盐酸莫西沙星氯化钠注射液说明书
盐酸莫西沙星氯化钠注射液
盐酸莫西沙星氯化钠注射液【药品名称】通用名称:盐酸莫西沙星氯化钠注射液英文名称:Moxifloxacin Hydrochloride and Sodium Chloride Injection【成份】本品主要成份为盐酸莫西沙星,化学名为:1-环丙基-7-[(s,s)-2,8-重氮-二环[4.3.0]壬-8-基]-6-氟-8-甲氧-1,4-二氢-4-氧-3-11奎啉羧酸盐酸盐。
【适应症】成人(≥18岁)上呼吸道和下呼吸道感染,如:急性窦炎、慢性支气管炎急性发作、社区获得性肺炎;以及皮肤和软组织感染。
【用法用量】400 mg qd,口服或静滴90分钟。
疗程:慢性支气管炎急性发作- 5天;社区获得性肺炎:序贯给药(静脉给药后继续口服用药)总疗程为7-14天;急性鼻窦炎- 7天;皮肤和软组织感染- 7天。
最多14天。
【不良反应】在莫西沙星的临床试验中,绝大多数的不良反应为轻中度(约90%),由于不良反应导致停用莫西沙星治疗的病人为36%,序贯治疗(静脉给药后继续口服用药)为5.7%。
根据莫西沙星的临床试验总结出的常见不良反应列表如下:发生率≥1%<10%全身症状:腹痛、头痛、注射部位反应(如水肿/过敏/炎症/疼痛)心血管系统:合并低血钾症患者QT间期延长消化系统:恶心、腹泻、呕吐、消化不良、肝功能化验异常特殊感官:味觉倒错神经系统:头晕发生率≥0.1%<1%全身症状:乏力、念珠菌病、疼痛、不适、胸痛心血管系统:心动过速、高血压、心悸、QT间期延长、静脉炎(注射部位)消化系统:口干、恶心和呕吐、腹胀、便秘、口腔念珠菌病、食欲下降、口腔炎、胃肠功能失调、舌炎、γGT(γ谷氨酰转肽酶)增高血液和淋巴系统:白细胞减少、凝血酶原减少/国际标准化比值增高、嗜酸细胞增多、血小板增多症代谢和营养:淀粉酶增加骨骼肌肉系统:关节痛、肌肉痛神经系统失眠、眩晕、神经质、嗜睡、焦虑、震颤、感觉异常呼吸系统:呼吸困难皮肤和附件:皮疹、瘙痒、多汗泌尿生殖系统:阴道念珠菌病、阴道炎发生率≥0.01%<0.1%全身症状:骨盆疼、面部浮肿、背疼、实验室检验异常、过敏反应、腿疼心血管系统:低血压、血管扩张、外周性水肿消化系统:胃炎、舌变色、吞咽困难、黄疸(主要为胆汁淤积性)、腹泻(难辨梭菌)血液和淋巴系统:凝血活酶减少、凝血酶原增加/国际标准化比值降低、血小板减少、贫血代谢和营养:高血糖、高血脂、高尿酸血症、LDH(乳酸脱氢酶)增高(与肝功能检查异常有关)骨骼肌肉:关节炎、肌腱异常神经系统:幻觉、人格解体、紧张、动作失调、激动不安、健忘症、失语症、情绪不稳定、睡眠障碍、语言障碍、思维异常、感觉减退、梦异常、惊厥、精神错乱、忧郁症呼吸系统:哮喘皮肤和附件:皮疹(斑丘疹、紫癜、脓泡)、荨麻疹特殊感官:耳鸣、视觉异常、味觉丧失、嗅觉倒错(包括嗅觉倒错,嗅觉减低及嗅觉丧失)、弱视泌尿生殖系统:肾功能异常(肌酐或尿素升高)上市后报道的不良反应:发生率≥0.01%<0.1%心血管系统:晕厥发生率<0.01%过敏性:过敏反应、过敏性休克(可危及生命)、血管性水肿(包括喉头水肿;潜在生命危险)消化系统:伪膜性结肠炎(在极少数病例伴有危及生命的并发症),肝炎(主要为胆汁淤积性)肌肉骨胳系统:肌腱断裂皮肤和附件:斯蒂文斯-约翰逊综合征(Stevens-JohnsonSyndrome)神经系统:精神病反应心血管系统:报道在极少数病例尤其是在有严重的潜在性致心律失常条件的病人出现,包括尖端扭转型室速的室性快速性心律失常和心脏停搏。
2023年关于“盐酸莫西沙星注射液”解析

注意事项
1、致残和潜在的不可逆转的严重不良反应,包括肌腱炎和肌腱断裂、周围神经病变和中枢神经系统的影响:使用氟喹诺酮类 药物(包括盐酸莫西沙星),已有报告在同一患者的身体不同器官系统同时发生致残和潜在的不可逆转的严重不良反应,通 常包括:肌腱炎,肌腱断裂,关节痛,肌痛,周围神经病变和中枢神经系统反应(幻觉,焦虑,抑郁,失眠,严重头痛和错 乱)。这些不良反应可发生在使用盐酸莫西沙星后数小时至数周。任何年龄段的患者,之前没有相关风险因素,均有报告发 生这些不良反应。
由于缺乏这些患者的用药经验,本品应避免用于下列患者:
(1)已知QT间期延长;
(2)室性心律失常,包括尖端扭转型,因为QT间期延长可能导致发生这些状况的风险增加;
(3)持续的心律失常状况,如具有临床显著性的心动过缓和急性心肌缺血;
(4)未治疗的低钾血症或低镁血症;
(5)使用抗心律失常IA类药物(例如,奎尼丁、普鲁卡因胺)或III类药物(例如,胺碘酮、索他洛尔);
用法用量
盐酸莫西沙星氯化钠注射液: 盐酸莫西沙星氯化钠注射液用于感染性疾病的治疗,通用的用法用量如下所示,但必须结合疾病严重程度由临床医生最终确定。 4、给药说明: (1)给药前应检查本品是否有不溶颗粒或变色。应使用澄明,无不溶颗粒的本品。穿刺使用前应对本品进行目视检查,不得使用变色、存在颗粒物质或容器存在破损的 产品。 (2)盐酸莫西沙星氯化钠注射液为静脉注射剂,只能用于静脉滴注,不能用于动脉内、肌内、鞘内注射,不能腹膜内或皮下给药。 (3)由于本品与其他注射液的相容性数据较少,本品中不得加入溶媒或其他药物,也不得使用同根静脉输液管同时输注本品,溶媒或其他药物。如使用同根静脉输液管 或Y型管来连续滴注其他药物,或采用背负式输液,在滴注本品之前和之后,应使用和本品和其他滴注药物相容的注射液冲洗该管路。 (4)当开具盐酸莫西沙星来治疗某种细菌感染时,应告知患者:尽管在疗程早期病情通常会好转,但仍应遵医嘱使用药物。跳过剂量或不完成整个疗程可能会降低紧急 治疗的有效性,增加细菌耐药性形成的可能性,未来将不能使用盐酸莫西沙星或其他抗菌药进行治疗。 5、药物相容性:比例在1:10至10:1之间时,本品与下列静脉注射液相容: (1)0.9%氯化钠注射液,无菌注射用水。 (2)1M氯化钠注射液,10%葡萄糖注射液。 (3)5%葡萄糖注射液,乳酸林格注射液 6、种族差异:对高加索人、日本人、黑人及其他种族人群进行了可能的种族间差别试验,未发现临床相关的药代动力学差别。因此,不同种族间不必调整药物剂量。
氯化钠注射液说明书
【药品名称】通用名称:氯化钠注射液英文名称:Sodium Chloride Injection汉语拼音:Lühuana Zhusheye【成份】本品的主要成份及化学名称为氯化钠,每1000ml中含氯化钠9g。
分子式:NaCl分子量:Cas No:7647-14-5【性状】本品为无色的澄明液体;味微咸。
【适应症】各种原因所致的失水,包括低渗性、等渗性和高渗性失水;高渗性非酮症糖尿病昏迷,应用等渗或低渗氯化钠可纠正失水和高渗状态;低氯性代谢性碱中毒;外用生理盐水冲洗眼部、洗涤伤口等;还用于产科的水囊引产。
【规格】100ml:0.9g;250ml:2.25g; 500ml:4.5g【用法用量】1.高渗性失水高渗性失水时患者脑细胞和脑脊液渗透浓度升高,若治疗使血浆和细胞外液钠浓度和渗透浓度过快下降,可致脑水肿。
故一般认为,在治疗开始的48 小时内,血浆钠浓度每小时下降不超过L。
若患者存在休克,应先予氯化钠注射液,并酌情补充胶体,待休克纠正,血钠>155mmol/L,血浆渗透浓度>350mOsm/L,可予%低渗氯化钠注射液。
待血浆渗透浓度<330mOsm/L,改用%氯化钠注射液。
补液总量根据下列公式计算,作为参考:[血钠浓度(mmol/L)-142]所需补液量(L)= 血钠浓度(mmol/L)××体重(Kg)一般第一日补给半量,余量在以后2~3 日内补给,并根据心肺肾功能酌情调节。
2.等渗性失水原则给予等渗溶液,如%氯化钠注射液或复方氯化钠注射液,但上述溶液氯浓度明显高于血浆,单独大量使用可致高氯血症,故可将%氯化钠注射液和%碳酸氢钠或%(1/6M)乳酸钠以7:3 的比例配制后补给。
后者氯浓度为107mmol/L,并可纠正代谢性酸中毒。
补给量可按体重或红细胞压积计算,作为参考。
(1)按体重计算:补液量(L)=(体重下降(kg)×142)/154;(2)按红细胞压积计算:补液量(L)=(实际红细胞压积-正常红细胞压积×体重(kg)×)/正常红细胞压积。
来盐酸莫西沙星氯化钠注射液的配伍禁忌
来盐酸莫西沙星氯化钠注射液的配伍禁忌盐酸莫西沙星氯化钠注射液(商品名:拜复乐),黄色澄明液体,规格250ml,是第4代新型8-甲氧基氟喹诺酮类抗菌药物,具有抗菌谱广、抗菌力强、体内分布广、体内药物浓度高、半衰期长、疗效好、不良反应小、与其他抗菌药物无交叉耐药性、几乎无光敏反应等优点。
临床上主要应用于治疗呼吸系统、泌尿生殖系统、皮肤系统等感染性疾病。
在近几年的临床用药过程中,笔者发现盐酸莫西沙星氯化钠注射液与多种药物之间存在配伍禁忌,经混合后,均出现白色浑浊现象或者有晶体析出。
为保证临床用药安全,本文查阅了国内相关文献,对其配伍禁忌进行综述,以供临床合理配伍药品参考,保证患者用药安全。
1 抗感染类药物1.1头孢菌素类与头孢哌酮钠他唑巴坦钠存在配伍禁忌。
有研究报道,头孢哌酮钠他唑巴坦钠组滴注完予更换盐酸莫西沙星氯化钠注射剂组液体5s后,茂菲氏滴管内出现白色浑浊,经摇晃不消失[1]。
1.2青霉素类与氟氯西林钠存在配伍禁忌。
有研究报道,将盐酸莫西沙星氯化钠注射剂与0.9%氯化钠注射液100ml+注射用氟氯西林钠联合应用,盐酸莫西沙星氯化钠注射剂更换注射用氟氯西林钠组液体时,输液管内立即出现乳白色浑浊及絮状物;将两种溶液直接混合,发现混合液立即变为乳白色浑浊液,轻摇晃后不溶解,放置30min后观察乳白色浑浊液未恢复澄清[2]。
1.3利福霉素与注射用利福霉素钠存在配伍禁忌。
有研究报道,将注射用利福霉素钠1.0g溶解于5%葡萄糖250ml,抽取2ml注射用利福霉素钠溶液,再抽取2ml 盐酸莫西沙星氯化钠注射剂,将两者混合,或更换两者顺序抽取,混合液均立即出现红色絮状混浊物,剧烈振荡后无变化[3]。
1.4米卡芬净钠与注射用米卡芬净钠存在配伍禁忌。
有研究报道,盐酸莫西沙星氯化钠注射剂输注完毕更换米卡芬净钠时,输液器内溶液呈现乳黄色混浊并有絮状物[4]。
1.5夫西地酸钠与注射用夫西地酸钠存在配伍禁忌。
有研究报道,用20ml 注射器分别抽取夫西地酸钠和莫西沙星注射液各5ml。
拜复乐(莫西沙星)
【药品名称】通用名称:拜复乐商品名称:拜复乐【英文名称】汉语拼音:baifule【成份】盐酸莫西沙星氯化钠【性状】本品为黄色的澄明液体【作用类别】【适应症】成人(大于18岁)上呼吸道和下呼吸道感染,如,急性窦炎,慢性支气管炎急性发作,社区获得性肺炎,及皮肤及软组织感染。
【规格】250ml:0.4g × 1【用法用量】推荐剂量一次400mg,一日一次,慢性支气管炎急性发作:5天。
社区获得性肺炎:序贯给药推荐总疗程为7—14天。
急性窦炎:7天。
治疗皮肤及软组织感染的推荐为7天。
【不良反应】绝大多数不良反应为轻中度胃肠道反应,中枢神精系统不良反应,皮肤过敏等【禁忌】已知对该注射液的任何成份或其他喹诺酮类过敏者。
禁用于儿童,青少年,孕妇及哺乳期妇女。
【药物毒理】莫西沙星是具有广谱活性和杀菌作用的8—甲氧基氟喹诺酮类药物。
莫西沙星在体外显示对革兰阳性菌,革兰阴性菌,厌氧菌,抗酸菌和非典型微生物和支原体,衣原体和军团菌具有广谱抗菌活性。
杀菌作用机制为干扰拓扑异构酶Ⅱ和Ⅳ。
拓朴异构酶是控制DNA拓朴和在DNA复制,修复和转录中关键的酶。
【贮藏】干燥条件下贮藏。
【包装】瓶批准文号:国药准字J20040068生产企业:德国拜耳(拜耳医药保健分装)处方类型:本品为处方药!基本药理本品是广谱和具有抗菌活性的8-甲氧基氟喹诺酮类抗菌药。
抗菌机制为干扰II、IV拓扑异构酶。
本品是具有浓度依赖性的杀菌活性。
临床用途本品适应症为治疗患有上呼吸道和下呼吸道感染的成人,如急性窦炎,慢性支气管炎急性发作,社区获得性肺炎,以及皮肤和软组织感染给药途径及用量任何适应症推荐一次400mg,一日一次,服用时间不受饮食影响治疗时间:慢性支气管炎急性发作:5天;社区获得性肺炎:10天;急性窦炎:7天;治疗皮肤和软组织感染推荐治疗时间为7天药物相互作用抗酸药、矿物质和多种维生素同服,本品会形成多价螯合而减少药物吸收,因此抗酸药、含镁、铝和其它矿物质如铁等制剂需服用本品4小时前或2小时后慎与下列药物合用:1a类(如奎宁丁普鲁卡因)或III类(如胺碘酮索托落尔)抗心律失常药西沙必利红霉素抗精神病药物和三环类抗抑郁药食物和乳制品:食物的摄入不影响莫西沙星的吸收因此莫西沙星的服用时间不受进食的影响抗酸药矿物质和多种维生素:莫西沙星与抗酸药矿物质和多种维生素同时服用会因为与这些物质形成多价螯合物而减少药物的吸收这将导致血浆中的药物浓度比预定值低因此抗酸药抗逆转录病毒和其他含有镁铝和其他矿物质如铁等的制剂需要在口服莫西沙星4小时前或2小时后服用雷尼替丁:与雷尼替丁同时服用不会影响莫西沙星的吸收特性其吸收参数(CmaxTmaxAUC)均提示莫西沙星不受胃酸缺乏的影响钙补充剂:当给予高剂量补充剂时仅观察到吸收率稍有减少而吸收范围保持不变高剂量钙补充剂对莫西沙星的吸收不具有临床意义茶碱:莫西沙星对稳态时茶碱的药代动力学无影响提示莫西沙星对P450酶的1A2亚型无影响当服用莫西沙星治疗时达到稳态的茶碱浓度未升高因此服用莫西沙星时不必调整茶碱的用量华法令:据观察莫西沙星与华法令同时服用未发现对凝血酶原时间和凝血的其他参数有影响口服避孕药:莫西沙星与口服避孕药同时服用未发现有相互作用抗糖尿病药:优降糖和莫西沙星同时服用未发现有相互作用伊曲康唑:莫西沙星与伊曲康唑同时服用时伊曲康唑的药时曲线下面积(AUC)仅少量改变伊曲康唑对莫西沙星的药代动力学无显著性影响当服用伊曲康唑时给予莫西沙星不需要调整剂量反之亦然地高辛:莫西沙星对地高辛的药代动力学没有严重影响反之亦然吗啡:肠外给予吗啡同时服用莫西沙星并不减少口服莫西沙星的生物利用度且Cmax(17%)仅稍有下降普鲁苯辛:在一项观察普鲁苯辛对肾脏排泄功能影响的研究中未发现对莫西沙星的全身清除和肾脏清除有明显影响因此当这两种药同时服用时不必调整剂量炭:同时口服炭及400 mg莫西沙星能减少药物的全身利用在体内能阻止80%药物吸收药物过量时利用活性炭能在吸收早期阻止药物的进一步进入全身系统注意事项1.喹诺酮药物使用可诱发癫痫的发作,因此此类病人服用本品要注意2.本品应避免用QT间期延长的患者。
盐酸左氧氟沙星氯化钠注射液
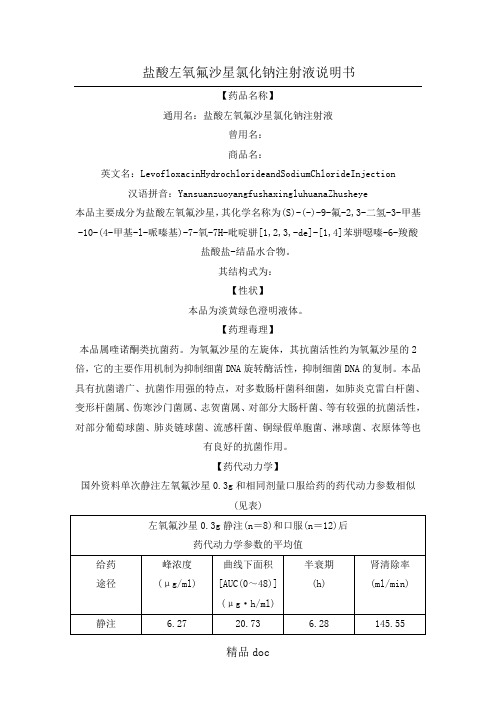
盐酸左氧氟沙星氯化钠注射液说明书【药品名称】通用名:盐酸左氧氟沙星氯化钠注射液曾用名:商品名:英文名:LevofloxacinHydrochlorideandSodiumChlorideInjection 汉语拼音:YansuanzuoyangfushaxingluhuanaZhusheye多剂量静注研究中(0.3g每日两次静脉滴注,共6天),其血药浓度于24~48小时达稳态,首次及末次剂量后的血药峰浓度分别为5.35和6.12ug/ml,表明无明显蓄积。
左氧氟沙星在体内组织中分布广泛。
主要以原型药由尿中排出。
肾功能减退的患静脉滴注:成人一日400ml(0.4g),分2次静滴。
重度感染患者及病原菌对本品敏感性较差者(如铜绿假单胞菌),每日最大剂量可增至600ml(0.6g),分2次静滴。
【不良反应】用药期间可能出现恶心、呕吐、腹部不适、腹泻、食欲缺乏、腹痛、腹胀等胃肠道症状,失眠、头晕、头痛等神经系统症状以及皮疹、瘙痒等。
亦可出现一过性肝功能异常,如血清氨基转移酶增高、血清总胆红素增加高等。
上述不良反应发生率在0.1~5%之间。
偶见血中尿素氮升高、倦怠、发热、心悸、味觉异常等。
一般均能耐受,疗程结束后迅速消失。
【禁忌症】对喹诺酮类药物过敏者禁用。
【注意事项】1.本制剂专供静脉滴注,滴注时间为每100ml至少60分钟。
本制剂不宜与其它妊娠、哺乳期妇女禁用。
【儿童用药】18岁以下患者禁用。
【老年患者用药】【药物相互作用】1.避免与茶碱同时使用。
如需同时应用,应监测茶碱的血药浓度,以调整剂量。
2.与华法林或其衍生物同时应用时,应监测凝血酶原时间或其它凝血试验。
3.与非甾体类消炎药物同时应用,有引发抽搐的可能。
4.与口服降血糖药同时使用时可能引起血糖失调,包括高血糖及低血糖,因此用药过程中应注意监测血糖浓度,一旦发生低血糖时应立即停用本品,并给予适当处理。
【药物过量】左氧氟沙星无法通过血液透析或腹膜透析被有效地排除。
盐酸莫西沙星氯化钠注射液说明书产品手册

核准日期:修改日期:盐酸莫西沙星氯化钠注射液说明书请仔细阅读说明书并在医师指导下使用。
【药品名称】通用名称:盐酸莫西沙星氯化钠注射液商品名称:拜复乐Avelox 英文名称:Moxifloxacin Hydrochloride and Sodium Chloride Injection 汉语拼音:Yansuan Moxishaxing Lühuana Zhusheye【成份】化学名称:1-环丙基-7-(S,S)-2,8-重氮-二环4.3.0壬-8-基-6-氟-8-甲氧-1,4-二氢-4-氧-3-喹啉羧酸盐酸盐。
化学结构式:O F COOH H H N N N O H3C H x HCl 分子式:C21H24FN3O4HCl 分子量:437.9 辅料:氯化钠、盐酸、氢氧化钠、注射用水。
【性状】本品为黄色的澄清液体。
【适应症】成人≥18岁上呼吸道和下呼吸道感染,如:急性窦炎,慢性支气管炎急性发作,社区获得性肺炎;以及皮肤和软组织感染。
【规格】250ml : 莫西沙星0.4g与氯化钠2.0g。
【用法用量】给药方法:根据中国健康受试者心脏所能耐受的输液速率以及国内I、II、III期临床研究的结果,推荐本品的输液时间应为90分钟。
国外推荐0.4g莫西沙星静脉给药的输液时间应大于60分钟。
剂量范围成人:推荐剂量为一次0.4g,一日一次一次1瓶,一日一次。
疗程:根据症状的严重程度或临床反应决定疗程。
治疗上呼吸道和下呼吸道感染时通常可按照下列疗程:慢性支气管炎急性发作:5天社区获得性肺炎:序贯给药静脉给药后继续口服用药推荐的总疗程为7~14天。
急性窦炎:7天治疗皮肤和软组织感染的推荐疗程为7天。
莫西沙星可以在开始治疗时静脉给药,之后再根据患者情况口服片剂给药。
0.4g莫西沙星注射液在临床试验中最多用过14天。
给药方法:静脉给药0.4g的时间应为90分钟。
莫西沙星既可以单独给药也可以与一些相容的溶液一同滴注。
盐酸莫西沙星氯化钠注射液说明书
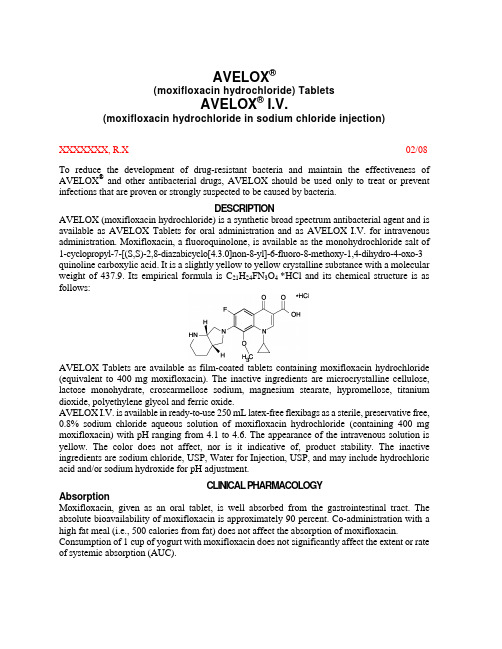
AVELOX®(moxifloxacin hydrochloride) TabletsAVELOX® I.V.(moxifloxacin hydrochloride in sodium chloride injection)XXXXXXX, R.X02/08 To reduce the development of drug-resistant bacteria and maintain the effectiveness of AVELOX® and other antibacterial drugs, AVELOX should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONAVELOX (moxifloxacin hydrochloride) is a synthetic broad spectrum antibacterial agent and is available as AVELOX Tablets for oral administration and as AVELOX I.V. for intravenous administration. Moxifloxacin, a fluoroquinolone, is available as the monohydrochloride salt of 1-cyclopropyl-7-[(S,S)-2,8-diazabicyclo[4.3.0]non-8-yl]-6-fluoro-8-methoxy-1,4-dihydro-4-oxo-3 quinoline carboxylic acid. It is a slightly yellow to yellow crystalline substance with a molecular weight of 437.9. Its empirical formula is C21H24FN3O4 *HCl and its chemical structure is as follows:AVELOX Tablets are available as film-coated tablets containing moxifloxacin hydrochloride (equivalent to 400 mg moxifloxacin). The inactive ingredients are microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, magnesium stearate, hypromellose, titanium dioxide, polyethylene glycol and ferric oxide.AVELOX I.V. is available in ready-to-use 250 mL latex-free flexibags as a sterile, preservative free, 0.8% sodium chloride aqueous solution of moxifloxacin hydrochloride (containing 400 mg moxifloxacin) with pH ranging from 4.1 to 4.6. The appearance of the intravenous solution is yellow. The color does not affect, nor is it indicative of, product stability. The inactive ingredients are sodium chloride, USP, Water for Injection, USP, and may include hydrochloric acid and/or sodium hydroxide for pH adjustment.CLINICAL PHARMACOLOGYAbsorptionMoxifloxacin, given as an oral tablet, is well absorbed from the gastrointestinal tract. The absolute bioavailability of moxifloxacin is approximately 90 percent. Co-administration with a high fat meal (i.e., 500 calories from fat) does not affect the absorption of moxifloxacin. Consumption of 1 cup of yogurt with moxifloxacin does not significantly affect the extent or rate of systemic absorption (AUC).The mean (± SD) C max and AUC values following single and multiple doses of 400 mg moxifloxacin given orally are summarized below.C max (mg/L)AUC(mg•h/L)Half-life(hr)Single Dose OralHealthy (n = 372) 3.1 ± 1.036.1 ± 9.111.5 - 15.6* Multiple Dose OralHealthy young male/female (n = 15) 4.5 ± 0.548.0 ± 2.712.7 ± 1.9 Healthy elderly male (n = 8) 3.8 ± 0.351.8 ± 6.7Healthy elderly female (n = 8) 4.6 ± 0.654.6 ± 6.7Healthy young male (n = 8) 3.6 ± 0.548.2 ± 9.0Healthy young female (n = 9) 4.2 ± 0.549.3 ± 9.5* Range of means from different studiesThe mean (± SD) C max and AUC values following single and multiple doses of 400 mg moxifloxacin given by 1 hour I.V. infusion are summarized below.C max (mg/L)AUC(mg•h/L)Half-life(hr)Single Dose I.V.Healthy young male/female (n = 56) 3.9 ± 0.939.3 ± 8.68.2 - 15.4* Patients (n = 118)Male (n = 64) 4.4 ± 3.7Female (n = 54) 4.5 ± 2.0< 65 years (n = 58) 4.6 ± 4.2≥ 65 years (n = 60) 4.3 ± 1.3Multiple Dose I.V.Healthy young male (n = 8) 4.2 ± 0.838.0 ± 4.714.8 ± 2.2 Healthy elderly (n =12; 8 male, 4 female) 6.1 ± 1.348.2 ± 0.910.1 ± 1.6 Patients** (n = 107)Male (n = 58) 4.2 ± 2.6Female (n = 49) 4.6 ± 1.5< 65 years (n = 52) 4.1 ± 1.4≥ 65 years (n = 55) 4.7 ± 2.7* Range of means from different studies** Expected C max (concentration obtained around the time of the end of the infusion)Plasma concentrations increase proportionately with dose up to the highest dose tested (1200 mg single oral dose). The mean (± SD) elimination half-life from plasma is 12 ± 1.3 hours; steady-state is achieved after at least three days with a 400 mg once daily regimen.Mean Steady-State Plasma Concentrations of Moxifloxacin Obtained With Once Daily Dosing of 400 mg Either Orally (n=10) or by I.V. Infusion (n=12)DistributionMoxifloxacin is approximately 30-50% bound to serum proteins, independent of drug concentration. The volume of distribution of moxifloxacin ranges from 1.7 to 2.7 L/kg. Moxifloxacin is widely distributed throughout the body, with tissue concentrations often exceeding plasma concentrations. Moxifloxacin has been detected in the saliva, nasal and bronchial secretions, mucosa of the sinuses, skin blister fluid, subcutaneous tissue, skeletal muscle, and abdominal tissues and fluids following oral or intravenous administration of 400 mg. Moxifloxacin concentrations measured post-dose in various tissues and fluids following a 400 mg oral or I.V. dose are summarized in the following table. The rates of elimination of moxifloxacin from tissues generally parallel the elimination from plasma.Moxifloxacin Concentrations (mean ± SD) in Tissuesand the Corresponding Plasma Concentrations After a Single 400 mg Oral orIntravenous Dose §Tissue or Fluid NPlasmaConcentration(µg/mL)Tissue or FluidConcentration(µg/mL or µg/g)TissuePlasmaRatio:RespiratoryAlveolar Macrophages5 3.3± 0.761.8± 27.321.2 ± 10.0 Bronchial Mucosa8 3.3± 0.7 5.5± 1.3 1.7 ± 0.3 Epithelial Lining Fluid5 3.3± 0.724.4± 14.78.7 ± 6.1 SinusMaxillary Sinus Mucosa4 3.7± 1.1†7.6± 1.7 2.0 ± 0.3 Anterior Ethmoid Mucosa3 3.7± 1.1†8.8± 4.3 2.2 ± 0.6 Nasal Polyps4 3.7± 1.1†9.8± 4.5 2.6 ± 0.6 Skin, MusculoskeletalBlister Fluid5 3.0± 0.5‡ 2.6± 0.9 0.9 ± 0.2 Subcutaneous Tissue6 2.3± 0.4#0.9± 0.3* 0.4 ± 0.6 Skeletal Muscle6 2.3± 0.4#0.9± 0.2* 0.4 ± 0.1 Intra-AbdominalAbdominal tissue 8 2.9± 0.5 7.6 ± 2.0 2.7 ± 0.8 Abdominal exudate 10 2.3±0.5 3.5 ±1.2 1.6 ± 0.7 Abscess fluid 6 2.7± 0.7 2.3 ±1.5 0.8±0.4§all moxifloxacin concentrations were measured 3 hours after a single 400 mg dose, except the abdominal tissue and exudate concentrations which were measured at 2 hours post-dose and the sinus concentrations which were measured 3 hours post-dose after 5 days of dosing.† N = 5‡N = 7#N = 12* Reflects only non-protein bound concentrations of drug.MetabolismApproximately 52% of an oral or intravenous dose of moxifloxacin is metabolized via glucuronide and sulfate conjugation. The cytochrome P450 system is not involved in moxifloxacin metabolism, and is not affected by moxifloxacin. The sulfate conjugate (M1) accounts for approximately 38% of the dose, and is eliminated primarily in the feces. Approximately 14% of an oral or intravenous dose is converted to a glucuronide conjugate (M2), which is excreted exclusively in the urine. Peak plasma concentrations of M2 are approximately 40% those of the parent drug, while plasma concentrations of M1 are generally less than 10% those of moxifloxacin.In vitro studies with cytochrome (CYP) P450 enzymes indicate that moxifloxacin does not inhibit CYP3A4, CYP2D6, CYP2C9, CYP2C19, or CYP1A2, suggesting that moxifloxacin is unlikely to alter the pharmacokinetics of drugs metabolized by these enzymes.ExcretionApproximately 45% of an oral or intravenous dose of moxifloxacin is excreted as unchanged drug (~20% in urine and ~25% in feces). A total of 96% ± 4% of an oral dose is excreted as either unchanged drug or known metabolites. The mean (± SD) apparent total body clearance and renal clearance are 12 ± 2.0 L/hr and 2.6 ± 0.5 L/hr, respectively.Special PopulationsGeriatricFollowing oral administration of 400 mg moxifloxacin for 10 days in 16 elderly (8 male; 8 female) and 17 young (8 male; 9 female) healthy volunteers, there were no age-related changes in moxifloxacin pharmacokinetics. In 16 healthy male volunteers (8 young; 8 elderly) given a single 200 mg dose of oral moxifloxacin, the extent of systemic exposure (AUC and C max)was not statistically different between young and elderly males and elimination half-life was unchanged. No dosage adjustment is necessary based on age. In large phase III studies, the concentrations around the time of the end of the infusion in elderly patients following intravenous infusion of 400 mg were similar to those observed in young patients.PediatricThe pharmacokinetics of moxifloxacin in pediatric subjects have not been studied.GenderFollowing oral administration of 400 mg moxifloxacin daily for 10 days to 23 healthy males (19-75 years) and 24 healthy females (19-70 years), the mean AUC and C max were 8% and 16% higher, respectively, in females compared to males. There are no significant differences in moxifloxacin pharmacokinetics between male and female subjects when differences in body weight are taken into consideration.A 400 mg single dose study was conducted in 18 young males and females. The comparison of moxifloxacin pharmacokinetics in this study (9 young females and 9 young males) showed no differences in AUC or C max due to gender. Dosage adjustments based on gender are not necessary. RaceSteady-state moxifloxacin pharmacokinetics in male Japanese subjects were similar to those determined in Caucasians, with a mean C max of 4.1 µg/mL, an AUC24 of 47 µg•h/mL, and an elimination half-life of 14 hours, following 400 mg p.o. daily.Renal InsufficiencyThe pharmacokinetic parameters of moxifloxacin are not significantly altered in mild, moderate, severe, or end-stage renal disease. No dosage adjustment is necessary in patients with renal impairment, including those patients requiring hemodialysis (HD) or continuous ambulatory peritoneal dialysis (CAPD).In a single oral dose study of 24 patients with varying degrees of renal function from normal to severely impaired, the mean peak concentrations (C max) of moxifloxacin were reduced by 21% and 28% in the patients with moderate (CL CR ≥30 and ≤ 60 mL/min) and severe (CL CR < 30 mL/min) renal impairment, respectively. The mean systemic exposure (AUC) in these patients was increased by 13%. In the moderate and severe renally impaired patients, the mean AUC for the sulfate conjugate (M1) increased by 1.7-fold (ranging up to 2.8-fold) and mean AUC andC max for the glucuronide conjugate (M2) increased by 2.8-fold (ranging up to 4.8-fold) and1.4-fold (ranging up to2.5-fold), respectively.The pharmacokinetics of single dose and multiple dose moxifloxacin were studied in patients with CL CR < 20 mL/min on either hemodialysis or continuous ambulatory peritoneal dialysis (8 HD, 8 CAPD). Following a single 400 mg oral dose, the AUC of moxifloxacin in these HD and CAPD patients did not vary significantly from the AUC generally found in healthy volunteers. C max values of moxifloxacin were reduced by about 45% and 33% in HD and CAPD patients, respectively, compared to healthy, historical controls. The exposure (AUC) to the sulfate conjugate (M1) increased by 1.4- to 1.5-fold in these patients. The mean AUC of the glucuronide conjugate (M2) increased by a factor of 7.5, whereas the mean C max values of the glucuronide conjugate (M2) increased by a factor of 2.5 to 3, compared to healthy subjects. The sulfate and the glucuronide conjugates of moxifloxacin are not microbiologically active, and the clinical implication of increased exposure to these metabolites in patients with renal disease including those undergoing HD and CAPD has not been studied.Oral administration of 400 mg QD moxifloxacin for 7 days to patients on HD or CAPD produced mean systemic exposure (AUC ss) to moxifloxacin similar to that generally seen in healthy volunteers. Steady-state C max values were about 22% lower in HD patients but were comparable between CAPD patients and healthy volunteers. Both HD and CAPD removed only small amounts of moxifloxacin from the body (approximately 9% by HD, and 3% by CAPD). HD and CAPD also removed about 4% and 2% of the glucuronide metabolite (M2), respectively. Hepatic InsufficiencyIn 400 mg single oral dose studies in 6 patients with mild (Child Pugh Class A), and 10 patients with moderate (Child Pugh Class B), hepatic insufficiency, moxifloxacin mean systemic exposure (AUC) was 78% and 102%, respectively, of 18 healthy controls and mean peak concentration (C max)was 79% and 84% of controls.The mean AUC of the sulfate conjugate of moxifloxacin (M1) increased by 3.9-fold (ranging up to 5.9-fold) and 5.7-fold (ranging up to 8.0-fold) in the mild and moderate groups, respectively. The mean C max of M1 increased by approximately 3-fold in both groups (ranging up to 4.7- and 3.9-fold). The mean AUC of the glucuronide conjugate of moxifloxacin (M2) increased by 1.5-fold (ranging up to 2.5-fold) in both groups. The mean C max of M2 increased by 1.6- and 1.3-fold (ranging up to 2.7- and 2.1-fold), respectively. The clinical significance of increased exposure to the sulfate and glucuronide conjugates has not been studied. No dosage adjustment is recommended for mild or moderate hepatic insufficiency (Child Pugh Classes A and B). The pharmacokinetics of moxifloxacin in severe hepatic insufficiency (Child Pugh Class C) have not been studied. (See DOSAGE AND ADMINISTRATION.)Photosensitivity PotentialA study of the skin response to ultraviolet (UVA and UVB) and visible radiation conducted in 32 healthy volunteers (8 per group) demonstrated that moxifloxacin does not show phototoxicity in comparison to placebo. The minimum erythematous dose (MED) was measured before and after treatment with moxifloxacin (200 mg or 400 mg once daily), lomefloxacin (400 mg once daily), or placebo. In this study, the MED measured for both doses of moxifloxacin were not significantly different from placebo, while lomefloxacin significantly lowered the MED. (See PRECAUTIONS, Information for Patients.)It is difficult to ascribe relative photosensitivity/phototoxicity among various fluoroquinolones during actual patient use because other factors play a role in determining a subject’s susceptibility to this adverse event such as: a patient’s skin pigmentation, frequency and duration of sun and artificial ultraviolet light (UV) exposure, wearing of sunscreen andprotective clothing, the use of other concomitant drugs and the dosage and duration of fluoroquinolone therapy (See ADVERSE REACTIONS and ADVERSEREACTIONS/Post-Marketing Adverse Event Reports).Drug-drug InteractionsThe potential for pharmacokinetic drug interactions between moxifloxacin and itraconazole, theophylline, warfarin, digoxin, atenolol, probenecid, morphine, oral contraceptives, ranitidine, glyburide, calcium, iron, and antacids has been evaluated. There was no clinically significant effect of moxifloxacin on itraconazole, theophylline, warfarin, digoxin, atenolol, oral contraceptives, or glyburide kinetics. Itraconazole, theophylline, warfarin, digoxin, probenecid, morphine, ranitidine, and calcium did not significantly affect the pharmacokinetics of moxifloxacin. These results and the data from in vitro studies suggest that moxifloxacin is unlikely to significantly alter the metabolic clearance of drugs metabolized by CYP3A4, CYP2D6, CYP2C9, CYP2C19, or CYP1A2 enzymes.As with all other quinolones, iron and antacids significantly reduced bioavailability of moxifloxacin.Itraconazole:In a study involving 11 healthy volunteers, there was no significant effect of itraconazole (200 mg once daily for 9 days), a potent inhibitor of cytochrome P4503A4, on the pharmacokinetics of moxifloxacin (a single 400 mg dose given on the 7th day of itraconazole dosing). In addition, moxifloxacin was shown not to affect the pharmacokinetics of itraconazole. Theophylline:No significant effect of moxifloxacin (200 mg every twelve hours for 3 days) on the pharmacokinetics of theophylline (400 mg every twelve hours for 3 days) was detected in a study involving 12 healthy volunteers. In addition, theophylline was not shown to affect the pharmacokinetics of moxifloxacin. The effect of co-administration of a 400 mg dose of moxifloxacin with theophylline has not been studied, but it is not expected to be clinically significant based on in vitro metabolic data showing that moxifloxacin does not inhibit the CYP1A2 isoenzyme.Warfarin:No significant effect of moxifloxacin (400 mg once daily for eight days) on the pharmacokinetics of R- and S-warfarin (25 mg single dose of warfarin sodium on the fifth day) was detected in a study involving 24 healthy volunteers. No significant change in prothrombin time was observed. (See PRECAUTIONS, Drug Interactions.)Digoxin:No significant effect of moxifloxacin (400 mg once daily for two days) on digoxin (0.6 mg as a single dose) AUC was detected in a study involving 12 healthy volunteers. The mean digoxin C max increased by about 50% during the distribution phase of digoxin. This transient increase in digoxin C max is not viewed to be clinically significant. Moxifloxacin pharmacokinetics were similar in the presence or absence of digoxin. No dosage adjustment for moxifloxacin or digoxin is required when these drugs are administered concomitantly. Atenolol:In a crossover study involving 24 healthy volunteers (12 male; 12 female), the mean atenolol AUC following a single oral dose of 50 mg atenolol with placebo was similar to that observed when atenolol was given concomitantly with a single 400 mg oral dose of moxifloxacin. The mean C max of single dose atenolol decreased by about 10% following co-administration with a single dose of moxifloxacin.Morphine:No significant effect of morphine sulfate (a single 10 mg intramuscular dose) on the mean AUC and C max of moxifloxacin (400 mg single dose) was observed in a study of 20 healthy male and female volunteers.Oral Contraceptives:A placebo-controlled study in 29 healthy female subjects showed that moxifloxacin 400 mg daily for 7 days did not interfere with the hormonal suppression of oral contraception with 0.15 mg levonorgestrel/0.03 mg ethinylestradiol (as measured by serum progesterone, FSH, estradiol, and LH), or with the pharmacokinetics of the administered contraceptive agents.Probenecid:Probenecid (500 mg twice daily for two days) did not alter the renal clearance and total amount of moxifloxacin (400 mg single dose) excreted renally in a study of 12 healthy volunteers.Ranitidine:No significant effect of ranitidine (150 mg twice daily for three days as pretreatment) on the pharmacokinetics of moxifloxacin (400 mg single dose) was detected in a study involving 10 healthy volunteers.Antidiabetic agents:In diabetics, glyburide (2.5 mg once daily for two weeks pretreatment and for five days concurrently) mean AUC and C max were 12% and 21% lower, respectively, when taken with moxifloxacin (400 mg once daily for five days) in comparison to placebo. Nonetheless, blood glucose levels were decreased slightly in patients taking glyburide and moxifloxacin in comparison to those taking glyburide alone, suggesting no interference by moxifloxacin on the activity of glyburide. These interaction results are not viewed as clinically significant. Calcium:Twelve healthy volunteers were administered concomitant moxifloxacin (single 400 mg dose) and calcium (single dose of 500 mg Ca++ dietary supplement) followed by an additional two doses of calcium 12 and 24 hours after moxifloxacin administration. Calcium had no significant effect on the mean AUC of moxifloxacin. The mean C max was slightly reduced and the time to maximum plasma concentration was prolonged when moxifloxacin was given with calcium compared to when moxifloxacin was given alone (2.5 hours versus 0.9 hours). These differences are not considered to be clinically significant.Antacids:When moxifloxacin (single 400 mg tablet dose) was administered two hours before, concomitantly, or 4 hours after an aluminum/magnesium-containing antacid (900 mg aluminum hydroxide and 600 mg magnesium hydroxide as a single oral dose) to 12 healthy volunteers there was a 26%, 60% and 23% reduction in the mean AUC of moxifloxacin, respectively. Moxifloxacin should be taken at least 4 hours before or 8 hours after antacids containing magnesium or aluminum, as well as sucralfate, metal cations such as iron, and multivitamin preparations with zinc, or VIDEX® (didanosine) chewable/ buffered tablets or the pediatric powder for oral solution. (See PRECAUTIONS, Drug Interactions and DOSAGE AND ADMINISTRATION.) Iron:When moxifloxacin tablets were administered concomitantly with iron (ferrous sulfate 100 mg once daily for two days), the mean AUC and C max of moxifloxacin was reduced by 39% and 59%, respectively. Moxifloxacin should only be taken more than 4 hours before or 8 hours after iron products. (See PRECAUTIONS, Drug Interactions and DOSAGE AND ADMINISTRATION.) Electrocardiogram:Prolongation of the QT interval in the ECG has been observed in some patients receiving moxifloxacin. Following oral dosing with 400 mg of moxifloxacin the mean (± SD) change in QTc from the pre-dose value at the time of maximum drug concentration was 6 msec (± 26) (n = 787). Following a course of daily intravenous dosing (400 mg; 1 hour infusion each day) the mean change in QTc from the Day 1 pre-dose value was 9 msec (± 24) on Day 1 (n = 69) and 3 msec (± 29) on Day 3 (n = 290). (See WARNINGS.)There is limited information available on the potential for a pharmacodynamic interaction in humans between moxifloxacin and other drugs that prolong the QTc interval of the electrocardiogram. Sotalol, a Class III antiarrhythmic, has been shown to further increase the QTc interval when combined with high doses of intravenous (I.V.) moxifloxacin in dogs. Therefore, moxifloxacin should be avoided with Class IA and Class III antiarrhythmics. (See ANIMAL PHARMACOLOGY, WARNINGS,and PRECAUTIONS.)MICROBIOLOGYMoxifloxacin has in vitro activity against a wide range of Gram-positive and Gram-negative microorganisms. The bactericidal action of moxifloxacin results from inhibition of the topoisomerase II (DNA gyrase) and topoisomerase IV required for bacterial DNA replication, transcription, repair, and recombination. It appears that the C8-methoxy moiety contributes to enhanced activity and lower selection of resistant mutants of Gram-positive bacteria compared to the C8-H moiety. The presence of the bulky bicycloamine substituent at the C-7 position prevents active efflux, associated with the NorA or pmrA genes seen in certain Gram-positive bacteria. The mechanism of action for quinolones, including moxifloxacin, is different from that of macrolides, beta-lactams, aminoglycosides, or tetracyclines; therefore, microorganisms resistant to these classes of drugs may be susceptible to moxifloxacin and other quinolones. There is no known cross-resistance between moxifloxacin and other classes of antimicrobials.In vitro resistance to moxifloxacin develops slowly via multiple-step mutations. Resistance to moxifloxacin occurs in vitro at a general frequency of between 1.8 x 10–9 to < 1 x 10–11 for Gram-positive bacteria.Cross-resistance has been observed between moxifloxacin and other fluoroquinolones against Gram-negative bacteria. Gram-positive bacteria resistant to other fluoroquinolones may, however, still be susceptible to moxifloxacin.Moxifloxacin has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section. Aerobic Gram-positive microorganismsEnterococcus faecalis (many strains are only moderately susceptible)Staphylococcus aureus (methicillin-susceptible strains only)Streptococcus anginosusStreptococcus constellatusStreptococcus pneumoniae (including multi-drug resistant strains [MDRSP]*) Streptococcus pyogenes* MDRSP, Multi-drug resistant Streptococcus pneumoniae includes isolates previously known as PRSP (Penicillin-resistant S. pneumoniae), and are strains resistant to two or more of the following antibiotics: penicillin (MIC ≥ 2 μg/mL), 2nd generation cephalosporins (e.g., cefuroxime), macrolides, tetracyclines, and trimethoprim/sulfamethoxazole.Aerobic Gram-negative microorganismsEnterobacter cloacaeEscherichia coliHaemophilus influenzaeHaemophilus parainfluenzaeKlebsiella pneumoniaeMoraxella catarrhalisProteus mirabilisAnaerobic microorganismsBacteroides fragilisBacteroides thetaiotaomicronClostridium perfringensPeptostreptococcus speciesOther microorganismsChlamydia pneumoniaeMycoplasma pneumoniaeThe following in vitro data are available, but their clinical significance is unknown.Moxifloxacin exhibits in vitro minimum inhibitory concentrations (MICs) of 2 µg/mL or lessagainst most (≥ 90%) strains of the following microorganisms; however, the safety andeffectiveness of moxifloxacin in treating clinical infections due to these microorganisms have notbeen established in adequate and well-controlled clinical trials.Aerobic Gram-positive microorganismsStaphylococcus epidermidis (methicillin-susceptible strains only)Streptococcus agalactiaeStreptococcus viridans groupAerobic Gram-negative microorganismsCitrobacter freundiiKlebsiella oxytocaLegionella pneumophilaAnaerobic microorganismsFusobacterium speciesPrevotella speciesSusceptibility TestsDilution Techniques:Quantitative methods are used to determine antimicrobial minimuminhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteriato antimicrobial compounds. The MICs should be determined using a standardized procedure.Standardized procedures are based on a dilution method1 (broth or agar) or equivalent withstandardized inoculum concentrations and standardized concentrations of moxifloxacin powder.The MIC values should be interpreted according to the following criteria:For testing Enterobacteriaceae and methicillin-susceptible Staphylococcus aureus:MIC (µg/mL)Interpretation≤2.0 Susceptible(S)4.0Intermediate(I)≥8.0Resistant(R)For testing Haemophilus influenzae and Haemophilus parainfluenzae a:MIC (µg/mL) Interpretation(S) ≤1.0 Susceptiblea This interpretive standard is applicable only to broth microdilution susceptibility tests withHaemophilus influenzae and Haemophilus parainfluenzae using Haemophilus Test Medium1.The current absence of data on resistant strains precludes defining any results other than“Susceptible”. Strains yielding MIC results suggestive of a “nonsusceptible” category should besubmitted to a reference laboratory for further testing.For testing Streptococcus species including Streptococcus pneumoniae b and Enterococcus faecalis:MIC (µg/mL)Interpretation≤1.0 Susceptible(S)2.0Intermediate(I)≥ 4.0Resistant(R)b These interpretive standards are applicable only to broth microdilution susceptibility tests using cation-adjusted Mueller-Hinton broth with 2 - 5% lysed horse blood.A report of “Susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable. A report of “Intermediate” indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where a high dosage of drug can be used. This category also provides a buffer zone which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “Resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable; other therapy should be selected.Standardized susceptibility test procedures require the use of laboratory control microorganisms to control the technical aspects of the laboratory procedures. Standard moxifloxacin powder should provide the following MIC values:Microorganism MIC (µg/mL)Enterococcus faecalis ATCC 292120.06- 0.5Escherichia coli ATCC 259220.008- 0.06Haemophilus influenzae ATCC 49247c0.008- 0.03Staphylococcus aureus ATCC 292130.015- 0.06Streptococcus pneumoniae ATCC 49619d0.06- 0.25c This quality control range is applicable to only H. influenzae ATCC 49247 tested by a broth microdilution procedure using Haemophilus Test Medium (HTM)1.d This quality control range is applicable to only S. pneumoniae ATCC 49619 tested by a broth microdilution procedure using cation-adjusted Mueller-Hinton broth with 2 - 5% lysed horse blood.Diffusion Techniques:Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure2 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 5-µg moxifloxacin to test the susceptibility of microorganisms to moxifloxacin.Reports from the laboratory providing results of the standard single-disk susceptibility test with a 5-µg moxifloxacin disk should be interpreted according to the following criteria:。
盐酸左氧氟沙星氯化钠注射液

盐酸左氧氟沙星氯化钠注射液说明书【药品名称】通用名:盐酸左氧氟沙星氯化钠注射液曾用名:商品名:英文名:Levofloxacin Hydrochloride and Sodium Chloride Injection汉语拼音:Yan sua nzuoya ngfushax in gluhua na Zhusheye本品主要成分为盐酸左氧氟沙星,其化学名称为(S)-(-)-9-氟-2,3-二氢-3-甲基-10-(4-甲基-l-哌嗪基)-7-氧-7H-吡啶骈[1,2,3,-de]-[1,4]苯骈恶嗪-6-羧酸盐酸盐-结晶水合物。
其结构式为:【性状】本品为淡黄绿色澄明液体。
【药理毒理】本品属喹诺酮类抗菌药。
为氧氟沙星的左旋体,其抗菌活性约为氧氟沙星的2倍,它的主要作用机制为抑制细菌DNA旋转酶活性,抑制细菌DNA的复制。
本品具有抗菌谱广、抗菌作用强的特点,对多数肠杆菌科细菌,如肺炎克雷白杆菌、变形杆菌属、伤寒沙门菌属、志贺菌属、对部分大肠杆菌、等有较强的抗菌活性,对部分葡萄球菌、肺炎链球菌、流感杆菌、铜绿假单胞菌、淋球菌、衣原体等也有良好的抗菌作用。
【药代动力学】国外资料单次静注左氧氟沙星和相同剂量口服给药的药代动力参数相似(见表)多剂量静注研究中每日两次静脉滴注,共6天),其血药浓度于24〜48小时达稳态,首次及末次剂量后的血药峰浓度分别为和ml,表明无明显蓄积。
左氧氟沙星在体内组织中分布广泛。
主要以原型药由尿中排出。
肾功能减退的患者左氧氟沙星清除率下降,清除半衰期延长,为避免药物蓄积,应进行剂量调整。
血液透析和连续腹膜透析(CAPD)不影响左氧氟沙星从体内排除。
【适应症】本品适用于敏感细菌引起的下列中、重度感染:1•呼吸系统感染:急性支气管炎、慢性支气管炎急性发作、弥漫性支气管炎、支气管扩张合并感染、肺炎、扁桃体炎(扁桃体周围脓肿)。
2.泌尿系统感染:肾盂肾炎、复杂性尿路感染等。
3.生殖系统感染:急性前列腺炎、急性副睾炎、宫腔感染、子宫附件炎、盆腔炎(疑有厌氧菌感染时可合用甲硝唑)。
盐酸莫西沙星氯化钠注射液说明书
盐酸莫西沙星氯化钠注射液说明书
【药品名称】
通用名盐酸莫西沙星氯化钠
英文名Moxifloxacin Hydrochloride and Sodium Chloride Injection
拼音名Y ansuanmoxishaxing Luhuana Zhusheye
【性状】本品为黄色的澄明液体。
【药理毒理】莫西沙星是具有广谱活性和杀菌作用的8—甲氧基氟喹诺酮类药物。
莫西沙星在体外显示对革兰阳性菌,革兰阴性菌,厌氧菌,抗酸菌和非典型微生物和支原体,衣原体和军团菌具有广谱抗菌活性。
杀菌作用机制为干扰拓扑异构酶Ⅱ和Ⅳ。
拓朴异构酶是控制DNA拓朴和在DNA复制,修复和转录中关键的酶。
【功能主治/适应症】成人(大于18岁)上呼吸道和下呼吸道感染,如,急性窦炎,慢性支气管炎急性发作,社区获得性肺炎,及皮肤及软组织感染。
【用法用量】推荐剂量一次400mg,一日一次,慢性支气管炎急性发作:5天。
社区获得性肺炎:序贯给药推荐总疗程为7—14天。
急性窦炎:7天。
治疗皮肤及软组织感染的推荐为7天。
【不良反应】绝大多数不良反应为轻中度胃肠道反应,中枢神精系统不良反应,皮肤过敏等。
【禁忌】已知对该注射液的任何成份或其他喹诺酮类过敏者。
禁用于儿童,青少年,孕妇及哺乳期妇女。
【规格】250ml:0.4g莫西沙星,2.25g氯化钠
【贮藏】遮光、严封,在干燥阴凉处保存。
盐酸莫西沙星氯化钠注射液说明书

共 14981 例患者使用盐酸莫西沙星,平均年龄为 50 岁(约 73%的患者小于 65 岁),50%为男性,
63%是白人,12%是亚裔,9%是黑人。患者接受 0.4g 盐酸莫西沙星每日一次,口服、静脉滴注
或序贯给药(静脉滴注后改为口服)。治疗时间通常是 6-10 天,平均治疗天数为 9 天。
5%的患者由于发生不良事件停止使用盐酸莫西沙星。4.1%的患者口服 0.4g 盐酸莫西沙星,
不良反应 贫血 恶心 腹泻 呕吐 便秘 腹部疼痛 消化不良 发热 谷丙转氨酶升高 低钾血症 头痛 头晕 失眠
发生率% (N=14981) 1 7 6 2 2 2 1 1 1 1 4 3 2
表 3:盐酸莫西沙星与活性对照药物的临床试验中不常见(0.1%-<1%)不良反应(N=14981)
系统器官分类 血液和淋巴系统疾病
3、肾功能或肝功能不全患者
肝损害:
轻中度肝功能受损的患者(Child Pugh A级或B级)与健康志愿者或肝功能正常的患者
血浆药物浓度在临床上无明显差别。
肾损害:
肾功能受损的患者(包括肌酐清除率≤30ml/min/1.73m2)和慢性透析,如血液透析和连续
卧床腹膜透析的患者无需调整剂量。
4、给药说明
在获得培养结果之前可能已经选择盐酸莫西沙星进行治疗,一旦获得培养结果,应选择适当 的治疗。
盐酸莫西沙星氯化钠注射液用于治疗成人(≥18 岁)敏感细菌所引起的下列感染: 1、 急性细菌性鼻窦炎:由肺炎链球菌、流感嗜血杆菌或卡他莫拉菌引起。 由于使用氟喹诺酮类药物(包括盐酸莫西沙星)已有报道发生严重不良反应,且对于一些患 者,急性细菌性鼻窦炎有自限性,应在没有其它药物治疗时方可使用盐酸莫西沙星。 2、 慢性支气管炎急性发作:由肺炎链球菌、流感嗜血杆菌、副流感嗜血杆菌、肺炎克雷伯 菌、甲氧西林敏感的金黄色葡萄球菌或卡他莫拉菌引起。 由于使用氟喹诺酮类药物(包括盐酸莫西沙星)已有报道发生严重不良反应,且对于一些患 者,慢性支气管炎急性发作有自限性,应在没有其它药物治疗时方可使用盐酸莫西沙星。 3、社区获得性肺炎:由肺炎链球菌(包括多药耐药株)、流感嗜血杆菌、卡他莫拉菌、甲 氧西林敏感的金黄色葡萄球菌、肺炎克雷伯菌、肺炎支原体或肺炎衣原体引起。 4、非复杂性皮肤和皮肤组织感染:由甲氧西林敏感的金黄色葡萄球菌或化脓性链球菌引起。 5、复杂性皮肤和皮肤组织感染:由甲氧西林敏感的金黄色葡萄球菌、大肠埃希氏菌、肺炎 克雷伯氏菌或阴沟肠杆菌引起。 6、复杂性腹腔内感染:由大肠杆菌、脆弱类杆菌、咽峡炎链球菌、星座链球菌、粪肠球菌、 变形杆菌、产气荚膜梭菌、多形类杆菌或消化链球菌属等引起,包括腹腔脓肿。
盐酸莫西沙星氯化钠注射液说明书--拜复乐演示教学

盐酸莫西沙星氯化钠注射液说明书【药品名称】通用名:盐酸莫西沙星氯化钠注射液英文名:Moxifloxacin Hydrochloride and Sodium Chloride Injection汉语拼音:Yansuan Moxishaxing Lühuana Zhusheye商品名:拜复乐【成份】本品主要成份为盐酸莫西沙星。
化学名称:1-环丙基-7-{(S,S)-2,8-重氮–二环[4.3.0]壬-8-基}-6-氟-8-甲氧-1,4-二氢-4-氧-3-喹啉羧酸盐酸盐化学结构式:分子式:C21H24FN3O4·HCL分子量:437.9Cas No: 151096-09-2辅料:氯化钠、盐酸、氢氧化钠和注射用水。
【性状】本品为黄色的澄明液体。
【适应症】成人(≥18岁)上呼吸道和下呼吸道感染,如急性窦炎、慢性支气管炎急性发作、社区获得性肺炎,以及皮肤和软组织感染。
复杂腹腔感染包括混合细菌感染,如脓肿。
【用法用量】给药方法:根据中国健康受试者心脏所能耐受的输液速率以及国内I、II、III期临床研究的结果,推荐本品的输液时间为90分钟。
(国外推荐400mg莫西沙星静脉给药的输液时间应大于60分钟。
)剂量范围(成人):推荐剂量为一次400mg,一日一次(一次1瓶,一日一次)。
疗程:根据症状的严重程度或临床反应决定疗程。
治疗上呼吸道和下呼吸道感染时通常可按照下列疗程:慢性支气管炎急性发作:5天社区获得性肺炎:序贯给药(静脉给药后继续口服用药)推荐的总疗程为7-14天。
急性窦炎:7天治疗皮肤和软组织感染的推荐疗程为7天。
莫西沙星可以在开始治疗时静脉给药,之后再根据患者情况口服片剂给药。
400mg莫西沙星注射液在临床试验中最多用过14天。
给药方法:静脉给药400mg的时间应为90分钟。
莫西沙星既可以单独给药也可以与一些相容的溶液一同滴注。
下列注射液与莫西沙星注射液的混合液在室温条件下可保持稳定24小时以上,因此被认为可以合并给药:注射用水0.9%氯化钠注射液1摩尔氯化钠注射液5%葡萄糖注射液10%葡萄糖注射液40%葡萄糖注射液20%木糖醇注射液林格氏液乳酸林格氏液Aminofusin10%(生产厂家:Pharmacia&Upjohn)Jonosteril D5(生产厂家: Fresenius Kabi)若莫西沙星注射液需与其它药物合用,每种药物需单独给药(见不相容性)。
拜复乐说明书

【药品名称】通用名称:拜复乐商品名称:拜复乐【英文名称】汉语拼音:baifule【成份】盐酸莫西沙星氯化钠【性状】本品为黄色的澄明液体【作用类别】【适应症】成人(大于18岁)上呼吸道和下呼吸道感染,如,急性窦炎,慢性支气管炎急性发作,社区获得性肺炎,及皮肤及软组织感染。
【规格】250ml:0.4g ×1【用法用量】推荐剂量一次400mg,一日一次,慢性支气管炎急性发作:5天。
社区获得性肺炎:序贯给药推荐总疗程为7—14天。
急性窦炎:7天。
治疗皮肤及软组织感染的推荐为7天。
【不良反应】绝大多数不良反应为轻中度胃肠道反应,中枢神精系统不良反应,皮肤过敏等【禁忌】已知对该注射液的任何成份或其他喹诺酮类过敏者。
禁用于儿童,青少年,孕妇及哺乳期妇女。
【药物毒理】莫西沙星是具有广谱活性和杀菌作用的8—甲氧基氟喹诺酮类药物。
莫西沙星在体外显示对革兰阳性菌,革兰阴性菌,厌氧菌,抗酸菌和非典型微生物和支原体,衣原体和军团菌具有广谱抗菌活性。
杀菌作用机制为干扰拓扑异构酶Ⅱ和Ⅳ。
拓朴异构酶是控制DNA拓朴和在DNA复制,修复和转录中关键的酶。
【贮藏】干燥条件下贮藏。
【包装】瓶批准文号:国药准字J20040068生产企业:德国拜耳(拜耳医药保健分装)处方类型:本品为处方药!基本药理本品是广谱和具有抗菌活性的8-甲氧基氟喹诺酮类抗菌药。
抗菌机制为干扰II、IV拓扑异构酶。
本品是具有浓度依赖性的杀菌活性。
临床用途本品适应症为治疗患有上呼吸道和下呼吸道感染的成人,如急性窦炎,慢性支气管炎急性发作,社区获得性肺炎,以及皮肤和软组织感染给药途径及用量任何适应症推荐一次400mg,一日一次,服用时间不受饮食影响治疗时间:慢性支气管炎急性发作:5天;社区获得性肺炎:10天;急性窦炎:7天;治疗皮肤和软组织感染推荐治疗时间为7天药物相互作用抗酸药、矿物质和多种维生素同服,本品会形成多价螯合而减少药物吸收,因此抗酸药、含镁、铝和其它矿物质如铁等制剂需服用本品4小时前或2小时后慎与下列药物合用:1a类(如奎宁丁普鲁卡因)或III类(如胺碘酮索托落尔)抗心律失常药西沙必利红霉素抗精神病药物和三环类抗抑郁药食物和乳制品:食物的摄入不影响莫西沙星的吸收因此莫西沙星的服用时间不受进食的影响抗酸药矿物质和多种维生素:莫西沙星与抗酸药矿物质和多种维生素同时服用会因为与这些物质形成多价螯合物而减少药物的吸收这将导致血浆中的药物浓度比预定值低因此抗酸药抗逆转录病毒和其他含有镁铝和其他矿物质如铁等的制剂需要在口服莫西沙星4小时前或2小时后服用雷尼替丁:与雷尼替丁同时服用不会影响莫西沙星的吸收特性其吸收参数(CmaxTmaxAUC)均提示莫西沙星不受胃酸缺乏的影响钙补充剂:当给予高剂量补充剂时仅观察到吸收率稍有减少而吸收范围保持不变高剂量钙补充剂对莫西沙星的吸收不具有临床意义茶碱:莫西沙星对稳态时茶碱的药代动力学无影响提示莫西沙星对P450酶的1A2亚型无影响当服用莫西沙星治疗时达到稳态的茶碱浓度未升高因此服用莫西沙星时不必调整茶碱的用量华法令:据观察莫西沙星与华法令同时服用未发现对凝血酶原时间和凝血的其他参数有影响口服避孕药:莫西沙星与口服避孕药同时服用未发现有相互作用抗糖尿病药:优降糖和莫西沙星同时服用未发现有相互作用伊曲康唑:莫西沙星与伊曲康唑同时服用时伊曲康唑的药时曲线下面积(AUC)仅少量改变伊曲康唑对莫西沙星的药代动力学无显著性影响当服用伊曲康唑时给予莫西沙星不需要调整剂量反之亦然地高辛:莫西沙星对地高辛的药代动力学没有严重影响反之亦然吗啡:肠外给予吗啡同时服用莫西沙星并不减少口服莫西沙星的生物利用度且Cmax(17%)仅稍有下降普鲁苯辛:在一项观察普鲁苯辛对肾脏排泄功能影响的研究中未发现对莫西沙星的全身清除和肾脏清除有明显影响因此当这两种药同时服用时不必调整剂量炭:同时口服炭及400 mg莫西沙星能减少药物的全身利用在体内能阻止80%药物吸收药物过量时利用活性炭能在吸收早期阻止药物的进一步进入全身系统注意事项1.喹诺酮药物使用可诱发癫痫的发作,因此此类病人服用本品要注意2.本品应避免用QT间期延长的患者。
盐酸左氧氟沙星氯化钠注射液说明书

盐酸左氧氟沙星氯化钠注射液说明书一、药品名称:盐酸左氧氟沙星氯化钠注射液通用名称:左氧氟沙星氯化钠注射液二、成分该注射液主要成分为盐酸左氧氟沙星和氯化钠。
三、适应症1. 适用于敏感菌引起的下呼吸道感染,如呼吸道感染、肺炎等。
2. 适用于敏感菌引起的泌尿系统感染,如尿路感染、膀胱炎等。
3. 适用于敏感菌引起的皮肤和软组织感染。
四、禁忌症1. 对左氧氟沙星、氯化钠或氟喹诺酮类药物过敏的患者禁用本药品。
2. 对左氧氟沙星或其他喹诺酮类药物曾有过严重肝损害反应的患者禁用本药品。
3. 对肾功能严重受损的患者禁用本药品。
五、用法用量1.成人:按体重调整剂量,每日一次或每12小时一次,每次200~400毫克。
2.儿童:按体重调整剂量,每日一次或每12小时一次,每次5~10毫克/千克体重。
六、不良反应使用本药品可能出现的不良反应包括头痛、头晕、恶心、呕吐、腹泻、皮疹等。
少数患者可能出现过敏反应,如荨麻疹、哮喘等。
若出现严重不良反应,应立即停药并就医。
七、注意事项1. 在使用本药品期间,应仔细观察患者的反应,如出现不良反应应及时就医。
2. 使用本药品时应注意肝功能和肾功能,若出现异常应停药并就医。
3. 对于孕妇和哺乳期妇女,应避免使用本药品。
4. 对于老年患者或肝肾功能不全的患者,应调整剂量。
5. 在使用本药品期间需避免过度暴露于阳光下,以免引起光毒性反应。
八、药物相互作用1. 本药品不宜与铁盐、铝镁制剂等同服,以免影响吸收。
2. 本药品与硝酸铋、抗高血压药物、抗酸药物等可能发生药物相互作用,应在医生指导下合理搭配用药。
九、药物贮藏1. 本药品应存放于阴凉干燥处,避免阳光直射。
2. 请将本药品放在儿童无法触及的地方。
十、包装规格盐酸左氧氟沙星氯化钠注射液通常以玻璃瓶密封包装,每瓶容量为20毫升。
每盒内通常包含10瓶注射液。
十一、生产企业本药品的生产企业为xxxx公司。
以上所述是盐酸左氧氟沙星氯化钠注射液的说明书,请在使用前仔细阅读并按照医嘱或说明进行使用。
盐酸莫西沙星氯化钠注射液说明方案
精心整理盐酸莫西沙星氯化钠注射液说明书【药品名称】通用名:盐酸莫西沙星氯化钠注射液商品名:拜复乐?Avelox?英文名:MoxifloxacinHydrochlorideandSodiumChlorideInjection汉语拼音:YansuanMoxishaxingLuhuanaZhusheye本品主要成份为盐酸莫西沙星,化学名为:1-环丙基-7-{(S,S)-2,8-重氮-二环壬-8-基}-6-氟-8-甲氧-1,4-二氢-4-氧-3-喹啉羧酸盐酸盐。
其结构式为:分子式:C21H24FN3O4·HCl分子量:437.9【性状】本品为黄色的澄明液体。
【适应症】成人(≥18岁)上呼吸道和下呼吸道感染,如:以及皮肤和软组织感染。
【规格】250ml∶0.4g莫西沙星,2.0g氯化钠。
【用法用量】给药方法推荐本品的输液时间应为90分钟。
) 剂量范围(成人):推荐剂量为一次0.4g,一日一次()。
疗程:)推荐的总疗程为7~14天。
急性窦炎:77天。
0.4g14天。
给药方法:静脉给药0.4g的时间应为90分钟。
莫西沙星既可以单独给药也可以与一些相容的溶液一同滴注。
下列注射液与莫西沙星注射液的混合液在室温条件下可保持稳定24小时以上,因此被认为可以合并给药:注射用水0.9%氯化钠注射液1摩尔氯化钠注射液5%葡萄糖注射液10%葡萄糖注射液40%葡萄糖注射液20%木糖醇注射液林格氏液乳酸林格氏液Aminofusin10%(生产厂家:Pharmacia&Upjohn)JonosterilD5(生产厂家:FreseniusKabi)若莫西沙星注射液需与其它药物合用,每种药物需单独给药(见不相容性)。
只有澄明的溶液才能使用。
老年人老年人不必调整用药剂量。
儿童莫西沙星对儿童和青少年的疗效和安全性尚未确定。
(见特别提醒和注意事项)肝损害轻度肝功能损伤(Child-PughA,B)者(Child-PughC)的药代动力学数据。
盐酸莫西沙星氯化钠注射液用法用量
如对您有帮助,可购买打赏,谢谢盐酸莫西沙星氯化钠注射液用法用量
导语:注射液在治疗疾病上,都是有很好效果,不过根据自身疾病不同,使用注射液也是不一样的,盐酸莫西沙星氯化钠注射液是很多人不熟悉的,这样的
注射液在治疗疾病上,都是有很好效果,不过根据自身疾病不同,使用注射液也是不一样的,盐酸莫西沙星氯化钠注射液是很多人不熟悉的,这样的药物对疾病治疗有很好帮助,而且它的用量也不是很多,对盐酸莫西沙星氯化钠注射液用法用量都有什么呢,下面就详细的介绍下,使得对这样药物有一些了解。
盐酸莫西沙星氯化钠注射液:
用法用量
给药方法:根据中国健康受试者心脏所能耐受的输液速率以及国内I、II、III期临床研究的结果,推荐本品的输液时间应为90分钟。
(国外推荐0.4g莫西沙星静脉给药的输液时间应大于60分钟。
)
剂量范围(成人):
推荐剂量为一次0.4g,一日一次(一次1瓶,一日一次)。
疗程:
根据症状的严重程度或临床反应决定疗程。
治疗上呼吸道和下呼吸道感染时通常可按照下列疗程:
慢性支气管炎急性发作:5天
社区获得性肺炎:序贯给药(静脉给药后继续口服用药)推荐的总疗程为7~14天。
急性窦炎:7天
治疗皮肤和软组织感染的推荐疗程为7天。
莫西沙星可以在开始治疗时静脉给药,之后再根据患者情况口服片剂给药。
预防疾病常识分享,对您有帮助可购买打赏。
盐酸莫司沙星氯化钠注射液质量标准

盐酸莫司沙星氯化钠注射液质量标准下载提示:该文档是本店铺精心编制而成的,希望大家下载后,能够帮助大家解决实际问题。
文档下载后可定制修改,请根据实际需要进行调整和使用,谢谢!本店铺为大家提供各种类型的实用资料,如教育随笔、日记赏析、句子摘抄、古诗大全、经典美文、话题作文、工作总结、词语解析、文案摘录、其他资料等等,想了解不同资料格式和写法,敬请关注!Download tips: This document is carefully compiled by this editor. I hope that after you download it, it can help you solve practical problems. The document can be customized and modified after downloading, please adjust and use it according to actual needs, thank you! In addition, this shop provides you with various types of practical materials, such as educational essays, diary appreciation, sentence excerpts, ancient poems, classic articles, topic composition, work summary, word parsing, copy excerpts, other materials and so on, want to know different data formats and writing methods, please pay attention!盐酸莫司沙星氯化钠注射液质量标准一、总则本标准规定了盐酸莫司沙星氯化钠注射液的质量要求、检验方法、标志、包装、运输和贮存等。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
盐酸莫西沙星氯化钠注射液说明书【药品名称】通用名:盐酸莫西沙星氯化钠注射液商品名:拜复乐® Avelox®英文名:Moxifloxacin Hydrochloride and Sodium Chloride Injection汉语拼音:Yansuan Moxishaxing Luhuana Zhusheye本品主要成份为盐酸莫西沙星,化学名为:1-环丙基-7-{(S,S)-2,8-重氮-二环[壬-8-基}-6-氟-8-甲氧-1,4-二氢-4-氧-3-喹啉羧酸盐酸盐。
其结构式为:分子式:C21H24FN3O4·HCl分子量:【性状】本品为黄色的澄明液体。
【适应症】成人(≥18岁)上呼吸道和下呼吸道感染,如:急性窦炎,慢性支气管炎急性发作,社区获得性肺炎;以及皮肤和软组织感染。
【规格】250ml∶莫西沙星, 氯化钠。
【用法用量】给药方法:根据中国健康受试者心脏所能耐受的输液速率以及国内I、II、III 期临床研究的结果,推荐本品的输液时间应为90分钟。
(国外推荐莫西沙星静脉给药的输液时间应大于60分钟。
)剂量范围(成人):推荐剂量为一次,一日一次(一次1瓶,一日一次)。
疗程:根据症状的严重程度或临床反应决定疗程。
治疗上呼吸道和下呼吸道感染时通常可按照下列疗程:慢性支气管炎急性发作:5天社区获得性肺炎:序贯给药(静脉给药后继续口服用药)推荐的总疗程为7~14天。
急性窦炎:7天治疗皮肤和软组织感染的推荐疗程为7天。
莫西沙星可以在开始治疗时静脉给药,之后再根据患者情况口服片剂给药。
莫西沙星注射液在临床试验中最多用过14天。
给药方法:静脉给药的时间应为90分钟。
莫西沙星既可以单独给药也可以与一些相容的溶液一同滴注。
下列注射液与莫西沙星注射液的混合液在室温条件下可保持稳定24小时以上,因此被认为可以合并给药:注射用水%氯化钠注射液1摩尔氯化钠注射液5%葡萄糖注射液10%葡萄糖注射液40%葡萄糖注射液20%木糖醇注射液林格氏液乳酸林格氏液Aminofusin10%(生产厂家: Pharmacia&Upjohn)Jonosteril D5 (生产厂家: Fresenius Kabi)若莫西沙星注射液需与其它药物合用,每种药物需单独给药(见不相容性)。
只有澄明的溶液才能使用。
老年人老年人不必调整用药剂量。
儿童莫西沙星对儿童和青少年的疗效和安全性尚未确定。
(见特别提醒和注意事项)肝损害轻度肝功能损伤(Child-Pugh A,B)的患者不必调整莫西沙星的剂量。
目前尚缺乏严重肝功能损伤患者(Child-Pugh C)的药代动力学数据。
肾损害肾功能受损的病人(包括肌酐清除率≤30ml/min/和慢性透析,如血液透析和持续性不卧床腹膜透析的患者无需调整剂量。
种族差异对高加索人、日本人、黑人及其他种族人群进行了可能的种族间差别试验,未发现临床相关的药代动力学差别。
因此,不同种族间不必调整药物剂量。
【不良反应】在莫西沙星的临床试验中,绝大多数的不良反应为轻中度(约90%),由于不良反应导致停用莫西沙星治疗的病人为%,序贯治疗(静脉给药后继续口服用药)为%。
根据莫西沙星的临床试验总结出的常见不良反应(其相关程度分为很可能、可能和无法评估)列表如下:发生率≥1%<10%全身症状:腹痛、头痛、注射部位反应(如水肿/过敏/炎症/疼痛)心血管系统:合并低血钾症患者QT间期延长消化系统:恶心、腹泻、呕吐、消化不良、肝功能化验异常特殊感官:味觉倒错神经系统:眩晕发生率≥%<1%全身症状:乏力、念珠菌病、疼痛、不适、胸痛心血管系统:心动过速、高血压、心悸、QT间期延长、静脉炎(注射部位)消化系统:口干、恶心和呕吐、腹胀、便秘、口腔念珠菌病、食欲下降、口腔炎、胃肠功能失调、舌炎、γGT(γ谷氨酰转肽酶)增高血液和淋巴系统:白细胞减少、凝血酶原减少/国际标准化比值增高、嗜酸细胞增多、血小板增多症代谢和营养:淀粉酶增加骨骼肌肉系统:关节痛、肌肉痛神经系统:失眠、眩晕、神经质、嗜睡、焦虑、震颤、感觉异常呼吸系统:呼吸困难皮肤和附件:皮疹、瘙痒、多汗泌尿生殖系统:阴道念珠菌病、阴道炎发生率≥%<%全身症状:骨盆疼、面部浮肿、背疼、实验室检验异常、过敏反应、腿疼心血管系统:低血压、血管扩张、外周性水肿消化系统:胃炎、舌变色、吞咽困难、黄疸(主要为胆汁淤积性)、腹泻(难辨梭菌)血液和淋巴系统:凝血活酶减少、凝血酶原增加/国际标准化比值降低、血小板减少、贫血代谢和营养:高血糖、高血脂、高尿酸血症、LDH(乳酸脱氢酶)增高(与肝功能检查异常有关)骨骼肌肉:关节炎、肌腱异常神经系统:幻觉、人格解体、紧张、动作失调、激动不安、健忘症、失语症、情绪不稳定、睡眠障碍、语言障碍、思维异常、感觉减退、梦异常、惊厥、精神错乱、忧郁症呼吸系统:哮喘皮肤和附件:皮疹(斑丘疹、紫癜、脓泡)、荨麻疹特殊感官:耳鸣、视觉异常、味觉丧失、嗅觉倒错(包括嗅觉倒错、嗅觉减低及嗅觉丧失)、弱视泌尿生殖系统:肾功能异常(肌酐或尿素升高)上市后报道的不良反应:发生率≥%<%心血管系统:晕厥发生率<%过敏性:过敏反应、过敏性休克(可危及生命)、血管性水肿(包括喉头水肿;潜在生命危险)消化系统:伪膜性结肠炎(在极少数病例伴有危及生命的并发症),肝炎(主要为胆汁淤积性)肌肉骨胳系统:肌腱断裂皮肤和附件:斯蒂文斯-约翰逊综合征(Stevens-Johnson Syndrome)神经系统:精神病反应心血管系统:报道在极少数病例尤其是在有严重的潜在性致心律失常条件的病人出现,包括尖端扭转型室速的室性快速性心律失常和心脏停搏。
未在上述不良反应中列出的认为与药物无关的最常见的实验室参数异常为:血细胞压积增加或减少、白细胞增加、红细胞增加或减少、血糖下降、血红蛋白减少、碱性磷酸酶升高、SGOT/AST(血清谷氨酸草酰乙酸转氨酶/天冬氨酸氨基转移酶)升高、SGPT/ALT(血清谷氨酸丙酮酸转氨酶/丙氨酸氨基转移酶)升高、胆红素升高、尿素升高、肌酐升高、血尿素氮升高。
上述异常是否由该药或治疗时患者状况导致尚属未知。
【禁忌】已知对该注射液的任何成分或其他喹诺酮类药物过敏者。
该注射液禁用于儿童、处于发育阶段的青少年和孕妇。
喹诺酮类已知能大量分布到乳汁中。
临床前实验证实小量的莫西沙星可以分布到人类的乳汁中,尚缺乏哺乳期妇女的数据。
因此,莫西沙星禁用于怀孕和哺乳期的妇女。
【注意事项】使用喹诺酮类药物可诱发癫痫发作,对于已知或怀疑患有可导致癫痫发作或降低癫痫发作阈值的中枢神经系统疾病的病人,应慎用莫西沙星。
由于缺乏肝功能严重损伤(Child-Pugh C)病人使用莫西沙星的药代动力学和药效学的数据,故不推荐该药用于这类病人。
莫西沙星和其他喹诺酮类、大环内酯类抗生素一样,有些患者使用后可出现QT间期延长。
因为缺乏相关的临床资料,该药应避免用于QT间期延长的病人、患有低钾血症病人及接受Ia类(如:奎尼丁,普鲁卡因胺)或III类(如:胺碘酮,索他洛尔)抗心律失常药物治疗的病人。
莫西沙星与下列药合用不排除有延长QT间期的效应:西沙必利,红霉素,抗精神病药和三环类抗抑郁药。
所以,莫西沙星与这些药物合用应慎重。
莫西沙星在致心律失常的条件(如:严重的心动过缓或急性心肌缺血)存在时应慎用。
QT间期延长的数量随着药物浓度的增加而增加。
所以不应超过在90分钟内滴注400mg的推荐剂量和输注速度。
QT间期延长可导致发生室性心律失常包括尖端扭转型室速的危险。
在莫西沙星治疗的超过8000名患者(包括口服和胃肠道外给药)中,无心血管的发病率或死亡率归因于QT间期延长,但某些潜在条件可以增加室性心律失常的危险。
在使用包括莫西沙星的喹诺酮类治疗中有可能出现肌腱炎和肌腱断裂,特别是在老年病人和使用皮质激素治疗的病人中。
一旦出现肌腱疼痛或炎症,患者需要停止服药并休息患肢。
有报导在使用包括莫西沙星等广谱抗生素后出现伪膜性结肠炎,因此,值得高度注意的是,在使用莫西沙星治疗中如患者出现严重的腹泻时,应考虑这个诊断的可能性。
在这种情况下需立即采取适当的治疗措施。
光敏感性:其他喹诺酮类有导致光毒性的报导。
但是,在一项健康志愿者中进行的试验未发现莫西沙星有光过敏情况的出现。
尽管如此,仍应建议病人避免在紫外线及日光下过度暴露。
在有些病例,在首次服用后发生过敏反应和变态反应,应该立即告知医生。
过敏性反应在极少的病例能够在首次服药后导致休克,可能危及生命。
在这些病例应立即停用莫西沙星并给予治疗(如针对休克的治疗)。
不相容性下列注射液与莫西沙星注射液合并用药具有不相容性:10%氯化钠注射液20%氯化钠注射液%碳酸氢钠注射液%碳酸氢钠注射液对驾驶和操纵机器能力的影响在临床试验中,中枢神经系统反应的发生率较低,但病人在驾驶和操作机器前应谨慎观察对药物的反应。
【孕妇及哺乳期妇女用药】孕妇:人类在怀孕期间使用莫西沙星的安全性尚未被证实,儿童服用喹诺酮类药物可引起可逆性关节损伤,但是,这种作用在妊娠用药者的胎儿中尚未见报道。
动物研究显示莫西沙星有生殖毒性,但对人的潜在危险性尚不明确。
因此,妊娠期间不宜使用莫西沙星。
哺乳期妇女:与其它喹诺酮类药物相同,莫西沙星可造成未成年实验动物负重关节的软骨损伤。
临床前研究证实小量的莫西沙星可以分布到人类的乳汁中,尚缺乏应用于哺乳期妇女的数据。
因此,莫西沙星禁用于哺乳期的妇女。
【儿童用药】莫西沙星对儿童和青少年的疗效和安全性尚未确定。
【老年用药】莫西沙星的药代动力学不受年龄的影响。
【药物相互作用】华法林:据观察,莫西沙星与华法林同时用药未发现对凝血酶原时间和凝血的其他参数有影响。
国际标准化比值(INR)的改变:曾有报道患者同时服用抗凝剂和包括莫西沙星在内的抗生素抗凝活性升高。
其危险因素包括感染(及其炎症过程),年龄和患者的一般情况。
尽管莫西沙星和华法林的相互作用在临床试验中未经证实,但应监测INR,如有必要应调整口服抗凝剂的剂量。
地高辛:莫西沙星对地高辛的药代动力学无显著影响,反之亦然。
茶碱:人体外研究数据显示莫西沙星对稳态时茶碱的药代动力学无影响,提示莫西沙星对细胞色素P450酶的1A2亚型无影响。
丙磺舒:在一项观察丙磺舒对肾脏排泄功能的影响的临床研究中未发现丙磺舒对莫西沙星的全身清除和肾脏清除有明显影响。
因此,当这两种药同时使用时不必调整剂量。
抗糖尿病药:未见格列苯脲和莫西沙星间有临床相关的相互作用。
口服避孕药:莫西沙星与口服避孕药同时服用未发生相互作用。
吗啡:胃肠道外给予的吗啡与莫西沙星同时使用,并不减少口服莫西沙星的生物利用度。
伊曲康唑:与莫西沙星同时使用,伊曲康唑的药物暴露(AUC)仅少量改变。
伊曲康唑对莫西沙星药代动力学无显著性影响。