伊布替尼说明书解读
伊布替尼合理用药要点
伊布替尼合理用药要点通用名:伊布替尼胶囊制剂与规格:胶囊:140mg适应证:1.单药适用于既往至少接受过一种治疗的套细胞淋巴瘤患者的治疗。
2.单药适用于既往至少接受过一种治疗的慢性淋巴细胞白血病/小淋巴细胞淋巴瘤患者的治疗。
3.复发难治的华氏巨球蛋白血症,边缘区淋巴瘤及non-gcb亚型的弥漫大B细胞淋巴瘤。
合理用药要点:1.用药前必须明确诊断套细胞淋巴瘤或慢性淋巴细胞白血病,根据诊断不同,治疗剂量不同。
2.应该按照相关疾病指南,治疗前做基线评估,治疗期间定期监测治疗反应及毒性。
3.治疗MCL的推荐剂量为560mg,每日一次直至疾病进展或出现不可接受的毒性;治疗CLL/SLL的推荐剂量为420mg,每日一次直至疾病进展或出现不可接受的毒性。
4.轻度肝损伤患者(Child-Pugh-级)的推荐剂量是每天140mg 中度或重度肝损伤患者(Child-Pugh- B级和C级)应避免使用。
5.口服给药,每日一次,每天的用药时间大致固定。
应用水送整粒胶囊。
请勿打开、弄破或咀嚼胶囊。
如果未在计划时间服用本品,可以在当天尽快服用,第二天继续在正常计划时间服药。
请勿额外服用本品以弥补漏服剂量。
6.出现任何≥3级非血液学毒性、≥3级伴感染或发热的中性粒细胞减少症或者4级血液学毒性时,应中断治疗。
待毒性症状消退至1级或基线水平(恢复)时,可以起始剂量重新开始治疗。
如果该毒性再次发生,应将剂量减少140mg,如有需要,可以考虑再减少140mg。
如果在两次剂量降低后该毒性仍然存在或再次发生,应停用。
7.接受本药治疗的MCL患者最常发生的不良反应(≥20%)是腹泻、出血(如青肿)、疲乏、骨骼肌肉疼痛、恶心、上呼吸道感染、咳嗽和皮疹。
最常见的3级或4级不良反应(≥5%)是中性粒细胞减少症、血小板减少症、感染性肺炎和贫血。
接受本药治疗的CLL或SLL患者最常发生的不良反应(≥20%)是中性粒细胞减少症、血小板减少症、贫血、腹泻、骨骼肌肉疼痛、恶心、皮疹、青肿、疲乏、发热和出血。
甲磺酸伊马替尼片-详细说明书与重点

甲磺酸伊马替尼片【成分】本品活性成份为甲磺酸伊马替尼。
【性状】本品为深黄色至棕黄色双凸的薄膜衣片。
【适应症】用于治疗费城染色体阳性的慢性髓性白血病(Ph + CML)的慢性期、加速期或急变期;用于治疗不能切除和/或发生转移的恶性胃肠道间质瘤(GIST)的成人患者;联合化疗治疗新诊断的费城染色体阳性的急性淋巴细胞白血病(Ph + ALL)的儿童患者。
用于治疗复发的或难治的费城染色体阳性的急性淋巴细胞白血病(Ph + ALL)的成人患者。
用于以下适应症的安全有效性信息主要来自国外研究资料,中国人群数据有限:用于治疗嗜酸性粒细胞增多综合征(HES)和/或慢性嗜酸性粒细胞白血病(CEL)伴有FIP1L1-PDGFRα融合激酶的成年患者。
用于治疗骨髓增生异常综合征/骨髓增殖性疾病(MDS/MPD)伴有血小板衍生生长因子受体(PDGFR)基因重排的成年患者。
用于治疗侵袭性系统性肥大细胞增生症(ASM),无D816V c-Kit 基因突变或未知c-Kit 基因突变的成人患者。
用于治疗不能切除,复发的或发生转移的隆突性皮肤纤维肉瘤(DFSP)。
用于Kit(CD117)阳性GIST 手术切除后具有明显复发风险的成人患者的辅助治疗。
极低及低复发风险的患者不应该接受该辅助治疗。
【规格】0.1 g;0.4g【用法用量】治疗应由对恶性肿瘤患者有治疗经验的医师进行。
甲磺酸伊马替尼应在进餐时服用,并饮一大杯水,以使胃肠道紊乱的风险降到最小。
通常成人每日一次,每次400 mg 或600 mg,以及日服用量800 mg 即400 mg 剂量每天2 次(在早上及晚上)。
儿童和青少年每日一次或分两次服用(早晨和晚上)。
不能吞咽药片的患者(包括儿童),可以将药片分散于不含气体的水或苹果汁中(100 mg 片约用50 ml,400 mg 约用200 ml)。
应搅拌混悬液,一旦药片崩解完全应立即服用。
只要患者持续受益,本品治疗应持续进行。
伊布替尼治疗弥漫大B细胞淋巴瘤诱发噬血细胞综合征一例并文献复习
•182.广 i 血病•淋巴墙 202 丨’中• 3 /]第 30 役第 3 期 Jmirnal »f 【.《nikemia & I.vmphoma, Mar(、h 202 丨,V 〇l. 30,、•(>• 3梗死诊断依赖于病史、临床症状、体征和M R 丨检查,其中M K 丨检 查在骨梗死诊断中有发现¥•、准确、可直接和多层次反映骨梗 死范围及部位的优势临床中对于有骨梗死高危因素并出现 不能解释的骨痛患者,建议尽早行M K I 检查:利益冲突所有作者均声明不存在利益冲突参考文献[1 ]高文琴,张改连,张莉芸.系统性红斑狼疮并发广泛性骨梗死一例[J ].中华风湿病学杂志,2015,19(8):552-554. D 01:10.3760/ rma.j.issn. 1007-7480.2015.08.012.(iao WQ, Zhang C l., Zhang LY. A rase of systemic lupus erythematosus romplirated with extensive hone infarction [j ]. Chin J Rheumatol, 2015, 19(8): 552-554. DOI : 10.3760/rma.j.issn. 1007- 7480.2015.08.012.;2Jones LC , Hungerforrl I)S. Osteonecrosis : etiology, diagnosis, and treatment | J ]. Curr Opin Rheumatol, 2004, 16(4) : 443-449. 1)01: 10.1097/01 .moo.0000127829.34643.fd.[3」Koo KH , Kim R , Kim Y S, et al. Risk period for developingosteonecrosis of the femoral head in patients on steroid treatment, J •Clin Rheumatol, 2002, 21 (4) : 299-303. DOI : 10.1007/s 1006702 00078.Zhu ZA . ^ an MN. Etiology and pathogenesis of osteonecrosis of the femoral head in aflulls J . (!!hin J Orthop. 2010, 30( 1 ) : 6-9. DOI : 10.3760/cma.j.issn.0253-2352.2010.01.003.i 5 : Ghosh J , Manjunatha YC, Thulkar S , et al. Avascular necrosis offemoral head in childhood acute myeloid leukemia : complication of chemolherapy without steroids i JPediatr Blood Cancer, 2008, 51(2): 308-309. DOI : 10.1002/phr.21559.6 ^ Asano T , Takahashi KA, F^ujioka M, et al. ABCB1 (3435T andG2677T/A polymorphism derreaseci the risk for steroid - induced osteonecrosis of the femoral head after kiflney transplantation J . Pharmar 〇genetics,2003,13( 11 ) :675-682. 1)01:10.1097/00008571- 200311000-00003.i 7 ] Gluerk CJ , Freiberg RA , Wang P. Heritable fhromhophilia-hypofihrinolvsis and osteonecrosis of the femoral head !J |. Clin Orthop Helat R e s, 2008,466( 5 ): 1034-1040. DOI : 10.1007/si 1999- 008-0148-0.[8 ] Schulte (^M , FJeelen DW. Bone loss following hematopoietir stemfell transplantation : a long-term follow - up l J _ • Blood, 2004, 103(10): 3635-3643. DOI : 10.1182/blo 〇d-2003-09-3081.| 9 ] Fink JC , Ieisenring WM, Sullivan KM, el al. Avascular necrosisfollowing hone marrow transplantation : a case-control study[ J]- Bone,[4 ]朱振安,严孟宁.成人股骨头坏死的病因和发病机制[J .中肀骨1"8,22⑴:67-7L科杂志,20丨0, 30 (丨):6-9.丨)()丨:丨().3760/rma. j. issn.0253 - 2352. (收稿 H 期:2020-05-12)2010.01.003.(本文编辑:郎华校对:陈晶)伊布替尼治疗弥漫大B 细胞淋巴瘤诱发噬血细胞综合征 一例并文献复习向国强'姜利军2隗佳2黄亮21湖北省恩施土家族苗族自治州中心医院血液内科4450(H );:华中科技大学同济医学院 附属同济医院血液内科,武汉43003U 通信作者:姜利军,Email : 278308418@qti •com扫码阅读电子版【摘要】目的探讨伊布替尼治疗B 细胞恶性肿瘤诱发噬血细胞综合征(H P S )的临床特征,提高 对伊布替尼诱发H P S 的认识方法回顾性分析1例弥漫大B 细胞淋巴瘤(D L B C L )患者经伊布替尼治 疗后诱发H P S 的诊疗经过,并进行文献复习结果该患者接受伊布替尼治疗后第8天诱发H P S ,病情 迅速恶化结论伊布替尼不能精准抑制布鲁顿酪氨酸激酶抑制剂,存在脱靶效应,可抑制T 细胞激 酶,具有潜在有害性突变的D L B C L 患者在接受伊布替尼治疗时应意识到诱发H P S 这一潜在并发症【关键词】伊布替尼;淋巴瘤,大B 细胞,弥漫性;噬血细胞综合征 基金项目:湖北省ft 然科学基金(2019C F B 656)D O I : 10.3760/cma.j.rnl 15356-20200913-00224Ibrutinib in treatment of diffuse large B-cell lymphoma-induced hemophagocytic syndrome: report of one case and review of literatureXiang Guoqiang1, Jian g Lijun'. W ei Jin',Huang Liang2I’ 1血病•淋巴瘤2021 年 3 月第 30 卷第 3 期Journal of Lpukemia & Lym丨)homa,Marrh 2021,Vol. 30, No. 3•183-'Department of Hematology, the Central Hospital o f Enshi Tujia and Miao Autonomous Prefecture, Enshi445000, China: 'Department of Hematology, Tongji Hospital, Tongji Medical College of Huazhong University ofScience & Technology. Wuhan 430030, ChinaCorresponding author: Jian g Lijun, Email:****************Fund program:Natural Science Foundation of H u b e i Prov ince (2019C F B656)D O I: 10.3760/rma.j.rnl 15356-20200913-00224噬血细胞性淋巴组织细胞增多症(H L H)又称噬血细胞综合征(H P S),是一种由遗传性或获得性免疫功能异常导致的以病理性炎症反应为主要特征的临床综合征。
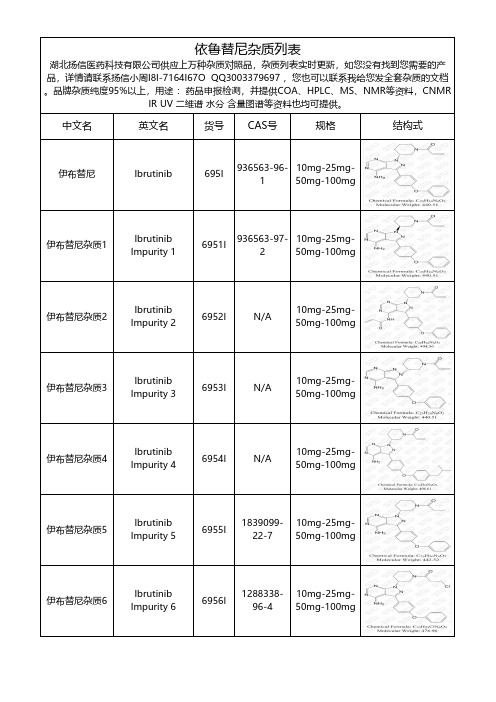
依鲁替尼杂质-(最新结构)列表
10mg-25mg50mg-100mg
伊布替尼杂质51
Ibrutinib Impurity 51
69551I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质52
Ibrutinib Impurity 52
69552I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质53
Ibrutinib Impurity 53
330793-492
10mg-25mg50mg-100mg
伊布替尼杂质38
Ibrutinib Impurity 38
69538I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质39
Ibrutinib Impurity 39
69539I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质40
Ibrutinib Impurity 15
69515I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质16
Ibrutinib Impurity 16
69516I
N/A
10mg-25mg50mg-100mg
伊布替尼杂质17
Ibrutinib Impurity 17
69517I
N/A
10mg-25mg50mg-100mg
Ibrutinib Impurity 35
69535I
151266-238
10mg-25mg50mg-100mg
伊布替尼杂质36
Ibrutinib Impurity 36
69536I
51067-38-0
10mg-25mg50mg-100mg
《中国慢性淋巴细胞白血病小淋巴细胞淋巴瘤的诊断与治疗指南(完整版)》解读

《中国慢性淋巴细胞白血病/小淋巴细胞淋巴瘤的诊断与治疗指南(完整版)》解读近年,在慢性淋巴细胞白血病(CLL)的基础研究、新的预后标志、诊断标准及治疗等方面取得了巨大进展,为提高我国血液科医师对CLL诊断、鉴别诊断及规范化治疗水平,中国抗癌协会血液肿瘤专业委员会、中华医学会血液学分会和中国CLL工作组组织相关专家对2015年版CLL/小淋巴细胞淋巴瘤(SLL)的诊断与治疗指南进行了更新修订。
现就2018年版新修订指南进行解读。
一、诊断CLL和SLL均为单克隆、成熟样小淋巴细胞的淋巴系统恶性疾病,两者的区别在于CLL临床多表现为外周血和骨髓异常淋巴细胞浸润的白血病样表现;而SLL多为淋巴器官肿大的淋巴瘤样表现和骨髓受累。
(一)诊断标准CLL诊断要求外周血B淋巴细胞≥5×109/L;外周血B淋巴细胞必须经流式细胞术检查确认为克隆性,即细胞表面限制性表达免疫球蛋白的κ或λ轻链(sIgκ或sIgλ);另外,sIg阴性CD19细胞>25%也支持克隆性。
外周血涂片的形态学特征为成熟样小淋巴细胞(观察CLL细胞形态学外周血涂片优于骨髓涂片),这些细胞可能混有大而不典型的细胞、分裂细胞或<55%的幼稚淋巴细胞(简称幼淋细胞)。
如果外周血幼淋细胞占淋巴细胞的比例≥55%则诊断为幼淋细胞白血病(PLL),细胞形态学对诊断B-PLL至关重要;10%~54%则诊断为CLL/PL(CLL的一种变异型),幼淋细胞比例增高者预后不佳,同时需结合其他指标确认是否转化,特别是进行性增高时。
对于外周血存在克隆性B细胞,但B淋巴细胞绝对计数<5×109/L,同时不伴有淋巴结和器官肿大(所有淋巴结<1.5 cm)、血细胞减少和淋巴增殖性疾病相关症状的患者,应诊断为单克隆B淋巴细胞增多症(MBL);MBL大多CD5+,且呈典型的CLL表型,也可CD5-;CLL表型的MBL,根据外周血B淋巴细胞绝对计数分为低计数MBL(<0.5×109/L)及高计数MBL(≥0.5×109/L),前者进展为CLL的风险很小,无需常规随访,后者每年1%~2%进展为需要治疗的CLL,所以处理原则同早期CLL。
伊布替尼说明书解读
导读此文为深入浅出的伊布替尼中文版说明书解读,阐述问题如下:1、伊布替尼适应症2、伊布替尼的规格用量和用法3、不宜使用伊布替尼的群体4、伊布替尼副作用及处理方法5、药物冲突注意事项官方版伊布替尼中文说明书百度文库即有,此文仅在于科普伊布替尼应用知识。
作为处方药物,患者在使用伊布替尼时,一定要谨遵医嘱。
一、伊布替尼适应症已获美国药监局审批的伊布替尼七大适应症中,除移植性抗宿主病外,其余皆为肿瘤适应症。
1、治疗前期接受过至少一次来那度胺或者其他药物治疗的套细胞淋巴瘤。
2、治疗既往接受过至少一次治疗的慢性淋巴细胞白血病。
3、治疗携带del 17p删除突变的慢性淋巴细胞白血病。
4、治疗华氏巨球蛋白血症。
5、一线治疗慢性淋巴细胞白血病。
6、治疗伴有或不伴有染色体17p删除突变(del 17p)的小淋巴细胞性淋巴瘤。
7、治疗先前有治疗失败经历的慢性移植物抗宿主病。
二、伊布替尼的规格用量和用法1、规格伊布替尼每粒含药物成分140毫克,有两种规格:(1)每瓶90粒。
(2)每颗120粒。
2、用量(1)套细胞淋巴瘤患者每日口服560毫克药物。
(2)其他肿瘤患者以及慢性移植物抗宿主病患者每日推荐剂量为420毫克。
3、用法每日定时口服一次,不应碾碎、咀嚼胶囊。
数据显示随餐或餐后服用较之空腹服用更有利于吸收,因此建议饭后半小时内温水送服。
漏服应立即补服;若发现漏服时距离下次定点用药时间较近,则跳过该次用药,于定点时间用药。
注意:不可因漏服而补服双倍剂量。
三、不宜使用伊布替尼的群体1、中至重度肝功能不全者不应用药,轻度肝受损者推荐剂量为140毫克每日。
2、尚无数据显示药物存于母乳,但禁止母乳喂养。
3、未确认儿童用药的安全性和有效性,儿童不应用药。
4、药物危害胎儿安全,妊娠期妇女禁用,用药女性应做好避孕措施。
5、女性患者用药结束后的一个月内避免怀孕,男性患者治疗结束后的3个月内避免生育。
四、伊布替尼副作用和处理方法1、伊布替尼一般性副作用有:恶心、腹泻、疲劳、外周水肿、淤血、皮疹、关节痛、肌肉骨骼疼痛、上呼吸道感染、肺炎等。
伊布替尼英文说明书

patients with mild impairment, reduce IMBRUVICA dose (8.7).See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.Revised: 1/2015 FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE1.1 Mantle Cell Lymphoma1.2 Chronic Lymphocytic Leukemia1.3 Chronic Lymphocytic Leukemia with 17p deletion1.4 Waldenström's Macroglobulinemia2 DOSAGE AND ADMINISTRATION2.1 Dosing Guidelines2.2 Dosage2.3 Dose Modifications for Adverse Reactions2.4 Dose Modifications for Use with CYP3A Inhibitors2.5 Dose Modifications for Use in Hepatic Impairment2.6 Missed Dose3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Hemorrhage5.2 Infections5.3 Cytopenias5.4 Atrial Fibrillation5.5 Second Primary Malignancies5.6 Tumor Lysis Syndrome5.7 Embryo-Fetal Toxicity6 ADVERSE REACTIONS6.1 Clinical Trials Experience6. 2 Postmarketing Experience7 DRUG INTERACTIONS7.1 CYP3A Inhibitors7.2 CYP3A Inducers8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use8.6 Renal Impairment8.7 Hepatic Impairment8.8 Females and Males of Reproductive Potential8.9 Plasmapheresis11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility14 CLINICAL STUDIES14.1 Mantle Cell Lymphoma14.2 Chronic Lymphocytic Leukemia14.3 Waldenström's Macroglobulinemia16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION*Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGE1.1 Mantle Cell LymphomaIMBRUVICA is indicated for the treatment of patients with mantle cell lymphoma (MCL) who have received at least one prior therapy.Accelerated approval was granted for this indication based on overall response rate. Continued approval for this indication may be contingent upon verification of clinical benefit in confirmatory trials [see Clinical Studies (14.1)].1.2 Chronic Lymphocytic LeukemiaIMBRUVICA is indicated for the treatment of patients with chronic lymphocytic leukemia (CLL) who have received at least one prior therapy [see Clinical Studies (14.2)].1.3 Chronic Lymphocytic Leukemia with 17p deletionIMBRUVICA is indicated for the treatment of patients with chronic lymphocytic leukemia (CLL) with 17p deletion [see Clinical Studies (14.2)].1.4 Waldenström's MacroglobulinemiaIMBRUVICA is indicated for the treatment of patients with Waldenström's macroglobulinemia (WM) [see Clinical Studies (14.3)].2 DOSAGE AND ADMINISTRATION2.1 Dosing GuidelinesAdminister IMBRUVICA orally once daily at approximately the same time each day. Swallow the capsules whole with water. Do not open, break, or chew the capsules.2.2 DosageMantle Cell LymphomaThe recommended dose of IMBRUVICA for MCL is 560 mg (four 140 mg capsules) orally once daily. Chronic Lymphocytic Leukemia and Waldenström's MacroglobulinemiaThe recommended dose of IMBRUVICA for CLL and WM is 420 mg (three 140 mg capsules) orally once daily.2.3 Dose Modifications for Adverse ReactionsInterrupt IMBRUVICA therapy for any Grade 3 or greater non-hematological, Grade 3 or greaterneutropenia with infection or fever, or Grade 4 hematological toxicities. Once the symptoms of the toxicity have resolved to Grade 1 or baseline (recovery), IMBRUVICA therapy may be reinitiated at the starting dose. If the toxicity reoccurs, reduce dose by one capsule (140 mg per day). A second reduction of dose by 140 mg may be considered as needed. If these toxicities persist or recur following two dose reductions, discontinue IMBRUVICA.Recommended dose modifications are described below:Toxicity Occurrence MCL Dose Modification AfterRecoveryStarting Dose = 560 mgCLL and WM DoseModification After RecoveryStarting Dose = 420 mgFirst Restart at 560 mg daily Restart at 420 mg dailySecond Restart at 420 mg daily Restart at 280 mg dailyThird Restart at 280 mg daily Restart at 140 mg dailyFourth Discontinue IMBRUVICA Discontinue IMBRUVICA2.4 Dose Modifications for Use with CYP3A InhibitorsAvoid co-administration with strong or moderate CYP3A inhibitors and consider alternative agents with less CYP3A inhibition.Concomitant use of strong CYP3A inhibitors which would be taken chronically (e.g., ritonavir, indinavir, nelfinavir, saquinavir, boceprevir, telaprevir, nefazodone) is not recommended. For short-term use (treatment for 7 days or less) of strong CYP3A inhibitors (e.g., antifungals and antibiotics) consider interrupting IMBRUVICA therapy until the CYP3A inhibitor is no longer needed [see Drug Interactions (7.1)].Reduce IMBRUVICA dose to 140 mg if a moderate CYP3A inhibitor must be used (e.g., fluconazole, darunavir, erythromycin, diltiazem, atazanavir, aprepitant, amprenavir, fosamprevir, crizotinib, imatinib, verapamil, and ciprofloxacin) [see Drug Interactions (7.1)].Patients taking concomitant strong or moderate CYP3A inhibitors should be monitored more closely for signs of IMBRUVICA toxicity.2.5 Dose Modifications for Use in Hepatic ImpairmentFor patients with mild liver impairment (Child-Pugh class A), the recommended dose is 140 mg daily (one capsule). Avoid the use of IMBRUVICA in patients with moderate or severe hepatic impairment (Child-Pugh classes B and C) [see Use in Specific Populations (8.7) and Clinical Pharmacology (12.3)]. 2.6 Missed DoseIf a dose of IMBRUVICA is not taken at the scheduled time, it can be taken as soon as possible on the same day with a return to the normal schedule the following day. Extra capsules of IMBRUVICA should not be taken to make up for the missed dose.3 DOSAGE FORMS AND STRENGTHS140 mg capsules4 CONTRAINDICATIONSNone5 WARNINGS AND PRECAUTIONS5.1 HemorrhageFatal bleeding events have occurred in patients treated with IMBRUVICA. Grade 3 or higher bleeding events (subdural hematoma, gastrointestinal bleeding, hematuria and post procedural hemorrhage) have occurred in up to 6% of patients. Bleeding events of any grade, including bruising and petechiae, occurred in approximately half of patients treated with IMBRUVICA.The mechanism for the bleeding events is not well understood.IMBRUVICA may increase the risk of hemorrhage in patients receiving antiplatelet or anticoagulant therapies.Consider the benefit-risk of withholding IMBRUVICA for at least 3 to 7 days pre and post-surgery depending upon the type of surgery and the risk of bleeding [see Clinical Studies (14)].5.2 InfectionsFatal and non-fatal infections have occurred with IMBRUVICA therapy. Grade 3 or greater infections occurred in 14% to 26% of patients. [See Adverse Reactions (6.1)]. Cases of progressive multifocal leukoencephalopathy (PML) have occurred in patients treated with IMBRUVICA. Monitor patients for fever and infections and evaluate promptly.5.3 CytopeniasTreatment-emergent Grade 3 or 4 cytopenias including neutropenia (range, 19 to 29%), thrombocytopenia (range, 5 to 17%), and anemia (range, 0 to 9%) occurred in patients treated with IMBRUVICA.Monitor complete blood counts monthly.5.4 Atrial FibrillationAtrial fibrillation and atrial flutter (range, 6 to 9%) have occurred in patients treated with IMBRUVICA, particularly in patients with cardiac risk factors, acute infections, and a previous history of atrial fibrillation. Periodically monitor patients clinically for atrial fibrillation. Patients who develop arrhythmic symptoms (e.g., palpitations, lightheadedness) or new onset dyspnea should have an ECG performed. If atrial fibrillation persists, consider the risks and benefits of IMBRUVICA treatment and dose modification [see Dosage and Administration (2.3)].5.5 Second Primary MalignanciesOther malignancies (range, 5 to 14%) including non-skin carcinomas (range, 1 to 3%) have occurred in patients treated with IMBRUVICA. The most frequent second primary malignancy was non-melanoma skin cancer (range, 4 to 11 %).5.6 Tumor Lysis SyndromeTumor lysis syndrome has been reported with IMBRUVICA therapy. Monitor patients closely and take appropriate precautions in patients at risk for tumor lysis syndrome (e.g. high tumor burden).5.7 Embryo-Fetal ToxicityBased on findings in animals, IMBRUVICA can cause fetal harm when administered to a pregnant woman. Ibrutinib caused malformations in rats at exposures 14 times those reported in patients with MCL and 20 times those reported in patients with CLL or WM, receiving the ibrutinib dose of 560 mg per day and 420 mg per day, respectively. Reduced fetal weights were observed at lower exposures. Advise women to avoid becoming pregnant while taking IMBRUVICA. If this drug is used during pregnancy or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to a fetus [see Use in Specific Populations (8.1)].System Organ Class Preferred Term All Grades (%)Grade 3 or 4 (%)*Gastrointestinal disordersDiarrhea 634Constipation 232Nausea 212Stomatitis 210Vomiting192Abdominal pain 150Dyspepsia13Infections and infestations Upper respiratory tractinfection 482Sinusitis216Skin infection 176Pneumonia108Urinary tract infection100General disorders and administrative site conditions Fatigue 314Pyrexia 252Peripheral edema230Asthenia 134Chills130Skin and subcutaneous tissue disorders Bruising 542Rash270Petechiae170Respiratory, thoracic and mediastinal disorders Cough 190Oropharyngeal pain150Dyspnea100Musculoskeletal and connective tissue disorders Musculoskeletal pain 276Arthralgia230Muscle spasms192Nervous system disorders Dizziness210Headache192Peripheral neuropathy100Metabolism and nutritiondisordersDecreased appetite172Neoplasms benign,malignant, unspecified Second malignancies 100Injury, poisoning andprocedural complications Laceration102Psychiatric disorders Anxiety100Insomnia100Vascular disorders Hypertension178Table 4: Treatment-Emergent Decrease of Hemoglobin, Platelets, or Neutrophils inPatients with CLL (N=48) in Study 1Percent of Patients (N=48)All Grades (%)Grade 3 or 4 (%)Platelets Decreased7110One patient death due to histiocytic sarcoma.****Neutrophils Decreased 5427Hemoglobin Decreased 440Study 2Adverse reactions and laboratory abnormalities described below in Tables 5 and 6 reflect exposure to IMBRUVICA with a median duration of 8.6 months and exposure to ofatumumab with a median of 5.3months in Study 2.Table 5: Non-Hematologic Adverse Reactions ≥ 10% Reported in Study 2IMBRUVICA (N=195)Ofatumumab (N=191)System Organ Class ADRTermAll Grades (%)Grade 3 or 4(%)All Grades (%)Grade 3 or 4(%)Subjects with multiple events for a given ADR term are counted once only for each ADR term.Gastrointestinal disorders Diarrhea 484182 Nausea 262180 Stomatitis 17161 Constipation 15090 Vomiting 14061General disorders andadministration site conditions Fatigue 282302 Pyrexia 242151Infections and infestations Upper respiratory tractinfection 161112Pneumonia 1510139 Sinusitis 11160 Urinary tract infection 10451Skin and subcutaneous tissue disorders Rash 243130 Petechiae 14010 Bruising 12010Musculoskeletal andconnective tissue disorders Musculoskeletal Pain 282181 Arthralgia 17170Nervous system disorders Headache 14160 Dizziness 11050Injury, poisoning and procedural complications Contusion 11030Eye disorders Vision blurred 10030Based on laboratory measurements per IWCLL criteria and adverse reactions******The system organ class and individual ADR terms are sorted in descending frequency order.*Nervous system disorders Dizziness140Headache 130Neoplasms benign, malignant,and unspecified (including cysts and polyps)Skin cancer 110Table 8: Treatment-Emergent Decrease of Hemoglobin, Platelets, or Neutrophils inPatients with WM (N=63)Percent of Patients (N=63)All Grades (%)Grade 3 or 4 (%)*Platelets Decreased 4313Neutrophils Decreased 4419Hemoglobin Decreased1386. 2 Postmarketing ExperienceThe following adverse reactions have been identified during post-approval use of IMBRUVICA.Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.Hypersensitivity reactions including anaphylactic shock (fatal), urticaria, and angioedema have been reported.7 DRUG INTERACTIONSIbrutinib is primarily metabolized by cytochrome P450 enzyme 3A.7.1 CYP3A InhibitorsIn healthy volunteers, co-administration of ketoconazole, a strong CYP3A inhibitor, increased C and AUC of ibrutinib by 29- and 24-fold, respectively. The highest ibrutinib dose evaluated in clinical trials was 12.5 mg/kg (actual doses of 840 – 1400 mg) given for 28 days with single dose AUC values of 1445 ± 869 ng · hr/mL which is approximately 50% greater than steady state exposures seen at the highest indicated dose (560 mg).Avoid concomitant administration of IMBRUVICA with strong or moderate inhibitors of CYP3A. For strong CYP3A inhibitors used short-term (e.g., antifungals and antibiotics for 7 days or less, e.g.,ketoconazole, itraconazole, voriconazole, posaconazole, clarithromycin, telithromycin) considerinterrupting IMBRUVICA therapy during the duration of inhibitor use. Avoid strong CYP3A inhibitors that are needed chronically. If a moderate CYP3A inhibitor must be used, reduce the IMBRUVICA dose. Patients taking concomitant strong or moderate CYP3A4 inhibitors should be monitored more closely for signs of IMBRUVICA toxicity [see Dosage and Administration (2.4)].Avoid grapefruit and Seville oranges during IMBRUVICA treatment, as these contain moderate inhibitors of CYP3A [see Dosage and Administration (2.4), and Clinical Pharmacology (12.3)].7.2 CYP3A InducersAdministration of IMBRUVICA with rifampin, a strong CYP3A inducer, decreased ibrutinib C and AUC by approximately 13- and 10-fold, respectively.Avoid concomitant use of strong CYP3A inducers (e.g., carbamazepine, rifampin, phenytoin and St.John's Wort). Consider alternative agents with less CYP3A induction [see Clinical Pharmacology (12.3)].Includes multiple ADR terms.**Based on laboratory measurements.max max8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category D [see Warnings and Precautions (5.7)].Risk SummaryBased on findings in animals, IMBRUVICA can cause fetal harm when administered to a pregnant woman. If IMBRUVICA is used during pregnancy or if the patient becomes pregnant while taking IMBRUVICA, the patient should be apprised of the potential hazard to the fetus.Animal DataIbrutinib was administered orally to pregnant rats during the period of organogenesis at oral doses of 10, 40 and 80 mg/kg/day. Ibrutinib at a dose of 80 mg/kg/day was associated with visceral malformations (heart and major vessels) and increased post-implantation loss. The dose of 80 mg/kg/day in animals is approximately 14 times the exposure (AUC) in patients with MCL and 20 times the exposure in patients with CLL or WM administered the dose of 560 mg daily and 420 mg daily, respectively. Ibrutinib at doses of 40 mg/kg/day or greater was associated with decreased fetal weights. The dose of 40 mg/kg/day in animals is approximately 6 times the exposure (AUC) in patients with MCL administered the dose of 560 mg daily.8.3 Nursing MothersIt is not known whether ibrutinib is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from IMBRUVICA, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.8.4 Pediatric UseThe safety and effectiveness of IMBRUVICA in pediatric patients has not been established.8.5 Geriatric UseOf the 111 patients treated for MCL, 63% were 65 years of age or older. No overall differences in effectiveness were observed between these patients and younger patients. Cardiac adverse events (atrial fibrillation and hypertension), infections (pneumonia and cellulitis) and gastrointestinal events (diarrhea and dehydration) occurred more frequently among elderly patients.Of the 391 patients randomized in Study 2, 61% were ≥ 65 years of age. No overall differences in effectiveness were observed between age groups. Grade 3 or higher adverse events occurred more frequently among elderly patients treated with IMBRUVICA (61% of patients age ≥ 65 versus 51% of younger patients) [see Clinical Studies (14.2)].Of the 63 patients treated for WM, 59% were 65 years of age or older. No overall differences in effectiveness were observed between these patients and younger patients. Cardiac adverse events (atrial fibrillation and hypertension), and infections (pneumonia and urinary tract infection) occurred more frequently among elderly patients.8.6 Renal ImpairmentLess than 1% of ibrutinib is excreted renally. Ibrutinib exposure is not altered in patients with Creatinine clearance (CLcr) > 25 mL/min. There are no data in patients with severe renal impairment (CLcr < 25 mL/min) or patients on dialysis [see Clinical Pharmacology (12.3)].8.7 Hepatic ImpairmentIbrutinib is metabolized in the liver. In a hepatic impairment study, data showed an increase in ibrutinib exposure. Following single dose administration, the AUC of ibrutinib increased 2.7-, 8.2- and 9.8-fold in subjects with mild (Child-Pugh class A), moderate (Child-Pugh class B), and severe (Child-Pugh class C) hepatic impairment compared to subjects with normal liver function. The safety of IMBRUVICA has not been evaluated in patients with hepatic impairment.Monitor patients for signs of IMBRUVICA toxicity and follow dose modification guidance as needed. It is not recommended to administer IMBRUVICA to patients with moderate or severe hepatic impairment (Child-Pugh classes B and C) [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3)].8.8 Females and Males of Reproductive PotentialAdvise women to avoid becoming pregnant while taking IMBRUVICA because IMBRUVICA can cause fetal harm [see Use in Specific Populations (8.1)].8.9 PlasmapheresisManagement of hyperviscosity in patients with WM may include plasmapheresis before and during treatment with IMBRUVICA. Modifications to IMBRUVICA dosing are not required.11 DESCRIPTIONIbrutinib is an inhibitor of Bruton's tyrosine kinase (BTK). It is a white to off-white solid with the empirical formula C25H24N6O2 and a molecular weight 440.50. Ibrutinib is freely soluble in dimethyl sulfoxide, soluble in methanol and practically insoluble in water.The chemical name for ibrutinib is 1-[(3R)-3-[4-amino-3-(4-phenoxyphenyl)-1H-pyrazolo[3,4-d]pyrimidin-1-yl]-1-piperidinyl]-2-propen-1-one and has the following structure:IMBRUVICA (ibrutinib) capsules for oral administration are supplied as white opaque capsules that contain 140 mg ibrutinib as the active ingredient. Each capsule also contains the following inactive ingredients: croscarmellose sodium, magnesium stearate, microcrystalline cellulose, sodium lauryl sulfate. The capsule shell contains gelatin, titanium dioxide and black ink. Each white opaque capsule is marked with "ibr 140 mg" in black ink.12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionIbrutinib is a small-molecule inhibitor of BTK. Ibrutinib forms a covalent bond with a cysteine residue in the BTK active site, leading to inhibition of BTK enzymatic activity. BTK is a signaling molecule of the B-cell antigen receptor (BCR) and cytokine receptor pathways. BTK's role in signaling through the B-cell surface receptors results in activation of pathways necessary for B-cell trafficking, chemotaxis,and adhesion. Nonclinical studies show that ibrutinib inhibits malignant B-cell proliferation and survival in vivo as well as cell migration and substrate adhesion in vitro.12.2 PharmacodynamicsIn patients with recurrent B-cell lymphoma > 90% occupancy of the BTK active site in peripheral blood mononuclear cells was observed up to 24 hours after ibrutinib doses of ≥ 2.5 mg/kg/day (≥ 175 mg/day for average weight of 70 kg).12.3 PharmacokineticsAbsorptionIbrutinib is absorbed after oral administration with a median T of 1 to 2 hours. Ibrutinib exposure increases with doses up to 840 mg. The steady-state AUC (mean ± standard deviation) observed in patients at 560 mg is 953 ± 705 ng·h/mL and in patients at 420 mg is 680 ± 517 ng·h/mL. Administration with food increased ibrutinib C and AUC by approximately 2 to 4- and 2-fold, respectively,compared with administration of ibrutinib after overnight fasting.DistributionReversible binding of ibrutinib to human plasma protein in vitro was 97.3% with no concentration dependence in the range of 50 to 1000 ng/mL. The volume of distribution at steady state (V ) was 683L, and the apparent volume of distribution at steady state (V /F) was approximately 10000 L.MetabolismMetabolism is the main route of elimination for ibrutinib. It is metabolized to several metabolitesprimarily by cytochrome P450, CYP3A, and to a minor extent by CYP2D6. The active metabolite, PCI-45227, is a dihydrodiol metabolite with inhibitory activity towards BTK approximately 15 times lower than that of ibrutinib. The range of the mean metabolite to parent ratio for PCI-45227 at steady-state is 1to 2.8.EliminationIntravenous clearance was 62 and 76 L/h in fasted and fed conditions, respectively. In line with the high first-pass effect, the apparent oral clearance is approximately 2000 and 1000 L/h in fasted and fed conditions, respectively. The half-life of ibrutinib is 4 to 6 hours.Ibrutinib, mainly in the form of metabolites, is eliminated primarily via feces. After a single oraladministration of radiolabeled [C]-ibrutinib in healthy subjects, approximately 90% of radioactivity was excreted within 168 hours, with the majority (80%) excreted in the feces and less than 10%accounted for in urine. Unchanged ibrutinib accounted for approximately 1% of the radiolabeled excretion product in feces and none in urine, with the remainder of the dose being metabolites.AgeAge (37 to 84 years) does not alter ibrutinib systemic clearance.GenderGender does not alter ibrutinib systemic clearance.Renal ImpairmentIbrutinib is not significantly cleared renally; urinary excretion of metabolites is < 10% of the dose.max max d,ss d,ss 14Creatinine clearance > 25 mL/min had no influence on the exposure to IMBRUVICA. There are no data in patients with severe renal impairment (CLcr < 25 mL/min) or in patients on dialysis.Hepatic ImpairmentIbrutinib is metabolized in the liver. In a hepatic impairment trial, a single dose of 140 mg ofIMBRUVICA was administered in non-cancer subjects. Ibrutinib AUC increased 2.7-, 8.2- and 9.8-fold,respectively, in subjects with mild (n=6), moderate (n=10) and severe (n=8) hepatic impairment relative to subjects with normal liver function. Ibrutinib C increased 5.2-, 8.8- and 7.0-fold, respectively, in subjects with mild, moderate and severe hepatic impairment relative to subjects with normal liver function [see Use in Specific Populations (8.7)].Drug InteractionsCoadministration of Ibrutinib with CYP3A InhibitorsIn a sequential design trial of 18 healthy, fasted volunteers, a single dose of 120 mg of IMBRUVICA was administered alone on Day 1 and a single dose of 40 mg of IMBRUVICA was administered on Day 7 in combination with 400 mg of ketoconazole (given daily on Days 4 – 9). Ketoconazole increased ibrutinib dose-normalized C and AUC 29-fold and 24-fold, respectively. Simulations using fasted conditions indicate that moderate CYP3A inhibitors diltiazem and erythromycin may increase AUC of ibrutinib by 5- to 8-fold.Coadministration of Ibrutinib with CYP3A InducersPK data from a dedicated drug interaction trial showed that rifampin (a strong CYP3A inducer)decreases ibrutinib C and AUC by more than 13- and 10-fold. Simulations using PBPK suggested that a moderate CYP3A inducer (efavirenz) may decrease the AUC of ibrutinib by up to 3-fold.Coadministration of Ibrutinib with CYP SubstratesIn vitro studies indicated that ibrutinib (I/Ki < 0.07 using mean C at 560 mg) and PCI-45227 (I/Ki <0.03) are unlikely to be inhibitors of any major CYPs at clinical doses. Both ibrutinib and the PCI-45227are weak inducers of CYP450 isoenzymes in vitro.Coadministration of Ibrutinib with Substrates of TransportersIn vitro studies indicated that ibrutinib is not a substrate of p-glycoprotein (P-gp). Systemic ibrutinib is unlikely to be an inhibitor of P-gp at clinical doses ([I]/Ki < 0.1). However, it may have an effect on P-gp substrates in the GI tract due to higher local concentrations after an oral dose. Co-administration of oral narrow therapeutic index P-gp substrates (e.g., digoxin) with IMBRUVICA may increase their blood concentration.13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenicity studies have not been conducted with ibrutinib.Ibrutinib was not mutagenic in a bacterial mutagenicity (Ames) assay, was not clastogenic in a chromosome aberration assay in mammalian (CHO) cells, nor was it clastogenic in an in vivo bone marrow micronucleus assay in mice at doses up to 2000 mg/kg.Fertility studies with ibrutinib have not been conducted in animals. In the general toxicology studies conducted in rats and dogs, orally administered ibrutinib did not result in adverse effects onreproductive organs.14 CLINICAL STUDIES14.1 Mantle Cell Lymphomamax max max max 1The safety and efficacy of IMBRUVICA in patients with MCL who have received at least one prior therapy were evaluated in an open-label, multi-center, single-arm trial of 111 previously treated patients. The median age was 68 years (range, 40 to 84 years), 77% were male, and 92% were Caucasian. At baseline, 89% of patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 42 months, and median number of prior treatments was 3 (range, 1 to 5 treatments), including 11% with prior stem cell transplant. At baseline, 39% of subjects had at least one tumor ≥ 5 cm, 49% had bone marrow involvement, and 54% had extranodal involvement at screening. IMBRUVICA was administered orally at 560 mg once daily until disease progression or unacceptable toxicity. Tumor response was assessed according to the revised International Working Group (IWG) for non-Hodgkin's lymphoma (NHL) criteria. The primary endpoint in this study was investigator-assessed overall response rate (ORR). Responses to IMBRUVICA are shown in Table 9.Table 9: Overall Response Rate (ORR) and Duration of Response (DOR)Based on Investigator Assessment in Patients with MCLTotal (N=111)ORR (%)65.895% CI (%)(56.2, 74.5)CR (%)17.1PR (%)48.6Median DOR months (95% CI)17.5 (15.8, NR)CI = confidence interval; CR = complete response; PR = partial response; NR =not reachedAn Independent Review Committee (IRC) performed independent reading and interpretation of imaging scans. The IRC review demonstrated an ORR of 69%.The median time to response was 1.9 months.LymphocytosisUpon initiation of IMBRUVICA, a temporary increase in lymphocyte counts (i.e., ≥ 50% increase from baseline and above absolute lymphocyte count of 5,000/mcL) occurred in 33% of patients in the MCL study. The onset of isolated lymphocytosis occurs during the first few weeks of IMBRUVICA therapy and resolves by a median of 8 weeks.14.2 Chronic Lymphocytic LeukemiaThe safety and efficacy of IMBRUVICA in patients with CLL who have received at least one prior therapy were demonstrated in one uncontrolled trial and one randomized, controlled trial.Study 1An open-label, multi-center trial was conducted in 48 previously treated CLL patients. The median age was 67 years (range, 37 to 82 years), 71% were male, and 94% were Caucasian. All patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 80 months and the median number of prior treatments was 4 (range, 1 to 12 treatments). At baseline, 46% of subjects had at least one tumor ≥ 5 cm.IMBRUVICA was administered orally at 420 mg once daily until disease progression or unacceptable toxicity. The ORR and DOR were assessed using a modified version of the International Workshop on CLL Criteria by an Independent Review Committee. The ORR was 58.3% (95% CI: 43.2%, 72.4%), all partial responses. None of the patients achieved a complete response. The DOR ranged from 5.6 to 24.2+ months. The median DOR was not reached.Study 2。
伊布替尼代谢产物-概述说明以及解释

伊布替尼代谢产物-概述说明以及解释1.引言1.1 概述伊布替尼是一种广泛应用于治疗癌症的药物,被广泛用于乳腺癌、结直肠癌和胃癌等。
伊布替尼的治疗效果和安全性已经得到了临床实践的验证,然而对其代谢产物的研究仍然相对有限。
伊布替尼代谢产物是指伊布替尼经过代谢反应后生成的化合物,这些代谢产物在体内扮演着重要的药理学作用。
了解伊布替尼的代谢过程对于进一步研究其药理学作用具有重要意义。
伊布替尼的化学结构和特性决定了它在体内的代谢途径和代谢产物。
伊布替尼主要通过肝脏中的细胞色素P450酶系统进行代谢。
在代谢过程中,伊布替尼会发生氧化、还原、脱甲基等反应,生成多种代谢产物。
这些伊布替尼代谢产物具有不同的药理学特性。
一些代谢产物可能具有更高的药物活性,从而增强治疗效果;而其他代谢产物可能具有较低的活性,或者具有与伊布替尼不同的生物活性。
了解这些代谢产物的药理学特性,可以帮助我们更好地理解伊布替尼的治疗机制,以及在临床应用中的合理用药。
此外,伊布替尼代谢产物也具有一定的临床应用前景。
一些代谢产物可能具有更好的药物代谢动力学特性,如更好的药物代谢稳定性和更低的毒副作用。
因此,将伊布替尼的代谢产物作为新的药物分子进行研发和应用,可能会为临床治疗提供更多的选择。
总之,伊布替尼代谢产物在伊布替尼的药理学作用和临床应用中具有重要性。
研究伊布替尼的代谢过程和代谢产物,有助于更全面地认识伊布替尼的药效机制,并为进一步探索其临床应用前景提供了基础。
未来的研究可以着重于伊布替尼代谢产物的药代动力学特性和临床疗效评价,以推动伊布替尼代谢产物的深入应用和开发。
1.2文章结构文章结构部分的内容可以根据以下内容进行编写:本文将分为三个部分进行介绍:引言、正文和结论。
在引言部分,将对伊布替尼代谢产物进行概述,并说明本文的目的和结构。
在正文部分,首先将详细介绍伊布替尼的代谢过程。
其中包括伊布替尼的化学结构和特性,以及伊布替尼在人体内的代谢途径和产物。
伊布替尼治疗套细胞淋巴瘤
预防伊布替尼不良反应的措施
在使用伊布替尼治疗前,应进行全 面的身体检查,以预防可能的不良 反应。
伊布替尼治疗套细胞淋巴瘤不良反应的预防与管理
伊布替尼的不良反应预防
定期进行身体检查,及时了解身体 状况,避免药物副作用。
伊布替尼的不良反应管理
一旦出现不良反应,应立即停药并寻 求医生帮助,以减轻症状。
伊布替尼治疗套细胞淋巴瘤的注意事 项
套细胞淋巴瘤的临床表现
套细胞淋巴瘤常表现为淋巴结肿大、 无痛性肿块等症状。
套细胞淋巴瘤的病因与发病机制
套细胞淋巴瘤的病因
套细胞淋巴瘤可能由基因突变、免疫 系统异常等因素引起。
套细胞淋巴瘤的发病机制
套细胞淋巴瘤的发病机制涉及细胞增殖 失控和免疫逃逸等过程。
套细胞淋巴瘤的遗传因素
部分套细胞淋巴瘤患者存在家族遗传 倾向,与特定基因突变有关。
伊布替尼治疗套细胞淋巴瘤的副作用
伊布替尼治疗套细胞淋巴瘤可能会引起一些不良反应 ,如恶心、呕吐等。
伊布替尼治疗套细胞 淋巴瘤的不良反应与
处理
伊布替尼治疗套细胞淋巴瘤的常见不良反应
01.
伊布替尼的常见副作用
伊布替尼治疗套细胞淋巴瘤时,可 能出现恶心、呕吐、腹泻等消化系 统不适。
02.
伊布替尼对血液系统的影响
在服用伊布替尼期间,应注意饮食和 生活习惯,保持良好的心态。
伊布替尼治疗套细胞 淋巴瘤的生活质量评
估
伊布替尼治疗套细胞淋巴瘤对患者生活质量的影响
伊布替尼治疗套细胞淋巴瘤的效果
伊布替尼是一种靶向药物,对套细胞淋巴瘤有显著的治疗效果。
伊布替尼治疗套细胞淋巴瘤的副作用
虽然伊布替尼能有效治疗套细胞淋巴瘤,但也可能带来一些副作用。
伊布替尼的耐药机制

1.BTK突变Bruton酪氨酸激酶(BTK)是一种非受体酪氨酸激酶,在B细胞受体(BCR)信号传导通路中起到关键作用,促使B细胞的生长和存活[1]。
伊布替尼作为一种BTK抑制剂,能有效抑制BTK的活性,从而对慢性淋巴细胞白血病(CLL)具有显著的治疗效果[2]。
然而,耐药现象已经成为一个临床难题。
研究发现,耐药CLL患者体内的BTK基因发生了突变,其中最常见的是C481S突变[3]。
这种突变使得伊布替尼与BTK的结合受到阻碍,从而降低了药物的疗效。
另外,还发现了其他一些较少见的BTK突变,如T316A和T474I等[4]。
针对BTK突变导致的耐药问题,研究者尝试开发新型BTK抑制剂,如ACP-196和ONO/GS-4059等,这些药物对C481S突变具有抑制作用,并在临床试验中取得了一定的疗效[5][6]。
为了充分了解BTK突变导致耐药的机制,研究者还在探索其他与BTK突变相关的信号通路,如PLCγ2、PI3K/Akt/mTOR和NF-κB等信号通路[7][8]。
这些信号通路在B细胞生存、增殖和抗凋亡中发挥关键作用,可能与伊布替尼耐药性的产生有关。
研究者还关注到非BTK突变引起的耐药机制,如信号通路相关基因突变、细胞表面受体改变等[9]。
这些非BTK突变的耐药机制可能与BTK突变共同作用,导致伊布替尼的治疗效果减弱。
BTK突变是伊布替尼耐药的重要原因之一,深入研究BTK突变和其他信号通路在耐药性中的作用,将有助于开发新型BTK抑制剂和优化慢性淋巴细胞白血病的治疗策略。
2.B细胞克隆演化慢性淋巴细胞白血病(CLL)的发展和进展是一个克隆演化的过程,其中患者体内的B细胞在治疗压力下不断演化和适应,导致耐药性的产生。
研究发现,CLL患者体内存在多个亚克隆(subclone),它们在治疗过程中通过竞争和选择逐渐产生抗药性亚克隆[10]。
Dan等人(2013)对一系列CLL患者进行了基因组测序,发现在伊布替尼治療過程中,部分患者体内的耐药亚克隆逐渐扩增,导致治疗失败[11]。
伊布替尼汇聚式合成策略
伊布替尼汇聚式合成策略
伊布替尼(Ibrutinib)是一种靶向治疗B细胞淋巴瘤和慢性淋巴细胞白血病的药物。
其汇聚式合成策略指的是通过多步反应将伊布替尼的结构单元逐步合成并连接起来,最终得到目标化合物的合成方法。
伊布替尼的汇聚式合成通常涉及以下关键步骤:
1.核心结构的合成:首先,合成伊布替尼的核心结构,这是药物的主要骨架。
核心结构通常包含多个芳香环和其他功能基团。
合成核心结构可以通过各种有机合成反应,如芳香化反应、羧酸衍生物的合成等。
2.功能基团的引入:接下来,在核心结构上引入特定的功能基团,这些功能基团对于药物的活性和选择性至关重要。
引入功能基团可以通过不同的官能团化反应,如亲核取代、还原反应、酯化等。
3.保护基团的应用:在合成过程中,可能需要在特定位置引入保护基团,以防止意外反应或保护化合物的特定官能团。
保护基团可以在适当的时机通过特定的保护反应引入,并在需要时通过去保护反应去除。
4.连接和最后步骤:在完成核心结构和功能基团的合成后,将它们连接在一起,并进行最后的化学转化步骤。
这可能包括环合反应、缩合反应、纯化和晶体化等步骤。
伊布替尼的汇聚式合成策略是一个复杂而精细的有机合成过程,需要合成化学家运用多种有机合成技术和策略,以高产率和高纯度合成目标化合物。
这样的合成方法在药物研发中具有重要的意义,可以为大规模生产提供可靠的合成路线。
1/ 1。
伊布替尼研究方法-概述说明以及解释

伊布替尼研究方法-概述说明以及解释1.引言1.1 概述概述:伊布替尼研究方法是一种针对伊布替尼进行研究的科学方法。
伊布替尼是一种广泛应用于临床治疗的药物,特别是在癌症治疗领域具有重要的价值。
因此,研究伊布替尼的方法至关重要,可以帮助科研人员更深入地了解其药理作用、药效、毒性等特性。
本文将就伊布替尼研究方法进行深入探讨,希望可以为相关领域的研究人员提供一定的参考和帮助。
1.2文章结构1.2 文章结构本文将分为以下几个部分来探讨伊布替尼研究方法。
首先,在引言部分中,将对伊布替尼以及其在医学领域的重要性进行概述,介绍本文的结构以及研究的目的。
接着在正文部分,将详细论述伊布替尼研究方法的要点,包括其特点、优势、应用范围等方面进行深入探讨。
最后,在结论部分,将对本文进行总结,同时探讨伊布替尼研究方法的意义和未来发展方向。
通过这样的结构安排,读者将能够全面了解伊布替尼研究方法的相关内容,为进一步深入研究提供基础和参考。
1.3 目的本文旨在探讨伊布替尼研究方法的关键要点,系统总结和归纳其在科学研究中的应用。
通过对伊布替尼研究方法的深入分析,可以帮助研究人员更加有效地设计实验方案,提高研究效率,优化实验结果的可靠性和准确性。
同时,对伊布替尼研究方法的探讨也有助于拓展学界对该领域的认识,推动相关领域的发展与进步。
通过本文的撰写,旨在为相关研究人员提供一定的参考和借鉴,促进伊布替尼领域更深入的研究和探讨。
2.正文2.1 伊布替尼研究方法要点1伊布替尼研究方法要点1:伊布替尼是一种常用的药物,用于治疗癫痫、焦虑症和其他神经系统疾病。
在研究伊布替尼的方法中,首先需要确定研究的目的和假设,以确保研究的科学性和可靠性。
其次,需要选择合适的研究对象和样本,例如动物模型或临床病例。
接着,确定研究的方法和实验设计,包括药物给药方案、实验组和对照组的设置等。
在实验过程中,需要准确记录实验数据,包括药物的剂量、疗效评估指标等,以便后续数据分析和结果解释。
伊布替尼治疗相关的淋巴细胞增多解读
IMBRUVICA® EU SmPC, October 2014.
淋巴细胞增多和欧盟说明书(EU SmPC)
支持信息
伊布替尼相关的淋巴细胞增多:不代表治疗失败
淋巴细胞增多代表淋巴细胞从淋巴组织外流1对于大多数患者,TR-L 在8个月内缓解1对于少数患者,淋巴细胞增多可能会持续>12个月1BTK 持续被抑制细胞不能通过BCR刺激这部分患者的PFS不劣于其他缓解类型的患者伊布替尼治疗时持久的淋巴细胞增多1:与独特的分子特征相关 不代表对治疗的响应不佳
1. Woyach JA, et al. Blood 2014;123(12):1810–7.
持续的淋巴细胞增多证据表明BTK和PLCγ2抑制, 但BCR信号通路下游分子上调1AKT和ERK基本保持胞质定位且不能被BCR信号的近端刺激激活,但可被CD40L激活 (即对BTK通路外的刺激敏感)1BCR靶基因未显示明显上调1没有证据表明克隆多样性,克隆进化,或不同的Zap-70甲基化1增殖不活跃且不会拘泥于一条信号通路1与伊布替尼治疗后不良预后无关1
4. Hallek M, et al. Blood 2012;; Accessed 12 March 2015. 5. Byrd JC, et al. N Engl J Med 2014;371(3):213–23.
伊布替尼的全面解析

伊布替尼在其他疾病中的应用
伊布替尼在癌症治疗中的应用
伊布替尼是一种靶向药物,主要用 于治疗慢性髓性白血病和胃肠道间 质瘤等恶性肿瘤。
伊布替尼在免疫性疾病中的作用
伊布替尼能够抑制免疫系统的过度 反应,被用于治疗类风湿关节炎等 自身免疫性疾病。
伊布替尼在心血管疾病中的疗效
伊布替尼可以降低心脏负荷,改善心 脏功能,对心力衰竭等心血管疾病有 一定的治疗效果。
02 03
伊布替尼在不同地区的市场规模差异
由于不同地区的医疗水平和经济条件的差异,伊布替尼在各个地区的市场规 模存在明显差异。
伊布替尼市场的发展趋势
随着人们对健康的重视和医疗技术的进步,伊布替尼市场有望继续保持稳定 增长的趋势。
伊布替尼的市场竞争情况
01
伊布替尼的市场占有率
伊布替尼在全球市场中占据着重要地位, 其销售额和市场份额均在稳步增长。
01
02
03
伊布替尼与药物的相互作用
伊布替尼可能与某些药物发生相互作用, 影响其疗效或增加不良反应的风险。
伊布替尼与食物的相互作用
伊布替尼在与某些食物同时摄入时可能会 影响其吸收和代谢,需注意合理搭配饮食 。
伊布替尼与其他治疗的相互作用
伊布替尼可能与其他治疗方法(如放疗、 化疗等)产生相互作用,需谨慎选择治疗 方案。
伊布替尼的市场竞争
尽管伊布替尼在肿瘤治疗领域表现 出色,但仍需面对来自其他药物的 竞争压力。
伊布替尼的市场潜力
由于其独特的治疗效果和较低的 副作用,伊布替尼具有巨大的市 场潜力和发展空间。
伊布替尼的市场风险
01
竞争风险
伊布替尼面临来自其他抗癌药物 的激烈竞争,可能导致市场份额 下降。
伊布替尼结构式
伊布替尼结构式
伊布替尼结构式是一种化学结构式,它是用来描述化学物质中原
子之间的连接方式和组成比例的。
在化学领域中,它是最基本的化学
符号之一。
本文将围绕伊布替尼结构式展开讲述,以帮助读者更好地
理解。
步骤1:理解伊布替尼结构式的基本概念
伊布替尼结构式的基本概念是原子、分子、化学键和分子式。
原
子是组成物质的最基本单元,而分子是由两个或多个原子通过化学键
连接而成的。
化学键是原子之间的一种物理连接方式,可以是共价键
或离子键。
分子式则是用来表示化学物质中各元素的相对数量的符号
和数字组合,例如H2O表示一个水分子中有两个氢原子和一个氧原子。
步骤2:学习如何绘制伊布替尼结构式
绘制伊布替尼结构式需要使用化学元素符号和化学键。
化学元素
符号是用以表示化学元素的缩写符号,例如H代表氢,O代表氧等等。
化学键包括共价键和离子键,在绘制化学结构式时需要注意选择适当
的化学键来连接各个原子。
步骤3:掌握伊布替尼结构式的应用
伊布替尼结构式在化学中有着广泛的应用,例如可以用来表示有
机化合物、无机盐、酸和碱等物质。
通过伊布替尼结构式,可以更清
晰地表达化学物质的组成和性质,以便更好地理解和研究化学现象。
总结:伊布替尼结构式是化学中最基本的化学结构式之一,它用
化学元素符号和化学键来描述原子之间的连接方式和组成比例。
学习
伊布替尼结构式需要理解化学元素、分子式和化学键等基本概念,掌
握绘制技巧和应用场景。
只有深入掌握伊布替尼结构式,才能更好地
理解化学基础知识,为科学研究和应用做出贡献。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
导读
此文为深入浅出的伊布替尼中文版说明书解读,阐述问题如下:
1、伊布替尼适应症
2、伊布替尼的规格用量和用法
3、不宜使用伊布替尼的群体
4、伊布替尼副作用及处理方法
5、药物冲突注意事项
官方版伊布替尼中文说明书百度文库即有,此文仅在于科普伊布替尼应用知识。
作为处方药物,患者在使用伊布替尼时,一定要谨遵医嘱。
一、伊布替尼适应症
已获美国药监局审批的伊布替尼七大适应症中,除移植性抗宿主病外,其余皆为肿瘤适应症。
1、治疗前期接受过至少一次来那度胺或者其他药物治疗的套细胞淋巴瘤。
2、治疗既往接受过至少一次治疗的慢性淋巴细胞白血病。
3、治疗携带del 17p删除突变的慢性淋巴细胞白血病。
4、治疗华氏巨球蛋白血症。
5、一线治疗慢性淋巴细胞白血病。
6、治疗伴有或不伴有染色体17p删除突变(del 17p)的小淋巴细胞性淋巴瘤。
7、治疗先前有治疗失败经历的慢性移植物抗宿主病。
二、伊布替尼的规格用量和用法
1、规格
伊布替尼每粒含药物成分140毫克,有两种规格:
(1)每瓶90粒。
(2)每颗120粒。
2、用量
(1)套细胞淋巴瘤患者每日口服560毫克药物。
(2)其他肿瘤患者以及慢性移植物抗宿主病患者每日推荐剂量为420毫克。
3、用法
每日定时口服一次,不应碾碎、咀嚼胶囊。
数据显示随餐或餐后服用较之空腹服用更有利于吸收,因此建议饭后半小时内温水送服。
漏服应立即补服;若发现漏服时距离下次定点用药时间较近,则跳过该次用药,于定点时间用药。
注意:不可因漏服而补服双倍剂量。
三、不宜使用伊布替尼的群体
1、中至重度肝功能不全者不应用药,轻度肝受损者推荐剂量为140毫克每日。
2、尚无数据显示药物存于母乳,但禁止母乳喂养。
3、未确认儿童用药的安全性和有效性,儿童不应用药。
4、药物危害胎儿安全,妊娠期妇女禁用,用药女性应做好避孕措施。
5、女性患者用药结束后的一个月内避免怀孕,男性患者治疗结束后的3个月内避免生育。
四、伊布替尼副作用和处理方法
1、伊布替尼一般性副作用有:恶心、腹泻、疲劳、外周水肿、淤血、皮疹、关节痛、肌肉骨骼疼痛、上呼吸道感染、肺炎等。
2、服用伊布替尼后的具体副作用
(1)套细胞淋巴瘤用药后具体副作用为:疲惫贫血、恶心呕吐、腹泻、腹疼、便秘、皮疹、食欲降低、呼吸困难、上呼吸道感染、外周水肿、肌肉骨骼痛疼、瘀伤、血小板减少、中性粒细胞减少。
(2)慢性淋巴细胞白血病用药后具体副作用有:疲乏贫血、恶心眩晕、皮疹、发热、窦炎、口腔炎、腹泻或便秘、瘀伤、周边水肿、关节痛、肌肉骨骼痛、上呼吸道感染、血小板减少、中性粒细胞减少。
(3)华氏巨球蛋白血症用药后的具体副作用有:腹泻、贫血、疲乏、恶心、瘀伤、皮疹、肌肉骨骼疼痛、上呼吸道感染、血小板减少、中性粒细胞减少。
(4)慢性移植物抗宿主病用药后具体副作用是:疲劳、贫血、恶心、腹泻、瘀伤、肺炎、口腔炎症、肌肉筋挛、血小板减少、甚至出血。
3、伊布替尼严重副作用及处理方法
出血:对有出血症状的患者进行监视。
感染:对有发热和感染症状的患者跟踪监测以便及时处理。
全血细胞减少症:为骨髓造血功能衰竭所导致的一种全血减少综合征。
用药后应每月检查患者全血细胞计数。
肾毒性:半数患者用药后出现肌酐水平增加至正常上限的1.5倍。
用药后定期监视患者肾功能和保持水化。
注意:在针对套细胞淋巴瘤的临床实验中,共有5%的用药患者发生了其他恶性肿瘤,主要为皮肤癌。
4、药物副作用与剂量调整
(1)出现以下状况时中断用药:①非血液学不良反应≥3 级;②有感染或发热症状的中性粒细胞减少症≥3 级;③血液学毒性=4级。
(2)恢复剂量:中断用药后,当不良反应症状缓解至1 级或消失时,恢复最初的用药剂量。
(3)初次减量:恢复剂量后,不良反应若再次出现,可先减少胶囊1粒继续服用。
(4)再次减量:减少剂量后若不良反应仍然持续,再次减少胶囊1 粒继续服用。
(5)终止用药:不良反应仍持续出现或复发,终止用药。
注:MCL为套细胞淋巴瘤,CLL为慢性淋巴细胞白血病,WM为华氏巨球蛋白血症。
五、药物冲突与剂量调整
1、CYP3A抑制药
禁止与CYP3A 强抑制剂共同给药,如必须使用CYP3A 强抑制剂,则中断伊布替尼用药,;中度CYP3A抑制剂必须使用时,降低伊布替尼使用剂量至140毫克。
当CYP3A抑制药与伊布替尼共同使用时,密切观察使用者的不良反应。
在可以使用CYP3A 抑制作用较小的代替药物时,不要使用强或中抑制剂。
2、CYP3A诱导剂
CYP3A诱导剂会降低伊布替尼的血浆浓度,不宜与伊布替尼共同给药,如必须使用时,请选择较弱的CYP3A 诱导剂。
3、呋喃香豆素
呋喃香豆素天然存在于柑橘类水果中,该成分会抑制人体内分解药物的酶活性,从而导致进入血液的药量倍增,服用伊布替尼期间不用食用柑橘、柠檬类水果。
温情提示
作为抗癌靶向药物,伊布替尼的使用应谨遵医嘱,患者切不可凭一己之见、依靠对药物说明书的理解来解决问题,任何突发性情况或疑问都应联系主治医师予以应对。