头孢类新药ceftaroline
头孢洛林杂质种类整理列表

头孢洛林杂质列表中文名称:头孢洛林英文名称:Ceftaroline fosamilCAS No.: 400827-46-5分子式: C22H21N8O8PS4分子量: 684.69[中文名]头孢洛林杂质5英文名:Ceftaroline Fosamil Impurity 5CAS No.: 953037-71-3分子式:C22H20N8O5S4规格:10mg-25mg-50mg-100mg用途:项目报批纯度高于99.89%湖北扬信医药(现货)供应各种杂质对照品:泊沙康唑杂质、替卡格雷杂质、依折麦布杂质、索拉菲尼相关杂质、索非布韦杂质、氨氯地平杂质、Q2-853-78-6-052马来酸氯苯那敏杂质、头孢克肟杂质、瑞舒伐他汀杂质、瑞格列奈杂质等;代理中检所/EP/BP/USP/LGC/TRC/DR/TLC/MC/SIGMA/BACHEM等品牌湖北扬信医药专注各种杂质对照品、原研制剂用途:项目报批并提供COA、NMR、HPLC、MS等图谱。
详情请点击用户名[中文名]头孢洛林杂质1英文名:Ceftaroline Fosamil Impurity 1CAS No.: 1277090-03-5分子式:C28H34N12O10PS4规格:10mg-25mg-50mg-100mg用途:项目报批纯度高于99.89%[中文名]头孢洛林杂质2英文名:Ceftaroline Fosamil Impurity 2CAS No.: 1277090-04-6分子式:C28H34N12O10PS4规格:10mg-25mg-50mg-100mg用途:项目报批纯度高于99.89%[中文名]头孢洛林杂质3英文名:Ceftaroline Fosamil Impurity 3 CAS No.: 1286218-63-0分子式:C22H23N8O9PS4规格:10mg-25mg-50mg-100mg用途:项目报批纯度高于99.89%[中文名]头孢洛林杂质4英文名:Ceftaroline Fosamil Impurity 4 CAS No.: 1286218-64-1分子式:C22H22N8O11P2S4规格:10mg-25mg-50mg-100mg用途:项目报批纯度高于99.89%。
注射用头孢洛林酯说明书(美国,英文)

1 23 4 5 678 91011 12 1314151617 18192021 22 23242554HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TEFLARO safely and effectively. See full prescribing information for TEFLARO®.TEFLARO® (ceftaroline fosamil) injection for intravenous (IV) use Initial U.S. Approval: 2010To reduce the development of drug-resistant bacteria and maintain theeffectiveness of Teflaro and other antibacterial drugs, Teflaro should be used onlyto treat infections that are proven or strongly suspected to be caused by bacteria.-----------------------RECENT MAJOR CHANGES------------------------------------ Dosage and Administration (2.3) XX/2012 --------------------------INDICATIONS AND USAGE--------------------------------Teflaro ® is a cephalosporin antibacterial indicated for the treatment of the following infections caused by designated susceptible bacteria:• Acute bacterial skin and skin structure infections (ABSSSI)(1.1) • Community-acquired bacterial pneumonia (CABP) (1.2) ------------------------DOSAGE AND ADMINISTRATION-------------------------• 600 mg every 12 hours by IV infusion administered over 1 hour in adults ≥ 18 years of age (2.1) • Dosage adjustment in patients with renal impairment (2.2)Estimated CreatinineClearance # (mL/min) Teflaro Dosage Regimen > 50 No dosage adjustment necessary > 30 to ≤ 50 400 mg IV (over 1 hour) every 12 hours ≥ 15 to ≤ 30 300 mg IV (over 1 hour) every 12 hours End-stage renal disease (ESRD), including hemodialysis200 mg IV (over 1 hour) every 12 hours#As calculated using the Cockcroft-Gault formula -----------------------DOSAGE FORMS AND STRENGTHS -----------------------600 mg or 400 mg of sterile Teflaro powder in single-use 20 mL vials. (3) 26--------------------------CONTRAINDICATIONS---------------------------- 27 ∙Known serious hypersensitivity to ceftaroline or other members of28 the cephalosporin class. (4)29 -----------------------WARNINGS AND PRECAUTIONS----------------- 30 ∙Serious hypersensitivity (anaphylactic) reactions have been31 reported with beta-lactam antibiotics, including ceftaroline. 32 Exercise caution in patients with known hypersensitivity to beta33 lactam antibiotics. (5.1) 34 ∙Clostridium difficile -associated diarrhea (CDAD) has been35 reported with nearly all systemic antibacterial agents, including36 Teflaro. Evaluate if diarrhea occurs. (5.2)37 ∙Direct Coombs’ test seroconversion has been reported with38 Teflaro. If anemia develops during or after therapy, a diagnostic 39 workup for drug-induced hemolytic anemia should be performed 40 and consideration given to discontinuation of Teflaro. (5.3) 41 -----------------------------ADVERSE REACTIONS------------------------42 The most common adverse reactions occurring in >2 % of patients are 43 diarrhea, nausea, and rash. (6.3) 44 45 To report SUSPECTED ADVERSE REACTIONS, contact Forest46 Pharmaceuticals, Inc., at 1-800-678-1605 or FDA at 1-800-FDA47 1088 or /medwatch. 48 ---------------------------USE IN SPECIFIC POPULATIONS-------------49 ∙Dosage adjustment is required in patients with moderate or severe50 renal impairment and in ESRD patients, including patients on51 hemodialysis.(2.2, 12.3) 52 53See 17 for PATIENT COUNSELING INFORMATIONRevised:XX/2012 5556 FULL PRESCRIBING INFORMATION: CONTENTS* 84 8.4 Pediatric Use85 8.5 Geriatric Use 57 1 INDICATIONS AND USAGE86 8.6 Patients with Renal Impairment58 1.1 Acute Bacterial Skin and Skin Structure 87 10 OVERDOSAGE59 Infections 88 11 DESCRIPTION 60 1.2 Community-Acquired Bacterial Pneumonia 89 12 CLINICAL PHARMACOLOGY61 1.3 Usage90 12.1 Mechanism of Action62 2 DOSAGE ANDADMINISTRATION 91 12.2 Pharmacodynamics 63 2.1 Recommended Dosage 92 12.3 Pharmacokinetics64 2.2 Patients with Renal Impairment 93 12.4 Microbiology65 2.3 Preparation of Solutions 94 13 NONCLINICAL TOXICOLOGY66 3 DOSAGE FORMS AND STRENGTHS 95 13.1 Carcinogenesis,Mutagenesis, Impairment of 67 4 CONTRAINDICATIONS 96 Fertility 68 5 WARNINGS AND PRECAUTIONS 97 14 CLINICAL TRIALS69 5.1 Hypersensitivity Reactions 98 14.1 Acute Bacterial Skin and Skin Structure70 5.2 Clostridium difficile -associated Diarrhea 99 Infections71 5.3 Direct Coombs’ Test Seroconversion 100 14.2 Community-Acquired Bacterial Pneumonia72 5.4 Development of Drug-Resistant Bacteria 101 15 REFERENCES 73 6 ADVERSE REACTIONS 102 16 HOW SUPPLIED/STORAGE AND HANDLING 74 6.1 Adverse Reactions from Clinical Trials 103 17 PATIENT COUNSELING INFORMATION 75 6.2 Serious Adverse Events and Adverse 10476 Events Leading to Discontinuation 77 6.3 Most Common Adverse Reactions 10578 6.4 Other Adverse Reactions Observed During 106 *Sections or subsections omitted from the full prescribing information79 Clinical Trials of Teflaro107 are not listed.80 7 DRUGINTERACTIONS 81 8 USE IN SPECIFIC POPULATIONS82 8.1 Pregnancy83 8.3 Nursing MothersPage 1 of 13108 FULL PRESCRIBING INFORMATION 109 1. INDICATIONS AND USAGE110 Teflaro® (ceftaroline fosamil) is indicated for the treatment of patients with the following infections caused by susceptible isolates of the designated 111 microorganisms. 112 1.1Acute Bacterial Skin and Skin Structure Infections113 Teflaro is indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI) caused by susceptible isolates of the following Gram114 positive and Gram-negative microorganisms:Staphylococcus aureus (including methicillin-susceptible and -resistant isolates), Streptococcus pyogenes ,115 Streptococcus agalactiae , Escherichia coli , Klebsiella pneumoniae, and Klebsiella oxytoca. 116 1.2Community-Acquired Bacterial Pneumonia117 Teflaro is indicated for the treatment of community-acquired bacterial pneumonia (CABP) caused by susceptible isolates of the following Gram-positive118 and Gram-negative microorganisms: Streptococcus pneumoniae (including cases with concurrent bacteremia),Staphylococcus aureus (methicillin119 susceptible isolates only), Haemophilus influenzae, Klebsiella pneumoniae, Klebsiella oxytoca, and Escherichia coli. 120 1.3 Usage121 To reduce the development of drug-resistant bacteria and maintain the effectiveness of Teflaro and other antibacterial drugs, Teflaro should be used to 122 treat only ABSSSI or CABP that are proven or strongly suspected to be caused by susceptible bacteria. Appropriate specimens for microbiological123 examination should be obtained in order to isolate and identify the causative pathogens and to determine their susceptibility to ceftaroline. When culture124 and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local125 epidemiology and susceptibility patterns may contribute to the empiric selection of therapy. 126 2. DOSAGE AND ADMINISTRATION 127 2.1Recommended Dosage128 The recommended dosage of Teflaro is 600 mg administered every 12 hours by intravenous (IV) infusion over 1 hour in patients ≥ 18 years of age. The129 duration of therapy should be guided by the severity and site of infection and the patient’s clinical and bacteriological progress. 130 The recommended dosage and administration by infection is described in Table 1.131Table 1: Dosage of Teflaro by InfectionInfection Dosage FrequencyInfusion Time(hours)RecommendedDuration ofTotal Antimicrobial TreatmentAcute Bacterial Skin and Skin Structure Infection(ABSSSI) 600 mg Every 12 hours 1 5-14 days Community-Acquired Bacterial Pneumonia (CABP)600 mg Every 12 hours 1 5-7 days 132133 2.2 Patients with Renal Impairment 134Table 2: Dosage of Teflaro in Patients with Renal Impairment 135 136 137 138 139 140 141Estimated CrCl a (mL/min) Recommended Dosage Regimen for Teflaro> 50No dosage adjustment necessary > 30 to ≤ 50 400 mg IV (over 1 hour) every 12 hours ≥ 15 to ≤ 30 300 mg IV (over 1 hour) every 12 hours End-stage renal disease,including hemodialysis b 200 mg IV (over 1 hour) every 12 hours c ab End-stage renal disease is defined as CrCl < 15 mL/min.cTeflaro is hemodialyzable; thus Teflaro should be administered after hemodialysis on hemodialysis days.2.3 Preparation of SolutionsAseptic technique must be followed in preparing the infusion solution. The contents of Teflaro vial should be constituted with 20 mL Sterile Water forInjection, USP; or 0.9% of sodium chloride injection (normal saline); or 5% of dextrose injection; or lactated ringer’s injection . The preparation of Teflaro solutions is summarized in Table 3.143 Table 3: Preparation of Teflaro for Intravenous UseDosage Strength(mg) Volume of Diluent To BeAdded(mL)Approximate Ceftarolinefosamil Concentration(mg/mL)Amount to Be Withdrawn400 20 20 Total Volume600 20 30 Total Volume144145 The constituted solution must be further diluted in 250 mL before infusion. Use the same diluent for this further dilution, unless sterile water for 146 injection was used earlier. If sterile water for injection was used earlier, then appropriate infusion solutions include: 0.9% Sodium Chloride 147 Injection, USP (normal saline); 5% Dextrose Injection, USP; 2.5% Dextrose Injection, USP, and 0.45% Sodium Chloride Injection, USP; or Lactated 148 Ringer’s Injection, USP. The resulting solution should be administered over approximately 1 hour.149 Constitution time is less than 2 minutes. Mix gently to constitute and check to see that the contents have dissolved completely. Parenteral drug products 150 should be inspected visually for particulate matter prior to administration.151 The color of Teflaro infusion solutions ranges from clear, light to dark yellow depending on the concentration and storage conditions. When stored as 152 recommended, the product potency is not affected.153 Studies have shown that the constituted solution in the infusion bag should be used within 6 hours when stored at room temperature or within 24 hours 154 when stored under refrigeration at 2 to 8º C (36 to 46º F).155 The compatibility of Teflaro with other drugs has not been established. Teflaro should not be mixed with or physically added to solutions containing other 156 drugs.157 3. DOSAGE FORMS AND STRENGTHS158 Teflaro is supplied in single-use, clear glass vials containing either 600 mg or 400 mg of sterile ceftaroline fosamil powder.159 4. CONTRAINDICATIONS160 Teflaro is contraindicated in patients with known serious hypersensitivity to ceftaroline or other members of the cephalosporin class. Anaphylaxis and 161 anaphylactoid reactions have been reported with ceftaroline.162 5. WARNINGS AND PRECAUTIONS163 5.1 Hypersensitivity Reactions164 Serious and occasionally fatal hypersensitivity (anaphylactic) reactions and serious skin reactions have been reported in patients receiving beta-lactam 165 antibacterials. Before therapy with Teflaro is instituted, careful inquiry about previous hypersensitivity reactions to other cephalosporins, penicillins, or 166 carbapenems should be made. If this product is to be given to a penicillin- or other beta-lactam-allergic patient, caution should be exercised because cross 167 sensitivity among beta-lactam antibacterial agents has been clearly established.168 If an allergic reaction to Teflaro occurs, the drug should be discontinued. Serious acute hypersensitivity (anaphylactic) reactions require emergency 169 treatment with epinephrine and other emergency measures, that may include airway management, oxygen, intravenous fluids, antihistamines, 170 corticosteroids, and vasopressors as clinically indicated.171 5.2 Clostridium difficile-associated Diarrhea172 Clostridium difficile-associated diarrhea (CDAD) has been reported for nearly all systemic antibacterial agents, including Teflaro, and may range in 173 severity from mild diarrhea to fatal colitis.174 Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of C. difficile.175 C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin-producing strains of C. difficile cause increased 176 morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all 177 patients who present with diarrhea following antibiotic use. Careful medical history is necessary because CDAD has been reported to occur more than 2 178 months after the administration of antibacterial agents.179 If CDAD is suspected or confirmed, antibacterials not directed against C. difficile should be discontinued, if possible. Appropriate fluid and electrolyte 180 management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated [see Adverse 181 Reactions (6.3)].182 5.3 Direct Coombs’ Test Seroconversion183 Seroconversion from a negative to a positive direct Coombs’ test result occurred in 120/1114 (10.8%) of patients receiving Teflaro and 49/1116 (4.4%) of 184 patients receiving comparator drugs in the four pooled Phase 3 trials.185 In the pooled Phase 3 CABP trials, 51/520 (9.8%) of Teflaro-treated patients compared to 24/534 (4.5%) of ceftriaxone-treated patients seroconverted 186 from a negative to a positive direct Coombs’ test result. No adverse reactions representing hemolytic anemia were reported in any treatment group.187 If anemia develops during or after treatment with Teflaro, drug-induced hemolytic anemia should be considered. Diagnostic studies including a direct 188 Coombs’ test, should be performed. If drug-induced hemolytic anemia is suspected, discontinuation of Teflaro should be considered and supportive care 189 should be administered to the patient (i.e. transfusion) if clinically indicated.191192 5.4 Development of Drug-Resistant Bacteria193 Prescribing Teflaro in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk 194 of the development of drug-resistant bacteria.195 6. ADVERSEREACTIONS196 The following serious events are described in greater detail in the Warnings and Precautions section197 ∙Hypersensitivity reactions [see Warnings and Precautions (5.1)]198 ∙Clostridium difficile-associated diarrhea [see Warnings and Precautions (5.2)]199 ∙Direct Coombs’ test seroconversion [see Warnings and Precautions (5.3)]200 6.1 Adverse Reactions from Clinical Trials201 Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be compared 202 directly to rates from clinical trials of another drug and may not reflect rates observed in practice.203 Teflaro was evaluated in four controlled comparative Phase 3 clinical trials (two in ABSSSI and two in CABP) which included 1300 adult patients treated 204 with Teflaro (600 mg administered by IV over 1 hour every 12h) and 1297 patients treated with comparator (vancomycin plus aztreonam or ceftriaxone) 205 for a treatment period up to 21 days. The median age of patients treated with Teflaro was 54 years, ranging between 18 and 99 years old. Patients treated 206 with Teflaro were predominantly male (63%) and Caucasian (82%).207 6.2 Serious Adverse Events and Adverse Events Leading to Discontinuation208 In the four pooled Phase 3 clinical trials, serious adverse events occurred in 98/1300 (7.5%) of patients receiving Teflaro and 100/1297 (7.7%) of patients 209 receiving comparator drugs. The most common SAEs in both the Teflaro and comparator treatment groups were in the respiratory and infection system 210 organ classes (SOC). Treatment discontinuation due to adverse events occurred in 35/1300 (2.7%) of patients receiving Teflaro and 48/1297 (3.7%) of 211 patients receiving comparator drugs with the most common adverse events leading to discontinuation being hypersensitivity for both treatment groups at a 212 rate of 0.3% in the Teflaro group and 0.5% in comparator group.213 6.3 Most Common Adverse Reactions214 No adverse reactions occurred in greater than 5% of patients receiving Teflaro. The most common adverse reactions occurring in > 2% of patients 215 receiving Teflaro in the pooled phase 3 clinical trials were diarrhea, nausea, and rash.216 Table 4 lists adverse reactions occurring in ≥ 2% of patients receiving Teflaro in the pooled Phase 3 clinical trials.217 Table 4: Adverse Reactions Occurring in ≥ 2% of Patients Receiving Teflaro in the Pooled Phase 3 Clinical TrialsSystem Organ Class/ Preferred TermPooled Phase 3 Clinical Trials(four trials, two in ABSSSI and two in CABP)Teflaro(N=1300)Pooled Comparators a(N=1297) Gastrointestinal disordersDiarrhea 5 % 3 %Nausea 4 % 4 %Constipation 2 % 2 %Vomiting 2 % 2 %InvestigationsIncreased transaminases 2% 3 %Metabolism and nutrition disordersHypokalemia 2 % 3 %Skin and subcutaneous tissue disordersRash 3%2%Vascular disordersPhlebitis 2%1% 218 a219 IV every 24h in the Phase 3 CABP trials.220221222 6.4 Other Adverse Reactions Observed During Clinical Trials of Teflaro223 Following is a list of additional adverse reactions reported by the 1740 patients who received Teflaro in any clinical trial with incidences less than 2%. 224 Events are categorized by System Organ Class.225 Blood and lymphatic system disorders - Anemia, Eosinophilia, Neutropenia, Thrombocytopenia226 Cardiac disorders - Bradycardia, Palpitations227 Gastrointestinal disorders -Abdominal pain228 General disorders and administration site conditions - Pyrexia229 Hepatobiliary disorders - Hepatitis230 Immune system disorders - Hypersensitivity, Anaphylaxis231 Infections and infestations -Clostridium difficile colitis232 Metabolism and nutrition disorders - Hyperglycemia, Hyperkalemia233 Nervous system disorders -Dizziness, Convulsion234 Renal and urinary disorders - Renal failure235 Skin and subcutaneous tissue disorders - Urticaria236 7. DRUGINTERACTIONS237 No clinical drug-drug interaction studies have been conducted with Teflaro. There is minimal potential for drug-drug interactions between Teflaro and 238 CYP450 substrates, inhibitors, or inducers; drugs known to undergo active renal secretion; and drugs that may alter renal blood flow [see Clinical 239 Pharmacology (12.3)].240 8. USE IN SPECIFIC POPULATIONS241 8.1 Pregnancy242 Category B243 Developmental toxicity studies performed with ceftaroline fosamil in rats at IV doses up to 300 mg/kg demonstrated no maternal toxicity and no effects 244 on the fetus. A separate toxicokinetic study showed that ceftaroline exposure in rats (based on AUC) at this dose level was approximately 8 times the 245 exposure in humans given 600 mg every 12 hours. There were no drug-induced malformations in the offspring of rabbits given IV doses of 25, 50, and 246 100 mg/kg, despite maternal toxicity. Signs of maternal toxicity appeared secondary to the sensitivity of the rabbit gastrointestinal system to broad247 spectrum antibacterials and included changes in fecal output in all groups and dose-related reductions in body weight gain and food consumption at > 50 248 mg/kg; these were associated with an increase in spontaneous abortion at 50 and 100 mg/kg. The highest dose was also associated with maternal 249 moribundity and mortality. An increased incidence of a common rabbit skeletal variation, angulated hyoid alae, was also observed at the maternally toxic 250 doses of 50 and 100 mg/kg. A separate toxicokinetic study showed that ceftaroline exposure in rabbits (based on AUC) was approximately 0.8 times the 251 exposure in humans given 600 mg every 12 hours at 25 mg/kg and 1.5 times the human exposure at 50 mg/kg.252 Ceftaroline fosamil did not affect the postnatal development or reproductive performance of the offspring of rats given IV doses up to 450 mg/kg/day. 253 Results from a toxicokinetic study conducted in pregnant rats with doses up to 300 mg/kg suggest that exposure was ≥ 8 times the exposure in humans 254 given 600 mg every 12 hours.255 There are no adequate and well-controlled trials in pregnant women. Teflaro should be used during pregnancy only if the potential benefit justifies the 256 potential risk to the fetus.257 8.3 Nursing Mothers258 It is not known whether ceftaroline is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Teflaro 259 is administered to a nursing woman.260 8.4 Pediatric Use261 Safety and effectiveness in pediatric patients have not been established.262 8.5 Geriatric Use263 Of the 1300 patients treated with Teflaro in the Phase 3 ABSSSI and CABP trials, 397 (30.5%) were ≥65 years of age. The clinical cure rates in the 264 Teflaro group (Clinically Evaluable [CE] Population) were similar in patients ≥65 years of age compared with patients < 65 years of age in both the 265 ABSSSI and CABP trials.266 The adverse event profiles in patients ≥ 65 years of age and in patients < 65 years of age were similar. The percentage of patients in the Teflaro group who 267 had at least one adverse event was 52.4% in patients ≥ 65 years of age and 42.8% in patients < 65 years of age for the two indications combined.268 Ceftaroline is excreted primarily by the kidney, and the risk of adverse reactions may be greater in patients with impaired renal function. Because elderly 269 patients are more likely to have decreased renal function, care should be taken in dose selection in this age group and it may be useful to monitor renal 270 function. Elderly subjects had greater ceftaroline exposure relative to non-elderly subjects when administered the same single dose of Teflaro. However, 271 higher exposure in elderly subjects was mainly attributed to age-related changes in renal function. Dosage adjustment for elderly patients should be based 272 on renal function [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)].275 8.6 Patients with Renal Impairment276 Dosage adjustment is required in patients with moderate (CrCl > 30 to ≤50 mL/min) or severe (CrCl ≥ 15 to ≤30 mL/min) renal impairment and in 277 patients with end-stage renal disease (ESRD – defined as CrCl < 15 mL/min), including patients on hemodialysis (HD) [see Dosage and Administration 278 (2.2) and Clinical Pharmacology (12.3)].279 10. OVERDOSAGE280 In the event of overdose, Teflaro should be discontinued and general supportive treatment given.281 Ceftaroline can be removed by hemodialysis. In subjects with ESRD administered 400 mg of Teflaro, the mean total recovery of ceftaroline in the 282 dialysate following a 4-hour hemodialysis session started 4 hours after dosing was 76.5 mg (21.6% of the dose). However, no information is available on 283 the use of hemodialysis to treat overdosage [see Clinical Pharmacology (12.3)].284 11. DESCRIPTION285 Teflaro is a sterile, semi-synthetic, broad-spectrum, prodrug antibacterial of cephalosporin class of beta-lactams (β-lactams). Chemically, the prodrug, 286 ceftaroline fosamil monoacetate monohydrate is (6R,7R)-7-{(2Z)-2-(ethoxyimino)-2-[5-(phosphonoamino)-1,2,4-thiadiazol-3-yl]acetamido}-3-{[4-(1287 methylpyridin-1-ium-4-yl)-1,3-thiazol-2-yl]sulfanyl}-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate monoacetate monohydrate. Its molecular 288 weight is 762.75. The empirical formula is C22H21N8O8PS4.C2H4O2.H2O.289 Figure 1: Chemical structure of ceftaroline fosamil290291292293294295296297298299300 301 302 Teflaro vials contain either 600 mg or 400 mg of anhydrous ceftaroline fosamil. The powder for injection is formulated from ceftaroline fosamil monoacetate monohydrate, a pale yellowish-white to light yellow sterile powder. All references to ceftaroline activity are expressed in terms of the prodrug, ceftaroline fosamil. The powder is constituted for IV injection [see Dosage and Administration (2.3)].303 Each vial of Teflaro contains ceftaroline fosamil and L-arginine, which results in a constituted solution at pH 4.8 to 6.5. 304 12. CLINICAL PHARMACOLOGY305 Ceftaroline fosamil is the water-soluble prodrug of the bioactive ceftaroline [see Clinical Pharmacology (12.3)]. 306 12.1 Mechanism of Action307 Ceftaroline is an antibacterial drug [see Clinical Pharmacology (12.4)].308 12.2 Pharmacodynamics309 310 311 As with other beta-lactam antimicrobial agents, the time that unbound plasma concentration of ceftaroline exceeds the minimum inhibitory concentration (MIC) of the infecting organism has been shown to best correlate with efficacy in a neutropenic murine thigh infection model with S. aureus and S. pneumoniae.312 313 314 Exposure-response analysis of Phase 2/3 ABSSSI trials supports the recommended dosage regimen of Teflaro 600 mg every 12 hours by IV infusion over 1 hour. For Phase 3 CABP trials, an exposure-response relationship could not be identified due to the limited range of ceftaroline exposures in the majority of patients.315 Cardiac Electrophysiology316 317 318 In a randomized, positive- and placebo-controlled crossover thorough QTc study, 54 healthy subjects were each administered a single dose of Teflaro 1500 mg, placebo, and a positive control by IV infusion over 1 hour. At the 1500 mg dose of Teflaro, no significant effect on QTc interval was detected at peak plasma concentration or at any other time.319 12.3 Pharmacokinetics320 321 322 The mean pharmacokinetic parameters of ceftaroline in healthy adults (n=6) with normal renal function after single and multiple 1-hour IV infusions of 600 mg ceftaroline fosamil administered every 12 hours are summarized in Table 5. Pharmacokinetic parameters were similar for single and multiple dose administration.323326 Table 5: Mean (Standard Deviation) Pharmacokinetic Parameters of Ceftaroline IV in Healthy AdultsParameter Single 600 mg Dose Administered asa 1-Hour Infusion(n=6)Multiple 600 mg Doses Administered Every12 Hours as 1-Hour Infusions for 14Days(n=6)C max (mcg/mL) 19.0 (0.71) 21.3 (4.10)T max (h)a 1.00 (0.92-1.25) 0.92 (0.92-1.08)AUC (mcg h/mL) b 56.8 (9.31) 56.3 (8.90)T1/2 (h) 1.60 (0.38) 2.66 (0.40)CL (L/h) 9.58 (1.85) 9.60 (1.40)a Reported as median (range)b AUC0-∞,for single-dose administration; AUC0-tau, for multiple-dose administration; C max, maximum observed concentration; T max, time of C max; AUC0-∞, area under concentration-time curve from time 0 to infinity; AUC0-tau, area under concentration-time curveover dosing interval (0-12 hours); T1/2, terminal elimination half-life; CL, plasma clearance327328 The C max and AUC of ceftaroline increase approximately in proportion to dose within the single dose range of 50 to 1000 mg. No appreciable 329 accumulation of ceftaroline is observed following multiple IV infusions of 600 mg administered every 12 hours for up to 14 days in healthy adults with 330 normal renal function.331 Distribution332 The average binding of ceftaroline to human plasma proteins is approximately 20% and decreases slightly with increasing concentrations over 1-50 333 mcg/mL (14.5-28.0%). The median (range) steady-state volume of distribution of ceftaroline in healthy adult males (n=6) following a single 600 mg IV 334 dose of radiolabeled ceftaroline fosamil was 20.3 L (18.3-21.6 L), similar to extracellular fluid volume.335 Metabolism336 Ceftaroline fosamil is converted into bioactive ceftaroline in plasma by a phosphatase enzyme and concentrations of the prodrug are measurable in plasma 337 primarily during IV infusion. Hydrolysis of the beta-lactam ring of ceftaroline occurs to form the microbiologically inactive, open-ring metabolite 338 ceftaroline M-1. The mean (SD) plasma ceftaroline M-1 to ceftaroline AUC0-∞ ratio following a single 600 mg IV infusion of ceftaroline fosamil in 339 healthy adults (n=6) with normal renal function is 28% (3.1%).340 When incubated with pooled human liver microsomes, ceftaroline was metabolically stable (< 12% metabolic turnover), indicating that ceftaroline is not a 341 substrate for hepatic CYP450 enzymes.342 Excretion343 Ceftaroline and its metabolites are primarily eliminated by the kidneys. Following administration of a single 600 mg IV dose of radiolabeled ceftaroline 344 fosamil to healthy male adults (n=6), approximately 88% of radioactivity was recovered in urine and 6% in feces within 48 hours. Of the radioactivity 345 recovered in urine approximately 64% was excreted as ceftaroline and approximately 2% as ceftaroline M-1. The mean (SD) renal clearance of ceftaroline 346 was 5.56 (0.20) L/h, suggesting that ceftaroline is predominantly eliminated by glomerular filtration.347 Specific Populations348 Renal Impairment349 Following administration of a single 600 mg IV dose of Teflaro, the geometric mean AUC0-∞ of ceftaroline in subjects with mild (CrCl > 50 to ≤ 80 350 mL/min, n=6) or moderate (CrCl > 30 to ≤50 mL/min, n=6) renal impairment was 19% and 52% higher, respectively, compared to healthy subjects with 351 normal renal function (CrCl > 80 mL/min, n=6). Following administration of a single 400 mg IV dose of Teflaro, the geometric mean AUC0-∞ of 352 ceftaroline in subjects with severe (CrCl ≥ 15 to ≤30 mL/min, n=6) renal impairment was 115% higher compared to healthy subjects with normal renal 353 function (CrCl > 80 mL/min, n=6). Dosage adjustment is recommended in patients with moderate and severe renal impairment [see Dosage and 354 Administration (2.2)].355 A single 400 mg dose of Teflaro was administered to subjects with ESRD (n=6) either 4 hours prior to or 1 hour after hemodialysis (HD). The geometric 356 mean ceftaroline AUC0-∞ following the post-HD infusion was 167% higher compared to healthy subjects with normal renal function (CrCl > 80 mL/min, 357 n=6). The mean recovery of ceftaroline in the dialysate following a 4-hour HD session was 76.5 mg, or 21.6% of the administered dose. Dosage 358 adjustment is recommended in patients with ESRD (defined as CrCL < 15 mL/min), including patients on HD [see Dosage and Administration (2.2)]. 359 Hepatic Impairment360 The pharmacokinetics of ceftaroline in patients with hepatic impairment have not been established. As ceftaroline does not appear to undergo significant 361 hepatic metabolism, the systemic clearance of ceftaroline is not expected to be significantly affected by hepatic impairment.362 Geriatric Patients363 Following administration of a single 600 mg IV dose of Teflaro to healthy elderly subjects (≥65 years of age, n=16), the geometric mean AUC0-∞ of 364 ceftaroline was ~33% higher compared to healthy young adult subjects (18-45 years of age, n=16). The difference in AUC0-∞ was mainly attributable to。
2024年注射用盐酸头孢替安市场分析现状

2024年注射用盐酸头孢替安市场分析现状引言注射用盐酸头孢替安(Ceftriaxone Sodium)作为一种广泛应用于临床的抗生素药物,具有强效的抗菌能力。
本文旨在分析注射用盐酸头孢替安在市场上的现状,并评估其发展前景。
市场特点市场规模目前,全球注射用盐酸头孢替安市场规模庞大,并且持续增长。
根据行业报告,预计市场规模将以稳定的年均复合增长率增长,达到xx亿美元。
市场竞争注射用盐酸头孢替安市场竞争激烈,主要来自国内外制药企业。
目前,市场上存在多个品牌的注射用盐酸头孢替安,主要包括A公司、B公司和C公司等。
这些企业都在不断努力提高产品质量和研发能力,以获取更高的市场份额。
市场趋势随着全球医疗技术的不断进步和人们对医疗服务的需求增加,注射用盐酸头孢替安市场有望继续保持稳定增长。
同时,随着生物技术的快速发展,新的疗法和药物研发将为市场提供更多创新和增长机会。
市场机遇注射用盐酸头孢替安作为一种广谱抗生素,具有广泛的应用范围,可用于治疗各种感染疾病,为市场带来了巨大的机遇。
此外,随着全球老龄化人口的增加,对抗生素的需求也将进一步增长,为注射用盐酸头孢替安市场提供了有利条件。
市场挑战制度审批在市场发展过程中,注射用盐酸头孢替安需要经过严格的制度审批流程。
这些审批程序可能涉及国内外监管机构的批准,时间周期较长,对企业来说是一项重要而复杂的挑战。
竞争压力由于市场竞争激烈,注射用盐酸头孢替安企业面临着巨大的竞争压力。
为了提高市场份额,企业需要在产品质量、价格、服务等方面提供差异化竞争策略,以获得市场竞争优势。
技术创新在不断发展的医疗行业中,技术创新是市场发展的关键。
企业需要不断投入研发,提高产品技术含量和创新能力,以满足市场需求和应对新的竞争挑战。
市场前景基于上述市场特点和挑战,注射用盐酸头孢替安市场依然具有良好的发展前景。
预计在未来几年内,市场规模将继续增加,并且市场竞争将更加激烈。
企业需要加大技术创新和研发投入,提高产品质量和服务水平,以满足市场需求,获取更大的市场份额。
头孢噻肟说明书

通用名:注射用头孢噻肟钠英文名:CEFOTAXIME SODIUM FOR INJECTION产品类别:药品/化学药品/抗微生物药物用途分类:呼吸系统类主要成分:头孢噻肟钠剂型:注射剂适应症:适用于敏感细菌所致的肺炎及其他下呼吸道感染、尿路感染、脑膜炎、败血症、腹腔感染、盆腔感染、皮肤软组织感染、生殖道感染、骨和关节感染等。
头孢噻肟可以作为小儿脑膜炎的选用药物。
用法用量:成人一日2~6g 分2~3次静脉注射或静脉滴注;严重感染者每6~8小时2~3g一日最高剂量不超过12g。
治疗无并发症的肺炎链球菌肺炎或急性尿路感染每12小时1g。
新生儿日龄小于等于7日者每12小时50mg/kg 出生大于7日者每8小时50mg/kg。
治疗脑膜炎患者剂量可增至每6小时75mg/kg 均以静脉给药。
严重肾功能减退病人应用本品时须适当减量。
血清肌酐值超过424μmol/L(4.8mg)或肌酐清除率低于20ml/分时本品的维持量应减半;血清肌酐超过751μmol/L(8.5mg)时维持量为正常量的1/4。
需血液透析者一日0.5~2g。
但在透析后应加用1次剂量。
产品说明:【性状】本品为白色类白色或微黄白色结晶性粉末。
【药理毒理】头孢噻肟为第三代头孢菌素抗菌谱广对大肠埃希菌、奇异变形杆菌、克雷伯菌属和沙门菌属等肠杆菌科细菌等革兰阴性菌有强大活性。
对普通变形杆菌和枸橼酸杆菌属亦有良好作用。
阴沟肠杆菌、产气肠杆菌对本品比较耐药。
本品对铜绿假单胞菌和产碱杆菌无抗菌活性。
头孢噻肟对流感杆菌、淋病奈瑟菌(包括产β内酰胺酶株)、脑膜炎奈瑟菌和卡他莫拉菌等均有强大作用。
本品对金黄色葡萄球菌的抗菌活性较差对溶血性链球菌、肺炎链球菌等革兰阳性球菌的活性强肠球菌属对本品耐药。
【药代动力学】肌内注射本品0.5g或1.0g后0.5小时达血药峰浓度(Cmax) 分别为12mg/L和25mg/L 8小时后血中仍可测出有效浓度。
于5分钟内静脉注射本品1g或2g 即刻血药峰浓度分别为102mg/L和215mg/L 4小时后2g组尚可测得3.3mg/L。
注射用头孢唑林钠
注射用头孢唑林钠药品名称:【通用名称】注射用头胞唑林钠[药典]【商标名称】钠林【英文名称】 Cefazolin Sodium for Injection [药典]【汉语拼音】Zhu She Yong Tou Bao Zuo Lin Na成份:本品主要成份为头胞唑林钠,化学名称为:(6R,7R)-3-[[(5-甲基-1, 3, 4-嘎二唑-2-基)硫]甲基]-7-[(1H-四唑-1-基)乙酰氨基]-8-氧代-5-硫杂-1-氮杂双环[辛-2-烯-2-甲酸钠盐。
其结构式为:分子式:C14H13N8NaO4S3分子量:所属类别:化药及生物制品 >> 抗微生物药 >> 抗细菌药 >> 抗生素类性状:本品为白色或类白色的粉末或结晶性粉末;无臭。
适应症:适用于治疗敏感细菌所致的支气管炎及肺炎等呼吸道感染、尿路感染、皮肤软组织感染、骨和关节感染、败血症、感染性心内膜炎、肝胆系统感染及眼、耳、鼻、喉科等感染。
本品也可作为外科手术前的预防用药。
本品不宜用于中枢神经系统感染。
对慢性尿路感染,尤其伴有尿路解剖异常者的疗效较差。
本品不宜用于治疗淋病和梅毒。
规格:按 C14H14N8O4S3 计算(1)⑵ 用法用量: 可静脉缓慢推注、静脉滴注或肌肉注射。
肌肉注射:临用前加灭菌注射用水或氯化钠注射液溶解后使用。
也可用适量5%盐酸利多卡因注射液2-3ml溶解。
静脉注射:临用前加适量注射用水完全溶解后于3-5分钟静脉缓慢推注。
静脉滴注:加适量注射用水溶解后,再用氯化钠或葡萄糖注射液100ml稀释后静脉滴注。
成人常用剂量:一次〜1g, 一日2〜4次,严重感染可增加至一日68,分2〜4次静脉给予。
儿童常用剂量:一日50〜100mg/kg,分2〜3次静脉缓慢推注,静脉滴注或肌肉注射。
肾功能减退者的肌酐清除率大于50ml/min时,仍可按正常剂量给药。
肌酐清除率为20〜50ml/min时,每8小时;肌酐清除率为11〜34ml/min时,每12小时;肌酐清除率小于10ml/min 时,每18〜24小时。
头孢菌素致双硫仑样反应60例临床分析

头孢菌素致双硫仑样反应60例临床分析头孢菌素致双硫仑样反应(Ceftaroline-induced DRESS)是一种罕见但严重的药物过敏反应,其特征为发热、皮疹、内脏器官受累和嗜酸性粒细胞增多。
尽管头孢菌素致双硫仑样反应在临床上较为罕见,但一旦发生则会给患者带来严重的健康威胁。
本文通过对60例头孢菌素致双硫仑样反应的临床分析,旨在提高对该疾病的认识和诊疗水平,为临床医生提供参考。
1.临床特征头孢菌素致双硫仑样反应的临床特征多种多样,主要包括发热、皮疹、内脏器官受累和嗜酸性粒细胞增多等表现。
在60例头孢菌素致双硫仑样反应患者中,发热为最常见症状,达100%;其次是皮疹,为97%;患者还出现了肝脏功能异常、淋巴结肿大、心脏损害等内脏器官受累的症状;49%的患者出现嗜酸性粒细胞增多。
头孢菌素致双硫仑样反应的临床特征多种多样,且常常表现为多器官受累的临床症状。
2.诊断方法头孢菌素致双硫仑样反应的诊断主要依靠患者的临床表现和实验室检查。
对于临床上存在怀疑的患者,应当密切关注其症状的演变,并进行详细的实验室检查。
在60例头孢菌素致双硫仑样反应患者中,所有患者均出现了白细胞增高及嗜酸性粒细胞增多;血清肝功能检测也表现为肝脏功能异常。
还需排除其他引起相似症状的疾病,如传染病、肿瘤等。
3.治疗方法头孢菌素致双硫仑样反应的治疗主要是停用头孢菌素类药物,并及时给予激素治疗。
在60例头孢菌素致双硫仑样反应患者中,停用头孢菌素类药物后,症状逐渐缓解。
对于严重的症状,如呼吸困难、高热等,需要给予激素治疗。
对于内脏器官受累的患者,需要给予相应的支持治疗,如肝脏功能支持、心脏支持等。
头孢菌素致双硫仑样反应的治疗应当及早进行干预,停用致病药物,并根据患者的症状给予相应的治疗。
4.预后头孢菌素致双硫仑样反应的预后与患者的病情严重程度及治疗及时性有关。
在60例患者中,通过及时停用头孢菌素类药物,并给予激素治疗,患者的症状得到了明显缓解。
头孢洛林酯_ceftarolinefosamil_高健
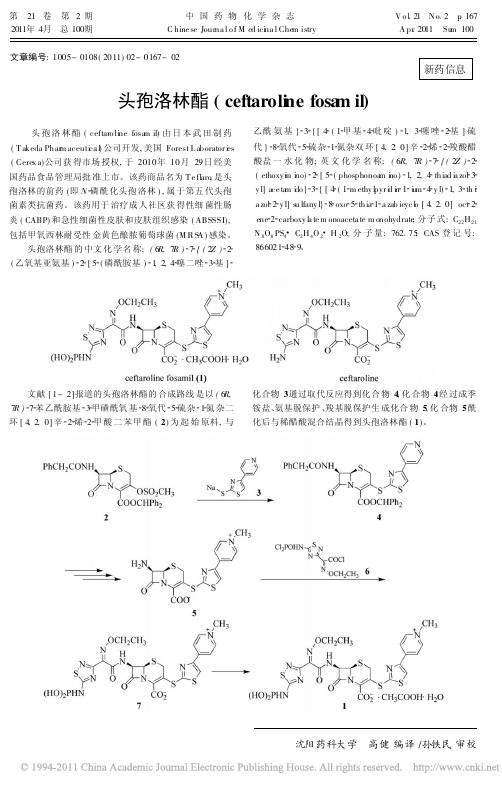
文章编号:1005-0108(2011)02-0167-02新药信息头孢洛林酯(ceftaroli ne fosa m il)头孢洛林酯(ceftaro li ne fosa m il)由日本武田制药(T akeda Phar m aceuti ca l )公司开发,美国Forest L aborator i es (Cerex a)公司获得市场授权,于2010年10月29日经美国药品食品管理局批准上市。
该药商品名为T e fl aro ,是头孢洛林的前药(即N 磷酰化头孢洛林),属于第五代头孢菌素类抗菌药。
该药用于治疗成人社区获得性细菌性肠炎(CABP)和急性细菌性皮肤和皮肤组织感染(ABSSSI),包括甲氧西林耐受性金黄色酿脓葡萄球菌(M R S A )感染。
头孢洛林酯的中文化学名称:(6R,7R ) 7 {(2Z ) 2 (乙氧基亚氨基) 2 [5 (磷酰胺基) 1,2,4 噻二唑 3 基]乙酰氨基} 3 {[4 (1 甲基 4 吡啶) 1,3 噻唑 2 基]硫代} 8 氧代 5 硫杂 1 氮杂双环[4.2.0]辛 2 烯 2 羧酸醋酸盐一水化物;英文化学名称:(6R,7R ) 7 {(2Z ) 2 (ethoxy i m i no) 2 [5 (phosphonoa m i no ) 1,2,4 thiad i a zol 3 y l]ace ta m i do } 3 {[4 (1 m ethy l pyr i d i n 1 i u m 4 y l) 1,3 th i a zol 2 y l]s u lfany l} 8 oxo 5 thia 1 a zab icyc l o [4.2.0]oct 2 ene 2 carboxy l a te m onoaceta te m onohydrate ;分子式:C 22H 21N 8O 8PS 4 C 2H 4O 2 H 2O;分子量:762 75;CAS 登记号:866021 48 9。
第五代头孢菌素——头孢洛林酯

头孢洛林酯
Ceftaroline fosamil
1
药物的研发
2 药物的合成 3 构效关系 4 药理作用 5
药代动力学
抗菌谱
革兰氏阳性菌 革兰氏阴性菌
卡他莫拉菌、ESBL阴 包括抗甲氧西林金黄色 性大肠杆菌、ESBL阴 葡萄球菌(MRSA)、 性肺炎克雷伯菌、流 多重耐药的肺炎链球菌 感嗜血杆菌 (MDRS)
头孢洛林酯
Ceftaroline fosamil
1
药物的研发
2 药物的合成 3 构效关系 4 药理作用 5
药代动力学
药代动力学参数
下表为单次给药600 mg 以及每隔12小时给药一次,持
续14天药测得的动学参数
参量 Cmax (mcg/mL) 单次给药600 mg (n=6) 19.0 (0.71) 多次给药600mg每隔12小时给药一次,持 续14天(n=6) 21.3 (4.10)
协同作用
头孢洛林与氨基糖苷类抗菌药共同使用 时,有较好的协同作用。
离体实验中,头孢洛林与丁胺卡那霉素共同使 用,对于90%受试菌种有着较好的抗菌活性 (包括ESBL阳性大肠杆菌、ESBL阳性肺炎克 并没有发现药 雷伯菌以及AmpC阻遏阴沟肠杆菌)
在与美罗培南共同使用时,对于大肠杆 物拮抗现象
菌有较好的协同抗菌作用
头孢菌素 抗菌谱 第一代 对G+比二 三代强,对 G-差 第二代 对G+较一 代低,对G明显增强, 部分对厌氧 菌有高效 第三代 第四代 第五代 对G+较一 对G+优于 对G+强于 二代低,对 三代,对G-、前四代,尤 G-、厌氧菌、厌氧菌、绿 其是MRSA 绿脓杆菌作 脓杆菌有强 最为有效, 用较强,对 效,对三代 对G-与四代 一二代的耐 的耐药株有 类似。对耐 药株有作用 作用 药株有效。 稳定 无肾毒性 头孢噻林、 头孢特伦、 高 无肾毒性 头孢匹罗、 头孢唑兰 很高 无肾毒性 头孢洛林
达力新(注射用头孢呋辛钠)

达力新(注射用头孢呋辛钠)【药品名称】商品名称:达力新通用名称:注射用头孢呋辛钠英文名称:Cefuroxime Sodium for Injection【成份】本品主要成份为:盐酸左布诺洛尔。
其化学名称为:消旋-5-[3- 叔丁氨基-2- 羟丙氧基]3,4- 双氢-1-(2H)萘酮。
分子式:C17H25NO3HCl 分子量:327.85【适应症】对原发性开角型青光眼具有良好的降低眼内压疗效。
对于某些继发性青光眼,高眼压症,手术后未完全控制的闭角型青光眼以及其他药物及手术无效的青光眼,加用本品滴眼可进一步增强降眼压效果。
【用法用量】滴眼,一次1滴,一日1-2次。
滴于结膜囊内,滴后用手指压迫内毗角泪囊部3〜5分钟。
【不良反应】1 /3 的患者出现暂时性眼烧灼及眼刺痛。
5% 的患者出现结膜炎。
一些患者出现心率减慢及血压下降。
1 其他少见眼部不良反应有:心律变化,呼吸困难,虹膜睫状体炎,头痛,头晕,一过性共济失调,嗜睡,瘙痒及荨麻疹。
2 应用本品还有以下非常罕见不良反应:(1 )全身症状:无力,胸痛。
(2)心血管系统:心动过缓,心率失常,低血压,晕厥,心传导阻滞,脑血管意外,脑缺血,心衰,心绞痛,心悸,心搏停止。
(3)消化系统:恶心,腹泻。
( 4 )神经系统:抑郁,精神错乱,加重重症肌无力的症状,感觉异常。
( 5 )皮肤:过敏反应,包括局禁忌】1支气管哮喘者或有支气管哮喘史者,严重慢性阻塞性肺部疾病。
2 窦性心动过缓,n或川度房室传导阻滞,明显心衰,心源性休克。
3 对本品过敏者。
【注意事项】1 本品慎用于已知是全身β- 肾上腺能阻断剂禁忌症的患者,包括异常心动过缓,I 度以上房室传导阻滞。
先天性心衰应到底适当控制后,才能使用本品。
2 对有明显心脏疾病患者应用本品应监测脉搏。
3 本品慎用于对其他β- 肾上腺能阻断剂过敏者。
4 已有肺功能低下的患者慎用。
5 本品慎用于自发性低血糖患者及接受胰岛素或降糖药治疗的患者,因β 受体阻滞剂可掩盖低血糖症状。
药物Ceftolozane(头孢洛生)合成检索总结报告
药物Ceftolozane(头孢洛生)合成检索总结报告
一、Ceftolozane(头孢洛生)简介
Ceftolozane(头孢洛生)于2014年12月19日在美国上市。
Ceftolozane(头孢洛生)用于治疗复杂腹内感染(clAI)和复杂性尿路感染(cUTI)。
Ceftolozane(头孢洛生)不良反应:恶心、腹泻、头痛和发热。
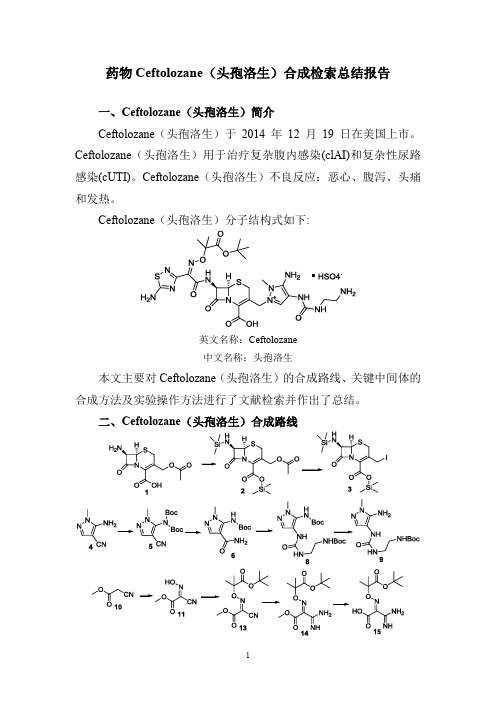
Ceftolozane(头孢洛生)分子结构式如下:
英文名称:Ceftolozane
中文名称:头孢洛生
本文主要对Ceftolozane(头孢洛生)的合成路线、关键中间体的合成方法及实验操作方法进行了文献检索并作出了总结。
二、Ceftolozane(头孢洛生)合成路线
三、Ceftolozane(头孢洛生)合成检索总结报告(一) Ceftolozane(头孢洛生)中间体3的合成
(二) Ceftolozane(头孢洛生)中间体5的合成。
头孢克肟为何不宜用于皮肤感染
头孢克肟为何不宜用于皮肤感染头孢克肟(Ceftaroline fosamil)是一种第五代头孢菌素,广泛应用于治疗革兰阳性菌引起的各种感染,包括复杂性皮肤和皮下组织感染。
尽管具有广谱抗菌活性,但头孢克肟并不是适用于所有皮肤感染的最佳选择。
以下是几个主要的原因:1.药物费用:头孢克肟是一种高效而昂贵的抗生素。
在治疗皮肤感染时,通常可以选择更便宜的抗生素,如头孢类、青霉素类、大环内酯类等。
对于一般的皮肤感染,使用头孢克肟被认为是不经济的。
2. 抗菌谱:尽管头孢克肟对许多致病菌具有活性,但它主要对耐药革兰阳性细菌和部分革兰阴性细菌有效。
对于一些常见的感染病原体,如表皮葡萄球菌(MRSA)、艰难梭菌(Clostridium difficile)等,头孢克肟的抗菌活性相对较弱。
因此,在皮肤感染的治疗中,尤其是当有更适合的抗生素可供选择时,头孢克肟的使用可能不是首选。
3.药物副作用:头孢克肟的副作用与其他头孢菌素类抗生素类似,但其毒性反应相对较低。
然而,在皮肤感染的治疗中,许多常见的致病菌可通过局部治疗(如外用药物)得到控制,因此使用口服或静脉给药的需要较少。
局部治疗不仅可以减少患者对系统性抗生素的依赖,还有助于减少药物的副作用和抗生素耐药性的发展。
4.抗生素耐药性:头孢克肟作为一种新的抗生素,尚未普遍应用于临床。
然而,随着其使用的增加,抗生素耐药性的出现和传播是值得关注的问题。
当头孢克肟被过度使用或滥用时,可能加速耐药菌株的产生,并限制该药物的疗效。
为了减缓抗生素耐药性的发展,临床医生应始终坚持遵循药物使用指南和抗菌药物理性使用原则。
综上所述,尽管头孢克肟在治疗复杂性皮肤感染中具有一定的疗效,但由于其药物费用高、抗菌谱有限、潜在的副作用和抗生素耐药性的产生,它并不是首选的皮肤感染治疗药物。
临床医生应在严格评估病情和细菌耐药性的基础上,选择适当的抗生素治疗方案,以保证患者的疗效和安全性。
头孢特仑新戊酯片

头孢特仑新戊酯片核准日期:2006年11月14日药品名称:【通用名称】头孢特仑新戊酯片【商品名称】富山龙Tomiron【英文名称】Cefteram Pivoxil Tablets【汉语拼音】Tou Bao Te Lun Xin Wu Zhi Pian成份:本品主要成分为:头孢特仑新戊酯化学名称:2,2-二甲丙酰基氧甲基(6R,7R)-7-[(Z)-2-(2-氨基噻唑-4-基)-2-(甲氧亚胺)乙酰胺]-3-(5-甲基-2H-四唑-2-基甲基)-8-氧-5-硫杂-1-氮杂二环[4,2,0]辛-2-烯-2-羧酸酯化学结构式:分子式:C22H37N9O7S2分子量:593.63所属类别:化药及生物制品>> 抗微生物药>> 抗细菌药>> 抗生素类性状:本品为浅橙色薄膜包衣片,除去包衣后显白色至类白色。
适应症:链球菌属(肠球菌除外)、肺炎球菌、化脓性链球菌属、淋球菌、大肠杆菌、柠檬酸菌属、克雷伯氏菌属、肠杆菌属、沙雷氏菌属、变形杆菌属、流感嗜血杆菌等敏感细菌引起的下列感染性疾病:1.咽喉炎(咽炎、喉炎)、扁桃体炎(扁桃体周围炎、扁桃体周围脓肿)、急性支气管炎、肺炎、慢性支气管炎、弥漫性细支气管炎、支气管扩张(感染时)、慢性呼吸系统疾病的重复感染;2.肾盂肾炎、膀胱炎;3.淋菌性尿道炎;4.子宫附件炎、子宫内膜炎、子宫内感染、巴氏腺炎、巴氏腺脓肿;5.中耳炎、副鼻窦炎;6.牙周炎、冠周炎、上颚炎。
规格:(1)50mg;(20)100mg用法用量:咽喉炎(咽炎、喉炎)、扁桃体炎(扁桃体周围炎、扁桃体周围脓肿)、急性支气管炎、肾盂肾炎、膀胱炎、子宫附件炎、子宫内膜炎、子宫内感染、巴氏腺炎、巴氏腺脓肿时:成人常规剂量为一日三次,一次50-100 mg,饭后口服。
慢性支气管炎、弥漫性细支气管炎、支气管扩张(感染时)、慢性呼吸系统疾病的重复感染、肺炎、中耳炎、副鼻窦炎、淋菌性尿道炎、牙周炎、冠周炎、上颚炎时:成人常规剂量为一日三次,一次100-200 mg,饭后口服。
头孢替唑钠的作用有哪些?

头孢替唑钠的作用有哪些?头孢替唑钠(Ceftriaxone Sodium)是一种广谱抗生素,属于头孢菌素类药物。
它的独特作用机制和广泛的抗菌谱使其在临床上得到了广泛的应用。
头孢替唑钠主要通过抑制细菌细胞壁合成来抑制细菌的生长和繁殖。
下面是头孢替唑钠的主要作用:1. 抗菌作用:头孢替唑钠对多种细菌具有广谱的抗菌活性,包括肺炎链球菌、流感嗜血杆菌、大肠埃希菌、肺结核杆菌等。
它对革兰氏阴性菌和革兰氏阳性菌均有较好的抗菌效果。
2. 对β-内酰胺酶的抵抗:头孢替唑钠具有很强的抗β-内酰胺酶的能力,因此可以有效作用于产β-内酰胺酶的细菌,使其产生杀菌作用。
3. 高浓度持续时间长:头孢替唑钠可以通过静脉给药而达到高浓度,在体内持续时间长,有利于维持药物的疗效。
4. 孕妇及婴幼儿治疗安全性高:头孢替唑钠在孕妇及婴幼儿体内的药代动力学特征良好,是治疗这些人群感染的优选药物。
5. 应用灵活性:头孢替唑钠不仅可以单独应用,也可以和其他药物联合使用,对于多种细菌感染,尤其是严重感染或耐药细菌感染,联合应用可以提高治疗效果。
6. 常用治疗范围广:头孢替唑钠广泛用于各个医疗领域,包括呼吸道感染、泌尿道感染、中耳炎、骨和关节感染、腹腔感染、性传播疾病等。
其在临床应用中广谱性和安全性使其成为常用的静脉给药抗菌药物。
7. 防治性头孢替唑钠:在手术前的预防性应用中,头孢替唑钠可有效地预防手术切口感染,减少手术并发症的发生率。
总结起来,头孢替唑钠作为一种广谱抗生素,在临床应用中具有广泛的适应症和有效的抗菌效果。
它具有抑制细菌细胞壁合成、对β-内酰胺酶的抵抗、高浓度持续时间长等独特特点,使其成为临床上常用的抗感染药物之一。
然而,使用头孢替唑钠时应注意合理用药,避免滥用和不当使用,以减少耐药菌株的产生。
同时,在应用过程中也应严格遵守药物的使用规范,以确保治疗效果的最大化。
8. 预防和治疗淋病:头孢替唑钠是临床上常用的治疗淋病的药物之一。
头孢类先锋5号
头孢类——先锋5号【药物别名】头孢菌素V,先锋霉素V、先锋5号、头孢唑林钠Cefamezin【分子式成分】化学名为(6R,7R)-3-[[(5-甲基-1,3,4-噻二唑-2-基)硫]甲基]-7-[(1H-四唑-1-基)乙酰氨基]-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-2-甲酸钠盐。
分子式:C14H13N8NaO4S3。
分子量:【制剂规格】粉针剂:0.25g,0.5g。
本品为白色或类白色的粉末或结晶性粉末;无臭。
【药理毒理】唑啉为第一代头孢菌素,抗菌谱广。
除肠球菌属、耐甲氧西林葡萄球菌属外,本品对其他革兰阳性球菌均有良好抗菌活性,肺炎链球菌和溶血性链球菌对本品高度敏感。
白喉杆菌、炭疽杆菌、李斯特菌和梭状芽胞杆菌对本品也甚敏感。
本品对部分大肠埃希菌、奇异变形杆菌和肺炎克雷伯菌具有良好抗菌活性,但对金葡菌的抗菌作用较差。
伤寒杆菌、志贺菌属和奈瑟菌属对本品敏感,其他肠杆菌科细菌、不动杆菌和铜绿假单胞菌耐药。
产酶淋球菌对本品耐药;嗜血杆菌仅中度敏感。
革兰阳性厌氧菌和某些革兰阴性厌氧菌对本品多敏感。
脆弱拟杆菌耐药。
【药动学】肌注后Tmax为1h,胆汁、尿中浓度很高,大部分以原形排出。
T1/2为。
详细见下:肌内注射本品500mg后,血药峰浓度(Cmax)经1~2小时达38mg/L(32~42mg/L),6小时血药浓度尚可测得7mg/L。
20分钟内静脉滴注本品0.5g,血药峰浓度为118mg/L,有效浓度维持8小时。
本品难以透过血-脑脊液屏障,脑脊液中不能测出药物浓度。
头孢唑林在胸水、腹水、心包液和滑囊液中可达较高浓度。
炎症渗出液中的药物浓度基本与血清浓度相等;胆汁中浓度等于或略超过同期血药浓度。
胎儿血药浓度为母体血药浓度的70%~90%,乳汁中含量低。
本品蛋白结合率为74%~86%。
正常成人的血消除半衰期(T1/2b)为~2小时,老年人中可延长至小时。
肾衰竭患者的T1/2b可延长,内生肌酐清除率为12~17ml/min和低于5ml/min时分别为12小时和57小时。
头孢的作用与功能主治
头孢的作用与功能主治概述头孢(Cephalosporin)是一类广泛应用于临床的抗生素药物,属于β-内酰胺类抗生素。
它们具有广谱抗菌活性,对许多常见细菌感染具有有效的治疗作用。
头孢分为多个代数,每一代的药物活性和抗菌谱有所不同,适用于不同类型的感染。
本文将介绍头孢的作用和功能主治。
头孢的作用1.抗菌作用:头孢药物通过抑制细菌细胞壁合成,破坏菌体结构,使细菌无法生存和繁殖。
不同代数的头孢具有不同的抗菌谱和活性,可以对抗多种细菌感染。
2.治疗感染:头孢可以用于治疗呼吸道感染、泌尿道感染、皮肤软组织感染、骨骼关节感染、腹腔感染等各种常见的细菌感染。
3.预防手术感染:头孢在手术前使用可以预防手术切口感染,减少手术后并发症的发生。
头孢的功能主治头孢根据代数和治疗范围的不同,具有不同的功能主治:头孢一代1.匹多福(Cefamandole):适用于皮肤软组织感染、呼吸道感染和泌尿道感染。
2.头孢噻啶(Cefazolin):广泛应用于手术预防,特别是术前皮肤消毒期间。
也可以治疗呼吸道感染、泌尿道感染等。
3.头孢孟多(Cephradine):适用于尿路感染、呼吸道感染、皮肤软组织感染等。
头孢二代1.头孢丙烯(Cefuroxime):广谱抗菌活性,适用于呼吸道感染、泌尿道感染、皮肤软组织感染等。
2.头孢呋辛(Cefuroxime-axetil):治疗上呼吸道感染、下呼吸道感染、尿路感染等。
头孢三代1.头孢地尼(Cefdinir):广谱抗菌活性,适用于上呼吸道感染、下呼吸道感染、皮肤软组织感染等。
2.头孢他啶(Ceftazidime):适用于严重感染,如肺炎、腹腔感染、骨骼关节感染等。
3.头孢克肟(Cefpodoxime-proxetil):适用于上呼吸道感染、泌尿道感染等。
头孢四代1.头孢美唑(Cefepime):广谱抗菌活性,适用于呼吸道感染、泌尿道感染、腹腔感染等。
2.头孢哌酮(Cefpirome):适用于严重感染,如败血症、腹腔感染、骨骼关节感染等。
美国FDA批准头孢类抗菌药物Teflaro上市

美国FDA批准头孢类抗菌药物Teflaro上市
佚名
【期刊名称】《中国执业药师》
【年(卷),期】2011(8)1
【摘要】美国FDA于2010年10月29日批准CEREXA公司的头孢类抗菌药物Ceftaroline Fosamil(商品名:Teflaro)上市,用于治疗敏感菌引起的急性细菌
性皮肤、皮肤结构感染以及社区获得性肺炎(包括肺炎链球菌引起的并发菌血症)。
【总页数】1页(P54-54)
【关键词】头孢类抗菌药物;美国FDA;FDA批准;上市;皮肤结构感染;社区获得性肺炎;急性细菌性;肺炎链球菌
【正文语种】中文
【中图分类】R914.1
【相关文献】
1.FDA批准医疗器械Optune用于治疗脑癌/CFDA批准首个卵巢储备功能检测上市/FDA批准帮助盲人通过舌头处理视觉信号的器械 [J],
2.美国FDA批准抗菌药物卢立康唑上市 [J],
3.FDA批准抗菌药物Ozenoxacin上市 [J],
4.美国FDA批准抗菌药物Tavaborole上市 [J],
5.美国FDA批准抗菌药物Finafloxacin上市 [J],
因版权原因,仅展示原文概要,查看原文内容请购买。
医学知识之头孢唑肟
头孢唑肟1概述头孢唑肟(Ceftizoxime)为半合成的第三代头孢菌素,抗菌谱较广,与头孢噻肟相似。
对一些革兰阳性菌有中度的抗菌作用,对革兰阴性菌的作用强。
抗菌谱包括金黄色葡萄球菌、链球菌属、肺炎球菌、流感嗜血杆菌、肺炎链球菌、大肠杆菌、克雷伯杆菌、变形杆菌及肠细菌属等。
耐第一代头孢菌素和庆大霉素的一些革兰阴性菌可对本品敏感,但粪肠球菌和耐甲氧西林的葡萄球菌对本品不敏感。
头孢唑肟广泛分布于全身各种组织和体液中,包括胸水、腹水、胆汁、胆囊壁、脑脊液(脑膜有炎症时)、前列腺液和骨组织,均可达治疗浓度。
2适应证敏感菌所致的下呼吸道感染、尿路感染、腹腔感染、盆腔感染、败血症、皮肤软组织感染、骨和关节感染、肺炎链球菌和流感嗜血杆菌所致脑膜炎和单纯性淋病。
3临床应用每日1~2g,重症可用到4g,A分2~4次给予,可肌注、静注或静滴。
4不良反应皮疹、瘙痒、药物热等过敏反应、腹泻、恶心、呕吐、食欲不振等。
碱性磷酸酶、血清氨基转移酶轻度升高等。
贫血(包括溶血性贫血)、白细胞减少、血小板减少。
偶见头痛、麻木、眩晕、维生素K和维生素B缺乏症、过敏性休克。
极少数病人可发生黏膜念珠菌病。
注射部位灼烧感、蜂窝织炎、静脉炎(静脉注射者)、疼痛、硬化和感觉异常等。
5注意事项结肠炎患者慎用。
妊娠期妇女慎用。
6个月以下小儿使用本品的安全性和有效性尚未确定。
大量长期给药可引起肾功能损害。
老年患者常伴有肾功能减退,应适当减少剂量或延长给药时间。
较长期应用可致菌群失调,甚至二重感染。
一次大剂量静脉注射时可引起血管痛、血栓性静脉炎,应尽量减慢注射速度。
本品溶解后在室温下放置不宜超过7小时,冰箱中放置不宜超过48小时。
6用药禁忌对本品及其他头孢类抗生素过敏者禁用。
7药物相互作用与丙磺舒合用时,可使本药的肾清除减少,血药浓度上升。
与氨基糖苷类联用,可加强对绿脓杆菌的抗菌作用,但肾毒性也相应增加。
与呋塞米等强利尿剂合用时,可致肾损害。
【注意事项】大家在用药的时候,药物说明书里面有三种标识,一般要注意一下:1.第一种就是禁用,就是绝对禁止使用。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
( P biHel l i l etr fl td oF d n iesy S ag a 2 10 ;2H ah n si l hn h i2 0 4 ) 1 u l a hCi c ne i e u a vri , h nh i 0 5 8 u sa pt ,S a g a 0 0 0 c t n aC a a t i Un t Ho a Ab t a t s r c Cet r l e ( fa o i n CPT) i o e, a e t r l r a —p c r m e h l s o i x i iig sr n sa n v l p r n e a,b o d s e t u c p ao p rn e h b tn to g
摘要: C f rl e( P e aoi C T)是一种 新型注射 用广 谱头孢菌 素,体 内外 实验表 明,C T i n P 对革兰阳性菌包括耐 甲氧西林金葡菌 ( MRS A)、多重耐药肺 炎链球菌 ( MDR P)、耐万 古霉素肠球菌 ( E)等 具有优 良的杀菌活性 ,对 常见革兰 阴性 菌也有 S VR 效 ;同时C T 具有 较佳的安全耐受性和 药动 学预测性强等特 点。该药现处于I 期 临床 开发阶段 ,适用 于MRS P还 I I A和 多种 病原菌
Sa h lcc u ues a c my i— s tn neo o cs a c l t yo o csa ru ;V n o cnr i at t c cu e a ̄ p es E r f
随 着 耐 甲氧 西 林 金 葡 菌 ( MRS A)的 明显 增 多
1 体 外 抗菌活 性
及其对万 古霉 素 ( a c m cnV N)等糖肽类药 v n o y i,A 物 敏 感 性 的 下 降 , 寻求 新 的抗 MRS A和 抗 耐 万 古霉 素革兰阳性菌 的有效药物 已成 为医药工作者所关注 的焦 点 。C f r l e ( P e aoi C T)是 由F rs L b rtr s l n oet a oaoi e 公 司 开 发 的一 种 新 型注 射 用 广 谱 头 孢 菌 素 ,适 用 于 治 疗 包括 MRS A、 多重 耐 药 肺 炎链 球 菌 ( RS ) MD P 等 革 兰 阳 性 菌 以及 常 见 革兰 阴性 菌感 染 [。 CP 1 1 T是 cf rl efsmi et oi a l a n o 的生 物活 性代 谢产 物 ,而 后者 是一 种 新 的N. 酰基 水 溶 性 头孢 菌 素前 体 药 物 ,进 入 体 膦 内后 经 脱磷 酸 化 作 用 变 为 C T,两 者 的分 子 结构 见 P F g 1 已有研 究 结 果表 明 ,C T 有 良好 的体 内外 i. 。 P具 抗 菌 活性 ,可 用 于 各种 院 内细 菌 性 感 染 的 治疗 , 临 床应 用前 景十 分广 阔 。
混合感染的治疗。
关键 词: C f rl e 抗 菌活性 ; 药动学 ; 安全性 ; MRS VR et oi ; a n A; E 中图分类号 : R 7 . 1 9 81 文献标识码 i fa o i , w e l s rn
中国抗生素杂志2 1 年1 0 0 月第3 卷第 1 5 期
文章编号 :10 —6 9( 00)0 —0 70 0 18 8 2 1 10 0 .6
头孢 类新药cf rl e et oi a n
孟现 民1 姚 晓英- 许 寅・ 周小花1 张永信z ,
( 上海市公共卫生临床 中心 ,上海 2 10 ;2华 山医院,上海 2 0 4 1 05 8 0 00)
M RS a dm i e f c i n . A n x d i e t s n o Ke r s y wo d Ce a o i e An i a t r a c i iy P a m a o i e i s S f t l f rl ; n tb c e i la t t ; h r c k n tc ; a e y; M e h c l n r s s a t v t i il - e i t n i
wela o l sc mmo r m— e ai ep t o e s CP lo h sa lto o dp o lss c sb a rs ft n oea it, n ga n g t ah g n . T as a fg o rf e u h a e e ae a d tlrb ly v o i y i
b ceiia at i g is ga p s ieogns ,n ldn tiii— s tn t h,c cu ues( S , at c l c vt a a t rm—oiv ra i r d i y n t ms ic igmehclnr ia t a )o o csa ru MR A) u l es S p l
p e itbep ama o ieisecT ea e t sc re t h s I d v lp n n a eu e o ete t n f r dca l h r c k n t t.h g n u rn l i p a eII e eo me t dc nb sd fr h ame t c i yn a t r o
mut rgrs tn t po o c s n u o ie( ldu — i a t r t c u e m na MDR P n a c my i- s tn neoo c s a c l VR ) a i es S e c p S )adv n o c r i a t trc cu ea ̄( E , s nes E f