肠系膜上动脉综合征SMA
肠系膜上动脉综合征的临床研究进展

作者单位:515041汕头大学医学院第二附属医院消化内科
万方数据
着诊断技术的不断发展,其发病率也逐渐升高,开始受到越来 越多临床工作者的重视。但是由于依然有许多临床医生过份 依赖消化内镜、腹部cT平扫等先进检查手段,肠系膜上动脉 综合征的误诊率仍较高,我国有学者统计其误诊率高达 47.1%。现就其发病机制、临床表现、诊断和治疗进展作一 综述。 1发病机制
川崎病临床表现多样,因就诊时间不同,病情轻重不一, 且由于该病高热持续时间长,大部份患儿口唇破裂,应用抗生 素无效,加之缺乏该病的知识,使家长容易产生焦虑心理,故 应对患儿进行精心细致的护理,同时对家长及患儿采取有效 的健康教育,帮助他们获得该病的相关知识及护理技能,能取 得较好的效果。
肠系膜上动脉综合征护理课件
保持呼吸道通畅,避免呕吐物误吸, 及时清理呕吐物,保持口腔清洁。
04
肠系膜上动脉综合征的康复与预防
康复训练
饮食调整
遵循低脂、低糖、高蛋白的饮食 原则,避免过饱,少量多餐。
运动指导
根据病情选择合适的运动方式, 如散步、太极拳等,以增强肠道
蠕动。
心理护理
关注患者的情绪变化,提供心理 支持,帮助患者树立康复信心。
临床表现
症状
SMAS患者主要表现为饱 胀、嗳气、呕吐等症状, 可伴有腹痛、体重下降等。
体征
体检可见上腹部轻压痛, 肠鸣音活跃,有时可触及
扩张的十二指肠。
并发症
长期反复发作的SMAS可 能导致营养不良、消瘦、 疲劳等症状,严重者可出 现脱水、电解质紊乱等。
02
肠系膜上动脉综合征的护理评估
评估方法
01
避免过度进食和暴饮暴食,减少高脂肪食物的摄入,以减轻肠
道负担。期发现肠系膜上动脉狭窄
或闭塞。
积极治疗原发病
03
对于存在高血压、糖尿病等基础疾病的患者,应积极治疗原发
病,以降低并发症的发生风险。
谢谢您的聆听
THANKS
肠系膜上动脉综合征的护理措施
一般护理
01
02
03
休息与活动
保证充足的休息,避免剧 烈运动,根据病情适当安 排活动量。
心理护理
关注患者情绪变化,给予 心理支持和疏导,增强治 疗信心。
病情监测
密切观察病情变化,记录 症状发作时间和程度,及 时报告医生。
饮食护理
饮食调整
少量多餐,避免过饱,选 择易消化、营养丰富的食 物,避免坚硬、刺激性食物。
观察法
观察患者的症状表现,如腹痛、呕吐、体 重下降等。
肠系膜上动脉综合征

适当运动
定期进行适量的有氧运动,如 散步、慢跑等,有助于促进肠
道蠕动,缓解症状。
避免诱因
避免长时间站立、久坐等可能 导致腹腔内压力升高的行为,
以及过度用力等动作。
护理方法
饮食护理
遵循低脂、低糖、高蛋白的饮 食原则,避免进食过饱,少量
多餐,以减轻肠道负担。
疼痛护理
对于腹痛症状明显的患者,可 采取适当的止痛措施,如口服 止痛药或进行热敷等。
心理护理
关注患者的心理状况,给予必 要的心理支持和疏导,帮助患 者保持乐观的心态。
病情监测
定期监测患者的病情变化,如 出现症状加重或持续不缓解等
情况,应及时就医。
康复指导
健康宣教
01
向患者及家属宣传肠系膜上动脉综合征的相关知识,提高对疾
病的认识和预防意识。
康复训练
02
在医生指导下进行适当的康复训练,如腹部按摩、肠道功能训
患者男性,38岁,因反复发作性腹痛、呕吐就诊 ,经检查诊断为肠系膜上动脉综合征。
治疗经过
患者在接受保守治疗无效后,接受手术治疗,解 除肠系膜上动脉压迫,术后恢复良好。
3
治疗经验
对于保守治疗无效的患者,应尽早考虑手术治疗 ;手术方式应根据患者具体情况选择;术后应加 强营养支持治疗。
特点
SMAS多见于体型瘦长、脊柱前凸的 年轻人,尤其是女性。其主要临床表 现为饱胀、腹痛、呕吐等症状,进食 后加重,呕吐物多为胆汁。
病因与发病机制
病因
SMAS的病因主要包括解剖学因素和动力学因素。解剖学因素包括脊柱前凸畸 形、十二指肠水平部位置异常等;动力学因素包括胃肠蠕动减弱、腹腔内压下 降等。
控制并发症
对于并发感染、电解质紊乱等并 发症的患者,需积极控制并发症
肠系膜上动脉压迫综合征科普讲座课件

演讲人:
目录
1. 什么是肠系膜上动脉压迫综合征? 2. 何时出现症状? 3. 如何诊断肠系膜上动脉压迫综合征? 4. 如何治疗肠系膜上动脉压迫综合征? 5. 如何预防肠系膜上动脉压迫综合征?
Байду номын сангаас
什么是肠系膜上动脉压迫综合 征?
什么是肠系膜上动脉压迫综合征?
定义
肠系膜上动脉压迫综合征(SMA Syndrome)是指 肠系膜上动脉因某种原因压迫十二指肠,导致消 化道症状。
该病症通常发生在体重减轻或长期卧床后,尤其 是青少年和年轻女性更常见。
什么是肠系膜上动脉压迫综合征?
病因
主要病因包括体重减轻、先天性解剖异常、腹部 肿瘤等。
这些因素可能导致肠系膜上动脉与腹主动脉之间 的角度变小,进而压迫到周围的结构。
什么是肠系膜上动脉压迫综合征?
流行病学
该病症相对少见,确切发病率尚无明确数据,但 近年来报告有所增加。
基于症状和体重变化,医生会考虑进一步的影像 学检查。
如何诊断肠系膜上动脉压迫综合征?
影像学检查
CT扫描和MRI是常用的诊断工具,可以帮助评估 肠系膜上动脉的状态。
这些检查可以清晰显示动脉与周围结构的关系, 帮助确定是否存在压迫。
如何诊断肠系膜上动脉压迫综合征? 内镜检查
在某些情况下,内镜检查可以评估消化道的具体 情况。
定期锻炼和均衡饮食是关键。
如何预防肠系膜上动脉压迫综合征? 注意身体变化
如果出现不明原因的体重减轻或消化道症状,应 及时就医。
早期干预可以防止病情加重。
如何预防肠系膜上动脉压迫综合征? 定期体检
定期进行健康检查,尤其是有家族史或相关病史 的人群。
腹腔干(CA)肠系膜上动脉(SMA)和肠系膜下动脉(IMA)疾病

一、目的肠系膜动脉(CA/SMA/IMA)多普勒超声检查的目的是为了诊断肠系膜动脉狭窄、动脉瘤和其它病变,并确定其病变类型、部位、严重程度和波及范围。
二、适应证1. 与进食有关的腹痛。
2. 持续性腹泻。
3. 明显的、不能解释的体重减轻。
4. 腹部听诊闻及杂音。
5. 术后评价。
6. 疑似肠系膜动脉、肝动脉或脾动脉瘤。
7. 疑似中弓韧带压迫综合征。
8. 疑似肠道缺血性病变。
三、禁忌证和局限性通常无禁忌证。
但对下列患者,超声检查有一定的局限性。
1. 严重肥胖患者;2. 腹部手术影响检查的患者;3. 有引流管的患者;4. 呼吸急促;5. 严重肠道积气;6. 不能合作的患者;四、仪器彩色多普勒超声仪,探头频率2~5MHz。
五、病人准备检查前晚清淡饮食,检查前12小时内禁食,禁吸烟,禁咀嚼口香糖等;禁食后,肠系膜上动脉和肠系膜下动脉为高阻血流,进食后变成低阻血流。
对于正常人而言,无论进食与否,腹腔动脉均为低阻血流,因为腹腔动脉主要供应低阻的肝和脾毛细血管床。
患者一般取平卧位。
六、检查技术1、灰阶超声(1)腹腔动脉恰位于肝尾状叶下方,肠系膜上动脉和胰腺上方。
横切时,腹腔动脉的分支呈“海鸥征”,左翅膀是脾动脉,右翅膀是肝总动脉。
(2)肠系膜上动脉起始部在腹腔动脉起始处下方,向下走行。
(3)肠系膜下动脉在左右髂总动脉分叉处上方约3.5cm处由腹主动脉左前壁发出,向左下走行。
并不是所有患者都能显示该动脉。
2、彩色多普勒超声(1)腹腔动脉和肠系膜上动脉长轴观。
如果肠系膜下动脉能显示,也要显示其长轴观。
(2)寻找提示动脉狭窄的征象:鲜亮的高速血流、彩色混叠等。
(3)记录靠近腹腔动脉分叉处或第一肝门处的肝总动脉血流方向。
如肝总动脉或胃十二指肠动脉的血流反向,提示腹腔动脉阻塞。
(4)记录腹主动脉和髂动脉的情况。
3、脉冲多普勒(1)先用彩色多普勒检查腹腔动脉和肠系膜上动脉,寻找彩色混叠处,然后用脉冲多普勒测量混叠处的峰值流速,以及其近段和远段的峰值流速。
高热卡肠外营养治疗肠系膜上动脉综合征

高热卡肠外营养治疗肠系膜上动脉综合征肠系膜上动脉综合征(superior mesentery artery syndrome,SMAS)系指肠系膜上动脉(SMA)及其伴行的静脉压迫十二指肠水平部引起的上消化道梗阻的系列症状[1]。
我科应用高热卡肠外营养(parenteral nutrition,PN)治疗肠系膜上动脉综合征患者3例,疗效满意。
现报道如下。
1 临床资料病例1:女,27岁,因“进食后饱胀、腹痛伴消瘦1年”入院,近三月体重下降10kg。
身高158cm,体重29 kg,BMI 11.22kg/m2。
实验室检查:白蛋白(ALB)32.4g/ L。
上消化道造影(GI)示:十二指肠水平部见压迹。
入院后给予禁食、PN支持治疗。
PN方案:每天总液体量为2000-2500mL,总热量按高热卡供给146.44-188.3kJ/(kg·d)[(35kcal/kg·d)],糖脂比为1:1,氮量0.20-0.25g/(kg·d),热氮比约110:1,糖和胰岛素比例10:1,维生素、电解质、微量元素每日给予生理需要量。
配制成全合一营养液经PICC输注,1次/d。
PN输注过程中监测血糖及肝功能。
同时鼓励病人逐渐恢复饮食,由少到多,由流质到半流质再到固体食物。
持续7周后,患者梗阻症状明显缓解,体重上升7kg;逐渐减少液体量及热量供应,继续PN2周,病人梗阻症状消失,体重升至41.8kg,恢复正常饮食。
复查GI示:造影剂通过十二指肠顺利,无压迹。
复查:ALB38.8g/L。
患者PN总时间61d,症状消失,饮食恢复,复查肝功能正常,出院。
病例2:女,15岁,因“进食后上腹部饱胀伴呕吐、消瘦1年余”入院,入院前体重下降9kg。
身高159cm,体重35.5kg,BMI14.04kg/m2。
GI示:十二指肠水平部见压迹。
入院给予高热卡PN,热量供给的方案同病例1。
持续5周后,患者饱胀、呕吐症状消失,饮食正常,体重升至40.5kg,ALB43.8g/L。
肠系膜上动脉综合征病人的护理课件

演讲人:
目录
1. 什么是肠系膜上动脉综合征? 2. 病人护理的目标是什么? 3. 如何实施护理方案? 4. 护理过程中需要注意什么? 5. 护理评估的关键指标有哪些?
什么是肠系膜上动脉综合征?
什么是肠系膜上动脉综合征?
定义
肠系膜上动脉综合征(SMAS)是由于肠系膜上动 脉受压导致的消化系统问题。
药物治疗
根据医生的建议,合理使用止痛药及其他药物。
需要定期监测药物的效果及副作用。
护理过程中需要注意什么?
护理过程中需要注意什么? 病人教育
向病人及家属普及有关SMAS的知识,提高自我管 理能力。
教育内容可包括饮食、症状监测和何时就医等。
护理过程中需要注意什么? 密切观察
密切观察病人的病情变化,尤其是腹痛及胃肠道 功能。
可以通过个别咨询或小组治疗来实现。
如何实施护理方案?
如何实施护理方案?
定期评估
定期评估病人的症状及营养状态,及时调整护理 计划。
使用评估工具如NRS(数字评分量表)监测疼痛 程度。
如何实施护理方案?
饮食管理
制定个性化的饮食计划,鼓励病人少量多餐。
避免刺激性食物,选择易消化的食物。
如何实施护理方案?
及时报告异常情况,预防并发症的发生。
护理过程中需要注意什么? 团队合作
与医生、营养师、心理医生等多学科团队密切合 作,提供全方位护理。
定期召开病例讨论会,共同制定最佳护理方案。
护理评估的关键指标有哪些?
护理评估的关键指标有哪些? 疼痛评估
使用标准化工具评估病人疼痛的性质与程度。
确保病人能够准确描述其疼痛感受。
病人护理的目标是什么?
小儿肠系膜上动脉综合征诊断与治疗方法的探讨
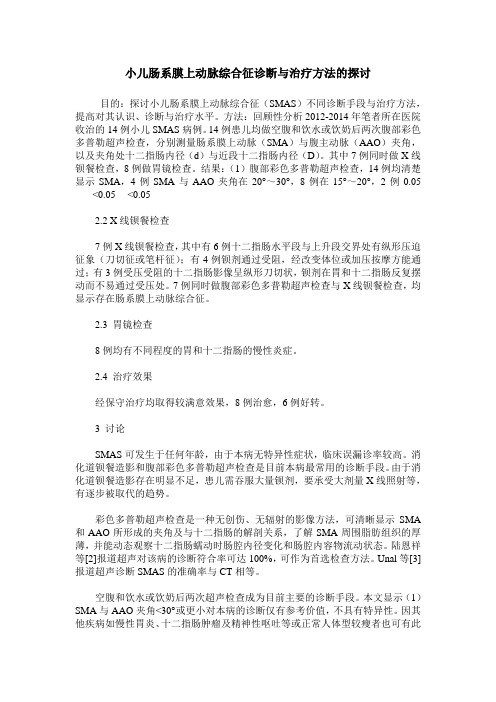
小儿肠系膜上动脉综合征诊断与治疗方法的探讨目的:探讨小儿肠系膜上动脉综合征(SMAS)不同诊断手段与治疗方法,提高对其认识、诊断与治疗水平。
方法:回顾性分析2012-2014年笔者所在医院收治的14例小儿SMAS病例。
14例患儿均做空腹和饮水或饮奶后两次腹部彩色多普勒超声检查,分别测量肠系膜上动脉(SMA)与腹主动脉(AAO)夹角,以及夹角处十二指肠内径(d)与近段十二指肠内径(D)。
其中7例同时做X线钡餐检查,8例做胃镜检查。
结果:(1)腹部彩色多普勒超声检查,14例均清楚显示SMA,4例SMA与AAO夹角在20°~30°,8例在15°~20°,2例0.05<0.05 <0.052.2 X线钡餐检查7例X线钡餐检查,其中有6例十二指肠水平段与上升段交界处有纵形压迫征象(刀切征或笔杆征);有4例钡剂通过受阻,经改变体位或加压按摩方能通过;有3例受压受阻的十二指肠影像呈纵形刀切状,钡剂在胃和十二指肠反复摆动而不易通过受压处。
7例同时做腹部彩色多普勒超声检查与X线钡餐检查,均显示存在肠系膜上动脉综合征。
2.3 胃镜检查8例均有不同程度的胃和十二指肠的慢性炎症。
2.4 治疗效果经保守治疗均取得较满意效果,8例治愈,6例好转。
3 讨论SMAS可发生于任何年龄,由于本病无特异性症状,临床误漏诊率较高。
消化道钡餐造影和腹部彩色多普勒超声检查是目前本病最常用的诊断手段。
由于消化道钡餐造影存在明显不足,患儿需吞服大量钡剂,要承受大剂量X线照射等,有逐步被取代的趋势。
彩色多普勒超声检查是一种无创伤、无辐射的影像方法,可清晰显示SMA 和AAO所形成的夹角及与十二指肠的解剖关系,了解SMA周围脂肪组织的厚薄,并能动态观察十二指肠蠕动时肠腔内径变化和肠腔内容物流动状态。
陆恩祥等[2]报道超声对该病的诊断符合率可达100%,可作为首选检查方法。
Unal等[3]报道超声诊断SMAS的准确率与CT相等。
肠系膜上动脉综合征危害及预防PPT

早期干预可以显著降低并发症的风险。
如何预防肠系膜上动脉综合征? 注意饮食
避免大量进食,尤其是油腻食物,减少对消化系 统的负担。
合理分配餐次,选择易于消化的食物。
肠系膜上动脉综合征的治疗
肠系膜上动脉综合征的治疗 保守治疗
包括营养支持、药物治疗等,适用于早期患 者。
提高公众认知
通过科普宣传,增强公众对肠系膜上动脉综合征 的认识。
早期识别和干预是改善预后的关键。
总结与展望
未来研究方向
进一步研究其发病机制和最佳治疗方案,以提高 治疗效果。
多学科合作将有助于患者的综合管理。
总结与展望
倡导健康生活方式
鼓励公众养成健康的饮食和生活习惯,降低发生 风险。
健康的生活方式是预防多种疾病的重要基础。
通过调节饮食和生活方式来改善症状。
肠系膜上动脉综合征的治疗
手术治疗
对于严重病例,可能需要手术解除压迫,恢 复血流。
手术风险需评估,通常在保守治疗无效后进 行。
肠系膜上动脉综合征的治疗 术后管理
术后需进行定期随访,监测恢复情况,防止 复发。
患者需遵循医嘱,保持良好的生活习惯。
总结与展望
总结与展望
肠系膜上动脉综合征的危害
肠系膜上动脉综合征的危害
对消化系统的影响
血供不足会导致肠道缺血,严重时可能引发 肠道坏死。
缺血性肠病是一种紧急情况,需要及时治疗 。
肠系膜上动脉综合征的危害 对营养吸收的影响
患者可能因为进食困难而导致营养不良,影 响身体健康。
长期的营养不良可能导致多脏器功能受损。
肠系膜上动脉综合征的危害 心理影响
长期的腹痛和不适会导致患者情绪低落、焦 虑等心理问题。
肠系膜上动脉综合征的临床研究进展

肠系膜上动脉综合征的临床研究进展作者:岑川黄聪武来源:《中国实用医药》2010年第11期【摘要】肠系膜上动脉综合征(SMAS)是指肠系膜上动脉或其分支压迫十二指肠水平段引起的餐后恶心、呕吐、腹胀和腹痛等临床症状,是十二指肠雍积症最常见的病因。
最常见的病因包括先天因素和后天因素导致的肠系膜上动脉和腹主动脉之间夹角变小。
X线钡餐造影和腹部彩色超声是主要的检查方法,内科营养支持等保守治疗仍是首选治疗方法,保守治疗失败者可首选十二指肠空肠吻合术或屈氏韧带松解下移术。
此文主要从病因、发病机制、临床诊断及治疗等方面对SMAS作一综述。
【关键词】肠系膜上动脉综合征;诊断;治疗肠系膜上动脉综合征(superior mesenteric artery sydrome,SMAS)是指肠系膜上动脉(superior mesenteric artery,SMA)或其分支(如:结肠中动脉)压迫十二指肠水平部引起的急、慢性肠梗阻,某些急性梗阻型可引起急性胃扩张,又称为十二指肠动脉压迫综合征,以反复发作的餐后恶心、呕吐、腹痛和腹胀等为主要临床表现,是十二指肠壅积症(duodenal stasis)最常见的病因(约占50%)[1,2],属于良性十二指肠雍积症。
其概念最早由Rokitansky在1861年提出,但直到1927年Wilkie等报道后才引起重视,故SMAS亦称Wilkie病[3]。
近年来随着诊断技术的不断发展,其发病率也逐渐升高,开始受到越来越多临床工作者的重视。
但是由于依然有许多临床医生过份依赖消化内镜、腹部CT平扫等先进检查手段,肠系膜上动脉综合征的误诊率仍较高,我国有学者统计其误诊率高达47.1%。
现就其发病机制、临床表现、诊断和治疗进展作一综述。
1 发病机制十二指肠、肠系膜上动脉(SMA)与腹主动脉(AO)三者的解剖关系与SMAS的发生有密切关系。
SMA约在第一腰椎水平起源于AO,在立位或卧位时,向下向右行走于小肠系膜内,与AO形成一锐角,并在进入小肠系膜前跨过十二指肠水平部。
脉综合征围论文:肠系膜上动脉综合征围手术期护理体会

脉综合征围论文:肠系膜上动脉综合征围手术期护理体会【关键词】肠系膜上动脉综合征护理肠系膜上动脉综合征(superior mesenteric artery compressing syndrome, smas)又称良性十二指肠淤滞症, 是由于肠系膜上动脉压迫十二指肠水平部引起梗阻而出现的一组临床病症[1]。
2008 年1 月~2010年9 月,我院曾对12例患肠系膜上动脉压迫综合征的患者施行手术治疗,对患者进行系统的整体护理,使患者更好地配合手术治疗,减少术后并发症的发生,提出了更高的要求,现将围手术期护理报道如下:1 临床资料1.1 一般资料本组病例12例,男7例,女5例,年龄16~43岁,平均年龄28.7岁。
病程5个月~16年,平均3.9年。
其中体型瘦长者7 例( 58.33% ) ,10 例( 83.33% ) 呈慢性发作,表现为反复发作性餐后上腹部胀痛、恶心、呕吐, 多发生在餐后15~40 min,呕吐物以胃内容物为主,酸臭,含胆汁及隔餐食物,无粪臭味。
呕吐后症状明显减轻,进食常为呕吐之诱因,其中11例( 91.67% ) 餐后更换体位( 膝胸卧位或俯卧位) 时症状可明显缓解;9例(75.00%)因长期反复发作而呈消瘦、体重明显减轻;11 例( 91.67% ) 有振水音;6 例( 50.00% ) 可见胃形和蠕动波。
本组所有病例均行手术治疗,其中2例行treitz韧带切断松解术,9例行十二指肠空肠吻合术,1例行十二指肠空肠roux—en—y吻合术。
1.2 结果本组12例患者均痊愈出院,经1-18个月随访,效果良好,本组患者未发生吻合口溃疡及吻合口狭窄等并发症,无一例发生反流性胃炎。
2 护理2.1 术前护理2.1.1 患者准备(1)常规检查:血、尿常规,出凝血时间,肝肾功能,肝炎系列,艾滋病抗体,血糖,心电图,胸片;(2)改善全身营养状况,纠正电解质紊乱。
2.1.2 心理护理术前应详细介绍麻醉方式、手术方法的选择,优点,适应证。
肠系膜上动脉压迫综合征 病情说明指导书

肠系膜上动脉压迫综合征病情说明指导书一、肠系膜上动脉压迫综合征概述肠系膜上动脉压迫综合征(Superior mesenteric artery syndrome,SMAS)是因肠系膜上动脉或其分支动脉压迫十二指肠水平部,进而引起一系列急、慢性十二指肠梗阻症状的一种疾病,亦称良性十二指肠淤滞症、十二指肠血管压迫综合征或 Wilkie 综合征。
可由多种病因引起,腹主动脉(AO)、肠系膜上动脉(SMA)及十二指肠三者解剖关系出现异常是其发病基础。
因其无典型临床表现,常被误诊为胃炎、胃下垂、功能性消化不良等,误诊率高达57.1%~67.3%。
该病临床表现以反复发作的餐后恶心、呕吐、腹痛和腹胀为主。
消化道造影、腹部彩超、内镜、腹部 CT、选择性 SMA 造影、磁共振血管成像等均已成为诊断 SMAS 的有效辅助检查手段。
目前以保守治疗为主,预后一般。
英文名称:superior mesenteric artery syndrome ,SMAS其它名称:良性十二指肠淤滞症、十二指肠血管压迫综合征、Wilkie 综合征相关中医疾病:腹痛ICD 疾病编码:暂无编码。
疾病分类:暂无资料。
是否纳入医保:部分药物、耗材、诊治项目在医保报销范围,具体报销比例请咨询当地医院医保中心。
遗传性:无遗传相关性发病部位:腹部-十二指肠常见症状:反复发作的餐后恶心、呕吐、腹痛、腹胀主要病因:解剖结构异常、恶性肿瘤、胃下垂、淋巴结肿大、医源性因素检查项目:体格检查、立位腹平片、血常规检查、便常规+潜血试验、肿瘤标志物检查、上消化道造影、腹部彩超、胃镜检查、胃黏膜组织活检、SMA 造影重要提醒:慢性肠系膜上动脉压迫综合征病程长、病情重,可进一步加重原发病,形成恶性循环,需引起重视。
外科脊柱矫形手术是诱发该病的主要危险因素,应当及时就医治疗。
临床分类:基于发病情况分类:1、急性肠系膜上动脉压迫综合征急性肠系膜上动脉压迫综合征较少见,其发生多与创伤、躯干石膏固定、牵引、卧于过度伸展的支架之上有关。
烧伤后肠系膜上动脉综合征
【疾病名烧伤后肠系膜上动脉综合征称】【英文名superior mesenteric artery syndrome after burn称】【别烧伤后肠系膜上动脉综合症名】烧伤/烧伤内脏并发症/烧伤后消化系统并发症【类别】【 ICD 号】K55.1【概述】肠系膜上动脉综合征(superior mesenteric artery syndrome)是由肠系膜上动脉压迫十二指肠横部而引起的综合征,其特征为胃、十二指肠球部和降部扩大、内容物滞留。
烧伤后发生肠系膜上动脉综合征是严重烧伤患者高代谢造成极度消瘦的结果。
本症多发生于伤后3周以后,体重下降10%以上的病人。
若体重下降不及5%,一般不会发生肠系膜上动脉压迫综合征。
从1972年以后,严重烧伤患者合并肠系膜上动脉综合征时有报道。
美国Brooke陆军外科研究所烧伤中心报告1678例严重烧伤患者中有19例发生肠系膜上动脉综合征,发病率约1.12%。
国内方之杨等报告了3122例烧伤患者中仅有5例发生肠系膜上动脉综合征(0.16%)。
【流行病学】【病因】【发病机制】1.解剖因素十二指肠横段(即第四段)位于肠系膜上动脉与腹主动脉构成的夹角内,它自右向左在腹主动脉前方横过第三腰椎前方被后腹膜固定,连接十二指肠升段的空肠曲为屈氏韧带所固定。
腹主动脉在第一腰椎平面分出肠系膜上动脉,该动脉在胰腺下通过,分出结肠中动脉后跨越十二指肠。
正常成年人的夹角平均为56°(范围47°~60°),从夹角顶点到十二指肠之间的距离平均为14cm。
如果夹角过小,十二指肠就会被肠系膜上动脉和腹主动脉夹住而发生十二指肠梗阻。
严重烧伤合并肠系膜上动脉综合征的患者,据测量夹角平均为14.6°,间距平均为2.3cm。
烧伤和严重脓毒症患者因高代谢反应,负氮平衡、体重下降或营养不良,引起脂肪分解以补充能量不足,使肠系膜及腹膜后脂肪明显减少。
此外,患者因长期平卧,致肠系膜上动脉牵拉,使腹主动脉和肠系膜上动脉的夹角变小,肠系膜上动脉压迫其后的十二指肠,发生十二指肠梗阻。
肠系膜上动脉夹层的护理常规(修改)

肠系膜上动脉夹层的护理常规【相关知识】肠系膜上动脉 (Superior mesentericartery ,SMA )夹层系动脉腔内的血液渗入动脉壁中层与外层之间形成夹层血肿,沿动脉壁延伸剥离导致血管严重损害的一种急症,是临床上少见的疾病,自1947 年Bauersfeld 发现第1例以来,近年来临床上报道逐年增多。
【治疗原则】除了出现肠道缺血坏死和 SMA 破裂者需要立即行开放手术外,其余患者均给予保守治疗。
经保守治疗后腹痛不缓解或C T A 提示夹层范围进展等情况时,给予腔内介入治疗。
对于解剖条件不适合或腔内治疗失败的患者,可考虑开放性手术治疗。
一、保守治疗1. 禁食水,必要时行胃肠减压,液体支持,密切观察病情变化及对症止痛处理。
2. 合并高血压者控制血压到合理的水平(130/80 mmHg 以下)。
3. 同时皮下注射低分子肝素钙注射液抗凝治疗,待病情平稳后,改用口服华法林抗凝(控制I NR 达到2~3)治疗,及口服阿司匹林100mg/d,防止血栓形成导致S MA 狭窄,也有应用抗血小板治疗者,避免肠系膜上动脉主干真腔及分支动脉继发血栓形成。
二、腔内支架治疗采用 Seldinger 技术常规穿刺股动脉,常规行腹腔干、肠系膜上下动脉造影。
根据造影结果,评价夹层部位、程度及肠道血供情况,导丝导管交换引入导引导管,送入支架,在狭窄处释放,再次造影,观察支架扩张、局部血流、周围分支动脉情况。
术后长期口服氯吡格雷(波立维)抗血小板治疗。
三、手术治疗常用术式包括:1. 腹主动脉-肠系膜上动脉旁路转流术2. 动脉内膜切除+补片成形术3. 切除已明确坏死的肠管【护理】一、术前护理(一)术前评估1. 健康史和相关因素(1)有无家族史(2)生活方式:吸烟,饮酒史(3)年龄、职业、体重、营养状况、排便情况(4)过去史:近期手术,目前用药情况(高血压,糖尿病,心脏疾病血管疾病;呼吸系统疾病)(5)活动耐力和自理能力(6)腹痛情况(7)全身皮肤黏膜情况(8)心理和社会支持状况(认知程度,心理承受程度和社会支持系统)2. 专科症状体征(1)生命体征(2)腹痛的部位,性质,时间和程度,有无休克症状及血液的异常。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
superior mesenteric artery syndrome is a very rare, life-threatening gastrovascular disorder characterized by a compression of the third portion of the duodenum by the superior mesenteric artery.
Mortality SMA syndrome is estimated to have a mortality rate of 1 in 3. Delay in the diagnosis of SMA syndrome can result in: fatal malnutrition dehydration oliguria electrolyte abnormalities hypokalemia acute gastric rupture intestinal perforation (from prolonged mesenteric ischemia) gastrectasia
causes
The syndrome is typically caused by an angle of 6-25°between the AA and the SMA, in comparison to the normal range of 38-56°due to a lack of retroperitoneal and visceral fat. In addition, the aorto-mesenteric distance is 2-8 millimeters, as opposed to the typical 10-20.
SMA syndrome was first described in 1861 by Carl Freiherr von Rokitansky in victims at autopsy, but remained pathologically undefined until 1927 when Wilkie published the first comprehensive series of 75 patients.With only about 500 reported cases in the history of English-language medical literature,SMA syndrome is estimated to have a mortality rate of 1 in 3.
Symptoms
This, in turn, increases the duodenal compression spurring a vicious cycle. Symptoms are partially relieved when in the left lateral ,prone or knee-to-chest position.
Less common surgical treatments for SMA syndrome include Roux-en-Y duodenojejunostomy, gastro-jejunostomy and lysis of the ligs first robotically-assisted intestinal bypass for SMA syndrome was performed on July 30, 2008 at the London Health Sciences Centre in Ontario, Canada.
Treatment
Conservative treatment should be attempted first, involving the reversal or removal of the precipitating factor with proper nutrition and replacement of fluid and electrolytes. Pro-motility agents such as metoclopramide may also be beneficial.
rapid linear adolescent growth spurt, weight loss starvation catabolic states(cancer and burns).
early satiety nausea bilious vomiting extreme"stabbing" postprandial abdominal pain (due to both the duodenal compression and the compensatory reversed peristalsis) severe malnutrition with spontaneous wasting.
Diagnosis postprandial abdominal pain nausea bilious vomiting wasting symptoms relieved via the left lateral ,prone or knee-to-chest position upper gastrointestinal barium abdominal and pelvic CT scan with contrast
SMA syndrome is also known as Wilkie's syndrome, cast syndrome, mesenteric root syndrome, chronic duodenal ileus It is distinct from Nutcracker syndrome,which is the entrapment of the left renal vein between the AA and the SMA.
Symptoms are often aggravated when leaning to the right or taking a supine position.
Demographics
SMA syndrome is extremely rare, evident in only 0.013 - 0.3% of uppergastrointestinal-tract barium studies. As the syndrome involves a lack of essential fat, four of every five afflicted are underweight, often to the point of sickliness and emaciation. Females are impacted twice as often as males, with 75% of cases occurring between the ages of 10 and 30.
Risk anatomic factors such as:
very thin or lanky body build, an unusually high insertion of the duodenum at the ligament of Treitz, a particularly low origin of the SMA.
If conservative treatment fails, or if the case is severe or chronic, surgical intervention is required. The most common operation for SMA syndrome, duodenojejunostomy, was first proposed in 1907 by Bloodgood.
Retroperitoneal fat and lymphatic tissue normally serve as a cushion for the duodenum, protecting it from compression by the SMA. SMA syndrome is thus triggered by any condition involving an insubstantial cushion and narrow mesenteric angle.SMA Syndrome can present in two forms: chronic/congenital or acute/induced .
Predisposition easily aggravated such as
poor motility of the digestive tract retroperitional tumors cachexia exaggerated lumbar lordosis visceroptosis abdominal wall laxity peritoneal adhesions abdominal trauma
Upper gastrointestinal series showing extreme duodenal dilation (white arrow) abruptly preceding constriction by the SMA
Abdominal and pelvic CT scan showing duodenal compression (black arrow) by the abdominal aorta and the superior mesenteric artery.