[34]Delmar 2017恶性胶质瘤治疗概况
脑胶质瘤治疗方法
脑胶质瘤治疗方法
脑胶质瘤是一种常见的恶性脑肿瘤,治疗方法通常包括手术切除、放疗和化疗。
1. 手术切除:手术是治疗脑胶质瘤最主要的方法。
通过手术切除部分或全部肿瘤组织,可以减轻症状、解除颅内压增高,并提供病理学诊断。
手术切除力求完整切除肿瘤,但对于那些位置较深或无法完全切除的病例,通常需要辅助其他治疗方法。
2. 放射治疗:放疗在手术后常常用于减少残留或复发肿瘤的风险,或者作为预防措施。
放射治疗使用高能射线破坏癌细胞,阻止其生长和分裂。
放射治疗通常进行数周甚至几个月,每天一次或每周几次。
3. 化疗:化疗是使用抗癌药物杀死癌细胞的方法。
化疗通常通过口服药物或静脉注射给药。
对于某些类型的脑胶质瘤,化疗可以用于术前缩小肿瘤的体积,或者用于术后减少复发的风险。
此外,还有一些新兴的治疗方法正在研究中,如靶向治疗、免疫疗法和基因治疗等。
这些治疗方法的目标是更加精准地攻击癌细胞,并减少对正常细胞的损害。
然而,这些新技术仍处于研究和发展阶段,尚未广泛应用于脑胶质瘤的临床治疗中。
胶质瘤最佳治疗方案
胶质瘤最佳治疗方案引言胶质瘤是一种常见的中枢神经系统肿瘤,起源于星形胶质细胞。
目前,胶质瘤的治疗方法较为多样化,包括手术切除、放射治疗、化学治疗等。
本文将讨论胶质瘤的最佳治疗方案,并对其中的主要治疗方法进行详细介绍。
手术切除手术切除是治疗胶质瘤最常用的方法之一。
手术切除可以通过开颅手术或经导管手术进行。
一般情况下,胶质瘤的切除率越高,患者的生存率就越高。
然而,对于一些位置较为特殊的胶质瘤,手术切除可能存在较高风险,因为这些胶质瘤位于脑干或其他重要的脑部结构附近。
在进行手术切除之前,医生需要评估患者的手术可行性和风险。
放射治疗放射治疗是治疗胶质瘤的重要方法之一。
放射治疗可以通过使用外部放射线(外放射治疗)或将放射源直接植入肿瘤组织(内放射治疗)进行。
放射治疗的原理是将高能射线引起的DNA损伤作用于肿瘤细胞,从而诱导肿瘤细胞死亡。
放射治疗一般在手术后进行,以减少胶质瘤的复发和扩散。
放射治疗的剂量和持续时间需要经过精确计算和评估。
剂量过高可能会损伤正常组织,而剂量过低又可能无法有效杀灭肿瘤细胞。
因此,确定合适的放射治疗剂量是非常重要的。
化学治疗化学治疗是胶质瘤治疗的另一重要方法。
化学治疗是通过使用抗肿瘤药物来杀灭肿瘤细胞或抑制其生长。
常用的抗肿瘤药物包括氮芥类药物、铂类药物、抗代谢药物等。
化学治疗可以通过口服药物或静脉注射进行。
化学治疗的选择和使用需要根据胶质瘤的类型、患者的整体情况和可能的副作用等因素进行综合考虑。
通常情况下,化学治疗常与手术切除或放射治疗结合使用,以达到最佳的治疗效果。
靶向治疗靶向治疗是近年来新兴的一种治疗方法,该方法通过作用于肿瘤细胞上的特定生物标志物,从而抑制肿瘤细胞的增殖和生长。
胶质瘤的靶向治疗主要包括针对EGFR、PI3K/AKT/mTOR等信号通路的药物治疗。
靶向治疗可以根据肿瘤的分子特征进行个体化的治疗选择,从而提高治疗效果。
然而,靶向治疗的应用仍存在一些限制,包括耐药性、副作用等。
胶质瘤治疗方法有哪些
胶质瘤治疗方法有哪些
一、概述
胶质瘤疾病是属于外科和神经外科疾病,胶质瘤疾病的肿瘤的发病起源是神经间质细胞,还有神经胶质和室管膜,还有脉络丛上皮和神经实质细胞都是引起起的胶质瘤疾病段主要原因,因为大多数肿瘤的起源都有不同类型的神经胶质,,所以对于发生在神经外胚层的各种肿瘤,一般都被人们称为视神经胶质瘤的,由于肿瘤的逐渐增大,形成颅内占位病变,患者会常伴有周围脑水肿症状的,
二、步骤/方法:
1、
神经胶质瘤疾病的病程还有病理类型和所在部位生长的长短是不一样的,神经胶质瘤患者在出现病情症状到就诊时间一般是为很多周期或者是很多月的,还有少数胶质瘤患者会达到数年的过程的,
2、
胶质瘤的症状主要是由两方面的表现,第一方面是颅内压增高,还有其他一般症状,其他一般症状,比如说患者会出现头痛和呕吐,还有视力减退,复视,癫痫发作和精神症状等等,
3、
神经胶质瘤是可以通过西医的治疗方法去治疗的,对于治疗神经胶质瘤疾病,西医是通过手术的治疗方法为主要的,一般胶质瘤患者都是主张综合治疗的,就是说手术以后配合放射治疗和化学治疗等等,
三、注意事项:
胶质瘤疾病患者的饮食治疗是缺一不可的,食疗的膳食中的许多食品是药品的一部分的,是有治疗胶质瘤疾病的一定效果的,但是食疗方法是不能完全取代药物治疗胶质瘤疾病的,。
恶性胶质瘤和目前的治疗方向
恶性胶质瘤和目前的治疗方向神经胶质瘤代表了大多数的恶性脑瘤。
在成人中,该病主要为弥漫性肿瘤,范围从I级到IV级。
不幸的是,大多数胶质瘤患者的生存率很低,最常见的亚型胶质母细胞瘤(GBM)患者中只有5%的患者在积极治疗后存活5年以上。
为了解决目前治疗策略的局限性,相关专家仍在不断探索。
值得一提的是,癌症免疫疗法已经为多种癌症类型带来了令人兴奋和重要的治疗结果,并引发了对神经胶质瘤治疗的前所未有的研究兴趣。
通过操纵免疫系统,免疫治疗可以实现肿瘤的长期缓解和极小的副作用。
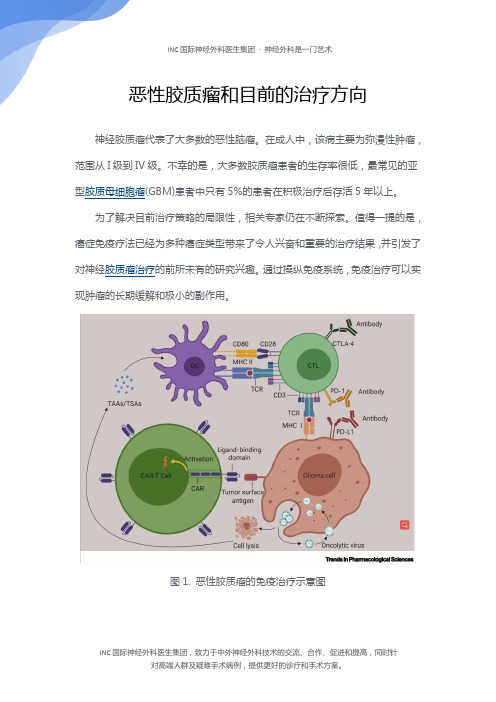
图1. 恶性胶质瘤的免疫治疗示意图新的研究表明,免疫治疗的抗肿瘤反应可能发生在大脑中,为开发治疗恶性胶质瘤的策略铺平了道路。
在这里,我们回顾了免疫疗法作为恶性胶质瘤的治疗方法(图1),讨论了该方法的挑战和争议,并研究了可能克服难治疾病的新方法。
目前恶性胶质瘤的免疫治疗策略两种抑制性免疫通路,程序性细胞死亡蛋白及其配体(PD-1和PD-L1)和细胞毒性T淋巴细胞相关抗原4 (CTLA-4),已被确定为阻碍免疫应答的主要效应因子。
抗PD-1 (nivolumab和pembrolizumab)、PD-L1 (atezolizumab和durvalumab)和CTLA-4 (ipilimumab)的单克隆抗体(mab)通过重新激活细胞毒性T淋巴细胞(CTLs)来增强抗肿瘤反应。
然而,第三期临床试验比较369个GBM复发病人,认为贝伐单抗(rGBM)没能证明纳武单抗的好处,只授予一个类似操作系统中位数(金属氧化物半导体,9.8 vs 10.0个月),但更短的无进展生存时间(PFS, 1.5 vs 3.5个月)与贝伐单抗。
尼鲁单抗与伊匹单抗联合或作为rGBM的单药治疗已进行了进一步的研究。
虽然单用尼鲁单抗的耐受性优于联合用药,且疗效相当,但40例患者中只有3例达到部分缓解(PR)。
与此同时,两项回顾性研究表明,抗pd -1挽救性治疗不能给复发性高级别胶质瘤(HGG)患者带来生存益处,在接受派姆单抗的患者中,mOS仅达到4个月。
胶质瘤的治疗方法有哪些

如对您有帮助,可购买打赏,谢谢
胶质瘤的治疗方法有哪些
导语:随着环境的不断恶化,现在胶质瘤的患者是越来越多,所以,很多得了胶质瘤的一些患者,都想尽快的让自己通过治疗让自己尽快康复,那么胶质瘤
随着环境的不断恶化,现在胶质瘤的患者是越来越多,所以,很多得了胶质瘤的一些患者,都想尽快的让自己通过治疗让自己尽快康复,那么胶质瘤的治疗方法有哪些?为了你尽快的康复,也为了能选择最好的治疗方法,就来看看下面的治疗方法介绍。
对神经胶质瘤的治疗以手术治疗为主,但由于肿瘤浸润性生长,与脑组织间无明显边界,除早期肿瘤小且位于适当部位者外,难以作到全部切除,一般都主张综合治疗,即术后配合以放射治疗、化学治疗等,可延缓复发及延长生存期。
并应争取作到早期确诊,及时治疗,以提高治疗效果。
1.手术治疗
原则是在保存神经功能的前提下尽可能切除肿瘤。
早期肿瘤较小者应争取全部切除肿瘤。
对位于额叶或颞叶前部较大的肿瘤,可作脑叶切除术,连同肿瘤一并切除。
肿瘤累及大脑半球两个脑叶以上已有偏瘫但未侵及基底节、丘脑及对侧者,亦可作大脑半球切除术。
肿瘤位于运动、言语区而无明显偏瘫、失语者,应注意保持神经功能适当切除肿瘤,避免遗有严重后遗症。
可同时作颞肌下或去骨瓣减压术。
亦可仅作活检后作减压术。
丘脑肿瘤压迫阻塞第三脑室者,可作分流术,否则亦可作减压术。
脑室肿瘤可根据所在部位从非重要功能区切开脑组织进入脑室,尽可能切除肿瘤,解除脑室梗阻。
应注意避免损伤肿瘤邻近下丘脑或脑干,以防发生危险。
脑干肿瘤除小的结节性或囊性者可作切除外,有
预防疾病常识分享,对您有帮助可购买打赏。
胶质瘤治疗方案

胶质瘤治疗方案引言胶质瘤(Glioma)是指起源于胶质组织的恶性肿瘤,是中枢神经系统最常见的原发性肿瘤之一。
胶质瘤的治疗方案因患者的年龄、肿瘤类型、肿瘤位置和病情分期等因素而有所不同。
本文将介绍常见的胶质瘤治疗方案,以供参考。
1. 手术治疗手术治疗是胶质瘤最常用的治疗方法之一。
手术的目标是尽可能完全切除肿瘤组织,从而达到缓解症状和延长生存时间的目的。
手术方法包括开颅手术和微创手术。
对于可切除的小型胶质瘤,手术通常是首选的治疗方案。
在手术前,患者需要进行相关检查以评估肿瘤的位置和大小。
手术中,外科医生会尽可能切除肿瘤组织,并确保不损害周围的正常脑组织。
手术后,患者需要密切观察并进行术后康复治疗。
2. 放射治疗放射治疗是胶质瘤治疗中的重要手段之一,可以用于术前、术后或单独治疗。
放射治疗利用高能辐射破坏肿瘤细胞的DNA,从而阻止其生长和扩散。
放射治疗可以减小胶质瘤的体积,缓解相关症状,并延长患者的生存时间。
放射治疗通常需要在专门的放射科医生的指导下进行。
治疗计划会根据肿瘤的位置、大小和患者的整体情况而定。
通常,放射治疗需要分为多个疗程进行,每个疗程之间有一定的间隔。
3. 化学治疗化学治疗是通过使用药物来杀死恶性肿瘤细胞的治疗方法。
对于胶质瘤患者来说,化学治疗通常与手术或放射治疗联合使用,以提高治疗效果。
化学治疗的药物包括化疗药物和靶向治疗药物。
化疗药物可以通过静脉注射或口服给药的方式使用。
靶向治疗药物则是通过靶向肿瘤细胞的特定分子来杀死肿瘤细胞。
化学治疗的方案和剂量会根据患者的情况和肿瘤的类型而定。
治疗过程中需要密切监测患者的身体反应和药物副作用。
4. 免疫治疗免疫治疗是近年来兴起的一种胶质瘤治疗方法。
它利用患者的免疫系统来攻击肿瘤细胞。
免疫治疗的方法包括细胞免疫疗法、癌症疫苗和免疫检查点抑制剂。
细胞免疫疗法是将患者体内的免疫细胞(如淋巴细胞)提取出来,经过处理后再注射回体内,以增强免疫细胞攻击肿瘤的能力。
胶质母瘤三到四级的最好治疗方案
胶质母瘤三到四级的最好治疗方案胶质母瘤三到四级的最佳治疗方案胶质母瘤是一种常见的中枢神经系统肿瘤,其中三到四级的胶质母瘤被认为是高度侵袭性和恶性的类型。
对于这一级别的瘤体,选择合适的治疗方案显得尤为重要。
本文将为您介绍胶质母瘤三到四级的最佳治疗方案。
一、手术切除手术切除是胶质母瘤治疗的首选。
通过手术切除病灶,可有效减少肿瘤负荷,缓解病人的症状,并提高患者的生存率。
手术切除的方式可以根据肿瘤的大小和位置进行选择,包括完全切除、次全切除和部分切除。
然而,在胶质母瘤治疗中,单纯的手术切除常常难以完全根除肿瘤,因此需要结合其他治疗手段以达到更好的疗效。
二、放射治疗放射治疗在胶质母瘤的治疗中起着重要作用。
通过高能射线的照射,可破坏肿瘤细胞的DNA结构,阻止其进一步增殖和扩散。
这一治疗方法几乎可用于所有胶质母瘤患者,不论是术前、术后还是病情复发的患者。
放射治疗可以单独应用,也可以与手术切除或化疗联合应用,以增强疗效。
三、化疗化疗是胶质母瘤治疗的重要手段之一。
通过使用抗肿瘤药物,可以干扰肿瘤细胞的生命周期,抑制其生长和扩散。
对于胶质母瘤三到四级患者,化疗通常作为综合治疗方案的一部分,可以在手术和放疗前后进行应用。
化疗药物的选择和方案可以根据患者的具体情况以及肿瘤的分级和分型进行个体化制定。
四、靶向治疗近年来,靶向治疗作为一种新的治疗策略逐渐应用于胶质母瘤的治疗中。
靶向药物通过特异性地作用于胶质母细胞中的特殊靶点,干扰信号传导通路,抑制肿瘤的增长和扩散。
靶向治疗的选择和使用需根据患者的遗传学和分子学特征进行个性化定制。
五、免疫治疗免疫治疗是近年来备受关注的胶质母瘤治疗领域的一个新兴方法。
通过激活和增强患者自身的免疫系统,免疫治疗可以识别并攻击肿瘤细胞,达到治疗的效果。
针对胶质母瘤的免疫治疗目前正在不断研究和发展中,包括使用免疫检查点抑制剂、CAR-T细胞疗法等。
综上所述,胶质母瘤三到四级的最佳治疗方案并不是单一的方法,而是一个多学科综合治疗的过程。
胶质母细胞瘤的治疗方法有哪些
胶质母细胞瘤的治疗方法有哪些胶质母细胞瘤是一种罕见但严重的颅内疾病。
它起源于神经系统的胶质细胞,主要发生在脑和脊髓中。
胶质母细胞瘤的治疗方法通常是综合性的,包括手术切除、放射治疗和化疗。
下面将详细介绍这些治疗方法。
1. 手术切除:手术切除是治疗胶质母细胞瘤的首选方法。
通过手术切除可以尽可能地去除瘤体,在一定程度上缓解症状并延长患者的生存期。
手术切除的难度和风险取决于肿瘤的大小、位置和周围组织的影响。
在手术中,医生会尽量去除肿瘤,并且留下正常的组织。
手术后可能需要进行康复治疗以恢复功能,并且密切监测病情。
2. 放射治疗:放射治疗是胶质母细胞瘤治疗中常用的一种方法。
放射治疗使用高能射线来杀死癌细胞。
它可以用于术后辅助治疗以消灭残留的癌细胞,也可以用于术前减小肿瘤尺寸。
放射治疗的剂量和方案会因患者的年龄、健康状况和肿瘤特点而有所不同。
副作用包括头发脱落、恶心和疲劳等,但一般是可控制的。
3. 化疗:化疗是使用药物杀死癌细胞的治疗方法。
胶质母细胞瘤通常对化疗敏感,这意味着化疗药物可以有效杀死肿瘤细胞。
常用的化疗药物包括环磷酰胺、卡巴班波和替莫唑胺等。
化疗通常与手术或放射治疗联合使用,以减小肿瘤的尺寸和防止复发。
副作用包括恶心、呕吐、免疫抑制等,但可以通过适当的支持疗法来减轻。
4. 靶向治疗:靶向治疗是一种针对某些特定分子或信号通路的药物治疗方法。
胶质母细胞瘤中常见的分子靶点包括表皮生长因子受体(EGFR)和PI3K-AKT-mTOR信号通路等。
针对这些分子的药物包括曲妥珠单抗和帕尼单抗等。
靶向治疗通常需要进行基因检测,以确定患者是否适合接受该治疗。
副作用可能包括皮疹、腹泻和高血压等,但与化疗相比较为轻微。
5. 免疫治疗:免疫治疗是通过激活机体免疫系统来抑制和杀死癌细胞的治疗方法。
胶质母细胞瘤中的免疫治疗包括免疫检查点抑制剂和CAR-T细胞疗法等。
免疫治疗的优势在于具有持久的疗效和较少的副作用,但目前在胶质母细胞瘤的应用仍处于早期阶段。
脑胶质瘤的治疗方法

脑胶质瘤的治疗方法脑胶质瘤是一种主要起源于神经胶质细胞的恶性肿瘤,常见于中枢神经系统。
它的治疗方法通常涉及手术切除、放射治疗和化学治疗等多种方法。
下面我将详细介绍脑胶质瘤的治疗方法。
1. 手术切除:手术切除是治疗脑胶质瘤的主要方法之一。
手术的目的是尽可能完整地切除肿瘤组织,减少肿瘤对健康脑组织的侵袭。
手术通常采用显微镜辅助技术进行,可以通过切除肿瘤组织来减轻症状,延长患者的生存期。
然而,脑胶质瘤通常有较高的复发率,因此手术往往需要与其他治疗方法联合应用。
2. 放射治疗:放射治疗是用高能射线照射肿瘤组织,破坏肿瘤细胞的生长和分裂,达到治疗目的的方法。
放射治疗可以用于术前辅助治疗,以减小肿瘤体积,提高手术切除的成功率;也可以用于术后辅助治疗,以杀死手术切除后残留的肿瘤细胞。
放射治疗有时也可以单独应用于无法手术切除的患者。
然而,放射治疗也会对正常脑组织产生一定的损伤,因此在剂量和治疗计划的确定上需要谨慎。
3. 化学治疗:化学治疗是使用化学药物抑制肿瘤细胞的生长和分裂的方法。
化学药物通过静脉注射或口服给药的方式进入全身循环,可以杀死远离肿瘤灶的转移细胞。
常用的化疗药物包括卡矽平、替莫唑胺、长春新碱等。
化学治疗通常与手术和/或放射治疗联合应用,以达到更好的治疗效果。
然而,脑胶质瘤对化疗药物的抵抗性较强,因此化疗的效果有限。
4. 靶向治疗:近年来,靶向治疗作为一种新兴的治疗方法,逐渐应用于脑胶质瘤的治疗中。
靶向治疗是基于研究发现脑胶质瘤细胞中存在特定的致病基因突变或异常表达的蛋白质,通过选择性地抑制这些致病基因或蛋白质的活性,从而达到治疗的目的。
目前,已经开发出一些针对脑胶质瘤的靶向治疗药物,例如透明质酸合成酶抑制剂(如贝伐珠单抗)和基因突变抑制剂(如特罗瑞必妥)。
靶向治疗的优势在于针对肿瘤细胞的特定靶点,具有较好的治疗效果和较少的毒副作用。
5. 免疫治疗:免疫治疗是利用身体的免疫系统来抑制肿瘤生长和扩散的一种治疗方法。
恶性脑胶质瘤能治好吗?

恶性脑胶质瘤能治好吗?恶性(高级)神经胶质瘤是快速进展的脑肿瘤,包括间变性少突胶质细胞瘤,间变性星形胶质细胞瘤,混合间变性少突星形胶质细胞瘤(均为世界卫生组织WHO III级)和胶质母细胞瘤(WHO IV级)。
年龄,肿瘤等级和身体状况是影响对治疗反应以及初始手术切除范围的三个重要的预后因素。
此外,对于刚诊断为胶质母细胞瘤的患者,已经开发出了将患者年龄,切除范围,术后替莫唑胺的使用(辅助),精神状态和皮质类固醇激素用作预后因素,以评估中位生存期和两年生存概率。
恶性胶质瘤预后和预测指标具有1p/19q缺失的少突胶质细胞瘤已被认为是对RT和化疗(ChT)特别敏感的独特病理实体。
在回顾性分析中,通过甲基化使肿瘤的表观遗传沉默甲基鸟嘌呤甲基转移酶(MGMT)基因启动子的患者受益于替莫唑胺。
肿瘤无法修复ChT诱导的DNA损伤。
IDH1(NADP+依赖性异柠檬酸脱氢酶)突变发生在绝大多数WHO WHO II级或III级神经胶质瘤和继发性胶质母细胞瘤中。
异柠檬酸脱氢酶1(IDH1R132H)的p.Arg132His突变(精氨酸被组氨酸取代)不仅是一种频繁的改变(>70%),而且还是神经胶质瘤的主要预后标志物。
IDH1突变的患者具有更好的治疗效果和更好的生存率。
恶性神经胶质瘤的术后(辅助)治疗胶质母细胞瘤由于其具有浸润性,因此无法通过手术彻底消除恶性神经胶质瘤。
如今,胶质母细胞瘤手术后的标准治疗是同时进行替莫唑胺RT-ChT(RT为60 Gy和替莫唑胺75 mg/m 2/day,持续6周),随后进行替莫唑胺辅助治疗(150-200 mg/m 2/day)每28天5天,共6个周期)。
据Stupp等报道。
这种RT-ChT)组合具有可接受的副作用,与单独使用RT(60 Gy进行6周)相比,增加了中位生存期(14.6个月vs.12.1个月,p<0.001)。
接受RT/CTh治疗的患者的存活率分别显着高于分别接受两年和五年的接受RT治疗的患者的存活率(26.5%vs.10.4%和10%vs.2%)。
脑胶质瘤的手术治疗解析

脑胶质瘤的手术治疗解析1. 简介脑胶质瘤是一种起源于脑胶质细胞的神经系统恶性肿瘤,约占脑肿瘤的40%-50%。
由于其位置深藏于大脑内部,手术治疗一直是脑胶质瘤治疗的重要手段。
本文将对脑胶质瘤的手术治疗进行详细解析。
2. 手术治疗的目标脑胶质瘤手术治疗的主要目标是尽可能完整地切除肿瘤组织,同时保留神经功能,降低复发率,延长患者生存期。
手术治疗还可以为后续的放疗、化疗等综合治疗提供基础。
3. 手术治疗方法3.1 传统开颅手术传统开颅手术是目前治疗脑胶质瘤最常见的方法。
手术过程中,医生会在患者头部切开一个切口,然后利用显微镜和手术器械尽可能地切除肿瘤组织。
传统开颅手术的优点是肿瘤切除程度高,手术视野清晰,但缺点是手术创伤大,术后恢复时间长。
3.2 微创手术微创手术是近年来发展起来的一种新型手术方法,包括内镜辅助手术和机器人辅助手术。
微创手术的优点是手术创伤小,术后恢复快,但肿瘤切除程度相对较低。
3.3 术中导航术中导航是一种利用影像学技术(如MRI、CT等)在手术过程中实时显示肿瘤位置的方法,有助于医生更准确地切除肿瘤组织,降低术后复发率。
3.4 术中荧光术中荧光是一种利用特定染料使肿瘤组织在手术过程中发出荧光的方法,有助于医生更清晰地识别肿瘤组织,提高肿瘤切除程度。
4. 手术治疗的优势与挑战4.1 优势- 肿瘤切除程度高:手术治疗可以尽可能地切除肿瘤组织,降低术后复发风险。
- 保留神经功能:手术过程中,医生会尽量保护周围正常神经组织,降低神经功能障碍的发生。
- 延长生存期:手术治疗可以为后续的放疗、化疗等综合治疗提供基础,从而延长患者生存期。
4.2 挑战- 手术创伤:传统开颅手术创伤较大,术后恢复时间长。
- 术后并发症:手术治疗可能引发术后出血、感染等并发症。
- 复发风险:脑胶质瘤具有较高的复发率,手术治疗后仍需密切监测和综合治疗。
5. 总结手术治疗是脑胶质瘤治疗的重要手段,具有肿瘤切除程度高、保留神经功能、延长生存期等优势。
胶质瘤的治疗方法

胶质瘤的治疗方法胶质瘤是一种发生在脑中的恶性肿瘤,起源于神经胶质细胞。
根据肿瘤的分级,胶质瘤分为四个等级:Ⅰ级为胶质瘤,Ⅱ级为低级别的胶质瘤,Ⅲ级为间变性胶质瘤,Ⅳ级为恶性胶质瘤,也就是常见的脑胶质瘤(Glioblastoma)。
胶质瘤的治疗方法包括手术切除、放射治疗和化疗,通常是通过综合治疗的方式来提高预后。
首先,对于可切除的胶质瘤,手术切除是主要的治疗方法之一。
手术切除的目的是尽量完全切除肿瘤,以减轻症状,延长生存时间。
手术切除的可行性取决于肿瘤的大小、位置和是否侵入重要的神经结构。
对于一些小的、浅在的胶质瘤,可以通过开颅手术或者微创手术进行切除,术后患者通常需要进行放射治疗和/或化疗来控制肿瘤的复发。
其次,放射治疗也是胶质瘤的主要治疗方式之一。
放射治疗通过使用高能射线来杀死肿瘤细胞,以减小肿瘤的体积和抑制其进一步生长。
放射治疗可以在手术切除后进行,也可以在手术之前进行,以减小肿瘤的体积,使手术切除更容易。
放射治疗可能会导致一些副作用,如疲劳、头痛、恶心和呕吐等,但这些副作用通常可以通过适当的药物治疗来缓解。
最后,化疗也是胶质瘤治疗的重要组成部分。
化疗通过使用抗肿瘤药物来杀死肿瘤细胞,以减小肿瘤的体积和抑制其进一步生长。
在胶质瘤治疗中使用的常见化疗药物包括卡铂(carboplatin)、替莫唑胺(temozolomide)等。
化疗通常与手术切除和/或放射治疗联合使用,以提高治疗效果。
化疗可能会引起一些副作用,如恶心、呕吐、毛发脱落和免疫系统抵抗力下降等,但这些副作用通常是暂时的,可以通过适当的药物治疗来缓解。
除了上述常规治疗方法之外,还有一些新的治疗方法被用于胶质瘤的治疗,如靶向治疗、免疫治疗和基因治疗等。
靶向治疗通过使用靶向肿瘤细胞表面特定分子的药物来阻断肿瘤细胞的生长和扩散。
免疫治疗通过激活和增强患者自身免疫系统对抗肿瘤细胞。
基因治疗通过将特定基因引入患者体内,以修复或改变肿瘤细胞的功能。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
RT 放疗 TMZ/RT 替莫唑胺或放疗 11.8 12.7 1.9% 13.8%
100 90
甲基状态的 MGMT
TMZ/RT
Median OS, mo: 15.3 21.7 2-yr survival: 22.7% 46.0%
Logrank : p = 0.062
80 70 60 50
Logrank : p = 0.0074
48.9%
23.1%
23.1%
13.8%
RT only
仅放疗
15.3 months
23.9%
7.8%
7.8%
5.2%
• Methylation of MGMT promoter is a strong predictor for outcome and benefit from temozolomide chemotherapy1,2
60戈瑞放疗与替莫唑胺联合治疗或放疗辅以佐剂替莫唑胺治疗
Unmethylated MGMT去甲基状态的MGMT
放疗 Randomization: 中位生存期:月数 Median OS, mo: 2年生存期
100 90 80
Methylated MGMT
Randomization: RT
2-yr survival:
5-yr
5年
MGMT 去甲基状态的MGMT 12.6 unmethylated months RT/TMZ 放疗或替莫唑胺治疗
14.8%
11.1%
11.1%
8.3%
RT only
仅使用放疗
11.8 months
1.8%
0%
0%
0%
MGMT 甲基化状态MGMT 23.4 methylated months RT/TMZ 放疗或替莫唑胺治疗
未治疗的预期寿命=仅数月 手术切除:可行性最大 术后治疗方法
– Untreated life expectancy = months only – Best evidence is 60Gy RT with concomitant temozolomide chemotherapy (RT/TMZ + 6 months adjuvant TMZ) – Decision factors
病因未明、遗传非唯一病因,病因还有特定职业、手机
Treatment Considerations for Newly Diagnosed Glioblastoma 新确诊多形性胶质母细胞瘤的治疗思路
• Surgical resection: maximum feasible • Post-op Therapy:
近半数患者的MGMT启动子甲基化的回顾性亚 组分析 Probability of overall survival (%): 总生存率(%) Radiotherapy plus temozolomide:放疗与替莫唑胺联合治疗 Months:月份 Radiotherapy:放疗 Treatment:治疗 OS:总生存期
40
months 月数
months 月数
MGMT Promoter Methylation: Outcomes
(Stupp Lancet Oncol. 2009; Hegi N Engl J Med. 2005)
MGMT启动子甲基化状态:结局
2-yr
2年
Median
中位生存期
3-yr
3年
4-yr
4年
• Primary study objective: determine if dose-intensifying the adjuvant temozolomide improves OS • Secondary objec替莫唑胺的剂量能否改善总生存期
替莫唑胺与放疗联合用药或作为放疗的佐剂
This trial was restricted to patients 70 years and younger
试验禁招募70岁及青年患者
Retrospective subgroup analysis of MGMT promoter methylation in about half of the patients
加拿大皇家内科医学院院士、加拿大多伦多神经肿瘤科讲席教授、医学博士詹姆斯R佩里
Prepared for KOL Luncheon, March 9, 2017, Lotte Palace Hotel, New York
供2017年3月9日于纽约乐天皇宫酒店举办的关键舆论领袖午宴使用
Disclosures
活化的MGMT
Guanine methylated by Temodal
repair by MGMT
通过MGMT修复
NH S CH 2 CH CO
由替莫唑胺甲基化的鸟嘌呤
O N N dR N NH NH 2
NH2
Inactive MGMT
失活MGMT
COOH
Normal Guanine
正常鸟嘌呤
Irreversible inactivation
MGMT启动子的甲基化状态是替莫唑胺化疗结局和获益的重要自变量 1,2
RTOG 0525/EORTC 26052-22053
• International randomized phase III clinical trial involving RTOG, EORTC and NCCTG
国际随机化3期临床试验包括RTOG、EORTC和NCCTG
Learning Objectives
学习目标 To understand current treatment standards in GBM 掌握现行多形性胶质瘤细胞治疗标准 To review the major pillars of therapy and the failures of the past 回顾核心疗法与总结失败经验
决策因素 年龄:各种放疗方案
临床证据是放疗剂量60戈瑞联合替莫唑胺化学治疗(放疗/替莫唑胺联合6个月替莫唑胺佐剂)
• Age: different RT schedules • Neurological status • MGMT promoter methylation status
MGMT启动子甲基化状态 神经系统状态
2016年5月版WHO脑瘤新分类
胶质瘤病的分子通路
Increasing Incidence of GBM
Hess et al, Cancer 101:2293-9, 2004
FBM发病率增加
Etiology unclear, rarely purely genetic (Li-Fraumeni, Turcots, NF), certain occupations, ? Cell phones
回顾VAL-083临床应用的机遇
A huge limitation is that the disease grows beyond the margins of current imaging and current therapy
Glioma: Beyond the Margins 神经胶质瘤:疾病过度增加
目前医学影像和疗法难以满足疾病增长过度的需求,这存在很大的局 限性
2017: Can’t we do a little better?
2017年:如何能再创佳绩?
New WHO Classification of Brain Tumors, May 2016 Based upon biomarkers moreso than histology
不可逆失活
MGMT Gene MGMT基因
MGMT Enzyme
MGMT酶
MGMT Gene
MGMT基因 MGMT启动子区
MGMT Promoter Region
Decreased response to TMZ treatment
Turned On
对替莫唑胺的治疗反应 减弱
X
MGMT Gene
MGMT基因
Temozolomide (Temodal, Temodar) 替莫唑胺 • • • • Well tolerated oral alkylating chemotherapy 耐受性良好的口服烷化剂化疗制剂 Mild non-cumulative myelotoxicity 非累积发生的中度骨髓抑制 Flexible schedules 灵活的方案 Level 1 evidence supporting concurrent chemoradiation and adjuvant treatment 第一级临床证据支持 放化疗与佐剂联合治疗 • Might be a radiation sensitizer 可充当放疗增敏剂 • Effective essentially only in cells harboring MGMT promoter methylation (low MGMT repair enzyme presence) – 40% of GBM
The Therapeutic Landscape of Glioblastoma - 2017
2017年恶性胶质瘤治疗概况 James R Perry MD, FRCPC Crolla Professor of Neuro-Oncology University of Toronto, Canada
信息披露
•
• •
•
• •
•
MSD Oncology (speaking honoraria) 演讲酬金赞助 Roche (advisory) 顾问 DelMar Pharma (advisory) 顾问 Vascular Biogenics (advisory) 顾问 Orbus Therapeutics (advisory, reviewer) 顾问、评审 Leadiant Biosciences (Sigma Tau) (advisory) 顾问 Midatech (UK) (advisory) 顾问