2019精品欧洲低钠血症诊疗指南文档
低钠血症诊疗指南

低钠血症诊疗指南低钠血症是指血液中钠离子的浓度低于正常范围。
钠是人体内重要的电解质之一,参与维持细胞内外的酸碱平衡和水分平衡。
低钠血症常见于肾脏疾病、心脏疾病、肺疾病、消化系统疾病等。
本文将介绍低钠血症的诊断和治疗指南。
诊断首先,对患者的病史进行详细询问,包括用药史、近期饮食情况、病前排尿情况等。
此外,还需要进行一系列实验室检查,包括血钠浓度、血浆渗透压、尿液渗透压、尿钠浓度等。
根据检查结果及患者病史,判断低钠血症的病因。
治疗低钠血症的治疗策略因病因而异,下面将根据病因分类介绍治疗方法。
1.药物引起的低钠血症:如果低钠血症是由其中一种药物引起的(如利尿剂、抗抽搐药物等),首要任务是停用或调整药物剂量。
同时,可以通过口服或静脉补钠的方式来提高血液中的钠离子浓度。
2.水过多引起的低钠血症:水过多是指体内的总水量超过正常范围。
常见的原因有过多饮水、肾功能不全等。
治疗上应限制液体摄入,控制饮水量。
此外,可以适量应用利尿剂增加尿液排出。
3.肾上腺皮质功能不全引起的低钠血症:顾名思义,是由于肾上腺皮质功能不全导致的。
治疗上主要是补充钠离子和糖皮质激素。
通常使用氢化可的松或氢氢可的松等糖皮质激素来治疗。
4.胃肠道疾病引起的低钠血症:如果低钠血症是由于胃肠道疾病导致的,如腹泻、呕吐引起的失水,治疗上应积极控制病情,避免进一步失水。
严重失水的患者需要静脉补液,补充水分和电解质。
5.其他病因引起的低钠血症:低钠血症还可能由于心脏疾病、肺疾病等引起,治疗上应积极治疗原发病,同时根据具体病情进行合理的补钠治疗。
需要注意的是,低钠血症的处理要个体化,根据患者的具体情况进行判断,避免过度或不足的补钠。
预防措施预防低钠血症的关键是注意饮食平衡和药物使用。
饮食上应保证摄入适量的钠离子,避免过度饮水或外源性摄入钠过多。
使用药物时应遵医嘱,注意药物剂量的合理调整,以及可能引起低钠血症的副作用。
总结低钠血症是一种常见的电解质紊乱,病因复杂。
欧洲指南低钠血症诊治流程 解读
低钠血症的治疗流程
是
否
症状严重的严重低钠 血症 (1)
中重度症状?
是
否
中重度症状的低钠血症 (2)
急性低钠血症?
是
无中重度症状的 急性低钠血症
(3)
否 慢性低钠血症
循环血容量不足?
低容量的
是
慢性低钠血症
(4)
否
细胞外液量增多?
高容量的
是
慢性低钠血症
(5)
否
SIADH (6)
严重症状?
低钠血症的治疗流程
循环血容量不足?
是
否
细胞外液量增多?
高容量的
是
慢性低钠血症
(5)
否
SIADH (6)
症状严重?
低钠血症的治疗流程
是
否
症状严重的严重低钠 血症 (1)
中度症状?
是
否
中度症状的低钠血症 (2)
急性低钠血症?
是
否
(6)SIAD
无急中性重低度钠症血状•症一的线:限制液体摄入慢性低钠血症 (3) •二线:0.25-0.5g/kg/d尿素口服
或低剂量袢利循尿环剂血容量不足? 或口服氯化钠
慢•不低 性容 低推量 钠荐的 血血症管加压是素受体拮抗剂
否
(4)
细胞外液量增多?
高容量的
是
慢性低钠血症
(5)
否
SIAD (6)
症状严重?
低钠血症的治疗流程
是
否
症状严重的严重低钠 血症 (1)
中重度症状?
是
否
中重度症状的低钠血症 (2)
急性低钠血症?
是
根据病程
•急性: <48h •慢性: ≥48h
低钠血症的诊断与治疗
中度症状低钠血症的治疗 (1)中度症状低钠血症应给予有限的高渗盐水、等渗盐水、口服钠盐、限水或普坦类药物治疗。 (2)寻找病因 (3)如果对因治疗中血钠进行性下降,建议如严重症状低钠血症一样管理。
无或轻度症状的慢性低钠血症的治疗 (1)不推荐以单纯升高血钠浓度为目标的治疗。 (2) 去除诱因、限水,停用可能引起低钠血症的药物或其他因素。
对因治疗
低容量性慢性低钠血症:以恢复细胞外容量治疗为主(补液--等渗盐水),对因治疗(停用导致低钠药 物,应用氢化可的松纠正盐皮质激素缺乏);
高容量性慢性低钠血症:以限制液体量,应用袢利尿剂,控制原发病,必要时使用普坦类药物治疗;
等容量性慢性低钠血症:对因治疗(停用导致低钠药物,激素缺乏的行替代治疗),限制液体量,普坦 类药物
慢性低钠血症过度纠正处理: (1)如果24 h血钠增加幅度>10 mmol /L,48 h>18 mmol /L,建议立即采取措施降低血钠并停止积极的补钠 治疗;
(2)在严密监测尿量和液体平衡的情况下口服补充水分或输注10 ml/kg 5%葡萄糖溶液,输注速度3 ml·kg·h -1;
(3)持续输液治疗,每小时复测血钠水平,直至血钠降至目标值;
(4)上述处理仍不能改善,可以考虑给予糖皮质激素(如地塞米松4 mg q6h)治疗24~48 h。
总结
低钠血症
排除高血糖及其他原因所 致的非低渗性低钠血症
低渗性低钠血症
症状是否紧急
是
立即治疗
心衰、肝硬 化、肾综
容量 增加
精神性多饮
否
>100
正常 容量
尿渗透压
<100
容量
经过体表、消化道、
下降
肾脏丢失
最新欧洲低钠血症诊疗指南学习ppt课件

欧洲低钠血症诊疗指南学习
低钠血症
定义: 血清钠低于135mmol/L
临床最常见的水盐失衡,其 发生率约占住院患者的30%
症状不一,从轻微到致命
为何以48小时为界限界定急慢性低钠血症?
当低钠血症发生快速发生 时,脑细胞几乎没有时间 来适应低渗环境。
大脑通过减少其细胞内渗 透活性物质如钾和有机溶 质以试图恢复脑容量。此 过程需时24~48小时。因 此,以48小时作为急性和 慢性低钠血症的界限
6.2.1.2 测得的渗透压<275 mOsm/kg 总提示为低渗性低钠 血症。
6.2.1.3 若无表10中所列非低渗 性低钠血症的证据则接受“低渗 性低钠血症”。
6.3 区别低渗性低钠血症的参数?
6.3.1.1 首先检测并解释尿渗透压 6.3.1.2 如果尿渗透压≤100
mOsm/kg,可认为水摄入相对过量是 低渗性低钠血症的原因。
进 入 夏 天 ,少 不了一 个热字 当头, 电扇空 调陆续 登场, 每逢此 时,总 会想起 那 一 把 蒲 扇 。蒲扇 ,是记 忆中的 农村, 夏季经 常用的 一件物 品。 记 忆 中 的故 乡 , 每 逢 进 入夏天 ,集市 上最常 见的便 是蒲扇 、凉席 ,不论 男女老 少,个 个手持 一 把 , 忽 闪 忽闪个 不停, 嘴里叨 叨着“ 怎么这 么热” ,于是 三五成 群,聚 在大树 下 , 或 站 着 ,或随 即坐在 石头上 ,手持 那把扇 子,边 唠嗑边 乘凉。 孩子们 却在周 围 跑 跑 跳 跳 ,热得 满头大 汗,不 时听到 “强子 ,别跑 了,快 来我给 你扇扇 ”。孩 子 们 才 不 听 这一套 ,跑个 没完, 直到累 气喘吁 吁,这 才一跑 一踮地 围过了 ,这时 母 亲总是 ,好似 生气的 样子, 边扇边 训,“ 你看热 的,跑 什么? ”此时 这把蒲 扇, 是 那 么 凉 快 ,那么 的温馨 幸福, 有母亲 的味道 ! 蒲 扇 是 中 国传 统工艺 品,在 我 国 已 有 三 千年多 年的历 史。取 材于棕 榈树, 制作简 单,方 便携带 ,且蒲 扇的表 面 光 滑 , 因 而,古 人常会 在上面 作画。 古有棕 扇、葵 扇、蒲 扇、蕉 扇诸名 ,实即 今 日 的 蒲 扇 ,江浙 称之为 芭蕉扇 。六七 十年代 ,人们 最常用 的就是 这种, 似圆非 圆 , 轻 巧 又 便宜的 蒲扇。 蒲 扇 流 传 至今, 我的记 忆中, 它跨越 了半个 世纪, 也 走 过 了 我 们的半 个人生 的轨迹 ,携带 着特有 的念想 ,一年 年,一 天天, 流向长
低钠血症诊疗指南

辅助检查(六)■ 7.30 心电图:下壁心梗■ 8.1 双下肢股动脉内膜粗糙不光滑;双颈动 脉、双下肢静脉未见明显异常■ B超右肾130mm; 左肾101mm■ MR 双颈内动脉动脉硬化改变
诊断■ 低钠血症肾小管功能不全冠心病■ 陈旧性脑梗死■ 肺心病阻塞性睡眠呼吸暂停综合征阑尾切除术后
讨论■ 低钠血症的原因?■ 低钠血症的分级、临床表现?■ 下一步的诊疗计划?
2014 欧洲低钠血症诊疗指南解读
Part One
定义:血清钠低于135 mmol/L临床最常见的水盐失衡,其 发生率约占住院患者的30%症状不一,从轻微到致命
Hyponatraemia, defined as aserum sodium concentration<
135 mmol/l, is the mostcommon disorder of body fluidand electrolyte balanceencountered in clinical practice .It occurs in up to 30% ofhospitalised patients and canlead to a wide spectrum ofclinical symptoms, from subtleto severe or even life
6.23
6.28
7.2
7.7
7.12
7.17
7.30
8.2
Na(mmol/L)
112
117
118
121
121
123
104
118
Cl(mmol/L)
80
82
83
84
84
86
74
85.7
低钠血症诊疗指南

03
低钠血症的治疗
急性低钠血症的治疗
去除病因
首先需要去除导致急性低钠血症 的病因,如停用利尿剂、治疗肺
部感染等。
限制水分摄入
对于轻度低钠血症患者,可以通 过限制水分摄入来纠正低钠状态
。
静脉补充高渗盐水
对于中度和重度低钠血症患者, 需要静脉补充高渗盐水,以迅速 提高血钠浓度。但需注意补充速 度和剂量,避免引起中央髓鞘溶
心电图检查
低钠血症可能导致心律失 常,心电图检查有助于发 现心脏受累情况。
胸部X线片
部分低钠血症患者可能合 并肺部感染或肺水肿,胸 部X线片有助于相关疾病的 诊断。
诊断标准和流程
诊断标准
根据血清钠浓度低于正常范围确定低钠血症,并结合病史、临床表现和实验室 检查结果,判断其病因和类型。
诊断流程
首先通过血清钠测定确诊低钠血症,然后进行尿液检查、血液其他电解质测定 、影像学和其他辅助检查,以明确病因和病情评估。最后,结合诊断结果制定 个体化的治疗方案。
03
倡导适量运动、保持充足睡眠、避免过度劳累等健康生活方式
,以降低低钠血症的发S
低钠血症可能导致头痛、恶心、呕吐、精 神错乱、癫痫发作等神经系统症状。
患者可能出现食欲不振、腹胀、腹泻等消 化系统症状。
循环系统症状
其他症状
低钠血症可能导致心悸、心率加快、血压 下降等循环系统症状。
患者还可能出现肌肉痉挛、呼吸困难、昏 迷等症状。需要注意的是,症状的严重程 度与血钠降低的速度和程度有关。
02
低钠血症的诊断
实验室检查
血清钠测定
通过测量血液中钠离子的浓度,确定低钠血症的存在和程度。
尿液检查
包括尿钠、尿渗透压等指标,帮助判断低钠血症的病因和类型。
欧洲更新低钠血症诊治指南
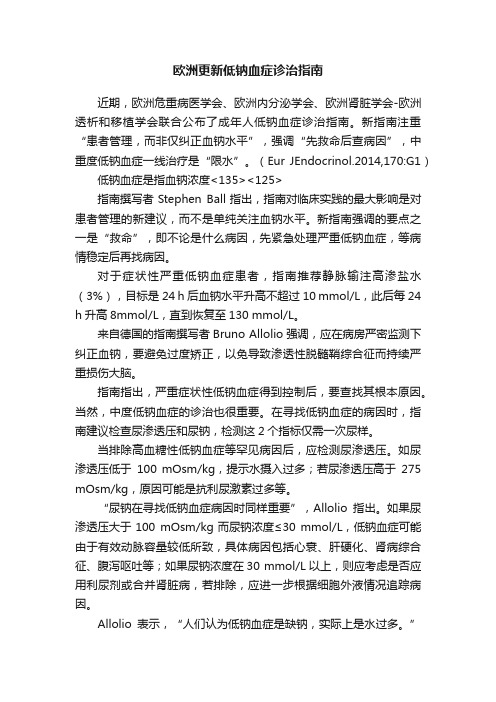
欧洲更新低钠血症诊治指南近期,欧洲危重病医学会、欧洲内分泌学会、欧洲肾脏学会-欧洲透析和移植学会联合公布了成年人低钠血症诊治指南。
新指南注重“患者管理,而非仅纠正血钠水平”,强调“先救命后查病因”,中重度低钠血症一线治疗是“限水”。
(Eur JEndocrinol.2014,170:G1)低钠血症是指血钠浓度<135><125>指南撰写者Stephen Ball指出,指南对临床实践的最大影响是对患者管理的新建议,而不是单纯关注血钠水平。
新指南强调的要点之一是“救命”,即不论是什么病因,先紧急处理严重低钠血症,等病情稳定后再找病因。
对于症状性严重低钠血症患者,指南推荐静脉输注高渗盐水(3%),目标是24 h后血钠水平升高不超过10 mmol/L,此后每24 h升高8mmol/L,直到恢复至130 mmol/L。
来自德国的指南撰写者Bruno Allolio强调,应在病房严密监测下纠正血钠,要避免过度矫正,以免导致渗透性脱髓鞘综合征而持续严重损伤大脑。
指南指出,严重症状性低钠血症得到控制后,要查找其根本原因。
当然,中度低钠血症的诊治也很重要。
在寻找低钠血症的病因时,指南建议检查尿渗透压和尿钠,检测这2个指标仅需一次尿样。
当排除高血糖性低钠血症等罕见病因后,应检测尿渗透压。
如尿渗透压低于100 mOsm/kg,提示水摄入过多;若尿渗透压高于275 mOsm/kg,原因可能是抗利尿激素过多等。
“尿钠在寻找低钠血症病因时同样重要”,Allolio指出。
如果尿渗透压大于100 mOsm/kg而尿钠浓度≤30 mmol/L,低钠血症可能由于有效动脉容量较低所致,具体病因包括心衰、肝硬化、肾病综合征、腹泻呕吐等;如果尿钠浓度在30 mmol/L以上,则应考虑是否应用利尿剂或合并肾脏病,若排除,应进一步根据细胞外液情况追踪病因。
Allolio表示,“人们认为低钠血症是缺钠,实际上是水过多。
欧洲新低钠血症指南要点
根据《国务院关于建立全科医师制度的指导意见》(国发〔2011〕23号)要求“到2020年,基本实现城乡每万名居民有2 3名合格的全科医师”的最低标准计算,非珠三角区全科医师缺口在6180人以上。
广东省社区护士资源匮乏明显,社区护士与全科医师的比例仅为1ʒ1,远低于全国评估参考标准2ʒ1的水平;而且社区护士配置公平性低于全科医师,建议充分挖掘社区现有资源,强化政府的主导作用,同时发挥市场机制作用,吸引社会力量参与,增加投入,拓宽全科医师培养渠道[9-10],切实加强全科医师培养体系建设;进一步完善社区护士教育与培养机制,结合社区护士的需求进行相应的教学改革和建立社区护理培训实践基地[11],加快护理人员培养,以促进社区护理适应社区卫生服务的发展[12-13]。
3.2社区卫生服务人力资源布局不合理,地理分布的公平性欠佳本研究结果显示虽然全省全科医师和社区护士按人口分布配置达到了比较公平的程度,但珠三角区的基尼系数和泰尔-L 指数最高,集中了省内80%以上的全科医师和社区护士资源,地理分布的不公平性较强;对总泰尔指数进行分解,结果显示区域间差异是造成广东省社区人力资源配置不公平的主要原因。
此外,由于广东省全科医生、社区护士按地理分布的基尼系数处于警戒状态,公平性欠佳,需要引起警惕。
建议卫生行政部门在进行社区人力资源分配时,充分考虑地理分布对社区卫生服务可及性的影响,进一步提高社区人力资源地理分布的公平性。
参考文献1刘莎娜,方小衡,刘海平,等.广东省社区卫生服务中心业务开展情况的调查分析[J ].中国全科医学,2011,14(8):2501-2503.2姚卫光,魏国文,徐爱光,等.广东省社区卫生服务机构卫生人力资源与工作现状的抽样调查[J ].中国全科医学,2011,14(4):1779-1781.3周巍.基层卫生人才队伍的现状、问题与建议[J ].中国全科医学,2010,13(7):685-688.4李泽杰,王碧华.广东省居民对社区卫生服务满意度调查与影响因素分析[J ].中国卫生事业管理,2012,29(4):251-255.5王春晓,马林,何磅礴,等.2002—2006年广东省卫生资源配置公平性的趋势研究[J ].中国卫生资源,2010,13(6):304-306.6张彦琦,唐贵立,王文昌,等.基尼系数和泰尔指数在卫生资源配置公平性研究中的应用[J ].中国卫生统计,2008,25(3):243-246.7沈沁,杨珺,黄亚芳,等.北京市社区卫生服务机构卫生人力资源现况研究[J ].中国全科医学,2009,12(8):2169-2172.8王芳,朱晓丽,丁雪,等.我国基层卫生人力资源配置现状及公平性分析[J ].中国卫生事业管理,2012,29(2):108-110.9线福华,路孝琴,吕兆丰,等.全科医师培养模式及其实施中相关问题的思考[J ].中国全科医学,2012,15(8):2498-2501.10张立威,黄婉霞,胡丙杰,等.广州市全科医师培训效果的追踪评价[J ].中国全科医学,2012,15(10):3278-3280.11杨玲,杜雪平,王永利,等.中国社区护士培训方法研究[J ].中国全科医学,2011,14(11):3608-3615,3619.12刘可仪,周颖清.社区护士角色功能的初步研究[J ].中国全科医学,2011,14(1):90-92.13吴亚君,王亚红,宋亚琴,等.社区护士在团队服务中的角色功能及影响因素研究[J ].护理学杂志,2010,25(17):69-71.(收稿日期:2013-10-20;修回日期:2014-02-12)(本文编辑:赵跃翠)·医学新闻·欧洲新低钠血症指南要点《欧洲内分泌学杂志》在线公布了最新的“低渗性低钠血症的诊断,分类和治疗指南”。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
3
2
30mmol/l
Fenske et al. also included hypervolaemicpatients. They assessed the same threshold for distinguishing hypovolaemia from euvolaemia and hypervolaemia but analyzed patients with and without diuretics separately (107)
patients with chronic hyponatraemia and no apparent symptoms can have subtle clinical abnormalities when analysed in more detail. Such abnormalities include gait disturbances, falls, concentration and cognitive deficits
classifying hyponatraemia as hypovolaemic,
euvolaemic or hypervolaemic (87, 101,
102). However, clinical assessment of volume status is generally not very accurate (90). Hence, we wanted to know which tests are most useful in
24~48 48
8
3,4-methylenedioxymethamfetamine MDMAXTC IV
6131
6132 Glasgow8
125mmol/l110125mmol/l,
48h48h
""
6.2275 mOsm/kg , as effective osmolality can never be higher than total or measured osmolality. 275 mOsm/kg By contrast, if calculated osmolality is275 mOsm/kg,
6.3.1.4 30mmol/l,
6.3.1.5 30mmol/l
6.3.1.6 SIADH.
G22
30 mmol/L SIAD6 SIAD
SIAD
275/ ,100/kg,
30 mmoll
0.24 mmolL 4/ 3.6 mmolL 21.6/ 0.9% 0.5 % 55 % 12 %
Severe symptoms of hyponatraemia are caused by brain oedema and increased intracranial pressure. Brain cells start to swell when water moves from the extracellular to the intracellular compartment because of a difference in effective osmolality between brain and plasma.
hyponatraemia can be hypotonic, isotonic or hypertonic, depending on which osmotically active agents are present and whether or not they are incorporated in the formula.
2
100 mOsm/kg
100 mOsm/kg ""
3
1 5
0.9% 430 mmol/l
five studies assessing diagnostic accuracy of urine sodium concentration for differentiating hypovolaemia from euvolaemia or hypervolaemia. All studies used a rise in serum sodium concentration after the infusion of 0.9% sodium chloride as the reference standard for diagnosing hypovolaemia (89).
2014
ESICM
ESE
European Renal Best Practice ERBP) ERA-EDTA
Hyponatraemia, defined as a serum sodium concentration 135 mmol/l, is the most common disorder of body fluid and electrolyte balance encountered in clinical practice. It occurs in up to 30% of hospitalised patients and can lead to a wide spectrum of clinical symptoms, from subtle to severe or even life threatening (10, 11)
6. Diagnosis of hyponatraemia 6.1. Classification of hyponatraemia
6111 (mild)
130~135mmol/l
6112 moderate 125~129mmol/l
6113 profound
<125mmol/l
SIAD 5.65.8
failure, liver cirrhosis and nephrotic
syndrome (see sections 5.6 and 5.8).
Clinicians have traditionally used the
clinical assessment of `volume status' for
ቤተ መጻሕፍቲ ባይዱ
135mmol/L
30%
In most cases, hyponatraemia reflects low effective osmolality or hypotonicity, which causes symptoms of cellular oedema.
However, hyponatraemia may also (rarely) occur with isotonic or hypertonic serum if the serum contains many additional osmoles, such as glucose or mannitol. Therefore, we discuss not only how hypo-osmolar but also how isosmolar and hyperosmolar states develop.
Why this question?
Hypotonic hyponatraemia has many possible underlying causes. These include, but are not limited to, non-renal sodium loss, diuretics, third spacing, adrenal insufficiency, SIAD, polydipsia, heart
6.2
6.2.1.1 9
6.2.1.2 275 mOsm/kg
6.2.1.3 10 " "
(Osmolality)(mOsm/kg H2O) (Osmolarity)(mOsm/L)
6.3
6.3.1.1 6.3.1.2 100
mOsm/kg,
6.3.1.3 100 mOsm/kg,
6121 <48h
6122: 48h
6123
8
48
This usually occurs when hyponatraemia develops rapidly, and the brain has had too little time to adapt to its hypotonic environment.
Clinical assessment of fluid status
We found two studies indicating that in patients with hyponatraemia, clinical assessment of volume status has both low sensitivity (0.5�0.8) and specificity (0.3�0.5)Similarly, it seems that clinicians often misclassify hyponatraemia when using algorithms that start with a clinical assessment of volume status .Using analgorithm in which urine osmolality and urine sodium concentration are prioritized over assessment of volume status, physicians in training had a better diagnostic performance than senior physicians who did not use the algorithm