缺血性脑血管病二级预防
缺血性脑血管病CISS分型治疗及二级预防
缺血性脑血管病CISS分型治疗及二级预防
缺血性脑血管病(CISS)是一种常见的神经系统疾病,其主要病理生理过程是血管壁的损伤和通透性增加,导致脑血管内和/或外的血液流出,进而导致脑组织缺血、缺氧和坏死。
CISS通常包括脑梗死和脑缺血(蛛网膜下腔出血、颅内出血、蛛网膜下腔积液等),是造成残疾和死亡的主要原因之一。
CISS的分型包括大血管病、小血管病和心源性栓塞三种类型。
不同类型的CISS需要不同的治疗方法和二级预防措施。
大血管病包括大脑血管内膜增厚、动脉硬化和颅内动脉粥样硬化。
治疗方式主要包括改变生活方式、药物治疗和手术治疗。
改变生活方式包括戒烟、减肥、控制高血压、控制高血脂和控制糖尿病等。
药物治疗主要包括抗血小板药物如阿司匹林、氯吡格雷和替格瑞洛等以及抗凝药物如华法林和达比加群酮等。
手术治疗主要包括颈动脉内膜剥除术、颅内动脉球囊扩张术、血管搭桥术等。
心源性栓塞包括心房颤动、心脏瓣膜病和心脏血栓。
治疗方式主要包括药物治疗和手术治疗。
药物治疗主要包括抗血小板药物、抗凝药物、利尿剂和心血管药物等。
手术治疗主要包括心脏瓣膜置换术、心脏瓣膜修复术和心房颤动消融术等。
对于不同类型的CISS,我们需要根据具体情况选择相应的治疗方法和二级预防措施。
更重要的是做好日常的健康管理,改变不良的生活方式,及时发现并控制高危因素,预防CISS的发生和复发。
缺血性脑血管病CISS分型治疗及二级预防

缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病是指脑动脉或颅内小血管阻塞或狭窄引起的大脑缺血综合征。
CISS (Chinese Ischemic Stroke Subclassification)分型是对缺血性脑血管病进行分类的一种方法,通过不同的分型可以指导治疗和二级预防措施的选择。
CISS分型将缺血性脑血管病分为5个亚型,分别是大动脉粥样硬化型(Large-Artery Atherosclerosis,LAA)、心源性栓塞型(Cardioembolism,CE)、小血管病变型(Small-Artery Disease,SAD)、其他特殊原因导致的缺血性脑血管病(Other Cause),以及未确定原因型(Undetermined Cause)。
对于不同的CISS分型,治疗和二级预防的策略也不同。
对于大动脉粥样硬化型,治疗的目标是控制动脉粥样硬化的进展,防止新的血栓形成。
常用的治疗措施包括抗血小板药物(如阿司匹林、氯吡格雷)、降压治疗、血脂调节药物(如他汀类药物)、戒烟、控制血糖等。
心源性栓塞型的治疗和预防重点在于抑制心房颤动、预防栓塞形成。
常用的治疗措施包括抗凝治疗(如华法林)、抗血小板药物、控制高血压和糖尿病等基础疾病。
对于小血管病变型,治疗的关键在于改善微循环和防止再次发作。
常用的治疗措施包括抗血小板药物、降压治疗、血脂调节药物、抗血小板药物等。
其他特殊原因导致的缺血性脑血管病的治疗和预防根据具体原因制定。
如有心脏瓣膜病变导致血栓形成,则需要行心脏手术治疗或抗凝治疗。
未确定原因型缺血性脑血管病的治疗和预防依然是一个难题,需要进一步研究和探索。
治疗和预防缺血性脑血管病的关键在于防止血栓形成、改善血液循环、控制基础疾病等。
具体的治疗方案应根据患者的具体情况制定,包括年龄、性别、病史、病情严重程度等因素的考虑。
在制定治疗策略时,应个体化治疗,以达到最佳的治疗效果。
二级预防措施也非常重要,包括控制血压、血糖、血脂、戒烟、适度运动等。
缺血性脑血管病二级预防浅述
脑 血 管 病 的预 防要 分 一 级 预 防 、二 级 预 防 。一 级 预 防就是要始终保 持健康体质 和 良好 的精神状态 。二级预
防即预 防中风 的复发 。对 于高血压脑 出血 的预防 ,控制 血压是有效 的方法 ;对缺血性脑 血管病复发的预防 ,要 实行个体化治疗 ,也就是因人而宜 。 1 二 级 预 防 的 重 要 性 缺 血 性 中 风 占所 有 类 型 中风 的 8 %左 右 。流 行 病 学 5 调查发现 ,我 国近年来 出血性 中风 的发病率 明显 下降, 缺血性 中风则明显上升。 复发性 中风 占所有中风 的1 / 4左 右 ,中风存 活者在 6个月内的复发率为 88 .%,5年 内为
第 8卷第 6期 总第 8 6期  ̄ O- O年三 月・ - 下半 月刊
◎
李
现 N DD擞 I远O SUF TCC AA 息 代T N程 CI EO
缺 血 性 脑 血 管 病 二 级 预 防 浅 述
松 黑龙 江省双城 市人 民医院急救 中心 ( 5 10 10 0 )
关键 词 :缺血 性脑 血管 病 ;治未 病 ;二级 预防 中医养 生学 d i 036 0i n17—792 1.614 o :1.99 .s. 22 7. 00.0 s 6 0 文章 编号 : 17-7 9 (00 0—1 1 1 622 7 2 1 )一602 ・ 0
再次梗塞 。
脑 组织代谢和促进神经 功能恢复的药物 。②进行正规的 语音功能康复训练 、肢体 功能锻炼 等。康复治疗对 缺血 性 中风 很重要 康 复 治疗 开始 的早晚对病 人 日后 的病 情 恢复关系密切 ,只要生命体征稳定 ,神经损 害症状 不再 发展 ( 常在病 发后第 四天 )就可开始康 复治疗 。这对 通 防止肢 体瘫痪 、关节僵硬 、肌 肉挛缩 ,促使肢体功 能的 恢 复在某 种意义上说 比药物还重要 。康 复治疗 的持续 时 间要长 ,病人 患病后动 与不动其后果很不一样 ,有些病
二级预防2 (2)

郑州大学第一附属医院神经内科
缺血性脑血管的二级预防
背景
概念及目的 如何进行二级预防
脑血管病的特点
发病率高:我国各地年均发病率为2 19/100万。 我国每年有200多万人发生脑血管病。 死亡率高:我国脑血管病死亡率为116/10万,占 全部死因的第二位。 致残率高:脑血管病经抢救存活者中,50%~ 80%留下不同程度的致残性后遗症 。 复发率高:脑血管病经抢救治疗存活者中,在5 年内约有20%~47%的复发率而在 1年内复发的 最多。 并发症多:感染、褥疮等。
1
粘附
3
聚集
Fibrinog en
Activated Gpllb/llla
Platelets Collagen Gpla/lla bind
von Williebrand Factor/Gplb bind
Lipid core
2
Thrombin ADP 5 HT TXA2
激活
4
血小板栓子
Kumar A et al. Exp Opin Invest Drugs. 1997;6:1257–1267.
大多数慢性高血压病人应该在几周内逐渐降低血压至目标水平, 这样对远期事件的减低有益。
2005年《中国高血压防治指南》
推荐应用长作用制剂,其作用可长达24小时,每日服用 一次,这样可以 减少血压的波动、降低主要心血管事件的发
生危险和防治靶器官损害,并提高用药的依从性。强调长期有 规律的抗高血压治疗,达到有效、平稳、长期控制的要求。 根据基线血压水平、有无靶器官损害和危险因素,选用单药治 疗或联合治疗
因此,卒中患者降压需平稳,以减少血管损害 与事件风险
高血压和卒中二级预防
缺血性脑血管病二级预防继续教育答案
缺血性脑血管病二级预防继续教育答案1、(单选题)非心源性短暂性脑缺血发作的患者应该首选用哪种药物预防卒中:A .阿司匹林B .氯吡格雷C .银杏叶片D .西洛他唑E .华法林2、(单选题)患者武某,男,49岁,突发头晕、视物旋转、伴恶心呕吐1.5小时入院,急诊头颅CT排除出血,考虑后循环脑梗死,行动脉溶栓治疗,应该何时给他应用抗血小板药物:A .立即给予B .12小时以后C .24小时以后D .48小时以后E .72小时以后3、(单选题)刘女士,55岁,半年内出现3次突然不能言语,每次持续30分钟左右,第3次伴右侧肢体麻木,既往有房颤病史,神经系统检查正常,最可能诊断是A .癫痫B .偏头痛C .颈椎病D .短暂性脑缺血发作(TIA)E .颅内肿瘤4、(单选题)患者马先生,65岁,以急性脑梗死入院,生化检查示:低密度脂蛋白胆固醇2.75 mmol/L,高密度脂蛋白胆固醇2.03mmol╱L ,丙氨酸氨基转移酶56 IU╱L,天冬氨酸氨基转移酶33 IU╱L,适合该患者的降脂治疗策略是:A .不需服用降脂药物B .阿托伐他汀5mg/dC .阿托伐他汀10mg/dD .瑞舒伐他汀5mg/dE .瑞舒伐他汀10mg/d5、(多选题)患者,男性,78岁,既往有吸烟史50年,40支/日,高血压病史30年。
患者入院前3日无明显诱因出现左侧肢体无力,不能持物及行走。
血管超声示双侧颈内动脉粥样硬化斑块形成,右侧椎动脉狭窄约40%。
头CT示多发脑梗死。
该患者脑梗死的可控危险因素包括:A .吸烟B .双侧颈内动脉粥样硬化C .高血压D .年龄78岁E .椎动脉狭窄。
中国缺血性脑卒中二级预防指南
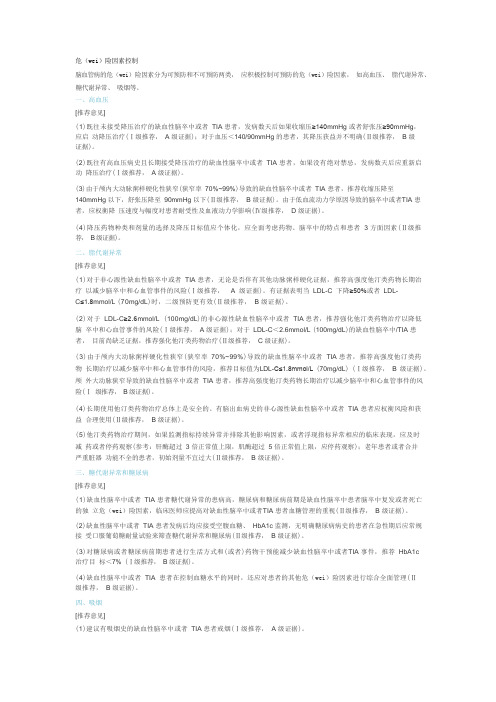
危(wei)险因素控制脑血管病的危(wei)险因素分为可预防和不可预防两类,应积极控制可预防的危(wei)险因素,如高血压、脂代谢异常、糖代谢异常、吸烟等。
一、高血压[推荐意见](1)既往未接受降压治疗的缺血性脑卒中或者TIA 患者,发病数天后如果收缩压≥140mmHg 或者舒张压≥90mmHg,应启动降压治疗(Ⅰ级推荐,A 级证据);对于血压<140/90mmHg 的患者,其降压获益并不明确(Ⅱ级推荐, B 级证据)。
(2)既往有高血压病史且长期接受降压治疗的缺血性脑卒中或者TIA 患者,如果没有绝对禁忌,发病数天后应重新启动降压治疗(Ⅰ级推荐,A 级证据)。
(3)由于颅内大动脉粥样硬化性狭窄(狭窄率70%~99%)导致的缺血性脑卒中或者TIA 患者,推荐收缩压降至140mmHg 以下,舒张压降至90mmHg 以下(Ⅱ级推荐,B 级证据)。
由于低血流动力学原因导致的脑卒中或者TIA 患者,应权衡降压速度与幅度对患者耐受性及血液动力学影响(Ⅳ级推荐, D 级证据)。
(4)降压药物种类和剂量的选择及降压目标值应个体化,应全面考虑药物、脑卒中的特点和患者 3 方面因素(Ⅱ级推荐,B 级证据)。
二、脂代谢异常[推荐意见](1)对于非心源性缺血性脑卒中或者TIA 患者,无论是否伴有其他动脉粥样硬化证据,推荐高强度他汀类药物长期治疗以减少脑卒中和心血管事件的风险(Ⅰ级推荐, A 级证据)。
有证据表明当LDL-C 下降≥50%或者LDL-C≤1.8mmol/L (70mg/dL)时,二级预防更有效(Ⅱ级推荐, B 级证据)。
(2)对于LDL-C≥2.6mmol/L (100mg/dL)的非心源性缺血性脑卒中或者TIA 患者,推荐强化他汀类药物治疗以降低脑卒中和心血管事件的风险(Ⅰ级推荐, A 级证据);对于LDL-C<2.6mmol/L (100mg/dL)的缺血性脑卒中/TIA 患者,目前尚缺乏证据,推荐强化他汀类药物治疗(Ⅱ级推荐,C 级证据)。
缺血性脑血管病和短暂性脑缺血的二级预防
脂代谢异常
目前常用调脂药物
目前常用调脂药物
主要作用 降胆固醇 (TC) 药名 考来烯胺 考来替泊 普罗布考 弹性酶 商品名 消胆胺 降胆宁 丙丁酚 舒降之 普拉固 来适可 阿乐/ 立普妥 常用量及用法 4-5g/次 口服 1-6次 10g/次 口服 2次 0.5g/次 口服 2次 300单位/次口服3次 每日晚饭后 : : : 主要副作用 恶心便秘 恶心便秘 恶心腹胀Q-T延长
同ACEI抑制剂
氯沙坦 50-100mg 1次/日 缬沙坦 80-160mg 1次/日 厄贝沙坦150mg 1次/日
表-2
推荐意见: 1、对于缺血性脑卒中TIA,建议进行抗高 血压治疗,以降低脑卒中和其他血管事件 复发的风险(Ⅰ级推荐,A级证据)。 在参考高龄、基础血压、平时用药、可耐 受性的情况,降压目标一般应该达到 ≤140/90mmhg,理想应该到达 ≤130/80mmhg(Ⅱ级推荐,B级证据)。
TIA症状:一般认为单纯性眩晕、头痛、尿 便失禁、EP、意识障碍、跌倒发作、记忆 障碍(短暂性全面遗忘综合症可部分为TIA) 不能诊断为TIA。
一般判断,一次TIA后一月内发生卒中危险 约4-8%,一年内约12-13%,5年内可达 24-29%。前循环TIA伴有颈动脉狭窄70% 的人预后不佳,2年内发生卒中几率是40%。 后循环TIA发生脑梗死比例较少。
一般认为年龄>70岁,糖尿病史、 TIA>10min,有肢体无力和障碍者,发生 卒中可能性大。
人们最近试图对TIA重新定义,2002年TIA 工作组的Albers教授提示(N.Engl.J Med):TIA是短时间发作的神经功能障碍, 由脑局灶性或视网膜缺失所致,症状在1h 内,并没有急性脑梗死的证据。
缺血性脑血管病CISS分型治疗及二级预防

缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病是指脑血管病的一种类型,它是由于脑动脉供血不足引起的脑组织缺氧缺血引起的疾病。
在缺血性脑血管病的治疗和预防中,CISS分型是一种常用的分类方法,根据病情划分为四个级别:C型、I型、S型和S型加重型。
下面将介绍缺血性脑血管病CISS分型的治疗及二级预防措施。
治疗:1. C型: C型是指缺血性脑血管病的早期阶段,治疗的重点是控制危险因素,包括高血压、高血脂、高血糖等。
首先要进行体检,核实高血压、高血脂等情况,然后进行适当的药物治疗,如降压药、降脂药等。
要进行生活方式的调整,包括戒烟、减少饮酒、控制体重等。
2. I型: I型是指缺血性脑血管病的轻度损伤阶段,治疗的重点是改善脑血管功能,缓解症状。
药物治疗方面,可以使用抗血小板药物,如阿司匹林、氯吡格雷等,以防止血小板凝聚,改善脑血液循环。
还可以使用脑血管扩张药物,如丙戊酸等,以增加脑血流量。
还可以进行物理治疗,如理疗、针灸等,以增加脑血流。
3. S型: S型是指缺血性脑血管病的中度损伤阶段,治疗的重点是控制病情发展,减少并发症。
药物治疗方面,除了使用抗血小板药物和脑血管扩张药物外,还可以使用脑保护剂,如脉络酸和丙戊酸钠等,以保护脑细胞免受损伤。
还可以进行康复训练和心理疏导,以提高患者的神经功能和心理状态。
二级预防:除了治疗阶段的措施外,二级预防措施是指在缺血性脑血管病发生后,为了预防再发和并发症的措施。
主要措施如下:1. 控制危险因素: 患者要继续控制高血压、高血脂、高血糖等危险因素,坚持规律的用药、定期复查,保持血压、血脂、血糖在正常范围内。
2. 正常生活: 患者要保持正常的生活作息,合理安排工作和休息时间,避免过度劳累和精神紧张,保持良好的心理状态。
3. 膳食调理: 患者要选择低盐、低脂、低糖的膳食,多吃新鲜蔬菜和水果,限制高热量、高脂食物的摄入。
4. 动态监测: 对于有再发风险的患者,需要定期进行脑血管超声、脑血流动力学监测、心电图等检查,以及定期复查血压、血脂、血糖等指标。
缺血性脑血管病CISS分型治疗及二级预防
缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病(cerebral infarction,CI)是指由于脑动脉栓塞或缺血性血管痉挛所引起的脑血流灌注不足导致脑组织缺血坏死的病变。
CI是一种常见的脑血管疾病,发病率和死亡率较高,严重影响患者的生活质量。
因此,早期确诊、及时治疗和科学管理已成为缺血性脑血管病治疗及二级预防的核心。
CISS分型是根据脑梗死的病变部位和大小对患者进行分型,根据分型制定相应的治疗方案,提高治疗效果和预后。
CISS分型包括5型:局灶型(LAA)、小血管型(SVO)、心源型(CE)、其他特殊型(OTS)和未分类型(UC)。
据临床研究,不同类型的CISS患者治疗方法各异,预后差异明显。
局灶型是指缺血性脑血管病患者的病变在一个颅内动脉分支或者一处脑区,感染范围较小。
LAA患者治疗方案应以降低血压、血脂和血糖等体内的风险因素为主,包括药物治疗和非药物治疗。
使用抗血小板药物和抗凝血药物有助于减少动脉栓塞的发生,协同使用利尿剂、钙通道阻滞剂、ACEI或ARB等药物有助于降低血压、抗炎和保护血管内皮。
LAA患者患有合并症,如糖尿病等,在治疗中需特别关注并加以控制。
小血管型是指脑梗死病变范围较小,多见于小动脉、细小分支颅内和脑外动脉,通常是由小血管闭塞、痉挛或微栓子所引起。
对于SVO患者,可采用抗凝、抗血小板和溶栓治疗,以及使用钙通道阻滞剂、ACEI和ARB等药物降低血脂、血压。
此外,SVO患者饮食上应注意控制油脂和钠的摄入,避免过度劳累。
心源型是指脑血管病变是由于心血管系统病变而引发,大多数心源型患者同时存在其他心血管疾病如冠心病、心律失常等。
治疗心源型患者需采用心血管药物治疗,包括β受体拮抗剂、钙通道阻滞剂和ACEI等,同时还需要控制高血压和高血糖等风险因素。
对于其他特殊型和未分类型患者,需进行深入的病因学检查和治疗,以便明确诊断和制定合理的治疗方案。
此外,对于所有CISS患者,二级预防非常重要。
中国缺血性卒中和短暂性脑缺血发作二级预防指南2022

中国缺血性卒中和短暂性脑缺血发作二级预防指南2022 缺血性卒中和短暂性脑缺血发作(TIA)是全球频发的脑血管疾病,严重影响各国国民的健康。
国家卫生健康委员会(NHC)于2022年出台了《中国缺血性卒中和短暂性脑缺血发作二级预防指南》,以改善中国国民的预防水平,降低缺血性卒中和短暂性脑缺血发作发病率。
《中国缺血性卒中和短暂性脑缺血发作二级预防指南》起步于血压控制和血脂治疗,包括认识患者高血压、高血压血糖、脂肪调节等方面的重要性,以及预防措施的重要性,包括饮食、运动和戒烟戒酒等。
此外,《中国缺血性卒中和短暂性脑缺血发作二级预防指南》还提出了以下的建议:1、励高危人群进行血压控制、血脂控制和血糖控制,以预防血液黏滞和肥胖,减少卒中患者的几率。
2、议患者积极采取饮食改变,健康饮食例如多吃鱼、蔬菜等,同时少吃高脂肪、高糖食物,还可以与服用药物一起控制血糖水平,减少TIA的发病率。
3、烈建议患者积极锻炼,增强体质、改善血液循环,以及减少肥胖等疾病的发病率。
4、烈反对吸烟、过量饮酒,积极推动健康生活方式,以最大限度减少缺血性卒中和TIA的发病率。
《中国缺血性卒中和短暂性脑缺血发作二级预防指南》一方面应充分发挥政府的指导作用,另一方面,应当积极鼓励和引导患者和他们的家人以及社会力量,以最大限度地改善病人的健康水平,降低缺血性卒中和短暂性脑缺血发作的发病率。
此外,政府应当加大对患者高血压、高脂血症和糖尿病等慢性病进行科学有效的治疗,也加强监督,以确保早期检测和及时有效的治疗。
在制定《中国缺血性卒中和短暂性脑缺血发作二级预防指南》的过程中,我国现有的TIA治疗机构应当更好地推广和实施二级预防措施,与政府的行动和合作,完善普及健康教育,提高脑血管疾病的预防水平和质量。
政府还应当促进医疗机构技术和设备的升级,便于病人早发现、早治疗,把疾病控制在较低水平。
《中国缺血性卒中和短暂性脑缺血发作二级预防指南》发布后,我国在疾病的防治上取得了重大的进步,这将有助于降低缺血性卒中和TIA的发病率,减少国民健康水平的下降,促进中国健康中国的建设。
缺血性脑血管病CISS分型治疗及二级预防

缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病(ischemic cerebrovascular disease)是指因各种原因导致脑部缺血性损害的疾病,主要表现为短暂性脑缺血发作和脑梗死。
CISS分型是世界卫生组织推出的缺血性脑血管病的分型标准,根据颅内、颅外和深部小动脉受损程度分为四型:C型、I 型、S型和SS型。
本文将介绍CISS分型的治疗及二级预防。
C型最常见的临床表现为大脑皮质缺血性病变,一般表现为偏瘫、失语、失认、失读、失写、空间定向障碍等症状。
治疗方法主要包括药物治疗和物理治疗。
药物治疗可使用抗血小板药物、抗凝药物、降脂药、调节免疫系统等。
物理治疗包括针灸、理疗、康复训练等,早期进行运动康复可减轻后遗症。
I型主要表现为颈内动脉中段狭窄或闭塞引起的缺血性病变,病情较C型严重。
治疗方法也包含药物治疗和物理治疗,但更加注重手术治疗,可进行颈动脉内膜剥脱术、支架植入术、颈内动脉外科手术等。
S型主要表现为小动脉硬化和致病菌感染导致小血管阻塞和微血管痉挛。
治疗方法主要包括血液液流变学、营养治疗等保护性治疗和中药治疗,如清热解毒、活血化瘀等。
SS型为CISS分型中最严重的一种类型,表现为大面积脑缺氧性损害。
治疗主要针对病因进行治疗,如降低血压、预防心脏病等。
同时进行神经强化治疗,包括康复训练、口服神经营养药物等,以抗氧化、清除自由基等措施保护脑神经细胞,加快康复。
二级预防对CISS分型缺血性脑血管病患者,必须强调二级预防,以预防复发及减轻后遗症。
营养、运动和心理保健很重要。
口服阿司匹林、复方丹参片等药物,预防血栓形成及抗血小板聚集。
戒烟、限酒、减肥,降低高脂、高蛋白饮食,降低脂蛋白水平。
控制高血压、糖尿病、高血脂等基础疾病,常规体检,防止心脑血管疾病并发症。
定期进行体检和脑血管影像学检查,如颈动脉彩色多普勒和头颅MRI等,早发现早治疗。
总之,对CISS分型缺血性脑血管病的治疗和二级预防应综合考虑病因、病情、年龄、基础疾病等因素,根据具体情况进行个体化治疗,并且尽量保持良好的生活方式和心理状态。
缺血性脑血管病CISS分型治疗及二级预防

缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病(Cerebral Infarction)是指因脑血管疾病引起,致使某一部分大脑皮层功能丧失,同时具有内脏或情感功能紊乱的一种综合征。
其临床表现为突发性局灶性神经功能缺损,以及一定程度的意识障碍。
CISS分型治疗及二级预防是对缺血性脑血管病进行全面、系统的治疗和预防措施,以降低病情的恶化程度,促进康复,预防病情的再次发作。
一、CISS分型治疗CISS分型治疗是依据脑血管疾病的特点和病情严重程度进行的分型治疗措施,包括药物治疗、手术治疗、康复治疗等多种方法。
对于CISS分型治疗,应根据具体情况制定个性化治疗方案,以达到最佳的治疗效果。
1. 药物治疗对于缺血性脑血管病,药物治疗是常见的治疗方式。
主要包括抗血小板药物、抗凝药物、扩血管药物、脱水药物等。
抗血小板药物可以有效防止血小板聚集,减少血栓形成;抗凝药物能够延长凝血时间,预防血栓形成;扩血管药物能够扩张血管,改善局部血流;脱水药物能够降低颅内压力,减轻脑水肿。
在具体应用时,应根据患者的具体情况和病情严重程度进行选择。
2. 手术治疗对于某些病情较为严重的患者,特别是合并颅内血肿或血管重建手术指征的患者,手术治疗是必要的。
手术治疗包括颅内血肿清除术、颅内血管重建手术等。
通过手术治疗,能够减轻脑组织的压迫,改善脑血流,提高患者的生存质量和康复效果。
3. 康复治疗对于缺血性脑血管病,康复治疗是非常重要的治疗方式。
康复治疗包括物理治疗、言语治疗、职业治疗等。
通过康复治疗,能够训练患者的神经功能,恢复患者的日常生活能力,提高患者的生活质量。
二、二级预防二级预防是指对已经发生过一次缺血性脑血管病的患者进行的预防措施,以降低病情的恶化程度,预防病情的再次发作。
二级预防措施主要包括药物预防、生活方式调整、定期随访等多方面。
1. 药物预防药物预防是对已经发生过一次缺血性脑血管病的患者进行的长期、规律的用药。
主要包括抗血小板药物、抗凝药物等。
脑血管病的二级预防的指南

脑血管病的二级预防的指南脑血管病是指发生在大脑血管系统中的各种疾病,包括脑梗死、脑出血和蛛网膜下腔出血等。
据统计,脑血管病在全球范围内是主要的致残和致死原因之一、针对脑血管病的威胁,二级预防是非常重要的措施,它主要包括从预防、检测到治疗等方面进行。
以下是脑血管病二级预防的指南。
一、生活方式改变:1.控制高血压、糖尿病和高血脂:这三个疾病是导致脑血管病的重要因素,所以保持血压、血糖和血脂的正常水平非常重要。
建议定期检查血压、血糖和血脂,根据医生的指导进行药物治疗和调整饮食习惯。
2.戒烟限酒:长期吸烟和过量饮酒是导致脑血管病的高危因素。
如果有吸烟和饮酒习惯,应该尽量戒烟和限制酒精摄入。
3.保持健康体重:肥胖是脑血管病的危险因素之一,因此要通过控制饮食和增加体能活动,维持健康的体重。
4.合理饮食:多摄入富含膳食纤维和维生素的食物,如蔬菜、水果、全谷类食品和低脂乳制品。
减少高盐、高胆固醇、高饱和脂肪和高糖的食物摄入。
5.适度运动:运动是保持心血管健康的重要方式。
适量的有氧运动,如快步走、游泳、骑自行车等,每周至少进行5次,每次30分钟以上。
二、药物治疗:1.抗血小板药物:对于有脑梗死或缺血性脑血管疾病风险较高的患者,如有冠心病、糖尿病、高血压等,可以考虑使用抗血小板药物,如阿司匹林或氯吡格雷,以减少血栓形成的风险。
2.抗凝药物:对于有心房颤动的患者,为了预防脑栓塞的发生,可以使用抗凝药物,如华法林或新型口服抗凝药物。
3.降压药物:对于有高血压的患者,根据血压水平和其他危险因素,可以使用降压药物,如β受体阻滞剂、钙通道阻滞剂等。
4.降脂药物:对于有高血脂的患者,根据血脂水平和其他危险因素,可以使用降脂药物,如他汀类药物。
三、定期随访:患者应定期进行医生随访,进行心血管疾病相关指标的检查,如血压、血糖、血脂等。
根据检查结果和病情发展,医生可以调整药物治疗方案。
四、教育和心理支持:对于脑血管病患者和家人,及早提供相关教育和心理支持是非常重要的。
缺血性脑血管疾病的二级预防_李焰生共47页PPT资料
上海交通大学医学院附属仁济医院 神经科 李焰生
脑血管疾病的危害
• 复发率高
– Framingham研究中5年复发危险,男性是42%, 女性是24%
– Rochester研究中5年复发危险是29% – 卒中后第1年复发危险为10%,之后每年5% – 卒中后第1月最危险,占5年危险的30% – DWI-MRI发现98例急性梗死中34%有新发灶 – TIA后90天内发生卒中危险为10%,其中半数
20.00% 15.00% 10.00%
高血压+血脂异常+血糖 高血压+血脂异常+缺乏锻炼
RF组合
5.00% 0.00%
1+2+5 1+2+3 1+2+4 1+2+6 2+4+5 1+4+5
1=高血压 2=血脂异常 3=糖代谢异常 4=缺乏锻炼 5=吸烟 6=卒中史
缺血性脑血管疾病 的二级预防基本认识
发生在2天内;TIA后第1年复发危险为12%,5年 为30%
脑血管疾病的危害
• 复发与类型有关
– 动脉粥样硬化性者最高,腔隙梗死者最低,心 源性/不明原因者居中
• 复发卒中危害大
– 病死率是首发的2倍,复发卒中30天内的病死 率达20-30%
– 50%非死亡复发卒中者有功能残疾 – 复发导致残疾加重、死亡增加、住院时间延长
高血脂 HD
缺血组 出血组
卒中
脑卒中患者常常有多重危险因素
5+RF 0+1RF 10% 10%
0+1
4RF
2
20%
2RF
缺血性脑血管病CISS分型治疗及二级预防
缺血性脑血管病CISS分型治疗及二级预防缺血性脑血管病(CISS)是指由于脑血管狭窄或闭塞导致脑组织缺血性损伤的一类疾病,包括脑梗死、短暂性脑缺血发作(TIA)和血管性脑病。
CISS在我国成年人中的患病率一直居高不下,已成为危害人类健康的重要疾病。
对CISS的分型治疗和二级预防非常重要。
一、CISS分型治疗1. 脑梗死的分型治疗脑梗死是CISS中最常见的类型之一,治疗时需根据患者的具体情况进行细致的分型处理。
(1)大血管病变:对大血管病变引起的脑梗死,首要的是恢复脑血流,可采取溶栓治疗、介入手术或外科手术等措施,以尽快恢复脑功能。
(2)小血管病变:对小血管性脑梗死,需重点注意降低动脉粥样硬化斑块的稳定性,常规采取抗血小板聚集药物、他汀类药物等治疗手段。
(3)半梗死状态:对半梗死状态的患者,需要立即进行抢救性处理,保证脑部血液供应,阻止病情进一步发展。
2. 短暂性脑缺血发作(TIA)的分型治疗TIA是CISS的一种预警信号,如不及时处理,易发展为脑梗死,因此分型治疗尤为关键。
(1)大动脉粥样硬化性TIA:对大动脉粥样硬化性TIA,应积极控制高血压、血糖、血脂等危险因素,同时给予抗血小板聚集药物治疗。
(2)动脉狭窄性TIA:对动脉狭窄性TIA,需采用介入手术或外科手术治疗,恢复受累脑部的血液供应。
对于血管性脑病,需要根据脑部血管分布情况进行分型治疗。
(1)脑动脉硬化性脑病:对脑动脉硬化性脑病,首要的是降低危险因素,同时采取药物治疗、改变生活方式等措施。
(2)脑动脉炎性脑病:对脑动脉炎性脑病,须经过充分的抗感染治疗和免疫调节治疗,尽量减少炎症损伤。
二、CISS的二级预防除了及时治疗不同类型的CISS之外,二级预防同样至关重要。
二级预防包括以下几个方面:1. 控制危险因素高血压、高血糖、高血脂等是CISS的重要危险因素,因此及时、有效地控制这些危险因素,可以大大降低CISS的发病风险。
2. 药物干预CISS的患者常常需要长期服用抗血小板聚集药物、他汀类药物等,以维持血管的通畅和稳定,预防病情的进一步恶化。
缺血性脑卒中二级预防研究进展
缺血性脑卒中二级预防研究进展缺血性脑卒中是一种常见的脑血管疾病,是由于脑血管堵塞引起的脑组织缺血性坏死而导致的,发病率和致残率较高。
在脑卒中的二级预防中,特别是对于缺血性脑卒中患者的防治显得尤为重要。
在近年来,针对缺血性脑卒中的二级预防研究取得了一些重要进展,本文将对这方面的研究进展进行归纳和总结。
一、脑卒中的二级预防意义及现状缺血性脑卒中是脑卒中的主要类型,也是导致人们致残和死亡的主要原因之一。
对于缺血性脑卒中的二级预防显得尤为重要。
目前,缺血性脑卒中的二级预防措施主要包括药物预防和非药物预防。
防治手段的选择和疗效的评价需要依据大量的研究证据,加强对缺血性脑卒中的二级预防研究具有非常重要的意义。
二、抗血小板治疗抗血小板治疗是缺血性脑卒中的一级预防和二级预防的重要手段,其目的是防止或减轻血栓栓塞引起的脑血管疾病。
抗血小板药物主要包括阿司匹林、氯吡格雷、肝素、华法林等。
近年来,多项临床研究验证了抗血小板治疗对脑卒中的二级预防效果显著。
CAPRIE研究显示,氯吡格雷与阿司匹林相比,在缺血性脑卒中患者中可以显著降低心脑血管事件的再发风险。
新型抗血小板药物——替格瑞洛在缺血性脑卒中的二级预防中也取得了良好的临床效果。
抗血小板治疗在缺血性脑卒中的二级预防中具有重要意义。
三、脂质代谢调节脂质代谢异常是脑卒中患者的常见情况,而脂质代谢异常又是导致脑卒中的重要危险因素之一。
脂质代谢调节在脑卒中的二级预防中具有重要意义。
目前,临床研究提示,降脂药物可以显著降低脑卒中患者的再发风险。
他汀类药物可以不仅明显降低血脂水平,减轻动脉粥样硬化,还可以显著降低脑卒中患者的再发风险。
在脑卒中的二级预防中,脂质代谢调节是一个重要的治疗手段。
四、抗凝治疗对于合并心房颤动的脑卒中患者来说,抗凝治疗是非常重要的。
抗凝治疗可以有效防止心房颤动引起的血栓栓塞,降低脑卒中的再发风险。
目前,临床上常用的抗凝药物包括华法林和新型抗凝药物达比加群。
缺血性脑卒中-从急性期到二级预防PPT课件

01
缺血性脑卒中是一种常见的脑血 管疾病,提高公众对缺血性脑卒 中的认识,有助于早期发现和预 防。
02
公众可以通过参加缺血性脑卒中 相关的健康讲座、阅读相关科普 文章和观看教育视频等方式,增 加对缺血性脑卒中的了解。
健康饮食和生活方式
保持健康的饮食习惯,如低盐、低脂 、高纤维等,有助于降低缺血性脑卒 中的风险。
临床表现和诊断
临床表现
缺血性脑卒中可表现为突然出现的单 侧肢体麻木、无力、口角歪斜、视力 模糊等症状。
诊断
诊断主要依靠临床表现和影像学检查 ,如CT或MRI。血液检查和血管检查 也可用于评估病情和确定病因。
02 缺血性脑卒中的急性期治 疗
急救措施
01
02
03
04
快速识别
及时识别卒中症状,如肢体无 力、言语不清等,并立即拨打
作业疗法
通过日常生活活动训练,如穿衣、 进食、洗澡等,提高患者的自理能 力。
言语和吞咽治疗
针对语言和吞咽障碍,通过特定的 训练和代偿方法,帮助患者恢复语 言和吞咽功能。
护理措施
急性期护理
长期护理
密切监测病情变化,保持呼吸道通畅, 预防并发症,如肺部感染、褥疮等。
对于长期卧床或行动不便的患者,提 供生活照顾和日常护理,预防并发症。
03 缺血性脑卒中的二级预防
控制危险因素
高血压
定期监测和控制高血压,保持 血压稳定在正常范围内,减少
脑卒中的风险。
糖尿病
积极治疗糖尿病,控制血糖水 平,预防糖尿病并发症的发生 。
血脂异常
通过饮食调整和药物治疗,降 低血脂水平,减少动脉粥样硬 化的发生。
吸烟和饮酒
戒烟和限制饮酒,避免烟草和 酒精对血管的损害。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
21
Hemorrhagic transforamtion is an very important clue to an embolic mechanism
22
23
Contents
Brain Embolism? Recipient Artery Donor Source Pathophysiology Nature of Embolic Particles Treatment﹠Prevention Complications
6
Brain Embolism Clinical Features
危险因素 -- 动脉粥样硬化较少 -- 心脏病因素较多(如AF、心肌病、心 瓣膜病、心衰等 -- 主动脉弓病变 -- 头颈部大血管病变 -- 静脉血栓形成条件 -- 其他部位栓塞证据
7
临床提示栓塞的证据
TIA或小中风通常单次或发作频率较低,但单 次发作持续时间比较长 症状在一开始就达高峰,或阶梯式发展 有时在活动、咳嗽、打喷嚏时发作 梗塞灶可累及不同形态的多个血管区域 出血转化多见,也是较为特征性的影像学改变 可发现远端血管内栓子 梗塞灶常成楔形,位于皮质或皮质下 存在心脏、动脉或静脉栓子源的证据
24
Donor Source
Heart Aorta Cervico-Cranial Arteries Veins (Paradoxical Embolism)
Dictionary
5
Prevalent Concepts
Embolism =Cardiac-origin embolism The hit rate is very high Treatment is based on the sourceanticoagulants for cardiac-origin embolism and antiplatelets for arterial source embolism
3
Contents
Brain Embolism? Donor Source Pathophysiology Nature of Embolic Particles Recipient Artery Treatment﹠Prevention Complications
4
Definition of an embolus
Undissolved material carried by the blood current and impacted in some part of the vascular system such as thrombi, tissue fragments, clumps of bacteria, fat globules, or air bubbles
14
常见的栓塞部位
15
16
The recipient arteries are responsible for the clinical
presentation
What information is used to classify a stroke as embolic
17
Recipient arteries Factors favoring an embolic stroke mechanism
19
Recipient arteries(At necropsy and imaging)
Open-no blockage Distal blockage beyond the infarct Abrupt occlusion without narrowing Absence of underlying AS or other intrinsic disease No attachment of thrombus to artery
Recipient Artery Donor Source -- Heart -- Aorta -- Cervico-Cranial Arteries -- Veins (Paradoxical Embolism) Embolic matter ( the “stuff” )
11
12
13
Clot in BA
缺血性脑血管病二级预防
1
Disclosures
2
Contents
Brain Embolism? Donor Source Pathophysiology of Embolic particles Recipient Artery Treatment﹠Prevention Complications
18
Size of Infarcts Stroke Data Bank
Size of infracts on CT scan -- Cardiac-origin embolism- the median volume of infracts was 2.4x that found in patients with intraarterial embolism 早期意识障碍发生率 -- 心源性 29.8% -- 动脉源性 6.1%
Timing of symptoms--max at onset or one step within 24~48 hours Size of infarct Infarct location--cortical, cortical/subcortical Hemorrhagic transformation Appearance on vascular imaging of recepient artery--no important underlying AS, passage of blockage, shape of block, filling defect
8
9
Contents
Brain Embolism? Recipient Artery Donor Source Pathophysiology Nature of Embolic Particles Treatment﹠Prevention Complications
10
Brain Embolism Actors in the Drama