肝癌肝移植的米兰外标准
肝移植标准
肝移植标准
肝移植是一项高风险的手术,一般只适用于以下患者:
1.晚期肝病患者:指肝功能逐渐恶化,已无法通过其他治疗手段控制或治愈的肝病患者。
2.急性肝功能衰竭患者:指肝功能在短时间内发生急性衰竭,出现昏迷和其他严重并发症的患者。
3.原发性肝癌患者:指肝癌仅局限于肝脏,无法通过手术或其他治疗手段控制或治愈的患者。
4.其他严重肝脏疾病患者:如Wilson病、α1-抗胰蛋白酶缺陷等。
除了病情符合上述标准之外,还需要满足以下几个条件:
1.患者年龄在18岁以上,没有重大的其他疾病。
2.患者在肝移植前必须停止饮酒和吸烟。
3.患者必须找到与自己血型相符合的捐赠者,并进行匹配。
4.患者和捐赠者必须经过全面的身体和心理检查,并签署手术同意书。
总之,在选择是否进行肝移植手术时,需考虑患者的病情、年龄、身体状况、家庭支持等多种因素,以及手术风险和后遗症。
医生和患者应共同探讨,制定最合适的治疗方案。
肝移植米兰标准

肝移植米兰标准肝移植是一种治疗肝功能衰竭或肝病晚期的重要手术方式,而米兰标准则是肝移植手术中的重要指南之一。
米兰标准是指1996年在意大利米兰召开的国际肝移植协会会议上提出的,它对于确定肝癌患者是否适合接受肝移植具有重要意义。
根据米兰标准,肝癌患者需要符合以下条件,单个肿瘤直径不超过5cm,或者有多个肿瘤但最大的肿瘤直径不超过3cm,并且没有血管侵犯或淋巴结转移。
米兰标准的提出,旨在规范肝移植手术的适应症,避免因为手术适应症的宽松而导致肝癌患者过度接受肝移植手术,从而浪费有限的器官资源。
同时,也为肝癌患者提供了更为公平的肝移植机会,使得那些符合条件的患者能够及时接受到必要的治疗。
在肝移植手术中,严格遵循米兰标准是非常重要的。
因为符合米兰标准的肝癌患者,其肿瘤生长缓慢,转移率低,手术切除后的生存率也相对较高。
而对于不符合米兰标准的肝癌患者,即使进行了肝移植手术,也很容易出现肿瘤复发和转移的情况,影响手术效果和患者生存率。
除了符合米兰标准外,肝移植手术的成功还需要患者的身体状况良好,手术团队的专业水平高超,手术后的护理和康复工作得到充分重视。
只有在这些条件齐备的情况下,肝移植手术才能取得良好的效果,使患者重获新生。
总之,肝移植米兰标准作为肝癌患者接受肝移植手术的重要指南,对于规范手术适应症,提高手术效果,保障患者生存率具有重要意义。
在今后的临床实践中,我们需要严格遵循米兰标准,合理利用有限的器官资源,为更多的肝癌患者提供及时有效的治疗,让他们重获新生。
同时,也需要不断提高手术技术水平,完善术后护理和康复工作,为肝移植手术的成功提供全方位的保障。
希望通过我们的努力,能够让更多的肝癌患者受益,重拾健康,重新享受生活。
up-to-7标准
up-to-7标准研究目的及背景:肝细胞癌(Hepatocellular Carcinoma,HCC,以下简称肝癌)是最常见的消化道恶性肿瘤之一,在所有恶性肿瘤中其发病率及死亡率分别位居第5位和第3位,由于早期缺乏特异性症状体征,多数患者一旦诊断已属晚期,预后极差。
据报道统计显示我国肝癌的发病人数就已经占了全球肝癌新发病例的一半以上,严重的威胁着国民的生命健康。
目前肝癌的治疗方式仍然以手术切除局部病灶为主,术前或术后辅以肝动脉化疗栓塞术或放疗,对于无法行手术治疗的患者可行单纯的放疗或口服靶向药物索拉非尼,这些治疗方式患者收益较小,主要原因之一即是肝癌极易复发、转移,随着医学的发展,肝移植在治疗肝癌的应用中越来越广泛,肝癌被认为是行肝移植的主要适应症之一。
经过近几十年的探索,对肝癌肝移植术后的疗效进行分析,目前公认的肝癌肝移植标准有Up-to-seven标准,UCSF标准、Milan标准、上海复旦标准,对于符合标准的肝癌移植患者预后明显优于不符合标准的患者,因此,目前通常在术前进行评估,优先对符合标准的患者进行肝移植。
在以往的研究中,对肝癌患者接受肝移植前用以上标准可进行评估预后,而对于影响符合以上标准的肝移植患者的研究较少。
Milan标准的应用使移植术后5年生存率达到70%,5年复发率低于15%。
而近年来有部分符合以上标准的病人在随访过程中发现肿瘤复发,部分患者肿瘤体积较小,且无明确的大血管侵犯,为我们的临床研究带来了新的方向。
研究方法:收集251例符合Up7标准接受肝移植的患者作为研究对象,通过对基本临床信息的分析,建立了基于Up7标准肝癌肝移植长期生存的预测模型(ATMD),同时根据UCSF标准、Milan标准、上海复旦标准进行验证,发现此模型对于各标准的患者的生存预后同样具有较好的预测效能,并将此模型在不同肝移植标准中进行验证,检验其预测效能。
研究结果:经过多因素COX 回归分析发现术前甲胎蛋白(AFP),术前总胆红素(t-Bil),微血管侵犯(MVI),肿瘤直径(Diameter)是肝移植患者长期生存的独立预测因素,建立ATMD模型,并界定高/低危组。
米兰标准肝癌消融标准

米兰标准肝癌消融标准1. 介绍肝癌是一种常见的恶性肿瘤,消融治疗是其中一种常用的治疗方法。
米兰标准肝癌消融标准是一套用于评估肝癌消融治疗效果的标准,旨在提供一个统一的评估体系,帮助医生更准确地评估治疗效果,制定个体化的治疗方案。
2. 米兰标准肝癌消融标准的背景肝癌是全球范围内的常见恶性肿瘤,其治疗方法包括手术切除、肝移植、化疗和消融治疗等。
消融治疗是一种以热或冷凝固的方式破坏肿瘤细胞的方法,可用于治疗早期肝癌、局部进展的肝癌和转移性肝癌。
然而,肝癌消融治疗的效果评估一直是一个难题。
传统的评估方法主要依靠影像学检查,如CT和MRI,但这些方法无法准确评估消融区域内肿瘤细胞的死亡情况。
因此,需要一个更准确、可重复性好的评估标准来指导临床实践。
3. 米兰标准肝癌消融标准的内容米兰标准肝癌消融标准是由国际消融学会(International Radiofrequency Ablation Study Group)制定的。
该标准主要包括以下几个方面:3.1 消融区域评估消融区域评估是评估消融治疗效果的关键步骤。
根据米兰标准,消融区域应该呈现为一个完整的椭圆形或椭球形,且边界清晰。
消融区域的直径和体积也是评估的重要指标。
3.2 残留肿瘤评估残留肿瘤是指在消融治疗后仍然存在的肿瘤组织。
根据米兰标准,残留肿瘤的直径和体积应该被准确测量,并与消融区域进行比较。
如果残留肿瘤的直径超过消融区域的30%,则被认为治疗效果不佳。
3.3 边缘增强区评估边缘增强区是指消融区域周围的一圈增强区域,可能是由于周围的肿瘤细胞未被完全消融所致。
根据米兰标准,边缘增强区的直径和体积也应该被准确测量,并与消融区域进行比较。
3.4 术后复发评估术后复发是指消融治疗后肿瘤再次出现的情况。
根据米兰标准,术后复发应该被准确记录,并评估复发的数量、位置和大小。
这些信息对于制定进一步治疗方案非常重要。
4. 米兰标准肝癌消融标准的应用米兰标准肝癌消融标准可以帮助医生更准确地评估肝癌消融治疗的效果,并制定个体化的治疗方案。
符合米兰标准的肝移植十年生存率

符合米兰标准的肝移植十年生存率全文共四篇示例,供读者参考第一篇示例:肝移植是目前治疗绝症肝病的最有效方法之一。
在肝脏疾病晚期,患者可能需要进行肝脏移植手术来拯救生命。
米兰标准是目前国际上用于评估肝脏肿瘤的标准之一,其制定的目的是筛选出适合接受肝移植治疗的患者,提高移植手术的成功率和患者的存活率。
米兰标准最早于1996年由意大利米兰大学医院提出,用于评估原发性肝癌(HCC)患者的肿瘤大小和数量。
根据米兰标准,适合进行肝移植手术的患者应符合以下标准:单个肿瘤直径不超过5厘米,或者最多三个独立肿瘤,每个肿瘤直径不超过3厘米,无血管侵犯和外部转移。
符合这一标准的患者通常具有较高的手术成功率和长期存活率。
十年的生存率是评估肝移植手术效果的重要指标之一。
根据研究数据显示,符合米兰标准的肝移植患者具有较高的十年生存率。
研究表明,符合米兰标准的患者在施行肝移植手术后十年存活率高达70%以上,远高于不符合标准的患者。
米兰标准的制定为肝移植手术的选择和治疗提供了重要的参考依据。
通过对患者的肿瘤大小和数量进行评估,可以有效地筛选出适合肝移植手术的患者,提高手术的成功率和患者的生存率。
米兰标准的应用也促进了医学研究的进展,为肝移植手术的临床实践提供了可靠的指导。
除了符合米兰标准外,患者的身体状况、手术前后的护理和恢复等因素也对肝移植手术的成功和生存率起着重要作用。
患者在手术后需要严格遵守医嘱,加强身体锻炼,保持良好的饮食习惯,定期复查和随访,以确保手术的效果和生存率。
符合米兰标准的肝移植患者具有较高的十年生存率,这为患者提供了新的生机和希望。
在接受肝移植手术前,患者应该积极配合医生的检查和治疗,全面评估自身的身体状况和手术风险,选择合适的治疗方案,以达到最佳的治疗效果和生存率。
希望未来科学技术的发展能够进一步提高肝移植手术的成功率和患者的生存率,为肝脏疾病患者带来更多的希望和福音。
【此文共计730字】接下来,我们将继续探讨肝移植手术的成功因素、并发症及术后护理等内容,以全面了解符合米兰标准的肝移植患者的十年生存率。
肝癌肝移植的标准
肝癌肝移植的标准
肝癌肝移植的标准并没有统一,以下是一些不同标准的介绍:
1. 米兰标准:要求单一癌灶直径不>5cm,或者多发癌灶数目不多于3个,而且最大的直径不能>3cm,肿瘤没有肝内大血管侵犯及远处转移。
2. 杭州标准:分为A、B、C三类。
A类指肿瘤直径≤8cm,或者肿瘤直径>8cm,但甲胎蛋白≤100μg/mL;B类为肿瘤直径>8cm,甲胎蛋白在100-400μg/mL。
3. 上海复旦标准:只要肿瘤直径不超过9厘米就可以实施肝脏移植。
经证实,符合“上海复旦标准”的肝移植病人术后的三年生存率达80%左右,由此,肝移植适应证人群扩大了40%左右。
请注意,肝癌肝移植是一个非常复杂的过程,需要综合评估患者的病情、身体状况、器官匹配程度等多种因素。
如果您或身边的人面临此类情况,建议尽早咨询专业医生或器官移植专家,获取最准确和合适的信息和建议。
肝癌肝移植的常用标准
肝癌肝移植的常用标准
肝癌肝移植的常用标准通常包括米兰标准、UCSF 标准和杭州标准等,以下是这些标准的简要介绍:
1. 米兰标准:这是最早也是应用最广泛的肝癌肝移植标准。
该标准要求单发肿瘤直径不超过5 厘米,或多发肿瘤数目不超过 3 个,且最大直径不超过3 厘米。
米兰标准的目的是选择肿瘤负荷较小、复发风险较低的患者进行肝移植,以提高手术的疗效和生存率。
2. UCSF 标准:该标准在米兰标准的基础上进行了扩展,将单发肿瘤直径上限放宽至6.5 厘米,或多发肿瘤数目放宽至4 个,且最大直径不超过4.5 厘米。
UCSF 标准的目的是扩大肝移植的适用范围,使更多的肝癌患者有机会接受肝移植。
3. 杭州标准:该标准是在中国提出的,适用于肝功能Child-Pugh A 级或B 级的肝癌患者。
杭州标准将单发肿瘤直径上限放宽至8 厘米,或多发肿瘤数目放宽至3 个,且最大直径不超过5 厘米,同时要求肿瘤无大血管侵犯和肝外转移。
需要注意的是,这些标准只是肝移植的筛选标准,实际的肝移植决策还需要综合考虑患者的肝功能、肿瘤分期、身体状况等因素。
此外,
随着对肝癌生物学行为的认识不断深入,肝移植的标准也在不断更新和完善。
MELD评分系统 肝移植病人术前评分或分级

●2002年美国器官共享网/全美器官获取和移植网
(Organ Procurement and Transplantation Network, OPTN)
R=0.378×log(胆红素μmol/L×0.058)+1.12×log(INR)+ 0.957×log(肌酐μmol/L×0.011)+0.643
患者评分0~40相当90%~7%的三个月生存率 R值越高,其风险越大,生存率越低。 △ R(30d内积分的差值)>0表明疾病在进展, ≤0表明疾病处于相对平稳期或在好转
●Mayo 医院 Dr.Kamath 改良公式:
R=3.8ln[胆红素(mg/dl)]+11.2ln(INR)+9.6ln [肌酐 (mg/dl)]+6.4*(病因:胆汁性或酒精性0,其他1)
ISI 由试剂商提供!
MELD的应用
在非移植患者预测肝病死亡率中的应用
对终末期肝病患者在TIPS中的良好预测能力 终末期肝病生存率的预测是有效
在肝移植中的应用
MELD可有效评价移植前患者等待供肝期间的死亡 率及预测患者移植术后的死亡率
在重型肝炎及人工肝中的应用
MELD评分具有下列优点:
2000年Malinchoc等首先应用MELD来预测终末期肝病 行经颈静脉肝内门-体分流术后的死亡率,并证实 MELD 可以预测终末期肝378ln[胆红素(mg/dl)]+1.12ln(INR)+0.95ln[肌酐(mg/dl)] +0.64(病因:胆汁性或酒精性0,其他1)。
临床诊疗规范|原发性肝癌诊疗规范(2019年完整版)

临床诊疗规范|原发性肝癌诊疗规范(2019年完整版)1、概述原发性肝癌是目前我国第4位常见恶性肿瘤及第2位肿瘤致死病因,严重威胁我国人民的生命和健康[1-2]。
原发性肝癌主要包括肝细胞癌(hepatocellular carcinoma,HCC)、肝内胆管癌(intrahepatic cholangiocarcinoma,ICC)和HCC-ICC混合型3种不同病理学类型,3者在发病机制、生物学行为、组织学形态、治疗方法以及预后等方面差异较大,其中HCC占85%~90%。
因此,本规范中的“肝癌”指HCC。
为进一步规范我国肝癌诊疗行为,原中华人民共和国卫生和计划生育委员会医政医管局于2017年6月主持制定和颁布了《原发性肝癌诊疗规范(2017年版)》。
该规范的颁布反映了当时我国肝癌诊断和多学科综合治疗以及研究的状况,对规范肝癌诊疗的临床行为、改善肝癌病人预后、保障医疗质量和医疗安全以及优化医疗资源发挥了重要作用。
自2017年至今,在肝癌的诊断、分期及治疗方面国内外新出现了许多符合循证医学原则的高级别证据,尤其是适应中国国情的研究成果。
为此,中华人民共和国国家卫生健康委员会医政医管局委托中华医学会肿瘤学分会组织全国肝癌领域的多学科专家,结合目前肝癌临床研究的实际,修订并更新形成《原发性肝癌诊疗规范(2019年版)》(以下简称规范)。
本规范参照的循证医学证据等级按照《牛津循证医学中心2011版》进行分级(附录1)。
2 筛查和诊断2.1 肝癌高危人群的监测筛查对肝癌高危人群的筛查有助于肝癌的早期发现、早期诊断、早期治疗,是提高肝癌疗效的关键。
在我国,肝癌高危人群主要包括:具有乙型肝炎病毒(hepatitis B virus,HBV)和(或)丙型肝炎病毒(hepatitis C virus,HCV)感染、过度饮酒、非酒精性脂肪性肝炎、长期食用被黄曲霉毒素污染的食物、各种其他原因引起的肝硬化以及有肝癌家族史等人群,尤其是年龄>40岁的男性风险更大。
符合米兰标准肝移植存活率

符合米兰标准肝移植存活率
肝移植是一种非常复杂的手术过程,需要高度专业技能和设备。
在手术完成后,肝脏移植的成功与否很大程度上取决于肝脏康复情况和适当的后续治疗。
在过去的几十年中,肝移植的技术和方法不断发展,许多技术和方法被应用在肝移植手术中,这些方法的改进和使用显著提高了移植的成功率。
在这个过程中,米兰标准助于提高肝移植的存活率。
米兰标准在肝移植领域被广泛使用。
该标准是一个肝癌评估系统,用于确定哪些肝移植患者最适合接受肝脏移植。
标准建议将肝移植限制在特定的人群中,这些人可能在手术后有更好的机会成功。
这些标准主要用于肝癌患者,因为这些患者需要特定的护理和后续治疗。
在实践中,米兰标准已被广泛采纳,并显示出肝移植存活率得到了显著提高。
据统计,在使用米兰标准后,肝癌患者的肝移植手术成功率和存活率都有了大幅提高。
这是因为米兰标准要求对肝脏状况进行更加深入的审查和评估,以确保选择的肝脏在患者身体中最好地工作。
在肝脏移植过程中,使用更先进的技术和手术方法也有助于提高成功率。
为了
确保肝脏移植手术的成功,患者在手术前需要接受基本的肝脏功能测
量和其他检查,以确定他们是否合格进行手术。
总的来说,米兰标准帮助提高了肝移植手术的存活率。
在实践中,这
些标准已被广泛采用,并且已被全球肝脏医学界普遍认可。
尽管有一
些潜在的挑战,但这些挑战通常可以通过更新和完善的技术处理并且
不影响标准的有效性。
最后,肝移植在医疗科技领域始终保持着十分
重要的地位,并且随着技术的不断改进,肝移植的成功率将继续提高,并为肝癌患者带来更多机会。
肝脏移植技术医疗质量控制指标(2020年版)
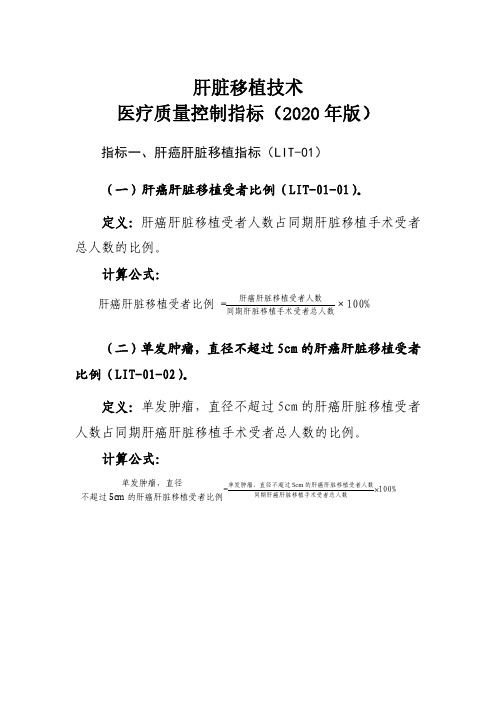
定义:肝脏移植手术后发生 EAD 的手术人数占同期肝脏 移植手术总人数的比例。
计算公式:
术后 EAD 发生率=
发生 EAD 的手术人数 ×100%
同期肝脏移植手术总人数
说明:符合下列一个或多个标准的病例视为发生 EAD:
(1)术后第 7 天总胆红素(TB)≥171 umol/L(10mg/dL)。
(2)术后第 7 天国际标准化比值(INR)≥1.6(应用 抗凝药物原因除外)。
定义:肝脏移植某一时间(1 年、3 年、5 年)随访尚存
活的受者人数占同期肝脏移植手术受者总人数的比例。
计算公式:
1.良性肝病肝脏移植受者术后生存率(LIT-04-02A)。
肝脏移植手术后某一时间随访尚存活的
良性肝病肝脏移植受者术后生存率=
良性肝病受者人数
×100%
同期良性肝病肝脏移植手术受者总人数
2.肝癌肝脏移植受者术后生存率(LIT-04-02B)。
肝脏移植手术后某一时间随访尚存活的
肝癌肝脏移植受者术后生存率=
肝癌肝脏移植受者人数
×100%
同期肝癌肝脏移植手术受者总人数
(三)肝癌肝脏移植受者术后无瘤生存率(1 年、3 年、 5 年)(LIT-04-03)。
定义:肝癌肝脏移植某一时间(1 年、3 年、5 年)无瘤
存活的受者人数占同期肝癌肝脏移植手术受者总人数的比
例。
计算公式:
肝癌肝脏移植受者移植后某一时间
肝癌肝脏移植受者术后无瘤生存率=
无瘤存活的受者人数
×100%
同期肝癌肝脏移植手术受者总人数
意义:反映肝脏移植的中远期疗效,与医疗机构手术技
术、术后医疗管理质量等情况密切相关,与同级医疗机构进
免疫治疗用于肝癌肝移植术前治疗的研究进展
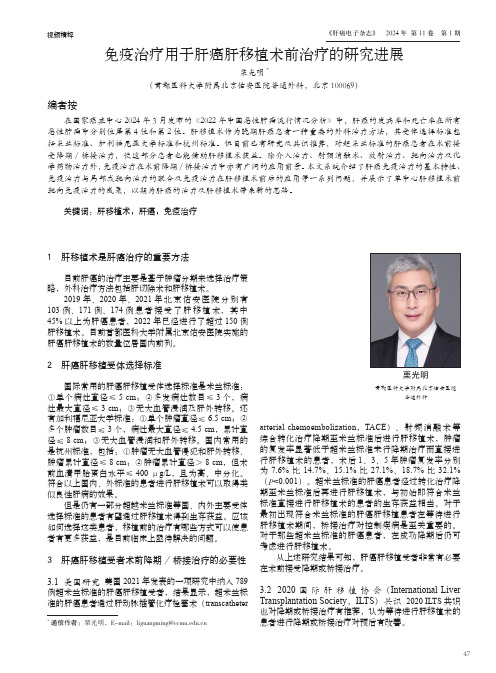
视频精粹471111 肝移植术是肝癌治疗的重要方法目前肝癌的治疗主要是基于肿瘤分期来选择治疗策略,外科治疗方法包括肝切除术和肝移植术。
2019年、2020年、2021年北京佑安医院分别有103例、171例、174例患者接受了肝移植术,其中45%以上为肝癌患者,2022年已经进行了超过150例肝移植术。
目前首都医科大学附属北京佑安医院实施的肝癌肝移植术的数量位居国内前列。
2 肝癌肝移植受体选择标准国际常用的肝癌肝移植受体选择标准是米兰标准:①单个病灶直径≤5 cm ;②多发病灶数目≤3个,病灶最大直径≤3 cm ;③无大血管浸润及肝外转移。
还有加利福尼亚大学标准:①单个肿瘤直径≤6.5 cm ;②多个肿瘤数目≤3个,病灶最大直径≤4.5 cm ,累计直径≤8 cm ;③无大血管浸润和肝外转移。
国内常用的是杭州标准,包括:①肿瘤无大血管侵犯和肝外转移、肿瘤累计直径≤8 cm ;②肿瘤累计直径>8 cm ,但术前血清甲胎蛋白水平≤400 μg/L ,且为高、中分化。
符合以上国内、外标准的患者进行肝移植术可以取得类似良性肝病的效果。
但是仍有一部分超越米兰标准等国、内外主要受体选择标准的患者有望通过肝移植术得到生存获益。
应该如何选择这类患者,移植前的治疗有哪些方式可以使患者有更多获益,是目前临床上亟待解决的问题。
3 肝癌肝移植受者术前降期/桥接治疗的必要性3.1 美国研究 美国2021年发表的一项研究中纳入789例超米兰标准的肝癌肝移植受者,结果显示,超米兰标准的肝癌患者通过肝动脉插管化疗栓塞术(transcatheterarterial chemoembolization ,TACE )、射频消融术等综合转化治疗降期至米兰标准后进行肝移植术,肿瘤的复发率显著低于超米兰标准未行降期治疗而直接进行肝移植术的患者,术后1、3、5年肿瘤复发率分别为7.6%比14.7%、15.1%比27.1%、18.7%比32.1%(P <0.001)。
肝移植常见标准
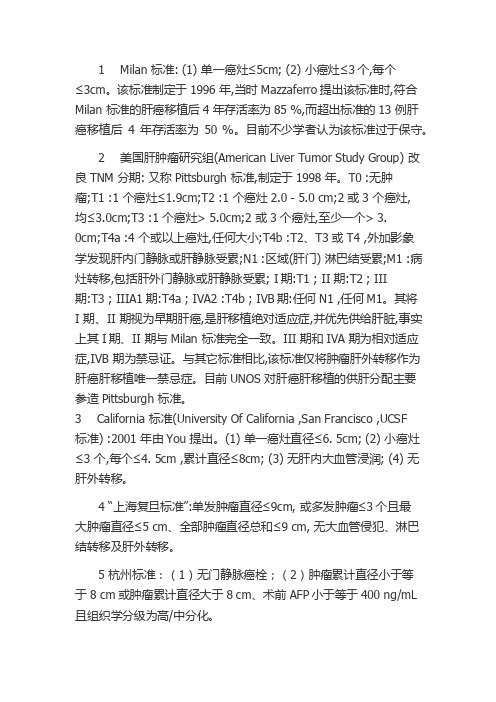
1 Milan 标准: (1) 单一癌灶≤5cm; (2) 小癌灶≤3个,每个≤3cm。
该标准制定于1996 年,当时Mazzaferro提出该标准时,符合Milan 标准的肝癌移植后4 年存活率为85 %,而超出标准的13 例肝癌移植后4 年存活率为50 %。
目前不少学者认为该标准过于保守。
2 美国肝肿瘤研究组(American Liver Tumor Study Group) 改良TNM 分期: 又称Pittsburgh 标准,制定于1998 年。
T0 :无肿瘤;T1 :1 个癌灶≤1.9cm;T2 :1 个癌灶2.0 - 5.0 cm;2 或3 个癌灶,均≤3.0cm;T3 :1 个癌灶> 5.0cm;2 或3 个癌灶,至少一个> 3.0cm;T4a :4 个或以上癌灶,任何大小;T4b :T2、T3 或T4 ,外加影象学发现肝内门静脉或肝静脉受累;N1 :区域(肝门) 淋巴结受累;M1 :病灶转移,包括肝外门静脉或肝静脉受累; I期:T1 ; II 期:T2 ; III期:T3 ; IIIA1 期:T4a ; IVA2 :T4b ; IVB期:任何N1 ,任何M1。
其将I 期、II 期视为早期肝癌,是肝移植绝对适应症,并优先供给肝脏,事实上其I期、II 期与Milan 标准完全一致。
III 期和IVA 期为相对适应症,IVB 期为禁忌证。
与其它标准相比,该标准仅将肿瘤肝外转移作为肝癌肝移植唯一禁忌症。
目前UNOS 对肝癌肝移植的供肝分配主要参造Pittsburgh 标准。
3 California 标准(University Of California ,San Francisco ,UCSF标准) :2001 年由You 提出。
(1) 单一癌灶直径≤6. 5cm; (2) 小癌灶≤3 个,每个≤4. 5cm ,累计直径≤8cm; (3) 无肝内大血管浸润; (4) 无肝外转移。
肝移植国际米兰标准
肝移植国际米兰标准1. 引言肝移植是一种治疗终末期肝疾病的有效方法,可以拯救许多患者的生命。
国际米兰标准是肝移植领域的一项重要指南,用于评估患者是否适合接受肝移植手术,以及选择合适的移植供体。
本文将对国际米兰标准进行全面、详细、完整和深入地探讨。
2. 肝移植的适应证2.1. 慢性肝疾病慢性肝疾病是肝移植的主要适应证之一。
常见的慢性肝疾病包括肝硬化、肝癌和肝衰竭等。
根据国际米兰标准,患者需要满足一定的诊断标准和病情严重程度,才能作为肝移植的适应证。
2.2. 肝癌的适应证肝癌是肝移植的另一个重要适应证。
国际米兰标准对于肝癌的适应证做出了详细的规定,包括肿瘤的大小、数量和侵袭性等因素。
只有符合这些标准的肝癌患者才能被纳入肝移植的适应证范围。
3. 肝移植的禁忌证除了适应证,国际米兰标准还规定了一些禁忌证,即那些不适合接受肝移植的情况。
禁忌证包括活动性滥用药物、不可控恶性肿瘤、智力障碍和慢性感染等。
遵循这些禁忌证是确保肝移植手术安全性和成功的重要因素。
4. 移植供体选择移植供体是肝移植手术的关键环节之一。
根据国际米兰标准,理想的供体应具备以下特征:4.1. 脑死亡供体国际米兰标准强调脑死亡供体的重要性。
这类供体的病理学特征更符合肝移植的要求,同时可以保证供体肝脏的数量和质量。
4.2. 供体质量供体肝脏的质量是影响移植手术成功率的重要因素之一。
国际米兰标准规定了供体肝脏质量的评估指标,包括供体肝脏的脂肪含量、胆固醇水平和肝功能等。
4.3. 移植供体的匹配度在选择移植供体时,与受者的排斥反应也是需要考虑的因素。
国际米兰标准建议进行HLA配型等测试,以确保移植供体与受者的组织相容性和免疫匹配度。
5. 肝移植的手术技术5.1. 手术前准备在进行肝移植手术前,需要对患者的身体状况进行评估和准备工作。
包括血液检查、免疫学评估和感染筛查等,以确保手术的安全性和成功率。
5.2. 供体肝脏切除和保存供体肝脏的切除和保存是肝移植手术的重要步骤之一。
1-癌症筛查课后作业

1、从生存获益原则来看,肝癌是早诊获益率相对较高的肿瘤正确答案:错2、防癌体检的概念是在常见癌症的高风险人群中发现早期的恶性肿瘤或部分常见恶性肿瘤的癌前病变,并对发现异常的人群及高风险人群进行有效管理的体检方式正确答案:对3、本次培训以专业技术培训为主正确答案:错4、美国癌症发病率和死亡率双率下降是因为治疗手段的进步正确答案:错5、甲状腺癌是近年来上升最快的肿瘤,应该重视其筛查早诊正确答案:错6、癌症发病率升高的根本原因正确答案:D 人口老龄化7、我国癌症治疗目前的五年生存率是正确答案:C 40%8、中国男性死亡率最高五种肿瘤是:正确答案:D肺癌、肝癌、胃癌、食管癌和结直肠癌9、中国早期结直肠癌筛查流程专家共识意见(2019,上海)提出的筛查短期目标是:正确答案:C 提高参与率,D 提高结肠镜筛查质量10、防癌体检的原则是:正确答案:A 常见癌症,B 高危人群,C 确切手段,D 合理间隔,E 安全微创11、1、机会性筛查一般不作卫生经济学评价正确答案:对12、大便潜血化学法(gFOBT)筛查结直肠癌的敏感性要高于免疫法(FIT)正确答案:错13、一个肿瘤筛查确切手段的确定一般需要做人群筛查验证,证明其可以降低该肿瘤的人群死亡率正确答案:对14、对于结直肠癌筛查来讲,序贯筛查的策略既适合于人群筛查,也适合于机会性筛查正确答案:对15、胃肠超声造影、胶囊胃镜的筛查手段适合于机会性筛查正确答案:对16、可独立作为肿瘤筛查的肿瘤标记物是正确答案:D 血PSA17、最适合筛查的两种肿瘤是:正确答案:D 结直肠癌和宫颈癌18、乙肝携带者筛查肝癌的合理间隔是:正确答案:B 六个月19、肠道肿瘤序贯筛查的方法包括正确答案:A 结肠镜,C 大便免疫法检测FIT ,D 大便DNA检测20、乳腺癌确切筛查方法是:正确答案:C 乳腺超声,D 乳腺钼靶21、大便化学法检测和免疫法检测在结直肠癌筛查中的效果是相当的正确答案:错22、结直肠癌是最适合筛查的肿瘤之一正确答案:对23、用结直肠镜检查作为大规模自然人群筛查的手段不适合我国正确答案:对24、粪便隐血普查可以使大肠癌死亡率降低正确答案:对25、我国结肠癌筛查的基本策略应该是正确答案:D 序贯筛查26、结直肠癌筛查中,有效性验证有循证医学证据(大样本随机对照筛查试验)的检查手段是正确答案:C 大便FIT定量检测27、阴性预测值高,结果阴性可有效排除结直肠癌的检查是正确答案:C 高敏大便FIT定量检测28、大便潜血检查最重要的质控指标是正确答案:A大便不能沾水29、适合我国结直肠癌筛查的手段有正确答案:A 高危问卷调查初筛,B 大便FIT 初筛,C 大便DNA检测,D 结肠镜筛查30、中国早期结直肠癌筛查流程专家共识意见(2019,上海)推荐的适合我国结直肠癌初筛手段是正确答案:A 高危问卷调查,B 大便FIT检测,C 大便DNA检测1、传统宫颈细胞学的分类方法是哪种,该分类方法将细胞分为几级正确答案:巴氏,五级2、宫颈液基薄层细胞学技术是哪方面技术的重大革新正确答案:制片技术3、HPV病毒属于正确答案:双链闭环的DNA病毒4、HPV病毒分为高危型和低危型,分别可引起的疾病是正确答案:宫颈癌前病变及宫颈癌,生殖道湿疣5、阴道镜检查的指征,以下不正确的是正确答案:宫颈柱状上皮外移6、张某,女,25岁,主因“孕16周,TCT提示HSIL,HPV52型(+),要求进一步诊治”就诊。
肝移植 米兰标准
肝移植米兰标准
在医学领域,肝移植已经成为一种较为常见的手术方式,可以有效治疗各种肝病,如肝硬化、肝癌等。
米兰标准是肝移植手术中常用的一种标准,它规定了肝移植手术的适应症和禁忌症,以及手术时机的选择和术后护理等方面的指导原则。
根据米兰标准,肝移植手术的适应症主要包括以下几个方面:
1. 肝衰竭:对于各种原因引起的肝衰竭,如肝炎、肝硬化、肝癌等,米兰标准认为肝移植是一种有效的治疗手段。
2. 遗传代谢性肝病:对于一些遗传代谢性肝病,如威尔森病、肝豆状核变性等,肝移植可以改善患者的生活质量。
3. 肝脏肿瘤:对于某些肝脏肿瘤,如肝癌等,肝移植是一种可行的治疗选择。
然而,米兰标准也规定了肝移植手术的禁忌症,包括以下几个方面:
1. 存在其他严重的器官疾病:如果病人存在其他严重的器官疾病,如心脏病、肾脏病等,肝移植手术的风险会很高。
2. 存在感染性疾病:如果病人存在感染性疾病,如艾滋病、结核病等,肝移植手术可能会加重感染。
3. 存在精神疾病:如果病人存在精神疾病,如抑郁症、焦虑症等,肝移植手术可能会影响患者的心理状态和生活质量。
在选择肝移植手术时机时,米兰标准提出了一些指导原则。
首先,
病人应该接受全面的医学评估,以确定是否适合进行肝移植手术。
其次,在等待肝源的过程中,病人应该接受必要的药物治疗和生活方式调整,以减轻病情并提高手术成功率。
最后,在手术后,病人应该接受长期的术后护理和随访,以确保手术效果和生活质量的提高。
总之,米兰标准为肝移植手术提供了一种较为全面的指导框架,有助于医生根据患者的具体情况做出更为准确和合适的治疗决策。
肝移植治疗肝恶性肿瘤的适应证选择
75%,这使得米兰标准成为了肝移植治疗肝恶性肿
瘤的金
'4打然,
于格的限制
以至于一些患者失去肝移植机会,因此一部分移
植中心尝试扩大适应证并提出了诸多标准⑸,这
其中包括加州旧金山大学提出的标准(单发肿瘤
小于或等于6.5cm,小于或等于3个肿瘤且每个肿
瘤小于4.5cm,肿瘤总和小于或等于8cm)'6(,东
(不多于5个肿瘤且最大肿瘤小于或等于
5cm)⑺,京都标准(不多于10个肿瘤且最大肿瘤
小于或等于5cm且DCP小于或等于400mAU/
ml)'8 (,牙山标准(不多于5个肿瘤且最大肿瘤小
于或等于5cm)⑼,我国提出的杭州标准(肿瘤直
径总合小于或等于8cm,若肿瘤直径总和大于
8cm,AFP需小于或等于400ngml且肿瘤病理分
瘤数量大于5个(所有肿瘤均不超过4cm,肿瘤直
径综合小于或等于12cm)或单发肿瘤直径大于
8cm者可考虑肿瘤降期治疗,据报道约24% -
69%的患者能够成功降期并行肝移植术,这些患者
的5年生存率可达55%〜94% '⑸。
肝门部胆管癌:手术切除一直是肝门部胆管
癌的有效治疗手段,但是对于无法行手术切除的
这类患者,肝移植后新辅助化疗被认为是治疗该 类疾病的另一选择'16(,据梅奥协议报道,丘
治疗手段下的
者可获得不低于68%的5
年无瘤生存率,此类患者的预后甚至优于一些其
他疾病行肝 的预后'17(。然而,梅奥协议中所
到的这部分“无法切除”的肝门部胆管癌病例
通讯作者:张升宁,Email: zsn813@
日本的研究认为肝母细胞瘤行肝移植预后主要取
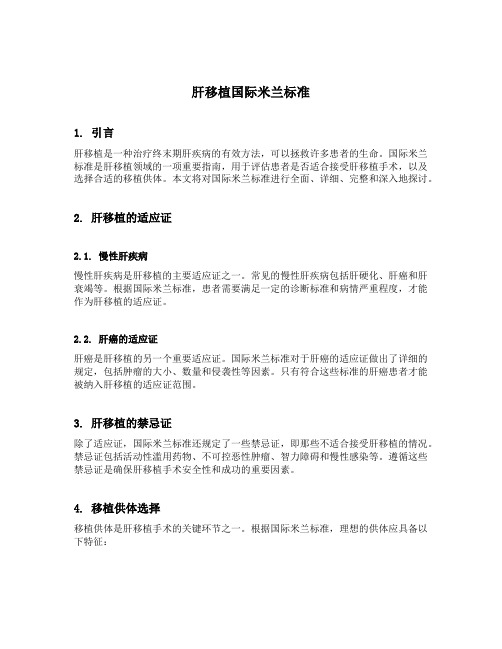
肝癌肝移植的米兰标准

• poor survival with transplant for tumors 5cm
– 18-30% at 5 years
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
LONG TERM RESULTS OF LIVER TRANSPLANTATION AND MULTIMODAL ADJUVANT THERAPY FOR THE
TREATMENT OF HEPATOCELLULAR CARCINOMA LARGER THAN 5CM
Sasan Roayaie, Sukru Emre, Thomas Fishbein, Patricia Sheiner, Charles Miller, and Myron Schwartz
Liver Transplantation for HCC Beyond the Milan Criteria
Charles M. Miller, MD
The Recanati-Miller Transplantation Institute Mount Sinai Medical Center New York, NY
Previous Studies
study
肝移植米兰标准
肝移植米兰标准肝移植是一种重要的外科手术,对于肝功能衰竭或肝癌等疾病患者来说,是拯救生命的唯一希望。
而米兰标准是肝移植手术的一种评估标准,它对于确定肝移植的适应症和手术效果具有重要意义。
米兰标准最早是在1996年由意大利米兰大学医学院提出的,它主要用于评估肝细胞癌患者是否适合进行肝移植手术。
根据米兰标准,肝细胞癌患者的肿瘤大小和数量是确定是否适合进行肝移植的关键指标。
具体来说,符合米兰标准的肝细胞癌患者应当满足以下条件,单个肿瘤直径不超过5厘米,或者最多3个肿瘤,每个肿瘤直径不超过3厘米,且没有血管侵犯和淋巴结转移。
只有符合这些条件的肝细胞癌患者才能被列入肝移植的候选名单。
米兰标准的提出,极大地提高了肝细胞癌患者的肝移植手术的成功率,避免了手术后肿瘤复发的风险。
同时,米兰标准的应用也使得肝移植手术的资源得到了更加合理的分配,让更多的患者受益于这一治疗手段。
除了在肝细胞癌患者中的应用,米兰标准也被逐渐引入到了其他肝脏疾病的评估中。
例如,在肝硬化和肝功能衰竭患者中,米兰标准也可以作为评估肝移植适应症的重要参考标准之一。
这样一来,米兰标准不仅仅局限于肝细胞癌患者,而是逐渐成为了评估肝移植适应症的通用标准。
然而,值得注意的是,米兰标准并不是肝移植手术的唯一评估标准,它只是其中的一部分。
在实际应用中,医生们还需要综合考虑患者的年龄、肝功能、全身情况等因素,才能最终确定是否适合进行肝移植手术。
因此,即使患者符合了米兰标准,也并不意味着就一定能够进行肝移植手术,还需要医生们进行全面评估。
总的来说,米兰标准作为肝移植手术的重要评估标准,对于提高手术的成功率、避免肿瘤复发、合理分配手术资源等方面具有重要意义。
但在实际应用中,还需要结合患者的具体情况进行综合评估,才能最终确定是否适合进行肝移植手术。
希望随着医学的不断发展,能够有更多更精准的评估标准出现,让更多的患者受益于肝移植手术,重获新生。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
LONG TERM RESULTS OF LIVER TRANSPLANTATION AND MULTIMODAL ADJUVANT THERAPY FOR THE TREATMENT OF HEPATOCELLULAR CARCINOMA LARGER THAN 5CM Sasan Roayaie, Sukru Emre, Thomas Fishbein, Patricia Sheiner, Charles Miller, and Myron Schwartz
Entry Criteria
• • • • no significant ascites or encephalopathy INR < 1.5 creatinine < 2mg/dl bilirubin < 2mg/dl
– unless suffering from cholestatic liver diber 1991 - January 1999 • 80 patients enrolled
– 43 transplanted – 37 eventually excluded
• • • • tumor progression main portal vein tumor liver failure lymph node metastasis 2 9 5 6 • • • • distant metastasis GI bleeding other malignancies patient preference 6 4 2 3
Carr et al-Pittsburgh 1993 TACE, chemo Cherqui et al-France 1994 TACE,rads,chemo Olthoff et al-UCLA chemo 1995
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
Follow-up
• CT scan chest and abdomen/pelvis
– every 3 months - 1st year – every 6 months thereafter
• AFP
– every 6 weeks - 1st year – every 3 months thereafter
Intra- Operative Protocol
• backup recipient in hospital • exploratory laparotomy for extrahepatic disease • standard hepatectomy and transplant • doxorubicin 10mg/m2 while anhepatic
• immunosuppression
– corticosteroids with cyclosporine or tacrolimus – pulse steroids ± OKT3 for rejection – no azathioprine
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
– 75% at 4 years
• poor survival with transplant for tumors ≥ 5cm
– 18-30% at 5 years
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
Background: HCC
• most common solid organ tumor worldwide • one million deaths annually • incidence rising in US
– 2.4 per 100,000
• good survival with transplant for tumors < 5cm
Liver Transplantation for HCC Beyond the Milan Criteria
Charles M. Miller, MD The Recanati-Miller Transplantation Institute Mount Sinai Medical Center New York, NY
• normal MUGA • no prior chemotherapy or radiation
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
The Recanati-Miller Transplantation Institute Mount Sinai Medical Center New York, NY Annals of Surgery Vol. 235, No. 4 533-539 April, 2002
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.
Pretransplant Management
• subselective arterial chemoembolization
– mitomycin-C, doxorubicin, cisplatin – collagen or polyvinyl alcohol
• CT scan & AFP level every 3 months
– response - AFP decrease >50% – TACE repeated as needed
• excluded when entry criteria no longer met
This presentation is reproduced on this site with the permission of the author(s). All opinions, research citations and analyses are those of the author(s) and may not reflect those of OPTN/UNOS committees or the OPTN/UNOS Board of Directors.