吲哚布芬(美国胸科协会抗血小板药物指南)
抗血小板药物介绍

抗血小板药物介绍因血小板的激活与聚集在动脉粥样硬化血栓形成中具有重要作用,故抗血小板是治疗冠心病关键。
抗血小板药物分类介绍如下:一:血小板环氧化酶(COX)-1抑制剂:①阿司匹林:不可逆地抑制COX-1阻止血栓素A2合成及释放,抑制血小板聚集;不同剂量阿司匹林可达到不同效应:小剂量阿司匹林(75-300mg/日)具有抗血小板作用;最佳剂量范围为75~150mg/d(常用剂量为100mg/d),急性情况下需至少首剂150mg负荷量。
中等剂量阿司匹林(500mg-3g/d)有解热镇痛效应;大剂量超过4g/d具有消炎及抗风湿作用。
改善阿司匹林耐受性方法包括:服用肠溶剂型;清除胃幽门螺杆菌,同时服用胃黏膜保护药。
②吲哚布芬:可逆性地抑制 COX-1,对前列腺素抑制率较低,胃肠道反应较小、出血风险较低,可考虑作为出血及胃溃疡风险高等阿司匹林不耐受者的替代治疗。
用药方法:每次100-200mg ,每日两次,饭后口服。
65岁以上老年患者及肾功能不全患者每天100-200mg为宜。
二:P2Y12受体抑制剂:二磷酸腺苷(ADP)是血小板活化与聚集过程中重要激动剂。
P2Y12受体抑制剂能阻碍ADP与血小板表面受体结合,有效减弱ADP级联反应,降低血小板聚集。
常用P2Y12受体抑制剂主要为氯吡格雷和替格瑞洛。
①氯吡格雷为前体药物,经肝脏细胞色素 P450酶代谢活化后,与P2Y12受体不可逆地结合,减少ADP介导的血小板激活和聚集。
负荷剂量需6~8h达到最大抑制效果(600mg负荷量2~6h起效),半衰期为6h。
常用维持剂量为75mg,每日1次口服。
氯吡格雷联合阿司匹林较单独使阿司匹林显著减少急性心肌梗死者不良心血管事件,且大出血事件发生率无明显增加。
氯吡格雷抗血小板疗效个体差异较大,部分表现低反应或无反应(即氯吡格雷抵抗),该现象受细胞色素P450酶基因(如 CYP2C19)多态性影响。
氯吡格雷抵抗者用常规剂量氯吡格雷无法达到预期血小板抑制效果,与缺血事件风险增高相关。
使用吲哚布芬或阿司匹林-双嘧达莫进行抗血小板治疗对冠状动脉旁路移植一年后移植物通畅性的影响
吲哚布芬是苯丁酸衍生物,通过可逆性抑制血小板环氧合酶来抑制血小板聚集。 14,15 阿司匹林不可 逆性地乙酰化环氧合酶,而吲哚布芬的药效时间较短,在停服吲哚布芬后,血小板功能在 24 小时内恢复。 16 另外,吲哚布芬对出血时间的影响比较温和。 17,18
I 组中有 278 名患者的随访血管造影结果可以使用,AD 组有 274 名,即占两个治疗组中随机患者的 69%。在那些进行随访血管造影的患者中,每组中有 3 名患者违反研究协议,I 组中有 135 名、AD 组中有 141 名不依从治疗。
移植物闭塞数据
I 组中有 169 名患者在术后 44 到 60 周时进行血管造影,AD 组有 159 名(分别占血管造影患者的 61% 和 58%);I 组中有 107 名(38%),AD 组中有 112 名(41%)在术后 60 周后进行血管造影。手术和血管 造影间最长的间隔期限为 98 周。只有三名患者(I 组中 1 名,AD 组中 2 名)在术后 44 周前接受血管造 影。每组中有一名患者未记录从手术到血管造影的时间。
所有患者在参加试验前都要签署知情同意书。此试验遵守赫尔辛基宣言的原则,并获得每个中心当地 伦理委员会的批准。
研究治疗和合并用药
手术前患者随机接受研究治疗。术前两周停用阿司匹林或其他任何血小板活性药物。
研究服药方案为口服吲哚布芬,200mg,2 次/天(I 组)和阿司匹林,300mg,3 次/日+双嘧达莫 75mg, 3 次/日(AD 组)。术前 24 小时开始服用吲哚布芬和双嘧达莫,手术前晚服用单次剂量的阿司匹林。如果 患者不能吞咽,则使用鼻胃管给药。之后继续进行 12 个月的规律研究治疗,安排随访的血管造影。吲哚 布芬、阿司匹林、双嘧达莫和对应的安慰剂由英国 St. Albans 的 Farmitalia Carlo Erba 公司提供。
吲哚布芬片说明书

吲哚布芬片意大利说明书翻译吲哚布芬片200mg药理:抗血小板药物适应症:具有抗血小板的作用,可以预防血栓发病如:心脑血管缺血、动脉粥样血栓、静脉血栓、血脂异常、预防体外血栓形成(血液透析);禁忌症:对吲哚布芬或任何一种辅料过敏的患者禁用;有胃溃疡、胃炎、十二指肠炎的患者禁用;肝、肾功能不全的患者禁用;对乙酰水杨酸或其他非甾体抗炎药有出血或过敏的患者禁用;不应给予患者诱发哮喘、鼻炎和荨麻疹的药物;注意事项:可能发生胃不适(如胃炽热、心口痛),我们建议减小剂量或停药作为临时治疗;口服治疗建议饭后服用;药物相互作用:与其他药物联合使用应该告知医生或药剂师,获得处方;由于吲哚布芬高蛋白结合率,对于二型糖尿病治疗口服降糖药如磺脲类药物应定期检查血糖水平;出于同样原因,口服抗凝药(香豆素衍生物)或肝素,定期测定凝血酶原时间;特别警告:胃肠道病变或使用其他抗血小板、非甾体镇痛药须谨慎使用该产品,可能发生消化不良(胃炽热,上腹疼痛)建议减小剂量或临时中断治疗,不同程度肾功能损伤同样减小剂量或中断治疗;勿让儿童误食,如果发生过敏反应、荨麻疹、治疗应当停止;肾功能衰竭的患者应酌情减少用药剂量;采取以下建议作为指导,肌酐清除:> 80 ml/min 100-200 mg 每天两次;40-80 ml/min: 100 mg/d - 100 mg每天两次;< 40 ml/min: 100 mg 隔日- 100 mg/天;老年患者,随着年龄的增长,应该考虑到肾功能的问题;机理:没有文献证明作用机理;怀孕和哺乳期妇女:虽然动物实验显示对胎儿不影响,但是不推荐使用,妊娠和怀孕哺乳期妇女慎用;一些成分的重要信息:一些医生认为该产品含有一些糖类物质;剂量和给药方法:每日剂量通常为:200-400mg口服,低剂量(200mg/天)特别适合长期治疗。
老年患者的用药剂量必须小心评估,65岁以上的老年患者建议剂量为100-200mg/天,口服,饭后服用。
吲哚布芬——心内科标准版(4)

血小板因子3(PF3)是血小板活化过
程中形成的一种膜表面磷脂,是人体凝血 的重要组成部分 血小板因子3(PF3)是凝血因子V的
固定部位,可加速凝血酶(凝血因子IIa)
的生成,促进凝血过程 Ⅸa与Ⅷ因子和PF3 及Ca2+(凝血因子 IV) 组成Ⅷ因子复合物,即可激活Ⅹ因子生 成Ⅹa 在Ca2+ 存在的条件下,Ⅹa因子、Ⅴ 因子与PF3形成复合物,此即凝血活酶(凝 血因子IIa)。在凝血酶作用下,纤维蛋白 原(凝血因子I)转变为纤维蛋白
吲哚布芬—— 抗栓新选择!
杭州中美华东制药有限公司
目录
一、吲哚布芬简介 二、预防冠心病——吲哚布芬有效更安全 三、预防房颤卒中——吲哚布芬更便捷 四、吲哚布芬的临床价值
一、吲哚布芬简介
基本信息
(±)2-[4-(1-氧代-2-异二氢吲哚基)苯基]丁酸
名称
类型
吲哚布芬 /Indobufen
选择性、可逆性的环氧化酶抑制剂,抗 血小板聚集药物。
Diabetes
29.0%
1.3%
UA
*Antiplatelet Therapy Discontinuation
Prior Brachy
Renal Failure
Bifurcations
ULM
*Premature discontinuation, From Milan/Sieburg Experience ACC 05/ JAMA-05
4.6 4.3
12.3
2.6
氯吡格雷+华法林
Lancet. 2009; 374:1967-1974.
四、吲哚布芬的临床价值
ACS合并AF患者三联疗法出血风险高
late major bleeding (LMB) [> 48 h]
吲哚布芬(易抗凝)

吲哚布芬(易抗凝)
【药理与适用症】: 吲哚布芬可抑制引起血小板激活的一些因子(如AD P、5-HT、血小板因子4、β―小板球蛋白等)的释放以及影响花生四烯酸代谢而抗血小板聚集,但不影响PGI2的血浓度。
对血液凝固的各种参数无影响,但能中等度地延长出血时间,停药后即可恢复。
口服后吸收迅速,血浆浓度达峰时间2小时;t1/2为8小时;与血浆蛋白结合率为99%。
用于动脉硬化所致的缺血性心、脑血管和周围血管疾病、静脉血栓形成、血酯代谢障碍等;也可用于体外循环手术时防止血栓形成。
【注意事项】: 偶有上腹不适、腹胀、胃肠道出血和鼻衄。
有时出现过敏反应(荨麻疹)。
禁用于有出血性疾病、妊娠及哺乳妇。
【用法与用量】: 每日剂量200―400mg,分2次口服或肌注或静注。
老人及肾功能不全者宜减半。
【包装】: 片剂:每片200mg。
注射液:每支200mg(2ml)。
中国卒中杂志,吲哚布芬在抗血小板治疗中的临床应用

生化功效还是临床有效性方面都与标准剂量 事件的情况。结果发现,二级缺血事件(卒中、
的阿司匹林具有可比性[3]。现就吲哚布芬抗血 心肌梗死、TIA、血管性死亡)的发生率,吲哚
中国卒中杂志 2013年9月 第8卷 第9期 787
布芬组显著低于未治疗组(9.5% vs 28.6%,P 组复发性卒中(包括所有重大的/ 致命的缺
TIS S)[5]中,对1632例发病1个月内的小卒中、 且在接受吲哚布芬的治疗者中所有的出血事件
TIA或者一过性黑 的患者,随机分为口服吲 (不包括脑出血)显著低于接受华法林的治疗
哚布芬(200 mg/d)和噻氯匹定(250 mg/d) 者(0.6% vs 5.1%,P<0.01)。可见,在预防患
对照组(n =32)。观察组患者术后给予吲哚布 芬200 mg bid,服用3 d后改为100 mg bid,氯 吡格雷首剂300 mg qd,以后改为75 mg qd;
study[J]. Thromb Haemost, 1993, 69:1349-1358. 5 Be rga ma sco B, Be n na P, Ca rolei A , et al. A
【Key Words】 Indobufen; Thromboembolic disease; Antiplatelet
血栓栓 塞 性 疾 病是 一类 影响心、脑、外 小板聚集作用在临床中的应用做一综述,以期
周血管的全身系统性疾病,分为动脉性和静 临床工作者更加关注血栓栓塞性疾病的抗血
脉性,临床上以缺血性卒中、心肌梗死、肺栓 小板治疗。
明对于阿司匹林过敏的冠脉PCI术后患者,应 用吲哚布芬联合氯吡格雷优于单独使用氯吡格 雷。另外,国内的一项研究[12]将64例PCI术后患 者随机分为吲哚布芬联合氯吡格雷治疗的观 察组(n =32)和阿司匹林联合氯吡格雷治疗的
辛贝(吲哚布芬)临床试验综述,最新应用

吲哚布芬在治疗血栓形成国内外临床试验综述首都医科大学附属北京安贞医院神经内科 100029【点睛】本文就吲哚布芬片在预防动脉硬化引起的缺血性心血管病变、缺血性脑血管病变、静脉血栓形成和间歇性跛行研究中的优势、特点进行综述。
【摘要】吲哚布芬片(Indobufen Tablets)通过可逆性、选择性的抑制血小板黏附、活化和聚集过程中多个促血栓形成成分的生成、数量和活性,达到快速有效阻止血栓形成的作用。
本文对比分析33篇相关文献,对有效性和安全性做出综述。
【关键词】吲哚布芬;临床有效性;安全性;血管栓塞;卒中;1、临床试验总结1.1生物药剂学研究总结急性毒性试验:LD50:380mg/kg(rat) 700—850mg/ke(mouse);长期毒性试验:1m5g/kg·14mon (rat) 80mg/kg·52wks(baboo);结果表明:吲哚布芬无致突变及生殖毒性,无溶血、过敏、肌肉及血管刺激作用[1,2]。
1.2临床药理学研究总结1.2.1药代动力学(PK)研究:吲哚布芬片口服吸收快,2小时后血浆浓度达峰值小时,血浆蛋白结合率>99%,75%~80%药物以葡萄糖酸结合物(glucuronide)形式随尿排泄,部分以原形排出;一次口服吲哚布芬片200mg后2小时达最大抑制作用,12小时后仍有显著抑制作用(90%),24小时内恢复[3];老年人和肾功能不全患者吲哚布芬的清除明显延长,因此给药剂量应该减小[4]。
1.2.2药效学(PD)研究总结吲哚布芬是一种旋光性复合物,其中S对映体起主要的抗血小板聚集作用[5,6]。
消旋体和S对映体抑制环氧化酶的能力没有明显差异。
可逆性抑制血小板环氧化酶(COX),减少血小板强效激活剂血栓素A2生成,增加前列环素生成,抑制血小板被活化[7];选择性抑制二磷酸腺苷(ADP)、肾上腺素、血小板活化因子、胶原和花生四烯酸诱导血小板聚集作用,抑制血小板聚集;选择性降低血小板三磷酸腺苷、血清素、血小板因子3、血小板因子4和β-凝血球蛋白(β-TG)的水平,抑制血小板黏附[8];抑制血小板膜糖蛋白GP Ⅱb-Ⅲa[9]抑制由多种途径所诱导的血小板聚集;有效改善红细胞变形能力[10];显著改善微循环指标(皮肤、静脉、小动脉血流)[11、12]。
新型抗血小板药物吲哚布芬,能否代替阿司匹林?
新型抗血小板药物吲哚布芬,相比于阿司匹林,有这四大优势提起来吲哚布芬,想必大家并不熟悉。
但提到它的同类药物阿司匹林,想必大家耳熟能详。
二者都是一种抗血小板聚集药,都可用于血栓性疾病的二级预防用药。
虽然两种药物有很多相似之处,但是,相比于阿司匹林,吲哚布芬有这四大优势。
今天一文说清。
一、作用机制更广泛
阿司匹林只抑制环氧合酶的活性,进而产生抗血栓的作用,作用机制比较单一。
而吲哚布芬除了可逆性地抑制环氧合酶外,还可通过抑制肾上腺素、血小板活化因子、ADP和花生四烯酸诱导的血小板聚集等。
作用途径更广泛。
二、抗凝效果更强
阿司匹林对环氧合酶没有选择性,可以同时作用于COX-1和COX-2,这也导致其对血栓素的生成抑制作用不强。
而吲哚布芬能够特异性作用于COX-2,对血栓素的生成具有明显的抑制作用,效应是阿司匹林的5-10倍。
此外,吲哚布芬对多种凝血因子具有一定的抑制作用,也能起到一定的抗凝效果。
三、对胃肠道的损害更弱
由于阿司匹林对环氧合酶没有选择性,作用于COX-1后,明显抑制前列腺素的生成,而前列腺素对胃肠道黏膜具有保护作用。
因此,阿司匹林服用过程中容易出现胃肠道刺激,诱发胃肠道溃疡和出血。
而吲哚布芬由于其对环氧合酶的高度选择性,因此,相较于阿司匹林,吲哚布芬对胃肠道的不良刺激更少,安全性更高。
四、血小板恢复更
众所周知,阿司匹林停止服用后,7天后血小板功能能够完全恢复。
而吲哚布芬停药后24小时,血小板即可完全恢复正常。
因此,相对而言,前者更适合于长期预防血栓的日常使用,而后者更适合于需要手术的短期抗血小板治疗。
吲哚布芬——心内科标准版(4)
二、预防冠心病——吲哚布芬有效更安全
与氯吡格雷联合治疗非ST段抬高型急性冠脉综合征疗效显著,安全可 靠(n=70)
0
结果:治疗组(IND 100mg bid+CPG 75mg qd)复合终点显著低于 对照组(ASA 100mg qd+CPG 75mg qd, P <0. 05) 。 结论:吲哚布芬联合氯吡格雷治疗非 ST 段抬高型急性冠脉综合征患者疗效显 著,心血管事件发生率低,安全、可靠。
Fuster V, et al. Journal of the American College of Cardiology, 2011, 57(11): e101-e198.
目录
一、吲哚布芬简介 二、预防冠心病——吲哚布芬有效更安全 三、预防房颤卒中——吲哚布芬更便捷 四、吲哚布芬的临床价值
四、吲哚布芬的临床价值
对血小板血栓素合成的影响:吲哚布芬可逆抑制血栓素的合成
100 90 80 70 60 50 40 30 20 10 0
98%
血小板血栓素合成抑制率(%)
89%
47%
2h
12h
24h
结果:吲哚布芬2h内抑制血小板血栓素合成,12h仍然显著,但在 24h时可逆。
Davi G, et al.Curr Ther Res 1988,43(6):1031-7.
目录
一、吲哚布芬简介 二、预防冠心病——吲哚布芬有效更安全 三、预防房颤卒中——吲哚布芬更便捷 四、吲哚布芬的临床价值
二、预防冠心病——吲哚布芬有效更安全
抗血小板是冠心病预防与治疗的基石 UA
NSTEMI
SIHD
STEMI
Primary
Prevention
吲哚布芬应用于PCI术后预防冠状动脉再狭窄的研究

吲哚布芬应用于PCI术后预防冠状动脉再狭窄的研究温继梨崔晓迎内蒙古医学院附属医院急救中心摘要:目的:探讨吲哚布芬对PCI术后患者的冠状动脉再狭窄的预防疗效。
方法:对入选的64例PCI术后患者随机分为观察组(n=32)和对照组(n=32),观察组给予吲哚布芬和氯吡格雷,对照组给予阿司匹林和氯吡格雷,进行为期6个月的观察。
6个月后行冠脉造影,对两组患者的再狭窄率进行比较,对两组间的临床安全性进行比较。
结果:观察组和对照组PCI术后6个月的冠脉再狭窄率相当(P>0.05),两组间比较临床安全性,观察组的安全性优于对照组。
结论:吲哚布芬与氯吡格雷联合使用预防冠状动脉再狭窄与阿司匹林联用氯吡格雷疗效相当,具有更好的临床应用安全性。
关键词:吲哚布芬氯吡格雷冠状动脉再狭窄中图分类号:R543.3 文献标识码:BTo explore the prevention effect of indobufen on PCI patients with coronary artery restenosis.Wen jili Cui xiaoyingEmergency Center of the Affiliated Hospital of Inner Mongolia Medical CollegeAbstract: Objective:To explore the prevention effect of indobufen on PCI patients with coronary artery restenosis. Methods: 64 patients with PCI were selected and randomly divided into the experiment group ( n = 32) and control group ( n = 32). The patients in experiment group were given anti-platelet indobufen and clopidogrel , in control group were given aspirin and clopidogrel for 6 months. After 6 months ,coronary angiography were done, two groups of patients with restenosis rates were compared between the two groups, to compare the clinical safety.Results: After 6 months, coronary restenosis rate ( P > 0.05) were similar in the experiment group and the control group , between the two groups clinical safety, the safety of experiment group was better than the control group. Conclusion: The prevention effect of coronary artery restenosis were similar in patients between Indobufen、Clopidogrel and Aspirin、Clopidogrel, but the Indobufen and Clopidogrel was more safe.Key words: Indobufen Clopidogrel Coronary artery restenosis近年来随着冠心病介入(Percutaneous Coronary Intervention ,PCI)技术的逐渐成熟和广泛应用,冠心病患者闭塞的血管得到及时开通,既减少了心肌梗死的面积改善了冠心病患者的预后,又降低了冠心病的死亡率。
吲哚布芬在预防血栓栓塞性疾病中的研究进展
吲哚布芬在预防血栓栓塞性疾病中的研究进展
刘延俊;李如意;杜荣品
【期刊名称】《临床合理用药杂志》
【年(卷),期】2021(14)1
【摘要】血栓栓塞性疾病是目前影响人类心、脑、外周血管等常见的一大类疾病,严重威胁人类的身心健康,快速抑制血小板的活化及凝血机制的形成是治疗血栓性
疾病的首要任务。
其中吲哚布芬作为一种抗血小板及新型的抗凝药物,可以有效地
阻断血小板聚集,减少血栓的形成,在血栓栓塞性疾病的预防和治疗中有一定的疗效。
文章就吲哚布吩在预防血栓栓塞性疾病中的作用机制及临床应用做一综述,以期对
临床治疗提出更多参考。
【总页数】3页(P176-178)
【作者】刘延俊;李如意;杜荣品
【作者单位】华北理工大学研究生学院;河北省人民医院心内科
【正文语种】中文
【中图分类】R73
【相关文献】
1.吲哚布芬治疗血栓性疾病研究进展
2.吲哚布芬在非瓣膜性房颤至心源性脑栓塞二级预防中的作用研究
3.吲哚布芬在心源性脑栓塞二级预防中的作用研究
4.吲哚布
芬与拜阿司匹林在预防PICC相关深静脉血栓中的疗效分析5.吲哚布芬在阿司匹林不耐受老年缺血性心脑血管疾病二级预防中作用及安全性研究
因版权原因,仅展示原文概要,查看原文内容请购买。
辛贝——吲哚布芬产品介绍

预防动脉血栓、混合性血栓、静脉血栓等相关缺 血性疾病治疗:
动脉粥样硬化引起的缺血性心血管病变(冠心病); 缺血性脑血管疾病(包括颈椎增生压迫) 心房颤动 ; 慢性肾脏病、糖尿病、高血脂症,高血压病; 冠脉旁路手术和冠心病血管支架术后(PCI);
外周动脉和静脉血栓疾病;
提高红细胞的变形能力 ;
抑制中性粒细胞活化 。
® 辛贝
吲哚布芬片 临床应用
彰显高质量抗血栓
基于循证
吲哚布芬临床研究内容:
吲哚布芬对活化血小板影响;
吲哚布芬预防心源性栓塞事件的疗效; 吲哚布芬用于短暂性脑缺血发作(TIA)的二级预防作用; 吲哚布芬在非风湿性房颤(NRAF)重要血管事件二级预防中的作用; 吲哚布芬维持大隐静脉冠状动脉旁路移植通畅性疗效及患者的耐受性; 吲哚布芬对间歇性跛行的疗效; 吲哚布芬上市后的安全性监测。
ACCP 7
意大利心房颤动研究所Morocutti C《卒中》
辛贝®100mg全面抗栓 在CABG患者术后应用中出血量更少,更安全
吻合口通畅率比较(30天) 手术后恶性出血量比较
结论:两组在维持大隐静脉冠状动脉旁路移植通畅性方面疗效一致( 82%vs83%), 但是患者对吲哚布芬具有更好的耐受性。吲哚布芬组从手术结束到次日 早晨8:00,从手术伤口引流的血量显著低于ASA+DIP组。
血液透析时预防血栓形成。
危险因素及预防治疗
二级 预防
一级 预防
心脑血管疾病的预防效果
一、二级预防是减少心脑血管疾病事件发生的关键措施
美国哈佛大学的一项研究显示:有效预防和改善高危因素
卒中全球发生率
85 %
吲哚布芬与氯吡格雷的区别是什么

吲哚布芬与氯吡格雷的区别是什么
吲哚布芬片要比氯吡格雷好一些,吲哚布芬片抗血栓效果是氯吡格雷2-5倍,而不良反应只有氯吡格雷、波立维的1/10左右。
吲哚布芬是一种新型的抗血小板抑制药物可以可逆地抑制血小板环氧化酶-1,减少血栓素的产生。
此外,临床上可用于预防动脉硬化引起的缺血性心血管疾病、缺血性脑血管疾病也可以用于静脉血栓形成,还可以用于血液透析时预防血栓的形成。
氯吡格雷是一种非选择性环氧化酶抑制剂,能抑制血小板和内皮前列环素的产生。
而且前列环素能保护胃粘膜,一旦受到抑制,胃粘膜就容易受损,从而增加溃疡和出血的风险。
因此,吲哚布芬对胃肠道的损伤明显低于氯吡格雷,胃肠道反应较少。
因此,吲哚布芬特别适老年、高血压控制不达标、有消化道疾病史的阳性患者,因为这些人服用氯吡格雷更容易出现胃肠反应和出血风险。
而吲哚布芬对血小板聚集的抑制作用是可逆的,而氯吡格雷则是不可逆的。
可逆性是指停药后,血小板的活性可以恢复到以前,不可逆性是停药后的抑制作用可以持续五六天,也就是说如果服用氯吡格雷后需要恢复血小板的功能,血小板需要7-10天才能再生,所以一旦出血,就很难控制。
吲哚布芬的抗血小板在24小时内会消失,所以吲哚布芬的出血风险低于氯吡格雷。
即使出血,也更容易控制止血,更安全。
尤其适合择期手术的病人,术前停药时间短,24小时停药即可。
杨波教授

荆门市第二人民医院 李琳 2019年7月3日
目录
一、抗血小板药物的应用现状 二、百年经典阿司匹林 三、抗栓治疗新选择---吲哚布芬 四、吲哚布芬的安全性分析 五、吲哚布芬的有效性分析
一、抗血小板药物的应用现状
1-1
抗血小板药物是冠心病防治的基石
UA
NSTEMI
850(13.54%)
P值
NS NS NS 0.0007 <0.0001
NS,无显著性、 Gaziano JM1, et al. Lancet. 2018 Sep 22;392(10152):1036-1046.
ARRIVE研究
ARRIVE研究——研究结论
主要复合终点总体上未见减少 安全性结果也与以前的研究一致,胃肠道出血的风险增大
1:1
无CVD和糖尿病病史的 心血管病中危受试者
随机 分组
n=12546
100mg阿司匹林肠溶片,每日一次 (n=6270)
安慰剂,每日一次 (n=6276)
中位随访60个月
主要有效性终点:复合终点(心 血管死亡、心肌梗死、不稳定 型心绞痛、卒中和短暂性脑缺 血发作)的首次发生时间
主要安全性终点:出血事件和 其他不良事件
ARRIVE研究
无CVD和糖尿病病史的心血管病中危患者中 阿司匹林未能减少主要终点事件
意向治疗人群 • 阿司匹林组(4.29%)与安慰剂组(4.48%)的主要终点事件发生率 无显著差异(HR 0.96; 95%CI 0.81-1.13; p=0.6038) • 两组的次要终点发生率也无显著差异
已充分证明阿司匹林可用于心血管病的二级预防 糖尿病可增大心血管风险,但不清楚是否应该常规使用阿司匹林预防首次心血管事件的发生 另外,据推测长期使用阿司匹林可预防胃肠道癌症和其他癌症
吲哚布芬在急性心肌梗死PCI术后合并消化道大出血1例报告

CHINESE COMMUNITY DOCTORS中国社区医师2021年第37卷第6期消化道出血是在冠心病合并消化道疾病患者中经皮冠状动脉介入治疗(PCI)术后较为严重并发症之一,发生率约为1%。
PCI 术后合并消化道出血短期预后差,如何抗栓治疗是PCI 术后的关键,停用抗栓药物容易导致急性支架内血栓形成,继续使用抗栓治疗可能导致致命性消化道出血,而使临床治疗选择面临两难局面。
因此,个体化的抗栓治疗策略至关重要。
病历资料患者,男,52岁。
因“突发胸痛30min”入院急诊。
患者于30min 前活动中突发胸骨后持续性胀痛,放射至左上肢,伴胸闷、呼吸困难、乏力、大汗淋漓,遂来我院急诊就诊。
急诊心电图示:V 1-V 4导联ST 段抬高、Ⅱ、Ⅲ、AVF、V 5-V 6ST段压低、AVR导联ST段抬高。
查体:体温36.5℃,脉搏120次/min,血压106/88mmHg,呼吸20次/min。
神清,平卧位,肺部查体无异常,心界不大,心率120次/min,律齐,各瓣膜听诊区未闻及病理性杂音。
既往史及家族史:吸烟史30余年,约20支/d。
其父有急性心肌梗死病史。
初步诊断:急性前壁ST 段抬高型心肌梗死。
予以阿司匹林300mg +替格瑞洛180mg+瑞舒伐他汀20mg 嚼服,并行急诊冠脉造影(图1A、图1B),前降支及开口严重狭窄,并可见血栓影,对角支开口严重狭窄,TIMI 血流Ⅱ级,于前降支(LAD)植入EXCEL(3.5mm×36mm)支架1枚,术中发生慢血流,予以尼可地尔、硝普钠、替罗非班冠脉内注入后血流改善,TIMI 血流达到Ⅲ级(图1C、图1D)。
术后予以低分子肝素钠7000U,每12h 1次皮下注射;阿司匹林100mg,1次/d;替格瑞洛90mg,2次/d;瑞舒伐他汀10mg,每晚;泮托拉唑胶囊40mg,1次/d。
入院5h 患者出现头晕,血压85/54mmHg,并出现恶心、呕吐,呕吐大量暗红色咖啡样液体,含胃内容物,1000mL 左右。
吲哚布芬—替代阿司匹林的新选择

吲哚布芬—替代阿司匹林的新选择郭治彬教授南昌大学第一附属医院心内科主任医师,硕士生导师阿司匹林是冠心病和脑梗死预防与治疗的常规选择,然而,阿司匹林胃肠道损伤严重、出血风险高。
抗血小板药物阿司匹林和氯吡格雷临床用药缺憾:出血风险、消化道损伤、药物抵抗。
是否可以有这样的药物:出血风险低、胃肠反应小、无耐药抵抗、不诱发哮喘、使用便捷、肾功能不全患者仍适用?吲哚布芬(indobufen )——替代阿司匹林的新药,效果与阿司匹林相当,胃肠反应小,出血风险低!二、吲哚布芬适应症:1、动脉硬化引起的缺血性心血管病变、缺血性脑血管病变。
2、静脉血栓形成。
3、也可用于血液透析时预防血栓形成。
三、抗血小板作用机制:1、可逆/ 高选择性抑制COX-1→阻断TXB2合成;2、抑制ADP、AA、胶原、肾上腺素、血小板因子诱导的血小板聚集。
四、抗凝作用机制:1、吲哚布芬可以抑制PF3、PF4的释放;2、显著抑制凝血因子Ⅱ、Ⅹ。
五、药代动力学:1、吲哚布芬口服吸收快,2小时后血浆浓度达峰值(血小板血栓素合成抑制98% )2、半衰期为6~8小时,停药后24小时即可恢复血小板功能(抑制率降到47%)3、75% 的药物以葡萄糖醛酸结合物形式随尿排泄,部分以原形排出。
使用吲哚布芬的出血风险较低,l血小板功能在停药后24小时恢复,发生出血后也更易止血。
六、指南推荐:1、美国胸科医师协会抗血小板药物指南(ACCP-8,2008)推荐:吲哚布芬是一种非常有效的血小板环氧化酶抑制剂,其生化、功效和临床效果与标准剂量的阿司匹林相当。
(Patrono C, et al. CHEST Journal, 2008, 133(6_suppl): 199S-233S. )2、急性ST段抬高型心肌梗死溶栓治疗的合理用药指南(2018)和人卫版第九版《内科学》(2018)一致推荐:l吲哚布芬用于胃肠出血或消化道溃疡病史等阿司匹林不耐受患者的替代治疗,用法为200mg(负荷量),继以100mg,每日2次。
长城心微网站
长城心微网站吲哚布芬——防治冠心病更安全!√可逆抑制环氧合酶,半衰期6-8小时,停药24h即可进行手术√消化道损伤小(发生率仅3.8%),出血风险低(发生率仅0.03%)√无药物“抵抗”,对阿司匹林过敏及哮喘患者亦可使用√肾功能不全患者亦可使用【正文】抗血小板药物是治疗冠心病的基石,但阿司匹林等抗血小板药物在减少心血管事件、避免梗死的同时,也会引起胃肠不适、出血、哮喘等众多不良反应。
吲哚布芬——防治冠心病更安全的新选择!吲哚布芬是一种可逆的血小板环氧合酶-1(COX-1)抑制剂,阻断血栓素B2(TXB2)合成,不影响血管内皮前列环素(PGI2)血浓度;抑制二磷酸腺苷(ADP)、肾上腺素等诱导的血小板聚集;抑制血小板因子3、血小板因子4的释放;同时兼具改善红细胞变形能力,舒张血管的作用。
主要用于防治动脉硬化引起的缺血性心血管病变、脑血管病变、静脉血栓形成,以及预防血液透析时血栓形成。
2008年美国胸科指南推荐吲哚布芬在缺血性心脑血管疾病中,特别是针对二级预防,该药物与阿司匹林疗效相当,但安全性更好,主要为出血风险低、消化道反应少,且无耐药抵抗,是阿司匹林不耐受患者的最佳选择。
2011年美国心脏协会卒中指南推荐在房颤脑血栓预防中吲哚布芬与华法林效果相当,安全性更高,使用更便捷,目前使用华法林要定期监测凝血酶原时间,且起效慢,个体差异大,需要及时调整剂量,出血风险也较高,而使用吲哚布芬无需监测凝血四项,安全性也更高。
2016年中国卫计委合理用药指南推荐在急性ST 段抬高型心肌梗死溶栓治疗后,应继续坚持双重抗血小板治疗,对于阿司匹林不耐受或胃肠道反应较大者,可考虑使用吲哚布芬100 mg/次,每日2 次。
多项欧洲循证医学研究证明在外周血管疾病中,特别在静脉血栓预防中,吲哚布芬是华法林不耐受者的最佳选择。
对于骨科大手术(髋关节置换、膝关节置换)预防深静脉血栓形成,吲哚布芬疗效优于与肝素(注射抗凝药)。
通过对血栓形成过程中多个路径、多个靶点的全面抑制,有效阻断动脉/静脉血栓形成,具备了速效、高效、安全、便捷、无耐药抵抗等多种临床应用优势,多年来国内外指南推荐及临床研究表明,吲哚布芬具有以下优势:1、吲哚布芬作为可逆性、选择性环氧合酶-1抑制剂,在心脑血管及周围血管抗血栓治疗中,疗效不劣于甚至高于阿司匹林、法华林、肝素。
吲哚布芬有机小分子分子类型
吲哚布芬有机小分子分子类型1.引言1.1概述吲哚布芬(Indobufen)是一种有机小分子,属于非甾体抗炎药物(Nonsteroidal anti-inflammatory drugs, NSAIDs)的一种。
NSAIDs 是一类广泛使用于临床的药物,常用于缓解炎症、退热、镇痛等功效。
吲哚布芬在这一类药物中具有独特的结构和药理学特性。
吲哚布芬的基本结构包含了吲哚环和苯环,这种特殊结构使其具有良好的溶解度和药代动力学特性。
吲哚布芬具有较强的抗炎作用,可抑制炎症介质的释放,从而减轻炎症反应和相关疼痛。
此外,吲哚布芬还具有抗血小板聚集的作用,可以防止血栓的形成,具有一定的抗血栓作用。
吲哚布芬的合成方法多样,常用的合成路线包括酰胺化反应、酰基化反应等。
近年来,随着有机合成技术的不断发展,吲哚布芬的合成方法也在不断优化,合成路线更加高效且产率较高。
吲哚布芬作为一种新型的非甾体抗炎药物,具有广阔的应用前景。
目前已有研究表明吲哚布芬在心脑血管疾病、风湿性关节炎等方面具有一定的临床效果。
同时,吲哚布芬的药效与副作用也需要进行更多的深入研究,以进一步优化其药物特性和确保安全性。
总而言之,吲哚布芬作为一种有机小分子,具有独特的药物结构和药理学特性,具备广泛的应用前景。
在未来的发展中,我们可以期待吲哚布芬在防治炎症性疾病、心脑血管疾病等方面的突破和应用。
然而,对于吲哚布芬的应用前景和发展趋势,仍需要更多的研究和实践来进一步证实和探索。
1.2文章结构1.2 文章结构本文将按照以下结构进行论述和分析吲哚布芬有机小分子的分子类型。
首先,引言部分将对吲哚布芬有机小分子的概述进行介绍,包括其基本结构和合成方法,并说明本篇文章的目的。
接下来,正文部分将分为两个主要部分,分别是吲哚布芬的基本结构和吲哚布芬的合成方法。
在吲哚布芬的基本结构一节中,我们将详细介绍吲哚布芬分子的基本组成和形状。
通过分析吲哚布芬的结构,我们将探讨吲哚布芬分子的特点和性质。
吲哚布芬(抗血小板药)临床文献资料
结论:在那些接受冠状动脉旁路移植手术后,由于临床事件而进行了再次血管造影的患者中,只有一 半可确定病因为桥血管相关疾病,12%的患者病变原因不明。因此,对冠状动脉旁路移植术后的有症候患 者进行治疗,方法应根据症状解剖学原因的不同而有所区别。
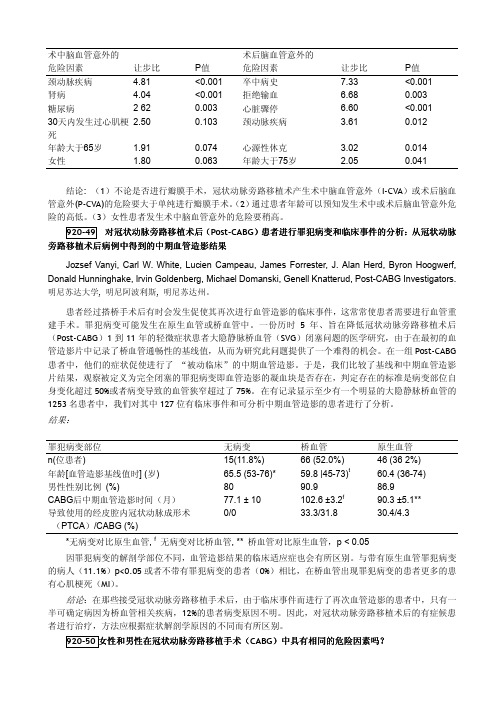
920-50 女性和男性在冠状动脉旁路移植手术(CABG)中具有相同的危险因素吗?
Eric D. Peterson, Lawrence H. Muhlbaier, Elizabeth R. DeLong, Allison B. Rosen, Donald F. Fortin, Edward F. Ellerbeck, Stephen F. Jencks, David B. Pryor. 杜克大学医学中心, 北卡罗来那州达拉谟
患者经过搭桥手术后有时会发生促使其再次进行血管造影的临床事件,这常常使患者需要进行血管重 建手术。罪犯病变可能发生在原生血管或桥血管中。一份历时 5 年、旨在降低冠状动脉旁路移植术后 (Post-CABG)1 到 11 年的轻微症状患者大隐静脉桥血管(SVG)闭塞问题的医学研究,由于在最初的血 管造影片中记录了桥血管通畅性的基线值,从而为研究此问题提供了一个难得的机会。在一组 Post-CABG 患者中,他们的症状促使进行了 “被动临床”的中期血管造影。于是,我们比较了基线和中期血管造影 片结果,观察被定义为完全闭塞的罪犯病变即血管造影的凝血块是否存在,判定存在的标准是病变部位自 身变化超过 50%或者病变导致的血管狭窄超过了 75%。在有记录显示至少有一个明显的大隐静脉桥血管的 1253 名患者中,我们对其中 127 位有临床事件和可分析中期血管造影的患者进行了分析。 结果:
90.9 102.6 ±3.2f
33.3/31.8
46 (36 2%) 60.4 (36-74) 86.9 90.3 ±5.1** 30.4/4.3
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
DOI 10.1378/chest.08-06722008;133;199S-233S ChestCarlo Patrono, Colin Baigent, Jack Hirsh and Gerald Roth*Antiplatelet Drugsull.html /content/133/6_suppl/199S.f and services can be found online on the World Wide Web at: The online version of this article, along with updated informationISSN:0012-3692)/site/misc/reprints.xhtml (of the copyright holder.may be reproduced or distributed without the prior written permission Northbrook, IL 60062. All rights reserved. No part of this article or PDF by the American College of Chest Physicians, 3300 Dundee Road, 2008Physicians. It has been published monthly since 1935. Copyright CHEST is the official journal of the American College of ChestAntiplatelet Drugs*American College of Chest PhysiciansEvidence-Based Clinical Practice Guidelines(8th Edition)Carlo Patrono,MD;Colin Baigent,MD;Jack Hirsh,MD,FCCP;and Gerald Roth,MDThis article about currently available antiplatelet drugs is part of the Antithrombotic and Thrombo-lytic Therapy:American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition).It describes the mechanism of action,pharmacokinetics,and pharmacodynamics of aspirin,reversible cyclooxygenase inhibitors,thienopyridines,and integrin␣IIb3receptor antago-nists.The relationships among dose,efficacy,and safety are thoroughly discussed,with a mechanistic overview of randomized clinical trials.The article does not provide specific management recommen-dations;however,it does highlight important practical aspects related to antiplatelet therapy, including the optimal dose of aspirin,the variable balance of benefits and hazards in different clinical settings,and the issue of interindividual variability in response to antiplatelet drugs.(CHEST2008;133:199S–233S)Key words:abciximab;antiplatelet drugs;aspirin;clopidogrel;dipyridamole;eptifibatide;platelet pharmacology;resistance; ticlopidine;tirofibanAbbreviations:ACEϭangiotensin-converting enzyme;ADPϭadenosine diphosphate;AMPϭadenosine monophos-phate;ATTϭAntithrombotic Trialists;CAPRIEϭClopidogrel vs Aspirin in Patients at Risk of Ischemic Events; CHDϭcoronary heart disease;CIϭconfidence interval;COMMITϭClopidogrel and Metoprolol Myocardial Infarction Trial;COXϭcyclooxygenase;CUREϭClopidogrel in Unstable Angina to Prevent Recurrent Events;EPICϭEvaluation of 7E3for the Prevention of Ischemic Complications;ESPSϭEuropean Stroke Prevention Study;ESPRITϭEuropean Stroke Prevention Reversible Ischemia Trial;FDAϭFood and Drug Administration;GPϭglycoprotein;INRϭinternational normalized ratio;MIϭmyocardial infarction;NSAIDϭnonsteroidal antiinflammatory drug;ORϭodds ratio; PCIϭpercutaneous coronary intervention;PEϭpulmonary embolism;PGϭprostaglandin;PTCAϭpercutaneous trans-luminal coronary angioplasty;RRϭrate ratio;TIAϭtransient ischemic attack;TXϭthromboxane;TTPϭthrombotic thrombocytopenic purpuraP latelets are vital components of normal hemosta-sis and key participants in atherothrombosis by virtue of their capacity to adhere to injured blood vessels and to accumulate at sites of injury.1Al-though platelet adhesion and activation can be viewed as a physiologic repair response to the sud-den fissuring or rupture of an atherosclerotic plaque, uncontrolled progression of such a process through a series of self-sustaining amplification loops can lead to intraluminal thrombus formation,vascular occlu-sion,and transient ischemia or infarction.Currently available antiplatelet drugs interfere with some steps in the activation process,including adhesion,release, and/or aggregation,1and have a measurable impact on the risk of arterial thrombosis that cannot be dissociated from an increased risk of bleeding.2In discussing antiplatelet drugs,it is important to appreciate that approximately1011platelets are pro-duced each day under physiologic circumstances,a level of production that can increase up to10-fold at*From the Catholic University School of Medicine(Dr.Patrono), Rome,Italy;Clinical Trial Service Unit(Dr.Baigent),University of Oxford,Oxford,UK;Hamilton Civic Hospitals(Dr.Hirsh), Henderson Research Centre,Hamilton,ON,Canada;and Seattle VA Medical Center(Dr.Roth),Seattle,WA.Dr.Patrono was supported in part by a grant from the European Commission FP6(LSHM-CT-2004-005033).Manauscript accepted December20,2007.Reproduction of this article is prohibited without written permission from the American College of Chest Physicians(www.chestjournal. org/misc/reprints.shtml).Correspondence to:Carlo Patrono,MD,Catholic University School of Medicine,Largo F.Vito1,00168Rome,Italy;e-mail: carlo.patrono@rm.unicatt.itDOI:10.1378/chest.08-0672SupplementANTITHROMBOTIC AND THROMBOLYTIC THERAPY8TH ED:ACCP GUIDELINES CHEST/133/6/JUNE,2008SUPPLEMENT199Stimes of increased need.3Platelets are anucleate blood cells that form by fragmentation of megakaryo-cyte cytoplasm and have a maximum circulating life span of about10days in humans.3Platelets provide a circulating source of chemokines,cytokines,and growth factors,which are preformed and packaged in storage granules.Moreover,activated platelets can synthesize prostanoids(primarily,thromboxane[TX] A2)from arachidonic acid released from membrane phospholipids through rapid coordinated activation of phospholipase(s),cyclooxygenase(COX)-1and TX synthase(Fig1).Newly formed platelets also express the inducible isoforms of COX(COX-2)and prosta-glandin(PG)E synthase,and this phenomenon is markedly amplified in association with accelerated platelet regeneration.4Although activated platelets are not thought to synthesize proteins de novo,they can translate constitutive messenger RNAs into pro-teins,including interleukin-1,over several hours.5 Thus,platelets may play previously unrecognized roles in inflammation and vascular injury,and anti-platelet strategies may be expected to affect platelet-derived protein signals for inflammatory and/or pro-liferative responses.1Negative modulation of platelet adhesion and aggre-gation is exerted by a variety of physiologic mecha-nisms,including endothelium-derived prostacyclin (PGI2),nitric oxide,CD39/ecto-ADPase,and platelet endothelial cell adhesion molecule-1.Some drugs may interfere with these regulatory pathways,as exempli-fied by the dose-dependent inhibition of PGI2produc-tion by aspirin and other COX inhibitors.22.0Aspirin and Other COX Inhibitors Aspirin has been thoroughly evaluated as an anti-platelet drug6and was found to prevent vascular death by approximately15%and nonfatal vascular events by about30%in a metaanalysis ofϾ100 randomized trials in high-risk patients.72.1Mechanism of Action of AspirinThe best characterized mechanism of action of the drug is related to its capacity to inactivate permanently the COX activity of prostaglandin H-synthase-1and-2 (also referred to as COX-1and COX-2).8–12These isozymes catalyze the first committed step in prosta-noid biosynthesis(ie,the conversion of arachidonic acid to PGH2)[Fig1].PGH2is the immediate precursor of PGD2,PGE2,PGF2␣,PGI2,and TXA2. COX-1and COX-2are homodimers of aϳ72kd monomeric unit.Each dimer has three independent folding units:an epidermal growth factor-like do-main;a membrane-binding domain;and anenzy-Figure1.Arachidonic acid metabolism and mechanism of action of aspirin.Arachidonic acid,a20-carbon fatty acid containing four double bonds,is liberated from the sn2position in membranephospholipids by several forms of phospholipase,which are activated by diverse stimuli.Arachidonicacid is converted by cytosolic PGH synthases,which have both COX and hydroperoxidase activity,tothe unstable intermediate PGH2.The synthases are colloquially termed COXs and exist in two forms,COX-1and COX-2.Low-dose aspirin selectively inhibits COX-1,and high-dose aspirin inhibits bothCOX-1and COX-2.PGH2is converted by tissue-specific isomerases to multiple prostanoids.Thesebioactive lipids activate specific cell membrane receptors of the superfamily of G-protein-coupledreceptors.DPϭPGD2receptor;EPϭPGE2receptor;FPϭPGF2␣receptor;IPϭprostacyclinreceptor;TPϭTX receptor.200S Antithrombotic and Thrombolytic Therapy8th Ed:ACCP Guidelinesmatic domain.12Within the enzymatic domain,there is the peroxidase catalytic site and a separate,but adjacent site for COX activity at the apex of a narrow, hydrophobic channel.The molecular mechanism of permanent inactiva-tion of COX activity by aspirin is related to blockade of the COX channel as a consequence of acetylation of a strategically located serine residue(Ser529in the human COX-1,Ser516in the human COX-2) that prevents access of the substrate to the catalytic site of the enzyme.13The hydrophobic environment of the COX channel stabilizes the modified serine side-chain against hydrolysis.13Thus,inhibition of COX-1–dependent platelet function can be achieved with low doses of aspirin given once daily.In con-trast,inhibition of COX-2–dependent pathophysio-logic processes(eg,hyperalgesia and inflammation) requires larger doses of aspirin(probably because acetylation is determined by the oxidative state of the enzyme and is inhibited in cells with high peroxide tone)14and a much shorter dosing interval(because nucleated cells rapidly resynthesize the enzyme).Thus, there is an approximately100-fold variation in daily doses of aspirin when used as an antiinflammatory rather than as an antiplatelet agent.Furthermore, the benefit/risk profile of the drug depends on the dose and indication because its GI toxicity is dose dependent(see below).Human platelets and vascular endothelial cells process PGH2to produce primarily TXA2and PGI2, respectively.11TXA2induces platelet aggregation and vasoconstriction,whereas PGI2inhibits platelet aggregation and induces vasodilation.11Whereas TXA2is largely a COX-1–derived product(mostly from platelets)and thus highly sensitive to aspirin inhibition,vascular PGI2can derive both from COX-1and,to a greater extent even under physio-logic conditions,from COX-2.16COX-1–dependent PGI2production occurs transiently in response to agonist stimulation(eg,bradykinin)15and is sensitive to aspirin inhibition.COX-2–mediated PGI2produc-tion occurs long term in response to laminar shear stress17and is largely insensitive to aspirin inhibition at conventional antiplatelet doses.This may explain the substantial residual COX-2–dependent PGI2 biosynthesis in vivo at daily doses of aspirin in the range of30to100mg,18despite transient suppres-sion of COX-1–dependent PGI2release.15It is not established that more profound suppression of PGI2 formation by higher doses of aspirin is sufficient to initiate or predispose to thrombosis.However,two lines of evidence suggest that PGI2is thrombopro-tective.The first is the observation that mice lacking the PGI2receptor had increased susceptibility to experimental thrombosis.19The second is the obser-vation of the cardiovascular toxicity associated with COX-2inhibitors20that also supports the concept of PGI2acting as an important mechanism of throm-boresistance in the setting of inadequate inhibition of platelet TXA2biosynthesis.212.2PharmacokineticsAspirin is rapidly absorbed in the stomach and upper intestine.Peak plasma levels occur30to40 min after aspirin ingestion,and inhibition of plate-let function is evident by1h.In contrast,it can take up to3to4h to reach peak plasma levels after administration of enteric-coated aspirin.If only enteric-coated tablets are available,and a rapid effect is required,the tablets should be chewed.The oral bioavailability of regular aspirin tablets is ap-proximately40to50%over a wide range of doses.22 A considerably lower bioavailability has been re-ported for enteric-coated tablets and sustained-release,microencapsulated preparations.22Lower bioavailability of some enteric-coated preparations and poor absorption from the higher pH environ-ment of the small intestine may result in inadequate platelet inhibition,particularly in heavier subjects.23 Both a controlled-release formulation15and a trans-dermal patch24with negligible systemic bioavailabil-ity have been developed in an attempt to achieve selective inhibition of platelet TXA2production with-out suppressing systemic PGI2synthesis.The former was used successfully in the Thrombosis Prevention Trial(see below),but it remains unknown whether there is any advantage to the controlled-release formulation vis-a`-vis plain aspirin.The plasma concentration of aspirin decays with a half-life of15to20min.Despite the rapid clearance of aspirin from the circulation,the platelet-inhibitory effect lasts for the life span of the platelet25because aspirin irreversibly inactivates platelet COX-1.8,9As-pirin also acetylates the enzyme in megakaryocytes before new platelets are released into the circula-tion.10,26–28The mean life span of human platelets is approximately8to10days.Therefore,about10to 12%of circulating platelets are replaced every 24h.29,30However,the recovery of TXA2biosynthe-sis in vivo following prolonged aspirin administration is somewhat faster than predicted by the rate of platelet turnover,18possibly because of the nonlinear relationship between inhibition of platelet COX-1 activity and inhibition of TXA2biosynthesis in vivo31 (Fig2).2.3Issues Concerning the Antithrombotic Effects of AspirinA number of issues related to the clinical efficacy of aspirin continue to be debated.These include the following:(1)the optimal dose of aspirin in order to CHEST/133/6/JUNE,2008SUPPLEMENT201Smaximize efficacy and minimize toxicity;(2)the suggestion that part of the antithrombotic effect of aspirin is unrelated to inhibition of platelet TXA 2;and (3)the possibility that some patients may be aspirin “resistant.”2.3.1The Optimal Dose of Aspirin:Well-designed,placebo-controlled randomized trials have shown that aspirin is an effective antithrombotic agent when used long term in doses ranging from 50to 100mg/d,and there is a suggestion that it is effective in doses as low as 30mg/d.6,7Aspirin,75mg/d,was shown to be effective in reducing the risk of acute myocardial infarction (MI)or death in patients with unstable angina 32and chronic stable angina,33as well as in reducing stroke or death in patients with transient cerebral ischemia 34and the risk of postoperative stroke after carotid endarterectomy.35In the Euro-pean Stroke Prevention Study (ESPS)-2,aspirin 25mg bid was effective in reducing the risks of stroke and of the composite outcome stroke or death in patients with prior stroke or transient ischemic attack (TIA).36Moreover,in the European Collaboration on Low-Dose Aspirin in Polycythemia vera Trial,37aspirin,100mg/d,was effective in preventing throm-botic complications in patients with polycythemia vera,despite a higher-than-normal platelet count.The lowest effective dose of aspirin for these various indications is shown in Table 1.The clinical effects of different doses of aspirin have been compared directly in a relatively small number of randomized trials.38–43In the United Kingdom TIA study,41no difference in efficacy was found between 300and 1,200mg/d of aspirin (see below).In a study of 3,131patients after a TIA or minor ischemic stroke,aspirin in a dose of 30mg/d was compared with a dose of 283mg/d,and theExtra Platelet SourcesPlatelet SynthesisTXA 2TXB 22,3-dinor-TXB 2& other metabolitesUrineTXB 2Production In VivoEnzymesLiver H 2OCalculated Rate of TXB 2Production In Vivo : 0.1 ng/kg/minP e r c e n t a g e I n h i b i t i o n o f U r i n a r y 2,3-d i n o r -T X B 2E x c r e t i o n I n V i v oPercentage Inhibition of SerumTXB 2Ex VivoPharmacologic InhibitionEx Vivo vs In VivoTXB 2Production Ex Vivo10020030003060 minS e r u m T X B 2n g /m lTimeWhole Blood Clotting at 37°CMaximal Biosynthetic Capacity 300-400 ng/ml in 1 hrFigure 2.Maximal capacity of human platelets to synthesize TXB 2,rate of TXB 2production in healthy subjects,and relationship between the inhibition of platelet COX activity and TXB 2biosynthesis in vivo .Left panel:The level of TXB 2production stimulated by endogenous thrombin during whole-blood clotting at 37°C.62Center panel:The metabolic fate of TXA 2in vivo and the calculated rate of its production in healthy subjects on the basis of TXB 2infusions and measurement of its major urinary metabolite.Right panel:The nonlinear relationship between inhibition of serum TXB 2measured ex vivo and the reduction in the excretion of TX metabolite measured in vivo .31Table 1—Vascular Disorders for Which Aspirin Has Been Shown To Be Effective and Lowest Effective Dose(Section 2.3.1)DisorderLowest Effective Daily Dose,mgTIA and ischemic stroke *50Men at high cardiovascular risk 75Hypertension 75Stable angina 75Unstable angina *75Severe carotid artery stenosis *75Polycythemia vera 100Acute MI160Acute ischemic stroke *160*Higher doses have been tested in other trials and were not found to confer any greater risk reduction.202SAntithrombotic and Thrombolytic Therapy 8th Ed:ACCP Guidelineshazard ratio for the group receiving the lower dose was0.91(95%confidence interval[CI],0.76to 1.09).42The Acetylsalicylic Acid and Carotid Endar-terectomy Trial reported that the risk of stroke,MI, or death within3months of carotid endarterectomy is significantly lower for patients taking81or325 mg/d aspirin than for those taking650or1,300mg (6.2%vs8.4%;pϭ0.03).43Thus,there is no con-vincing evidence from randomized studies that have compared different doses of aspirin that higher doses are more effective in reducing the risk of serious vascular events.In fact,both this limited set of randomized comparisons and the indirect compari-sons reported in the overview of the Antithrombotic Trialists’(ATT)Collaboration(Table2)are compat-ible with the reverse(ie,blunting of the antithrom-botic effect at higher doses of aspirin,consistent with dose-dependent inhibition of PGI2).Such inhibition of PGI2may be a potential mechanism by which COX-2inhibitors produce an excess risk of MI(see below).The antithrombotic effects of a range of doses of aspirin also have been compared with an untreated control group in a number of thrombotic vascular disorders.The doses have varied between50and 1,500mg/d.Aspirin has been shown to be effective in the following conditions:unstable angina in which the incidence of acute MI or death was significantly reduced in four separate studies using daily doses of 75mg,32325mg,44650mg,45and1,300mg46;stable angina in which a dose of75mg/d reduced the incidence of acute MI or sudden death33;aortocoro-nary bypass surgery in which the incidence of early occlusion was similarly reduced with daily doses of 100mg,47325mg,48975mg,49and1,200mg49; thromboprophylaxis of patients with prosthetic heart valves who also received warfarin in whom the incidence of systemic embolism was reduced with daily doses of100mg,50500mg,51and1,500mg52,53; thromboprophylaxis of patients with arterial venous shunts undergoing long-term hemodialysis in whom a dose of160mg/d was shown to be effective54;acute MI in which a dose of162.5mg/d reduced early (35-day)mortality as well as nonfatal reinfarction and stroke55;transient cerebral ischemia in which doses between50and1,200mg/d were effective34,36,41,56–58; acute ischemic stroke in which doses of160to300 mg/d were effective in reducing early mortality and stroke recurrence59,60;and polycythemia vera in which100mg,37but not900mg,61was effective in reducing fatal and nonfatal vascular events. Thus,aspirin is an effective antithrombotic agent in doses between50and1,500mg/d.It is also possible from the results of the Dutch TIA study that 30mg/d is effective.42There is no evidence that low doses(50to100mg/d)are less effective than high doses(650to1,500mg/d)and,in fact,the opposite may be true.These clinical findings are consistent with saturability of platelet COX-1inactivation at doses as low as30mg/d.62There is evidence,however,that doses of approx-imately300mg/d produce fewer GI side effects than doses of approximately1,200mg/d.41There is also some evidence that a dose of30mg/d produces fewer side effects than300mg/d.42The Clopidogrel in Unstable Angina To Prevent Recurrent Events (CURE)investigators have retrospectively investi-gated the relationship between the aspirin dose(the CURE protocol recommended75to325mg/d)and risk of major bleeding.63This study was a random-ized comparison of clopidogrel with placebo on a “background”of aspirin therapy.Patients with acute coronary syndromes receiving aspirin,Յ100mg/d, had the lowest rate of major or life-threatening bleeding complications both in the placebo(1.9%) and in the clopidogrel(3%)arms of the trial.Bleed-ing risks increased with increasing aspirin dose with or without clopidogrel.63In summary,the saturability of the antiplatelet effect of aspirin at low doses,the lack of dose-response relationship in clinical studies evaluating its antithrombotic effects,and the dose dependence of its side effects all support the use of as low a dose of aspirin as has been found to be effective in the treatment of various thromboembolic disorders(Ta-ble1).Use of the lowest effective dose of aspirin(50 to100mg/d for long-term treatment)is currently the most appropriate strategy to maximize its efficacy and minimize its toxicity.62.3.2Effects of Aspirin Not Related to TXA2: Aspirin has been reported to have effects on hemostasis that are unrelated to its ability to inactivate platelet COX-1.These include dose-dependent inhibition of platelet function,64–68enhancement of fibrinolysis,69–71 and suppression of plasma coagulation.72–75In contrast to the saturable and well-characterized (nanomolar aspirin concentration,rapid time course, physiologic conditions,single serine modification)Table2—Indirect Comparison of Aspirin Doses Reducing Vascular Events in High-RiskPatients(Section2.3.1)*Aspirin Dose,mg/d No.ofTrialsNo.ofPatientsOddsReduction500–1,5003422,45119Ϯ3%160–3251926,51326Ϯ3%75–150126,77632Ϯ6%Ͻ7533,65513Ϯ8%*Data are from Lindemann et al5/2001. CHEST/133/6/JUNE,2008SUPPLEMENT203Sinhibition of COX-1by aspirin,13,62,76the putative mechanisms underpinning the non-PG effects of aspirin on hemostasis are dose dependent and less clearly defined.For example,inhibition of shear-induced platelet aggregation depends on the level of aspirin provided,and enhanced fibrinolysis due to N-acetylation of lysyl residues of fibrinogen is seen in vivo with high doses of aspirin(650mg bid)69and proceeds more rapidly in vitro under nonphysiologic alkaline conditions.77Aspirin suppresses plasma co-agulation through several mechanisms.The first, initially described in1943by Link et al and con-firmed by others,72,73is caused by an antivitamin K effect of aspirin.It requires very high doses of aspirin and does not contribute to the antithrombotic effect of aspirin when the drug is used in doses up to1,500 mg/d.The second is platelet dependent and is characterized by inhibition of thrombin generation in a whole blood system.74,75A single dose of500mg depresses the rate of thrombin generation,whereas repeated daily dosing with300mg of aspirin reduces the total amount of thrombin formed.78An interac-tion with platelet phospholipids,which is blunted in hypercholesterolemia,has been proposed to explain the effects of aspirin on thrombin generation.78It is possible(but unproven)that this effect occurs as a consequence of impaired platelet coagulant activity secondary to inhibition of TX-dependent platelet aggregation.It is unknown whether lower doses of aspirin are able to produce this effect.This sort of in vitro effect has been shown for other platelet inhibi-tors,such as glycoprotein(GP)-IIb/IIIa antagonists(see below).Furthermore,high-dose aspirin can cause ab-normal coagulation in vitro by direct acetylation of one or more clotting factors.This can be demonstrated in platelet-poor plasma and,thus,is not related to platelet inhibition or vitamin K antagonism.Additional studies in both animal models and human subjects have reported antithrombotic effects of aspirin that may occur,at least in part,through mechanisms unrelated to inactivation of platelet COX-1.In animal models,Buchanan et al66and Hanson et al64reported that optimal antithrombotic activity of aspirin required doses in excess of those required to inhibit TXA2.In clinical studies,the results of a subgroup analysis of the North American Symptomatic Carotid Endarterectomy Trial study79 suggested that aspirin in doses ofՆ650mg/d might be more effective thanՅ325mg/d for the preven-tion of perioperative stroke in patients having carotid artery surgery.80This retrospective observation was refuted by a second prospective study,the Acetylsal-icylic Acid and Carotid Endarterectomy Trial,43 which tested the hypothesis that the wide area of collagen exposed by endarterectomy is a sufficiently strong stimulus to platelet aggregation to require a larger dose of aspirin.Approximately3,000patients scheduled for carotid endarterectomy were ran-domly assigned81,325,650,or1,300mg/d aspirin, started before surgery and continued for3months. The combined rate of stroke,MI,or death at3 months was significantly(pϭ0.03)lower in the low-dose groups(6.2%)than in the high-dose groups (8.4%)[primary analysis].There were no significant differences between the81-mg and325-mg groups or between the650-mg and1,300-mg groups in any of the secondary analyses of the data.43A subgroup analysis of the Physicians’Health Study,81based on post hoc measurements of baseline plasma C-reactive protein performed in543appar-ently healthy men who subsequently had MI,stroke, or venous thrombosis,and in543study participants who did not report vascular complications,has found that the reduction in the risk of a first MI associ-ated with the use of aspirin(325mg on alternate days)appears to be directly related to the level of C-reactive protein,raising the possibility of antiin-flammatory as well as antiplatelet effects of the drug in cardiovascular prophylaxis.82This hypothesis is unlikely to be correct because,as noted above,the antiinflammatory effects of aspirin and other nonste-roidal antiinflammatory drugs(NSAIDs)are largely related to their capacity to inhibit COX-2activity induced in response to inflammatory cytokines,12as these clinical effects can be fully reproduced by highly selective COX-2inhibitors(coxibs)in patients with rheumatoid arthritis.83As shown in Table3,the dose and time dependence of the effects of aspirin on nucleated inflammatory cells expressing COX-2 vs anucleated platelets expressing COX-1are mark-edly different,thus making a clinically relevant anti-inflammatory effect of the drug at325mg everyTable3—Dose and Time Dependence of the Effects of Aspirin on Platelets and Inflammatory Cells(Section2.3.2)Cellular Target EnzymeSingleDose,*mgDuration of ProstanoidSuppression,hCumulative Effects UponRepeated DosingDailyDose,†mgPlatelets COX-110024–48Yes50–81 Inflammatory cells COX-2Ն6503–4No3,000–5,000 *Dose causing full suppression of prostanoid formation and/or clinically detectable functional effect after single dosing.†Range of doses shown clinically effective in long-term trials of cardiovascular protection or rheumatoid arthritis.204S Antithrombotic and Thrombolytic Therapy8th Ed:ACCP Guidelinesother day pharmacologically implausible.Finally, aspirin has been reported to modify the way in which neutrophils and platelets84or erythrocytes and plate-lets85,86interact,to protect endothelial cells from oxidative stress,87and to improve endothelial dys-function in atherosclerotic patients.88However,nei-ther the molecular mechanism(s)nor the dose de-pendence of these effects have been clearly established.Although improved endothelial dysfunc-tion could reflect an antiinflammatory effect of aspirin of relevance to atherogenesis,it should be emphasized that the hypothesis has never been tested by an appropriately sized controlled prospec-tive study.All of the evidence detailed above suggesting dose-dependent effects for aspirin is indirect and inconsistent with the failure to show a dose effect in randomized clinical trials and in the ATT overview analysis.7This failure to show a dose effect is the critical point of the discussion because it correlates with the saturability of the aspirin effect on platelet COX-1.For example,in studies with purified en-zyme and with isolated platelets,nanomolar concen-trations of aspirin will completely block PG synthesis within20min after exposure.89Higher concentra-tions and longer exposures will not alter the inhibi-tory effect of aspirin on PG synthesis because of this saturable quality.Exactly the same feature(maximal effect at low doses,absence of dose effect)is seen in clinical trials with aspirin as an antithrombotic agent. When one raises the dose of aspirin in this situation, no further or additional effect can be appreciated because the critical event has already taken place, namely,maximal inhibition of platelet TX synthesis. Thus,the consistency of dose requirements and saturability of the effects of aspirin in acetylating the platelet enzyme,8inhibiting TXA2production,25,62 and preventing atherothrombotic complications6,7 constitutes the best evidence that aspirin prevents thrombosis through inhibition of TXA2production. It is likely,therefore,that any of the potential effects of aspirin on other determinants of arterial throm-bosis are much less important than the inhibition of platelet COX-1activity.2.3.3Aspirin“Resistance”:The term aspirin resis-tance has been used to describe a number of differ-ent phenomena,including the inability of aspirin to (1)protect individuals from thrombotic complica-tions,(2)cause a prolongation of the bleeding time, (3)reduce TXA2production,or(4)produce a typical effect on one or more in vitro tests of platelet function.90From a therapeutic standpoint,it is im-portant to establish whether aspirin resistance can be overcome by increasing the dose of aspirin,but unfortunately very few data bear directly on this issue.The fact that some patients may experience recurrent vascular events despite long-term aspirin therapy should be properly labeled as treatment failure rather than aspirin resistance.Treatment failure is a common phenomenon occurring with all drugs(eg,lipid-lowering or antihypertensive drugs). Given the multifactorial nature of atherothrombosis and the possibility that platelet-mediated thrombosis may not be responsible for all vascular events,it is not surprising that only a fraction(usually one fourth to one third)of all vascular complications can be prevented by any single preventive strategy.It has been reported that a variable proportion(up to one fourth)of patients with cerebrovascular dis-ease only achieve partial inhibition of platelet aggre-gation at initial testing,and some(up to one third) seem to develop resistance to aspirin over time,even with increasing doses.91–93The results of these long-term studies carried out by Helgason et al are at variance with those of a short-term study of Weksler et al,94showing that aspirin,40mg/d,inhibited platelet aggregation and TXA2formation as effec-tively as higher doses of aspirin in patients who had recent cerebral ischemia.Variable platelet responses to aspirin have also been described in patients with peripheral arterial disease95and with ischemic heart disease.96–98In the Buchanan and Brister study,96 aspirin nonresponders were identified on the basis of bleeding time measurements.Approximately40%of patients undergoing elective coronary artery bypass grafting showed no prolongation of bleeding time in response to aspirin.This finding was associated with increased platelet adhesion and12-HETE synthe-sis.96In contrast,repeated measurements of platelet aggregation performed over24months of placebo-controlled treatment by Berglund and Wallentin99 demonstrated that100patients with unstable coro-nary artery disease randomized to receive aspirin, 75mg/d,in the Research Group on Instability in Coronary Artery Disease in Southeast Sweden study32had consistently reduced platelet aggregation without attenuation during long-term treatment. Based on measurements of platelet aggregation in response to arachidonate and adenosine diphosphate (ADP),5%and24%of patients with stable cardio-vascular disease who were receiving aspirin(325 mg/d forՆ7days)were defined as resistant and semiresponders,respectively.97Using a variety of techniques,including conventional aggregometry, shear stress-induced activation,and the expression of platelet surface receptors,Sane et al98recently re-ported that57%of a group of88patients with documented heart failure who had been treated with aspirin,325mg/d,forՆ1month showed aspirin nonresponsiveness.Overall,the majority of these studies were characterized by the following major CHEST/133/6/JUNE,2008SUPPLEMENT205S。