2016ESC心力衰竭指南解读-李永乐
2016ESC急慢性心力衰竭诊治指南

推荐 类别
证据 水平
Ⅰ Ⅰ
C B
心衰合并房颤患者快速心室率处理推荐
房颤导致血流动力学不稳定情况下,推荐紧急电复律 纽约心功能Ⅳ级合并急性心衰发作患者,应考虑静脉推注胺碘酮或西地兰以减慢心室 率。 推荐口服β受体阻滞剂作为纽约心功能Ⅰ—Ⅲ级患者心室率控制一线用药。 纽约心功能Ⅰ—Ⅲ级,经β受体阻滞剂治疗后心室率仍快或β受体阻滞剂不耐受或存在 禁忌症的患者应考虑使用地高辛。 药物治疗无效或不耐受的患者,可考虑行房室结射频消融术。 不推荐使用决奈达隆 纽约心功能Ⅱ—Ⅳ级伴左心收缩功能障碍且无急性失代偿心衰患者房颤节律控制推荐 经优化药物治疗和充分控制心室率治疗,心衰症状和/或体征仍持续存在的患者,可考 虑电复律或药物复律。 经优化药物治疗和充分控制心室率治疗,心衰症状和/或体征仍持续存在的患者,可考 虑行房颤消融 电复律前后可考虑使用胺碘酮维持窦性心律 不推荐纽约心功能Ⅲ—Ⅳ级患者使用决奈达隆 不推荐使用Ⅰ类抗心律失常药物
症状+体征 症状+体征
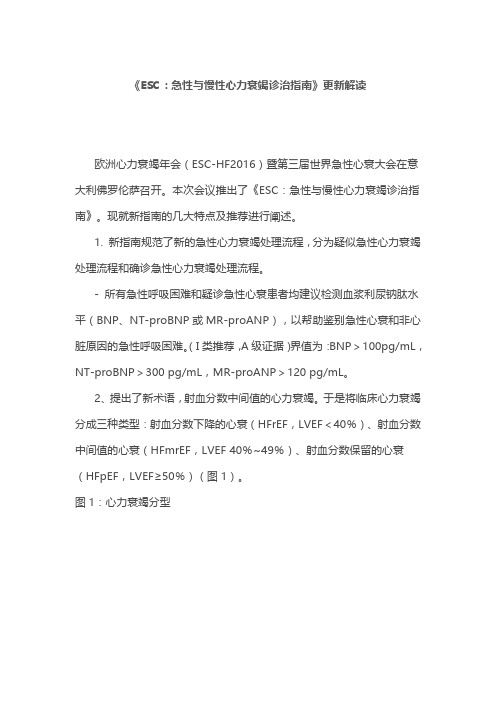
可疑心衰 (非急性发作)
评估心衰可能性 1.冠脉疾病病史(心梗、血运重建) 高血压病史 心脏毒性药物接触史 使用利尿剂 端坐呼吸/夜间阵发性呼吸困难 2.体格检查 肺部啰音 双侧脚踝浮肿 心脏杂音 颈静脉怒张 心尖搏动位置改变 3.心电图 存在任何异常
均不存在
至少一项阳性
临床工作中未常规开 展检测脑钠肽
推荐 类别
证据 水平
Ⅰ Ⅱa Ⅰ
C
B A
Ⅱa
Ⅱb Ⅲ
2016ESC心衰指南

征,患者具有典型的症状(如气
短、踝部水肿和疲乏)和体征 (如颈静脉压升高、肺部湿啰音 和心尖异位搏动)
1. McMurray JJ , et al. Eur Heart J. 2012 Jul;33(14):1787-847. 2. Ponikowski P, et al. Eur Heart J. 2016 May 20. pii: ehw128.
Internal Use Only
指南对预防心衰措施的部分推荐
推荐内容 推荐 级别 证据 水平
推荐治疗高血压,以预防或延缓心衰的发生,延长生命 对于冠心病高危人群,无论是否存在左心室收缩功能障碍,均推荐应用他汀, 以预防或延缓心衰的发生,延长生命 推荐ACEI用于无症状的左室功能障碍且有心梗病史的患者,以预防或延缓心 衰的发生,延长生命 推荐ACEI用于无症状的左室功能障碍且无心梗病史的患者,以预防或延缓心 衰的发生
Internal Use Only
ACEI、β受体阻滞剂、 MRA 在症状性(NYHA II-IV级)HFrEF患者的应用
•
除β受体阻滞剂外,ACEI也被推荐 应用于症状性HFrEF患者的治疗, 以减少心衰住院和死亡风险 除ACEI外,β受体阻滞剂也被推荐 应用于稳定、症状性HFrEF患者的 治疗,以减少心衰住院和死亡风险
Internal Use Only
2016ESC心衰指南更新十大要点:(三)
为预防或延缓心衰的发生,延长生命 推荐治疗高血压 推荐冠心病或冠心病高危人群应用他汀 推荐无症状的左室功能障碍患者应用
推荐三
ACEI
推荐无症状的左室功能障碍和既往有心梗 史患者使用β受体阻滞剂
Ponikowski P, et al. Eur Heart J. 2016 May 20. pii: ehw128.
2016ESC急慢性心衰指南

推荐使用利钠肽来排除心衰,但不用来确诊。
在出现症状前延缓或预防明显心衰的进展或预防死亡
推荐内容 为了预防或延缓心衰的发作和延长寿命推荐治疗高血压。 对于有 CAD 或存在 CAD 高风险的患者,无论其是否存在左室收缩功能不全,为了预防或延缓心 衰的发作和延长寿命,推荐用他汀治疗。 对于吸烟或过量饮酒的人,为了预防或延缓心衰的发作,推荐戒烟咨询和治疗,减少酒精摄入量。 为了预防或延缓心衰的发作,应考虑治疗其他的心衰危险因素(如肥胖,血糖异常)。 为了预防或延缓心衰的发作和延长寿命,应考虑用恩格列净治疗 2 型糖尿病。 推荐用ACEI治疗无症状性左室收缩功能不全并心肌梗死病史的患者,以预防或延缓心衰的发作和延 长寿命。 推荐用ACEI治疗没有心肌梗死病史、存在无症状性左室收缩功能不全的患者, 以预防或延缓心衰的发作。 对于稳定性CAD患者,即使没有左室收缩功能不全,应考虑用ACEI治疗,以预防或延缓心衰的发作。 推荐用β 受体阻滞剂治疗无症状性左室收缩功能不全并心肌梗死病史的患者,以预防或延缓心衰的 发作和延长寿命。 推荐级别 证据水平 I I I IIa IIa I A A C C B A
I
IIa I I
B
A B B
为了预防猝死和延长寿命,对如下患者推荐用 ICD: A)急性心肌梗死后至少40天,缺血性的无症状左室收缩功能不全(LVEF≤30%); B)接受了优化的药物治疗,非缺血性、无症状性扩张型心肌病(LVEF ≤30%);
在出现症状前延缓或预防明显心衰的进展或预防死亡
对于LVEF长期降低的无症状患者,无论病因如何,ACEI 都可降低需要住院的心衰风 险 。β 受体阻滞剂或MRA目前还没有显示出这种效果。 本指南将恩格列净推荐用于 2-型糖尿病患者心衰的一级预防。这基于去年8月公布具 有里程碑意义的EMPA-REG研究。 对于年龄≥40岁、AMI 后,无症状缺血性左室收缩功能不全(LVEF<30%)的患者, 为延长寿命,推荐用植入式心脏复律-除颤器(ICD) 。 在STEMI的最早期,行直接PCI以减少梗死面积,可降低随后LVEF发生显著减少和发 生HFrEF的风险。在一次心梗后,尤其是伴有左室收缩功能不全时,立即启动ACEI、 β 受体阻滞剂和MRA可降低心衰住院率和死亡率,他汀也是如此 。
2016 ESC心衰指南CRT建议解读

新: 以前是 IIa
心衰患者,EF降低,预计高心室起搏%,为了降低心衰恶化风险应该考
虑CRT
新: BLOCK HF
类别 I IIa
证据水平 B B
2016年ESC心衰指南
推荐级别降为IIb
升级为I类,A级
升的依据--BLOCK-HF
• 前瞻性、多中心、随机对照、双盲临床研究 • 目的:评价右室心尖部起搏和双室起搏对心室起搏依赖的轻中度心
Europace (2012) 14, 1490–1497
研究结果
一年期随访超声检查显示: 升级前起搏比例高者具有更好的CRT反应,EF提高也更明显
European Journal of Heart Failure (2014) 16, 1199–1205
研究结果
长期随访显示,研究一级终点全因死亡率及心衰入院复合终点,两组有明显差异, 升级前RV起搏比例高组其预后更好(HR=0.67,P=0.005);单一全因死亡率 终点,起搏比例高组也有降低风险的趋势(HR=0.73,P=0.055)
I A)在慢性HF,自身QRS> 120 ms 和LVEF< 35%, NYHA心功能分级III 和非卧床IV,优化药物治疗,BiV起搏可能接近100%的患者中应该考
IIa
B
虑CRT
新: 以前是 IIb
I B) 如果有不完全的BiV起搏,应该进行房室结消融
IIa
B
2) 心率不能控制考虑进行房室结消融的患者 ,在LVEF降低,因心率
I
A
窦律,QRS≥150ms,非LBBB,EF≤35%(药物优化后)的有症状心衰患者应该考 虑使用CRT改善症状,降低发病率和死亡率。
IIa
B
(完整版)2016ESC急性与慢性心力衰竭诊断与治疗指南

3. 基于心衰概律评估,提出新的非急性期心衰 诊断方法;
指南工作组主席、波兰
4. 建议旨在预防或延缓明显的心衰发展,或预 Piotr Ponikowski教授 防症状出现前的患者死亡;
背景(总结2016ESC新指南的更新及特点)
指南工作组主席、波兰 Piotr Ponikowski教授
内 容(慢性心衰)
概述 定义、病理生理、临床表现 诊断 评估 治疗 小结
概述
自2012年版欧洲心衰指南发布后,4年以来,有多 项大型心衰研究结果问世,为心衰防治带来了新技 术和新思路。
因此,指南撰写小组在汲取了这些重要研究结果, 对指南的各个主要章节都进行了更新或修改。
2016年5月21日~24日,欧洲心力衰竭年会(ESC-HF2016) 暨第三届世界急性心衰大会在意大利佛罗伦萨召开。本次会议
推出了《ESC2016:急性与慢性心力衰竭诊治指南》
背景(总结2016ESC新指南的更新及特点)
1. 提出新术语——射血分数中间值的心衰 (HFmrEF),即HF患者的左室射血分数(LVEF) 范围在40%-49%;
2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
2016 ESC急性与慢性心力衰竭 诊断与治疗指南
心衰诊断与治疗指南
2012年欧洲心衰指南
2013美国心衰诊断与管理指南
2016年ESC心衰指南发表
机制:俯身导致回心血量增加从而加 重心脏负荷。这与心衰「古老」的临床 表现之一,夜间阵发性呼吸困难而端坐 位有所缓解的表现,有异曲同工之妙。
2016年ESC心衰指南

心衰治疗
药物治疗
器械治疗
治疗流程解读
HFrEF治疗流程非常全面,涵盖了药物治疗和非药物治疗
用不同颜色标注了推荐级别,绿色为一级推荐,黄色为IIa级推荐。
存在充血症状和体征的患者,建议使用利尿剂;
经过最佳药物治疗LVEF仍≤35%或有症状性VT/VF病史的患者,推荐植 入ICD。
对于症状性HFrEF患者,首先给予ACEI和β 受体阻滞剂,并强调上调 到基于证据的最大耐受剂量。若无症状说明液体潴留不严重,可适当 考虑减少利尿剂的剂量;若仍有症状且LVEF≤35%,可加用醛固酮受 体拮抗剂(MRA)。
治疗流程解读
若仍有症状且LVEF≤35%,分为以下三种情况: ①若能够耐受ACEI或ARB,可替换为ARNI; ②窦性心律、QRS间期≥130msc,可考虑CRT; ③窦性心律、心率≥70bmp,可加用伊伐布雷定
EMPA-REG研究:与安慰剂组相比,在常规治疗基础上加用钠葡萄 糖共转运体-2(SGLT-2)抑制剂恩格列净可显著降低复合心血管 终点事件发生率。 获益机制:尿中排出体内多余的葡萄糖,通过渗透性利尿作用降 低血压并降低体重。
内容
概述 定义、病理生理、临床表现 诊断 评估 治疗 小结
5. 首个血管紧张素受体脑啡肽酶抑制剂 (ARNIs),Sacubitril /Valsartan(沙库必曲 /缬沙坦 LCZ696)复方制剂适应证的推荐;
6. 心脏再同步化治疗(CRT)适应证的修正;
7. 确定急性心衰患者应尽早接受适宜治疗的 “及时治疗”(time to therapy)理念。
8. 根据是否存在充血/低灌注的急性心衰诊断
对于难治性心衰患者,可考虑地高辛/肼苯哒嗪+硝酸异山 梨醇酯/LVAD,或心脏移植;
《ESC:急性与慢性心力衰竭诊治指南》更新解读
《ESC:急性与慢性心力衰竭诊治指南》更新解读欧洲心力衰竭年会(ESC-HF2016)暨第三届世界急性心衰大会在意大利佛罗伦萨召开。
本次会议推出了《ESC:急性与慢性心力衰竭诊治指南》。
现就新指南的几大特点及推荐进行阐述。
1. 新指南规范了新的急性心力衰竭处理流程,分为疑似急性心力衰竭处理流程和确诊急性心力衰竭处理流程。
- 所有急性呼吸困难和疑诊急性心衰患者均建议检测血浆利尿钠肽水平(BNP、NT-proBNP或MR-proANP),以帮助鉴别急性心衰和非心脏原因的急性呼吸困难。
(I类推荐,A级证据)界值为:BNP>100pg/mL,NT-proBNP>300 pg/mL,MR-proANP>120 pg/mL。
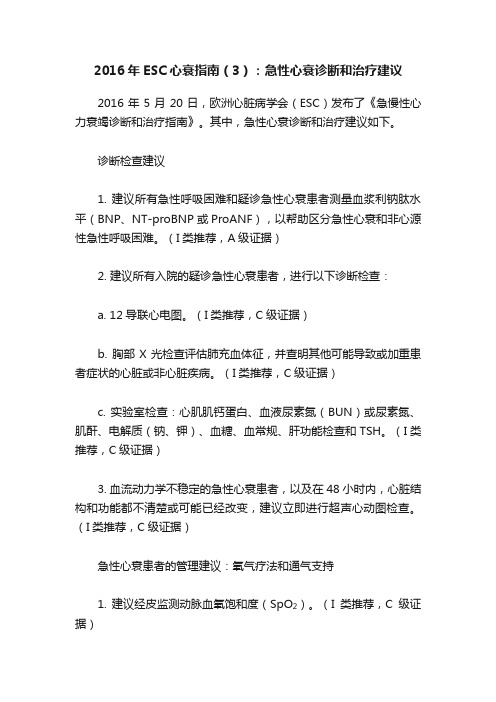
2、提出了新术语,射血分数中间值的心力衰竭。
于是将临床心力衰竭分成三种类型:射血分数下降的心衰(HFrEF,LVEF<40%)、射血分数中间值的心衰(HFmrEF,LVEF 40%~49%)、射血分数保留的心衰(HFpEF,LVEF≥50%)(图1)。
图1:心力衰竭分型3. 疑诊或确诊心衰患者心脏影像学检查的建议:- 疑诊心衰的患者,建议用经胸超声心动图(TTE)检查评估心脏结构和功能,以确定HFrEF、HFmrEF或HFpEF诊断。
(I类推荐,C级证据)- 建议用TTE评估LVEF,以便识别出适合循证药物和装置(ICD、CRT)治疗的HFrEF患者。
(I类推荐,C级证据)。
4. 预防或延缓心衰进展的建议:- 建议治疗高血压,以预防或延缓心衰发生、延长生命。
(I类推荐,A级证据)- 对于无症状左心室收缩功能障碍和有心肌梗死病史的患者,建议使用血管紧张素转换酶抑制剂(ACEI),以预防或延缓心衰发生、延长生命。
(I类推荐,A级证据)- 对于无症状左心室收缩功能障碍和有心肌梗死病史的患者,建议使用β受体阻滞剂,以预防或延缓心衰发生、延长生命。
(I类推荐,B级证据)。
5. 症状性HFrEF患者的药物治疗- 对于症状性HFrEF患者,建议在ACEI基础上应用β受体阻滞剂,以降低心衰住院和死亡风险。
2016ESC急性心衰指南

有些患者,在MCS期间左室发生逆重构和功能改善,可允许移除 LVAD[(“桥接到恢复”(BTR)]。多见急性暴发性但原因可逆的心 衰,如急性重症心肌炎,毒物或药物性心肌病,或围产期心肌病。 对于不太严重的患者,如还没有用正性肌力药物支持的患者,早期植 入心室辅助装置,已在最近的一项试验中得到检验,显示预后比继续 用药物治疗的患者更好。
临时经皮机械循环支持(MCS)治疗获益的证据是有限的。在一篇对 3项随机临床试验的汇总分析中,纳入了经皮MCS与IABP治疗,总共 100例心源性休克患者,经皮MCS似乎是安全的,证实血流动力学更 好,但不改善30天死亡率,且与更多的出血并发症相关。临时经皮 MCS不能推荐作为急性心源性休克已证明或有效的治疗。对选定的患 者,MCS可作为明确治疗的一种桥接。
常规动脉血气检查并不需要,且应限于氧合作用不能通过指脉氧评估的患 者。然而,当需要准确测定O2和CO2分压时,动脉血气分析是有用的。 可接受用静脉血样本检测pH和CO2。 对于非低氧血症的AHF患者,不应常规给氧,因为氧气可引起血管收缩并 降低心输出量。COPD的氧合过度可增加通气-灌注的不匹配,从而抑制 通气并引起高碳酸血症。在氧疗期间,应当监测酸-碱平衡和经皮监测动 脉血氧饱和度。 无创正压通气包括CPAP和双水平气道正压通气( Bi-level PPV )。 Bilevel PPV还支持吸气压力支持,提高每分钟通气量,这对高碳酸血症 (通常多数为COPD)患者,特别有用。 在酸中毒和高碳酸血症的情况下,仍有呼吸窘迫征象,特别是有COPD既 往史或疲劳征象的患者,应当继续用无创通气,最好是用PS-PEEP。 关于麻醉药的副作用应当谨慎,其中丙泊酚能引起低血压并有心脏抑制的 副作用。而咪达唑仑心脏副作用较少,故对于AHF或心源性休克患者属于 首选。
2016ESC急慢性心衰诊断治疗指南解读

射血分数中间范围的心衰(HFmrEF)
心衰分类增加了射血分数中间范围(EF 40-49%)的心衰(HFmrEF) HFmrEF约占心衰群体的10-20%,与HFrEF/HFpEF相比,有着独特的临床、 超声、血流动力学、和生物标记物特征 EF 40-49%患者与EF ≥ 50%患者临床表型不同,潜在治疗效果不同,将 HFmrEF作为一个特殊群体,有助于深入研究其临床特点、病理生理机制和 治疗方法
指南对预防心衰措施的部分推荐 Ponikowski P, et al. Eur Heart J. 2016 May 20. pii: ehw128.
2016ESC心衰指南更新十大要点:(四)
推荐四
• 推荐有症状的HFrEF患者终生应用可改善预后的药物治疗, 包括联合ACEI(如不能耐受ACEI则选用ARB)、β受体阻滞 剂和醛固酮受体拮抗剂(MRA)
ACEI、MRA、β受体阻滞剂可提高患者的生存率,推荐用于所有HFrEF患者的治 疗 根据患者的临床状况酌情使用利尿剂 ACEI和β受体阻滞剂可互补,患者一经确诊为HFrEF,即可开始联用ACEI与β受 体阻滞剂 无证据支持在ACEI之前起始β受体阻滞剂治疗。两者应不分先后,同时启动
MRA:醛固酮受体拮抗剂 Ponikowski P, et al. Eur Heart J. 2016 May 20. pii: ehw128.
ቤተ መጻሕፍቲ ባይዱ
2016ESC心衰指南更新十大要点:(五)
推荐五
• 对既往发生导致血流动力学不稳定的室性心律失常的, LVEF≤35%的症状性(至少给予最优化药物治疗3个月以 上)的心衰患者,推荐植入心律转复除颤器(ICD),以降 低猝死风险和全因死亡率
• 不推荐在心梗后40天内植入ICD,因为此时植入并不能 改善预后
2016 年欧洲急慢性心力衰竭诊治指南资料

2016 年欧洲急慢性心力衰竭诊治指南2016-07-01 09:24 来源:丁香园作者:iang字体大小-|+5 月21 日~24 日,欧洲心力衰竭年会在意大利佛罗伦萨召开,本次会议正式颁布2016 年欧洲心脏病学会(ESC)急性和慢性心力衰竭诊治指南。
与2012 年ESC 急性和慢性心衰指南相比,新指南更新主要包括以下几点:(1)针对左室射血分数位于40%~49% 之间的心衰患者,提出一个全新的概念:射血分数中等范围的心衰;(2)明确指出射血分数降低的心衰(HfrEF)、射血分数中等范围的心衰(HfmrEF)和射血分数保留的心衰(HFpEF)的诊断标准;(3)制定一套新的心衰诊断流程;(4)对预防和延缓临床型心衰发生或死亡作出推荐;(5)对血管紧张素受体- 脑啡肽酶抑制剂——Sacubitril/ 缬沙坦共晶化合物作出推荐;(6)修改了心脏再同步化治疗(CRT) 建议;(7)提出在完善急性心衰相关检查时早期进行合适干预的概念;(8)根据是否存在充血/ 低灌注制定急性心衰诊治结合方案。
下面,让我们来看指南具体内容。
1. 射血分数保留的心衰、射血分数中等范围的心衰以及射血分数降低的心衰三种心衰类型的定义2. 心衰诊断流程3. 可疑或确诊心衰患者心脏影像学检查推荐4. 心衰患者诊断检查推荐5. 预防或延缓临床型心衰发生或死亡的治疗推荐6. 有症状的射血分数降低的心衰患者药物治疗推荐7. 心衰患者植入式心脏复律除颤器(ICD)治疗推荐8. 心衰患者心脏再同步化治疗(CRT)推荐9. 射血分数保留以及射血分数中等范围的心衰的治疗推荐10. 心衰合并房颤治疗推荐11. 症状性心衰合并阵发性或持续性/ 永久性房颤血栓栓塞预防推荐12. 心衰合并室性心动过速治疗推荐13. 心衰合并心动过缓治疗推荐14. 合并稳定型心绞痛症状性(纽约心功能Ⅱ-Ⅳ级)射血分数降低的心衰患者的治疗推荐15. 合并高血压的症状性射血分数降低的心衰患者治疗推荐16. 心衰合并其它合并症的治疗推荐17. 急性心衰检查推荐18. 急性心衰氧气及机械通气治疗推荐19. 急性心衰药物治疗推荐20. 急性心衰患者肾脏替代治疗推荐21. 心源性休克患者管理推荐22. 急性心衰入院患者临床状态监测推荐23. 难治性心衰患者机械循环辅助装置治疗推荐指南中的「彩蛋」:玩味《2016 年欧洲急慢性心衰诊治指南》2016-06-16 12:05 来源:丁香园作者:麦憬霆字体大小-|+看指南,当然最重要的是看指南表格里面的推荐,其直接规范指导临床工作。
【ESC2016】ESC2016急慢性心力衰竭指南最新更新发布

【ESC2016】ESC2016急慢性心力衰竭指南最新更新发布编者按欧洲心脏病学学会(ECS)急慢性心力衰竭诊治指南已经在《欧洲心脏杂志》及《欧洲心力衰竭》杂志发表,并在心力衰竭2016年会及5月份举行的第三届世界急性心力衰竭大会上发布。
昨日,大会发布有关该指南的关键更新信息。
在发达国家中约有1%~2%的成人患有心力衰竭,55岁男性及女性的终身心力衰竭发生风险分别为33%和28%。
住院及稳定/门诊心力衰竭患者未来1年的死亡率可分别高达17%和7%,主要死因为猝死及心力衰竭加重。
首次将LCZ696(sacubitril/缬沙坦)列入指南推荐2016 ESC急慢性心力衰竭诊治指南首次涉及了LCZ696(sacubitril/缬沙坦)这一药物。
该药是一类血管紧张素受体脑啡肽酶抑制剂(ARNIs),曾被PARADIGM-HF研究证实“在符合入选及排除标准的射血分数降低的心力衰竭患者中,其降低死亡及心力衰竭住院风险的作用优于ACEI类药物依那普利”。
指南编写小组主席Piotr Ponikowski认为,指南编写时就有关如何将LCZ696引入到心力衰竭患者的治疗流程中开展了大量讨论。
新指南推荐,符合PARADIGM-HF研究标准的患者应选择LCZ696来替代ACEI类药物,但其在更广泛患者群中的应用仍有待进一步数据的支持。
指南编写小组联合主席Adriaan A. Voors指出,LCZ696在适宜患者中应用对预后有积极影响,但是,其应用还是面临一定挑战,因为患者及医生通常不愿意改变其已经应用了几十年的药物。
实际上,与能使寿命延长几个月的新型抗癌药物相比,换用LCZ696的成本相对较小。
指南新增了射血分数中间值的心力衰竭在有关心力衰竭分类方面,新指南新增了射血分数中间值的心力衰竭[HFmrEF,即左室射血分数(LVEF)为40%~49%的心力衰竭],将心力衰竭分为射血分数降低的心力衰竭(HFrEF即LVEF<40%的心力衰竭)、HFmrEF和射血分数保留的心力衰竭(LVEF≥50%的心力衰竭)三大类。
2016年ESC心衰指南(3):急性心衰诊断和治疗建议
2016年ESC心衰指南(3):急性心衰诊断和治疗建议2016年5月20日,欧洲心脏病学会(ESC)发布了《急慢性心力衰竭诊断和治疗指南》。
其中,急性心衰诊断和治疗建议如下。
诊断检查建议1. 建议所有急性呼吸困难和疑诊急性心衰患者测量血浆利钠肽水平(BNP、NT-proBNP或ProANF),以帮助区分急性心衰和非心源性急性呼吸困难。
(I类推荐,A级证据)2. 建议所有入院的疑诊急性心衰患者,进行以下诊断检查:a. 12导联心电图。
(I类推荐,C级证据)b. 胸部X光检查评估肺充血体征,并查明其他可能导致或加重患者症状的心脏或非心脏疾病。
(I类推荐,C级证据)c. 实验室检查:心肌肌钙蛋白、血液尿素氮(BUN)或尿素氮、肌酐、电解质(钠、钾)、血糖、血常规、肝功能检查和TSH。
(I类推荐,C级证据)3. 血流动力学不稳定的急性心衰患者,以及在48小时内,心脏结构和功能都不清楚或可能已经改变,建议立即进行超声心动图检查。
(I类推荐,C级证据)急性心衰患者的管理建议:氧气疗法和通气支持1. 建议经皮监测动脉血氧饱和度(SpO2)。
(I类推荐,C级证据)2. 应考虑测量静脉血的血液酸碱度和二氧化碳张力(可能包括乳酸),特别是急性肺水肿或慢性阻塞性肺病(COPD)史的患者。
心源性休克患者,优选动脉血。
(IIa类推荐,C级证据)3. 急性心衰和SpO2<90%或动脉血氧分压(PaO2)<60 mmHg (8.0 kPa)的患者,建议应用氧气疗法,以纠正低氧血症。
(I类推荐,C级证据)4. 呼吸窘迫(呼吸频率>25次/分,SpO2<90%)的患者,应考虑尽快无创正压通气(CPAP、BiPAP),以缓解呼吸窘迫和减少气管插管率。
由于无创正压通气可降低血压,低血压患者应谨慎使用。
无创正压通气时应定期监测血压。
(IIa类推荐,B级证据)5. 如果患者出现呼吸衰竭,导致低氧血症(PaO2<60 mmHg(8 kPa))、高碳酸血症(PaCO2 > 50 mmHg(6.65 kPa))和酸中毒(pH<7.35),建议插管。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
What is new?
2012 ESC HF Guidelines: Excellent starting point Space limitations: reduce “textbook knowledge” Further improve clinical applicibility New definition and classification HFrEF/HFmrEF/HFpEF New diagnostic algorythms for acute and chronic HF New therapeutic algorythms for acute and chronic HF Expand chapters on co-morbidities and multidisciplinary care Updated recommendations based on new evidence
/guidelines
5
第一部分
• 定义和分类 • 诊断流程:
– 首先评估心衰概率 – 然后检查 (NT-pro)BNP 和超声心动图 – 诊断过程中和之后一直要考虑病因
• 合并症、运动和多学理科管理的重要性
Definition
• HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral oedema) caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress
2016ESC心力衰竭指南解读
天津医科大学总医院
李永乐
Available at..
/Guidelines-&-Education/Clinical-PracticeGuidelines/Acute-and-Chronic-Heart-Failure
/guide conditions
- Hypertension
Arrhythmias
- Tachyarrhythmia
- Valvular defects - Bradyarrhythmia - Structural Myocardial defects During/after - Pericardial and diagnosis: always consider aetiology endomyocardial abnormalities - High Output states - Volume overload
/guidelines
Therapeutic algorithm for a patient with symptomatic HFrEF
/guidelines
ESC Heart Failure Guidelines: Take-home summary
HFpEF
symptoms (+/-signs) LVEF≥50%
1.Elevated (NT-pro) BNP 2.Relevantstructural heart disease(LVH or LAE)+/-diastolic dysfunction
/guidelines
yes ECHOCARDIOGRAPHY
HF unlikely: consider other diagnosis
normal
If HF confirmed (based on all available data): determine aetiology and start appropriate treatment
3
In the year 2016,… by applying all evidence-based discoveries, heart failure is becoming a preventable and treatable disease.
/guidelines
/guidelines
病因的识别非常重要
Diseased myocardium
- Ischemic heart disease
Toxic Damage Immune mediated Inflammtory damage Infiltration Metabolic derangements Genetic Abnormalities
Assessment of natriuretic peptides not routinely done in clinical practice
≥1 present
all absent
no
NATRIURETIC PEPTIDES •NT-proBNP ≥125 pg/mL •BNP ≥35 pg/mL
/guidelines
心衰患者运动和多学科管理
第二部分
• 预防和延缓心衰并延长生命的处理 • 使用降低死亡率的药物
• HFrEF的治疗流程
• ICD • CRT • HFmrER and HFpEF治疗建议 • 急性心竭的初始管理
• 急性心衰早期根据临床情况的处理流程
/guidelines
ESC Heart Failure Guidelines: Take-home summary
2. Implement life-saving pharmacotherapy in patients with symptomatic HFrEF, containing a combination of an ACE-I (or ARB if ACE-I not tolerated), a β-blocker and a MRA. If a patient still remains symptomatic sacubitril/valsartan is recommended to replace ACE-I. Use diuretics in order to improve symptoms and exercise capacity in patients with signs and/or symptoms of congestion.
-
Angina Cachexia and sarcopenia Cancer Central nervous system Diabetes Erectile dysfunction Gout and arthritis Hypo- hyperkalemia Hyperlipidemia Hypertension Iron deficiency and anemia Kidney dysfucntion Lung disease Obesity Sleep disordered breathing Valvular heart disease
/guidelines
9
PATIENT WITH SUSPECTED HF (non-acute onset)
ASSESSMENT OF HF PROBABILITY
1. Clinical history; 2. Physical examination; 3. ECG
/guidelines
New Classification of Heart Failure
HFrEF
Symptoms (+/-signs) LVEF<40%
HFmrEF
symptoms (+/-signs) LVEF40-49%
1.Elevated (NT-pro) BNP 2.Relevant structural heart disease(LVH or LAE)+/-diastolic dysfunction
PATIENT WITH SUSPECTED HF (non-acute onset) ASSESSMENT OF HF PROBABILITY
1. Clinical history: History of CAD (MI, revascularization) History of arterial hypertension Exposition to cardiotoxic drug/radiation Use of diuretics Orthopnoea / paroxysmal nocturnal dyspnoea 2. Physical examination: Rales Bilateral ankle oedema Heart murmur Jugular venous dilatation Laterally displaced/broadened apical beat 3. ECG: Any abnormality
ESC Heart Failure Guidelines: Take-home summary
1. To prevent or delay onset of HF and prolong life: • treatment of arterial hypertension, • use of statins in patients with or at high risk of CAD, • use of ACE-I in patients with asymptomatic left ventricular dysfunction • beta-blockers in those with asymptomatic LV dysfunction and a history of myocardial infarction are recommended.