnate Immunity5.Passive Immunization6.Active Immunization7. Antigenplete Antigen9.Incomplete Antigen10.Immunogenicity11.TD-Ag 12.TI-Ag13.Epitope14.Antigenic Determinants 15.Immunoglobulin16. CDR17.Hypervariable Regions 18.Polyclonal antibody 19.monoclonal antibody 22.ADCC23.BCR Complex24.TCR Complex 25.Interleukin(IL)26.Interferon27.Cell Adhesion Molecule CAM 细胞粘附分子28.Cluster Of Differentiation,CD 29.MHC(HLA)haplotype 32.APC33.CTL35.AICD,activation-induced cell death 39.AIDS40.Immunologic Tolerance 41.VaccineHypersensitivyAUTOIMMUNITY自身免疫TAA多态性(polymorphism)HLDACDAnergy 失能linkage disequilibriumNative T cellEffector T cell (Teff)Memory T cell (Tm)PerforinGranzymeSomatic hypermutationAffinity maturationClass switchingExogenous AgsEndogenous Agsimmunitymedical immunologymucosa-associated lymphoid tissue , MALTantigen,Agimmunogenicityantigenicityhaptenthymus dependent antigen, TD-Ag thymus independent antigen, TI-Ag antibody, AbImmunoglobulin,IgComplementcytokine CKleukocyte differentiation antigen LDAcell surface markeradhesion molecule AMMajor Histocompatibility Complex,MHC human leucocyte antigen HLA polygeneco-receptorpolyreactivity T cell coreceptorITIM基序-免疫受体酪氨酸抑制基序初始T细胞naive T cell效应T细胞effector T cell记忆性T细胞memory T cell-辅助性T细胞Th (helper T cell)细胞毒性T细胞Tc/CTL (cytotoxic T cell)调节性T细胞Tr (regulatory T cell) histamineleucotrienes,LTsprostaglandin-D2,PGD2platelet acti-vating factor,PAFDTHmonoclonal antibody,mAb polyclonal antibody凝集反应(agglutination reaction)沉淀反应(Precipitation reaction)妊娠检测(Pregnancy test)enzyme linked immunosorbent assay, ELISAHypersensitivityallergyallergenImmunoprophylaxisimmunotherapyvaccineLymphocyte Transformation Test artificial passive immunization artificial active immunization toxiodantigen-presenting cell,APC monocyte/macrophage, Mo/mf Antigen presenting cell;antigen processing;antigen presentingADCCimmune surveillanceimmune defenceimmune homeostasis Exogenous AgsEndogenous Ags。
不饱和脂肪酸与炎症性肠病因果关系的孟德尔随机化分析

不饱和脂肪酸与炎症性肠病因果关系的孟德尔随机化分析*李 健1 高建淑1,2 赵可可1,2 高鸿亮1,2#新疆医科大学第一附属医院消化病二科1(830054) 新疆医科大学研究生学院2背景:炎症性肠病(IBD )是一种慢性复发性胃肠道炎症性疾病,包括溃疡性结肠炎(UC )和克罗恩病(CD )。
目前尚不清楚不饱和脂肪酸与IBD 之间是否存在因果关系。
目的:采用两样本孟德尔随机化分析探究不饱和脂肪酸与IBD 之间的因果关系。
方法:不饱和脂肪酸和IBD 的全基因组关联研究(GWAS )数据均来源于网络公开数据库。
采用逆方差加权分析法进行两样本孟德尔随机化分析,使用加权中位数法和MR⁃Egger 回归分析验证因果效应,以OR 及其95% CI 评价不饱和脂肪酸与IBD 风险的因果关系。
结果:ω⁃6脂肪酸与CD 无直接因果关系,与UC 有直接因果关系,逆方差加权分析结果显示ω⁃6脂肪酸基因水平每增加一个标准差,UC 风险增加16%(OR =1.16,95% CI : 1.00~1.36,P =0.04)。
而ω⁃3脂肪酸、单不饱和脂肪酸与IBD 之间均未发现因果关系。
结论:ω⁃6脂肪酸可能仅与UC 存在因果关系,ω⁃3脂肪酸、单不饱和脂肪酸与IBD 之间均未发现因果关系。
关键词 脂肪酸类,不饱和; 脂肪酸类,ω⁃6; 炎症性肠病; 结肠炎, 溃疡性; Crohn 病; 孟德尔随机化分析Causal Association Between Unsaturated Fatty Acids and Inflammatory Bowel Disease: A Mendelian Random ⁃ization Analysis LI Jian 1, GAO Jianshu 1,2, ZHAO Keke 1,2, GAO Hongliang 1,2. 1The Second Department of Gastroenterology, the First Affiliated Hospital of Xinjiang Medical University, Urumqi (830054); 2Graduate School of Xinjiang Medical University, UrumqiCorrespondence to:GAOHongliang,Email:*************************.cnBackground: Inflammatory bowel disease (IBD) is a chronic recurrent inflammatory disease of gastrointestinal tract including ulcerative colitis (UC) and Crohn's disease (CD). It is unclear whether there is a causal association between unsaturated fatty acids and IBD. Aims: A two ⁃sample Mendelian randomization analysis was used to explore the causal association between unsaturated fatty acids and IBD. Methods: The data of the genome⁃wide association study (GWAS) of unsaturated fatty acids and IBD were obtained from web ⁃based public databases. Two ⁃sample Mendelian randomization analysis was performed by using inverse⁃variance weighted analysis, and weight median estimator and MR⁃Egger regression were conducted to validate the association of the causal effect. The causality of unsaturated fatty acids on the risk of IBDwas evaluated by OR and 95% CI . Results: No direct causal association was found between ω⁃6 fatty acids and CD, and a direct causal association was found with UC. Inverse⁃variance weighted analysis showed a 16% increase in the risk of UC for each standard deviation increase in ω⁃6 fatty acid gene levels (OR =1.16, 95% CI : 1.00⁃1.36, P =0.04). However, no causal association was found between ω⁃3 fatty acids, monounsaturated fatty acids and IBD. Conclusions: ω⁃6 fatty acids may be onlycausally associated with UC, and no causal association is found between ω⁃3 fatty acids, monounsaturated fatty acids and IBD.Key words Fatty Acids, Unsaturated; Fatty Acids, Omega⁃6; Inflammatory Bowel Disease; Colitis, Ulcerative; Crohn Disease; Mendelian Randomization AnalysisDOI : 10.3969/j.issn.1008⁃7125.2023.01.003*基金项目:新疆维吾尔自治区自然科学基金杰出青年科学基金项目(2022D01E25)炎症性肠病(inflammatory bowel disease, IBD )是一种免疫介导的胃肠道慢性炎症性疾病,包括溃疡性结肠炎(ulcerative colitis, UC )和克罗恩病(Crohn's disease, CD ),临床特征以腹痛和腹泻为主。
胃MALT淋巴瘤ppt课件

精选课件PPT
34
胃肠道NHL 的临床分期
期别 Ⅰ期
变 Ⅱ期
Ⅱ1 Ⅱ2
盆
ⅡE 期 Ⅱ1E Ⅱ2E 静脉
Ⅳ期
临床分期描述 肿瘤局限于胃肠道,单一原发灶或多个非连续性病
肿瘤侵及区域淋巴结 局部淋巴结(胃旁或肠道旁淋巴结) 受侵 远处膈下淋巴结(肠系膜、腹主动脉旁、腔静脉旁、
腔和腹股沟淋巴结) 受侵 肿瘤穿透浆膜侵及临近器官或组织 同时有局部淋巴结(胃旁或肠道旁淋巴结) 受侵 同时有远处膈下淋巴结(肠系膜、腹主动脉旁、腔
精选课件PPT
10
精选课件PPT
11
幽门螺旋杆菌检测
多采取快速尿素酶试验、病理活检 (银染)、碳-14呼气试验联合检测。
由于胃MALT淋巴瘤患者在确诊前多有 长期上腹部不适的症状,要注意患者所用 药物对幽门螺旋杆菌的检测结果的影响。 常因患者近期内服用了质子泵抑酸剂和抗 生素而导致假阴性。
精选课件PPT
精选课件PPT
24
胃淋巴瘤的CT 表现特点:
( 1) 胃壁广泛性明显增厚( 多> 2cm) , 并有一 定柔软度;
( 2) 增强早期可见受累胃壁的胃粘膜呈线样 强化;
( 3) 病灶一般边界清晰光整, 累及周围脏器较 少;
( 4) 继发性胃淋巴瘤, 可见其它部位的淋巴瘤 同时存在
精选课件PPT
25
骨髓活检
3
诊断
胃MALT淋巴瘤临床表现缺乏特异性, 最初症状为模糊的上腹部不适、上腹部疼 痛, 随病变进展逐渐出现呕吐、胃肠道出血 和体质量减轻等, 另有部分患者无任何症状 而在健康体检时检出。
精选课件PPT
4
并发症
1. 出血:是胃MALT淋巴瘤最常见的并发症。 甚至有病人因消化道大出血导致失血性休 克而不得不采取急诊外科手术。在根除HP 并随访观察的过程中,患者也会因治疗效 果不佳,反复出现黑便。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Submit a Manuscript: https:// World J Gastroenterol 2019 May 14; 25(18): 2204-2216 DOI: 10.3748/wjg.v25.i18.2204ISSN 1007-9327 (print) ISSN 2219-2840 (online)ORIGINAL ARTICLE Basic StudyCharacteristics of mucosa-associated gut microbiota during treatment in Crohn’s diseaseCong He, Huan Wang, Wang-Di Liao, Chao Peng, Xu Shu, Xuan Zhu, Zhen-Hua ZhuORCID number: Cong He(0000-0002-1185-5456); Huan Wang (0000-0002-2118-238X); Wang-Di Liao (0000-0003-2064-2628); Chao Peng (0000-0001-7368-3904); Xu Shu (0000-0002-0861-5742); Xuan Zhu (0000-0003-1226-7653); Zhen-Hua zhu (0000-0001-8092-3582).Author contributions: He C, Wang H and Liao WD contributed to equally to this work; He C and Zhu ZH designed the research; Wang H, Liao WD, Peng C, Shu X and Zhu X enrolled the qualified patients and collected the mucosal samples; Wang H analyzed the information of the patients during treatment; He C performed the bioinformatic analysis and wrote the paper; all authors have read and approved the final version to be published.Supported by: the National Natural Science Foundation of China, No. 81660101 and No. 81860106; the Special Scientific Research Fund of Public Welfare Profession of National Health and Family Planning Commission, No. 201502026; and the Graduate Innovation Fund of Nanchang University, No. CX2017251. Institutional review board statement: The study was reviewed and approved by the Medical Ethics Committee of Nanfang Hospital. All routine colonic biopsy specimens from the patients were taken after informed consent and ethical permission was obtained for participation in the study.Conflict-of-interest statement: To the best of our knowledge, no Cong He, Huan Wang, Wang-Di Liao, Chao Peng, Xu Shu, Xuan Zhu, Zhen-Hua Zhu, Department of Gastroenterology, The First Affiliated Hospital of Nanchang University, Nanchang 330006, Jiangxi Province, ChinaCorresponding author: Zhen-Hua Zhu, PhD, Doctor, Department of Gastroenterology, The First Affiliated Hospital of Nanchang University, 17 Yong Waizheng Street, Donghu District, Nanchang 330006, Jiangxi Province, China. zhuzhenhua19820122@Telephone: +86-791-88692705Fax: +86-791-88623153AbstractBACKGROUNDThe dysbiosis of the gut microbiome is evident in Crohn’s disease (CD) compared with healthy controls (HC), although the alterations from active CD to remission after treatment are unclear.AIMTo characterize the mucosa-associated gut microbiota in patients with CD before and after the induction therapy.METHODSThe basic information was collected from the subjects and the CD activity index (CDAI) was calculated in patients. A 16S rRNA sequencing approach was applied to determine the structures of microbial communities in mucosal samples including the terminal ileal, ascending colon, descending colon and rectum. The composition and function of mucosa-associated gut microbiota were compared between samples from the same cohort of patients before and after treatment. Differential taxa were identified to calculate the microbial dysbiosis index (MDI) and the correlation between MDI and CDAI was analyzed using Pearson correlation test. Predictive functional profiling of microbial communities was obtained with PICRUSt.RESULTSThere were no significant differences in microbial richness among the four anatomical sites in individuals. Compared to active disease, the alpha diversity of CD in remission was increased towards the level of HC compared to the active stage. The principal coordinate analysis revealed that samples of active CD were clearly separated from those in remission, which clustered close to HC. Sixty-five genera were identified as differentially abundant between active and quiescent CD, with a loss of Fusobacterium and a gain of potential beneficial bacteriaconflict of interest exists.Open-Access: This article is anopen-access article which wasselected by an in-house editor andfully peer-reviewed by externalreviewers. It is distributed inaccordance with the CreativeCommons Attribution NonCommercial (CC BY-NC 4.0)license, which permits others todistribute, remix, adapt, buildupon this work non-commercially,and license their derivative workson different terms, provided theoriginal work is properly cited andthe use is non-commercial. See:/licenses/by-nc/4.0/Manuscript source : Unsolicited manuscript Received: January 6, 2019Peer-review started: January 7,2019First decision: March 13, 2019Revised: March 25, 2019Accepted: April 10, 2019Article in press: April 10, 2019Published online: May 14, 2019P-Reviewer: Kolios GS-Editor: Yan JPL-Editor: AE-Editor: Zhang YL including Lactobacillus , Akkermansia , Roseburia , Ruminococcus and Lachnospira after the induction of remission. The combination of these taxa into a MDI showed a positive correlation with clinical disease severity and a negative correlation with species richness. The increased capacity for the inferred pathways including Lipopolysaccharide biosynthesis and Lipopolysaccharide biosynthesis proteins in patients before treatment negatively correlated with the abundance of Roseburia ,Ruminococcus and Lachnospira .CONCLUSION The dysbiosis of mucosa-associated microbiota was associated with the disease phenotype and may become a potential diagnostic tool for the recurrence of disease.Key words: Crohn’s disease; Mucosa-associated gut microbiota; Active; Remission; 16S rRNA sequence©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.Core tip: The dysbiosis of gut microbiome is associated with the development of Crohn’sdisease (CD), although the alteration from active CD to remission after treatment isunclear. This study illustrated that the composition of mucosa-associated gut microbiotain active CD significantly changed after the induction of remission regardless of drugsused, which got close to healthy subjects. We speculate that the maintenance of gutmicrobiota balance may be potential therapeutic target for reducing the risk of diseaserelapse.Citation: He C, Wang H, Liao WD, Peng C, Shu X, Zhu X, Zhu ZH. Characteristics of mucosa-associated gut microbiota during treatment in Crohn’s disease. World J Gastroenterol 2019; 25(18): 2204-2216URL : https:///1007-9327/full/v25/i18/2204.htmDOI : https:///10.3748/wjg.v25.i18.2204INTRODUCTIONCrohn’s disease (CD), a subtype of inflammatory bowel disease (IBD), has become aglobal disease with accelerating incidence over the last few decades [1]. CD ischaracterized by multiple episodes of exacerbation and remission, with clinicalmanifestations of diarrhea, abdominal pain, fistulas and perianal lesions, which mayaffect the whole digestive tract and cause systemic symptoms [2]. Current therapies forIBD include anti-inflammatory and immunomodulatory treatments such as 5-aminosalicylates, corticosteroids, thiopurines, thalidomide and anti-tumor necrosisfactor alpha, all of which aim to achieve clinical remission and mucosal healing [3,4].The pathogenesis of CD is multifactorial and involves the interplay of host genetics,immune dysregulation and environmental factors resulting in an aberrant immuneresponse and subsequent intestinal inflammation [5].Recent progress in understanding the composition and function of humanmicrobiota has revealed the important role of microbiota in immune homeostasis [6].Accumulating studies using culture-independent techniques have shown thedysbiosis of gut microbiota in patients with CD, including decreased bacterialdiversity, with an expansion of putative aggressive groups (such as Enterobacteriaceae ,Fusobacterium ) combined with decreases in protective groups (such as Faecalibacterium ,Roseburia )[7,8]. In addition to observing the characteristics of gut microbiota in CD, astudy by Wang et al [9] evaluated their dynamic changes after infliximab (IFX) therapyand found that the dysbiosis could be corrected in patients with a sustainedtherapeutic response. Furthermore, a prospective study assessed the stoolmetagenomes of IBD patients starting biologic therapy and demonstrated a higherabundance of butyrate producers at baseline in therapy-responsive CD patients,indicating the predicative effect of the gut microbiome in treatment response [10]. Dueto the dysregulated microbiota in the pathogenesis of IBD, several studies havereported the potential effect of restoring dysbiotic gut microbiota, including the use ofprobiotics and unprocessed donor feces, in the management of IBD [11]. It is necessaryHe C et al. Crohn’s disease and gut microbiotaHe C et al. Crohn’s disease and gut microbiotato clarify the key bacteria that play a role in disease remission and relapse, and then,precise manipulation of these bacteria may become a therapeutic target in the future.To date, most studies investigating the gut microbiota of CD have typically usedfecal samples since they are readily obtained[7-9]. However, the composition of fecalmicrobiota has been shown to be significantly different from mucosal microbiota; thisdifference is believed to directly affect epithelial and mucosal function and to be moredeeply involved in the pathophysiology of CD[12,13]. To collect sufficient mucosalsamples, we processed endoscopically uninflamed mucosa, which was thicker thanthe inflamed mucosa and probably more appropriate for microbial analysis[14]. Inaddition, only limited differences in microbiota composition were observed betweeninflamed and uninflamed mucosa in patients[15]. The previous cross-sectional study ofthe alterations between CD patients and healthy controls (HC) could be misreadbased on the interindividual differences, which make it difficult to characterize thecritical bacteria in CD. Thus, we investigated the mucosal-associated microbiome inpaired samples from CD patients before and after clinical treatment by 16S rRNAgene sequencing to determine the association between gut microbiota and diseaseactivity.MATERIALS AND METHODSStudy cohortA prospective study was performed in nine CD patients who were enrolled in flare atbaseline and then induced remission after clinical therapy. Inclusion criteria were adiagnosis of CD confirmed by endoscopy and histology and the activity of the diseasewas measured by the CD activity index (CDAI). Six HC without previous history ofchronic disease were also recruited in the study from the First Affiliated Hospital ofNanchang University, China. Exclusion criteria for the two groups included severeconcomitant disease involving the liver, heart, lung or kidney, pregnancy or breast-feeding, and treatment with antibiotics and prebiotics during the previous 4 wk. Themucosal samples were collected during the colonoscopy and both the patients andhealthy subjects underwent intestinal washing before the examination. We did notcollect both inflamed and noninflamed tissues since a previous study showed that themucosal microbiota of inflamed and noninflamed regions of the gastrointestinal tractin CD or ulcerative colitis (UC) were indistinguishable, with virtually no taxademonstrating disproportional abundances at a significant threshold nor anysignificant diversity differences observed[15]. Written informed consent was obtainedfrom all the subjects and this study was approved by the Medical Ethics Committee ofNanfang Hospital.Sample collection and DNA extractionA total of 74 mucosal biopsies were collected from 15 participants, including 9patients with CD and 6 healthy individuals. Specimens of terminal ileum, ascendingcolon, descending colon and rectum in noninflamed mucosa were taken duringcolonoscopic examination. Sampling included both active and remission stages foreach patient who underwent clinical treatment. All the samples were immediately putin liquid nitrogen and stored at - 80 °C before processing.Microbial DNA was extracted from the mucosal biopsies using the E.Z.N.A. stoolDNA kit (Omega Biotek, Norcross, GA, United States) according to themanufacturer’s protocols. The 16S rDNA V3-V4 region of the Eukaryotic ribosomalRNA gene was amplified by PCR (95 °C for 2 min, followed by 27 cycles at 98 °C for10 s, 62 °C for 30 s, and 68 °C for 30 s and a final extension at 68 °C for 10 min) usingprimers 341F: CCTACGGGNGGCWGCAG; 806R: GGACTACHVGGGTATCTAAT,where the barcode is an eight-base sequence unique to each sample. PCRs wereperformed in triplicate 50 μL mixture containing 5 μL of 10 × KOD Buffer, 5 μL of 2.5mM dNTPs, 1.5 μL of each primer (5 μM), 1 μL of KOD Polymerase, and 100 ng oftemplate DNA.16S rRNA gene sequencingAmplicons were extracted from 2% agarose gels and purified using the AxyPrepDNA Gel Extraction Kit (Axygen Biosciences, Union City, CA, United States)according to the manufacturer’s instructions and qualified using QuantiFluor-ST(Promega, United States). Purified amplicons were pooled in equimolar and paired-end sequenced (2 × 250) using Illumina Hiseq 2500 following standard protocols. Theraw reads were deposited into the NCBI Sequence Read Archive database (AccessionNumber: SRP157001).Sequencing data analysisHe C et al. Crohn’s disease and gut microbiota The raw data were filtered to obtain clean reads by eliminating the adapter pollution and low-quality sequences. Paired end clean reads were merged as raw tags using FLASH (Fast Length Adjustment of Short reads, v 1.2.11) with a minimum overlap of 10 bp and mismatch error rates of 2%[16]. Noisy sequences of raw tags were filtered by QIIME (v1.9.1) pipeline under specific filtering conditions to obtain high-quality clean tags[17]. The tags were then clustered as Operational Taxonomic Unit (OTU) by scripts of USEARCH (v 7.0.1090) software with a 97% similarity threshold[18]. The representative OTU sequences were taxonomically classified using Ribosomal Database Project classifier v.2.2 trained on the Greengenes database[19,20]. Finally, an OTU table and a phylogenetic tree were generated for diversity analysis. To estimate the diversity of the microbial community of the sample, we calculated the within-sample (alpha) diversity by Wilcoxon rank test for two groups and multiple group comparisons were made using Kruskal-Wallis test. Beta diversity was estimated by computing weighted Unifrac distance and was visualized with principal coordinate analysis (PCoA). Statistical differences (P < 0.05) between the two groups in the relative abundance of bacterial phyla and genera were evaluated using Metastats (Kruskal-Wallis test for more than two groups).According to the genera average abundance in patients before and after treatment, genera were divided into before-enriched and after-enriched. The correlation network of genera differentially enriched in before and after group was constructed by Pearson correlation test based on the abundance. The correlation network was visualized using Cytoscape (version 3.3.0). Pearson correlation test was also performed for investigating microbial dysbiosis index (MDI) and CDAI, as well as differential genera and predicted pathways.Functional annotationThe metagenomes of the gut microbiome were imputed from 16S rRNA sequences with PICRUSt (Phylogenetic Investigation of Communities by Reconstruction of Unobserved States). This method predicts the gene family abundance from the phylogenetic information with an estimated accuracy of 0.8. The closed OTU table was used as the input for metagenome imputation and was first rarefied to an even sequencing depth prior to the PICRUSt analysis. Next, the resulting OTU table was normalized by 16S rRNA gene copy number. The gene content was predicted for each individual. Then, the predicted functional composition profiles were collapsed into level 3 of the KEGG database pathways. The output file was further analyzed using Statistical Analysis of Metagenomic Profiles (STAMP) software package[21]. RESULTSBacterial microbiota diversityTo determine the effect of disease activity on microbial composition, we collected four parts of mucosal samples including ileum, ascending colon, descending colon and rectum from nine patients in active and remission stages. Patients characteristics are described in Supplement Table 1. The CDAI was significantly decreased in the After group compared to the Before group, indicating that the remission had been induced after clinical treatments (Figure S1). The Before group included samples from three anatomical sites (ileum, ascending colon, descending colon) and the After group supplemented with rectum mucosa, except for three samples that were unqualified for sequencing. Given the ethical issue, we did not collect mucosa from the four sites in healthy subjects, but the samples in each site were relatively uniform (3 from ileum, 4 from ascending colon, 3 from descending colon and 4 from rectum). After filtering and bioinformatic processing, a median yield of 275041 high-quality reads were obtained per sample.The gut microbiota richness, measured by observed species and Shannon index, was not significantly different among ileum, ascending colon, descending colon and rectum in both CD and HC (Figure S2, numbers of observed species, P = 0.12 for CD and P = 0.49 for HC; Shannon index, P = 0.78 for CD and P = 0.91 for HC, Kruskal-Wallis test). The analysis of beta diversity based on the unweighted UniFrac distances showed that there was no significant difference among the four regions of intestinal tract in both CD and HC (Adonis analysis,P = 0.85 for CD,P = 0.94 for HC). Interestingly, analysis of alpha diversity as calculated by number of observed species and Chao1 index revealed that the microbial biodiversity of the patients in remission was significantly increased towards the HC compared to their active stage before treatment (Figure 1A, numbers of observed species, P < 0.0001; Chao1 index, P < 0.0001; Kruskal-Wallis test). Beta diversity represented by PCoA analysis clearly showed that the samples from patients after treatment, which clustered separatelyHe C et al. Crohn’s disease and gut microbiotafrom those before treatment, tended to approach that of HC (Figure 1B, Adonisanalysis, P = 0.001).Bacterial microbiota composition and correlationsTo investigate the specific changes of microbiota in patients with active and remissionCD, we assessed the relative abundance of taxa before and after treatment. At thephylum level, the Fusobacteria was lower in the After group than the Before group(Figure 2A). In addition, the Firmicutes was significantly decreased in CD whereas theProteobacteria was overrepresented in CD relative to HC. At the genus level, weobserved 65 bacterial taxa that displayed different abundance between Before andAfter group. Compared with the After group, 14 bacterial taxa were enriched in theBefore group, while 51 bacterial taxa were depleted in the Before group. The Before-enriched bacterial taxa included Fusobacterium, Streptococcus, Bacillaceae, etc. Bacterialtaxa that were depleted in the Before group included Anaerostipes,Roseburia,Ruminococcus, Lactobacillus, Akkermansia, Lachnospira, etc, which were significantlymore abundant in HC than CD (Figure 2B). Then, we used these taxa to calculate theMDI, which is the log of (total abundance in organisms increased in Before group)over (total abundance of organisms decreased in Before group) for the samples. TheMDI showed a positive correlation with clinical disease severity (CDAI), and anegative correlation with species richness (Figure 2C), suggesting the close associationbetween gut microbiota disorder and disease activity.We further compared the effect of different medications including thalidomide,azathioprine (AZA), AZA plus prednisolone and IFX on gut microbiota. First, theobserved species and Chao1 index, which represents alpha diversity, tended toincrease after treatment in four groups, although without significance in IFX and AZA(Figure S3, numbers of observed species, P < 0.05 for thalidomide, P < 0.01 for AZAplus prednisolone, P > 0.05 for AZA and IFX; Chao1 index, P < 0.05 for thalidomide, P< 0.01 for AZA plus prednisolone, P > 0.05 for AZA and IFX, t test). The analysis ofbeta diversity based on the unweighted UniFrac distances showed that the overallmicrobial composition of the After group was significantly different from the Beforegroup regardless of treatment drugs (Adonis analysis, P = 0.005 for thalidomide, P =0.019 for AZA, P = 0.004 for AZA plus prednisolone, P = 0.018 for IFX). Furthermore,the differential taxa between After and Before groups were identified according toeach treatment. The relative abundance of Roseburia, Ruminococcus and Anaerostipeswas significantly increased after IFX treatment while the number of Fusobacterium andStreptococcus was lower. The relative abundance of Roseburia, Ruminococcaceae andLachnospira was significantly increased while Fusobacteriaceae was decreased afterpatients were treated with AZA. In the AZA plus prednisolone group, the relativeabundance of Lactobacillus, Ruminococcus and Lachnospiraceae was increased while thatof Fusobacterium and Bacillaceae was decreased after treatment. In the thalidomidegroup, the relative abundance of Lactobacillus and Roseburia was also increased aftertreatment (Supplement Table 2). Collectively, these alterations in microbiotacomposition between Before and After group were similar among the fourmedications.Spearman correlation test was performed to evaluate the relationships among thegenera identified in MDI. Significant positive correlations were found in the generadepleted in the Before group including Lachnospira,Roseburia,Anaerostipes,Ruminococcus, which were abundant in HC, suggesting their synergy as commensalbacteria in maintaining gut microbiota homeostasis and promoting the mucosalhealing process (Figure 3). On the other hand, the genera enriched in the Before groupsuch as Fusobacterium and Bacillaceae showed negative correlations with thosedepleted in the Before group, indicating an antagonistic relationship between harmfulbacteria in the active stage and beneficial bacteria in the remission stage.Microbial functions altered during CD treatmentTo infer the metagenome functional content based on the microbial communityprofiles obtained from the 16S rRNA gene sequences, we used PICRUSt[22]. Thepathways including Lipopolysaccharide (LPS) biosynthesis proteins and LPSbiosynthesis, which were enriched in patients before treatment compared to HC,tended to decrease after the induction of remission (Figures 4A and S4). On the otherhand, the pathways including Folate biosynthesis, Starch and sucrose metabolism aswell as Glycolysis/Gluconeogenesis which were deficient in active CD patientstended to increase after treatment and approached that of HC. Intriguingly, theabundance of LPS biosynthesis proteins and LPS biosynthesis were negativelycorrelated with three genera including Roseburia, Ruminococcus and Lachnospira, whichwere more abundant in HC and patients in remission, suggesting their potential rolein anti-inflammation in CD (Figure 4B-D).Figure 1 Richness and diversity in the mucosa-associated microbiota of the patients with Crohn’s disease and healthy controls before and after induction of remission. A: The number of observed species was 388.26 ± 94.22 in the Before group, 475.03 ± 96.01 in the After group and 547.85 ± 52.85 in the healthy controls (HC) group. The Chao1 index was 617.78 ± 161.04 in the Before group, 771.40 ± 146.62 in the After group and 864.08 ± 91.59 in the HC group; B: Plots shown were generated using the weighted version of the UniFrac-based Principal coordinate analysis. Samples from After group (green triangle) clustered separately from Before group (blue circle) while got close to the HC group (red square). HC: Healthy controls.DISCUSSIONIn the current study, we analyzed, using a 16S rRNA sequencing approach, thealterations of the gut mucosal microbiota in CD patients during their treatment. Thecomparison from the same cohort showed that the composition of mucosa-associatedmicrobiota changed significantly after the induction of remission, with increaseddiversity as well as a restoration of potential beneficial bacteria. The MDI that wasidentified using differential microbiota between patients before and after treatmentshowed the correlation of microbial dysbiosis with disease activity.Accumulating evidence has demonstrated the disorder of gut microbiota in CD,and this disorder is considered as an essential factor in driving inflammation [7,23]. Thegut microbial community of CD patients is characterized by reduced diversity as wellas compositional changes in phylum level, including a decreased abundance ofFirmicutes and an increased abundance of Proteobacteria when compared to HC [24].However, it remains unclear whether these alterations of gut microbiota areassociated with disease activity. Consistent with previous studies, we found thedysbiosis of mucosa-associated microbiota in patients with CD and then analyzed itscomposition before and after the induction of remission. Due to the distinctmicrobiome signatures in different sub-phenotypes of CD, we enrolled the patientswith the same behavioral phenotype to exclude bias [25]. Both the alpha and beta diversity showed that the structure of gut microbiota in patients before treatment wasHe C et al. Crohn’s disease and gut microbiotaFigure 2 The microbial dysbiosis index characterizes the activity of Crohn’s disease. A: The composition of mucosa-associated microbiota at phylum level; B:He C et al. Crohn’s disease and gut microbiotaHe C et al. Crohn’s disease and gut microbiota The heatmap of 65 differentially abundant genera between patients before and after treatment. Each column represented a mucosal sample from patients before and after treatment as well as healthy controls. The first letter means the site of the colon (L: Ascending colon; R: Descending colon; i: Terminal ileum; Z: Rectum); C: The identified 65 genera were used to calculate the microbial dysbiosis index (MDI). The Pearson correlation analysis was constructed between MDI and the Crohn’s disease activity index as well as MDI and Chao index. MDI: Microbial dysbiosis index; HC: Healthy controls; CDAI: Crohn’s disease activity index.significantly different from those after treatment, approaching that of HC andindicating the partial restoration of microbial balance after treatment. A previousstudy by Wang et al[9] reported the dynamic changes of fecal microbiota during IFXtherapy in pediatric CD, and IFX has been demonstrated to diminish CD-associatedgut microbial dysbiosis. Another earlier study using a polymerase chain reaction-denaturing gradient gel electrophoresis also found that treatment with Adalimumabinduced short-term changes in the microbiota composition, and these changes seem toparallel the partial recovery of the gut bacterial ecology[26]. AZA is the most commonlyemployed 6-mercaptopurines drug, and these drugs have been found to exert anti-inflammatory effects by targeting not only human macrophages but also the gutmicrobiota linked to CD[27]. Consistent with these previous findings, the present studyshowed that the mucosa-associated gut microbiota changed after treatment,regardless of the drug used, and thus we speculate that the alterations of gutmicrobiota may be associated with the change in disease status from active toremission. The causal relationship between disease activity and microbiota, however,needs further investigation using a germ-free animal model.To further clarify the critical taxa that may be associated with the activity of CD, weidentified 65 genera showing significant difference before and after treatment, andthese genera were used to calculate the MDI. Interestingly, the positive correlationbetween MDI and CDAI indicates that the activity of CD may be associated with thedysbiosis of gut microbiota. A previous study in treatment-naïve children with CDalso described the MDI using the differential taxa between CD and healthy subjects,and then demonstrated that the MDI characterized CD severity[28]. Some MDI-associated taxa were common to both studies including Fusobacterium, Lachnospira,Ruminococcus and Parabacteroides. The relative abundance of Lachnospira, Ruminococcusand Roseburia, which are known to produce short chain fatty acids (SCFAs) wassignificantly increased in patients with clinical remission compared to those withactive CD. SCFAs, which are mainly composed of acetate, propionate and butyrate,are the end products of the fermentation of dietary fiber by the gut microbiota andhave been shown to exert multiple beneficial effects on mammalian energymetabolism[29]. Recently, numerous studies have shown the loss of SCFA-producingtaxa in CD and that IFX treatment was able to restore their levels in responsivepatients, indicating their association with disease severity[9,24,30]. The beneficial effect ofSCFAs on CD is probably due to their anti-inflammation capacity which isdocumented both in vitro and in vivo[31]. Chronic inflammation is a hallmark of CD andresults from the recruitment and activation of immune cells from the circulation.Butyrate elicits anti-inflammatory effects via the inhibition of IL-12 and theupregulation of IL-10 production in human monocytes, repressing production of pro-inflammatory molecules TNF-α, IL-1β, nitric oxide, and reducing NF-κBactivation[32,33]. A clinical study explored the therapeutic effect of butyrate on patientswith CD and found that the administration of butyrate induced clinical improvementand remission in 53% of patients, in whom butyrate successfully downregulatedmucosal levels of NF-κB and IL-1β[34]. Thus, it is conceivable to modulate the dysbioticgut microbiota using probiotics, prebiotics and fecal microbiota transplantation (FMT)for the management of CD. Several studies have reported the potential of FMT for CDtreatment, and we speculate that it may helpful to select donors with a highabundance of the beneficial bacteria, which are deficient in patients to improve thetherapeutic efficacy[35].Analysis of the inferred metagenome in our study showed that the abundance ofLPS biosynthesis proteins and the LPS biosynthesis pathway in patients with CD weresignificantly decreased after treatment while the abundance of Folate biosynthesis,glycolysis/gluconeogenesis, starch and sucrose metabolism were increased,suggesting that the induction of remission could partially rectify the dysbiosis of gutmicrobiota and restore the homeostasis of metabolic function. LPS, one importantcomponent in the outer membrane of gram-negative bacteria, plays a critical role intriggering inflammatory responses that could further result in various diseases suchas CD[36]. The serum levels of LPS were demonstrated to increased markedly in activeCD patients compared with patients in remission and HC and were positivelycorrelated with the severity of the disease[37]. Moreover, the blockade of intestinalmucosal inflammation with IFX could reduce the levels of LPS and IFX has beenreported to diminish the CD-associated gut microbial dysbiosis[9,37]. Analysis of。