最新美国临床内分泌学家协会和美国内分泌外科协会治疗肾上腺偶发瘤的管理准则
偶发性肾上腺皮质肿瘤34例诊治体会

偶发性肾上腺皮质肿瘤34例诊治体会
郭彬;吴开俊
【期刊名称】《实用医学杂志》
【年(卷),期】2002(018)005
【摘要】目的:为提高偶发性肾上腺皮质肿瘤的诊治效果.方法:采取回顾性研究对34例偶发性肾上腺皮质肿瘤进行总结.结果:偶发性肾上腺皮质肿瘤中良性肿瘤29例,肾上腺皮质癌5例.在良性肿瘤中无功能性肿瘤8例,有激素分泌功能者21例,其中临床前原发性醛固酮增多症10例,血醛固酮轻度增高,肾素偏低;临床前柯兴氏征11例,血皮质醇轻度增高.肾上腺皮质球状带肿瘤直径为0.7~2.6 cm,CT值-7~25.3 Hu.束状带肿瘤直径2.5~6.0 cm,CT值25.6~39.5 Hu.肾上腺皮质癌24 h 尿17 KS增高.结论:偶发性肾上腺皮质肿瘤应根据影像检查和内分泌测定综合分析作出诊断,肿瘤直径>2 cm,具有激素分泌功能的肿瘤应采取手术治疗.
【总页数】2页(P496-497)
【作者】郭彬;吴开俊
【作者单位】510120,广州医学院第一附属医院泌尿外科;510120,广州医学院第一附属医院泌尿外科
【正文语种】中文
【中图分类】R73
【相关文献】
1.偶发性小肾癌的诊治体会(附31例报告) [J], 庄乾元;周四维;郭小林;杜光辉;管维
2.偶发性肾癌28例诊治体会 [J], 周树军;张跃平
3.黏液性肾上腺皮质肿瘤1例 [J], 黄东东;左志博;邬万新;汪静宇;袁琳娜;王振;郭志琴
4.偶发性肾癌的诊治体会(附44例报告) [J], 颜克钧;王林辉;孙颖浩;钱松溪;马永江
5.无症状性(偶发性)嗜铬细胞瘤诊治体会 [J], 罗尉;杨之明;经霄;杜传军;顾才校因版权原因,仅展示原文概要,查看原文内容请购买。
胰腺导管内乳头状黏液性肿瘤的管更新要点及解读2024
胰腺导管内乳头状黏液性肿瘤的管更新要点及解读2024摘要胰腺导管内乳头状黏液性肿瘤(IPMN)是胰腺癌的主要癌前病变之一,一旦考虑其发生癌变,则需及时手术干预。
2022-07-07,第26届国际胰腺病会议在日本京都举行,期间就进一步修订IPMN诊治指南展开讨论,并制订了新版IPMN诊治指南——京都指南。
该版指南系统评价5个主题的证据:高危征象和担忧特征的定义、非手术切除IPMN的随访原则、手术切除IPMN的随访原则、病理学特征及囊液分子标记物的研究。
2006年,国际胰腺病协会(International Association of Pancreatology,IAP)发布首部胰腺导管内乳头状黏液性肿瘤(intraductal papillary mucinous neoplasm,IPMN)和黏液囊性肿瘤的诊治指南[1];并分别于2012年和2017年进行修订[2-3]。
2022-07-07,第26届国际胰腺病会议在日本京都举行,期间就进一步修订IPMN诊治指南展开讨论,依据2019年苏格兰校际指南网络(Scottish Intercollegiate Guidelines Network,SIGN)对以下5个主题的证据以临床问题(clinical question,CQ)的形式进行系统评价(表1):高危征象(high-risk stigmata,HRS)和担忧特征(worrisome features,WF)的定义、非手术切除IPMN的随访原则、手术切除IPMN的随访原则、病理学特征、囊液分子标记物的研究,并对IPMN诊治指南进行更新(以下简称新版IPMN指南),于2023-12-28在线发表于Pancreatology杂志[4]。
本文将对新版IPMN指南更新要点进行解读。
1 风险评估及手术指征自2012年版IPMN和黏液囊性肿瘤的诊治指南发布以来,IPMN病人出现高级别异型增生(high-grade dysplasia, HGD)或侵袭性癌(invasive carcinoma,IC)的临床和影像学特征被称为HRS和WF[2]。
肾上腺肿瘤的外科治疗
• 这个手术径路的问题是,相当大的皮肤切口影响 病人在术后恢复和切口愈合过程中得舒适性,同 时降低了抵抗感染的能力。后路经腰部肌肉的径 路(腹膜外经路),患者能更好的耐受,同时有 更低的感染率。胸腹腔径路和前外侧的胸腔径路 (打开膈肌),很少使用,主要是在恶性的巨大 的肾上腺肿瘤时使用。
• 腹腔镜手术已成为手术治疗肾上腺的参考方法, 尽管不断的有反对意见提出,主要是针对恶性肿 瘤的情况。不过,许多的研究证实,该方法能够 允许医生遵守肿瘤外科的治疗原则,同时一并清 除侵入性的肿瘤。由于这个原因,微创肾上腺切 除术不同的变化已经成为一种不可分割的一部分, 被认为是内分泌外科手术治疗的根本途径。
• 这三个事件对肾上腺肿瘤的外科治疗的策略,已 经造成了一个根本的影响。外科医生现在不仅可 以选择到达肾上腺径路,而且可以选择手术的技 术:传统或腹腔镜技术。后者,和传统的外科相 比,由于被广泛接受,已经导致了剧烈的增长从 而快速发展。其外科治疗的原理和目的仍然是相 同。手术方法取决于:病理情况、肿瘤的大小、 性能状况以及科医生的经验。
• 激素不活跃的肿瘤(偶发瘤)恶性的危险性估计 在4–5%左右。如果直径超过4cm,那么危险性随 着体积的增大逐渐按百分比增加。直径4cm,危 险估计10%左右, 如果肿瘤超过6cm,危险估计 25–98%左右。所以,对没有激素活性的肿瘤, 外科治疗的标准,仍然是肿瘤的尺寸。能够被接 受的分界点是4cm。在一些中心,自从引进了腹 腔镜肾上腺切除术治疗肾上腺病变的方法之后, 直径> 3 cm 的肿瘤,低危的年轻病人可以手术。
• 在其他情况下(无激素活性病灶,偶发瘤,转 移性肿瘤特别是异时性肿瘤),电视腹腔镜 / 腹腔镜方法是优选的方法。这也发生在我 们的经验 。 • 有肾上腺病理学支持的肾上腺病人,具体 的方法如图3所示。
肾上腺切除术介绍
肾上腺切除术介绍肾上腺切除术是针对良性和恶性肿瘤进行的治疗。
肾上腺切除术的手术方式逐渐趋于微创的方式进行。
无论采用什么方式进行手术,肾上腺切除术都是一项难度较大的手术。
手术方法的选择:肾上腺切除术可以经腹部,腹膜后或经胸部进行。
经腹肾上腺切除术更常进行,可以采用开放式或微创手术技术完成。
开腹经腹肾上腺切除术可以通过前腹部或胸腹联合入路进行。
开腹腹膜后肾上腺切除术是通过后路手术完成的。
微创的手术方法包括腹腔镜经腹和后腹膜后镜(RPA)。
胸腹部肾上腺切除术是一种罕见的手术,用于非常大的肿瘤,通常伴有膈肌受累或肿瘤扩展到胸腔。
切除原则:无论手术方法如何,尽量减少肾上腺切除术的术中并发症的基本手术原则均相同,包括:手术区域必须在很好的视野下进行。
注意保护手术区域周围重要血管、神经、器官。
使用整体切除技术,完整切除肾上腺和肿瘤,以避免发生破裂。
肿瘤大小与手术入路的关系:在美国,无论大小如何,建议对已知或疑似的肾上腺皮质癌进行开放性肾上腺切除术并切除相邻淋巴结。
该建议得到了国家综合癌症网络(NCCN),美国临床内分泌学家协会(AACE)和美国内分泌外科医师协会(AAES)的认可。
开放手术有助于在必要时控制或切除相邻结构。
在欧洲,腹腔镜肾上腺切除术是针对直径<10cm的I期或II期ACC进行的。
该建议得到了欧洲内分泌外科医师学会的认可。
嗜铬细胞瘤:肾上腺嗜铬细胞瘤一般可在安全可行的情况下通过腹腔镜手术切除,术中在腹腔镜可视条件下不能很好止血的情况,需要中转开腹进行手术治疗。
随着影像学检查方法的进步,在治疗其他疾病的时候会越来越多的发现肾上腺病变(即肾上腺偶发瘤)。
这是需要评估所有肾上腺偶发瘤患者的恶性和激素功能亢进的可能性。
由于影像学研究中的侵略性特征(例如,不均匀,不规则边缘和局部侵袭)而对恶性肿瘤可疑的病变应该与已知的恶性肿瘤相同的方法治疗。
有时需要进行手术治疗。
这种情况下的肿瘤,微创手术是去除功能性和非功能性良性肾上腺肿块的金标准,包括嗜铬细胞瘤。
NCCN神经内分泌和肾上腺肿瘤指南2019.1版(5)
NCCN神经内分泌和肾上腺肿瘤指南2019.1版(5)目录病理诊断和病理报告原则(NE-A)NE-A,1/3报告内容英文版中文版必需报告的信息:●肿瘤的解剖部位●诊断●级别 (见表1)●有丝分裂率和/或Ki-67●肿瘤的大小●有无多中心性病灶●有无脉管侵犯●有无神经束侵犯●有无其它病理成分(如非神经内分泌成分)●淋巴结转移,包括阳性淋巴结数目以及送检淋巴结总数●切缘状况(报告阴性或阳性)●按AJCC TNM分期系统进行分期(见分期)可选择报告的信息:●一般的神经内分泌标志物的免疫组化染色结果●特殊肽的标志物的免疫组化染色结果●有无非缺血性肿瘤坏死●有无异常的组织学特征(如嗜酸瘤细胞、透明细胞、腺体形成等)●如果切缘距离肿瘤<0.5cm,要报告精确的距离●肿瘤所在器官除肿瘤外的病理背景(如胰腺腺管内上皮瘤、ECL 细胞增生)表1 a脚注:a.经授权许可转自以下文献:Bosman FT, Carneiro F, Hruban RH, Theise ND. World Health Organization Classification of Tumours of the Digestive System. IARC, Lyon, 2010.Travis WD, Brambilla E, Burke AP, et al. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. IARC, Lyon; 2015.Lloyd RV, Osamaru RY, Klöppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs. IARC, Lyon, 2017.b.预计与胃肠道神经内分泌肿瘤的分类相似。
NE-A,2/3功能状态;免疫组化和其它辅助技术;分类和分级;有丝分裂率;Ki-67指数英文版中文版功能状态●相同解剖部位的NET, 不论是功能性还是无功能性,不影响其病理诊断,因为肿瘤有无功能需依据临床症状进行判断,但不应改变其病理诊断。
业务学习-肾上腺偶发瘤

肾上腺偶发瘤肾上腺意外瘤(adrenal incidentaloma)是指那些没有明显肾上腺疾病的临床表现,在体格检查或检查非肾上腺疾病时经由腹部影像检查意外发现的肾上腺占位性病变。
由于计算机断层扫描(CT)、磁共振成像(MRI)和超声诊断技术的进步和广泛应用,肾上腺意外瘤的发现率很高,目前,已成为临床医生最常见的肾上腺疾病。
症状体征大多数肾上腺意外瘤为无高分泌功能的良性腺瘤,临床和实验室检查均无激素分泌增多的表现。
高功能的肾上腺意外瘤主要分泌皮质醇、雄激素、雌激素、盐皮质激素或儿茶酚胺,以相应激素增多引起的临床表现为主,如皮质醇增多常有向心性肥胖、高血压、糖耐量异常及骨质疏松等表现。
部分高分泌功能的肾上腺意外瘤无明显的临床症状称为寂静型高功能腺瘤,包括皮质醇分泌瘤、醛固酮分泌瘤及嗜铬细胞瘤,对此类皮质醇分泌瘤有人称为亚临床库欣综合征。
用药治疗1.肾上腺意外瘤的治疗原则①有激素分泌功能的应手术切除。
②肿瘤直径≥4cm的应手术切除。
③如明确为转移瘤,只影响一侧肾上腺,对侧肾上腺及其他部位都未发现转移瘤者,也可以将肾上腺转移瘤手术切除。
④直径<4cm者,如无恶性肿瘤的影像学特征,也无激素分泌功能,可以观察随访。
每3个月重复1次超声检查,每半年至1年重复CT和(或)MRI检查。
如发现肿瘤有明显增大,或激素测定显示有激素分泌功能,也应予以手术切除。
⑤肾上腺囊肿、髓脂瘤、血肿/出血、肾上腺结核,先天性肾上腺皮质增生等无手术的必要。
经典的手术方法是经腰切口入路的开放式手术。
现在国内外都有用腹腔镜进行手术的报道。
腹腔镜手术有经腹腔,也有不经腹腔在腹膜后进入的。
这种内镜手术创伤小,出血少、恢复快,但要求的技术比较高。
肿瘤比较大或怀疑是恶性肿瘤者,最好选择开放式手术。
2.目前对肾上腺意外瘤的处理,国外更倾向于采取积极主动的措施,对有激素分泌功能的肿块行手术切除,无激素分泌功能的肿块进行细针穿刺活检,如为恶性肿瘤或转移癌则采取手术切除或治疗原发癌;对于肿块体积大于5cm以及影像学疑为癌的患者也采取手术切除,小于5cm的肿块则随访观察,定期复查。
recist1标准

recist1标准RECIST1标准。
RECIST1标准是肿瘤疗效评价的国际通用标准,其全称为Response Evaluation Criteria in Solid Tumors。
该标准是由美国癌症研究协会(AACR)、国际抗癌联盟(UICC)和国家癌症研究所(NCI)共同制定的,旨在为临床试验和治疗提供一致的肿瘤反应评价标准。
RECIST1标准主要用于评估固体肿瘤的治疗效果,包括肿瘤的缩小、增大、稳定等情况。
该标准通过测量肿瘤的直径和体积变化,对肿瘤的治疗效果进行客观、标准化的评价,为临床医生提供科学依据,指导临床决策。
根据RECIST1标准,肿瘤治疗效果主要分为完全缩小(CR)、部分缩小(PR)、稳定(SD)、进展(PD)四种情况。
完全缩小指肿瘤在治疗后完全消失,部分缩小指肿瘤直径或体积减小超过一定比例,稳定指肿瘤直径或体积变化在一定范围内,进展指肿瘤直径或体积增大或出现新的病灶。
在临床实践中,RECIST1标准被广泛应用于肿瘤药物临床试验和临床治疗中。
通过对肿瘤治疗效果的准确评估,可以帮助临床医生及时调整治疗方案,提高患者的治疗效果和生存率。
同时,该标准也为不同临床试验结果的比较提供了统一的评价标准,促进了临床试验的开展和结果的解释。
需要注意的是,RECIST1标准虽然在临床实践中被广泛应用,但并不适用于所有类型的肿瘤治疗效果评价。
对于一些非固体肿瘤、转移性肿瘤或特殊类型肿瘤,需要结合其他评价指标进行综合评估。
因此,在使用RECIST1标准进行肿瘤治疗效果评价时,临床医生需要根据具体情况综合考虑,不可片面依赖标准结果。
总之,RECIST1标准作为肿瘤治疗效果评价的国际通用标准,对于临床试验和治疗具有重要意义。
通过对肿瘤治疗效果的客观、标准化评价,可以为临床医生提供科学依据,指导临床决策,提高患者的治疗效果和生存率。
然而,在实际应用中,需要结合具体情况综合考虑,不可片面依赖标准结果。
希望未来能够进一步完善和优化肿瘤疗效评价标准,为肿瘤患者的治疗带来更多的益处。
肾上腺偶发瘤的诊治(附30例报告)
肾上腺偶发瘤的诊治(附30例报告)
陈静;陆曙炎;周忠兴;吴小鹏
【期刊名称】《临床和实验医学杂志》
【年(卷),期】2006(5)12
【摘要】目的提高肾上腺偶发瘤的诊治水平.方法结合文献讨论30例肾上腺偶发瘤未被早期发现的原因,潜在的手术危险性,及需警惕恶性病变等临床特点.结果 30例患者均经内分泌功能测定、B超、CT等检查,23例手术中15例(65%)患者行后腹腔镜肾上腺肿瘤摘除术,8例(35%)行经腹或经腰肾上腺肿瘤摘除术.结论对于肾上腺偶发瘤必须结合内分泌检查,影像学检查,以排除有无内分泌功能及是否为恶性,后腹腔镜手术为肾上腺良性疾病的首选.
【总页数】2页(P1902,1905)
【作者】陈静;陆曙炎;周忠兴;吴小鹏
【作者单位】常州二院泌尿外科,江苏,常州,213003;常州二院泌尿外科,江苏,常州,213003;常州二院泌尿外科,江苏,常州,213003;常州二院泌尿外科,江苏,常
州,213003
【正文语种】中文
【中图分类】R73
【相关文献】
1.肾上腺成熟畸胎瘤的临床诊治(附2例报告) [J], 李杨乐;吴洪涛;姚干;赵晓昆
2.成人肾上腺神经母细胞瘤诊治(附病例报告) [J], 张英晨;蒋立城;程玉峰;王洪同;丁
吉阳
3.后腹腔镜治疗肾上腺偶发瘤(附18例报告) [J], 宋华;孙颖浩;许传亮
4.肾上腺偶发瘤的手术治疗(附47例报告) [J], 祝宇;吴瑜璇;孙福康;张祖豹
5.肾上腺偶发瘤的临床探讨(附50例报告) [J], 祝捷;唐孝达;朱江
因版权原因,仅展示原文概要,查看原文内容请购买。
肾上腺外科疾病诊断治疗指南

十五、肾上腺外科疾病诊断治疗指南一、嗜铬细胞瘤/副神经节瘤一、【概述】儿茶酚胺增多症(hypercatecholaminemia):由于肾上腺嗜铬细胞瘤、副神经节瘤(肾上腺外嗜铬细胞瘤)与肾上腺髓质增生的共同特点是肿瘤或肾上腺髓质的嗜铬细胞分泌过量的儿茶酚胺(肾上腺素、去甲肾上腺素和/或多巴胺),而引起相似的临床症状,统称为儿茶酚胺增多症。
嗜铬细胞瘤( pheochromocytoma,PHEO ):起源于肾上腺髓质嗜铬细胞的肿瘤,合成、存储和分解代谢儿茶酚胺,并因后者的释放引起症状。
副神经节瘤(paraganglioma,PGL):起源于肾上腺外的嗜铬细胞的肿瘤,包括源于交感神经(腹部、盆腔、胸部)和副交感神经(头颈部)者。
前者多具有儿茶酚胺激素功能活性,而后者罕见过量儿茶酚胺产生。
2004年,WHO的内分泌肿瘤分类[1]将嗜铬细胞瘤定义为来源于肾上腺髓质的产生儿茶酚胺的嗜铬细胞的肿瘤,即肾上腺内副神经节瘤;而将交感神经和副交感神经节来源者定义为肾上腺外副神经节瘤。
目前比较统一的观点是嗜铬细胞瘤特指肾上腺嗜铬细胞瘤,而将传统概念的肾上腺外或异位嗜铬细胞瘤统称为副神经节瘤。
恶性嗜铬细胞瘤(malignant pheochromocytoma):WHO的诊断标准[1]是在没有嗜铬组织的区域出现嗜铬细胞(转移灶)如骨、淋巴结、肝、肺等。
局部浸润和肿瘤细胞分化程度均不能用于区分嗜铬细胞瘤的良恶性。
二、【临床表现】高血压是最常见的临床症状,发生率约80%~90%[28]。
50%~60%为持续性,40%~50%为发作性,10%~50%可出现体位性低血压,5%血压正常。
可伴有典型的头痛、心悸、多汗“三联征”,其发生率为50%以上[29]。
伴有血糖增高的发生率约40%。
部分患者可能会以心肌病、高钙血症、血尿、糖尿病、库欣综合征、肠梗阻、甚至视力下降等原因就诊[30];家族性PHEO/PGL可以相关综合征的临床症状和体征为主要表现:如MEN-2(甲状腺髓样癌、甲状旁腺功能亢进症、多发粘膜神经瘤)、VHL病(视网膜和中枢神经系统血管母细胞瘤、肾囊肿或肾细胞癌、胰腺囊肿或肿瘤、附睾囊腺瘤)、NF-1(皮肤多发神经纤维瘤、色斑、虹膜“利舍结节”)、家族性PHEO-PGL综合征(头颈部副交感神经副神经节瘤、嗜铬细胞瘤、交感神经副神经节瘤)等[2, 5, 31, 32]。
美国临床内分泌医师协会《甲状腺结节诊断和治疗临床实践医学指南》解读
2、诊断标准
根据指南,甲状腺结节的诊断主要依赖于影像学检查和细针抽吸活检 (FNA)。对于大于1cm的结节,FNA的诊断准确率可达到80%-90%,对于小于1cm 的结节,其诊断准确率略低。对于可疑恶性的结节,应考虑进行分子标记物检测, 如BRAF突变检测等,以提高诊断准确率。
三、治疗建议
1、观察与随访
谢谢观看
对于直径小于1cm、超声检查提示良性征象的结节,指南建议观察并定期随 访。观察期间,患者需定期进行颈部超声检查和血清甲状腺激素水平检测,以监 测结节的变化。
2、手术干预
对于可疑恶性、直径大于1cm的结节,指南建议进行手术干预。术式可选择 甲状腺腺叶切除术或全甲状腺切除术,具体术式应根据患者情况和医生经验进行 选择。同时,指南强调,手术时应遵循无瘤原则,尽量避免损伤甲状旁腺和喉返 神经。
1、指南建议并非绝对,需根据患者具体情况进行调整。在临床实践中,医 生应根据患者的病史、体查、辅助检查结果等因素,综合分析并制定个体化的诊 断和治疗方案。
2、对于甲状腺结节的诊断,应重视多学科联合诊疗的作用。在评估和诊断 过程中,内分泌科医生应与超声科、病理科医生紧密合作,以提高诊断准确率。
3、在治疗过程中,应患者的生育需求和心理健康。对于有生育需求的患者, 应在治疗前告知可能存在的风险和注意事项,并根据患者情况选择合适的术式和 治疗方法。同时,要患者的心理健康,加强心理疏导和关爱。
2024年美国临床内分泌医师协会 《甲状腺结节诊断和治疗临床实践
医学指南》解读
01 一、指南概述
目录
02 二、诊断建议
03 三、治疗建议
04 四、注意事项
05 参考内容
美国临床内分泌医师协会《甲状腺结节诊断和治疗临床实践医学指南》解读: 应该知道的都在这里
美国临床内分泌学医师学会发布2型糖尿病治疗新指南

w i t h s e l e r o s i n g p a n c r e a t i t i s[ J ] .N E n g l J
Me d ,2 0 0 1 ,3 4 4( 4 ) :7 3 2— 7 3 8 .
5 Wa k ha a y a s h i T, Ka wa u r a K ," S a t o mu r a Y, e t 1 . Cl a i n i c a l a n d i ma g i n g f e a t u r e s o f a u t o i m—
2 0 0 3,9 8( 6 ) :2 6 7 9— 2 6 8 7 .
Ta k a y o s h i N , F u mmi mk e T, Hi r o y a s u 0,
病的可能性 ,再进一步完善相关检查 ,也 6
血清学 ( 必备 1条 ) :( 1 )血 清 I g G 可行 诊断性治疗 ,就能 明确诊断 A l P 。 或I g G 4水平 升高 ;( 2 )其他 自身 抗体 阳 参 考 文 献
mu n e p nc a r e a t i c wi t h f o c a l p nc a r e a t i c a we l l i n g o r ma s s f o r ma t i o n: c o mp a is r o n w i t h S O —
[ J ] .I n t e na r l Me d i c i n e ,2 0 0 6 ,4 5( 8) :
4 9 7 .
组 织学 :发 现胰 腺 淋 巴细 胞 、浆 细 胞 浸 润 以及 纤 维 化 ,有 大 量 I g G 4 阳性 细 胞
浸润 。
e t 1.A a u t o i m mu n e p a n e r e a t i t i s[ J ] .N E n — g l J M e d ,2 0 0 6,3 5 5( 1 ) :2 6 7 0—2 6 7 6 .
肾上腺素能肿瘤的131I-MIBG治疗
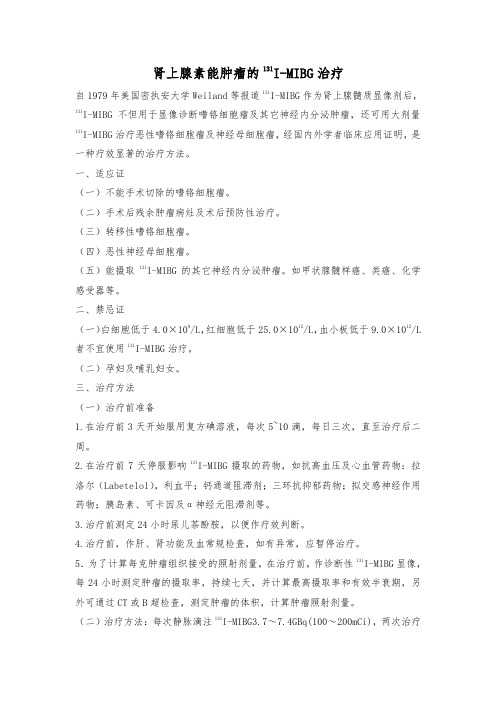
肾上腺素能肿瘤的131I-MIBG治疗自1979年美国密执安大学Weiland等报道131I-MIBG作为肾上腺髓质显像剂后,131I-MIBG不但用于显像诊断嗜铬细胞瘤及其它神经内分泌肿瘤,还可用大剂量131I-MIBG治疗恶性嗜铬细胞瘤及神经母细胞瘤,经国内外学者临床应用证明,是一种疗效显著的治疗方法。
一、适应证(一)不能手术切除的嗜铬细胞瘤。
(二)手术后残余肿瘤病灶及术后预防性治疗。
(三)转移性嗜铬细胞瘤。
(四)恶性神经母细胞瘤。
(五)能摄取131I-MIBG的其它神经内分泌肿瘤。
如甲状腺髓样癌、类癌、化学感受器等。
二、禁忌证(一)白细胞低于4.0×109/L,红细胞低于25.0×1012/L,血小板低于9.0×1012/L 者不宜使用131I-MIBG治疗。
(二)孕妇及哺乳妇女。
三、治疗方法(一)治疗前准备1.在治疗前3天开始服用复方碘溶液,每次5~10滴,每日三次,直至治疗后二周。
2.在治疗前7天停服影响131I-MIBG摄取的药物,如抗高血压及心血管药物:拉洛尔(Labetelol),利血平;钙通道阻滞剂;三环抗抑郁药物;拟交感神经作用药物;胰岛素、可卡因及α神经元阻滞剂等。
3.治疗前测定24小时尿儿茶酚胺,以便作疗效判断。
4.治疗前,作肝、肾功能及血常规检查,如有异常,应暂停治疗。
5.为了计算每克肿瘤组织接受的照射剂量,在治疗前,作诊断性131I-MIBG显像,每24小时测定肿瘤的摄取率,持续七天,并计算最高摄取率和有效半衰期,另外可通过CT或B超检查,测定肿瘤的体积,计算肿瘤照射剂量。
(二)治疗方法:每次静脉滴注131I-MIBG3.7~7.4GBq(100~200mCi),两次治疗间隔时间一般为4~12月,根据病情和病人身体状况可缩短治疗间隔时间。
具体操作:131I-MIBG溶液注入250ml生理盐水中,缓慢静脉滴注,约需90~120分钟,滴注过程中检测脉率、血压,必要时进行EKG监护。
recist 初始肿瘤标准

recist 初始肿瘤标准全文共四篇示例,供读者参考第一篇示例:RECIST(Response Evaluation Criteria in Solid Tumors)是一种被广泛应用于肿瘤治疗临床试验中的评估标准,用于评估肿瘤治疗效果及观察肿瘤的生长和缩小情况。
RECIST于2000年由美国癌症研究院(NCI)提出,其初衷是为了解决肿瘤治疗疗效评估的一致性问题,为临床试验提供一个统一的标准。
RECIST标准主要是针对固体肿瘤的大小进行评估,通过包括体积测量和直径测量等多种指标,来判断肿瘤的生长和缩小程度。
在临床试验中,医生可以通过对患者进行定期检查来评估治疗效果,根据RECIST标准的要求进行肿瘤大小的测量和记录,最终确定病人的肿瘤反应类型。
RECIST标准已经成为了临床试验中最常用的肿瘤评估标准之一,被广泛应用于临床试验中。
RECIST标准主要有四个版本,分别是RECIST 1.0、2.0、1.1和1.1R1。
其中RECIST 1.0是RECIST标准的最初版本,主要根据肿瘤的直径来评估肿瘤的生长和缩小情况,其缺点是没有考虑到肿瘤形状的变化和异质性,导致对肿瘤反应的评估不够准确。
RECIST 2.0在RECIST 1.0的基础上做了一些改进,主要是引入了新的肿瘤形状测量指标,提高了对肿瘤反应的评估准确性。
RECIST 1.1在RECIST 2.0的基础上进一步改进了肿瘤测量的方法和评估标准,使其更加符合临床实际情况,提高了其可操作性和实用性。
RECIST 1.1R1是RECIST 1.1的更新版本,主要是对RECIST 1.1进行了一些细微的调整和修正,以进一步提高对肿瘤反应的评估准确性和可靠性。
RECIST标准的评估主要包括完全缩小(CR)、部分缩小(PR)、稳定(SD)和进展(PD)四种类型。
完全缩小表示肿瘤完全消失,部分缩小表示肿瘤体积缩小了至少30%,稳定表示肿瘤体积变化在正负20%之间,进展表示肿瘤体积增加了至少20%。
CT偶发肾脏肿块的管理——美国放射学院(ACR)偶发病变委员会白皮书
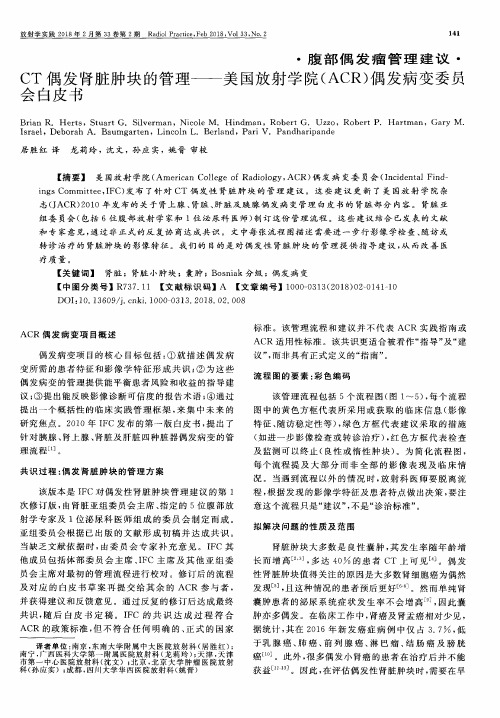
标 准 。该 管理流 程 和建 议 并 不代 表 ACR实 践 指南 或 ACR适 用性 标准 。该 共识更 适合 被看作 “指导 ”及 “建 议 ”,而非具 有正 式定 义 的“指南 ”。
流 程 图 的 要 素 :彩 色 编 码
该 管理 流程 包括 5个 流程 图 (图 1~5),每 个 流程 图 中的黄色 方框 代表 所 采 用或 获 取 的 临床 信 息 (影 像 特 征 、随访稳 定性 等 ),绿 色 方 框 代表 建 议 采 取 的措 施 (如 进 一步影 像 检查 或 转诊 治 疗 ),红色 方 框 代 表检 查 及 监测 可 以终止 (良性 或 惰 性 肿块 )。为 简 化流 程 图 , 每个 流 程提 及 大部 分 而 非 全 部 的 影 像 表 现 及 临 床 情 况 。当遇到 流程 以外 的情 况 时 ,放射 科 医师 要脱 离 流 程 ,根 据发现 的影 像学 特征及 患者 特点 做 出决策 ,要注 意 这个 流程 只是 “建议 ”,不 是“诊 治标 准”。
拟 解 决 问 题 的 性 质 及 范 围
肾脏 肿块 大 多数 是 良性 囊 肿 ,其 发 生 率 随年 龄 增 长 而增 高 。 ,多 达 40 的 患 者 CT 上 可 见 。偶 发 性 肾脏肿 块值 得关 注 的原 因是大 多数 肾细胞 癌为偶 然 发现 -5],且 这种 情况 的患 者预后 更好 ]。然 而单 纯 肾 囊肿 患者 的泌 尿 系统 症 状 发 生 率不 会 增 高 ],因此 囊 肿亦 多偶 发 。在 临床工作 中 ,肾癌及 肾盂 癌相对 少见 , 据统 计 ,其在 2016年新 发 癌 症 病 例 中仅 占 3.7 ,低 于乳 腺 癌 、肺 癌 、前 列 腺 癌 、淋 巴瘤 、结 肠 癌 及 膀 胱 癌 。此外 ,很 多偶 发小 肾癌 的患者 在 治 疗后 并 不能 获益 L1 。因此 ,在 评估 偶发性 肾脏 肿块 时 ,需要 在早
肾上腺肿瘤的诊断和治疗
肾上腺肿瘤的诊断和治疗
龚任余;王毅;钱坤
【期刊名称】《美国中华临床医学杂志》
【年(卷),期】2004(006)002
【摘要】目的提高肾上腺肿瘤的诊断和外科治疗水平。
方法回顾性分析72例肾上腺肿瘤的诊疗资料,其中库欣综合征32例,原醛症24例,嗜铬细胞瘤11例,偶发瘤5例。
结果72例中有功能性肿瘤67例(93.1%),其中恶性5例(7.4%);无功能性肿瘤5例(6.9%),其中恶性1例。
恶性肿瘤中皮质癌1例,恶性嗜铬
细胞瘤4例,非霍奇金淋巴瘤1例。
本组手术切除肿瘤68例,无手术死亡病例。
结论肾上腺肿瘤中库欣综合征和原醛症女多于男。
肾上腺肿瘤主要依据,临床表现,内分泌检查,CT等定位影像检查确诊。
术前充分准备是保证手术成功的重要
因素。
手术是治疗肾上腺肿瘤的有效方法。
【总页数】3页(P96-97,113)
【作者】龚任余;王毅;钱坤
【作者单位】南华大学附属第二医院,湖南衡阳421001
【正文语种】中文
【中图分类】R736.6
【相关文献】
1.肾上腺肿瘤的影像诊断及治疗进展 [J], 胡春兰
2.肾上腺肿瘤22例诊断与治疗分析 [J], 郭海峰;齐文旭
3.肾上腺肿瘤的诊断和外科治疗 [J], 胡中民;陈合群;陈湘
4.肾上腺肿瘤的临床诊断和外科治疗进展 [J], 刘宇军;郭剑明
5.无功能性肾上腺肿瘤的诊断与治疗(附39例报告) [J], 易路;杨罗艳;刘任;赵晓昆;杨金瑞;张选志;刘紫庭
因版权原因,仅展示原文概要,查看原文内容请购买。
CT偶发肾上腺肿块的管理--美国放射学院(ACR)偶发病变委员会白皮书

CT偶发肾上腺肿块的管理--美国放射学院(ACR)偶发病变委员会白皮书William W. Mayo-Smith;Julie H. Song;Giles L. Boland;Isaac R. Francis;Gary M. Israel;Peter J. Mazzaglia;Lincoln L. Berland;Pari V. Pandharipande;张惠茅【期刊名称】《放射学实践》【年(卷),期】2018(33)2【摘要】美国放射学院(American College of Radiology,ACR)偶发病变委员会(Incidental Findings Committee,IFC)针对CT和MRI上偶然发现的肾上腺肿块,提出了新的管理建议.该建议是对美国放射学院杂志(JACR) 2010版肾上腺、肾脏、肝脏及胰腺偶发病变管理白皮书中肾上腺部分的更新.由腹部放射科医师和1位内分泌外科医生组成的肾上腺亚组委员会制定了该方案.该方案结合已发表的文献和专家意见,经过反复推敲最终达成共识.该方案依据患者的特征和图像的特点对偶然发现的肾上腺肿块进行分类.对于每种特定的组合,总结良性或惰性的特征(足以终止随访),并提出后续管理建议.该方案涵盖了很多、但并非适用于所有的病理及临床情况,旨在通过提供肾上腺偶发肿块的管理意见以提升医疗质量.【总页数】7页(P134-140)【作者】William W. Mayo-Smith;Julie H. Song;Giles L. Boland;Isaac R. Francis;Gary M. Israel;Peter J. Mazzaglia;Lincoln L. Berland;Pari V. Pandharipande;张惠茅【作者单位】;;;;;;;;长春,吉林大学第一医院放射科【正文语种】中文【中图分类】R736.6【相关文献】1.美国放射学会甲状腺结节影像报告系统和影像偶发甲状腺结节管理系列白皮书解读 [J], 刘如玉;张波2.CT偶发肾脏肿块的管理--美国放射学院(ACR)偶发病变委员会白皮书 [J], Brian R. Herts;居胜红;Stuart G. Silverman;Nicole M. Hindman;Robert G.Uzzo;Robert P. Hartman;Gary M.Israel;Deborah A. Baumgarten;Lincoln L. Berland;Pari V. Pandharipande3.美国放射学院(ACR)偶发病变委员会白皮书简介 [J], 居胜红;宋彬;张惠茅;赵心明;严福华4.CT肝脏偶发病灶管理--美国放射学院(ACR)偶发病变委员会白皮书 [J], Richard M. Gore;宋彬;Perry J. Pickhardt;Koenraad J. Mortele;Elliot K. Fishman;Jeanne M. Horowitz;Claus J. Fimmel;Mark S. Talamonti;Lincoln L. Berland;Pari V. Pandharipande5.胰腺偶发囊肿的管理--美国放射学院(ACR)偶发病变委员会白皮书 [J], Alec J. Megibow;赵心明;Mark E. Baker;Desiree E. Morgan;Ihab R. Kamel;Dushyant V. Sahani;Elliot Newman;William R. Brugge;Lincoln L. Berland;Pari V. Pandharipande因版权原因,仅展示原文概要,查看原文内容请购买。
肾上腺偶发瘤57例临床分析
肾上腺偶发瘤57例临床分析
杨长海;强万明;刘桂彬;李黎明;韩树楠
【期刊名称】《天津医药》
【年(卷),期】2001(029)010
【摘要】@@ 肾上腺偶发瘤是指无明显临床症状,由于其他原因进行腹部影像学检查或手术时偶然发现的肾上腺肿瘤.近年来,随着医学影像技术的不断发展,肾上腺偶发瘤的发现率逐渐增加.我院自1982~2000年4月收治肾上腺偶发瘤57例,报告如下.rn1临床资料rn1.1一般资料本组57例,男26例,女31例.年龄7~69岁,平均44.6岁.左侧17例,右侧35例,双侧5例.肿瘤直径1~20 cm,平均6.53 cm.57例中33例因高血压、腹痛或腰痛行B超或CT检查时发现,19例为健康查体时发现,5例术中发现.51例患者术前行血尿皮质醇、醛固酮、尿3-甲氧基-4-羟基扁桃酸(VMA)和血电解质等内分泌检查,结果正常.
【总页数】2页(P618-169)
【作者】杨长海;强万明;刘桂彬;李黎明;韩树楠
【作者单位】天津医科大学总医院泌尿外科,;天津医科大学总医院泌尿外科,;天津医科大学总医院泌尿外科,;天津医科大学总医院泌尿外科,;天津医科大学总医院泌尿外科,
【正文语种】中文
【中图分类】R73
【相关文献】
1.肾上腺偶发瘤19例临床分析 [J], 李励献;谢锦来;罗立君;谢建兵;林国伟;吴志清
2.667例肾上腺偶发瘤的临床分析 [J], 谭磊;秦自科;郑付甫;叶云林
3.无症状肾上腺偶发瘤46例临床分析 [J], 潘周辉;谭付清
4.肾上腺偶发瘤42例临床分析 [J], 王海鹏;于福芳
5.肾上腺偶发瘤46例临床分析 [J], 徐刚;张关富;吴刚峰;阎家骏
因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
ENDOCRINE PRACTICE Vol 15 (Suppl 1) July/August 2009 1AACE/AAES Guidelines© 2009 AACE.AmERICAN ASSOCIATION Of ClINICAl ENDOCRINOlOgISTSAND AmERICAN ASSOCIATION Of ENDOCRINE SuRgEONSmEDICAl guIDElINES fOR ThE mANAgEmENTOf ADRENAl INCIDENTAlOmASMartha A. Zeiger, MD, FACS, FACE; Geoffrey B. Thompson, MD, FACS, FACE;Quan-Yang Duh, MD, FACS; Amir H. Hamrahian, MD, FACE;Peter Angelos, MD, PhD, FACS, FACE; Dina Elaraj, MD;Elliot Fishman, MD; Julia Kharlip, MDThe American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons Medical Guidelines for the Management of Adrenal Incidentalomas are systematically developed statements to assist health care providers in medical decision making for specific clinical conditions. Most of the content herein is based on literature reviews. In areas of uncertainty, professional judgment was applied. These guidelines are a working document that reflects the state of the field at the time of publication. Because rapid changes in this area are expected, periodic revisions are inevitable. We encourage medical professionals to use this information in conjunction with their best clinical judgment. The presented recommendations may not be appropriate in all situations. Any decision by practitioners to apply these guidelines must be made in light of local resources and indi -vidual circumstances.2 AACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)WRITING COMMITTEECochairpersonsMartha A. Zeiger, MD, F ACS, F ACEGeoffrey B. Thompson, MD, F ACS, F ACEQuan-Yang Duh, MD, F ACSAmir H. Hamrahian, MD, F ACEPrimary WritersMartha A. Zeiger, MD, F ACS, F ACEGeoffrey B. Thompson, MD, F ACS, F ACEQuan-Yang Duh, MD, F ACSPeter Angelos, MD, PhD, F ACS, F ACEDina Elaraj, MDElliot Fishman, MDAmir H. Hamrahian, MD, F ACEJulia Kharlip, MDREVIEWERSAmerican Association of Clinical Endocrinologists ReviewersJeffrey R. Garber, MD, F ACP, F ACEJeffrey I. Mechanick, MD, F ACP, F ACE, F ACNAmerican Association of Endocrine Surgeons ReviewersMichael J. Demeure, MD, MBA, F ACS, F ACEWilliam B. Inabnet, MD, F ACSAACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)Abbreviations:AACE = American Association of Clinical Endocrinologists; AAES = American Association of Endocrine Surgeons; ACC = adrenocortical carci-noma; ACE = angiotensin-converting enzyme; ACTH = adrenocorticotropic hormone; APA = aldosterone-producing adenoma; ARBs = angiotensin II recep-tor blockers; ARR = aldosterone-to-renin ratio; A VS = adrenal venous sampling; BEL = “best evidence” rating level; CT = computed tomographic; EL = evi-dence level;FDG= fludeoxyglucose; FNA= fine-needle aspiration; HPA = hypothalamic-pituitary-adre-nal; HU = Hounsfield units; IHA = bilateral idiopathic hyperaldosteronism; MRI = magnetic resonance imag-ing; PAC = plasma aldosterone concentration; PAH = primary adrenal hyperplasia; PET = positron emission tomography; PRA = plasma renin activity; R = rec-ommendation; SCS = subclinical Cushing syndrome; UFC = urine free cortisol1. INTRODUCTIONThe incidence of adrenal incidentaloma, a term coined in reference to the phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic imaging, has been increasing and now approaches the 8.7% incidence reported in autopsy series (1 [evidence level or EL 3], 2 [EL 3]). The definition of incidentaloma excludes patients undergo-ing imaging procedures as part of staging and work-up for cancer. Not only are more incidentalomas being detected by imaging but they are increasingly more likely to be functional because of the more common evaluations for subclinical syndromes (3 [EL 2]). During the evaluation of an adrenal mass, 3 questions need to be addressed: (1) Is the tumor hormonally active? (2) Does it have radio-logic characteristics suggestive of a malignant lesion? and (3) Does the patient have a history of a previous malig-nant lesion? The patient should be tested for evidence of hypercortisolism, aldosteronism (if hypertensive), and the presence of a pheochromocytoma. A summary of the lit-erature revealed that approximately 80% of patients with incidentalomas had a nonfunctioning adenoma, 5% had subclinical Cushing syndrome (SCS), 5% had a pheochro-mocytoma, 1% had an aldosteronoma, <5% had an adre-nocortical carcinoma (ACC), and 2.5% had a metastatic lesion; the remaining incidentalomas were ganglioneuro-mas, myelolipomas, or benign cysts (4 [EL 4], 5 [EL 4]). Before consideration of surgical resection, a high degree of certainty of the diagnosis is critical and can be achieved with a combination of biochemical and radio-graphic studies. Patients who present with an adrenal incidentaloma should be referred to an endocrinologist or endocrine surgeon for assessment. Pheochromocytomas necessitate careful preoperative preparation to avoid intra-operative and postoperative morbidity and mortality. In patients with primary aldosteronism, a thorough evalua-tion should be performed to ensure that they do not have adrenocortical hyperplasia and a nonfunctioning adrenal adenoma. Patients with adrenal Cushing syndrome develop adrenal insufficiency after resection and will require steroid coverage and careful withdrawal. Whether those with SCS require surgical treatment is controversial. Those patients with ACC require preoperative planning in collaboration with an endocrinologist or oncologist because the effec-tiveness of the initial resection can be a major predictor of survival. Finally, nonfunctioning adrenal tumors ≥4 cm (Fig. 1) should be considered for surgical resection. In con-trast, small myelolipomas, benign cysts, or nonfunctioning adenomas can be diagnosed with considerable certainty and usually do not necessitate surgical resection unless symptomatic. Depending on the clinical circumstances, resection may be indicated.The only previously published clinical practice guide-lines on the management of patients with adrenal inciden-talomas originated from a National Institutes of Health consensus conference and was published in 2002 (6 [EL 4]). This current set of clinical practice guidelines sum-marizes the relevant literature as it pertains to the differ-ential diagnosis, laboratory and radiologic evaluation, and clinical management and includes recommendations (each labeled “R” in the subsequent section) based on the “best evidence” rating level (BEL) of the published sources. 2. ExECUTIVE SUMMARy OF RECOMMENDATIONS• R1. Patients with an adrenal incidentaloma should undergo evaluation clinically, biochemically, and radio-graphically for signs and symptoms of hypercortisolism, aldosteronism (if hypertensive), the presence of a pheo-chromocytoma, or a malignant tumor (Grade C; BEL 3).• R2. Patients with adrenal incidentalomas who do not ful-fill the criteria for surgical resection need to have radio-graphic reevaluation at 3 to 6 months and then annually for 1 to 2 years. For all adrenal tumors, hormonal evalu-ation should be performed at the time of diagnosis and then annually for 5 years (Grade C; BEL 3).• R3. All patients found to have an incidental adrenal mass should be screened for cortisol excess. Although the best strategy for patients with incidentalomas has not been established, the simplest screening test for autono-mous cortisol secretion from an incidentaloma is a 1-mg overnight dexamethasone suppression test. If clinical suspicion is high, such as in patients with hypertension, obesity, diabetes mellitus, or osteoporosis, 3 tests (sali-AACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)vary cortisol, dexamethasone suppression, and urine free cortisol [UFC]) can be used (Grade C; BEL 3).• R4. After adrenalectomy for a cortisol-producing ade-noma, patients should be treated with exogenous gluco -corticoids until the hypothalamic-pituitary-adrenal (HPA) axis has recovered. This process may take 6 to 18 months after unilateral adrenalectomy (Grade C; BEL 3).• R5. A diagnosis of SCS is made if the serum cortisol level is more than 5.0 m g/dL after a 1-mg dexamethasone sup -pression test, in a patient with an adrenal adenoma and absence of typical physical stigmas of hypercortisolism. A low or suppressed level of adrenocorticotropic hor-mone (ACTH) or a low dehydroepiandrosterone sulfate concentration supports the diagnosis (Grade D; BEL 4). A second abnormal test result of HPA axis function, such as a 2-day low-dose dexamethasone suppression test, may also be needed to establish the diagnosis of SCS (Grade B; BEL 2).• R6. In patients with SCS, until further evidence is avail-able regarding the long-term benefits of adrenalectomy, surgical resection should be reserved for those withworsening of hypertension, abnormal glucose tolerance, dyslipidemia, or osteoporosis (Grade D; BEL 4).• R7. Perioperative glucocorticoid therapy and postop-erative assessment of HPA axis recovery are indicated in patients with SCS (Grade C; BEL 3).• R8. Patients thought to have a pheochromocytoma should undergo measurement of plasma fractionated metanephrines and normetanephrines or 24-hour total urinary metanephrines and fractionated catecholamines (or both plasma and urine studies) (Grade A; BEL 1).• R9. About one-quarter of patients with a pheochromo-cytoma will have associated familial syndromes caused by mutations in the RET gene (multiple endocrine neo-plasia type 2), VHL gene (von Hippel-Lindau disease), or succinate dehydrogenase genes; genetic study and counseling should be performed, especially for young patients or patients with an extra-adrenal pheochromo -cytoma (Grade C; BEL 3).• R10. Surgical resection should be performed for all pheochromocytomas (Grade C; BEL 3).Fig. 1. Algorithm for the evaluation and management of an adrenal incidentaloma. * = Reimage in 3 to 6 months and annually for 1 to 2 years; repeat functional studies annu-ally for 5 years. If mass grows more than 1 cm or becomes hormonally active, then adrenalectomy is recommended. CT = computed tomographic; HU = Hounsfield units; P AC = plasma aldosterone concentration; PRA = plasma renin activity.AACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1) 5• R11. In all patients with a pheochromocytoma, an α-adrenergic blocking agent should be administered pre-operatively, in an effort to prevent intraoperative hemo-dynamic instability (Grade C; BEL 3).• R12. In patients who have undergone resection of a pheochromocytoma, long-term follow-up is necessary because 10% to 15% may have recurrence (Grade B; BEL 2).• R13. Screening for aldosteronism should be performed in patients with an aldosterone-to-renin ratio (ARR) of >20 (Grade C; BEL 3).• R14. Primary aldosteronism is confirmed in the setting of an adrenal incidentaloma by demonstrating lack of aldosterone suppression (24-hour urine study) with salt loading (Grade C; BEL 3).• R15. Subtype evaluation should be achieved with high-resolution computed tomographic (CT) scanning in all patients and adrenal venous sampling (A VS) in the majority of patients older than 40 years (Grade C; BEL 3).• R16. In patients with primary aldosteronism and a uni-lateral source of aldosterone excess, laparoscopic total adrenalectomy is the treatment of choice because it yields excellent outcomes with low associated morbid-ity relative to open approaches (Grade C; BEL 3).• R17. Patients with bilateral idiopathic hyperaldosteron-ism (IHA) or those not amenable or agreeable to sur-gical intervention should be managed with selective and nonselective mineralocorticoid receptor blockers (Grade A; BEL 1).• R18. Any adrenal mass with concerning radiographic characteristics and most lesions ≥4 cm should be resected because of increased risk of adrenal cancer (Grade C; BEL 3).• R19. The presence of pheochromocytoma should be ruled out biochemically before an attempted resection of any adrenal mass (Grade C; BEL 3).• R20. All patients suspected of having an ACC should undergo biochemical evaluation to identify any poten-tial hormone excess that serves as a tumor marker and to determine whether the patient requires steroid replace-ment perioperatively in cases of hypercortisolism (Grade D; BEL 4).• R21. Open adrenalectomy should be performed if ACC is suspected (Grade C; BEL 3).• R22. A metastatic lesion should be suspected in a patient with a history of cancer and an adrenal mass that does not fulfill the criteria for an incidentaloma (Grade C; BEL 3).• R23.In very rare instances, pathologic confirmation with CT-guided needle biopsy may be required for stag-ing and planning of oncologic treatments (Grade D; BEL 4).• R24. The presence of pheochromocytoma should be ruled out with biochemical testing before performance of a biopsy (Grade C; BEL 3).• R25. Patients with bilateral adrenal metastatic lesions should undergo evaluation for adrenal insufficiency (Grade D; BEL 4).• R26. Adrenal metastasectomy is rarely indicated but should be considered in the case of an isolated adrenal metastatic lesion (Grade C; BEL 3).3. METHODS FOR DEVELOPMENT OF THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN ASSOCIATION OF ENDOCRINE SURGEONS MEDICAL GUIDELINES FOR THE MANAGEMENT OF ADRENAL INCIDENTALOMASIn 2004, the American Association of Clinical Endocrinologists (AACE) Protocol for Standardized Production of Clinical Practice Guidelines was published in Endocrine Practice (7 [EL 4]). Those recommenda-tions were used for the preparation of this document. The American Association of Endocrine Surgeons (AAES) and AACE cochairpersons and primary writers are experts in the clinical management of adrenal diseases. After the completion of the first draft created by the primary writers, the chairpersons reviewed the technical assignment of evi-dence levels (inserted in the reference list and in the text) and recommendation grades (in the Executive Summary). The document was subsequently reviewed by the AAES and AACE publication and executive committees and then finally completed by the chairpersons.4. ADRENAL INCIDENTALOMA4.1. History and Physical ExaminationPatients who have an adrenal incidentaloma identi-fied on CT or magnetic resonance imaging (MRI) need to undergo a thorough clinical evaluation. The history should be aimed at excluding a functional tumor. For patients with hypercortisolism or Cushing syndrome, the investigation should include inquiries about substantial weight gainAACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)or development of centripetal obesity, easy bruisability, severe hypertension, diabetes, virilization, proximal mus-cle weakness, or fatigue. For patients with pheochromocy-toma, inquiries should address the development of sudden or severe headaches, weight loss, anxiety attacks, sweat-ing, cardiac arrhythmias, or palpitations. For patients with aldosteronism, the clinician should ask about the presence of hypertension, fluid retention, or a history of hypokale-mia. The clinician should inquire about a history of cancer, recent weight loss, and a smoking history because an adre-nal mass may be a metastatic lesion. Physical examination should include measurement of the patient’s blood pres-sure and pulse as well as assessment for evidence of central obesity, ecchymoses, striae, muscle wasting, hirsutism, or other signs of virilization. A review of photographs taken over several years, such as those on a driver’s license, may make changes in appearance obvious.4.2. Biochemical EvaluationThe detection of an adrenal lesion should prompt biochemical evaluation unless it is an obvious myeloli-poma. Adrenal myelolipomas are of low CT attenuation and also contain fat (-10 to -20 Hounsfield units [HU]); therefore, the diagnosis is generally clear (8 [EL 2]). Any hormonally hyperfunctioning adenoma needs to be surgi-cally resected. Patients are screened for SCS with a 1-mg overnight dexamethasone suppression test. A diagnosis of SCS is suspected if the serum cortisol level exceeds 5.0 m g/dL after a 1-mg dexamethasone suppression test. A low or suppressed level of ACTH or a low dehydroepiandros-terone sulfate concentration further supports the diagnosis.A second abnormal test result of HPA axis function, such as a 2-day low-dose dexamethasone suppression test, may be needed to establish the diagnosis of SCS(9 [EL 2]). Patients with hypertension who have a ratio of plasma aldosterone concentration (PAC) (ng/dL) to plasma renin activity (PRA) (ng/mL per hour) of >20 while not taking spironolactone and mineralocorticoid receptor blockers should undergo further assessment for the presence of pri-mary aldosteronism (4 [EL 4], 10 [EL 4]). Finally, elevated plasma free metanephrine and normetanephrine levels and 24-hour total urinary metanephrines and fractionated cat-echolamines suggest the presence of a pheochromocytoma (11 [EL 4], 12 [EL 3]). In general, testing the patient for the production of excess sex hormones is not indicated unless the patient has obvious clinical stigmas.4.3. Radiologic ImagingThe primary goal of imaging is to distinguish among adrenal adenoma, adrenal carcinoma, pheochromocytoma, and metastatic lesions. It is important to emphasize that imaging cannot reliably distinguish between functioning and nonfunctioning adrenal adenomas. The diagnosis of an adenoma relies on the presence of intracellular lipid in the adrenal lesion, which can be identified by density mea-surement on noncontrast CT or in-phase and out-of-phase MRI. Alternatively, an adenoma can be identified by mea-suring contrast-washout kinetics on CT. Lesions that have an attenuation value below 10 HU on noncontrast CT scan are adenomas (8 [EL 2], 13 [EL 3], 14 [EL 3]). Adenomas constitute about 70% of adrenal masses seen in the clinical setting.The differential diagnosis can be further delineated by CT scans done immediately after intravenous administra-tion of a contrast agent and then again after a 10- to 15-min-ute delay. Benign adrenal lesions will commonly enhance up to 80 to 90 HU and wash out more than 50% on the delayed scan, whereas lesions such as metastatic tumors, carcinomas, or pheochromocytomas will not (8 [EL 2]). Pheochromocytomas usually show enhancement to more than 100 HU, diagnostically separating them from adeno-mas. On noncontrast CT, some benign adrenal lesions do not have attenuation values of less than 10 HU and may have values of 20 to 40 HU. This result is found in lipid-poor adenomas. In these cases, a washout of >50% will often allow the diagnosis of an adenoma to be made. This observation, however, needs to be confirmed with larger studies.4.4. Follow-up of Patients With a Nonfunctioning Adrenal IncidentalomaPatients with adrenal incidentalomas smaller than 4 cm and radiologic characteristics consistent with a benign adenoma need to have radiographic reevaluation at 3 to 6 months and then annually for 1 to 2 years (6 [EL 4], 15 [EL 3], 16 [EL 3]). Hormonal evaluation should be per-formed at the time of diagnosis and then annually for up to 5 years (3 [EL 2]). The risk of the mass enlarging during 1, 2, and 5 years is 6%, 14%, and 29%, respectively, and the risk of the mass becoming hormonally active during those time periods is 17%, 29%, and 47%, respectively (3 [EL 2]). The most common hormonally active lesion in patients with previously inactive adenomas is SCS. The rate of a benign adenoma or hyperplasia developing into an ACC is not well known, but such a change seems to be extremely rare (15 [EL 3], 17 [EL 2], 18-20 [EL 3]). Should the tumor grow more than 1 cm or become hormonally active during follow-up, surgical excision should be considered. Currently, it is unclear what the recommendations should be after 5 years of follow-up for a stable, nonfunctioning adrenal mass.5. CORTISOL-PRODUCING ADRENAL ADENOMA 5.1. OverviewAdrenocortical adenoma can cause both overt Cushing syndrome and SCS. Those patients with an incidental radiographic finding of the adrenal lesion are more likely than others to have SCS. With better understanding of SCS and more frequent testing for it (4 [EL 4], 21-23 [EL 4]),AACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)this disease entity is being identified more frequently. Of the hormonally active incidentalomas, this diagnosis con-stitutes the most common form—5.3% of more than 2,000 cases reported in the world literature (4 [EL 4]). Overt clin-ical signs and symptoms of Cushing disease are not always present; thus, biochemical testing is necessary to secure the diagnosis. Overt adrenal Cushing syndrome is character-ized by all the typical stigmas of hypercortisolism.5.2. History and Physical ExaminationParticular attention should be directed at eliciting a history of fatigue, depression, sleep disturbances, weight gain, menstrual irregularities, hypertension, glucose intol-erance, easy bruising, or fracture with minimal trauma. On physical examination, the physician should measure the patient’s blood pressure and pulse and look for central obe-sity, supraclavicular fat accumulation, a dorsocervical fat pad, facial plethora, thinned skin, purple and wide (>1 cm) striae, acne, ecchymoses, hirsutism, and proximal muscle weakness or wasting. Changes on photographs taken over several years (such as those on driver’s licenses) may be of particular help. All these signs and symptoms should raise the level of suspicion for Cushing syndrome. Many patients with mild Cushing syndrome, however, will have only a few of these signs and symptoms present, and many patients without Cushing syndrome may also exhibit one or more of these findings. Therefore, Cushing syndrome cannot be diagnosed on purely clinical grounds, and a care-ful biochemical evaluation is necessary.5.3. Biochemical Evaluation for Adrenal Cushing SyndromeBiochemical evaluation for adrenal Cushing syndrome is a 2-step process that first includes screening with 1 or 2 screening tests. If the screening test results are positive, confirmatory tests are then performed. Testing is based on demonstrating 3 pathophysiologic derangements typical of Cushing syndrome: (1) loss of a normal diurnal pattern, with abnormally high late-night cortisol secretion (late-night salivary cortisol test); (2) failure to discontinue the production of cortisol, despite the absence of ACTH stimu-lation (dexamethasone suppression test); and (3) excess production of cortisol (24-hour UFC test).5.4. Screening Tests5.4.1. Late-Night Salivary CortisolThe late-night salivary cortisol test is the most recent assay to be used for screening for Cushing syndrome and is now available through most laboratories. Patients with a regular sleep pattern can collect a specimen of saliva at bedtime at home and then bring or mail the samples to the laboratory for testing. Several investigators have shown that elevated nighttime cortisol levels appear to be the earliest and most sensitive markers for Cushing syndrome (24 [EL 4], 25 [EL 4]), with sensitivity and specificity approaching 90% to 95% (26 [EL 3]).5.4.2. Overnight 1-mg Dexamethasone Suppression TestThe overnight 1-mg dexamethasone suppression test is performed by administration of 1 mg of dexamethasone at 11 pm and determination of a fasting plasma cortisol level between 8 am and 9 am the following day. Suppression of the plasma cortisol level to <1.8 m g/dL has the best nega-tive predictive value for Cushing syndrome (5 [EL 4]). A positive test result should be followed by further testing, including 24-hour UFC, midnight salivary cortisol, or a 2-day low-dose dexamethasone suppression test.5.4.3. 24-Hour UFCBecause UFC levels are not affected by factors that influence corticosteroid-binding globulin, UFC is a better reflection of cortisol levels than plasma cortisol levels and is an integrated measure of excess production of cortisol. An elevated UFC level warrants further investigation, and a UFC that is more than 4 times the normal value is con-sidered diagnostic of Cushing syndrome (27 [EL 4]). Up to 3-fold elevation of UFC can be associated with pseudo-Cushing syndrome attributable to chronic anxiety, depres-sion, alcoholism, or obesity or can accompany use of certain medications (24 [EL 4], 28 [EL 3]). Thus, further confirmatory testing is needed in such a case.No currently available screening test has a 100% sensitivity and thus, when used alone, cannot completely exclude the presence of hypercortisolism. Because these tests target different aspects or pathophysiologic features of Cushing syndrome, they are complementary in the screening process. Although the best diagnostic strategy for patients with incidentalomas has not been established, the simplest screening test for autonomous cortisol secre-tion from an incidentaloma is a 1-mg overnight dexameth-asone suppression test. If clinical suspicion is high, such as in patients with hypertension, obesity, diabetes mellitus, or osteoporosis, all 3 tests (salivary cortisol, dexamethasone suppression, and UFC) can be used.A low or suppressed ACTH level would confirm an adrenal origin of Cushing syndrome. The lack of ACTH response during the corticotropin-releasing hormone stim-ulation test may be used in those patients with borderline ACTH levels to distinguish ACTH-dependent from ACTH-independent Cushing syndrome (29 [EL 4]).5.5. Perioperative ManagementIn patients with elevated cortisol levels, care should be exercised during the preoperative period to ensure that dia-betes and hypertension, if present, are treated adequately. Because these patients are at increased relative risk for thromboembolic complications, measures must be imple-mented to prevent these complications during the periop-erative period. In the unusual patient with long-standingAACE/AAES Adrenal Incidentaloma guidelines, Endocr Pract. 2009;15(Suppl 1)and very high levels of cortisol, the presence of severe immunosuppression must be considered, and prophylactic perioperative antibiotics should be used. Peptic ulcer pro-phylaxis should also be provided.Patients with Cushing syndrome also have a suppressed HPA axis. Excess cortisol secretion from an adrenocorti-cal adenoma suppresses the production of ACTH by the pituitary. This situation leads to atrophy of the contralateral adrenal gland that is devoid of the trophic effects of ACTH. Once a cortisol-producing adenoma has been removed, physicians must administer glucocorticoid replacement because the remaining adrenal gland is suppressed (30 [EL 3]). High stress doses can usually be weaned to mainte-nance doses of hydrocortisone of approximately 12 to 15 mg/m2 (31 [EL 4]). After an adrenal surgical procedure for Cushing syndrome, physicians should be prepared to treat patients with exogenous glucocorticoids until the HPA axis has recovered. The amount of time for recovery varies from 6 to 18 months after a unilateral adrenalectomy. Doherty et al (32 [EL 2]) reported a median time of 15 months to recover a normal response to the ACTH stimulation test and 19 months (range, 12 to 24) to allow discontinuation of hydrocortisone. During preoperative informed consent discussions, all patients should also be cautioned about the importance of long-term corticosteroid replacement. 6. SUBCLINICAL CUSHING SyNDROME6.1. OverviewMore than 5% of patients with adrenal incidentalo-mas may have SCS (4 [EL 4]). This poorly defined entity may be unique to patients with adrenal incidentalomas. It is characterized by subtle autonomous production of corti-sol by an adrenal tumor, which is usually associated with suppressed production of cortisol from the contralateral gland but no overt clinical features of Cushing syndrome such as atypical fat redistribution, skin fragility, or proxi-mal muscle weakness. Ultimately, the best proof for the presence of this disorder is the development of adrenal insufficiency postoperatively. It has been postulated that long-term exposure to subtle cortisol excess may lead to the metabolic derangements seen in patients with overt Cushing syndrome. Many, although not all, studies found higher prevalences of hypertension, obesity, insulin resis-tance, dyslipidemia, and osteoporosis in patients with SCS (33-36 [EL 3]). Nevertheless, no conclusive evidence exists for a causal relationship between subtle autonomous production of cortisol and such metabolic derangements. In fact, Reincke (37 [EL 4]) theorized that adrenal nod-ules might represent a manifestation of the metabolic syn-drome and develop because of a trophic effect of excess insulin on the adrenal glands. Little information is avail-able about the natural history of this condition. It has been shown that progression to overt Cushing syndrome is a rare event within 1 to 7 years of follow-up (3 [EL 2], 17 [EL 2]). Otherwise, long-term morbidity and mortality data are lacking. Similarly, there are no long-term outcome data for patients who were treated medically with risk factor modi-fication alone versus those who underwent surgical resec-tion of adrenal adenomas.6.2. DiagnosisThe diagnosis of SCS is made biochemically; however, the variability among diagnostic criteria used in research studies is significant. The 1-mg dexamethasone suppres-sion test is more sensitive than UFC in diagnosing this con-dition (29 [EL 4]). An abnormal result of the dexametha-sone suppression test was the most common biochemical abnormality seen in patients undergoing follow-up by the Study Group on Adrenal Tumors of the Italian Society of Endocrinology (9 [EL 2]) and others who have studied the condition. Consequently, the dexamethasone suppression test is the most frequently used initial screening test, but the appropriate cutoff cortisol level is debated. A cutoff point of 5 m g/dL was associated with a specificity of 100% and a sensitivity of 58% in 1 study, whereas a lower cutoff point of about 1.8 m g/dL had a 75% to 100% sensitivity and a 72% to 82% specificity (38 [EL 3], 39 [EL 3]). Hence, we recommend use of the higher cutoff point (5 m g/dL), which has a higher specificity. In addition, because yearly biochemical reevaluation is recommended for 5 years in patients with nonfunctioning lesions, those patients with false-negative results on the initial evaluation may be iden-tified at later reassessment. A low or suppressed level of ACTH or low dehydroepiandrosterone sulfate concentra-tion supports the diagnosis of SCS. Some investigators have required a second abnormal test result of HPA axis function, such as a 2-day low-dose dexamethasone sup-pression test, to establish the diagnosis of SCS(9 [EL 2]). A consultation with an endocrinologist experienced in interpreting tests of the HPA axis should be sought (29 [EL 4]).6.3. ManagementAt this time, no long-term prospective data are avail-able for guidance in the choice between medical and sur-gical therapy for these patients. Although several studies report improvement in individual cardiovascular risk fac-tors, particularly hypertension, after adrenalectomy, most metabolic derangements persist. Young (40 [EL 4]) has proposed a commonsense strategy to operate on younger patients (<40 years old) with a recent onset or worsening of diabetes, hypertension, or osteoporosis. In older patients with worsening of clinical comorbidities, clinical judg-ment should be used about referral for surgical treatment. In all patients undergoing a surgical procedure for SCS, corticosteroid replacement should be initiated on postop-erative day 1 after a blood sample has been obtained for determination of a morning serum cortisol value, and they should be followed until HPA axis functionality is restored,。