Prospective randomized trial of TVT and TOT
系统性红斑狼疮诊断治疗的最新进展1
系统性红斑狼疮诊断治疗的最新进展蒋明系统性红斑狼疮(SLE)在风湿病中是一个较常见的疾病。
据我国流行病学的初步统计,此病的患病率为70~100/10万人,如果以全国12亿人口计算。
我国的SLE患者已达84~120万之多。
自50年代起,人们对SLE的诊断已经给予相当的重视。
1958年,美国风湿病协会首次提出SLE的分类标准,经过多年的反复临床实践,该协会于1982年对SLE的分类标准进行了修改,并成为国际通用的诊断SLE的标准。
这一诊断标准共有11条,凡符合其中4条者即可诊断SLE。
这11条标准简述为:(1)颊部红斑;(2)盘状红斑;(3)光敏感;(4)口腔溃疡;(5)关节炎;(6)浆膜炎;(7)肾脏病变;(8)神经系统异常;(9)血液学异常;(10)免疫学异常;(11)抗核抗体异常。
这一分类标准的敏感性及特异性均为96%。
不过,此标准是根据已经确诊的SLE患者的各种临床资料经过计算机分析处理而得出的,它对于早期或有特殊表现的SLE的诊断尚有一定的困难。
多年来一直采用肾上腺皮质激素和其它免疫抑制剂治疗SLE,效果虽较肯定,但有明显的副作用,这是因为这类药物非选择性地抑制T、B淋巴细胞功能,对病理性和生理性的淋巴细胞都有作用,因而在用药过程中会出现多种不良反应。
迄今,对SLE的药物治疗方面尚无突破性的进展。
由于SLE的病因和发病机制尚未完全明了,在诊断及治疗上虽均无突破性的进展,不过,近年来随着有关SLE基础研究的深入,新的检查技术和设备的发展,以及临床经验的积累,对此病的诊断与治疗较前已有显著的进展,现将近年来有关诊断和治疗SLE的一些新的报道作一扼要的介绍。
1 诊断1.1 NO对SLE脑病的诊断经过数十年的研究,对一氧化氮(NO)在体内作为一种介质的信息传递作用的了解有了很大的发展,因而于1998年给有突出成就的研究者授予诺贝尔奖金。
最近有学者报告,SLE脑病患者的脑脊液中的NO水平明显增高,增高的程度与其脑病的严重性具有一致的关系。
特利加压素治疗门静脉高压食管胃底曲张静脉破裂大出血
特利加压素治疗门静脉高压食管胃底曲张静脉破裂大出血郑骁【摘要】目的:观察特利加压素治疗肝硬化门静脉高压食管胃底曲张静脉破裂大出血的效果。
方法将2009年3月~2012年8月收治的46例肝硬化门静脉高压食管胃底曲张静脉破裂大出血患者分为两组,分别给予特利加压素和生长抑素,观察24 h 止血率、总止血率、1周再出血率、1周死亡率和副反应发生率。
结果特利加压素组24h 止血率、总止血率和副反应发生率明显高于生长抑素组(P<0.05),1周再出血率和死亡率明显低于生长抑素组(P <0.05)。
结论特利加压素用于肝硬化门静脉高压食管胃底曲张静脉破裂大出血,止血效果确切,可以明显降低死亡率。
%Objective:To investigate the efficiency of terlipressin for treatment of esophagogastric varices in patients with portal hypertension due to liver cirrhosis. Methods:46 cases with esophagogastric varices and portal hypertension, from March 2009 to August 2012,were randomized into terlipressin - treated group( n = 24)and somatostatin - treated group. The rates of hemostais within 24h and 72h,repeated bleeding,mortality and occurent of side effect were recorded. Results:The rates of hemostais within 24h and 72h and occurent of side effect in terlipressin group were higher than those of somatostatin group(P < 0. 05),the rates of repeated bleeding andmortality were lower than those of somatostatin group (P < 0.05). Conclusions:Terlipressin is more effective in treatment of esophagogastric varices complicated in portal hyper-tension due to liver cirrhosis,which could quickly?and?effectively?arrest?the?hemorrhage and reduce the mortality rate.【期刊名称】《泰山医学院学报》【年(卷),期】2014(000)008【总页数】3页(P757-759)【关键词】特利加压素;门静脉高压症;食管胃底静脉曲张【作者】郑骁【作者单位】泰山医学院附属泰山医院普外科,山东泰安 271000【正文语种】中文【中图分类】R656.6食管胃底静脉曲张破裂出血是肝硬化门静脉高压症最严重的并发症[1],是导致肝硬化失代偿期患者的最主要原因。
不同危重评分对急性肾功能衰竭预后判断价值

不同危重评分对急性肾功能衰竭预后判断价值[摘要] 目的:分析不同危重评分对急性肾功能衰竭(Acute renal failure,ARF)预后判断价值,为ARF患者预后判断提供参考依据。
方法:选取我院2013年5月―2015年5月收治的129例ARF患者,均于其确诊后24 h内行急性生理学和慢性健康状况评分(APACHE II)、简化急性生理评分(SAPS II)及序贯器官衰竭估计评分(SOFA),并按照其预后情况分为存活组与病死组,比较2组患者各项评分差异,并以受试者工作特征曲线(ROC)分析不同危重评分判断患者预后价值。
观察APACHE II评分与病死率、死亡风险的关系。
结果:129例患者病死86例,病死率66.7%。
存活组APACHE II、SAPS II评分显著低于病死组,差异有统计学意义(P0.05)。
APACHE II评分的ROC曲线下面积显著高于SAPS II评分、SOFA 评分,差异有统计学意义(P0.05)。
随着患者APACHE II评分的增加,其病死率、R值均呈上升趋势。
结论:APACHE II对ARF患者预后的判断价值最高,建议作为临床预测患者预后的首选评分手段。
[关键词] 危重评分;急性肾功能衰竭;预后;判断中图分类号:R692.5 文献标识码:A 文章编号:2095-5200(2016)02-018-03DOI:10.11876/mimt201602007急性肾功能衰竭(Acute renal failure,ARF)属临床常见危急重症之一[1]。
ARF患者肾小球滤过率可降至正常值的50%以下,由此引发血肌酐、尿素氮等氮质分解代谢产物增加,导致尿量减少甚至无尿,继而引发水电解质及酸碱平衡失调,严重者可出现急性尿毒症[2]。
因此,早期判断患者预后,是明确病情状态、延缓症状恶化的重要基础。
急性生理学和慢性健康状况评分(APACHE II)、简化急性生理评分(SAPS II)及序贯器官衰竭估计评分(SOFA)在各类危重病患者预后评估中已得到广泛应用,但目前关于上述评分预测ARF患者预后价值的研究较为缺乏[3]。
氯吡格雷与奥美拉唑药物相互作用的应用分析
氯吡格雷与奥美拉唑药物相互作用的应用分析一、案例背景知识简介氯吡格雷是一种血小板聚集抑制剂,选择性地抑制二磷酸腺苷(ADP)与它的血小板受体的结合及继发的ADP介导的糖蛋白GPⅡb/Ⅲa复合物的活化,因此可抑制血小板聚集,是冠心病患者尤其是PCI 术后必不可少的抗血小板药物,其应用已经相当普遍。
对于老年冠心病患者,常常会合并有高血压,糖尿病等多种疾病,因此服用药物种类较多,临床药师应密切关注合并有多种疾病的老年冠心病患者可能存在的药物间的相互作用。
本病例通过探讨氯吡格雷与质子泵抑制剂之间的相互作用及处理对策,强调临床药师在临床中的积极作用,从药师的角度发现问题,解决问题,为患者制订出最大获益的个体化治疗方案。
二、病例内容简介患者,男性,79岁,主因反复心前区不适5个月余入院。
患者于2007年活动后出现心前区疼痛,体力活动时加重,休息后可缓解。
2009年10月于夜间睡眠时再次出现心前区疼痛,伴胸闷气短,向背部、咽喉部放射,约5分钟后自行缓解,此后患者反复于静息状态下出现上述症状。
今为进一步诊治以“冠心病、不稳定型心绞痛”于2010年3月16日收入心内科。
患者既往糖尿病10年,长期服用阿卡波糖,血糖控制满意。
有慢性胃炎病史20年,门诊胃镜(2009-10-26)提示胃食管反流、糜烂性胃炎,服用奥美拉唑肠溶片保护胃黏膜。
入院查体:体温36.3℃,脉搏71次/分,呼吸18次/分,血压144/74mmHg。
辅助检查:生化监测:ALT 23.6U/L,AST 22.1U/L,肌钙蛋白 T 0.020ng/ml,肌酐 101.8μmol/L,血清尿酸 463.3μmol/L,肌酸激酶 127.8U/L,钾3.74mmol/L,BNP 92.07pg/ml。
凝血检查:血浆活化部分凝血酶原时间测定33.0秒,血浆凝血酶原活动度测定120%,血浆纤维蛋白原测定3.23g/L,血浆D-二聚体测定2.66μg/ml ↑。
关于PROSPECT建议的说明PROSPECT根据已发表的证据和-Esra
关于PROSPECT 建议的说明
PROSPECT 根据已发表的证据和专家意见,为临床医生提供赞成和反对使用各种术后疼痛干预措施的支持性论据。
临床医生必须根据临床情况和当地法规做出判断。
任何时候都必须参考所提及药物的当地处方信息。
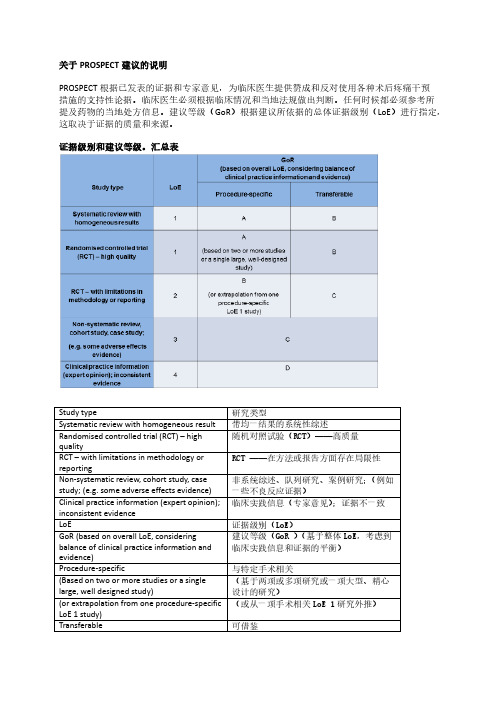
建议等级(GoR )根据建议所依据的总体证据级别(LoE )进行指定,这取决于证据的质量和来源。
证据级别和建议等级。
汇总表
Study type
研究类型
可以在以下链接中找到如何执行研究质量评估以确定LoE和GoR的说明:剖宫产:证据级别和建议等级。
研究和评估指南(AGREE) II的工具(Brouwers,2010年)在国际上被用于评估实践指南的方法严谨性和透明度。
PROSPECT剖宫产审核的方法尽可能符合AGREE II工具“领域3:制定的严谨性”的要求:
∙用系统方法来搜索证据。
∙清楚地描述了选择证据的标准。
∙明确描述了证据的优点和局限性。
∙清楚地描述了制定建议的方法。
∙在制定建议时考虑了健康益处、副作用和风险。
∙建议与支持性证据之间存在明确的联系。
∙专家在该指南出版前已对该指南进行了外部审核。
[证据和建议将在PROSPECT网站上公布后提交给同行评审]
∙提供了更新指南的程序。
[提供方法,以便根据需要对系统性评价进行更新]
摘要建议
总体建议:择期剖宫产手术的疼痛管理
不建议用于剖宫产。
米索前列醇舌下含服用于早孕药物流产

,即能否研制出体积较小、水果口味、易含化崩解的Miso舌下含服剂型。
2.2 尚无舌下Miso与口服Miso的对照性研究 由现有资料可见,尚无舌下与口
服的对照性研究,而口服给药恰是我国早孕药物流产的标准方法。许多文献都提及
无统计学意义,可能与样本较小有关,尚需大样本的研究。Hamoda等 [15] 研
究中舌下组的排囊时间显著短于阴道组,但由于该研究为非随机试验,舌下组的孕
龄也显著短于阴道组,故缺乏说服力。而在设计较完善的Tang等 [16] 中,两
组的平均排囊时间差异无显著性。
2.1.3 术后带血天数及血红蛋白含量变化 现有5个研究统计了药流术后的平均
米索前列醇舌下含服用于早孕药物流产
更新日期: 12-04 [关键词] 米索前列醇 药物流产
健康网讯: 张钰娟(综述) 李奕(审校) 300211天津医科大学第二医院妇产科
米索前列醇(Misoprostol,Miso)是20世纪80年代人工合成的前列腺素E 1
衍生物,原用于治疗消化性溃疡,自1987年Rabe等首次提出Miso有终止早期妊娠
1.3 Miso经不同给药途径的兴奋子宫肌作用研究 Aronsson等 [4] 测定了
舌下、口服、阴道给予Miso400μg后的子宫张力变化。宫内压开始增加的时间分别
为11.5min、7.8min、19.4min,舌下组与口服组差异无显著性,但均显著快于阴道
组。最大压值未明确指出,但除了给药后15min时舌下组的宫内压稍低于口服组外
g等 [10] 统计了孕龄<7周、7~9周、>9周的完全流产率分别为100%、85.2%和
类风湿性关节炎毕业设计计划书

类风湿性关节炎毕业设计计划书(中英文版)英文文档:Title: Rheumatoid Arthritis Thesis ProposalIntroduction:Rheumatoid arthritis (RA) is a chronic autoimmune disease that primarily affects the joints but can also impact other body systems.This thesis proposal aims to explore the pathogenesis, diagnosis, and treatment strategies for RA, with the goal of improving the quality of life for patients.Objectives:1.To review the current literature on the pathogenesis of RA, focusing on the role of inflammation and autoimmunity.2.To investigate novel diagnostic markers for RA, including biomarkers and imaging techniques.3.To evaluate existing treatment modalities for RA, such as disease-modifying antirheumatic drugs (DMARDs) and biologics.4.To propose a comprehensive treatment plan that combines conventional medications with alternative therapies, such as physical therapy and lifestyle modifications.Methods:1.A systematic review of the literature will be conducted to identifykey factors contributing to the pathogenesis of RA.boratory experiments will be performed to validate the diagnostic potential of novel biomarkers and imaging techniques.3.A retrospective cohort study will be conducted to assess the efficacy and safety of various treatment modalities for RA.4.A prospective randomized controlled trial will be conducted to evaluate the effectiveness of a comprehensive treatment plan.Expected Results:1.A better understanding of the pathogenesis of RA, leading to improved diagnostic and treatment strategies.2.The identification of novel diagnostic markers that can accurately predict RA onset and progression.3.An evidence-based comprehensive treatment plan that optimizes the management of RA, reducing disease activity and improving patient outcomes.Conclusion:This thesis proposal aims to contribute to the advancement of knowledge in the field of rheumatology by investigating the pathogenesis, diagnosis, and treatment of RA.The expected results will have a significant impact on the diagnosis and management of RA, ultimately improving the quality of life for patients.中文文档:标题:类风湿性关节炎毕业设计计划书引言:类风湿性关节炎(RA)是一种慢性自身免疫性疾病,主要影响关节,但也可能影响其他身体系统。
降钙素原的临床价值和最新进展

降钙素原的临床价值和最新进展1. 引言降钙素原(procalcitonin,PCT)是一种由甲状腺细胞合成的前体多肽,其主要作用是调控钙离子代谢。
近年来,随着对降钙素原的深入研究,人们逐渐发现降钙素原在临床应用中具有重要的价值。
本文将介绍降钙素原的临床价值以及最新的研究进展。
2. 降钙素原的临床价值降钙素原在临床上可作为一种生物标志物,用于评估感染性疾病的严重程度和预后。
以下是降钙素原的临床价值的几个方面:2.1. 临床诊断降钙素原可以帮助区分细菌感染和其他炎症状态,如病毒感染或创伤。
一般来说,细菌感染引起的降钙素原水平增高较明显,而其他原因引起的炎症状态较低。
因此,通过监测降钙素原水平可以辅助医生进行感染的早期诊断。
2.2. 感染的严重程度评估降钙素原水平与感染的严重程度密切相关。
高水平的降钙素原提示感染较为严重,需要及时采取治疗措施。
而低水平的降钙素原可能表明感染轻微或已经得到控制。
2.3. 感染预后评估降钙素原水平的动态变化可以反映患者感染的预后情况。
降钙素原水平下降速度慢或持续升高可能提示感染治疗效果不佳或并发症的出现。
因此,监测降钙素原水平可以帮助医生评估患者的治疗反应和预后情况。
3. 降钙素原的最新进展近年来,不断有新的研究成果揭示了降钙素原的新的临床应用。
以下是关于降钙素原的最新研究进展:3.1. 降钙素原与败血症的关系降钙素原在败血症的早期诊断和评估中起着重要作用。
最新的研究表明,通过降钙素原的监测可以帮助医生更早地发现败血症,并评估其严重程度和预后。
此外,降钙素原还可以用于指导败血症的治疗策略。
3.2. 降钙素原在呼吸道感染中的应用降钙素原可以作为辅助指标用于评估呼吸道感染的严重程度和预后。
最新的研究发现,降钙素原水平与肺炎的严重程度和治疗效果密切相关。
因此,通过监测降钙素原水平可以帮助医生制定更个性化的治疗方案。
3.3. 降钙素原与免疫反应的关系降钙素原在免疫反应中扮演着重要的角色。
《膀胱占位性病变的诊疗方案》诊疗建议(一)
㊃诊疗征询㊃‘膀胱占位性病变的诊疗方案“诊疗建议(一)窦卫超李响d o i:10.3870/j.i s s n.1674-4624.2020.06.017患者体检发现膀胱占位10d㊂诊疗征询原文见‘现代泌尿生殖肿瘤杂志“2019年第11卷第1期第64页㊂本例患者特点总结如下:老年男性,体检发现膀胱占位,既往有多年吸烟史㊁膀胱结石手术史㊂影像学检查:膀胱左侧壁恶性肿瘤可能;双肺结节㊂膀胱镜检查:膀胱内球形肿物,基底较宽㊂经尿道膀胱肿瘤电切术(t r a n s u r e t h r a l r e s e c t i o n o f b l a d d e r t u m o r,T U R B T)后肿物病检:伴有恶性血管球样瘤特征的肉瘤样癌,浸润固有层,未侵犯肌层,部分区域可见坏死㊂周围黏膜腺性膀胱炎改变伴尿路上皮原位癌㊂切缘阴性,基底部未见平滑肌受累㊂随机活检:膀胱左右侧壁均见高级别尿路上皮原位癌;膀胱底壁见高级别非浸润性乳头状尿路上皮癌,伴内翻生长㊂患者目前诊断:1.膀胱恶性肿瘤:①肉瘤样癌(具有恶性血管球瘤样特征)(p T1N x M x);②高级别尿路上皮原位癌(p T i s N x M x);2.双肺结节性质待诊:转移灶?;3.膀胱结石(膀胱切开取石术后)㊂该患者考虑为复杂病理类型的膀胱肿瘤,属于E A U指南中提到的最高危非肌层浸润性膀胱癌,进展为肌层浸润性膀胱癌(m u s c l e i n v a s i v e b l a d d e r c a n c e r,M I B C)的风险较高,最合理的治疗方式为根治性膀胱切除术(r a d i c a l c y s t e c t m y, R C),但患者拒绝上述治疗,要求行保留膀胱的治疗方案㊂目前缺乏最高危非肌层浸润性膀胱癌的治疗证据㊂在所有表浅的膀胱癌中,T a约占70%,T1占20%,原位癌占10%[1]㊂高级别T1期(旧称T1G3)膀胱癌具有异质性特点,治疗颇具挑战性㊂高级别T1期膀胱癌发生进展的风险增加约17%[2]㊂M a r t i n-D o y l e等[3]的荟萃分析显示,T1期膀胱癌5年复发率为42%,进展率为21%,肿瘤特异性生存率为87%㊂肿瘤分期的不确定性及初次行T U R B T病理分期不足导致高级别T1期的病理诊断困难㊂K u l k a r n i等[4]总结文献认为,所有T1G3患者均应再次接受T U R B T㊂M a t u l e w i c z等[5]回顾性分析国立癌症数据库2010~2012年18277例高级别T1期膀胱癌患者的数据,结果显示行根治膀胱切除术时41%的患者出现疾病进展(p T2或更高), 12.7%的患者发生淋巴结转移㊂高级别T1期膀胱癌理想的治疗方法尚存在争议㊂尽管从治愈肿瘤的角度上讲,R C为最佳选择,但手术相关并发症㊁生活质量下降㊁精神心理因素成为患者要求行保留膀胱治疗的主要原因;对某些非进展肿瘤患者而言,根治性膀胱切除则意味着过度治疗㊂对于不适合或拒绝根治性手术的高级别T1期膀胱癌患者,选择哪种保膀胱治疗方案是泌尿外科医生面临的主要挑战㊂目前保留膀胱的治疗主要为多模式治疗,包括T U R B T㊁放疗及化疗㊂初次行T U R B T较高的肿瘤残留率是导致术后患者复发㊁进展的重要因素㊂D i v r i k等[6]前瞻性的随机研究比较p T1期膀胱癌初次T U R B T后2~6周再次T U R B T+膀胱灌注丝裂霉素C(m i t o m y c i n C,MM C)与未行再次T U R B T +MM C的生存差异,结果显示初次电切后较高的肿瘤残留率导致未接受二次T U R B T的患者具有较高的复发率,且残余肿瘤与肿瘤病理分级有关(P=0.009)㊂尽管总生存率相似,3年无复发生存率二次电切组明显高于对照组(69%v s. 37%),尤其是高级别肿瘤组㊂作者建议对于高级别T1期疾病的患者推荐二次电切以实现更好的无复发生存㊂国外学者研究报道二次T U R B T不含肌层与含肌层的标本低估病变的风险分别为40%~69%[7-8]㊁30%[7]㊂D u t t a等[7]回顾分析214例接受根治性膀胱切除的患者,其中分期为T1或低于T1的患者占26%,结果显示40%的患者分期不足,作者进一步分析显示影像学怀疑肿瘤㊁标本中缺乏肌层患者更容易出现分期不足㊂上述研究提示二次电切的必要性㊂尽管辅助治疗的证据不如新辅助治疗,当前大量证据支持对未接受新辅助治疗的高复发风险的患者行辅助化疗㊂三联治疗主要包括最大限度T U R B T+同期放化疗,对治疗无反应或M I B C行补救性膀胱切除㊂化疗可根除微转移灶,使肿瘤细胞对放疗敏感㊂三联治疗被视为M I B C最有效的保留膀胱的治疗方式,为根治性膀胱切除的替代治疗方案㊂尿路上皮癌对于放疗及化疗敏感,体现出三联治疗的合理性㊂Röd e l等[9]研究显示T U R B T后辅助放疗或放化疗可为高危表浅的膀胱癌患者提供较高的治愈及保留膀胱机会㊂但初次T U R B T时,约20%~30%表浅的肿瘤分期不足[7-8,10],可能已存在肿瘤肌层浸润,放疗/放化疗有可能降低肿瘤进展及盆腔淋巴结转移率,p T1期微转移发生率约5%~10%, R C后超过35%的表浅膀胱癌进展至p T2期[10]㊂W e i s s 等[11]研究显示与单纯T U R B T相比,术后辅助膀胱灌注卡介苗(b a c i l l e c a l m e t t e g u e r i n,B C G)或化疗药物如MM C可使总复发率降低30%,5年内疾病进展率约15%~40%㊂A r e n d s等[12]的随机试验比较了中高危非肌层浸润性膀胱癌患者T U R B T后辅助热灌注化疗MM C与B C G灌注治疗的疗效,结果显示热灌注化疗的2年无复发生存期高于B C G 灌注治疗㊂但该研究过早结束,研究动力不足㊂此外,很难做到对患者及医生的盲法导致不可避免的偏倚㊂S y l v e s t e r 等[13]的分析显示与单纯T U R B T相比,术后即刻膀胱灌注化疗药物使T a㊁T1期患者复发风险降低40%㊂Röd e l等[14]研究评价高危T1㊁M I B C患者接受保留膀胱的T U R B T联合5-F U/顺铂及放疗的安全性㊁耐受性㊁疾病控制情况,结果显示T1期患者无肌层浸润复发局部控制率为85%,5年无转移生存率为74%;此外该方案治疗的耐受性较好,76%的患者完成该治疗方案,且疗效似乎优于单纯放疗或联合卡铂或顺铂的放化疗㊂新型化疗药物如紫杉醇及吉西他滨正在被实验用于联合放疗,有望进一步改善膀胱癌的膀胱保留㊂W i t t l i n g e r等[15]评价了T U R B T+同步放化疗+局部深部热疗四联治疗模式用于高危T1及T2期膀胱癌患者的疗效及安全性,结果显示3年的病理学完全缓解率(c o m p l e t e r e-s p o n s e,C R)为96%(43/45),局部无复发生存率为85%,总生存率为80%,疾病特异性生存率为88%,无转移生存率为㊃673㊃现代泌尿生殖肿瘤杂志2020年12月第12卷第6期J C o n t e m p U r o l R e p r o d O n c o l,D e c e m b e r2020,V o l12,N o.6作者单位:610041四川大学华西医院泌尿外科泌尿外科研究所通信作者:李响,E-m a i l:x i a n g l i.87@163.c o m89%,81%的患者无肌层浸润性复发或局部进展,保留膀胱生存率为96%㊂在不良反应方面,3㊁4级急性毒性反应发生率为29%㊂生活质量分析提示多数患者对其膀胱功能满意㊂W e i s s等[16]研究了T U R B T后放疗联合铂类为基础的放化疗治疗141例高危T1膀胱癌(其中高级别T1期84例)的治疗效果,研究显示C R为88%(121/137),高级别T1期膀胱癌患者的5年㊁10年C R分别为13%㊁29%,疾病特异性生存率分别为80%㊁71%,80%以上患者保留膀胱生存,多数患者对排尿功能满意㊂T U R B T后放疗/放化疗的选择性保留膀胱治疗方案为高级别T1期膀胱癌膀胱灌注治疗或早期膀胱切除术的合理的替代治疗方案㊂S h i p l e y[17]认为,若W e i s s 提出的三联治疗证实优于B C G治疗,可以通过密切随访,对复发患者行R C可取代即刻膀胱切除术作为高级别T1期患者的标准治疗方案㊂A kçe t i n等[18]的研究报道T1膀胱癌T U R B T后放化疗的长期治疗结果,结果显示,C R为90.2%,总的疾病进展率为14%,5年总存率及无病生存率分别为76%㊁93%㊂在多学科团队协助下的多模式联合治疗是高级别T1期膀胱癌患者安全㊁治愈性的治疗选择㊂作者认为放化疗联合T U R B T作为高级别T1期膀胱癌的一线治疗选择是合理的㊂G i a c a l o n e等[19]研究分析了麻省总医院425例c T2~T4a M I B C患者接受多学科综合治疗的长期结果,中位随访时间7.21年,其5年㊁10年疾病特异性生存率分别为66%㊁59%,5年㊁10年总生存率分别为57%㊁39%,5年膀胱保留率达71%㊂接受多学科综合治疗患者的C R及保膀胱率均较高㊂多因素分析显示T2㊁放化疗的完全反应率及出现肿瘤相关的原位癌为总生存期及疾病特异性生存率的独立预测因素㊂该研究提示多学科综合治疗用于高危非肌层浸润性膀胱癌的合理性㊂就该患者而言,膀胱内存在多种病理类型的肿瘤,且病理分级为高分级,含原位癌㊂因此,我们建议患者在初次手术后4~6周再次行T U R B T,术后行顺铂/5-F U为基础的同步放化疗㊂此外,患者肺部结节诊断不清,建议患者完善胸部薄层增强C T或P E T/C T进一步明确肺部结节病变性质,若证实为转移灶,则应按照转移性膀胱癌治疗㊂若患者二次T U R B T证实疾病进展或肿瘤复发,建议行补救性膀胱切除术㊂对该病例二次T U R B T后随访建议:前2年每3个月行膀胱镜检查;2年后可延长随访间隔㊂对于该患者应当每年行上尿路影像学检查㊂若患者随访过程中出现疾病进展㊁复发,建议行补救性膀胱切除术㊂有学者认为由于变异的组织学类型的膀胱癌进展风险较高,对于该类型的膀胱肿瘤患者当考虑行R C[20]㊂需要注意的是,对变异病理类型的膀胱癌的合理治疗目前缺乏相关证据,仍需要进一步研究㊂在决定选择R C及保守治疗时,需要综合考虑T1亚分期㊁合并原位癌㊁肿瘤大小㊁外观㊁淋巴血管侵犯㊁肾盂积水等因素㊂目前尚缺乏R C与保留膀胱多模式综合治疗直接对比的随机对照试验数据,我们期待上述研究能够更好地指导用于高级别T1期膀胱癌的治疗㊂参考文献[1] K i r k a l i Z,C h a n T,M a n o h a r a n M,e t a l.B l a d d e r c a n c e r:e p i-d e m i o l o g y,s t a g i n g a n d g r a d i n g,a n d d i a g n o s i s[J].U r o l o g y,2005,66(6S u p p l1):4-34.[2] P a l o u J,S y l v e s t e r R J,F a b a O R,e t a l.F e m a l e g e n d e r a n dc a r c i n o m a i n s i t u i n t h e p r o s t a t i c u r e t h r a a r e p r o g n o s t i c f a c-t o r s f o r r e c u r r e n c e,p r o g r e s s i o n,a n d d i s e a s e-s p e c i f i c m o r t a l i-t y i n T1G3b l a d d e r c a n c e r p a t i e n t s t r e a t e d w i t h b a c i l l u sC a l m e t t e-G u e r i n[J].E u r U r o l,2012,62(1):118-125.[3] M a r t i n-D o y l e W,L e o w J J,O r s o l a A,e t a l.I m p r o v i n g s e l e c-t i o n c r i t e r i a f o r e a r l y c y s t e c t o m y i n h i g h-g r a d e t1b l a d d e rc a n c e r:a m e t a-a n a l y s i s o f15,215p a t i e n t s[J].J C l i n O n c o l,2015,33(6):643-650.[4] K u l k a r n i G S,H a k e n b e r g OW,G s c h w e n d J E,e t a l.A n u p-d a te d c r i t i c a l a n a l y s i s of t h e t r e a t m e n t s t r a t eg y f o r n e w l y d i-a g n o s e d h i g h-g r a d e T1(p r e v i o u s l y T1G3)b l a d d e rc a n c e r[J].E u r U r o l,2010,57(1):60-70.[5]M a t u l e w i c z R S,F r a i n e y B T,O b e r l i n D T,e t a l.H i g h-R i s ko f A d v e r s e P a t h o l o g i c F e a t u r e s i n P a t i e n t s W i t h C l i n i c a l T1H i g h-G r a d e B l a d d e r C a n c e r U n d e r g o i n g R a d i c a l C y s t e c t o m y[J].J N a t l C o m p r C a n c N e t w,2016,14(11):1403-1411.[6] D i̇v r i̇k R T,Y i l d i r i mÜt,Z o r l u F,e t a l.T h e E f f e c t o f R e p e a tT r a n s u r e t h r a l R e s e c t i o n o n R e c u r r e n c e a n d P r o g r e s s i o n R a t e si n P a t i e n t s W i t h T1T u m o r s o f t h e B l a d d e r W h o R e c e i v e d I n-t r a v e s i c a l M i t o m y c i n:A P r o s p e c t i v e,R a n d o m i z e d C l i n i c a lT r i a l[J].J U r o l,2006,175(5):1641-1644.[7] D u t t a S C,S m i t h J A J r,S h a p p e l l S B,e t a l.C l i n i c a l u n d e rs t a g i n g o f h i g h r i s k n o n m u s c l e i n v a s i v e u r o t h e r a l c a r c i n o m a t r e a t e d w i t h r a d i c a l c y s t e c t o m y[J].J U r o l,2001,166(2): 490-493.[8] H e r r HW.T h e v a l u e o f a s e c o n d t r a n s u r e t h r a l r e s e c t i o n i n e-v a l u a t i n g p a t i e n t s w i t h b l a d d e r t u m o r s[J].J U r o l,1999,162(1):74-76.[9] Röd e l C,D u n s t J,G r a b e n b a u e r G G,e t a l.R a d i o t h e r a p y i sa n e f f e c t i v e t r e a t m e n t f o r h i g h-r i s k T1-b l a d d e rc a n c e r[J].S t-r a h l e n t h e r O n k o l,2001,177(2):82-88.[10] W e i s s C,O t t O J,W i t t l i n g e r M,e t a l.T r e a t m e n t o p t i o n s f o rh i g h-r i s k T1b l a d d e r c a n c e r:s t a t u s q u o a n d f u t u r e p e r s p e c-t i v e s o f r a d i o c h e m o t h e r a p y[J].S t r a h l e n t h e r O n k o l,2008,184(9):443-449.[11] W e i s s C,W o l z e C,E n g e h a u s e n D G,e t a l.R a d i o c h e m o t h e r a-p y a f t e r t r a n s u r e t h r a l r e s e c t i o n f o r h i g h-r i s k T1b l a d d e r c a n c-e r:a n a l t e r n a t i v e t o i n t r a v e s i c a l t h e r a p y o r e a r l y c y s t e c t o m y?[J].J C l i n O n c o l,2006,24(15):2318-2324.[12] A r e n d s T J,N a t i v O,M a f f e z z i n i M,e t a l.R e s u l t s o f a R a n-d o m i se d C o n t r o l l e d T r i a l C o m p a r i n g I n t r a v e s i c a l C h e m o h y-p e r t h e r m i a w i t h M i t o m y c i n C V e r s u s B a c i l l u s C a l m e t t e-G u e r-i n f o r A d j u v a n t T r e a t m e n t o f P a t i e n t s w i t h I n t e r m e d i a t e-a n dH i g h-r i s k N o n-M u s c l e-i n v a s i v e B l a d d e r C a n c e r[J].E u r U r o l,2016,69(6):1046-1052.[13]S y l v e s t e r R J,O o s t e r l i n c k W,v a n d e r M e i j d e n A P.A s i n g l ei mm e d i a t e p o s t o p e r a t i v e i n s t i l l a t i o n o f c h e m o t h e r a p y d e c r e a-s e s t h e r i s k o f r e c u r r e n c e i n p a t i e n t s w i t h s t a g e T a T1b l a d d e rc a n c e r:a m e t a-a n a l y s i s o f p u b l i s h ed re s u l t s of r a n d o m i z e dc l i n i c a l t r i a l s[J].J U r o l,2004,171(6P t1):2186-2190.[14] Röd e l C,G r a b e n b a u e r G G,Küh n R,e t a l.O r g a n p r e s e r v a-t i o n i n p a t i e n t s w i t h i n v a s i v e b l a d d e r c a n c e r:i n i t i a l r e s u l t s o fa n i n t e n s i f i e d p r o t o c o l o f t r a n s u r e t h r a l s u r g e r y a n d r a d i a t i o nt h e r a p y p l u s c o n c u r r e n t c i s p l a t i n a n d5-f l u o r o u r a c i l[J].I n t JR a d i a t O n c o l B i o l P h y s,2002,52(5):1303-1309. [15] W i t t l i n g e r M,R o d e l C M,W e i s s C,e t a l.Q u a d r i m o d a l t r e a t-m e n t o f h i g h-r i s k T1a n d T2b l a d d e r c a n c e r:t r a n s u r e t h r a l t u m o r r e s e c t i o n f o l l o w e d b y c o n c u r r e n t r a d i o c h e m o t h e r a p ya n d r e g i o n a l d e e p h y p e r t h e r m i a[J].R a d i o t h e r O n c o l,2009,93(2):358-363.[16] W e i s s C,E n g e h a u s e n D G,K r a u s e F S,e t a l.R a d i o c h e m o t h-e r a p y w i t h c i s p l a t i n a n d5-f l u o r o u r a c i l a f t e r t r a n s u r e t h r a l s u r-g e r y i n p a t i e n t s w i t h b l a d d e r c a n c e r[J].I n t J R a d i a t O n c o lB i o l P h y s,2007,68(4):1072-1080.[17] S h i p l e y WU.R a d i a t i o n-s e n s i t i z i n g c h e m o t h e r a p y a f t e r t r a n-s u r e t h r a l r e s e c t i o n a s a n a l t e r n a t i v e t r e a t m e n t f o r h i g h-r i s k㊃773㊃现代泌尿生殖肿瘤杂志2020年12月第12卷第6期J C o n t e m p U r o l R e p r o d O n c o l,D e c e m b e r2020,V o l12,N o.6T1b l a d d e r c a n c e r[J].N a t C l i n P r a c t U r o l,2007,4(1):24-25.[18] A kçe t i n Z,T o d o r o v J,Tüz e l E,e t a l.R a d i o c h e m o t h e r a p y a f-t e r t r a n s u r e t h r a l r e s e c t i o n i s a n e f f e c t i v e t r e a t m e n t m e t h o d i nT1G3b l a d d e r c a n c e r[J].A n t i c a n c e r R e s,2005,25(3A): 1623-1628.[19] G i a c a l o n e N J,S h i p l e y WU,C l a y m a n R H,e t a l.L o n g-t e r mO u t c o m e s A f t e r B l a d d e r-p r e s e r v i n g T r i-m o d a l i t y T h e r a p y f o rP a t i e n t s w i t h M u s c l e-i n v a s i v e B l a d d e r C a n c e r:A n U p d a t e dA n a l y s i s o f t h e M a s s a c h u s e t t s G e n e r a l H o s p i t a l E x p e r i e n c e[J].E u r U r o l,2017,71(6):952-960.[20] C h a n g S S,B o o r j i a n S A,C h o u R,e t a l.D i a g n o s i s a n d T r e a t-m e n t o f N o n-M u s c l e I n v a s i v e B l a d d e r C a n c e r:A U A/S U OG u i d e l i n e[J].J U r o l,2016,196(4):1021-1029.(收稿日期:2020-08-31)(本文编辑:刘倩倩)作者单位:430030武汉,华中科技大学同济医学院附属同济医院泌尿外科通信作者:刘征,E-m a i l:l z2013t j@163.c o m ㊃诊疗征询㊃‘膀胱占位性病变的诊疗方案“诊疗建议(二)刘征d o i:10.3870/j.i s s n.1674-4624.2020.06.018患者为62岁男性,初次发现膀胱肿瘤,予以充分经尿道膀胱电切术(瘤体㊁切缘㊁基底㊁左侧壁㊁右侧壁㊁顶壁㊁底壁),术后病理为肉瘤样癌(p T1N x M x),合并高级别尿路上皮癌㊁原位癌(p T i s N x M x)㊂对于这样的病人如何开展下一步处理呢?我们可以看看文献再做参考㊂文献报告,膀胱的肉瘤样癌属于膀胱原发性肉瘤,罕见㊂膀胱原发性肉瘤是发生在膀胱的恶性软组织非上皮肿瘤,发病率不超过膀胱肿瘤的1%; 50%为平滑肌肉瘤,好发于中老年人,20%为横纹肌肉瘤,好发于儿童和青少年[1];剩下的为血管肉瘤㊁骨源性肉瘤㊁黏液脂肪肉瘤㊁纤维肉瘤和未分化的肉瘤[2]㊂未分化的肉瘤包括肉瘤样癌(s a r c o m a t o i d c a r c i n o m a,S C)和癌肉瘤(c a r c i n o s a r-c o m a,C S),其更为罕见,在膀胱恶性肿瘤中占0.07%和0.09%[3]㊂病理上,S C呈间充质梭状,细胞中存在上皮样分化,免疫组化表现为上皮细胞分子如细胞角蛋白㊁C K-8/18㊁G A T A3呈阳性[4];而C S具有恶性上皮与典型肉瘤组织学结构,具有肉瘤的生物学行为特征㊂膀胱S C由癌性和肉瘤性两部分组成㊂最近的WHO组织分类将此术语应用于所有显示恶性上皮和间充质分化的形态学或免疫学证据的肿瘤,这类肿瘤被认为是多克隆组合的肿瘤或分化程度不同的单克隆肿瘤,W r i g h t等[3]的分子研究支持后一种理论㊂在临床表现上,这两种未分化的肉瘤预后相当差, W r i g h t等[3]统计对比了46515例尿路上皮癌㊁135例S C和166例C S患者,1年未校正生存率分别为77%㊁54%和48%,5年未校正生存率分别为47%㊁37%和17%㊂S C和C S与尿路上皮癌相比,发病年龄相近,但发现时T期较高,局部和远处转移更为频繁㊂多因素分析显示,S C(H R: 1.18,95%C I:0.91~1.52)和C S(H R:2.00,95%C I;1.65 ~2.41)患者的死亡风险高于尿路上皮癌患者㊂C S的总死亡率比S C差(H R:1.70,95%C I:1.23~2.34)㊂所以,与尿路上皮癌患者相比,S C和C S处于更晚期,即使在校正后,其死亡风险也更大㊂发现S C这样的病理类型,目前文献不支持保留膀胱㊂S u i等[5]统计了489例S C患者的预后,中位生存期只有18.4个月,在多变量C o x比例分析中,与单纯膀胱保留手术相比,单纯根治性膀胱切除术或联合多模式治疗(化疗或放疗)可显著降低死亡风险㊂高剂量术中放射治疗(H D-I O R T)也许可以尝试,K a t e s等[6]对4例高危局部晚期的S C 患者行H D-I O R T治疗,随访2年以上,均存活,相比25例没有行H D-I O R T治疗的患者,1年生存率为52%㊂综上所述,对于这样的诊断性电切后病理发现为膀胱S C的患者,预后差,不建议保留膀胱,若行膀胱根治性切除,术后辅助放疗或放疗,或许能延长患者生存时间㊂参考文献[1] P a r e k h D J,J u n g C,O'C o n n e r J,e t a l.L e i o m y o s a r c o m a i n u-r i n a r y b l a d d e r a f t e r c y c l o p h o s p h a m i d e t h e r a p y f o r r e t i n o b l a s-t o m a a n d r e v i e w o f b l a d d e r s a r c o m a s[J].U r o l o g y,2002,60(1):164.[2] L o t t S,L o p e z-B e l t r a n A,M o n t i r o n i R,e t a l.S o f t t i s s u e t u-m o r s o f t h e u r i n a r y b l a d d e r P a r t I I:m a l i g n a n t n e o p l a s m s[J].H u m P a t h o l,2007,38(7):963-977.[3] W r i g h t J L,B l a c k P C,B r o w n G A,e t a l.D i f f e r e n c e s i n s u r-v i v a l a m o n g p a t i e n t s w i t h s a r c o m a t o i d c a r c i n o m a,c a r c i n o s a r-c o m a a nd u r o t he l i a l c a r c i n o m a of t h e b l a d d e r[J].J U r o l,2007,178(6):2302-2306.[4] D a g a G,K e r k a r P.S a r c o m a t o i d C a r c i n o m a o f U r i n a r y B l a d d e r:aC a s e R e p o r t[J].I n d i a n J S u r g O n c o l,2018,9(4):644-646.[5] S u i W,M a t u l a y J T,O n y e j i I C,e t a l.C o n t e m p o r a r y t r e a t-m e n t p a t t e r n s a n d o u t c o m e s o f s a r c o m a t o i d b l a d d e r c a n c e r[J].W o r l d J U r o l,2017,35(7):1055-1061.[6] K a t e s M,C h a p p i d i M R,B r a n t A,e t a l.H i g h d o s e-r a t e I n-t r a-O p e r a t i v e R a d i a t i o n T h e r a p y D u r i n g H i g h R i s k G e n i t o u r i-n a r y S u r g e r y:I n i t i a l O b s e r v a t i o n s a n d a P r o p o s a l f o r i t s S t u d-y i n B l a d d e r C a n c e r[J].B l a d d e r C a n c e r,2017,3(3):191-199.(收稿日期:2020-09-04)(本文编辑:刘倩倩)㊃873㊃现代泌尿生殖肿瘤杂志2020年12月第12卷第6期J C o n t e m p U r o l R e p r o d O n c o l,D e c e m b e r2020,V o l12,N o.6。
rhBMP-2综述1(修订版)
隐患浮现-关于rhBMP-2的脊柱外科运用的批判性综述以往,脊柱融合术须依靠自体骨移植或异体骨移植,但当患者存在全身性代谢异常或不利的局部条件时,传统的骨移植技术难以奏效。
因此,人们开始寻找骨移植的替代物,重组人骨形态发生蛋白(rhBMP-2)为人们带来希望。
rhBMP-2在2003年由美国FDA批准上市,近年来随着其临床运用的增多,人们逐渐认识到其潜在的巨大风险,在回过头来审视早期的研究时,人们发现研究中存在巨大的不良事件漏报和本身的试验设计缺陷,其中可能存在的利益关联更是引起巨大的争议。
当然本文并不旨在评价这项工作,而在试图给出一个可能不完整但很清晰的信息。
一.公正性面临挑战-相关利益关系在13个早期研究中,其中一个的研究者们与rhBMP-2制造商利益关系不清楚。
剩余12个研究中,每项研究已知的经济资助平均在1200万到1600万美元之间,另外每位研究者还有着100万到1000万美元不等的津贴[1-3]。
二.可能长期被低估的rhBMP-2相关不良事件发生风险企业资助的13篇论著中,共纳入了780例使用了rhBMP-2的患者,但未报告任何rhBMP-2相关不良反应事件,而根据FDA数据及随访资料,在脊柱融合术中,rhBMP-2相关不良事件发生率均高于上述13篇论著所述的结论,而且在后外侧融合及后路腰椎椎间融合术的试验中,对照组采用的研究设计有缺陷,其髂嵴供区的疼痛发生率也严重高估。
当然,欲更准确得进行临床效果优劣的评价,尚需更细致和广泛的数据和研究。
(一)在进行后外侧融合术(PLF)时,rhBMP-2组与髂骨自体骨移植组在早期后背及腿部疼痛,硬膜外血肿及伤口并发症的发生率比较。
Boden于2002年报道的研究里,认为没有rhBMP-2相关并发症[4]。
不过,Boden指出了可能的不良事件,在早期(此时评估对髂骨自体骨移植组不利),腿痛在实验组有所增加,早期的功能恢复评价也处于劣势。
该研究规模虽小,但与事先猜测的rhBMP-2相关并发症一致。
原发性自发性气胸的临床治疗进展
DOI:10.16096/ki.nmgyxzz.2021.53.04.015原发性自发性气胸的临床治疗进展隋璐1▲,贺钢枫川(1.内蒙古医科大学包头临床医学院,内蒙古包头014040;2.包头市中心医院,内蒙古包头014010)[摘要]原发性自发性气胸(primary spontaneous pneumothorax PSP)的发生机制尚不明确,在健康的成年人及青少年中依然可以发生。
现就目前原发性自发性气胸的治疗方式及进展进行综述。
[关键词]原发性自发性气胸;治疗[中图分类号]R561.4[文献标识码]A[论文编号]1004-0951(2021)04-0431-04胸膜腔是不含气体的密闭潜在性腔隙,当气体进入胸膜腔造成积气状态时,称为气胸(Pneumothorax)o资料显示“气胸”概念由Laennec最早提出(分别在1803年和1819年提出)⑴,气胸作为全球范围内是发病率较高的疾病,尚缺乏大数据证实其流行病学指向和趋势。
原发性自发性气胸(primary spontaneous pneumothorax PSP)的发生机制尚不明确,在健康的成年人及青少年中依然可以发生。
现就目前PSP的治疗方式及进展进行综述。
1PSP的保守治疗PSP的积气量小于20%或肺尖与胸膜顶距离小于3cm,无临床表现(稳定性小量气胸),经观察和氧气支持治疗即可痊愈。
保守治疗需密切监测病情变化。
若病人年龄偏大且有肺基础疾病如COPD,其胸膜破裂口愈合慢,呼吸困难等症状严重,即使气胸量较小亦不主张保守治疗。
2PSP的排气疗法包括简单手动抽吸及胸腔闭式引流。
气胸量大于20%的原发性自发性气胸可以用简单手动抽吸来治疗。
气胸量大于20%、临床症状稳定(或临床症状不稳定、呼吸困难明显、肺压缩程度较重)的患者也可选用胸腔闭式引流治疗。
经研究表明,简单抽吸与胸导管引流对于原发性自发性气胸的治疗成功率、近期效果无明显差异⑵,一项前瞻性随机试验证实,针吸术是首发PSP 发作及稳定PSP患者的良好初始治疗方法⑶。
选择性COX-2抑制剂引起心血管风险的研究进展

目前临床上广泛使用的抗炎药物主要有两种,甾体抗炎药(steroidal anti-inflammatory drugs ,SAIDs )和非甾体抗炎药[1](non-steroid anti-inflammatory drugs ,NSAIDs )。
其中NSAIDs 是最常用的抗炎药物[2],全世界每天有上亿人服用[3]。
2019年全球NSAIDs 市场规模为155.8亿美元,预计在2027年将达到243.5亿美元[4]。
所有NSAIDs 通过抑制环氧合酶(cyclooxygen‑ase ,COX )的亚型COX-1和/或COX-2发挥作用,该酶参与疼痛和炎症有关的前列腺素的形成[5]。
NSAIDs 通过抑制COX-1和/或COX-2,抑制前列腺素的合成,产生抗炎、解热和镇痛的作用,常用于调节炎症、发热和疼痛,但也会引起一系列的不良反应,比如损害胃肠道粘膜,升高血压,损害肾功能,并导致不良心血管事件,尤其是对老年人和心血管疾病患者来说风险更高[6-7]。
越来越多的证据表明,长期服用NSAIDs ,尤其是选择性的COX-2抑制剂,不论是在有已知疾病的患者中还是健康人群中,将显著增加心血管疾病的风险[8-9]。
我们就选择性COX-2抑制剂引起心血管风险的研究进行综述,以期为临床合理用药提供参考,减少不良反应,提高用药安全性。
1NSAIDs 的分类与发展NSAIDs 最早的类型是从柳树皮中提取的口服水杨酸酯类化合物[10],在19世纪中叶被用来缓解疼痛、发热和炎症反应。
对这类天然化合物的研究,促成了世上第一个NSAIDs ——阿司匹林于1898年诞生[11]。
至今阿司匹林仍然是世界上最常用的药物之一,每年大约消耗4万吨[12]。
非阿司匹林类NSAIDs 例如布洛芬于20世纪60年代初推出[13],此后种类迅速增多,发展至今已有上百种药物[14],按化学结构主要可分为以下几类:水杨酸类药物(如阿司匹林)、邻氨基苯甲酸衍生物(如甲芬那酸)、乙酸衍生物(如吲哚美辛、双氯芬酸醋、酮咯酸、舒林酸)、丙酸衍生物(如布洛芬、萘普生、酮洛芬和氟比洛芬)和烯酸衍生物(如吡罗昔康、美洛昔康)[15-18]。
消萎汤辨证加味治疗慢性萎缩性胃炎62例_张太坤
83第11卷 第1期 2009 年 1 月辽宁中医药大学学报JOURNAL OF LIAONING UNIVERSITY OF TCMVol. 11 No. 1 Jan . ,2009慢性萎缩性胃炎,是常见而又难治胃病之一,属于癌前病变,因此,阻止其发展、逆转其病变具有消萎汤辨证加味治疗慢性萎缩性胃炎62例张太坤,符 莹(东莞市太平人民医院,广东 东莞 523900)摘 要:以活血化瘀为主,采用自拟消萎汤辨证加味治疗慢性萎缩性胃炎62例,总有效率为93.55%。
提示该方能缓解该病临床症状,促进其胃镜和病理征象的改善,反映中医中药治疗本病的疗效较好,有其优越性。
关键词:慢性萎缩性胃炎;活血化瘀;消萎汤中图分类号:R573.3 文献标识码:B 文章编号:1673-842X (2009) 01- 0083- 02收稿日期:2008-07-20作者简介:张太坤(1971-),男(土家族),贵州思南人,主治医师,硕士研究生,研究方向:中西医结合治疗消化系统疾病。
Xiao Wei Decoction in chronic atrophic gastritis treatment:A clinical report of 62 casesZHANG Tai-kun, FU ying(Taiping People's Hospital of Dongguan City, Dongguan 523900, Guangdong, China)Abstract:In the method of activating blood circulation to dissipate blood stasis, used self-make Xiao Wei Decoction treatment of chronic atrophic gastritis 62 cases. The total effective rate was 93.55 percent. This method could alleviate the symptoms of this disease, and promote gastroscopy and pathological signs of improvement. The traditional Chinese medicine in the treatment of this disease was effective.Key words:Chronic atrophic gastritis; Activating blood circulation to dissipate blood stasis; Xiao Wei Decoction报道其最大扭矩为29.4Nm,在抗扭转力失效时,骨折端对合仍紧密,说明其有较好的抗扭转性能对稳定型转子间骨折经解剖复位后即可获得可靠固定,对不稳定性骨折,经解剖复位后可利用负重情况下骨折近端在固定装置上伸缩以寻找自身稳定位置,即所谓动力加压,对后内侧大块骨折片,可经过钢板近端螺钉行骨折片固定。
依托考昔在膝关节置换术后的镇痛效果_胡健

全膝关节置换(total knee anhroplasty,TKA)已成为治疗中老年终末期膝关节疾病的有效方式之一,是患者恢复运动机能,提高生活质量的常用术式。
术后早期功能锻炼离不开充分的术后镇痛。
有效的术后镇痛并非单纯在于减轻疼痛,还在于帮助患者早日下床活动,尽可能地恢复膝关节活动度并预防深静脉血栓形成等并发症的发生。
除此之外,有效的术后镇痛可减轻患者的焦虑,提高生活质量。
术后疼痛是TKA患者的主要顾虑,充分、有效的术后镇痛能够减轻患者痛苦,进行早期功能锻炼,直接关系到功能恢复和手术效果。
临床较常用的术后镇痛方法包括口服、肌肉或静脉注射以及椎管内给药等,都有一定的效果。
口服非甾体类抗炎药(NSAIDs)是镇痛的经典药物,对炎性疼痛有良好治疗效果,已在临床上广泛应用。
然而胃肠道及肾脏等系统的不良反应一直制约着临床使用,为此,许多科研工作者一直在寻找一种高效的NSAIDs。
上世纪90年代提出环氧化酶-2(cyclo-oxygen2,COX-2)后,国内外研究者做了大量的研究,研制出了许多选择性的COX-2抑制剂,统称昔布类(coxibs)[1],包括塞来昔布(celecoxib)、罗非昔布(rofecoxib)、依托昔布(etoricoxib)等。
目前临床上较广泛地应用选择性COX-2抑制剂治疗围术期的急性疼痛[2]。
本文就高选择性COX-2抑制剂依托考昔在TKA术后镇痛效果相关研究做一综述。
1依托考昔的相关药理特性TKA手术创伤和术中应用止血带会产生缺血-再灌注损伤,带来一系列的炎症反应,导致炎性介质和疼痛因子如组胺、5-羟色胺缓激肽和花生四烯酸等释放,除直接导致疼痛外还可使C0X-2的表达迅速增加,最终促使花生四烯酸转化为前列腺素,引起神经末梢的痛觉感受器敏感性增加,同时中枢C0X-2的表达上调,患者的疼痛阈值下降,产生痛觉过敏现象[3]。
阿片类药物是经典的术后镇痛药物,但由于其严重副作用如恶心、呕吐、便秘、呼吸抑制等,长期应用后可产生耐受性和依赖性,部分TKA患者术后抵触使用阿片类药物,临床医师对阿片类药物的使用也非常慎重。
一次性纤维环缝合器

2013年,纤维环缝合器,中国
纤维环缝合组:手术时间35—65min,平均48 min;出血量10—150ml,平均30 ml。对照组:手术时间30—60 min,平均45 min;出血量10-160 min,平均30 ml。两组术中无并发症发生。两组术前、术后7天、术后3个月VAS评分:
单击此处添加大标题内容
结论
Anular repair can be successfully accomplished in greater than 90% of cases if the discectomy is performed with the ultimate goal of repair being appreciated. Repairing the anulus fibrosus was shown to be beneficial by reducing the need for additional surgery, in particular those re-operations for true recurrent herniation. Repair of the annulus fiberosus thus closing the pathway for recurrent herniation has been proposed as an adjunctive method to further improve outcomes by mitigating the need for subsequent surgery.
美国34家临床机构,共58名医生 723名椎间盘摘除手术患者24个月的临床随访 经纤维环缝合后的患者,其复发率显著降低 与对照组相比,复发的患者数量减少了85%
血小板凝胶治疗Ⅲ~Ⅳ期压疮效果观察
血小板凝胶治疗Ⅲ~Ⅳ期压疮效果观察郭声敏; 吴显和; 韩兴平【期刊名称】《《护理学杂志》》【年(卷),期】2012(027)007【总页数】3页(P57-59)【关键词】压疮; 血小板凝胶; 康复护理【作者】郭声敏; 吴显和; 韩兴平【作者单位】泸州医学院附院康复医学科(四川泸州 646000)【正文语种】中文【中图分类】R472压疮是局部组织长时间受压后,血液循环障碍,持续缺血、缺氧、营养不良而致软组织溃烂和坏死。
压疮的愈合障碍一直是临床护理工作难题。
国内外学者将自体富血小板凝胶治疗技术用于治疗难治性皮肤溃疡[1-2]。
笔者对自体血小板凝胶治疗技术进行改进,并应用到重症压疮的处理中,取得较好效果,报告如下。
1 资料与方法1.1 一般资料 2009年6月至20011年4月,我科共收治51例压疮患者,其中根据欧洲压疮专家组(European Pressure Ulcer Advisory Panel,EPUAP)压疮分级标准[3]确诊创面为Ⅲ~Ⅳ期,年龄18~80岁,无低蛋白血症、无糖尿病病史、无贫血、未使用免疫抑制剂,且意识清楚、吞咽功能正常、生命体征正常、体重指数(BMI)≥18.5,对治疗方案知情同意的32例(36处创面)纳入本研究,男20例、女12例;年龄29~72(48.32±7.24)岁;尾骶部19处,髋部15处,外踝1处,后跟1处;病程7~128 d。
按入院先后顺序单数分为观察组,双数为对照组;同一例患者有2个或多个创面的,则以抛硬币的方式分组,正面为观察组,反面为对照组,观察组创面17处,对照组19处。
两组患者的年龄、性别、部位、体重指数和治疗前创面PUSH评分比较,差异无统计学意义(均P>0.05),具有可比性。
1.2 方法1.2.1 干预方法本研究经医院伦理道德委员会批准,参与人员经系统培训。
所有感染创面做“十点法”取分泌物进行细菌培养和药物敏感试验,全身使用敏感抗生素,创面均行局部标准处理(清创、引流、减压、定时更换敷料等)(12.25±1.02)d后,创面坏死组织基本清除且血供良好。
D-二聚体与纤维蛋白水平与代偿期肝硬化和失代偿期肝硬化的相关性分析
纤维蛋白原(FIB)为一类经肝脏合成的糖蛋白物质,其能 够反映出患者机体是否存在凝血功能障碍情况 [1];而 D- 二聚体 则为一类交联纤维蛋白纤溶酶降解之后产生的一类具有特异性 功能的降解产物,通过观察该项指标能够判断高凝状态以及继 发性纤溶亢进 [1]。结合实际情况,本文全面探讨 D- 二聚体与纤 维蛋白的测定在代偿期肝硬化和失代偿期肝硬化中的相关性, 为患者的疾病诊断以及治理方案制定提供帮助。 1 资料与方法
174 中国处方药 第 19 卷 第 6 期
·临床研究·
D- 二聚体与纤维蛋白水平与代偿期肝硬化 和失代偿期肝硬化的相关性分析
王海燕,谢丽莉* (天津市第一中心医院检验科,天津 300192)
【摘要】目的 分析 D- 二聚体与纤维蛋白的测定在代偿期肝硬化和失代偿期肝硬化中的相关性,旨在为相关人员的研究工作提供参考文献。方 法 选择 2017 年 4 月 22 日~ 2020 年 4 月 22 日就诊的肝硬化患者 136 例为研究对象。另外选择同期间内接受健康检查的 30 例健康人群为对照组。 开展 D- 二聚体与纤维蛋白、凝血四项检测工作,同时开展肝功能检验,分析结果。结果 和对照组相比,代偿期肝硬化以及失代偿期肝硬化者的 D二聚体、APTT、TT、PT 指标更高,FIB 指标低;和代偿期肝硬化者相比,失代偿期患者 D- 二聚体、TT、APTT、PT 指标更高,FIB 指标低(P < 0.05);和 对照组相比,肝硬化者的 PA、CHE、ALB、TP 更低,TBA、ADA、DBil、TBil、GGT、ALP、AST、ALT 更高(P < 0.05)。和代偿期者相比,失代偿期者 PA、 CHE、ALB、TP 低,TBA、ADA、DBil、TBil、GGT、ALP、AST、ALT 高(P < 0.05)。PT 和 D- 二聚体、TT、APTT、ADA、TBA、DBil、TBil 呈正相关;和 FIB、 PA、CHE、ALB、GGT 呈负相关。APTT 和 D- 二聚体、TT、ADA、TBA、DBil、TBil 呈正相关,和 FIB、PA、GGT 为呈负相关。FIB 和 D- 二聚体、ADA、 TBA、DBil、TBil 呈负相关;和 PA 以及 GGT 呈正相关。TT 和 ADA、TBA、DBil、TBil 呈正相关;和 FIB、PA、GGT 呈负相关。结论 以 TT、APTT、PT 为 基础,联合应用 D- 二聚体以及 FIB 检测法诊断肝硬化有着相当重要的价值,这一点重点体现在失代偿期肝硬化疾病诊断中。在此同时分析患者的 肝脏功能,可精准诊断失代偿期肝硬化以及代偿期肝硬化。可实现全程病程监测,准确判断疾病预后、方便观察患者治疗效果。
伴高危因素的低级别脑胶质瘤患者辅助治疗策略的选择
伴高危因素的低级别脑胶质瘤患者辅助治疗策略的选择霍伟康;桂小娟【摘要】目的探讨在伴高危因素的低级别脑胶质瘤(LGGs)的辅助治疗中,放射治疗和化学药物治疗(放化疗)联合治疗的意义.方法 93例术后伴有高危因素的低级别胶质瘤LGGs患者作为研究对象,随机分为对照组(20例)、化疗组(28例)、放疗组(21例)及联合治疗组(24例).对照组不处理,化疗组采用替莫唑胺(TMZ)化疗,放疗组采用单纯放疗治疗,联合治疗组采用放化疗联合治疗,比较四组患者术后无进展生存期(PFS)时间.结果对照组、化疗组、放疗组、联合治疗组PFS分别为(36.250±1.430)、(48.652±3.305)、(46.588±2.257)、(56.100±2.862)个月,平均PFS为(47.539±1.571)个月,四组患者PFS比较,差异有统计学意义(P<0.05);化疗组、放疗组、联合治疗组的PFS和对照组比较,差异有统计学意义(P<0.05);联合治疗组PFS明显长于化疗组、放疗组,差异有统计学意义(P<0.05);放疗组PFS与化疗组比较,差异无统计学意义(P>0.05).结论放化疗联合比单独放疗或者化疗可进一步提高患者的PFS.【期刊名称】《中国实用医药》【年(卷),期】2018(013)017【总页数】3页(P6-8)【关键词】伴高危因素的低级别脑胶质瘤;放疗;化疗;放化疗联合治疗;无进展生存期【作者】霍伟康;桂小娟【作者单位】518100 南方医科大学深圳医院神经外科;518100 南方医科大学深圳医院神经外科【正文语种】中文在颅内原发恶性肿瘤中胶质瘤最为常见,在世界卫生组织(WHO)分类中将其分为四级,其中Ⅰ、Ⅱ级为低级别胶质瘤 (low-grade gliomas,L GGs),Ⅲ、Ⅳ级为高级别胶质瘤 (highgrade gliomas,HGGs)[1]。
客观结构化教学评估(OSTE)在教学查房能力训练中的应用
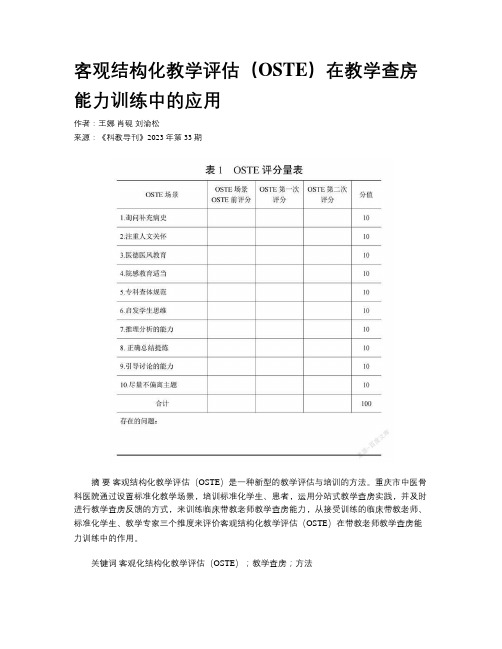
客观结构化教学评估(OSTE)在教学查房能力训练中的应用作者:王娜肖砚刘渝松来源:《科教导刊》2023年第33期摘要客观结构化教学评估(OSTE)是一种新型的教学评估与培训的方法。
重庆市中医骨科医院通过设置标准化教学场景,培训标准化学生、患者,运用分站式教学查房实践,并及时进行教学查房反馈的方式,来训练临床带教老师教学查房能力,从接受训练的临床带教老师、标准化学生、教学专家三个维度来评价客观结构化教学评估(OSTE)在带教老师教学查房能力训练中的作用。
关键词客观化结构化教学评估(OSTE);教学查房;方法中图分类号:G642 文献标识码:A DOI:10.16400/ki.kjdk.2023.33.016The Application of Objective Structured Teaching Evaluation (OSTE) in theTraining of Teaching Ward Rounds AbilityWANG Na, XIAO Yan, LIU Yusong(Science and Education Department, Chongqing Orthopedic Hospital of Traditional Chinese Medicine, Chongqing 400010)Abstract Objective Structured Teaching Evaluation (OSTE) is a new method of teaching evaluation and training. Chongqing Traditional Chinese Medicine Orthopedic Hospital trains standardized students and patients through setting up standardized teaching scenarios, utilizing a step-by-step teaching practice for ward rounds, and providing timely feedback on teaching rounds to train clinical teaching teachers in their ability to conduct ward rounds. This includes training clinical teaching teachers, standardized students, and more Teaching experts evaluate the role of Objective Structured Teaching Evaluation (OSTE) in the training of teaching rounds ability for mentors from three dimensions.Keywords Objective Structured Teaching Evaluation (OSTE); teaching ward rounds; method現代医院把“医疗、教学、科研”称为促进医院发展的“三驾马车”,2020年国务院办公厅发布了《关于加快医学教育创新发展的指导意见》,指出医学教育是卫生健康事业发展的重要基石,需要夯实高校附属医院医学人才培养主阵地,将医院教学工作提到更高的地位。
肩袖修补术后关节内注射倍他米松联合罗哌卡因的临床疗效对比
肩袖修补术后关节内注射倍他米松联合罗哌卡因的临床疗效对比曹青刚;赵建宁;包倪荣【摘要】目的现已明确肩部手术可导致中重度疼痛,但对最佳镇痛方法缺乏共识.文章评估关节镜下肩袖修补术后关节腔注射盐酸倍他米松联合罗哌卡因的临床效果.方法回顾性分析2017年3月至2017年10月于南京总医院行关节镜下肩袖修补的86例患者,并按不同治疗方案分为联合组(罗哌卡因75 mg+盐酸倍他米松2 mL)以及对照组(盐酸倍他米松4 mL),每组43例.通过视觉疼痛评分、患者满意度对患者术前及术后4、8、12、24、48 h疼痛进行评价.结果联合组术前及术后48 h VAS评分与对照组比较,差异无统计学意义(P>0.05);在术后4、8、12、24 h,联合组VAS评分明显低于对照组,差异有统计学意义(P<0.05);术后4、8、12、24 h,联合组患者满意度明显高于对照组(P<0.01);但在术后48 h,2组患者满意度差异无统计学意义(P>0.05).结论倍他米松联合罗哌卡因经关节腔注射较单纯倍他米松注射能显著减轻患者术后24 h内疼痛,提高患者对手术的满意度.【期刊名称】《医学研究生学报》【年(卷),期】2018(031)012【总页数】4页(P1289-1292)【关键词】倍他米松联合罗哌卡因;关节镜;肩袖损伤;疼痛【作者】曹青刚;赵建宁;包倪荣【作者单位】210002 南京,南京大学医学院附属金陵医院(南京军区南京总医院)骨科;210002 南京,南京大学医学院附属金陵医院(南京军区南京总医院)骨科;210002 南京,南京大学医学院附属金陵医院(南京军区南京总医院)骨科【正文语种】中文【中图分类】R6840 引言肩部手术与中重度疼痛相关[1]。
类固醇抗炎药能够缓解疼痛,促进早期康复和改善术后关节的活动范围;但皮质类固醇注射可引起皮肤萎缩、色素脱失,并增加局部感染发生率,甚至引起关节内软骨退化和肌腱断裂[2]。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Arch Gynecol Obstet (2010) 281:279–286DOI 10.1007/s00404-009-1098-9ORIGINAL ARTICLEProspective randomized trial of TVT and TOT as primary treatment for female stress urinary incontinence withor without pelvic organ prolapse in Southeast ChinaFengmei Wang · Yanfeng Song · Huijuan HuangReceived: 22 January 2009 / Accepted: 15 April 2009 / Published online: 30 April 2009© Springer-Verlag 2009AbstractObjective To compare the outcomes of tension- free vaginal tape (TVT) and transobturator tape (TOT) in the treatment of female stress urinary incontinence with or without con-comitant pelvic organ prolapse (POP).Methods One hundred and forty patients with SUI were randomly allocated to TVT (n=70) or TOT (n=70). The objective outcomes were assessed with a stress test, 1-h pad test. Subjective outcomes were assessed with UDI-6/(IIQ-7) questionnaires.Results The surgical outcomes revealed no signi W cant di V erence between TVT and TOT surgical route. Both the subjective and objective cure rates were 91.4% in the TOT group, while 90 and 92.8% in the TVT group, respectively. The results showed the association to pelvic X oor surgical techniques did not diminish a year later. TOT procedure has a shorter operative time for patients without concomi-tant surgery.Conclusion The e Y cacy and safety of TVT procedure were similar to that of TOT procedure for female stress uri-nary incontinence with or without concomitant POP. Keywords Tension-free vaginal tape · Transobturator tape · Stress urinary incontinence · Surgical outcomes IntroductionThe tension-free vaginal tape (TVT) procedure for the treatment of urodynamic stress urinary incontinence in women was reported in 1996 by Ulmsten et al. with an ini-tial 2-year cure rate of 84% [1]. This minimally invasive procedure has been shown to be a safe and e V ective treat-ment for GSI with good long-term results [2]. However, the TVT procedure has been related with various and poten-tially serious complications, such as urine retention, blad-der perforation, vaginal erosion, retropubic hematoma, or abscess and injuries at vessels, nerves, and intestine [3–8].In 2001, Delorme [9] described the transobturator (TOT) access ‘outside–inside’, aiming at the reduction of compli-cations by avoiding entering the space beyond the endopel-vic fascia. In this technique, the tape is inserted through the obturator foramens from outside to inside (in extenso from the thigh folds toward underneath the urethra). Delorme showed that TOT procedure is accompanied with high suc-cess rates and few perioperative complications.The aim of this study is to compare the TOT procedure with the TVT procedure in a randomized clinical trial set-ting and compare their e Y cacy in the treatment of SUI associated with or without pelvic organ prolapse (POP). Materials and methodsPatients, who urodynamically had proven stress urinary incontinence, were recruited for the study between Septem-ber 2003 and December 2007. Seventy patients in TVT group between 42 and 87years of age and 70 patients in TOT group between 37 and 75 were enrolled. Patients with urge incontinence or overactive bladder were excluded (Fig.1). Our study was a single-blind randomized trial andF. Wang · Y. Song (&) · H. HuangDepartment of Obstetrics and Gynecology,Fuzhou General Hospital, 350025 Fuzhou, Fujian, China e-mail: carnation1002@the patients were randomly allocated to either TVT or TOT group. All procedures were performed by Y. F. Song. The patients were not blinded to the operative procedure. Post-operative assessment was done by F.M. Wang, who did not take part in the operations. Y.F. Song was not involved in the follow-up.All patients gave an informed consent, and the study protocol was approved by the ethics committee of our hospital. Preoperative evaluation included clinical history, urinalysis, QoL assessment and clinical examination, uro-dynamic study with cystomanometry urethral pro W le if there was suspicion of sphincter insu Y ciency (severe from of stress incontinence with a Valsalva leak point pressure less than 100cm H2O) and measurement of postvoid residual urine by ultrasound examination. Urodynamic and prolapse quanti W cation methods, de W nitions and units conformed to the standards recommended by the International Conti-nence Society.A positive cough test was a necessary condition for per-forming an incontinence stress surgery. Intrinsic sphincter de W ciency was de W ned as urodynamic stress incontinence with maximum urethral closure pressure <20cm H2O and/ or valsalva leak point pressure <60cm H2O. Also, any pel-vic X oor defect was evaluated according to the POP quanti-W cation (POPQ) staging. In all prolapse cases, a cough test was made after bladder W lling to 200ml reducing prolapse for the diagnosis of occult stress incontinence.The TVT procedures were performed in accordance with the technique by Ulmsten et al. [1]. The patient was positioned in the dorsal lithotomy position. The sites of the suprapubic stab incisions were located along the superior rim of the pubic bone, two W ngerbreadths lateral to themidline, each 0.5–1cm in length. The bladder was drained with a Foley catheter and a 1.5 midline incision was made at the mid-urethra. Metzenbaum scissors were used to dissect under the vaginal epithelium laterally to create a periurethral spaces to the inferior pubic ramus. Once the periurethral spaces were ready, a special prolene tape (Ethi-con, Sommerville, NJ, USA) covered by a plastic sheath was introduced using a two-component needle instrument. The tip of this needle W rst perforates the urogenital dia-phragm and is then moved upwards within the retropubic space (keeping the tip close to the pubic bone). After perfo-ration of the rectus sheath, a small 1-cm incision is made over the needle point in the skin just above the superior rim of the pubic bone. This procedure is then repeated on the other side with the other needle, ensuring that the skin inci-sions are <5cm apart. At this time, cystoscopy was per-formed because of the risk of bladder perforation. The tape is, therefore, placed in a U-form shape around the mid-ure-thra. During this step, a Metzenbaum scissors is placed between the urethra and the tape to prevent an increase in the tension of the tape. The vaginal incision was closed with absorbable suture. The remaining sling mesh is cut at the abdominal skin. The Foley catheter is then replaced in the bladder.The TOT procedures were performed in accordance with the technique by Delorme et al. [9]. The anterior vaginal wall is suspended with two Allis clamps on either side of the midline, 0.5cm proximally to the urethral meatus. A vertical midline incision of the vaginal wall is started at this level and is continued proximally over a 1.5cm distance. Both vaginal mucosal and submucosal tissues are incised. Using scissors, dissection of the para-urethral space is made bilaterally, toward the ischiopubic rami. The lateral margin of the ischiopubic is identi W ed and the index W nger placed in the latero-vaginal fornix and thumb placed in front of the obturator foramen. The external needle entry point is made in the genitofemoral fold by a shallow cutaneous stab incision slightly above a horizontal line passing through the clitoral hood, just under the adductor longus tendon insertion. The semicir-cular, corkscrew-shaped needle of the device is intro-duced through the stab incision, held in the same hand as the side on which the surgeon is working. Once the needle passes through the obturator membrane, it reaches the W ngertip inserted in the para-urethral space. It is then passed around the ischiopubic ramus, while the protecting W nger remains in contact with the needle until it is visual-ized at the suburethral incision. Once this procedure has been completed, the vagina is evaluated for any unwanted perforations. The tape is then connected to the needle tip. Next, with a rotating wrist motion, the tape is guided through the tunnel and exist the skin incision. The same procedure is carried out on the contralateral side. Tension-free adjustment is made to the tape under the mid-urethra. Vaginal closures are made with interrupted absorbable sutures.The urinary catheter was removed 12–24h after surgery. In the patients, who also underwent various other vaginal reconstructive procedure, urinary catheter was removed 24–72h after surgery. The two procedures were performed under local anesthesia supplemented by an intravenous sed-ative, unless the patients were also undergoing vaginal hys-terectomy or pelvic X oor repair. In these cases, they were given spinal anesthesia.In TVT group, 40 patients had isolated urinary inconti-nence, 30 patients had concomitant uterine or vaginal vault prolapse. Patients, who had uterine prolapse, underwent transvaginal hysterectomy, anterior–posterior colporrhaphy (APC) and posterior intravaginal slingplasty reconstructive surgeries, and TVT procedure. The patients who had vagi-nal vault prolapse underwent APC and TVT procedure. Of the 70 patients in TOT group, 48 had isolated urinary incontinence, 22 had concomitant uterine or vaginal vault prolapse. Patients who had uterine prolapse underwent transvaginal hysterectomy, APC and/or posterior IVS reconstructive surgeries and TOT procedure. The patients who had vaginal vault prolapse underwent APC and TOT procedure.Intraoperative and postoperative complications were evaluated. The QoL assessment was carried out preopera-tively and 1year from surgery with the use of the Urogeni-tal Distress Inventory Short Form (UDI-6) and the Incontinence Impact Questionnaire Short Form (IIQ-7) questionnaires. The short form of IIQ-7 and UDI-6 vali-dated by Uebersax et al. [10] consists of seven and six questions, respectively. These questionnaires had been translated into Chinese and validated for female population in China [11]. Subjective outcomes were assessed by the two questionnaires. The cough test, 1-h pad test and urody-namic examination were performed if the patient referred voiding dysfunction. The operations were all conducted by the same gynecologist. A voiding trial as described by Kle-eman et al. [12] was performed on all patients before dis-charge. If patients failed their voiding trial, they were taught to perform intermittent self-catheterization with a Foley catheter. The length of hospital stay was de W ned as number of days between the completion of surgery and hos-pital discharge.Outcome measures were categorized as follows: objec-tive cure was de W ned as no stress incontinence during cough stress test (300cm X uid in the bladder, cough force-fully, visible leakage means a positive test), a 1-h pad test (1-h pad test) of <2g. Patients were considered ‘improved’if they did not leak on the cough stress test, but may have had occasional urine leakage during stress; this occasion leakage did not in X uence their daily activities or requirefurther treatment. Besides, urine weight by the 1-h pad test was decreased by more than 50%. All other cases were reported as objective failures. The patient’s subjective assessment of the outcome of incontinence was classi W ed as cured (UDI-6 and IIQ-7 postoperative <10), improved (UDI-6 and IIQ-7 if postoperative>preoperative) and worsened (UDI-6 and IIQ-7 if postoperative<preoperative). Statistical analysisAll data were recorded using standard forms. We used SPSS 11.5. A P value of less than 0.05 was considered signi W cant.ResultsAll of patients were followed up at the end of 12 months. Thus, we obtained the preoperative and postoperative data from 140 patients. There were no signi W cant di V erences in the preoperative characteristics of patients who under-went TVT or TOT procedure (Table1). We also found that there was no major intraoperative complication in the both TVT and TOT group (Table2). However, the dura-tion of the operation was signi W cantly shorter in the TOT group (12min) compared with the TVT group (21min) for patients without concomitant POP (P=0.012). No perioperative injury to the urethra, nerves, vessel or bowel happened in each group. But a bladder perforation occurred in three patients in TVT group, and one of them had been operated on twice before for urinary inconti-nence. In TOT group, one patient had bladder perforation. With cystoscopy, we withdrew and re-implanted the tape which did not a V ect the e Y ciency. Until the 12-month fol-low-up, we did not W nd any declined e Y ciency of this patient. About 3 patients (4.2%) in the TVT group and 8 (11.4%) in the TOT group complained of postoperative inner thigh or buttock discomfort, but all of these transient symptoms of discomfort disappeared in all patients at 1-month follow-up. After surgery, 8 patients (11.4%) in the TVT group and 6 (8.57%) in the TOT group had short-term voiding di Y culty. With a longer catheter time, all patients voided well following removal of the catheter. Three patients had vaginal tape erosion: one in the TVT group at 1month’s follow-up and two in the TOT group at 3months’ follow-up.Surgical results were similar in both groups. Concomi-tant pelvic reconstructive procedure had no e V ect on the surgical results (Tables3, 4, 5, 6). At the 1-year follow-up, the objective cure rates were 91.4% in the TOT group and 92.8% in the TVT group. In comparison with the complete cure rate, there were no signi W cant di V erences between the TOT group and the TVT group. The objective cure rates for patients with isolated SUI were 95% in the TVT group and 93.75% in the TOT group. For patients with concomitant POP, the cure rates were 90% in the TVT group and 86.36% in the TOT group (Tables3, 4). On subjective Table1Patient characteristics, preoperative clinical, quality of life, and urodynamic parametersValues are given as mean§SDP value denotes the comparison between two groups using two sample t test, chi-squareQmax maximum X ow rate, ALPP abdominal leak point pressure, SUI stress urinary incontinence, UDI-6 Urogenital Distress Inventory Short Form, IIQ-7 Incontinence Impact Questionnaire Short Forma Student’s t testb Chi-square testTVT (n=70)TOT (n=70)PAge (years)60§10.858§11.60.595a Isolated SUI58§11.259§13.50.606a Concomitant pelvicorgan prolapse62§12.361§12.90.612aBody mass index (kg/m2)24§2.424.6§2.60.332a Isolated SUI23§2.722.9§3.10.295a Concomitant pelvicorgan prolapse25§3.123.1§2.50.301aHormone replacementtherapy16 (22.86%)14 (20%)0.832a Previous surgery for SUI 5 (7.14%) 3 (4.29%)0.643b Duration of SUI (years) 4.7§4.6 4.3§3.90.496a Isolated SUI 5.1§4.2 4.7§4.10.398a Concomitant pelvicorgan prolapse3.7§3.1 3.9§3.10.402aPostvoid residualurine (ml)17.9§27.923.7§23.70.967a Isolated SUI18.9§24.321.3§20.10.879a Concomitant pelvicorgan prolapse17.2§25.223.5§24.20.921a Qmax (ml/s)27.6§13.829.8§11.30.413a Isolated SUI30.8§14.932.8§15.30.362a Concomitant pelvicorgan prolapse24.3§11.224.5§11.10.377a ALPP (cm H2O)92.3§41.881.2§43.60.104a Isolated SUI91.4§42.492.4§41.80.314a Concomitant pelvicorgan prolapse89.3§39.282.5§40.10.234a UDI-649§2149§190.699a Isolated SUI52§1748§200.605a Concomitant pelvicorgan prolapse45§2445§210.586a IIQ-740§2840§250.712a Isolated SUI45§2541§260.597a Concomitant pelvicorgan prolapse35§3038§310.801aassessment, the cure rate of TVT group and TOT group was 90 and 91.4%, respectively.The scores of UDI-6 and IIQ-7 were signi W cantly less than the preoperative scores on each scale. These statistical di V erences between pre- and postsurgery with the QoL test were independent of the association of pelvic X oor repair surgery.DiscussionBecause of the pelvic structure, stress incontinence and POP often occur together because of the pelvic structure. POP can a V ect the urethra by pulling and open the posterior urethral wall, thereby causing urethral sphincter inconti-nence by mechanically obstructing the urethra or by dissi-pating the e V ects of abdominal pressure on the urethra. This might be the main cause of the stress incontinence that occurs after correcting POP [13, 14]. Since the introduction in 1996 [1], TVT procedure had become a popular treat-ment for urinary incontinence. With some complications including bowel and major blood vessel injuries, bladder and urethral perforation, and postoperative voiding di Y cul-ties or urgencies, a new surgical technique of mid-urethral prosthetic suspension called the TOT tape was introduced in 2001 [3]. There were large occidental studies reporting that TOT was safer and more e Y cient for the treatment of stress urinary incontinence than TVT, mainly with fewer complications. Thus, it was hypothesized that there would be no di V erence in the outcome between TVT and TOTTable2Intraoperative compli-cations, operation time, catheter time, and length of hospitaliza-tion and postoperative complica-tionsTVT (n=70)TOT (n=70)P Mean operation timein min (range)35.5 (18–80)29.8 (10–80)0.082aIsolated SUI21 (18–30)12 (10–21)0.012a Concomitant pelvicorgan prolapse62 (35–80)65 (30–75)0.324a Cystoscopy performed70/703/70Bladder perforation 3 (4.3%) 1 (1.4%)0.310b Nerves or vessel lesionsor hemorrhage00Mean catheter timein hours (range)34 (12–72)32 (12–72)0.356a Isolated SUI18 (12–24)16 (12–24)0.567a Concomitant pelvicorgan prolapse28 (24–72)30 (24–72)0.348aMean length of hospitalizationin days (range)3.6 (1–6) 3.2 (1–5)0.708a Isolated SUI 1.4 (1–3) 1.5 (1–3)0.712a Concomitant pelvicorgan prolapse4.3 (3–6) 3.9 (3–5)0.612a Infection00Tape division01Postoperative residualvolume (ml)37.3§50.348.4§61.10.643a Isolated SUI33.3§46.142.4§55.60.419a Concomitant pelvicorgan prolapse38.2§48.748.3§58.40.732a Postoperative complicationsPain 3 (4.2%)8 (11.4%)0.116b Short-term voiding di Y culty8 (11.4%) 6 (8.57%)0.317b Frequency430.698 Urgency31 1.320 Leakage of urine whenstraining120.559 Rejection of tape120.559 Overactive bladder140.172P value denotes the comparison between two groups using two-sample t test, chi-squarea Student’s t testb Chi-square testapproach where the safety and e Y cacy were concerned, if we made the optimal prophylactic measures in our country.Meanwhile, we were interested in whether the concomitant surgical procedures would a V ect the di V erences in safety and e Y cacy between TOT procedure and TVT procedure.Therefore, a prospective study was performed to evaluate the postoperative continence situation of those USI women with POP, who underwent anti-incontinence surgery com-bined with reconstructive surgery.In our study, average time of discharge and catheteriza-tion were comparable to the data reported previously [15].Bladder perforation was the only perioperative complica-tion that happened in both TVT group and TOT group. In the TVT procedure, it may occur due to a defect in the W xa-tion of the endopelvic fascia at the level of the arcus tendin-eus of the levator ani muscle. This may give room to the lateral parts of the bladder base to sink into this paravaginal space. The instrument can perforate the bladder base at that point. Pulling back the instrument or removing the tape and transurethral catheter for 24h is su Y cient. In di Y cult cases with known paravaginal defect, we strongly suggest to per-form a cystoscopy. In TOT group, there was only one case of bladder perforation, which hinted us that the periopera-tive cystoscopy might be imperative (particularly in patients who had undergone previous pelvic surgery),although many studies thought that there was no essential-ity of the perioperative cystoscopy as the procedure path-way was more far away from the bladder in the TOT surgery. Other perioperative complications, such as hema-toma and hemorrhea and infection were not found in each group. As the procedure route was closer relative to the obturator canal, a higher frequency of thigh pain was found in TOT group than that in TVT group. But these pains often would not exceed over 1month.A lthough TVT and TOT procedure are commonly applied to treatment female SUI, tape rejection is also a well-reported complication. The vaginal tape erosion rates reported in the literature were 2.2% in the TVT and 3.6% inTable 3Pad-test results at 12months follow-upaP =0.852 the number of patients with isolated SUI whose 1-h pad test of less than 2g in the TVT group vs that in the TOT groupbP =0.400 the number of patients with Concomitant pelvic organ pro-lapse whose 1-h pad test of less than 2g in the TVT group vs that in the TOT group1-h pad test <2g >2gTVTTOT TVT TOT Isolated SUI 38/40a 46/482/402/48Concomitant pelvic organ prolapse28/30b19/222/303/22Table 4Cough test results at 12months follow-upaP =0.801 the number of patients with isolated SUI whose cough test being negative in the TVT group versus that in the TOT group bP =0.685 the number of patients with Concomitant pelvic organ pro-lapse whose cough test being negative in the TVT group versus that in the TOT groupThe cough test Negative PositiveTVTTOT TVT TOT Isolated SUI 38/40a 45/482/403/48Concomitant pelvic organ prolapse27/30b19/223/303/22Table 5Preoperative and 1-year follow-up di V erences in the UDI-6scoresaP <0.05 preoperative versus 1-year follow-up in the TVT group (P =0.014)bP >0.05 preoperative in the TVT group vs preoperative in the TOT group cP >0.05 1-year follow-up in the TVT group versus 1-year follow-up in the TOT group dP <0.05 preoperative versus 1-year follow-up in the TOT group (P =0.008)UDI-6Preoperative 1-year follow-up TVT TOT TVT TOT Total 49§21a 46§20b 15§15c 14§17d Isolated SUI 52§1850§1718§1219§12Concomitant pelvic organ prolapse45§2545§2116§1414§15Table 6Preoperative and 1-year follow-up di V erences in the IIQ-7scoresaP <0.05 preoperative versus 1-year follow-up in the TVT group (P =0.020)bP >0.05 preoperative in the TVT group versus preoperative in the TOT group cP >0.05 1-year follow-up in the TVT group versus 1-year follow-up in the TOT group dP <0.05 preoperative versus 1-year follow-up in the TOT group (P =0.012)UDI-6Preoperative 1-year follow-up TVTTOT TVT TOT Total 40§21a 42§20b 13§12c 10§12d Isolated SUI 45§2341§318§129§11Concomitant pelvic organ prolapse40§2745§2112§1411§15the TOT procedures [14]. In our study, all three patients with tape erosion presented with vaginal tape protrusion. Since all of the protruding vaginal tapes seen in our study were <1cm long and no signs of infection were present, we adopted a more conservative surgical approach to trim o V the extruded portion of the tape, and closed the cleaned vaginal wound over it without tension. All patients recov-ered well and were symptom-free without any evidence of tape rejection recurrence at 12month’s of follow-up.Objective cure rates of stress incontinence surgery are determined by 1-h pad test and cough stress test. As showed in Tables3, 4, there was no signi W cant di V erence in the cure rate between the TVT group and the TOT group. DeTayrac et al. [15] had reported, in a randomized study, a 1-year cure rate of 83.9% with the TVT versus 90.0% with the TOT. Fisher et al. [16] reported a cure rate of 81% with TOT procedure compared with 76% with TVT. In our study, 92.8% with the TVT procedure and 91.4% with the TOT procedure were reported, which were higher than other reports. All these assessments, however, merely re X-ect the continence state at a single moment in time. The patient’s concept of cure was shown to have important in the rate of the outcome of incontinence surgery [17]. With a QoL analysis, we can provide di V erent information over a longer period of time and show the outcome of inconti-nence surgery more sensitively [18]. We chose to assess patients subjectively by asking them to express their satis-faction level via the UDI-6 and the IIQ-7 questionnaires because they are easy to administer and have been appro-priately validated in the Chinese language [11]. In our study, 90% with the TVT procedure and 91.4% with the TOT procedure were reported.We have also attempted in this report to determine if there could be any di V erence in outcome when a pelvic X oor reconstructive surgery was added to a TVT procedure or a TOT procedure. No signi W cant di V erences were found in the patients undergoing TVT procedure or TOT proce-dure. For patients with isolated SUI, an objective cure rate of 95% with the TVT group and 93.75% with the TOT group were reported. The objective cure rates of patients with associated pelvic reconstructive surgery were 90 and 86.36%, respectively. Neither UDI-6 nor IIQ-7 showed any di V erence between groups with and without pelvic repair. There were also no di V erences in the UDI-6 and IIQ-7 pre-operative and postoperative scores in women with pelvic X oor repair or women with just the TOT/TVT procedure.Until now, many reports comparing the e Y cacy and safety of TOT procedure to that of TVT procedure were published. But there are no published trials about the e Y cacy of TVT combined with prolapse repair surgery compared to that of TOT procedure in the same circum-stances. We W rst report our experience on the outcomes of tension-free vaginal (TVT) and TOT suburethral tape in the treatment of female stress urinary incontinence with or without concomitant POP. We found that the e Y cacy and safety of TVT procedure was similar to that of TOT proce-dure for female stress urinary incontinence with or without concomitant POP.Con X ict of interest statement We declare that we have no con X ict of interest.References1.Ulmsten U, Falconer C, Johnson P, Jomaa M, Lanner L, NilssonCG, Olsson I (1998) A multicenter study of tension-free vaginal tape (TVT) for surgical treatment of stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 9(4):210–213. doi:10.1007/ BF019016062.Bergman A, Koonings PP, Ballard CA (1998) Predicting postop-erative urinary incontinence development in women undergoing operation for genitourinary prolapse. Am J Obstet Gynecol 158(5):1171–11753.Rezapour M, Ulmsten U (2001) Tension-free vaginal tape (TVT)in women with recurrent stress urinary incontinence: a long-term follow up. Int Urogynecol J Pelvic Floor Dysfunct 12(Suppl 2):9–11. doi:10.1007/s0019201700044.Kuuva N, Nilsson CG (2002) A nationwide analysis of complica-tions associated with the tension-free vaginal tape (TVT) procedure.Acta Obstet Gynecol Scand 81:72–77. doi:10.1034/j.1600-0412.2002.810113.x5.Kobashi KC, Govier FE (2003) Management of vaginal erosion ofpolypropylene mesh slings. J Urol 269:2242–2243. doi:10.1097/01.ju.0000060119.43064.f66.Fourie T, Cohen PL (2003) Delayed bowel erosion by tension-freevaginal tape (TVT). Int Urogynecol J Pelvic Floor Dysfunct 14:362–364. doi:10.1007/s00192-003-1068-x7.Leboeuf L, Mendez LE, Gousse AE (2004) Small bowel obstruc-tion associated with tension-free vaginal tape. Urology 63:1182–1184. doi:10.1016/j.urology.2004.02.0148.Sergent F, Sebban A, Verspyck E, Sentilhes L, Lemoine JP,Marpeau L (2003) Per-and postoperative complications of TVT (tension-free vaginal tape). Prog Urol 13:648–6559.Delorme E (2001) Trans-obturator urethral suspension: miniinva-sive invasive procedure in the treatment of stress urinary inconti-nence in women. Prog Urol 11(6):1306–131310.Uebersax JS, Wyman JF, Shumaker SA, McClish DK, Fantl JA(1995) Short forms to assess life quality and symptom distress for urinary incontinence in women: the incontinence impact question-naire and the urogenital distress inventory. Continence Program for Women Research Group. Neurourol Urodyn 14:131–139.doi:10.1002/nau.193014020611.Zhang W, Song Y, He X (2005) Prevalence and risk of lower uri-nary tract symptoms in Fuzhou Chinese women. Eur Urol 48:309–313. doi:10.1016/j.eururo.2005.03.00312.Kleeman S, Goldwasser S, Vassallo B (2002) Predicting voidinge Y ciency after surgery for incontinence and prolapse. Am J ObstetGynecol 187(1):49–52. doi:10.1067/mob.2002.12484113.Bump RC, Fantl JA, Hurt WG (1998) The mechanism of urinarycontinence in women with severe uterovaginal prolapse: results of barrier studies. Obstet Gynecol 72(3 Pt 1):291–295tte PM, Foon R, Toozs-Hobson P (2007) Transobturator and ret-ropubic tape procedures in stress urinary incontinence: a system-atic review and meta-analysis of e V ectiveness and complications.Br J Obstet Gynecol 114(10):522–531. doi:10.1111/j.1471-0528.2007.01268.x。