脊柱外科临床指南
强直性脊柱炎临床诊疗指南(简洁国内版)
强直性脊柱炎临床诊疗指南(简洁国内版)强直性脊柱炎(Ankylosing Spondylitis,AS)是⼀种慢性进⾏性疾病,主要侵犯骶髂关节,脊柱⾻突,脊柱旁软组织及外周关节,并可伴发关节外表现。
严重者可发⽣脊柱畸形和关节强直。
AS是脊柱关节病的原型或称原发性AS;其它脊柱关节病并发的骶髂关节炎为继发性AS。
通常所指及本指南所指均为前者。
AS 的患病率以往认为本病男性多见,男⼥之⽐为10.6:1;现报告男⼥之⽐为为2:1到3:1,只不过⼥性发病较缓慢及病情较轻。
发病年龄通常在13-31岁,30岁以后及8岁以前发病者少见。
AS的病因未明。
基因和环境因素共同在发病中发挥作⽤。
HLA-B27(下称B27)与AS的发病密切相关,并有明显家族发病倾向,我国阳性率为2%-7%,AS患者B27的阳性率达91%。
普通⼈群AS的患病率约为0.1%,在AS患者的家系中为4%,在B27阳性的AS患者中,其⼀级亲属中AS患病率⾼达11%-25%。
⼤约80%的B27阳性者并不发⽣AS,以及⼤约10%的AS患者为B27阴性。
AS的发⽣还有如肠道细菌及肠道炎症等其他因素参与。
AS的病理性标志和早期表现之⼀为骶髂关节炎。
脊柱受累到晚期的典型表现为⽵节状脊柱。
本病发病隐袭。
最常见的症状是腰背痛,⾮典型者可以周围关节炎开始。
患者逐渐出现腰背部或骶髂部疼痛和/或发僵,半夜痛醒,翻⾝困难,晨起或久坐后起⽴时腰部发僵明显,但活动后减轻。
有些患者感臀部钝痛或骶髂部剧痛,偶向周边放射。
咳嗽、打喷嚏、突然扭动腰部疼痛可加重。
疾病早期疼痛多在⼀侧呈间断性,数⽉后疼痛多为双侧呈持续性。
随病变由腰椎向胸颈部脊椎发展,则出现相应部位疼痛、活动受限或脊柱畸形。
24%-75%的AS患者在病初或病程中出现外周关节病变,以膝、髋、踝和肩关节居多,肘及⼿和⾜⼩关节偶有受累。
⾮对称性、少数关节或单关节,及下肢⼤关节的关节炎为本病外周关节炎的特征。
我国患者除髋关节外,膝和其他关节的关节炎或关节痛多为暂时性,极少或⼏乎不引起关节破坏和残疾。
诊疗指南 脊椎骨折

诊疗指南脊椎骨折
诊疗指南:脊椎骨折
概述
脊椎骨折是一个常见的骨折类型,常见于骨质疏松、高峰时段
和外伤等因素影响下。
本指南旨在提供脊椎骨折的诊断和治疗指导,以便提高患者的治疗效果和预后。
诊断
1. 病史询问:详细询问患者受伤情况和症状表现,包括疼痛部位、活动受限等。
2. 体格检查:进行脊柱检查,包括感觉和运动功能评估。
3. 影像学检查:常规使用X射线、CT或MRI进行检查,以确
定骨折类型和程度。
分类
脊椎骨折按照骨折位置和类型进行分类,其中常见的骨折类型
包括:
1. 横行骨折:横向断裂脊椎骨的一种骨折。
2. 纵行骨折:纵向断裂脊椎骨的一种骨折。
3. 压缩性骨折:脊椎骨在一个方向上受到压缩而发生的骨折。
治疗
1. 保守治疗:适用于稳定骨折,包括卧床休息、疼痛控制、牵
引等。
2. 手术治疗:适用于不稳定骨折,包括内固定和植骨等手术方法。
预后
1. 随访:对患者进行定期随访,评估治疗效果和功能恢复情况。
2. 康复训练:提供康复训练指导,帮助患者恢复脊柱功能和日
常活动能力。
以上是脊椎骨折的诊疗指南,旨在为医生提供明确的诊断和治
疗策略,以便改善患者的治疗效果和预后。
脊柱外科临床路径
根据《临床诊疗指南-骨科学分册》(年制和7年制教材临床医学专用,人民卫生出版社)
1。病史:单侧或双侧神经根损伤或马尾神经损伤的症状。
2。体征:单侧或双侧神经根损伤或马尾神经损伤的阳性体征。
3.影像学检查:有椎间盘突出或脱出压迫神经根或马尾神经的表现。
(2)术前可能需要肌电图、诱发电位检查;
(3)有相关疾病者必要时请相应科室会诊。
(七)选择用药。
抗菌药物:按照《抗菌药物临床应用指导原则》(卫医发〔2004〕285号)执行。
(八)手术日为入院第4-6天。
1。麻醉方式:局麻+强化或全麻。
2.手术方式:颈前路减压植骨固定、颈后路减压植骨固定、颈前后联合入路减压植骨固定术。
3.有上胸椎同时累及者,可能同期手术。
4。内植物的选择:由于病情不同,使用不同的内植物,可能导致住院费用存在差异。
二、颈椎病(脊髓型)临床路径表单
适用对象:第一诊断为颈椎病(ICD-10:M47。1↑G99。2*)
行颈前路减压植骨固定、颈后路减压植骨固定、颈前后联合入路减压植骨固定术(ICD—9-CM-3:81。02—81.03)
3.手术内植物:前路钛板、Cage或后路螺钉、固定板(棒)、钛缆、钛网、人工椎间盘、各种植骨材料。
4。输血:视术中情况而定。
(九)术后住院恢复5—11天.
1.必须复查的检查项目:颈椎正侧位片.
2.术后处理:
(1)抗菌药物:按照《抗菌药物临床应用指导原则》(卫医发〔2004〕285号)执行;
(2)术后镇痛:参照《骨科常见疼痛的处理专家建议》;
□注意神经功能变化
□注意伤口情况
□上级医师查房,进行手术及伤口评估,确定有无手术并发症和切口愈合不良情况,明确是否出院
脊柱骨折诊疗常规指南骨科及治疗方案

脊柱骨折诊疗常规指南骨科及治疗方案【概述】脊柱骨折十分常见,约占全身骨折的5%〜6%,胸腰段脊柱骨折多见。
脊柱骨折可并发脊髓或马尾神经损伤,特别是颈椎骨折一脱位合并有脊髓损伤者,据报告可达70%,能严重致残甚至丧失生命。
1、解剖概要每块脊柱骨分椎体与附件两部分。
可将整个脊柱分为前、中、后三柱。
前柱包含了椎体的前2/3、纤维环的前半部分和后纵韧带;中柱包含了椎体的后1/3、纤维环的后半部分和后纵韧带;而后柱包含了后关节囊、黄韧带、脊椎的附件、关节突和脊上以及脊间韧带。
中柱和后柱包裹了脊髓和马尾神经,该区的损伤能够累及神经系统,特别是中柱的损伤,碎骨片和髓核组织能够突入椎管的前半部,损伤脊髓,所以对每个脊柱骨折病例都必须了解有无中柱损伤。
胸腰段脊柱(胸10〜腰2)处于两个生理弧度的交汇处,活动度达,是应力集中之处,所以该处骨折十分常见。
2、病因和分类暴力是引起胸腰椎体骨折的主要原因。
暴力的方向能够通过X、Y、Z轴。
脊柱右六中运动:在Y轴上有压缩、牵拉和旋转;在X轴上有屈、伸和侧方移动;在Z轴上则有侧屈和前后方向移动。
有三种力量能够作用于中轴:轴向的压缩、轴向的牵拉和在横面上的移动。
三种病因不会同时存在,例如轴向的压痛和轴向的牵拉就不可能同时存在。
所以胸腰椎骨折和颈椎骨折分别能够有六中类型损伤。
【诊断标准】1、诊断依据(1)外伤史,伤后右局部疼痛,站立即翻身困难。
(2)胸腰段后突畸形。
(3)X线影像学检查有助于明确诊断,明确损伤部位,类型和移位情况。
2.分类诊断(1)胸腰椎骨折的分类1)单纯性楔形压缩性骨折:这是脊柱前柱损伤的结果。
该型骨折部损伤脊柱,脊柱仍可保持其稳定性。
此类骨折通常为高空坠落伤,足、臀部着地,身体猛烈屈曲,产生了椎体前半部压痛。
2)稳定性爆破型骨折:这是脊柱前柱和中柱损伤的结果。
暴力来自Y轴的轴向压缩。
通常亦为高空坠落伤,足臀部着地,脊柱保持正直,胸腰段脊柱的椎体受力最大,因挤压而破碎,因为不存在旋转力量,脊柱的后柱不受影响,因而仍保留了脊柱的稳定性,但破碎的椎体及椎间盘能够突出于椎管前方,损伤脊髓而产生神经症状。
脊柱外科临床路径表单3.19-1

脊柱外科临床路径表单3.19-1
脊柱外科临床路径表单
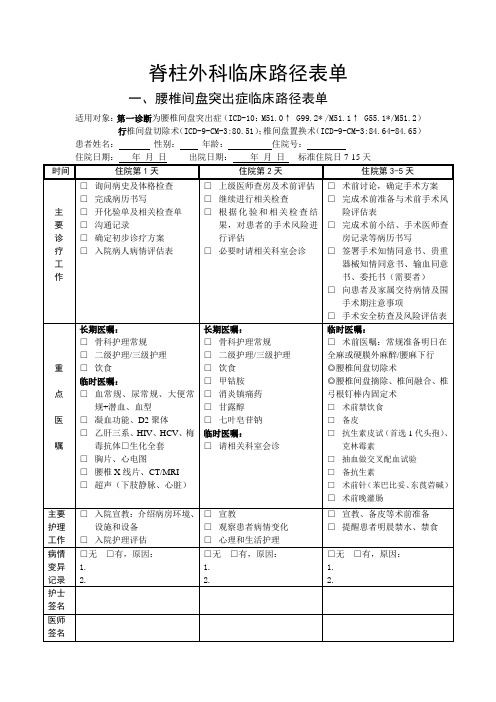
一、腰椎间盘突出症临床路径表单
适用对象:第一诊断为腰椎间盘突出症(ICD-10:M51.0↑ G99.2* /M51.1↑ G55.1*/M51.2)行椎间盘切除术(ICD-9-CM-3:80.51);椎间盘置换术(ICD-9-CM-3:84.64-84.65)患者姓名:性别:年龄:住院号:
二、颈椎病(脊髓型)临床路径表单
适用对象:第一诊断为颈椎病(ICD-10:M47.1↑G99.2*)
行颈前路减压植骨固定、颈后路减压植骨固定、颈前后联合入路减压植骨固定术
(ICD-9-CM-3:81.02-81.03)
患者姓名:性别:年龄:住院号:
住院日期:年月日出院日期:年月日标准住院日7-15天
三、腰椎管狭窄症临床路径表单
适用对象:第一诊断为腰椎管狭窄症
行椎间盘切除椎间融合内固定术
患者姓名:性别:年龄:住院号:
四、骨质疏松症临床路径表单
适用对象:第一诊断为骨质疏松伴有病理性骨折
行经皮椎体成形术或静滴唑来膦酸治疗
患者姓名:性别:年龄:住院号:
住院日期:年月日出院日期:年月日标准住院日10-28天
五、脊柱骨折临床路径表单
适用对象:第一诊断为颈椎、胸腰椎骨折
行颈胸腰椎切开复位内固定术
患者姓名:性别:年龄:住院号:
六、骨折取内固定装置临床路径表单
适用对象:第一诊断为胸腰椎骨折术后
行胸腰椎椎骨取内固定术
患者姓名:性别:年龄:住院号:
七、坐骨神经痛临床路径表单
适用对象:第一诊断为坐骨神经痛、腰椎间盘突出症行保守治疗
患者姓名:性别:年龄:住院号:。
脊柱外科临床路径表单3.19-1
脊柱外科临床路径表单
一、腰椎间盘突出症临床路径表单
适用对象:第一诊断为腰椎间盘突出症(ICD-10:M51.0↑ G99.2* /M51.1↑ G55.1*/M51.2)行椎间盘切除术(ICD-9-CM-3:80.51);椎间盘置换术(ICD-9-CM-3:84.64-84.65)患者姓名:性别:年龄:住院号:
二、颈椎病(脊髓型)临床路径表单
适用对象:第一诊断为颈椎病(ICD-10:M47.1↑G99.2*)
行颈前路减压植骨固定、颈后路减压植骨固定、颈前后联合入路减压植骨固定术
(ICD-9-CM-3:81.02-81.03)
患者姓名:性别:年龄:住院号:
住院日期:年月日出院日期:年月日标准住院日7-15天
三、腰椎管狭窄症临床路径表单
适用对象:第一诊断为腰椎管狭窄症
行椎间盘切除椎间融合内固定术
患者姓名:性别:年龄:住院号:
四、骨质疏松症临床路径表单
适用对象:第一诊断为骨质疏松伴有病理性骨折
行经皮椎体成形术或静滴唑来膦酸治疗
患者姓名:性别:年龄:住院号:
住院日期:年月日出院日期:年月日标准住院日10-28天
五、脊柱骨折临床路径表单
适用对象:第一诊断为颈椎、胸腰椎骨折
行颈胸腰椎切开复位内固定术
患者姓名:性别:年龄:住院号:
六、骨折取内固定装置临床路径表单
适用对象:第一诊断为胸腰椎骨折术后
行胸腰椎椎骨取内固定术
患者姓名:性别:年龄:住院号:
七、坐骨神经痛临床路径表单
适用对象:第一诊断为坐骨神经痛、腰椎间盘突出症
行保守治疗
患者姓名:性别:年龄:住院号:。
NASS循证临床指南:脊柱外科手术中的抗凝治疗(2009版)
North American Spine SocietyEvidence-Based Clinical Guidelines for Multidisciplinary Spine CareAntithrombotic Therapies in Spine SurgeryNASS Evidence-Based Guideline Development CommitteeChristopher M. Bono, MD, Committee Chair William C. Watters III, MD, Committee Chair Michael H. Heggeness, MD, PhD Daniel K. Resnick, MD, William O. Shaffer, MD Jamie Baisden, MD Peleg Ben-Galim, MD John E. Easa, MDRobert Fernand, MD Tim Lamer, MD Paul G. Matz, MDRichard C. Mendel, MD Rajeev K. Patel, MD Charles A. Reitman, MD John F . T oton, MDFinancial StatementThis clinical guideline was developed and funded in its entirety by the North American Spine Society (NASS). All participating authors have submitted a disclosure form relative to potential conflicts of interest which is kept on file at NASS.CommentsComments regarding the guideline may be submitted to the North American Spine Society and will be consid-ered in development of future revisions of the work.North American Spine SocietyEvidence-Based Clinical Guidelines for Multidisciplinary Spine CareAntithrombotic Therapies in Spine SurgeryCopyright © 2009 North American Spine Society7075 Veterans BoulevardBurr Ridge, IL 60527630.230.3600ISBN: 1-929988-26-5This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is toI. IntroductionObjectiveThe objective of the North American Spine So-ciety (NASS) Evidence-Based Clinical Guideline on Antithrombotic Therapies in Spine Surgery is to provide evidence-based recommendations to address key clinical questions surrounding the use of antithrombotic therapies in spine surgery. The guideline is intended to address these questions based on the highest quality clinical literature avail-able on this subject as of February 2008. The goals of the guideline recommendations are to assist in delivering optimum, efficacious treatment with the goal of preventing thromboembolic events.Scope, Purpose and Intended User This document was developed by the North American Spine Society Evidence-based Guideline Development Committee as an educational toolto assist spine surgeons in minimizing the risk of deep venous thrombosis (DVT) and pulmonary embolism (PE). The NASS Clinical Guideline on Antithrombotic Therapies in Spine Surgery dis-cusses the incidence of DVT/PE in the population of patients undergoing spinal surgery. Recom-mendations are made to address the utilization of chemoprophylaxis and mechanical prophylaxis, with discussion of wound complications and risks associated with prophylactic measures.THIS GUIDELINE DOES NOT REPRESENT A “STANDARD OF CARE,” nor is it intended as a fixed treatment protocol. It is anticipated that there will be patients who will require less or more extensive prophylaxis than the average. It is also ac-knowledged that in atypical cases, treatment falling outside this guideline will sometimes be necessary. This guideline should not be seen as prescribing the type, frequency or duration of intervention. Treat-ment should be based on the individual patient’s need and doctor’s professional judgment. This document is designed to function as a guideline and should not be used as the sole reason for denial of treatment and services. This guideline is not in-tended to expand or restrict a health care provider’s scope of practice or to supersede applicable ethical standards or provisions of law.Patient PopulationThe patient population for this guideline encom-passes adults (18 years or older) undergoing spine surgery.This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is toII. Guideline Development MethodologyThrough objective evaluation of the evidence and transparency in the process of making recom-mendations, it is NASS’ goal to develop evidence-based clinical practice guidelines for the diagnosis and treatment of adult patients with various spinal conditions. These guidelines are developed for educational purposes to assist practitioners in their clinical decision-making processes. It is anticipated that where evidence is very strong in support of recommendations, these recommendations will be operationalized into performance measures.Multidisciplinary CollaborationWith the goal of ensuring the best possible carefor adult patients suffering with back pain, NASS is committed to multidisciplinary involvement in the process of guideline and performance measure development. To this end, NASS has ensured that representatives from medical, interventional and surgical spine specialties have participated in the development and review of all NASS guidelines.It is also important that primary care providers and musculoskeletal specialists who care for pa-tients with spinal complaints are represented in the development and review of guidelines that address treatment by first contact physicians, and NASS has involved these providers in the development process as well. To ensure broad-based representa-tion, NASS has invited and welcomes input from other societies and specialties.Evidence Analysis T raining of All NASS Guideline DevelopersNASS has initiated, in conjunction with the Uni-versity of Alberta’s Centre for Health Evidence, an online training program geared toward educat-ing guideline developers about evidence analysis and guideline development. All participants in guideline development for NASS have completed the training prior to participating in the guide-line development program at NASS. This train-ing includes a series of readings and exercises, or interactivities, to prepare guideline developers for systematically evaluating literature and developing evidence-based guidelines. The online course takes approximately 15-30 hours to complete and partici-pants are awarded CME credit upon completion of the course.Disclosure of Potential Conflicts of InterestAll participants involved in guideline development have disclosed potential conflicts of interest to their colleagues and their potential conflicts have been documented for future reference. They will not be published in any guideline, but kept on file for ref-erence, if needed. Participants have been asked to update their disclosures regularly throughout the guideline development process.Levels of Evidence and Grades of RecommendationNASS has adopted standardized levels of evidence (Appendix B) and grades of recommendation (Appendix C) to assist practitioners in easily un-derstanding the strength of the evidence and rec-ommendations within the guidelines. The levels of evidence range from Level I (high quality random-ized controlled trial) to Level V (expert consensus). Grades of recommendation indicate the strength of the recommendations made in the guideline based on the quality of the literature.Grades of Recommendation:A: Good evidence (Level I studies with consistent finding) for or against recommending intervention.B: Fair evidence (Level II or III studies with consistent findings) for or against recommending intervention.This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is toC: Poor quality evidence (Level IV or V studies) for or against recommending intervention.I: Insufficient or conflicting evidence not allow-ing a recommendation for or against intervention.The criteria for assigning these levels of evidence and grades of recommendation are the same as those used by the Journal of Bone and Joint Sur-gery, the American Academy of Orthopaedic Surgeons, Clinical Orthopaedics and Related Re-search, the journal Spine and the Pediatric Ortho-paedic Society of North America.In evaluating studies as to levels of evidence for this guideline, the study design was interpretedas establishing only a potential level of evidence. As an example, a therapeutic study designed as a randomized controlled trial would be considered a potential Level I study. The study would then be further analyzed as to how well the study design was implemented and significant short comings in the execution of the study would be used to down-grade the levels of evidence for the study’s conclu-sions. In the example cited previously, reasons to downgrade the results of a potential Level I ran-domized controlled trial to a Level II study would include, among other possibilities, an underpow-ered study (patient sample too small, variance too high), inadequate randomization or masking of the group assignments and lack of validated outcome measures.In addition, a number of studies were reviewed several times in answering different questions within this guideline. How a given question was asked might influence how a study was evaluated and interpreted as to its level of evidence in an-swering that particular question. For example, a randomized control trial reviewed to evaluate the differences between the outcomes of patients who received antibiotic prophylaxis with those who did not might be a well designed and implemented Level I therapeutic study. This same study, howev-er, might be classified as giving Level II prognostic evidence if the data for the untreated controls were extracted and evaluated prognostically.Guideline Development Process⏹Step 1: Identification of Clinical Questions Trained guideline participants were asked to submit a list of clinical questions that the guideline should address. The lists were compiled into a master list, which was then circulated to each member with a request that they independently rank the questions in order of importance for consideration in the guideline. The most highly ranked questions, as determined by the participants, served to focus the guideline.⏹Step 2: Identification of Work Groups Multidisciplinary teams were assigned to work groups and assigned specific clinical questions to address. Because NASS is comprised of surgical, medical and interventional specialists, it is impera-tive to the guideline development process that a cross section of NASS membership is represented on each group whenever feasible. This also helps to ensure that the potential for inadvertent biases in evaluating the literature and formulating recom-mendations is minimized.⏹Step 3: Identification of Search T erms andParametersOne of the most crucial elements of evidence analysis to support development of recommenda-tions for appropriate clinical care is the compre-hensive literature search. Thorough assessment of the literature is the basis for the review of existing evidence and the formulation of evidence-based recommendations. In order to ensure a thorough literature search, NASS has instituted a Literature Search Protocol (Appendix D) which has been fol-lowed to identify literature for evaluation in guide-line development. In keeping with the Literature Search Protocol, work group members have iden-This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is totified appropriate search terms and parameters to direct the literature search.Specific search strategies, including search terms, parameters and databases searched, are documented in the appendices (Appendix E).⏹Step 4: Completion of the LiteratureSearchAfter each work group identified search terms/ parameters, the literature search was implemented by a medical/research librarian, consistent with the Literature Search Protocol.Following these protocols ensures that NASS rec-ommendations (1) are based on a thorough review of relevant literature; (2) are truly based on a uni-form, comprehensive search strategy; and (3) rep-resent the current best research evidence available. NASS maintains a search history in EndNote,™ for future use or reference.⏹Step 5: Review of Search Results/Identification of Literature to Review Work group members reviewed all abstracts yield-ed from the literature search and identified the literature they would review in order to address the clinical questions, in accordance with the Litera-ture Search Protocol. Members identified the best research evidence available to answer the targeted clinical questions. That is, if Level I, II and/or III literature is available to answer specific questions, the work group was not required to review Level IV or V studies.⏹Step 6: Evidence AnalysisMembers of the work group independently devel-oped evidentiary tables summarizing study conclu-sions, identifying strengths and weaknesses and assigning levels of evidence. In order to systemati-cally control for potential biases, at least two work group members reviewed each article selected and independently assigned levels of evidence to the literature using the NASS levels of evidence. Any discrepancies in scoring have been addressed by two or more reviewers. The consensus level (the level upon which two thirds of reviewers were in agreement) was then assigned to the article.As a final step in the evidence analysis process, members identified and documented gaps in the evidence to educate guideline readers about where evidence is lacking and help guide further needed research by NASS and other societies.⏹Step 7: Formulation of Evidence-BasedRecommendations and Incorporation ofExpert ConsensusWork groups held Web casts to discuss the evi-dence-based answers to the clinical questions, the grades of recommendations and the incorporation of expert consensus. Expert consensus has been incorporated only where Level I-IV evidence is insufficient and the work group has deemed that a recommendation is warranted. Transparency in the incorporation of consensus is crucial, and all con-sensus-based recommendations made in this guide-line very clearly indicate that Level I-IV evidence is insufficient to support a recommendation and that the recommendation is based only on expert con-sensus.Consensus Development ProcessVoting on guideline recommendations was con-ducted using a modification of the nominal group technique in which each work group member independently and anonymously ranked a recom-mendation on a scale ranging from 1 (“extremely inappropriate”) to 9 (“extremely appropriate”). Consensus was obtained when at least 80% of work group members ranked the recommendation as 7, 8 or 9. When the 80% threshold was not at-tained, up to three rounds of discussion and voting were held to resolve disagreements. If disagree-ments were not resolved after these rounds, no recommendation was adopted.This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is toAfter the recommendations were established, work group members developed the guideline content, addressing the literature which supports the recom-mendations.⏹Step 8: Submission of the Draft Guidelinesfor Review/CommentGuidelines were submitted to the full Evidence-based Guideline Development Committee, the Research Council Director and the Advisory Panel for review and comment. The Advisory Panel is comprised of representatives from physical medi-cine and rehab, pain medicine/management, or-thopedic surgery, neurosurgery, anesthesiology, rheumatology, psychology/psychiatry and family practice. Revisions to recommendations were con-sidered for incorporation only when substantiated by a preponderance of appropriate level evidence.⏹Step 9: Submission for Board Approval After any evidence-based revisions were incorpo-rated, the drafts were prepared for NASS Board review and approval. Edits and revisions to recom-mendations and any other content were considered for incorporation only when substantiated by a preponderance of appropriate level evidence.⏹Step 10: Submission for Endorsement,Publication and National GuidelineClearinghouse (NGC) InclusionFollowing NASS Board approval, the guidelines were slated for publication, submitted for endorse-ment to all appropriate societies and submitted for inclusion in the National Guidelines Clearinghouse (NGC). No revisions were made at this point in the process, but comments have been and will be saved for the next iteration.⏹Step 11: Identification and Development ofPerformance MeasuresThe recommendations will be reviewed by a group experienced in performance measure development (eg, the AMA Physician’s Consortium for Per-formance Improvement) to identify those recom-mendations rigorous enough for measure develop-ment. All relevant medical specialties involved in the guideline development and at the Consortium will be invited to collaborate in the developmentof evidence-based performance measures related to spine care.⏹Step 12: Review and Revision ProcessThe guideline recommendations will be reviewed every three years by an EBM-trained multidisci-plinary team and revised as appropriate based on a thorough review and assessment of relevant litera-ture published since the development of this ver-sion of the guideline.This clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is toThis clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is to III. Incidence of DVT/PE in Spine SurgeryIn order to appreciate the incidence of these thrombo-sis-related complications in patients undergoing spinal surgery without antithrombotic prophylaxis, the work group performed a comprehensive literature search and analysis. The group reviewed 45 articles that were selected from a search of MEDLINE (PubMed), Co-chrane Register of Controlled Trials, Web of Science and EMBASE Drugs & Pharmacology that addressed the incidence and natural history of DVT and PE as-sociated with spinal surgery.Analysis of the questions related to the natural history of DVT in spinal surgery patients not receiving any prophylactic therapies was difficult due to a number of issues.1. Very few studies have been done in recent years inwhich absolutely no prophylaxis was used. Me-chanical pumps and/or compressive stockings are widely and routinely used after spinal surgery so that studies without such are rare.2. The diagnostic method for DVT and PE varywidely between publications. Older studies report only clinically evident thrombotic events. More recent studies, in large part due to evolving tech-nology, rely on a variety of different diagnostic methods including radionuclide scans, venogramsor ultrasound-based imaging. Thus, comparison of outcomes between different studies that use distinctly different diagnostic criteria is of ques-tionable validity.3. The patient populations addressed in the worldliterature vary widely. The study groups varied in age, ethnicity (potentially influencing genetic susceptibility), magnitude and length of surgery, and postoperative mobilization, all of which might influence the risk for thromboembolic disease. For example, it is well-established that bed rest isa risk factor for DVT. However, the pace at which patients are mobilized after spinal surgery varies widely. Mobilization protocols are rarely reported in detail in spine surgical studies.Because of these issues, the work group was unable to definitively answer the posed questions related to incidence of DVT/PE in spinal surgery patients not re-ceiving prophylactic antithrombotic therapies. How-ever, the work group felt that several important sug-gestions can be made based on the literature reviewed. These are included below along with a detailed analy-sis of the small subset of papers that met the guide-line’s inclusion criteria and provided information that was germane to the discussion of incidence in this patient population.The body of scientific and clinical literature on the topic of deep vein thrombosis (DVT) and pulmonary embolism (PE) is extensive. Either can occur spon-taneously or after a risk-enhancing event such as an injury or a surgical procedure. A variety of factors, including the patient’s health and genetic background, can influence the risk of this life threatening complica -tion.A. Incidence of DVT/PE in Unprophylaxed PatientsManaging this risk in patients undergoing spinalsurgery can pose substantial challenges. Treatment of DVT or a PE using anticoagulants in the immediate postoperative period may potentially lead to cata-strophic neurologic decline from epidural bleeding at the surgical site.What is the overallrate (symptomatic and asymptomatic) of DVT or PE following elective spinal surgery without any form of prophylaxis? What are the relative rates of clinically symptomatic DVT or PE (including fatal PE) without any form or prophylaxis following elective cervical, thoracic, and lumbar surgery?Work Group Conclusions/Suggestions:1. Deep vein thrombosis and subsequent pulmonary embolus can occur following spinal surgery, which in turn can lead to morbidity and death. Anyone participating in the careof spinal surgery patients should be aware of these conditions as known potential events.2. The incidence of DVT and PE in patients undergoing spinal surgery likely varies according to the magnitude of the surgery and perioperative mobilization.3. The use of “historical controls” to address the incidence of DVT or PE in a perioperative population is probably not appropriate.4. Clinical examination alone is not a reliable method to confirm the diagnosisof a DVT. Objective diagnostic methods,such as venography or Doppler ultrasound, should be used to confirm a suspected DVTin postoperative spine patients. Future studies to characterize the incidence ofDVT in postoperative spine patients should use objective diagnostic methods such as venography or Doppler ultrasound.Gruber et al18 performed a prospective comparative study to determine the incidence of bleeding compli-cations in patients undergoing lumbar disc surgery treated with minidose heparin-dihydroergotamine (DHE) or placebo. Of the 50 patients included in the study, 25 received 2500IU heparin-DHE twice daily and 25 were assigned to the placebo group. Injections were administered two hours preoperatively, with postoperative administration at 12-hour intervals for at least seven days or until the patient was discharged from the hospital. Of the 25 assigned to the control group, five had received heparin at another hospi-tal and were excluded from the analysis. Surgeons reported bleeding and, if clinically suspected, DVT was diagnosed by phlebogram, plethysmography, Doppler ultrasound or I125 fibrinogen test. If a PE was suspected, a chest radiograph, ECG, ventilation-perfusion scan or pulmonary angiogram was obtained. The authors reported no clinically evident DVT or PE events in this small series of consecutive patients. The authors noted increased intraoperative bleeding in 24% (6/25) of patients in the heparin-DHE group and 28% in the placebo group, a difference that was not statistically significant.In critique of this study, diagnostic methods for DVT were not standardized and only conducted when prompted by clinical suspicion. Furthermore, patient numbers were quite low and the definition of “lum-bar disc operations” was unclear. Due to these meth-odological limitations, this potential Level II study provides Level III evidence of a low risk of DVT/PE in patients undergoing lumbar disc surgery.Joffe et al20 reported results of a prospective case se-ries investigating the incidence of DVT in patients un-dergoing elective neurosurgical procedures. Of the 23 neurosurgical patients included in the study, only 10 were spinal cases. All patients were screened daily for the duration of their hospital stay (which was at least seven days) for DVT with an I125 fibrinogen test and Doppler ultrasound. The authors reported that 60% of the spinal patients (6/10) developed asymptomatic postoperative DVT. They concluded that neurosurgi-cal patients are at risk for DVT and that these patientsThis clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods ofare often asymptomatic. Based on their findings, the authors further suggested that DVT will be underdiag-nosed by clinical criteria alone.In critique, this was a very small study consisting of only a few spinal patients without details about the type and extent of spine surgery. Due to these weak-nesses, this potential Level IV study provides Level V evidence that asymptomatic DVT is not uncommon in a nonselect group of patients undergoing elective spinal surgery likely followed by prolonged periods of bed rest, an assumption made based on the year the study was published. The applicability of these find-ings today is questionable given that prolonged peri-ods of bed rest are no longer recommended following surgery.Lee et al22 conducted a prospective comparative study to determine the rate of DVT following elective major reconstructive spinal surgery without antithrombotic therapies in an East Asian (Korean) population. All 313 patients included in the study were screened via duplex ultrasonography between the fifth and seventh postoperative days. Authors reported a 1.3% (4/313) overall incidence of DVT, with a clinically symptom-atic presentation in only 0.3% (1/313) of patients. The authors concluded that East Asians undergoing these procedures do not get DVT often enough to warrant prophylaxis. The authors further suggested that rou-tine screening and prophylaxis in this specific patient population is not warranted.In critique of this study, an unknown number of pe-diatric patients were included. A subgroup analysis addressing the adult population was not provided. In addition, patients were treated with postoperative bed rest for a mean of 7.4 days. This potential Level I study provides Level II evidence suggesting a lower incidence of DVT after elective major reconstructive spinal surgery without antithrombotic therapy than previously reported. Although the authors concluded this incidence was related to the ethnicity of the pa-tient group, it should be noted that other unidentified factors may have influenced the DVT rate.Oda et al30 reported a prospective comparative study documenting the prevalence of DVT after posterior spinal surgery in patients not receiving antithrombotic therapies. Of the 134 patients included in the study, 110 were screened for DVT by venography within 14 days of surgery (mean = 7.2 days) and clinically fol-lowed for at least three months. Authors reported that 15.5% (17/110) of patients had venographic evidence of DVT, while none had clinical manifestations of DVT. The authors also indicated the prevalence of DVT by surgical region; 26.5% of lumbar, 14.3% of thoracic and 5.6% of cervical patients had venograph-ic evidence of DVT. Statistical comparison between patients who did and did not have DVT demonstrated that increased age was a statistically significant risk factor (Mann–Whitney test; P< 0.05). The authors concluded that the incidence of DVT after posterior spinal surgery is higher than generally appreciated. Therefore, they felt that further study is necessary to clarify the appropriate screening method for and pro-phylaxis of DVT after spinal surgery.This study provides Level II evidence that the rateof DVT in postoperative spine surgery patients may be underestimated. Clinical manifestations are not reliable for the diagnosis of DVT. Increased age and posterior lumbar surgery are risk factors. It should also be noted that all patients included in this study had an interval of bed rest following surgery. The applicability of these findings today is questionable given that prolonged periods of bed rest are no longer recommended following surgery.Uden et al40 described a retrospective case series documenting the rate of clinically evident DVT in a population of 1229 patients treated surgically with Harrington instrumentation followed by three to five weeks of bed rest. Diagnosis of DVT was confirmed via contrast and/or isotope phlebography only when clinically suspected or by autopsy. The authors re-ported a 0.65% (8/1229) incidence of DVT and 0.08% (1/1229) incidence of PE in this scoliosis patient population.In critique of this study, patients were not enrolled at the same point in their disease and some patients wereThis clinical guideline should not be construed as including all proper methods of care or excluding other acceptable methods of。
脊柱疾病患者指南
脊柱疾病患者指南疾病描述退变性椎间盘疾病老化和/或外伤导致椎间盘(脊柱椎体间的减震器)磨损。
退变性脊柱不稳退变性脊柱不稳脊柱关节(椎间盘和小关节)软骨随年龄增加而磨损,导致脊柱不稳。
坐骨神经痛疼痛、麻木、麻刺感、一侧或双侧下肢无力,这是由于一个或多个坐骨神经分支的炎症或压迫导致的(神经症状)。
椎间盘脱出椎间盘破裂,有时会导致对神经或脊髓的压迫,产生一侧或双侧上肢或下肢的疼痛、麻木、无力(神经症状),椎间盘脱出导致的神经疼痛在坐位时通常会加重。
狭窄狭窄椎管面积缩小,如果狭窄压迫神经,则导致神经分布区疼痛。
通常站立或是行走一段时间后,压迫会导致一侧或双侧腿痛,坐位可缓解疼痛。
腰椎滑脱症由于椎间盘退变或是儿童或青少年时期的骨折导致一个椎体相对于另一个椎体滑移,滑移和不稳可能导致神经压迫症状,除此之外,还造成活动能力丧失的疼痛。
脊柱侧凸脊柱曲度通常是由于先天原因,或是未知或退变的原因导致的,最常见的原因是青少年特发性胸椎侧凸,青春期女孩多见。
骨质疏松脊柱钙质丢失,最常见于绝经后老年妇女,它是一种悄无声息的疾病,可能直到脆弱的骨骼出现骨折才被发现。
骨折/脱位脊柱骨折通常由外伤导致(最常见的原因是交通事故)和高空坠落,也可能出现在骨质疏松症患者的轻微创伤后。
另一方面,脊柱脱位几乎总是由高能量损伤导致。
肿瘤肿瘤可能是良性或恶性,尽管肿瘤可以是脊柱原发性的,但大多数情况下,是由其他器官的恶性肿瘤转移导致的(转移灶),脊柱肿瘤典型的是夜间痛,全身不适,偶尔出现截瘫。
感染脊柱的骨骼和椎间盘可能发生感染,通常是由血液或尿液源性细菌引起的,它通常发生在很老的患者或是很年轻的患者,另外就是免疫功能低下的患者。
可选择的治疗方式治疗退化性椎间盘疾病,脊柱不稳,坐骨神经痛,椎间盘脱出,狭窄和滑脱,通常最初先使用止痛药、物理治疗、脊柱类固醇注射进行治疗,当这些治疗失败后,可采用手术治疗,手术通常为神经减压,然后可进行脊柱融合或者不进行融合。
脊柱骨折诊治指南

脊柱骨折诊治指南
诊断
临床表现
•脊柱骨折常伴随严重疼痛和活动受限。
•患者有可能出现神经系统症状,如感觉障碍、肌力减退等。
影像学检查
•X光、CT和MRI等影像学检查是确诊脊柱骨折的必要手段。
•影像学检查能够明确骨折部位、类型和严重程度,为后续治疗提供重要参考。
治疗
保守治疗
•轻度脊柱骨折可考虑保守治疗,包括静卧休息、颈颈固定等。
•保守治疗需要密切监测患者症状和影像学变化,避免并发症的发生。
手术治疗
•严重脊柱骨折或有严重神经系统损伤的患者常需手术治疗。
•手术治疗能够稳定脊柱、复位骨折部位,减少神经系统损伤风险。
康复
•脊柱骨折康复过程需要经过康复训练和康复理疗,帮助患者恢复功能和活动能力。
•康复过程中需要注意避免再次受伤和保持良好的体态。
结语
脊柱骨折是一种常见但严重的创伤,诊断和治疗需由专业医生进行。
本指南旨在帮助临床医生更好地处理脊柱骨折患者,提供了诊断、治疗和随访等方面的指导,希望能对临床工作有所帮助。
请根据需要调整分级。
临床技术操作规范及诊疗指南骨科学分册
临床技术操作规范及诊疗指南骨科学分册脊柱外科篇叶正云荆门市第一人民医院脊柱外科编著目录临床技术操作规范1.神经系统体格检查2.骨科无菌术概述伤口感染的来源手术医师和护士的准备手术部位的准备3.经椎弓根脊柱内固定术胸椎椎弓根螺钉技术腰椎椎弓根螺钉技术骶椎椎弓根螺钉技术椎弓根螺钉置入手术操作步骤4.脊柱融合术脊柱融合术改良融合术脊柱外科诊疗指南1.颈椎骨折2.胸椎及腰椎骨折脱位3.颈椎病4.颈椎管狭窄症5.胸椎椎管狭窄症6.腰椎间盘突出症7.腰椎椎管狭窄症8.腰椎失稳症9.脊柱滑脱症10.椎间盘炎11.第三腰椎横突综合征12.特发性脊柱侧凸神经系统检查1.感觉一般只测定痛觉及触觉,必要时还可测定温觉、位置觉、振动觉、两点辨别觉及本体感觉。
末梢神经损伤时,相应的神经分布区域就会有感觉障碍。
横贯性脊髓损伤,在损害平面及其以下有感觉障碍,损害水平以上有一感觉过敏带。
半侧脊髓损伤可在受伤节段以下对侧出现痛觉、温觉障碍以及同侧的运动障碍。
2.运动观察肌肉外形、周径、肌力及肌张力。
正常肌肉在静止时保持一定程度的张力。
上运动元神经损伤时肌张力增强,被动运动受阻;下运动神经元损伤时肌张力减弱,肌肉松弛无力。
3.反射应在肌肉放松的体位进行,两侧对比,常用的检查如下。
(1)深反射:刺激肌腱、关节内的本位感受器而引起的肌肉收缩反应。
肱二头肌反射(C57);肱三头肌反射(C68);膝腱反射(L24);跟腱反射(L42).。
(2)浅反射:刺激皮肤的体表感受器而引起的肌肉收缩反应。
腹壁反射:上腹(T79),中腹(T911),下腹(T111);提睾反射(L12);肛门反射(S45)。
(3)病理反射:一般在中枢神经受损时才出现,如征、征、髌阵挛、踝阵挛等。
4.自主神经(1)皮肤、毛发、指(趾)甲营养状态:自主神经受损区的皮肤失去正常的光泽,粗糙,毛发脱落;指(趾)甲失去光泽,易裂,变形。
(2)皮肤划痕试验:钝针快划皮肤,几秒后出现白色条纹,持续1~5,见于交感神经兴奋性高者。
骨科前20种疾病诊疗指南(脊柱部分)

骨科前20种疾病诊疗指南(脊柱部分)1.过伸性颈椎毁伤2.腰椎间盘凸起症3.腰椎椎管狭小症4.颈椎病5.胸腰椎骨折兴义市人平易近病院脊柱外科2013年12月28日过伸性颈椎毁伤[界说]颈椎过度伸展性暴力造成的颈脊髓毁伤,常伴随稍微或隐匿的骨毁伤,X线多无平常表示,故易被疏漏,影响治疗.该毁伤可占全颈椎各类毁伤的29~50%,多见于中老年人,常伴脊髓中心管分解征.[诊断]一.症状额面及鼻部擦伤和皮肤裂伤是最明显.多见的临床表示,系毁伤时额面部或鼻部撞击物体或遭遇打击所致.该特点常能提醒颈椎毁伤的外力感化机制,是断定颈椎过伸性毁伤较有价值特点之一.因神经体系毁伤程度不一,临床表示轻重程度有很大不同.二.体征局部压痛及活念头能受限.毁伤节段椎前压痛明显,尔后构造压痛少见.神经体系毁伤多表示为脊髓中心分解征和前脊髓分解征,少数表示为部分和轻微脊髓毁伤.脊髓中心分解征典范表示为:上肢瘫痪重于下肢,手部重于臂部,触.痛觉伤害重于深感到.轻微和部分脊髓毁伤无明显的脊髓中心管毁伤的特点.三.特别检讨:无.四.帮助检讨X线表示:颈椎过伸性毁伤以软组织毁伤为明显,骨性毁伤小而隐匿,需细心不雅察,以免漏诊.其重要X线现象有:(一) 伤椎体前下缘三角形撕脱骨折片,需与前纵韧带节段性骨化辨别.(二) 毁伤节段颈椎间盘和椎前软组织影的变更.颈椎椎前毁伤出血或水肿时,造成毁伤处椎前软组织影肿胀,椎间隙增宽.(三)中老年患者常伴随颈椎退行性转变及椎管矢状径缩小,毁伤多产生于C4~5.C5~6节段.MR检讨是须要的,可明白脊髓毁伤程度和规模,以及脊髓受压的程度和致压物的起源和性质.[辨别诊断]颈椎过伸性毁伤易漏诊,诊断时应留意以下几点:一. 详尽病史的收集,常能供给毁伤机制;颅脑伤患者,也应设法懂得毁伤时姿态和暴力.二.颅面部毁伤均应通例摄颈椎X线片,以免因其他部位毁伤而掩饰颈椎毁伤.三.侧位X线片必须清楚显示高低颈椎构造.上颈椎毁伤而神经症状表示低位时,需留意不雅察低.位颈椎有无变更.伸屈侧位X线片有必定诊断价值.但必须慎用,以免加重脊髓毁伤.四.典范脊髓中心分解征,常能提醒颈椎过伸性毁伤;而其他类型脊髓毁伤,必须联合上述各项再作断定.五.斟酌其他机制引起的颈脊髓伤,如椎体垂直紧缩骨折也可造成脊髓中心分解征.[治疗]一经确诊,以非手术治疗为首选.一.非手术治疗通例运用颌枕带或者头环牵引,重量2~3kg,牵引地位宜取颈椎略屈150,中断牵引2—3周,然后以头颈胸石膏或颈托固定1~2月.牵引时代,运用速尿或地塞米松10~20mg,静脉滴注,每日2次,以利减轻脊髓水肿及进步机体应激才能.二.手术治疗(一)顺应证:1.脊髓毁伤后经非手术治疗无明显后果,并已精确肯定毁伤节段者;2.影像学检讨显示有明显骨毁伤,并对脊髓形成明显榨取者;3.临床症状中断消失,保守治疗进程中有加重趋向者;4.归并颈椎病和后纵韧带骨化,因外伤诱发发病者,待病情稳固后行手术治疗.(二)手术办法:根据脊髓致压物的部位和规模,选择合适的手术入路和减压办法.单个或少数节段的前方榨取宜施行前路减压;今后方为主的榨取或普遍后纵韧带骨化的前方榨取,行后路减压.(1).颈椎前路减压椎间植骨融会加钛板内固定术(颈5/6为例)手术步调:4-6厘米斜行瘦语,切开皮肤.皮下组织.颈阔肌,于颈动脉鞘与颈内脏鞘间隙分别达椎体前部,将颈内脏鞘牵向左侧,切开颈椎前筋膜,用打针针头标识表记标帜,C型臂透视定位颈5/6椎间隙,将指导钻芯的扁刀打入颈5/6椎间隙正中,用13mm环锯套入指导钻芯,加压并顺时针扭转,钻通颈椎后将环锯连同钻芯和骨与椎间盘组织掏出,再用刮匙刮除残留椎间盘和边周骨质进行充分减压,用心理盐水反复冲洗,清除组织碎片. 3.取左髂前上棘后外侧长约6厘米瘦语,逐层切开,吐露髂骨后凿取恰当大小骨块,再根据减压孔大小进行修整后用槌骨器轻轻打入.再于颈5.6椎体前朴直中置入4孔H型钛板,依次经钻孔.攻丝后拧入螺钉4枚固定,术中不雅察及C型臂透视钛板服帖优胜,地位满足. 4.充分冲洗瘦语,颈部瘦语置橡皮引流条或引流管1根,逐层缝合,手术顺遂,术中出血不久不多,纱布器械盘点无误,术后患者安返病房.(2).颈椎病后路单开门减压术手术步调:患者右侧卧位,通例消毒铺单,取颈部后正中长约15厘米纵行瘦语,逐层切开,定位明白后,紧贴颈3-7棘突两侧割断剥离竖棘肌,显露颈3-7两侧椎板,逐个咬断颈3-7左侧椎板以及颈2-3棘间韧带和颈7-胸1棘间韧带,切除黄韧带,显露硬膜,术中见硬膜搏动优胜.再咬断颈3-7右侧椎板外板,咬除颈6.7部分棘突,颈3-7棘突打孔后穿入双粗线.将颈3-7棘突向右侧翻开,使左侧椎板启齿约1.5厘米,再用粗丝线将棘突缝系至右侧小关节四周.用大量心理盐水充分冲洗瘦语,瘦语内置引流管一根,逐层缝合,手术顺遂,术中出血不久不多,纱布器械盘点无误,术后予颈托外固定,患者安返病房.三.药物治疗牵引时代,运用速尿或地塞米松10~20mg,静脉滴注,每日2次,以利减轻脊髓水肿及进步机体应激才能.四.康复治疗.(一)功效锤炼:1),四肢力气及关节活动度练习.2),肺功效练习.3).膀胱功效练习.4),自动按摩肌肉.(二)物理治疗:电针.神经肌肉治疗仪等治疗.腰椎间盘凸起症[界说]腰椎间盘凸起症是骨科罕有病和多发病,又称腰椎纤维决裂症.腰椎髓核凸起症,是腰腿痛最罕有的原因.本病好发于20~50岁的青丁壮,男性和重体力劳动者多见.[诊断]一.诊断根据(一)有腰部外伤.慢性劳损史.大部分患者发病前有慢性腰痛史.(二)腰痛并向臀部和下肢放射,腹压增长苦楚悲伤加剧(咳嗽.喷嚏时),可有间歇性跛行,并局限于特别体位以缓解苦楚悲伤,少数病人有大小便功效障碍.(三)脊柱活动受限,并有侧弯,腰椎心理前凸削减或消掉,病变部位棘突旁压痛并向下肢放射,表示为典范的跛行步态,又始需扶拐行走,甚至不克不及行走.(四)下肢受累神经安排区有感到减退或过敏,肌肉无力或萎缩,甚或瘫痪,膝.跟腱反射削弱或消掉,偶有二便掉控或/和鞍区麻痹.(五)直腿举高和增强实验阳性,起坐屈膝实验阳性,昂首屈颈实验阳性.健腿举高实验阳性(根腋型),屈髋屈膝实验阳性,仰卧挺腹实验阳性.股神经牵拉实验阳性(L2~3.L3~4).(六)X线摄片检讨见脊柱侧弯.腰心理前凸消掉,病变椎间隙变窄,相邻椎体边沿有骨赘增生,碘油造影摄片精确率在70%~90%,CT和MRI检讨可确诊椎间盘脱出的部位和程度.二.临床分型病理分型1.旁侧型多半为一侧凸起,少数为双侧凸起.(1)肩上型髓核凸起位于神经根的外前方,将神经根压向后内侧,临床表示为根性放射痛,脊柱多向健侧曲折,向患侧崛起,患侧椎旁压痛及放射痛.(2)腋下型髓核凸起位于神经根前方,将神经根向后挤压,临床表示为轻微根性放射痛,脊柱心理前凸消掉,前后活动均受限,多无侧弯畸形,椎旁压痛及放射痛明显.2.中心型髓核从间盘后方中心凸起.(1)偏中心型髓核凸起位于椎间盘后方中心偏于一侧,重要榨取一侧神经根及马尾神经,或两侧均受压,但一侧较轻而另一侧较重.(2)正中心型髓核凸起位于椎间盘后朴直中心,一般凸起规模较大,重要表示为普遍瘫痪及鞍区感到障碍,二便功效障碍,并没有神经根刺激或榨取症状.[辨别诊断]一.急性腰肌筋膜炎又称纤维组织炎.好发于腰背筋膜.棘上和肌腱韧带以及髂嵴后部等肌筋膜附着处,属软组织风湿性疾病.其发生发火时腰痛激烈.活动受限.腰肌痉挛,苦楚悲伤有时牵扯到臀部.大腿两侧,甚至小腿,但其性质属牵扯性苦楚悲伤,与腰椎间盘凸起症所引起的根性苦楚悲伤本质不合.该病缺少阳性体征,无感到及反射转变,偶可摸到硬结或条索状物,可有明显的压痛点,痛点关闭可使苦楚悲伤症状消掉.二.腰椎管狭小症多产生于中年人,起病迟缓,重要症状为腰痛.腿痛及神经性间歇性跛行,站立行走时症状加重,歇息.下蹲时减轻,一般影像学检讨可明白辨别.三.腰3横突分解征该病可有外伤或劳损史,表示为腰痛.臀部苦楚悲伤,活动时加重,苦楚悲伤可牵扯到大腿后侧,少数到小腿.但查体直腿举高实验阴性,无下肢放射痛及神经根受累转变.常可触及腰3横突过长,于骶棘肌外缘横突处,局部有明显压痛点,作横突及四周浸润关闭,症状可明显缓解.四.梨状肌分解征常为慢性也可急性发生发火,走路活动时加重,歇息后可减轻,直腿举高实验可为阳性,但神经症状不明显,虽有感到平常,但无具体散布.查体时可有臀肌萎缩,坐骨大切迹区有压痛,屈髋位抗阻外旋或自动内旋髋关节可诱发苦楚悲伤.梨状肌局部痛点关闭可使症状缓解或消掉,此乃与腰椎间盘凸起症的辨别要点.五.慢性腰肌劳损该病病程较长,多有急性腰部扭伤或外伤史,患肢常诉腰骶部有酸痛.钝痛感,有时消失下肢反射性苦楚悲伤,但症状具有歇息时轻.劳顿后重的特色,病人常以拳击腰部以缓解苦楚悲伤,且症状与风寒湿关系亲密.一般经歇息.理疗.按摩按摩可治愈.六.脊柱肿瘤脊柱肿瘤的腰痛为中断性进行性加重,不因卧床歇息而减轻,随肿瘤的发展侵润,榨取神经根产生坐骨神经痛,当侵及脊髓时可产生截瘫现象,患者一般多伴随身材日趋瘦削.贫血.血沉增快.碱性磷酸酶增高级.影像学检讨多显示椎体或椎管内有占位性病变.七.腰椎结核和骶髂关节结核部分腰椎结核患者可消失以腰痛或坐骨神经痛为主的临床表示,易于腰椎间盘凸起症相混杂.但结核病发病迟缓,进行性加重,无间歇期,多伴随午后潮热.全身乏力,身材逐渐瘦削,且血沉加速,肺部多有原发病灶.X线片可发明椎间隙变窄,椎体边沿隐约不清,有明显骨质损坏及寒性脓肿形成,有时可发明腰椎小关节及骶髂关节的损坏.[治疗]一.手段治疗(一)仰卧按摩法实用于症状较轻,脊柱侧弯不重,直腿举高可达50°者,患者仰卧,术者在腰腿把柄及相干穴位依次作按压揉摩.拿捏.提腿拌动等手段.(二)斜搬伸腿法实用于个体症状轻微,不克不及起坐的急性期患者,患者仰卧,术者一手按其髂骨后缘,一手放于病人肩部,两手同时向相反偏向用力斜搬,这是可在腰骶部闻及弹响声,然后伸直下肢作腰髋过伸动作各3次,术毕可换体位作另一侧.二.牵引治疗牵引可以拉宽椎间隙,扩展椎间孔和神经根管,促使凸起物回纳和减轻对神经根的榨取.经常运用骨盆牵引,每侧牵引重量10~20gk,每次牵拉30min,隔日1次,10次为1疗程.三.关闭治疗经常运用痛点.穴位关闭,关闭液为醋酸强的龙松2ml加%普鲁卡因4ml,也有采取硬脊膜外腔激素关闭.四.经皮椎间盘射频臭氧消融术手术步调:1.取俯卧位,腹下垫枕减轻腰骶角,按术前检讨.体查或椎间盘造影阳性椎间盘为治疗椎间盘(义务椎间盘).2.C型臂下定位,以脊柱旁开10-20cm视患者体形调剂)及棘突旁经椎板间隙为穿刺入路点(椎板间隙入路重要针对有下肢症状者).3.局麻下,予射频针穿刺进入椎间盘,拔出针芯后拔出射频热凝针,分别在椎间盘2点.中间.8点用70°进行一次热凝,时光60S,将温度调至80°再进行一次热凝,时光2-3分钟.在治疗进程中患者可消失苦楚悲伤复制,同时暗示义务椎间盘精确.伴随下肢症状患者,可经同侧椎板间隙穿刺到椎间盘后缘,拔出针芯后拔出射频热凝针,予70°进行一次热凝,时光60S,将温度调至80°再进行一次热凝,时光根据患者术中耐受程度决议,平日情形下为2分钟.对MRI提醒椎间盘纤维环后方高旌旗灯号区病例,可直接在C型臂下定位下穿刺至椎间盘纤维环后方高旌旗灯号区进行热凝,温度调至80°,时光2分钟.拔出射频热凝针,在椎间盘中间或中后1/3接壤脉冲式注入浓度50ug/ml臭氧.根据患者耐受情形可推注5-10ml不等.术后卧床歇息1-2天,佩带弹力腰围下床.五.手术治疗(“开窗”腰4/5椎间盘摘除术)对于症状轻微,影响工作,生涯,不克不及接收牵引.手段治疗,或经保守治疗无效者,应采取手术治疗.手术多选用局部侵润麻醉或硬脊膜外麻醉,手术瘦语为腰部后正中或稍偏向患侧的纵瘦语,长度应包含术前诊断病变的椎间隙上.下各一椎体.切开皮肤.皮下组织后显露椎板,根据术前病变部位的肯定及椎间盘凸起的程度,选择性的进行开窗式椎间盘髓核摘除术,Quadrant通道下椎间盘髓核摘除术.(一)“开窗”腰4/5椎间盘摘除术手术步调:1.患者麻醉成功后,取俯卧位,通例消毒铺单. 2.以腰4.5棘间为中间,取腰正中长约7厘米纵行瘦语,切开皮肤.浅筋膜.腰背筋膜,紧贴腰4.5棘突左侧向前向外割断剥离骶棘肌,分别显露腰4.5左侧椎板,经由过程C型臂透视确认定位后,咬除腰4椎板下缘以及腰5椎板上缘,进行“开窗”,再剥离切除黄韧带,分别显露硬膜以及腰5左侧神经根,术中见椎间盘髓核组织凸起,榨取腰5神经根. 3.手术扩展神经根管,游离神经根,切除黄韧带,将神经根与硬膜轻柔牵向内侧后,掏取髓核组织,并深刻至椎间隙将髄核组织取清洁.不雅察掏出量满足,探察神经根管通行.再次C型臂透视确认椎间隙无误. 4.盘点器械无误,用大量心理盐水冲洗椎间隙及瘦语后,瘦语内置引流管一根,逐层缝合瘦语.手术顺遂,术中出血不久不多,标本送病理,术后患者安返病房.术中在分别粘连以及牵拉神经根及硬脊膜时,必须手段轻柔,防止造成对神经根和马尾神经的毁伤;术中要完全止血,术后通例放置引流条,防止渗血榨取神经.(二)Quadrant通道下椎间盘髓核摘除术手术步调:1.患者麻醉成功后,取俯卧位,通例消毒铺单. 2.瘦语位于腰4.5棘间左侧约0.5-1cm,长约3cm,切开皮肤.浅筋膜.腰背筋膜,沿骶棘肌肌间隙剥离骶棘肌,装配Quadrant通道分别显露腰4.5左侧椎板,咬除腰4椎板下缘以及腰5椎板上缘,再剥离切除黄韧带,分别显露硬膜以及腰5左侧神经根,术中见椎间盘髓核组织凸起,榨取腰5神经根. 3.手术扩展神经根管,游离神经根,切除黄韧带,将神经根与硬膜轻柔牵向内侧后,掏取髓核组织,并深刻至椎间隙将髄核组织取清洁.不雅察掏出量满足,探察神经根管通行.4.盘点器械无误,用大量心理盐水冲洗椎间隙及瘦语后,瘦语内置引流管一根,逐层缝合瘦语.手术顺遂,术中出血约20ml,标本送病理,术后患者安返病房.(注:术中在分别粘连以及牵拉神经根及硬脊膜时,必须手段轻柔,防止造成对神经根和马尾神经的毁伤;术中要完全止血,术后通例放置引流条,防止渗血榨取神经.)六.药物治疗气血瘀阻型宜活血化瘀,舒筋止痛,药用桃红四物汤加味内服,也可选用三七片,红药片等中成药;肝肾亏虚型宜滋补肝肾.舒筋通络,方用杜仲散加味内服,也可选用六味地黄丸等中成药;寒湿侵袭型治疗宜祛风除湿,药用独活寄生汤加味内服,中成药可选大活络丹,疏风定痛丸等.七.功效锤炼(一)重手段治疗后,应严厉卧床3d,再合营床上腰背肌锤炼1周,留意限制腰部前屈活动,然后带护腰下床活动,慢慢做腰部前屈.下蹲活动.(二)开窗摘除术后4周可下床活动,椎板切除后摘除者恰当延缓下床活动时光.[疗效评定尺度]根据《中医病症诊断疗效尺度》:痊愈:腰部苦楚悲伤根本消掉,直腿举高实验隐性,恢复正常工作;显效:腰部苦楚悲伤部分消掉,无明显压痛点,直腿举高实验阴性;有用:有轻度腰腿苦楚悲伤,直腿举高可疑阳性,部分恢复工作;无效:腰腿苦楚悲伤好转,直腿举高实验阳性,不克不及胜任工作.腰椎椎管狭小症[界说]是指腰椎椎管.神经根管及椎间孔变性或狭小并引起腰腿痛,间歇性跛行等临床症状.多发于40岁以上中年人,尤其是体力劳动者.[诊断]一.诊断根据(一)常有慢性下腰痛病史,部分病人有创伤病史.(二)多发于40岁以上中年患者.体力劳动者多见.(三)长期反复的腰腿痛和间歇性跛行.站立或走路过久症状加重,躺下或蹲位以及骑自行车症状可减轻或消掉,前屈时减轻,后伸时加重.大多半患者在走路或锤炼时消失单侧或双侧下肢麻痹,沉重.苦楚悲伤.乏力,歇息或下蹲后好转.偶有尿频或排尿艰苦.(四)脊柱可有侧弯,心理前突减小,可有下肢感到障碍,腱反射迟钝以及肌力削弱或肌肉萎缩.(五)直腿举高实验阳性,腰部过伸实验阳性.(六)X线摄片可以帮忙诊断,CT及MRI能进一步肯定并定性.二.临床分型病理分型1.中心椎管狭小腰腿苦楚悲伤,双下肢麻痹,跛行,可一侧轻,一着重.重者有鞍区感到减退,排尿功效障碍,下肢感到与肌力减退规模也较大.2.侧隐窝狭小体征较局限,常有明显的腰肌重要及响应的椎旁压痛点,响应神经根安排区功效减退或障碍.3.神经根管狭小也是榨取单一神经根,症状和体征与侧隐窝狭小类似,重要表示为神经根痛,而无明显的间歇性跛行.临床上很难与单纯后外方椎间盘凸起症相辨别,前者症状较重.4.混杂型狭小兼有以上两个或三个原因,症状与体征更轻微.[辨别诊断]一.腰椎间盘凸起症本病多见于青丁壮,急性起病,腰痛归并下肢放射痛,多有腰前屈受限,查体可有脊柱侧凸,棘旁压痛.叩击痛阳性并向下肢放射,屈颈实验.颈静脉榨取实验.直腿举高实验和增强实验均为阳性.二.动脉源性间歇跛行是因为动脉血液轮回缺少引起的,其特点是肢体在活动时有一组或多组肌肉产生苦楚悲伤症状,苦楚悲伤为钝痛,也可为痉挛性苦楚悲伤或锐痛,无感到障碍,无腱反射平常,患肢皮温常下降,动脉搏动常削弱,行走时可消掉,动脉造影有助于诊断.[治疗]一.手段治疗实用于早期狭小,症状较轻着,先用按摩.按摩.揉捏等手段在局部舒筋活络,目标是放松腰背部肌肉.尔后根据病情类型分别采取活络散搓法.顺督按压法.通痹推脊法.牵抖法.屈腿圈晃法.补肾摩肤法等手段.手段应懈弛轻柔,不成粗暴,手段的目标在于舒通经络,促进局部软组织炎性水肿的清除,解除榨取,缓解症状.二.牵引治疗顺应症同上.经常运用骨盆牵引,目标在于放松腰部肌肉,减轻榨取症状,每日1次,每次30min,10d为1疗程.三.其它治疗拔取痛点及相干穴位行针刺疗法,隔日1次,10次为1疗程,腰腿痛甚时,或作痛点关闭,经常运用关闭液为当归打针液或强的松龙混杂液,每周1次,3次为1疗程;急性发生发火时,可采取歇息法,取屈髋.屈膝侧卧位歇息,应尽量卧床,直至症状缓解.四.手术治疗腰椎管的骨纤维性狭小一般不会自行解除,故有中断榨取而症状较重者宜采取手术治疗.手术均选用硬脊膜外麻醉.(一)全椎板切除术实用于中心椎管狭小.手术选用脊柱后正中瘦语,显露出定位椎板.先将欲切除椎板的棘突咬除,再切除两椎板间黄韧带,用咬骨钳将椎板的中心部分咬除,可在直视下向两侧扩展,咬除椎板及黄韧带,直至小关节突邻近.细心检讨硬膜和神经根榨取的狭小身分,切除造成狭小的骨纤维构造.全椎板切除术显露好,视野清楚,但对术后脊柱的稳固性有必定的影响.(二)半椎板切除术顺应于单侧的侧隐窝狭小.神经根管狭小及关节突肥大.沿棘突作直皮肤瘦语,显露术侧的椎板及小关节,切除患部椎板及黄韧带,进入椎管,然后慢慢向上咬除,直至上一个椎板间隙,须要时也可切除上一节段及下一节段的部分半椎板.直视下切除上.下小关节突的内侧半,探查侧窝及神经根,完全解除榨取.此法对脊柱的稳固性影响很小.(三)椎板间扩展开窗术对诊断明白的单一侧隐窝狭小可用此术式.其办法是先切除椎板间的黄韧带,再向上.下咬除部分高低椎板缘,即可显露椎管,办法与半椎板入路雷同.(四)腰椎后路椎板减压椎间融会椎弓根钉内固定术实用于减压规模广归并节段不稳,具体手术步调如下: 1.麻醉安稳后,患者俯卧位,通例消毒铺单. 2.以腰4棘突为中间,取腰正中长约12厘米纵行瘦语,切开皮肤.浅筋膜.腰背筋膜,紧贴腰4-5棘突两侧向前向外割断剥离骶棘肌,分别显露腰4-5双侧椎板.关节突.横突. 3.C型臂透视确认定位后,选择腰4两侧横突中点连线与上关节突外侧缘切线交点为进针点,打入定位针2枚,并留意保持其与矢状面成角约15度,与横断面平行,再同理于腰5两侧打入定位针2枚,与矢状面成角约15度,C型臂透视进针地位偏向满足. 4.拔出定位针,依次经启齿.扩孔.触探孔壁后,分别按原偏向拧入椎弓根螺钉4枚,C型臂透视确认进钉地位深度满足.5.手术咬除腰4棘突及椎板,充分减压,显露硬膜松解双侧腰5神经根,切除腰4/5椎间盘.用刮匙刮除残留椎间盘和椎间盘周边高低终板,将咬除碎骨粒及合适大小椎间融会器置入腰4/5椎间隙.6.装配连杆,分别拧紧锁固螺母.C型臂透视确认椎体.椎间隙地位满足.用大量心理盐水反复冲洗瘦语.7.逐层缝合伤口,放置引流管1根,记载术中出血量.手术顺遂,患者安返病房.(五)术后处理术后均应放置引流条,防止积血,卧硬板床或围腰固定6~8周.五.药物治疗风寒痹阻型宜温经散寒,通络行痹,经常运用蠲痹汤加味内服;肾气亏虚者宜补气益肾,舒筋通络,药用芪仲腰舒丸.壮腰健肾丸.金匮肾气丸内服;气虚血瘀。
脊柱骨折临床诊疗指南

脊柱骨折临床诊疗指南第一节颈椎骨折【概述】有头部外伤痕迹者,应注意是否有颈椎损伤的可能。
颈椎骨折分类:按损伤节段(1)寰枢椎骨折脱位(2)寰椎爆裂性骨折(Jefferson骨折)(3)枢椎齿突骨折及伸展型骨折(Hangman骨折)(4)C3-C7椎体骨折按损伤部位(1)单纯椎体压缩性骨折(2)椎体压缩性骨折合并附件骨折、脱位(3)一侧或两侧小关节交锁导致颈椎脱位(4)无骨折脱位的颈脊髓损伤(挥鞭伤)按稳定程度(1)稳定性颈椎损伤①单纯椎体楔形压缩性骨折,椎体前缘压缩不超过1/3,后纵韧带无损伤。
②椎体前缘失脱骨折③单纯椎板骨折④单纯棘突骨折⑤无移位的侧块骨折⑥单纯横突骨折(2)不稳定性颈椎损伤①颈椎屈曲压缩型骨折②泪滴样骨折③颈椎前脱位④颈椎爆裂骨折⑤颈椎后脱位【临床表现】颈椎损伤后,头颈枕部疼痛,活动受限,损伤部位有压痛。
脊髓休克表现:损伤平面以下感觉消失,胸式呼吸消失;四肢迟缓性瘫痪,生理反射消失。
肢体感觉运动障碍:上颈髓(C1-C4):累及呼吸中枢,导致呼吸麻痹,同时因膈肌瘫痪造成呼吸困难。
不同程度的四肢痉挛性瘫痪。
可伴有心血管症状。
中颈髓(C5-C7):累及躯干部位感觉平面;下肢痉挛性瘫痪;上肢迟缓性瘫痪。
下颈髓(C8-T1):累及躯干部位感觉平面;下肢痉挛性瘫痪;上肢可见爪形手。
诊断:根据严重外伤史,临床表现和X线可以明确诊断。
X线正侧位片不仅可以显示骨折,并能判断骨折类型及移位情况,必要时应行脊髓造影、CT或MRI,以明确骨折、椎间盘突出及脊髓损伤。
注意评估患者的生命征和脊髓损伤情况。
【治疗原则和方案】1.现场急救2.支持治疗:首先对患者的生命征进行评估,积极抢救患者生命。
呼吸困难者,要保持患者呼吸道通畅,甚至机械通气。
待病情稳定后再处理脊椎骨折。
3.保守治疗:稳定性颈椎骨折脱位、压缩或移位较轻者,可行保守治疗。
常用方法包括:卧床休息、枕颌带卧床牵引复位、颅骨牵引、Halo头胸固定架牵引等。
脊柱外科诊疗操作规范

脊柱外科常用诊疗技术操作规范腹膜腔穿刺术【适应证】1.诊断性穿刺,以明确腹腔内有无积脓、积血,或抽液作化验和病理检查。
2.大量腹水引起严重胸闷、气短者,适量放液以缓解症状。
3.行人工气腹作为诊断和治疗手段。
4.腹腔内注射药物。
【禁忌证】1.严重肠胀气。
2.妊娠。
3.因既往手术或炎症腹腔内有广泛粘连者。
4.躁动、不能合作或肝昏迷先兆。
【操作】1.嘱患者排尿,以免刺伤膀胱。
2.取平卧位或斜卧位;如放腹水,背部先垫好腹带。
3.穿刺点的选择:(1)脐和髂前上棘间连线外1/3和中1/3的交点为穿刺点;放腹水时通常选用左侧穿刺点。
(2)脐和耻骨联合连线的中点上方1cm,偏左和右1~1.5cm处。
(3)若行诊断性腹腔灌洗术,在腹中线上取穿刺点。
4.常规消毒皮肤,术者带无菌手套,铺无菌孔巾,并用1%~2%普鲁卡因2ml作局麻,须深达腹膜。
5.作诊断性抽液时,可用17~18号长针头连接注射器,穿刺针垂直刺入皮下在皮下潜行后再垂直刺入腹腔;抽液后拔出穿刺针,揉压针孔,局部涂以碘酒,盖上无菌纱布,用胶布固定。
6.腹腔内积液不多,腹腔穿刺不成功,为明确诊断,可行诊断性腹腔灌洗,采用与诊断性腹腔穿刺相同的穿刺方法,把有侧孔的塑料管尾端连接一盛有500~1000ml无菌生理盐水的输液瓶,使生理盐水缓缓流入腹腔,当液体流完或病人感觉腹胀时,把瓶放正,转至床下,使腹内灌洗液借虹吸作用流回输液瓶中;灌洗后取瓶中液体作检验;拔出穿刺针,局部碘酒消毒后,盖无菌纱布,用胶布固定。
7.腹腔放液减压时,用胸腔穿刺的长针外连一长的消毒橡皮管,用血管钳夹住橡皮管,从穿刺点自下向上斜行徐徐刺入,进入腹腔后腹水自然流出,再接乳胶管放液于容器内;放液不宜过多、过快,一般每次不超过3000ml;放液完毕拔出穿刺针,用力按压局部,碘酒消毒后盖上无菌纱布,用胶布固定,缚紧腹带。
中心静脉压测量【适应证】1.测量中心静脉压。
2.利用其进行输液或静脉高营养(TPN)。
骨科前种疾病诊疗指南脊柱部分

骨科前20种疾病诊疗指南〔脊柱局部〕1、过伸性颈椎损伤2、腰椎间盘突出症3、腰椎椎管狭窄症4、颈椎病5、胸腰椎骨折X市人民医院脊柱外科202X年12月28日过伸性颈椎损伤[定义]颈椎过度伸展性暴力造成的颈脊髓损伤,常伴有轻微或隐匿的骨损伤,X 线多无异常表现,故易被疏漏,影响医治。
该损伤可占全颈椎各类损伤的29~50%,多见于中老年人,常伴脊髓中央管综合征。
[诊断]一、病症额面及鼻部擦伤和皮肤裂伤是最明显、多见的临床表现,系损伤时额面部或鼻部撞击物体或受到打击所致。
该特征常能提示颈椎损伤的外力作用机制,是推断颈椎过伸性损伤较有价值特征之一。
因神经系统损伤程度不一,临床表现轻重程度有很大差异。
二、体征局部压痛及活动机能受限。
损伤节段椎前压痛明显,而后结构压痛少见。
神经系统损伤多表现为脊髓中央综合征和前脊髓综合征,少数表现为局部和严峻脊髓损伤。
脊髓中央综合征典型表现为:上肢瘫痪重于下肢,手部重于臂部,触、痛觉损害重于深感觉。
严峻和局部脊髓损伤无明显的脊髓中央管损伤的特征。
三、特别检查:无。
四、辅助检查X线表现:颈椎过伸性损伤以软组织损伤为明显,骨性损伤小而隐匿,需认真观察,以免漏诊。
其主要X线征象有:(一) 伤椎体前下缘三角形撕脱骨折片,需与前纵韧带节段性骨化鉴别。
(二) 损伤节段颈椎间盘和椎前软组织影的变化。
颈椎椎前损伤出血或水肿时,造成损伤处椎前软组织影肿胀,椎间隙增宽。
(三)中老年患者常伴有颈椎退行性改变及椎管矢状径缩小,损伤多发生于C4~5、C5~6节段。
MR检查是必要的,可明确脊髓损伤程度和范围,以及脊髓受压的程度和致压物的X和性质。
[鉴别诊断]颈椎过伸性损伤易漏诊,诊断时应注意以下几点:一、详尽病史的采集,常能提供损伤机制;颅脑伤患者,也应设法了解损伤时姿态和暴力。
二、颅面部损伤均应常规摄颈椎X线片,以免因其他部位损伤而掩盖颈椎损伤。
三、侧位X线片必须清楚显示上下颈椎结构。
上颈椎损伤而神经病症表现低位时,需注意观察低.位颈椎有无变化。
脊柱系列——老年骨质疏松性胸腰椎骨折后脊柱重建临床指南(2022版)

脊柱系列——老年骨质疏松性胸腰椎骨折后脊柱重建临床指南(2022版)经皮椎体成形术 (PVP)、经皮椎体后凸成形术 (PKP)、后路固定术、后路固定联合伤椎强化术、前后联合固定术及后路截骨矫形术等是最主要的手术治疗方式,对老年急性(<6周)或陈旧性(>3个月)骨质疏松性胸腰椎骨折引起的脊柱形态异常或功能缺失,在快速缓解疼痛、恢复和维持脊柱形态和功能等方面疗效良好。
《老年骨质疏松性胸腰椎骨折后脊柱重建临床指南(2022版)》,针对老年骨质疏松性胸腰椎骨折治疗中最为重要的骨折分型、非手术治疗策略、手术治疗策略等10个方面的相关问题提出了基于循证医学证据的建议。
注:推荐强度分为3级,从1-3级依次递减。
推荐意见 1:对于老年骨质疏松性胸腰椎骨折的分型,推荐采用胸腰椎骨质疏松性骨折评估系统 (ASTLOF) 和骨质疏松性骨折分型系统 (OF分型)(推荐强度:3级)根据脊柱骨折进行合理分型是选择最佳治疗策略的基础,一直以来都是学界关注的焦点。
本指南中,骨质疏松诊断标准参考双能X线吸收测定法,T值≤-2.5 SD,或者定量CT法,骨密度≤80mg/cm3。
对老年骨质疏松性椎体骨折的分型,目前主要有以下两类。
(1) ASTLOF:2015年Xu等提出ASTLOF来评估骨质疏松性胸腰椎骨折的严重程度。
Du等提出基于该分型系统所推荐的治疗策略。
李庆达等将该分型系统应用于临床,获得良好的临床疗效。
该分型系统包括四个方面:① 形态学改变:正常为0分,压缩性骨折 (单凹改变/双凹改变/楔形改变) 为1分,爆裂性骨折 (累及中柱骨折) 为2分;② MRI检查:正常为0分,长T1、长T2信号改变为1分,椎体内真空现象或积液征为2 分;③骨密度:T值>-2.5 SD为0分,-3.5 SD<T值<-2.5 SD为1分,T值<-3.5 SD为2分;④临床表现:无明显疼痛为0分,腰背痛(体位改变诱发痛) 为1分,持续性疼痛/脊髓损伤为2分。
医院脊柱外科临床技术操作规范与手术失误防范处理手册

医院脊柱外科临床技术操作规范与手术失误防范处理手册者:李联忠(中国医科大学教授)出版社:中国医科大学出版社2005年7月出版册数规格:全三卷+1CD检索光盘16开精装定价:¥798元优惠价:¥350元内容如下第一编总论第一章绪论第二章脊柱外科应用解剖第三章脊柱生物力学第四章脊柱外科术前准备、术中及术后处理及护理第五章脊柱外科常用手术入路第六章脊柱牵引与固定第七章脊柱内固定概论第八章脊柱融合术概论第九章脊柱内固定器生物力学第二编脊柱外科临床检验及诊疗技术操作规范第一章影像诊断第二章诱发电位第三编脊柱损伤诊断及外科治疗临床技术操作规范第一章脊柱损伤概论第二章上颈椎损伤第三章下颈损伤第四章胸椎与腰椎损伤第五章经椎弓尾椎损伤第六章骶椎与尾椎损伤第七章脊柱附件损伤第八章脊柱开放性损伤第九章脊柱和骨髓损伤第四编脊柱感染与肿瘤诊断与治疗技术操作规范第一章脊柱结核概论第二章脊柱结合手术治疗第三章化脓性脊椎炎第四章脊柱肿瘤概论第五章脊柱肿瘤手术治疗第六章脊柱退变与相关疾患第七章颈椎退变性疾患第八章颈椎前路手术第九章颈椎前路手术内固定手术第十章腰椎间盘突出症第十一章腰椎退变性疾患第十二章腰骶部脊柱发育异常第十三章椎弓不连和脊柱滑脱症第十四章骨质疏松症与处科处理第五编人工椎间盘置换术第六编人工髓核置换第七编脊柱畸形诊断与治疗技术操作规范第一章脊柱畸形矫正术概论第二章颈部畸形第三章脊柱后凸畸形第四章脊柱侧凸第五章先天性脊柱侧凸第六章成年人脊柱侧凸第七章全脊截骨束矫正脊柱弯曲第八章脊柱侧凸的补救性手术第九章骨移植治疗脊柱不稳定第八编脊柱内固定治疗稳定第一章颈椎内固定治疗方法第二章胸腰椎内固定治疗方法第三章骶椎内固定治疗方法第四章Harring ton 与Luguen内固定治疗方法第五章CD脊柱内固定系统第六章Tsrh脊柱内固定系统第七章CD Horizon脊柱固定治疗方法第八章节MCSS—Mizni脊柱固定治疗方法第九章ISOLA脊柱固定治疗方法第十章RF和AF脊柱固定治疗方法第九编脊柱外科手术失误防范与并发症临床处理第一章颈椎骨折和脊髓损伤第二章颈椎手术的损伤晚期第三章胸椎及胸腰椎手术并发症第四章脊柱内固定术第五章椎板切除后硬膜周围粘加机制及预防第十编相关法律法规。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
脊柱脊髓损伤定义:脊柱脊髓损伤常发发生于工矿,交通事故,战时和自然灾害时可成批发生。
伤情严重复杂,多发伤、复合伤较多,并发症多,合并脊髓伤时预后差,甚至造成终生残废或危及生命。
症状体征一,脊柱骨折1,有严重外伤史,如高空落下,重物打击头颈或肩背部,塌方事故,交通事故等。
2,病人感受伤局部疼痛,颈部活动障碍,腰背部肌肉痉挛,不能翻身起立,骨折局部可扪及局限性后突畸形。
3,由于腹膜后血肿对植物神经刺激,肠蠕动减慢,常出现腹胀,腹痛等症状,有时需与腹腔脏器损伤相鉴别。
二,合并脊髓和神经根损伤脊髓损伤后,在损伤平面以下的运动,感觉,反射及括约肌和植物神经功能受到损害。
1,感觉障碍损伤平面以下的痛觉,温度觉,触觉及本体觉减弱或消失。
2,运动障碍脊髓休克期,脊髓损伤节段以下表现为软瘫,反射消失,休克期过后若是脊髓横断伤则出现上运动神经元性瘫痪,肌张力增高,腱反射亢进,出现髌阵挛和踝阵挛及病理反射。
3,括约肌功能障碍脊髓休克期表现为尿潴留,系膀胱逼尿肌麻痹形成无张力性膀胱所致,休克期过后,若脊髓损伤在骶髓平面以上,可形成自动反射膀胱,残余尿少于100ml,但不能随意排尿,若脊髓损伤平面在圆锥部骶髓或骶神经根损伤,则出现尿失禁,膀胱的排空需通过增加腹压(用手挤压腹部)或用导尿管来排空尿液,大便也同样出现便秘和失禁。
4,不完全性脊髓损伤损伤平面远侧脊髓运动或感觉仍有部分保存时称之为不完全性脊髓损伤,临床上有以下几型:(1)脊髓前部损伤:表现为损伤平面以下的自主运动和痛觉消失,由于脊髓后柱无损伤,病人的触觉、位置觉、振动觉、运动觉和深压觉完好。
(2)脊髓中央性损伤:在颈髓损伤时多见,表现上肢运动丧失,但下肢运动功能存在或上肢运动功能丧失明显比下肢严重,损伤平面的腱反射消失而损伤平面以下的腱反射亢进。
(3)脊髓半侧损伤综合症(Brown-Sequards Symdrome):表现损伤平面以下的对侧痛温觉消失,同侧的运动功能,位置觉,运动觉和两点辨觉丧失。
(4)脊髓后部损伤:表现损伤平面以下的深感觉,深压觉,位置觉丧失,而痛温觉和运动功能完全正常,多见于椎板骨折伤员。
检查方法本病的辅助检查方法有以下几种:1. X线检查常规摄脊柱正侧位,必要时照斜位,阅片时测量椎体前部和后部的高度与上下邻椎相比较;测量椎弓根间距和椎体宽度;测量棘突间距及椎间盘间隙宽度并与上下邻近椎间隙相比较,测量正侧位上椎弓根高度,X片基本可确定骨折部位及类型。
2. CT检查有利于判定移位骨折块侵犯椎管程度和发现突入椎管的骨块或椎间盘。
3. MRI(磁共振)检查对判定脊髓损伤状况极有价值,MRI可显示脊髓损伤早期的水肿,出血,并可显示脊髓损伤的各种病理变化,脊髓受压,脊髓横断,脊髓不完全性损伤,脊髓萎缩或囊性变等。
4. SEP(体感诱发电位) 是测定躯体感觉系统(以脊髓后索为主)的传导功能的检测法,对判定脊髓损伤程度有一定帮助,现在已有MEP(运动诱导电位)。
本病的治疗有包括以下几点:(一)急救和搬运1. 脊柱脊髓伤有时合并严重的颅脑损伤、胸部或腹部脏器损伤、四肢血管伤,危及伤员生命安全时应首先抢救。
2. 凡疑有脊柱骨折者,应使病人脊柱保持正常生理曲线。
切忌使脊柱作过伸、过屈的搬运动作,应使脊柱在无旋转外力的情况下,三人用手同时平抬平放至木板上,人少时可用滚动法。
对颈椎损伤的病人,要有专人扶托下颌和枕骨,沿纵轴略加牵引力,使颈部保持中立位,病人置木板上后用砂袋或折好的衣物放在头颈的两侧,防止头部转动,并保持呼吸道通畅。
(二)单纯脊柱骨折的治疗1. 胸腰段骨折轻度椎体压缩属于稳定型。
患者可平卧硬板床,腰部垫高。
数日后即可背伸肌锻炼。
经功能疗法可使压缩椎体自行复位,恢复原状。
3~4周后即可在胸背支架保护下下床活动。
2. 胸腰段重度压缩超过三分之一应予以闭合复位。
可用两桌法过伸复位。
用两张高度相差30cm左右的桌子,桌上各放一软枕,伤员俯卧,头部置于高桌上,两手把住桌边,两大腿放于低桌上,要使胸骨柄和耻骨联合部悬空,利用悬垂的体重逐渐复位。
复位后在此位置上石膏背心固定。
固定时间为3个月。
3. 胸腰段不稳定型脊柱骨折椎体压缩超过1/3以上、畸形角大于20°、或伴有脱位可考虑开放复位内固定。
4. 颈椎骨折或脱位压缩移位轻者,用颌枕带牵引复位,牵引重量3 ~ 5kg。
复位后用头胸石膏固定3个月。
压缩移位重者,可持续颅骨牵引复位。
牵引重量可增加到6 ~ 10kg。
摄X线片复查,复位后用头胸石膏或头胸支架固定3个月,牵引复位失败者需切开复位内固定。
(三)脊柱骨折合并脊髓损伤脊髓损伤的功能恢复主要取决于脊髓损伤程度,但及早解除对脊髓的压迫是保证脊髓功能恢复的首要问题。
手术治疗是对脊髓损伤患者全面康复治疗的重要部分。
手术目的是恢复脊柱正常轴线,恢复椎管内径,直接或间接地解除骨折块或脱位对脊髓神经根的压迫,稳定脊柱(通过内固定加植骨融合)。
其手术方法有:1.颈椎前路减压植骨融合术对颈3以下的颈椎骨折可行牵引复位,前路减压或次全椎体切除、植骨融合术,用钢板螺钉内固定或颈围外固定。
明显不稳者可继续颅骨牵引或头胸石膏固定。
2.颈椎后路手术脱位为主者牵引复位后可行后路金属夹内固定及植骨融合术或用钢丝棘突内固定植骨融合,必要时行后路减压钢板螺钉内固定植骨融合术。
3.胸腰段骨折前路手术对胸腰段椎体爆裂性或粉碎性骨折,多行前路减压、植骨融合、钢板螺钉内固定术。
对陈旧性骨折可行侧前方减压术。
4.胸腰段骨折后路手术后路手术包括椎板切除减压、用椎弓根螺定钢板或钢棒复位内固定,必要时行植骨融合术也可用哈灵顿棒或鲁凯棒钢丝内固定。
(四)综合症法1.脱水疗法应用20%甘露醇250ml;2次/d,目的是减轻脊髓水肿。
2. 激素治疗应用地塞米松10 ~ 20mg静脉滴注,一次/d。
对缓解脊髓的创伤性反应有一定意义。
3. 一些自由基清除剂如维生素E、A、C及辅酶Q等,钙通道阻滞剂,利多卡因等的应用被认为对防止脊髓损伤后的继发损害有一定好处。
4. 促进神经功能恢复的药物如三磷酸胞苷二钠、维生素B1、B6、B12等。
支持疗法注意维持伤员的水和电解质平衡,热量、营养和维生素的补充。
骨质疏松性骨折骨质疏松性骨折是中老年最常见的骨骼疾病,也是骨质疏松症的严重阶段,具有发病率高、致残致死率高、医疗花费高的特点。
而我国骨质疏松性骨折的诊疗现状是诊断率低、治疗率低、治疗依从性和规范性低。
一、定义(一)骨质疏松性骨折为低能量或非暴力骨折,指在日常生活中未受到明显外力或受到“通常不会引起骨折外力”而发生的骨折,亦称脆性骨折(“通常不会引起骨折外力”指人体从站立高度或低于站立高度跌倒产生的作用力。
骨质疏松性骨折与创伤性骨折不同,是基于全身骨质疏松存在的一个局部骨组织病变,是骨强度下降的明确体现,也是骨质疏松症的最终结果(二)骨质疏松症(osteoporosis,OP)以骨强度下降、骨折风险增加为特征的骨骼系统疾病。
骨强度反映骨骼的两个主要方面,即骨密度和骨质量。
骨质疏松症分为原发性和继发性两大类。
二、骨质疏松性骨折具有以下特点:①骨折患者卧床制动后,将发生快速骨丢失,会加重骨质疏松症;②骨重建异常、骨折愈合过程缓慢,恢复时间长,易发生骨折延迟愈合甚至不愈合;③同一部位及其他部位发生再骨折的风险明显增大;④骨折部位骨量低,骨质量差,且多为粉碎性骨折,复位困难,不易达到满意效果;⑤内固定治疗稳定性差,内固定物及植入物易松动、脱出,植骨易被吸收;⑥多见于老年人群,常合并其他器官或系统疾病,全身状况差,治疗时易发生并发症,增加治疗的复杂性。
骨质疏松性骨折多见于老年人群,尤其是绝经后女性。
发生的常见部位有:胸腰段椎体、髋部(股骨近端)、腕部(桡骨远端)、肱骨近端等;发生了脆性骨折临床上即可诊断骨质疏松症三、骨质疏松性骨折的诊断:(一)临床表现可有疼痛、肿胀和功能障碍,可出现畸形、骨擦感(音)、反常活动;但也有患者缺乏上述典型表现。
具有骨质疏松症的一般表现。
(二)影像学检查1.X线:可确定骨折的部位、类型、移位方向和程度,对骨折诊断和治疗具有重要价值。
X线片除具有骨折的表现外,还有骨质疏松的表现。
2.CT:常用于判断骨折的程度和粉碎情况、椎体压缩程度、椎体周壁是否完整、椎管内的压迫情况。
3.MRI:常用于判断椎体压缩骨折是否愈合、疼痛责任椎及发现隐匿性骨折,并进行鉴别诊断等。
4.全身骨扫描(ECT):适用于无法行MR检查或排除肿瘤骨转移等。
(三)行骨密度检查。
双能X线吸收法测量值是世界卫生组织推荐的骨质疏松症评估方法,是公认的骨质疏松诊断的金标准。
参照WHO推荐的诊断标准,DXA测定骨密度值低于同性别、同种族健康成人的骨峰值不足1个标准差为正常(T值≥-1.0SD);降低1~2.5个标准差为骨量低下或骨量减少(-2.5SD<T值<-1.0SD);降低程度等于或大于2.5个标准差为骨质疏松(T值≤-2.5SD);降低程度符合骨质疏松诊断标准,同时伴有一处或多处骨折为严重骨质疏松。
(四)实验室检查在诊断原发性骨质疏松性骨折时,应排除转移性骨肿瘤、胸腰椎结核、多发性骨髓瘤、甲状旁腺功能亢进等内分泌疾病、类风湿关节炎等免疫性疾病、长期服用糖皮质激素或其他影响骨代谢药物以及各种先天或获得性骨代谢异常疾病。
1.基本检查项目:血尿常规,肝肾功能,血钙、磷、碱性磷酸酶等。
2.选择性检查项目:红细胞沉降率、性腺激素、血清25羟基维生素D (25hydroxyvitaminD,25OHD)、1,25(OH)2D、甲状旁腺激素、24h尿钙和磷、甲状腺功能、皮质醇、血气分析、血尿轻链、肿瘤标志物、放射性核素骨扫描、骨髓穿刺或骨活检等。
3.骨转换生化标志物:IOF推荐Ⅰ型骨胶原氨基末端肽(P1NP)和Ⅰ型胶原羧基末端肽(S⁃CTX),有条件的单位可检测。
(五)诊疗原则及流程骨质疏松性骨折的诊断应结合患者的年龄、性别、绝经史、脆性骨折史、临床表现及影像学和(或)骨密度检查结果进行综合分析,作出诊断。
四、骨质疏松性骨折的治疗原则复位、固定、功能锻炼和抗骨质疏松治疗是治疗骨质疏松性骨折的基本原则。
骨质疏松性骨折的治疗应强调个体化,可采用非手术或手术治疗。
2.治疗(1)非手术治疗适用于症状和体征较轻,影像学检查显示为轻度椎体压缩骨折,或不能耐受手术者。
治疗可采用卧床、支具及药物等方法,但需要定期进行X线片检查,以了解椎体压缩是否进行性加重。
(2)手术治疗椎体强化手术,包括椎体成形术(PVP)和椎体后凸成形术(PKP),是目前最常用的微创手术治疗方法[25-36],适用于非手术治疗无效,疼痛剧烈;不稳定的椎体压缩性骨折;椎体骨折不愈合或椎体内部囊性变、椎体坏死;不宜长时间卧床;能耐受手术者。