simultaneous PET-MRI a new approach for functional and morphological imaging
PET-MR-大基医疗
辐射剂量:
Type of radiation MR* PET(chest) A bomb CT(chest) PET/CT 18F-FDG** Relevant dose(mSv) 0.001 0.10 40(5-150) 10 20 5***
times 0.01 1 400 100 200 50
北京大基康明医疗设备有限公司 PET/MR机器人医学影像系统
.
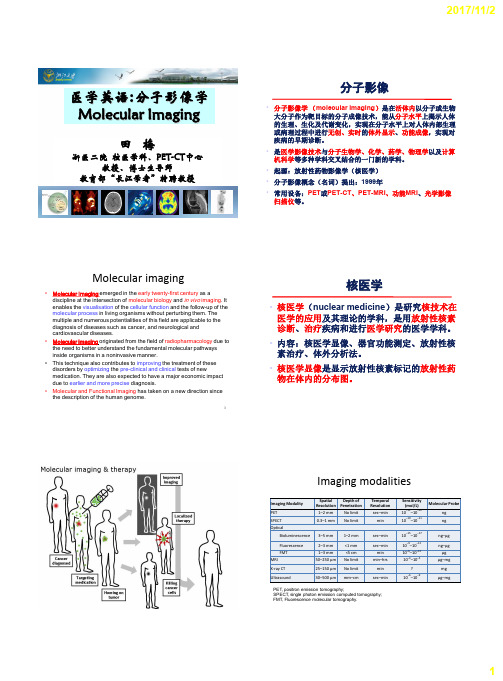
什么是PET?
PET(Positron Emission Tomography) 正电子发射断层摄影,是将微量的正电子 核素示踪剂注入人体内,用体外探测装置探测其体内分布,通过计算机断层显像显示人 体组织的代谢和受体功能分布情况,是人体的生理生化断层,是一种生命显像(Life Imaging)。 它是反映病变的基因、分子、代谢及功能状态的显像设备。它是利用正电子核素标 记葡萄糖等人体代谢物作为显像剂,通过病灶对显像剂的摄取来反映其代谢变化,从而 为临床提供疾病的生物代谢信息。PET的诞生是当今生命科学、医学影像技术发展的新里 程碑。它以其能显示脏器或组织的代谢活性及受体的功能与分布而受到临床广泛的重视, 也称之为“活体生化显像”。
•
2007年,美国食品和药物管理局对越来越多的放射医生对滥用CT和PET/CT发 出了警告,严禁将它们用于健康体检。
•
美国临床肿瘤学协会根据多年的临床研究发现,几十年来,美国2%的癌症源 于CT扫描,每次CT扫描将增加千分之一的致癌机率。与普通X线相比,检查 同一部位CT辐射剂量是普通X线摄片的十倍以上。
肛管癌术后,肝转移。最小病灶4mm
PET/MR
直肠癌术后,肝及盆腔转移。最小病灶2.5mm
PET/CT
PET/MR
SIMULTANEOUS MRI IMAGING OF MULTIPLE SUBJECTS

专利名称:SIMULTANEOUS MRI IMAGING OF MULTIPLE SUBJECTS发明人:DANNELS, Wayne, R.,DIMITROV,Ivan,LEUSSLER, Christoph申请号:EP07798721.2申请日:20070619公开号:EP2035851A1公开日:20090318专利内容由知识产权出版社提供摘要:A magnetic resonance scanner includes a main magnet (20) that generates a static magnetic field at least in a scanning region (14), and a gradient system (26, 28) that selectively imposes selected magnetic field gradients on the static magnetic field at least in the scanning region. A structure (40) is provided for supporting a plurality of small subjects (80) in the scanning region. The structure includes a plurality of subject supports (82, 82') each configured to support a small subject, and a plurality of solenoid coils (44, 44', 44'') corresponding to the plurality of subject supports. Each solenoid coil is arranged with the corresponding subject support to operatively couple with a small subject supported by the corresponding subject support.申请人:Koninklijke Philips Electronics N.V.,Philips Intellectual Property & Standards GmbH地址:Groenewoudseweg 1 5621 BA Eindhoven NL,Lübeckertordamm 5 20099 Hamburg DE国籍:NL,DE代理机构:Schouten, Marcus Maria 更多信息请下载全文后查看。
医学英语
Molecular Pathways
Molecular targets/ Receptors/Binding sites
PET: Position Emission Tomography
7
正电子发射断层显像(PET)
PET:可活体、无创、反复地从分子水平将体内生化过程影像化
PET-CT
Cells
PET影像探针 T-cell NK cell
Sensitivity (mol/L)
10−11–10−12
10−10–10−11
Molecular Probe ng ng
10−15–10−17
10−9–10−12 10−6–10−12 10−3–10−5
? 10−6–10−9
ng–μg
ng–μg μg
μg–mg mg
μg–mg
1
2017/11/2
1–2 mm No limit 0.3–1 mm No limit
3–5 mm 1–2 mm
Fluorescence FMT MRI X-ray CT Ultrasound
心理学专业英语词汇pdf
心理学专业英语词汇pdf.专业英语1Psychology:n.心理学mind:n心理;心灵,精神soul:n.灵魂behaviour:n.行为The scientific study of behaviour and mental processes:行为与心理过程的科学研究psychologist:n.心理学家philosophy:n.哲学philosopher:n.哲学家Empiricism:n.经验主义,源于英国哲学家洛克,认为知识源于后天学习经验。
行为主义坚持这一观点,强调必须通过观察与实验来研究客观事实为对象的心理现象,例如外显行为。
Positivism:n.实证主义,源于法国哲学家孔德,认为科学只研究可以观察到或经验到的事实,实证即只承认能确证的事实。
biology:n.生物学evolution:n.进化genetics:n.遗传学physiology:n.生理学endocrine:n. 内分泌,激素physics:n. 物理学physicist:n.物理学家psychophysics:n.心理物理学separate scientific discipline:独立的科学学科Principlesof psychology:心理学原理structuralism:结构主义conscious:a.有意识的introspection:n.内省image:n.意象;心象sensation:n.感觉,知觉feeling:n.触觉,知觉,感觉,感情,情感functionalism:n.功能主义thought:n.思想psychoanalysis:n.精神分析(或疗法);心理分析(或疗法) therapy:n.治疗,疗法The interpretation of dreams:梦的解析unconscious mind:无(潜)意识心理Behaviorism:行为主义experimental psychology:实验心理学cognitive:a.认知的humanistic:a.人本主义的cognitive psychology:认知心理学专业英语2variables:变量aggression:攻击;侵犯intelligence:智力operationalisation:操作化abstract concepts:抽象概念observable behaviour:可观察行为puzzle:测验智力的间题(或玩具);难题reification:(抽象概念等)具体化,观念与现象混淆case studies:个案研究法surveys:调查法observations:观察法correlations:相关性experiments:实验法independent variable:自变量dependent variable:因变量extraneous variables:外扰变量,无关变量controls:控制random:随机confounding variables:混杂变量constant:恒定hypotheses:假设2-tailed hypotheses:双极假设1-tailed hypotheses:单极假设operationalised variables:操作性的变量statistically singnificant:统计学意义上的显著null hypotheses:零假设significant effect:显著性效果manipulation of the independent variable:自变量的操纵laboratory:实验室deliberately manipulates:仔细操纵strict control:严格控制subject:被试natural environment:自然环境quasi experiment:准实验专业英语3Perception:知觉Sense:感觉,感官visual perception:视觉,视知觉two-dimensional:二维的retina:视网膜three-dimensional:三维的viewpoin:察点,注视点shape constancy:形状恒常性size constancy:大小恒常性luminescence:发光brightness constancy:明度恒常性illusions :错觉Necker cube:尼克尔立方体emergent properties:突变特性Gestalt:格式塔Phiphenomenon:似动现象Law of Pragnanz :完形倾向性定律proximity:邻近性similarity:相似性closure:闭合continuity:连续性figure-ground:图形-背景mon fate:共同命运,以相同方向运动的物体会被组织在一起专业英语4Attention:注意sensory stimuli:感觉刺激focused or selective attention:集中或选择注意divided attention:分配注意visual field:视野vision:视觉hearing:听觉target:目标;靶专业英语5encode:编码memory:记忆photon:光子,见光度(等千通过一平方厘米大的瞳孔看到每平方米一支蜡烛的照明度)represent:描述;代表;象征representation:表征echoic (auditory):回声的,声象的imagery memory:形象记忆iconic (visual):映象的,形象的recall:回忆tune:声调working memory:工作记忆Visuospatial scratchpad:视觉空间模板photographic (eidetic) memory:映象记忆implicit memory:内隐记忆the central executive:中央执行器phonological loop:语音回路procedural memory:程序记忆enactive mode:动作性模式,指人们用“动作”来表达他们关于世界的知识和经验。
形容词后缀大全以与词例

形容词后缀大全以及词例1.-able表示“可⋯的,能⋯”【例】knowable ['n?u?bl] adj. 可知的inflammable [?n'fl?m?b(?)l] adj. 易燃的(inflame点燃)conceivable [k?n'si?v?b(?)l]adj. 想象得出的(conceive 设想,想象)2.-aceous表示“具有⋯特征的”【例】herbaceous curvaceous foliaceous[h??'be???s][k??'ve???s][,f??l?'e???s]adj.adj.adj.草本植物的(有曲线美的(叶状的( foliherb 草)curve 曲线)叶+aceous;参考:foliage树叶)3.-acious表示“有特征的,多⋯的”【例】sagacious [s?'ge???s] adj. 睿智的( sage智者)capacious [k?'pe???s] adj. 宽敞的(cap 能→的+acious;参考:capble 有能力的)fallacious [f?'le???s] adj. 错误的( fall 错;参考: fallacy 谬误)4.-al表示“⋯的”【例】personal ['p??s(?)n(?)l]adj.continertal [k?nt?'nent(?)l]exceptional[?k'sep?(?)n(?) l] 个人的( person 人)adj. 大陆的( contonent 大陆)adj. 例外的( exception 例外)5.-an可表名词和形容词,“⋯地方, . ⋯人【例】American [?mer?k?n] adj. 美洲的n. 美洲人republica n [r?'p?bl?k(?)n]adj. 共和国的n.共和党人suburban [s?'b??b(?)n]adj. 郊区的6.-aneors表示“⋯有;⋯特征的”【例】simultaneous [,s?m(?)l'te ?n??s] adj. 同时发生的spontaneous [sp?n'te ?n??s]adj. 自发的miscellaneous [,m?s?'le?n??s]adj. 各种各样的(miscell 混杂)7.-ant表示“ 的⋯”【例】discordant [d?'sk??d(?)nt] adj. 不一致的(dis 不+cord 心⋯不是一条心)resista nt [r?'z?st?nt]adj. 抵抗的(resist 抵抗,对抗)repentan t [r?'pent ?nt]adj. 后悔的(pent 难过,repent后悔)8.-ar表示“⋯的”【例】titul ar ['t ?tj?l?]adj. 名义上的(来自title名义)linea r ['l ?n??]adj. 线的( line线)famili ar [f?'m?l??]adj. 熟悉的(family家庭)9.-arian表示“⋯的(人)”【例】humanitarian [hj ?,m? n?'te?r??n] adj./n. 人道主义的(人)(human人)vegetarian [v?d???t??r??n] a dj./n. 素食的(人)(vegetable 蔬菜)10.-ary表示“⋯的”【例】honorary ['?n(?)(r?)r?]adj. 荣誉的(honor 荣誉)imaginary [?'m?d??n(?)r?]adj. 想象的(imagine 想象)stationar y ['ste??(?)n(?)r?]adj. 静止的(station车站;驻扎)11.-ate表示“具有⋯的”【例】considerat e [k?n's?d(?)r?t]adj. 考虑周到的(consider 考虑)moderate ['m ?d(?)r?t]adj. 有节制的(moder 模,规矩)effeminat e [?'fem?n?t]adj. 柔弱的(ef+femin 女人)12.-atic表示“有⋯性质的”【例】dogmatic [d?g'm? t?k] adj. 教条的(dogma 教条)aromaticadj. 芳香的(aroma 芳香)[? r?'m?t?k]fanatic [f?'n? t?k] a dj. 狂热的( fan 入迷者)13.-arive表示“有⋯倾向(性质)的”【例】talkative ['t ??k?t?v] adj. 好说话的( talk 讲话)argumentative [ɑ ?gj?'ment?t?v+adj. 好争吵的( argument 争论)sedative ['sed?t?v] adj. 镇静的( sed 坐+ative)14.-atory表示“有⋯性质的”【例】adj. 谴责的(condemn 谴责)condemnatory [,k?nd?m'ne?t(?)r?]adj. 诽谤的(defame 诽谤)defamatory [d?'f?m?t(?)r?]mandatory ['m?adj. 命令性的(mand 命令 +atory)nd?t(?)r?]15.-en表示“由⋯制成”,通常加在名词后面【例】adj. 木制的(wood 木头)wooden ['w ?d(?)n]woolen ['wul ?adj. 羊毛制的(wool 羊毛)n]waxen['w? ks(?)n] adj. 蜡wax 蜡)制的(16.-ent表示“⋯的”【例】sentien t *?senti?nt]adj. 有知觉的(sent 感觉 +I+ent)obedient [?'bi?d??nt]adj. 服从的(obey 服从)insiste nt [?n's?st(?)nt]adj. 坚持的(insist坚持)17.-eous表示“有⋯的”【例】righteou s ['ra?t??s]adj. 正义的(right正确 +eous)gaseous ['g?s??s]adj. 气体的(gas气体)aqueous ['e?kw??s]adj. 水的(aqu 水+eous)18.-ern表示“⋯方向的”【例】western ['west(?)n]adj. 西方的southern ['s?e(?)n]adj. 南方的northeastern[,n?: θ'i:st?n] adj. 东北方的19.-esque表示“如⋯的”【例】picturesque [,p?kt??'resk] adj. 如画的( picture 图画)arabesque [,? r?'besk] adj. 阿拉伯式的( arab 阿拉伯)gigantesque [,d?a?'ɡ ?ntesk+ adj. 巨人一般的( gigant 巨人)20.-etic表示“属于⋯的”【例】theoretic * θ?r'rt?k] adj. 理论上的( theory 理论)energetic [,en?'d?et?k] adj. 精力旺盛的( energy 精力)sympathetic [s?mp?' θ et?k] adj. 同情的( sympathy 同情)21.-fold表形容词或副词,“倍,双重”【例】twofold *'tu?f??ld] adj./adv. 两倍threefold *' θ ri?f??ld] adj./adv. 三倍manifold ['m? n?f??ld] adj. 繁多的( mani=many)22.-form表示“有⋯形状的”【例】dentifor m [dent?f??m+ adj. 牙齿状的(denti牙齿 +form)crucifor m *'kru?s?f??m+adj.十字形的(cruci十字 +form)cubiform *'kju?b?f??m+adj.立方体的(cube 立方体 +form)23.-ful表示“有⋯的”【例】gratefu l ['gre?tf?l]adj. 感激的(grate 感激)ruefulhopefu l *'ru?f?l]adj.['h??pf?l]后悔的( rue 悔恨)adj. 有希望的( hope 希望)24.-ial表示“有⋯的”【例】benefici al [ben?'f??(?)l]adj. 有好处的(bene 好+fic 做+ial)imparti al [?m'pɑ ??(?)l+adj.公正的(in不+part 部分;偏见+ial)commercial [k?'m???()l]adj. 商业的(commerce 商业 +ial)25.-ian表示“⋯国家的”【例】Egyptian [?'d??p?(?)n] adj. 埃及的Canadian [k?'ne?d??n] adj. 加拿大的Athenian [?' θ i:nj?n] adj. 雅典的26.-ible表示“能⋯的”【例】invincible [?n'v?ns?b(?)l] adj. 不可征服的( in 不+vinc 战胜 +ible)eligible ['el?d??b(?)l] adj. 合格的(e 出+lig 选择 +ible 挑⋯选出来的⋯合格的)irascible [?'r? s?b(?)l] adj. 易发怒的( irasc 愤怒 +ible)ible 该词缀在意义上与“- able 相”同,但主要用于拉丁语后。
日立AIRIS Light开放式MRI详细信息卡说明书
snuecwh ai ms RaAgDeArRe canodn sVtArSuCc-tAi oS Ln. Amdadtirtiixonoafll2y,0i4t 8coxm e2s0w4 i8t,h wa hn ei cwh i p r o v i d e s m a g e
rheicgohn-sdter uf icntiitoino ns yismteamg itnhga.t re a li ze s im a g e re con s t r u c t ion m a t r i x
4
FITT
MR angiography is an important imaging function for MRI diagnosis, considering that the basic performance of a system is essential in MRA imaging. AIRIS Light is equipped with “FITT,” Hitachi’s comprehensive imaging technology which allows improvement in multi-slab MRA.
Benefit: 02 E x a m i n a t i o n | Easy Operation / Patient-centric Design
14
Opening up new possibilities in your daily routine.
Benefit: 03 D e c i s i o n M a k i n g | Attractive Cost of Ownership
2 FLAIR without RADAR (AX)
recist中英文对照全文

New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1。
1)新版实体瘤疗效评价标准:修订的RECIST指南(1。
1版本)Abstract摘要Background背景介绍Assessment of the change in tumour burden is an important feature of the clinical evaluation of cancer therapeutics:both tumour shrinkage (objective response) and disease progression are useful endpoints in clinical trials. Since RECIST was published in 2000,many investigators,cooperative groups,industry and government authorities have adopted these criteria in the assessment of treatment outcomes. However,a number of questions and issues have arisen which have led to the development of a revised RECIST guideline (version 1。
1). Evidence for changes, summarised in separate papers in this special issue,has come from assessment of a large data warehouse (〉6500 patients), simulation studies and literature reviews。
一体化PETMR在神经系统中的应用进展

综 述一体化PET/MR在神经系统中的应用进展马 璐,杨 斌综述,郑 玲,刁 强审校 [摘要] 一体化PET/MR集多模态、多参数、多种无创检查于一体的综合评估模式推动了现代精准医学的发展。
随着一体化PET/MR对神经系统数据的同步采集、多种优化校正、动态建模等技术的提高,进一步拓宽了临床及科研领域的应用。
文章主要就一体化PET/MR在神经系统中的应用优势、应用限制以及改进等方面进行综述。
[关键词] 一体化;PET/MRI;神经系统 [中图分类号] R445.2;R817 [文献标志码] A [文章编号] 1008 8199(2020)11 1209 05 [DOI] 10.16571/j.cnki.1008 8199.2020.11.017基金项目:国家自然科学基金(81790653)作者单位:210002南京,东部战区总医院(原南京军区南京总医院)放射诊断科[马 璐(医学硕士研究生)、杨 斌、郑 玲、刁 强]通信作者:刁 强,E-mail:Diaoqiang999@126.comApplicationprogressofintegratedPET/MRinnervoussystemMALu,YANGBinreviewing,ZHENGLing,DIAOQiangchecking(DepartmentofMedicalImaging,GeneralHospitalofEasternTheaterCommand,PLA,Nanjing210002,Jiangsu,China) [Abstract] TheintegratedPET/MR,acomprehensiveevaluationmodel,includingmulti-modes,multi-parametersandmul tiplenon-invasivetests,whichhaspromotedthedevelopmentofmodernprecisionmedicine.WiththeimprovementofintegratedPET/MRtechnologyinneuralsystem,suchasdatasimultaneouscollection,multipleoptimizationcorrection,dynamicmodelingandothertechnologies,itsapplicationinclinicalandscientificresearchfieldshasbeenfurtherbroadened.Thispaperreviewstheadvantages,limitationsandimprovementsofintegratedPET/MRinthenervoussystem. [Keywords] integrated;PET/MR;nervoussystem0 引 言 随着对磁场不敏感的硅光电倍增管(SIPM)的研发成功[1],使两个光子到达晶体的时间差可被时间分辨率提高1000倍的SIMP所测量,这种时间飞跃(timeofflow,TOF)技术可精确计算出正电子湮灭的位置,一体化PET/MR复合型影像设备通过将基于TOF技术的正电子发射型计算机断层扫描(positronemissioncomputertomography,PET)探测器整体进行静磁场屏蔽、射频屏蔽及r射线屏蔽后置入到磁共振(magneticresonanceimaging,MRI)扫描系统中,使其在同一呼吸、心电和指脉门控等信号下,一次扫描即可在时间、空间上真正实现解剖结构、功能、分子生化代谢的精确配准融合[2];这种实时、高分辨率、多参数的独特优势,为精准医学提供了利器,为绝对定量研究中枢神经系统疾病提供新方法[3]。
圣诞惊喜英语作文
圣诞惊喜英语作文It was a chilly December evening as the Johnson family gathered around the crackling fireplace in their cozy living room. The air was filled with the scent of freshly baked gingerbread cookies and the twinkling of the Christmas tree lights cast a warm glow throughout the room. Eight-year-old Emma sat on the floor, her eyes wide with anticipation as she watched her parents carefully place the final ornaments on the tree. Her younger brother, Ethan, was nestled on the sofa, clutching his favorite stuffed reindeer and humming along to the familiar Christmas carols playing softly in the background."Alright, the tree is all ready for Santa's visit!" Emma's father announced with a proud smile. Emma jumped up excitedly, racing over to the tree to admire the sparkling decorations. "Can we open one present tonight, please?" she begged, tugging on her mother's sleeve. Her mother chuckled and shook her head. "Not yet, sweetheart. You and Ethan need to be patient and wait until Christmas morning." Emma pouted, but she knew better than to argue.As the evening wore on, the family enjoyed a hearty meal of roasted turkey, mashed potatoes, and homemade cranberry sauce. Afterwards, they sipped hot cocoa and took turns reading passages from the classic Christmas tale, "A Christmas Carol." Emma and Ethan listened intently, their eyes shining with wonder at the story's magical elements.When it was finally time for bed, Emma and Ethan reluctantly said goodnight and trudged upstairs to their rooms, their little feet dragging with exhaustion. Emma plopped down on her bed, clutching her favorite stuffed animal - a fluffy white puppy named Snowflake. "I can't wait for tomorrow, Snowflake," she whispered, gazing out the frosty window at the glistening snowfall outside. "I wonder what surprises Santa has in store for us!"The next morning, Emma and Ethan bounded down the stairs, their pajamas rumpled and their hair tousled from sleep. They gasped in delight at the sight of the overflowing stocking and the towering pile of presents under the tree. "Look, Ethan! Santa came!" Emma cried, rushing over to the tree. Ethan giggled and clapped his hands excitedly, diving headfirst into the sea of brightly wrapped gifts.For the next hour, the children tore open present after present, their squeals of joy echoing throughout the house. Emma received a brand-new bike, a set of art supplies, and a beautiful porcelain doll.Ethan was thrilled to find a remote-controlled race car, a fuzzy teddy bear, and a box of building blocks. Their parents watched on, their hearts swelling with love and pride at the pure, unadulterated happiness on their children's faces.Once the frenzy of gift-opening had subsided, Emma and Ethan settled down to play with their new toys. Their father turned on the television, and the family gathered around to watch the annual Christmas parade. Emma was mesmerized by the colorful floats and the marching bands, while Ethan giggled at the silly costumes worn by the performers.As the parade drew to a close, their mother stood up and cleared her throat. "Alright, you two. I have one more surprise for you." Emma and Ethan perked up, their eyes shining with excitement. Their mother disappeared into the kitchen and returned a moment later, carrying a large, beautifully wrapped box. "Merry Christmas, my darlings!" she exclaimed, handing the box to the children.Emma and Ethan tore into the wrapping paper, their fingers trembling with anticipation. When they finally lifted the lid, they let out simultaneous gasps of delight. Inside the box was the most adorable puppy they had ever seen - a fluffy white bundle of energy with big brown eyes and a wagging tail. "Oh my gosh, it's a puppy!" Emma cried, scooping the puppy up in her arms and showering itwith kisses. Ethan giggled and reached out to pet the soft fur, his face lit up with pure joy.Their parents watched the children play with the puppy, their hearts overflowing with happiness. "What are you going to name him?" their father asked. Emma and Ethan looked at each other, their faces scrunched in concentration. "How about...Snowflake?" Emma suggested, and Ethan nodded enthusiastically. "Snowflake it is!" their mother exclaimed, clapping her hands.For the rest of the day, the Johnson family reveled in the joy of their new furry family member. Snowflake quickly became the center of attention, chasing after the children and snuggling up with them on the couch. Emma and Ethan took turns feeding him, bathing him, and playing fetch in the backyard. Their laughter and shrieks of delight filled the air, and their parents couldn't help but smile at the pure, unadulterated happiness on their children's faces.As the sun began to set, the family gathered around the table for a delicious Christmas dinner. They shared stories, laughed, and savored the delicious meal, all the while marveling at the incredible surprise that had been bestowed upon them. When the dishes were cleared and the children were tucked into bed, Emma and Ethan's parents exchanged a knowing glance, their hearts swelling with gratitude and love."This has been the best Christmas ever," Emma whispered to Snowflake as she drifted off to sleep, her arms wrapped tightly around the puppy. "I'm so glad Santa brought you to us." Snowflake let out a contented sigh and snuggled closer to Emma, his soft fur tickling her cheek. As Emma's eyes fluttered shut, she couldn't help but feel a sense of pure, unadulterated joy - a Christmas surprise that would stay with her for the rest of her life.。
ClinicallyProven
By Nadia Di Muzio, M.D., Radiotherapy Department(collaborators: Berardi G, Cozzarini C, Dell’Oca I, Motta M, Fodor A, Passoni P)San Raffaele Hospital, a nationally-recognized Scientific Institute, was the first radiotherapy department in Europe to offer TomoTherapy treatments in 2004. We chose the advanced technology to help us take our biomedical and clinical research even further. We demonstrated that hypofractionation and dose escalation can be administered safely and efficiently, especially when TomoTherapy is combined with metabolic imaging. Through clinical studies, we continue to demonstrate that combining TomoTherapy’s advanced IG/IMRT technology with PET/CT imaging allows for highly-advanced treatments that deliver significant patient benefit.Institution:San Raffaele Hospital Milan, Italy Clinically ProvenMetabolically-Guided TomoTherapy SMTreatments Advancing Cancer CareCHOOSING THE MOST ADVANCED TECHNOLOGY TO PURSUE A NEW IDEAWe view TomoTherapy as the most sophisticated technology for radiation treatment using external beams. For thepast seven years, our patients have benefited from helical treatment delivery and fully integrated megavoltage CT (MVCT) imaging for each of their daily treatment fractions. TomoTherapy’s design concept for IG-IMRT gives us the advanced technology needed to expand our research interest in the role of PET/CT in radiation oncology.Our TomoTherapy Hi·Art® is used with a PET/CT scanner, creating what we call “Metabolically-Guided TomoTherapy.” The combination provides excellent tumor definition, highly advanced treatment delivery and improved control of the patient’s position. In particular, this gives us the precision needed for hypofractionated treatment regimes.PROVING THE CONCEPT WITH PROSTATE STUDIESIn 2007, we published our first results on the positive effectof TomoTherapy in reducing toxicity of prostate cancer treatment 1, 2. One of the reasons for our success is that TomoTherapy is an excellent planning solution for prostate cancer. Our physics team has shown it to be highly efficient in a simultaneous integrated boost (SIB) scenario 3. Therefore, we were not surprised that our hypofractionated SIB approach for prostate cancer — delivering 71.4-74.2 Gy in 28 fractions — shows excellent results with regard to acute toxicity 4.Our experience in prostate cancer patients treated with hypofractionated TomoTherapy has demonstrated excellent results in terms of acute and late toxicity. No patients experienced acute rectal or upper intestinal toxicity greater than grade 1, and only 2% had late rectal toxicity. In addition, the three-year biochemical-free survival of 89% seems better than that reported in other studies in the literature.To learn more about this promising concept, a research project has been started to define molecular profiles indicative of better response to hypofractionated radiation therapy. The goal is greater efficacy and precision in patient selection. To do so, we will correlate semi-quantitative data provided by PET/CT to proteomic data, in order to find a possible relationship between the effects of radiotherapy on [11C]Choline uptake and proteomic characteristics.ESCALATING DOSESBecause TomoTherapy allows us to expand clinical opportunities of radiotherapy, we also conducted a feasibility study to understand whether it is safe to escalate dose to single or multiple highly radio-resistant dominant intra-prostatic lesions (DILs).Within a feasibility study, we simulated a TomoTherapy treatment delivering an SIB to one or two DILs in seven patients and found that safe escalation may be possible to at least 113 Gy without significant increase in the rectal normal tissue complication probability (NTCP). A Phase I–II study will allow us to investigate the clinical possibilities further 5.Another highlight is the [11C]Choline-PET-guided helical TomoTherapy that we perform in patients with abdomino-pelvic lymph nodal recurrent prostate cancer. With a mean follow-up of 26 months, all patients showed significant prostate-specific antigen (PSA) reduction and in many cases (50%) PSA became undetectable. Few cases experiencedSAN FAFFAELE HOSPITAL TOMOTHERAPY INSTALLATIONS2004FIRST TOMOTHERAPY® HI·ART®2007SECOND TOMOTHERAPY® HI·ART®2011FIRST TOMOTHERAPY TOMOHD™2012REPLACING FIRST HI·ART® WITH MORE ADVANCED TOMOHD™PROSTATERECTUMPANCREASGYNECOLOGYLUNGPITUITARYHEAD AND NECK SITES TREATEDgrade 1 or 2 acute toxicity and no late toxicities were recorded. A disease-free survival of 26 months, in the absence of any type of systemic therapy, is uncommonin metastatic prostate cancer 6.EXPANDING INNOVATIVE TREATMENTSTO MANY DISEASE SITESFollowing our successes with prostate treatments, we started studies on many different disease sites with the combination of TomoTherapy and PET/CT. Detailed information onour approach for rectal adenocarcinoma, head andneck, lung, malignant pleural mesothelioma, pancreas, gynecological, brain and cranio-spinal irradiation canbe found in the appendix.SUMMARYTomoTherapy has allowed us to demonstrate the viability of new, highly effective radiation oncology treatments that show real benefits for our patients. We are excited to continue our work collecting clinical outcomes data related to acute and late toxicity. The addition of our third TomoTherapy system, the more advanced TomoHD™ with new core technologies, will allow us to treat patients even faster — this will speed our research and potentially help even more patients around the world receive the advanced treatment care they deserve.APPENDIXRECTAL ADENOCARCINOMABetween 2007 and 2009, we enrolled 20 patients in a PhaseII study to investigate the effect of preoperative, moderately hypofractionated, image-guided TomoTherapy treatment concomitant to oxaliplatin and 5-FU in rectal adenocarcinoma. Preliminary results were promising, particularly in terms of low rate of acute toxicity 7.In order to further improve the complete pathologic control rate, we explored the possibility of delivering a concomitant boost. A retrospective estimation of rectal volume variations during the TomoTherapy treatment was performed (an overall average shrinkage of more than 50% was detected) and a reduced variation of rectal volume in the second half of the treatment suggested an advantage in delivering the concomitant boost during the last six fractions. Moreover,we decided to apply a boost to the residual tumor assessed by an intermediate treatment course CT/MR simulation. Preliminary results are encouraging 8.HEAD AND NECKWe published our first results on the positive effect of TomoTherapy treatments for the toxicity profile of head and neck cancer in 2006 9. Due to the capability to spare organs at risk and increase dose delivered to the target, TomoTherapy is an excellent solution for head and neck cancer, particularly in a simultaneous integrated boost (SIB) scenario 10 when administered concurrently with chemotherapy.To identify potentially radio-resistant tumor sub-volumesfor head and neck tumors, which could benefit from a dose escalation program, we use multimodality imaging (MRIand PET/CT) for the planning. We found that TomoTherapy enables us to achieve low acute toxicity while shortening the overall treatment time in radical treatment of patients with advanced head and neck cancer, and in an adjuvant setting.LUNGIn 2008 we published the results of a treatment planning comparison between conformal radiotherapy and helical TomoTherapy. We found that TomoTherapy is an excellent planning solution for locally advanced tumors, which usually involve large volumes 11. Due to its sophisticated organ at risk sparing capability, TomoTherapy also allows the delivery of hypofractionated treatments in patients with inoperable locally-advanced non-small-cell lung cancer (NSCLC). To fully use TomoTherapy’s capabilities for minimizing side effects, along with improved target definition, for treatment planning we evaluated lung perfusion using PET/CT and SPECT/CT imaging in order to spare functional lung as much as possible. In general we can say that TomoTherapy enables hypofractionation with an excellent toxicity profile and ashortened overall treatment time.In addition we obtained excellent results in hypofractionated TomoTherapy treatment of small lung lesions (primaryand metastatic). It is possible to deliver a high dose in afew fractions thanks to a 65% reduction of the irradiated surrounding tissue achieved by considering motion with the help of 4D PET/CT images. None of the treated patients experienced acute or late toxicity.MALIGNANT PLEURAL MESOTHELIOMAThere is no clear consensus on the optimal treatmentof malignant pleural mesothelioma (MPM). Recent developments in the field of intensity-modulated and image-guided radiotherapy have led radiation oncologiststo reconsider the role of radiotherapy in treating this disease. The role of FDG-PET/CT in the definition of the target volume in MPM treatment is not mentioned even in the most recent papers. Its prognostic value has been demonstrated however and some publications have shown that PET could play an important role in MPM diagnosis.Using this evidence we started a feasibility study of dose escalation with TomoTherapy, based on FDG-PET/CT images taken for planning purposes, with the patient in the treatment position. A first group of 12 consecutive MPM patients was treated with 56 Gy in 25 fractions to the Planning Target Volume (PTV). FDG-PET/CT simulation was always performed for these patients to include all positive lymph nodes and MPM infiltrations. Subsequently, a second group of 12 consecutive patients was treated with the same dose to the whole pleura while adding a simultaneous integrated boost of 62.5 Gy to the FDG-PET/CT positive areas.Good dosimetric results were obtained in both groups. No grade 3 (RTOG/EORTC) acute or late toxicities were reported in the first group; three cases of grade 3 late pneumonitis were registered in the second group, with the duration of symptoms being two to ten weeks. Median overall survival was eight months (1.2 to 50.5 months) and 20 months (4.3 to 33.8 months) from the beginning of radiotherapy, for groups I and II respectively (p= 0.19). A significant impact on local relapse from radiotherapy was seen (median time to local relapse of 8 versus 17 months; one-year local relapse-free rate of 16% versus 81%, p=0.003). In the second group, distant relapses were dominant, reproducing to some extent the result found in post-extra-pleural pneumonectomy radiotherapy with high-dose IMRT.PANCREASFor unresectable pancreatic cancer, contrast enhanced4D-PET/CT is helpful in definition of target volumes.The first results of our Phase I-II dose escalation trial on hypofractionated image-guided radiation therapy, in both radical and adjuvant pancreatic cancer, indicate an acceptable grade-3 acute toxicity rate, while providing stabilization or improvement of local control 12, 13.GYNECOLOGYAn exciting gynecology project will start shortly. We will investigate TomoTherapy versus RapidArc™ and static IMRT in gynecologic cancers, and also the use of TomoTherapy for brachytherapy substitution. Two protocols will be followed:• Protocol I: whole pelvis irradiation, comparing static IMRT with RapidArc™ and helical TomoTherapy to determinethe dosimetric differences among the three techniques,and the impact on acute and late toxicity in all cases.• Protocol II: SIB for PET/CT-positive lymph nodes in the pelvic or lomboaortic region, while treating the wholepelvis with or without the lomboartic region. For thisapproach, RapidArc™ and helical TomoTherapy willbe compared. Our hope is that the treatment-relatedmortality rate due to toxicity with standard radiotherapycan be reduced.BRAINHelical TomoTherapy has been a useful tool in treating skull base tumors. Since June 2005, we have treated 23 patients, all evaluated with computer-based perimetry for assessingtheir visual field. This was done prior to treatment and every six months after treatment, for the first two years of follow up, then on a yearly basis. In addition, MRI imaging was performed for treatment planning and every three months after treatment for evaluation during the first two years of follow up. After that, MRI imaging was performed every six months or yearly.In all cases, good PTV coverage was achieved (averageV95% = 96%) with an acceptable sparing of critical structures. Twenty-one patients showed stable disease at their last follow-up with only one extra-field recurrence for a patient with meningiomatosis, who was scheduled for a salvagere-irradiation with TomoTherapy. Visual function was evaluated with computerized campimetric assessment in15 of the 23 patients treated. In 11 of these 15 patients visual function was stable, while in four patients it improved. In one instance, a patient with a recurrence of atypical meningioma experienced vision loss the week before treatment. After TomoTherapy treatment and high-dose dexamethasone, her vision improved, being able to see 4/10 diopters in the eye contralateral to the recurrence. Furthermore, no moderateor severe acute or late toxicities have been reported. These promising results will be presented at the International Course of Neurosurgery for skull base tumors that will be held in San Raffaele Hospital in 2011.CRANIO-SPINAL IRRADIATIONAnother field of interest is the capability of helical TomoTherapy in cranio-spinal irradiation (CSI) for patients with primitive brain tumors at risk for spine seeding.Our series includes seven patients treated for disseminated ependymomas and medulloblastomas. All patients were adults. The advantage of helical TomoTherapy in performing CSI is the ability to remove the need for junctions in the treatment field and junction shifts used to avoid beams overlapping in the spine. Moreover, patients can be treated in the supine position and the daily MVCT allows the best setup check for these treatments. The preliminary results of our work were presented at the 2009 International Conference on Translational Research and Pre-Clinical Strategies in Radiation Oncology (ICTR) in Geneva, Switzerland.REFERENCES1 Cozzarini C et al. Significant Reduction of Acute T oxicity Following Pelvic irradiation with Helical T omotherapy in Patients with Localized Prostate Cancer. Radiother Oncol. 2007 Aug;84(2):164-70.2 Cozzarini C et al. Hypofractionated Adjuvant Radiotherapy with Helical T omotherapy After Radical Prostatectomy: Planning Data and T oxicity Results of a Phase I-II Study. Radiother Oncol. 2008 Jul;88(1):26-33.3 Fiorino C et al. Physics Aspects of Prostate T omotherapy: Planning Optimization and Image-guidance Issues. Acta Oncol. 2008;47(7):1309-16.4Di Muzio N et al. Phase I-II Study of Hypofractionated Simultaneous Integrated Boost with T omotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys. 2009 Jun1;74(2):392-8.5Maggio A, et al. Feasibility of Safe Ultra-high (EQD(2)>100 Gy) Dose Escalation on Dominant Intra-prostatic Lesions (DILs) by Helical T omotherapy. Acta Oncol. 2011Jan;50(1):25-34.6Alongi F et al. [11C]Choline-PET-guided Helical T omotherapy and Estramustine in a Patient with Pelvic-recurrent Prostate Cancer: Local Control and T oxicity ProfileAfter 24 Months. Tumori. 2010 Jul-Aug;96(4):613-7.7Passoni P et al. Preoperative, Moderately Hyperfractionated Radiotherapy with Image-guided T omoTherapy Concomitant to Chemotherapy in Rectal Adenocarcinoma: Early results of a Phase II Study. Int J Radiat Oncol Biol Phys, Vol 75, Number 3, Supplement, 2009.8Passoni P et al. Early Clinical Experience in Adaptive Image-guided T omoTherapy of Rectal Cancer. Int J Radiat Oncol Biol Phys. Volume 78, Number3, Supplement, 2010.9Fiorino C et al. Significant Improvement in Normal Tissue Sparing and T arget Coverage for Head and Neck Cancer by Means of Helical T omotherapy. Radiother Oncol. 2006 Mar;78(3):276-82.10Fiorino C et al. Simultaneous Integrated Boost (SIB) for Nasopharynx Cancer with Helical T omotherapy. A Planning Study. Strahlenther Onkol. 2007 Sep;183(9):497-505.11 Cattaneo GM et al. Treatment Planning Comparison Between Conformal Radiotherapy and Helical T omotherapy in the Case of Locally Advanced-stage NSCLC. Radiother Oncol. 2008 Sep;88(3):310-8.12Slim N et al. Hypofractionated T omotherapy with Concomitant Chemotherapy in Pancreatic Adenocarcinoma: Preliminary Result of a Phase I Study. Int J Radiat OncolBiol Phys, Volume 75, Number 3, Supplement, 2009.13Slim N et al. Hypofractionated Image-guided T omotherapy Concomitant to Capecitabine in Advanced Pancreatic Adenocarcinoma. Preliminary Result of a Phase II Study. Int J Radiat Oncol Biol Phys, Volume 78, Number 3, Supplement, 2010.© Copyright 2011 Accuray Incorporated. All Rights Reserved.The following words and logos as used herein are registered or common law trademarks or servicemarks of Accuray Incorporated in the United States and other countries: TomoTherapy; Reshaping Radiation Therapy; Hi·Art; TomoHD; CTrue; Every Patient, Every Day; and Tomo. All other trademarks are the property of their respective owners. TomoTherapy is a wholly owned subsidiary of Accuray Incorporated. M-CLN-028-0511。
移植胰腺病理学诊断标准及其进展

第13卷 第2期2022年3月Vol. 13 No.2Mar. 2022器官移植Organ Transplantation·Banff移植病理学·移植胰腺病理学诊断标准及其进展郭晖 明长生 陈实【摘要】 胰腺移植和胰肾联合移植是治疗1型糖尿病和部分2型糖尿病及其并发症导致的肾衰竭的最佳治疗方法。
胰腺移植的类型主要包括同期胰肾联合移植(SPK )、肾移植后胰腺移植(PAK )和单纯胰腺移植(PTA )。
在所有的胰腺移植类型中,对移植胰腺的活组织检查(活检)仍然是明确诊断其排斥反应并与其他并发症进行鉴别的最佳方法。
本文对移植胰腺活检的方法及其相关的研究进展、移植胰腺活检排斥反应诊断标准及其进展、移植胰腺主要的并发症及其病理学表现进行阐述,旨在为指导临床对上述并发症予以准确诊断,良好地保障移植胰腺和受者的长期存活提供参考。
【关键词】 同期胰肾联合移植(SPK );肾移植后胰腺移植(PAK );单纯胰腺移植(PTA );抗体介导的排斥反应(AMR );T 细胞介导的排斥反应(TCMR );供者特异性抗体(DSA );慢性移植物动脉血管病(CTA );移植后淋巴组织增生性疾病(PTLD )【中图分类号】R617,R36 【文献标志码】A 【文章编号】1674-7445(2022)02-0005-11DOI: 10.3969/j.issn.1674-7445.2022.02.005基金项目:中国医学科学院中央级公益性科研院所基本科研业务费专项资金(2019PT320014)作者单位:430030 武汉,华中科技大学同济医学院附属同济医院器官移植研究所 器官移植教育部重点实验室 国家卫生健康委员会器官移植重点实验室 中国医学科学院器官移植重点实验室作者简介:郭晖,研究方向为移植病理学基础与临床应用研究,Email :************** 通信作者:陈实,Email :**************【Abstract 】 Pancreas transplantation and pancreas-kidney transplantation are the optimal treatment for renal failure caused by type 1 diabetes mellitus, partial type 2 diabetes mellitus and their complications. Pancreas transplantation mainly includes simultaneous pancreas-kidney transplantation (SPK), pancreas transplantation after kidney transplantation (PAK) and pancreas transplantation alone (PTA). Among all types of pancreas transplantation, biopsy of pancreas allograft remains the best method for definitively diagnosing rejection and differentiate it from other complications. In this article, biopsy methods of pancreas allograft and related research progress, diagnostic criteria and research progress on rejection of pancreas allograft biopsy, and main complications and pathological manifestations of pancreas allograft were illustrated, aiming to provide reference for guiding the clinical diagnosis of the above mentioned complications and ensuring the long-term survival of pancreas allografts and recipients.【Key words 】 Simultaneous pancreas-kidney transplantation (SPK); Pancreas transplantation after kidney transplantation (PAK); Pancreas transplantation alone (PTA); Antibody-mediated rejection (AMR); T cell-mediated rejection (TCMR); Donor specific antibody (DSA); Chronic transplant arteriopathy (CTA); Posttransplant lymphoproliferative disease (PTLD)Diagnostic criteria and research progress on pancreas allograft pathology Guo Hui, Ming Changsheng, Chen Shi. Institute of Organ Transplantation, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Key Laboratory of Organ Transplantation of Ministry of Education, Key Laboratory of Organ Transplantation of National Health Commission of China, Key Laboratory of Organ Transplantation of Chinese Academy of Medical Sciences, Wuhan 430030, China Corresponding author: Chen Shi, Email :**************郭晖等.移植胰腺病理学诊断标准及其进展第2期·177·胰腺移植和胰肾联合移植是治疗1型糖尿病和部分2型糖尿病及其并发症导致的肾衰竭的最佳方法。
多发性肺结节非手术治疗的研究进展

[7]RamaswamyV.Pathologyofmucinousappendicealtumorsandpseud⁃omyxomaperitonei[J].IndianJSurgOncol,2016,7(2):258-267.[8]RizviSA,SyedW,ShergillR.Approachtopseudomyxomaperitonei[J].WorldJGastrointestSurg,2018,10(5):49-56.[9]中国抗癌协会腹膜肿瘤专业委员会,广东省抗癌协会肿瘤热疗专业委员会.中国腹腔热灌注化疗技术临床应用专家共识(2019版)[J].中华医学杂志,2020,100(2):89-96.[10]YanF,LinY,ZhouQ,etal.Pathologicalprognosticfactorsofpseud⁃omyxomaperitonei:comprehensiveclinicopathologicalanalysisof155cases[J].HumPathol,2020,97:9-18.[11]ZhouS,ZhaoH,HeX.Theprognosticimpactofpathologyonpatientswithpseudomyxomaperitoneiundergoingdebulkingsurgery:asys⁃tematicreviewandmeta⁃analysisofretrospectivestudies[J].FrontSurg,2020,7:554910.[收稿日期㊀2023-04-09][本文编辑㊀韦㊀颖]本文引用格式范仕嘉,万宇智,李成龙,等.以腹股沟疝为主要表现的腹膜假性黏液瘤一例[J].中国临床新医学,2023,16(9):971-973.㊀㊀[摘要]㊀肺癌是目前全球发病率和病死率较高的恶性肿瘤㊂人们越来越重视肺癌早期筛查㊂多发性肺结节(MPNs)与多原发肺癌(MPLC)关系密切㊂低剂量CT筛查肺癌发现,MPNs在人群中的检出率呈逐年增高趋势㊂目前MPNs治疗主要方式是手术切除,还有放射治疗㊁局部消融㊁分子靶向治疗㊁免疫治疗㊁化疗等非手术方式㊂该文对近年来MPNs非手术治疗的研究进展进行综述㊂㊀㊀[关键词]㊀多发性肺结节;㊀多原发肺癌;㊀非手术治疗;㊀综述㊀㊀[中图分类号]㊀R655 3㊀[文献标识码]㊀A㊀[文章编号]㊀1674-3806(2023)09-0973-05㊀㊀doi:10.3969/j.issn.1674-3806.2023.09.20Advancesinnon⁃operativetreatmentsofmultiplepulmonarynodules㊀QITao,LILun,CHUHeng,etal.GraduateSchoolofDalianMedicalUniversity,Liaoning116044,China㊀㊀[Abstract]㊀Atpresent,lungcancerisamalignanttumorwithrelativelyhighmorbidityandmortalityintheworld.Peoplepaymoreandmoreattentiontotheearlyscreeningoflungcancer.Multiplepulmonarynodules(MPNs)arecloselyrelatedtomultipleprimarylungcancer(MPLC).MPNsareusuallyfoundinlow⁃dosecomputedtomography(LDCT)screeningforlungcancer,andthedetectionrateofMPNsinthepopulationincreasesyearbyyear.Currently,themaintreatmentmethodsforMPNsaresurgicalresectionandothernon⁃operativetreatmentmethodswhichincluderadiotherapy,localablation,moleculartargetedtherapy,immunotherapyandchemotherapy.Thispaperreviewstheresearchprogressinthenon⁃operativetreatmentsofMPNsinrecentyears.㊀㊀[Keywords]㊀Multiplepulmonarynodules(MPNs);㊀Multipleprimarylungcancer(MPLC);㊀Non⁃operativetreatment;㊀Review㊀㊀肺癌早期筛查越来越受到重视,多家权威医学组织均推荐低剂量CT(low⁃dosecomputedtomography,LDCT)作为肺癌的筛查手段[1]㊂LDCT筛查肺癌时,肺结节在人群中的总检出率可达16 02% 26 32%,其中多发性肺结节(multiplepulmonarynodules,MPNs)超过20%,肺癌的检出率为0 72% 1 23%[2⁃4]㊂MPNs是一种与肺癌密切相关的疾病,有研究发现,肺多发亚实性结节是同时性多原发肺癌(simultaneousmultipleprimarylungcancer,sMPLC)的最常见表现之一[5],肺多发磨玻璃结节(ground⁃glassnodules,GGNs)手术切除的病灶多数为癌前病变(占98 9%)或腺癌[6]㊂经3 6个月随访后仍持续存在的亚实性结节多提示癌前病变或恶性病变[7],积极的外科干预十分重要㊂手术是MPNs常用且有效的治疗方法,但最佳手术策略仍有争议,应遵循优先切除主病灶并兼顾次病灶的原则,在根治肿瘤的前提下尽可能多地保留肺实质[8]㊂选择何种术式需综合考虑肺结节数目㊁大小㊁分布特点㊁医师习惯及手术对肺功能的影响等因素决策㊂对于双侧MPNs,单孔胸腔镜同期手术切除是可行且有效的[9]㊂因此,严格把握手术指征,个体化设计手术思路,才能使患者获得最大收益㊂由于MPNs各个病灶具有组织异质性[10],未切除的残余结节仍存在进展可能,术后需要定期监测并适时干预㊂鉴于MPNs惰性生长的特点,激进的手术干预是不可取的,而且单纯手术切除无法满足所有MPNs患者的临床治疗需求㊂对于肺功能储备不足,难以耐受手术或不愿接受手术的患者,非手术治疗就成了可供选择的干预措施㊂目前常用的非手术治疗手段包括立体定向全身放射治疗(stereotacticbodyradiationtherapy,SBRT)㊁消融治疗㊁分子靶向治疗㊁免疫治疗等㊂本文在回顾相关文献的基础上概述MPNs的治疗手段,重点阐述非手术治疗的指征㊁方法及疗效,期望能为患者提供更好的个体化治疗方案㊂1㊀MPNs的定义及分类MPNs是指在肺内出现至少2个直径均ɤ3cm的局灶性㊁类圆形㊁密度增高的病灶,在影像学上多呈磨玻璃样阴影㊂MPNs在病理学上常提示早期多原发肺腺癌[8],也可能是非肿瘤性或其他原发性恶性肿瘤的转移性肿瘤㊂多原发肺癌(multipleprimarylungcancer,MPLC)是指在肺内同时或先后出现至少2个原发性肺癌灶,而这些病灶在解剖和起源上均相互独立,临床上,MPLC又可根据2次诊断的时间间隔分为sMPLC与异时性多原发肺癌(metachronousmultipleprimarylungcancer,mMPLC)[11]㊂MPNs根据结节密度可分为纯实性肺结节和亚实性肺结节㊂亚实性肺结节可进一步分为:(1)非实性结节,常称为GGNs或磨玻璃病灶,即不含有任何实性成分;(2)部分实性结节(part⁃solidnodules,PSNs),即同时兼有实性和磨玻璃的成分㊂其中PSNs的恶性概率最高,其次为纯GGNs及实性结节[12⁃13]㊂然而,以上分类方法仍存在较多不足,临床上需要综合考虑结节的大小㊁数量㊁位置分布㊁影像学特征及浸润范围等因素制定治疗策略㊂因此,迫切需要更符合临床需求的MPNs分类方式来帮助评估肺结节㊂2㊀非手术治疗2 1㊀放射治疗㊀SBRT也称为立体定向消融放射治疗,该疗法更适用于空间上集中的结节,具有良好的局部控制及副作用小的优点,但对分散的结节效果较差㊂此外,质子束治疗也可用于MPLC患者,但其价格昂贵限制了临床应用㊂‘中华医学会肺癌临床诊疗指南(2022版)“[1]指出,对于不能或不愿接受手术的Ⅰ期非小细胞肺癌(non⁃small⁃celllungcarci⁃noma,NSCLC)患者,SBRT是首选治疗方法(1类推荐证据),已成为拒绝手术或无法手术的早期肺癌患者的标准治疗方案,是T3N0M0及同时性多原发NSCLC的相对适应证㊂已有研究证明SBRT与早期肺癌手术切除具有相似的预后效果[14],SBRT应用于MPLC患者时也可实现良好的局部控制和长期生存率[15]㊂另外有学者[16]报道,对于经手术切除原发性肺癌后进展为MPLC的患者,SBRT相比于广泛的根治性外科手术有更好的疗效㊂一项研究验证了为单个肿瘤设计的SBRT方案治疗NSCLC肺内转移的可行性,SBRT可以提高肺部转移性肿瘤患者的生存率[17]㊂然而,SBRT治疗多发性肺部病变的剂量限制问题尚未明确㊂当SBRT治疗ȡ2个肺部靶点(尤其是涉及双肺)时,需要特别考虑剂量问题㊂隔天治疗或分期治疗或许能降低肺毒性风险[18]㊂总之,为了尽可能多地保留正常肺实质,提高患者的可耐受性,SBRT单独或与手术等其他方式联合是治疗MPNs患者的合理选择㊂因此,仍需要更多相关研究数据来证实SBRT在MPNs治疗中的积极作用㊂2 2㊀热消融治疗㊀热消融是利用热产生的生物学效应直接导致病灶组织中的肿瘤细胞发生不可逆损伤或凝固性坏死的一种治疗技术,是肺部疾病局部治疗的常用手段,包括射频消融(radiofrequencyablation,RFA)㊁微波消融(microwaveablation,MWA)㊁冷冻消融等,具有创伤小㊁安全性高㊁可重复等优点㊂研究证明,手术联合热消融是治疗肺部多灶性GGNs型腺癌的有效方案[19]㊂热消融治疗周围型MPNs时可适用于以下情况[20⁃21]:(1)因心肺功能受限㊁高龄难以耐受手术或拒绝手术;(2)手术切除后又新发的结节或遗留结节而患者无法耐受或拒绝再次手术;(3)各种原因导致的胸膜腔闭锁或重度胸膜粘连;(4)单肺或一侧肺缺如;(5)经心理或药物治疗无法缓解的重度焦虑;(6)消融MPNs的主病灶后,其余病灶视发展情况再消融㊂2 2 1㊀RFA治疗㊀RFA是目前应用最为广泛的肿瘤消融技术,可以在几乎无肺功能受损的同时有效去除局部肿瘤组织㊂当射频温度升至60ħ以上时,能使细胞内外水分蒸发㊁干燥㊁固缩脱落,造成无菌性坏死,进而达到治疗目的㊂RFA治疗肺GGNs的安全性和临床疗效已得到证实[22]㊂Li等[23]研究表明,RFA和褪黑素联合治疗可以最大限度地减少肺功能损伤,降低未消融区域结节恶性转化或扩大的可能性,极大地改善早期肺多发癌灶患者的临床结果,为早期恶性MPNs的治疗提供了新的微创策略㊂尽管通过RFA可以局部消融癌灶,但并未改变人体的肿瘤微环境和代谢重编程㊂因此,单纯RFA在治疗早期肺癌合并多发GGNs时同样面临残余结节再增大或复发可能㊂2 2 2㊀MWA治疗㊀MWA是利用电磁方法,依靠偶极分子(如水分子)的旋转产生热量破坏肿瘤组织㊂灭活的肿瘤组织还可产生热休克蛋白,刺激机体的免疫系统,达到抑制肿瘤细胞扩散的作用㊂与RFA相比,MWA具有消融速度快㊁热沉效应小㊁消融区大㊁降低对组织阻抗的敏感性以及同时使用多个天线等优点[24]㊂对于最大径>3cm(尤其是>5cm)的肺部病变,MWA的疗效明显优于RFA㊂此外,多个MWA天线能定位到目标病变中并同时激活,可以使接近球形的消融区域最大化㊂一项研究结果显示,电视辅助胸腔镜手术与MWA在治疗肺GGNs的3年总生存期㊁局部无进展生存率和癌症特异性生存率等方面有相似结果,且MWA的费用明显降低,住院时间更短[25]㊂Ni等[26]研究纳入103例NSCLC行肺癌根治术后再次复发患者,经过143次MWA,最终仅20例(占19 4%)患者出现远处转移㊂结果表明,对于NSCLC根治术后复发的肺结节,MWA是一种有效㊁安全的治疗方法㊂Qu等[27]探讨了一种新技术 电磁导航支气管镜引导下MWA联合单侧电视辅助胸腔镜手术治疗多发GGNs患者的安全性和可行性㊂针对11例患者中的37个病灶,其中21个病灶经MWA,16个病灶经手术切除㊂仅1例患者出现轻微并发症,对症治疗后顺利出院,其余患者无其他严重并发症及手术相关死亡,随访期间均未发生局部转移或复发㊂消融治疗最严重的并发症有出血㊁气胸㊁胸腔内出血及支气管胸膜瘘㊂电磁导航支气管镜可以通过自然腔隙精准引导至全肺任何位置,显著减少并发症的发生率㊂但该研究对患者的随访时间较短,长期预后仍需进一步验证㊂2 2 3㊀冷冻消融治疗㊀常用的冷冻消融技术包括氩氦冷冻消融和液氮冷冻消融㊂通过急速温度梯度变化可以导致[22]:(1)靶组织蛋白质变性;(2)细胞内外渗透压改变和 结冰 效应造成细胞裂解;(3)微血管栓塞引起组织缺血坏死等㊂通过CT或MRI观察到的 冰球 可以将消融区域与肿瘤边界进行区分,准确测定冷冻的边界㊂与RFA相比,冷冻消融不会导致大量的胶原蛋白被破坏㊂因此,当体内存在金属植入物,或病灶邻近神经㊁大血管等重要脏器无法安全实施RFA和MWA时,冷冻消融或许是一个更好的选择[28]㊂然而,目前仅有少量临床报道将冷冻消融技术应用于MPNs的治疗㊂Kim等[29]报道了1例多发GGNs的肺癌患者在多次手术切除后仍然存在的纯GGNs进行冷冻消融的初步经验㊂经过6个月的随访,位于左肺下叶5mm的纯GGNs被成功冷冻消除且无复发㊂另有涉及28例GGNs患者中35枚结节的报道显示,在接受CT引导下经皮冷冻消融后,所有患者的GGNs均被成功消融,除出现气胸㊁痰中带血,均无其他严重并发症,术后1个月肺功能恢复>95%,随访36个月无复发[30]㊂此研究表明CT引导下经皮冷冻消融治疗多发GGNs是可行㊁安全㊁有效的㊂总之,冷冻消融是多发GGNs有效的辅助治疗策略,可以不经额外的手术降低残余GGNs发展为晚期癌症的可能性,其更多积极作用仍需要进一步的前瞻性研究和长期随访㊂2 3㊀分子靶向治疗㊀分子靶向治疗已成功应用于具有驱动致癌基因的癌症治疗[31]㊂MPLC的表皮生长因子受体(epidermalgrowthfactorreceptor,EGFR)突变率在亚洲患者中占比可达45 8% 76 0%[32]㊂因此,对于无法手术的MPLC患者,靶向治疗可行,尤其是EGFR靶向酪氨酸激酶抑制剂(tyrosinekinaseinhib⁃itors,TKIs)㊂Ye等[33]报道了1例靶向治疗MPLC的病例,患者表现出异质性EGFR和K⁃ras突变阳性以及对吉非替尼治疗的不同反应,接受一段时间吉非替尼治疗后仍无法手术切除所有病灶㊂考虑到多发性病变的不同反应,嘱患者继续口服吉非替尼治疗对其敏感的双侧GGNs病变,同时手术切除对吉非替尼不敏感的病灶,病情完全缓解且1 5年内无进展㊂该研究证明了靶向治疗在MPLC多学科管理中的潜在作用,主病灶手术切除联合EGFR⁃TKIs治疗残余病灶可能是实现长期疾病控制的合理方法㊂Aredo等[34]报道了1例具有不同EGFR及RET突变的MPLC患者的治疗经验,奥希替尼和其他新靶向药物(如阿来替尼)的组合治疗具有不同分子特征的MPLC是有效的和可耐受的㊂因此,携带多种驱动基因突变的MPLC患者可能受益于靶向药物的组合,治疗决策应仔细考虑这些药物的安全性,以便为MPLC患者制定个体化靶向治疗方案㊂由于MPLC中不同肿瘤之间具有不同分子特征,活检或切除病变的基因突变测试结果不能完全反映肺内所有病变的基因情况[10],且驱动基因突变的差异率相对较高,有文献报道可达80 0% 92 1%[35],这可能会极大地限制靶向治疗在MPNs中的应用㊂挽救性靶向治疗的最佳治疗持续时间尚不清楚,这些新的靶向药物的长期副作用也有待研究㊂靶向治疗仍然是一种合理的替代策略,需要更多的多中心前瞻性随机对照试验来证实EGFR⁃TKIs在治疗MPNs中的疗效㊂2 4㊀免疫治疗㊀近年来,许多免疫检查点抑制剂(immunecheckpointinhibitors,ICIs)已被批准用于治疗晚期肺癌,特别是靶向程序性死亡配体1(programmeddeathligand1,PD⁃L1)或细胞程序性死亡受体1(programmedcelldeathprotein1,PD⁃1)的治疗性抗体,目前是无驱动致癌基因的晚期NSCLC患者一线治疗的支柱㊂PD⁃L1在肿瘤细胞中的表达是选择ICIs治疗患者的最重要的生物标志物㊂ICIs对sMPLC患者有良好的疗效和安全性[36],然而,ICIs对MPNs中不同组织学类型的结节是否有效仍未知㊂有研究报道了1例PD⁃L1抑制剂成功治疗mMPLC的病例,但患者对PD⁃1抑制剂耐药,这提示PD⁃L1治疗MPLC可能比PD⁃1有更好的效果[37]㊂此外,MPLC的多组学分析表明,由于不同病变之间基因组改变和免疫微环境的差异,单独使用PD⁃1或PD⁃L1抑制剂可能不是MPLC的最佳治疗策略[38],ICIs的联合应用可为mMPLC患者提供潜在的治疗方案[37]㊂另一项研究提出,在原发NSCLC用ICIs控制良好的情况下,应对第二原发NSCLC进行手术治疗[39]㊂有报道显示,ICIs在治疗不可切除的表现为GGNs的sMPLC时取得了良好结果[40]㊂Zhang等[38]测试了抗PD⁃L1药物阿替利珠单抗作为MPLC患者新辅助治疗的疗效,并观察每个病灶的治疗反应,结果显示实体结节显著缩小,而另外2个亚实体结节无变化㊂对于免疫疗法,仍有许多问题亟待解决,如是否存在最佳生物标志物,以及如何平衡单一疗法和联合疗法之间的有效性㊁成本和安全性问题㊂由于不同病变之间基因组改变和免疫微环境的差异,ICIs在MPLC新辅助或辅助治疗中的应用具有挑战性,需要进一步使用多组学分析来阐明GGNs的进化和免疫治疗的效果㊂2 5㊀化疗㊀化疗已不限于全身静脉途径,晚期肺癌患者也可采用支气管动脉灌注和栓塞等局部治疗方式㊂晚期MPLC患者如肺内多个病灶具有相同的组织学类型,可参考肺癌美国国立综合癌症网络(NationalComprehensiveCancerNetwork,NCCN)指南制定化疗方案;目前暂无明确的化疗方案指导组织学类型不同的晚期MPLC的治疗㊂另外,多发肺GGNs呈惰性生长趋势,适合采取长期随诊观察的治疗策略,而化疗对增殖旺盛及幼稚细胞更为敏感,因此化疗不适用于MPNs㊂一项回顾性研究通过单变量Cox回归和倾向性评分匹配分析证明了化疗对第二原发性肺癌有显著疗效[31]㊂但到目前为止,还没有关于在MPLC患者中使用化疗的随机试验㊂3㊀结语目前,MPNs的诊断与治疗仍未达成统一指南,这为后续更深入的研究带来了一定困难㊂对于经过长期随访怀疑恶性的结节,及早的外科干预十分必要㊂临床医师要科学把握干预时机,制定对患者有益的个体化方案㊂多学科诊疗模式规范化诊疗受到更多的关注,手术与消融㊁放射㊁靶向㊁免疫等非手术疗法的联合应用或将成为新的研究热点㊂参考文献[1]中华医学会肿瘤学分会,中华医学会杂志社.中华医学会肺癌临床诊疗指南(2022版)[J].中华医学杂志,2022,102(23):1706-1740.[2]FanL,WangY,ZhouY,etal.Lungcancerscreeningwithlow⁃doseCT:baselinescreeningresultsinShanghai[J].AcadRadiol,2019,26(10):1283-1291.[3]HeYT,ZhangYC,ShiGF,etal.RiskfactorsforpulmonarynodulesinnorthChina:aprospectivecohortstudy[J].LungCancer,2018,120:122-129.[4]田㊀田,魏东华,徐叶红,等.2015-2019年合肥市城市居民肺癌筛查结果分析[J].中华肿瘤防治杂志,2022,29(23):1653-1658.[5]HuoJW,LuoTY,HeXQ,etal.Radiologicalclassification,gene⁃mutationstatus,andsurgicalprognosisofsynchronousmultiplepri⁃marylungcancer[J].EurRadiol,2022,32(6):4264-4274.[6]HattoriA,MatsunagaT,TakamochiK,etal.Surgicalmanagementofmultifocalground⁃glassopacitiesofthelung:correlationofclinico⁃pathologicandradiologicfindings[J].ThoracCardiovascSurg,2017,65(2):142-149.[7]BorghesiA,MicheliniS,GolemiS,etal.Whatᶄsnewonquantita⁃tiveCTanalysisasatooltopredictgrowthinpersistentpulmonarysub⁃solidnodules?Aliteraturereview[J].Diagnostics(Basel),2020,10(2):55.[8]史文松,胡玉缀,王㊀慧,等.肺多发结节与混合磨玻璃结节的应对策略解析[J].医学与哲学,2022,43(8):59-61,66.[9]袁晓龙,闫云龙,刘㊀建,等.单孔胸腔镜同期治疗双肺多发肺结节的效果分析[J].中国临床新医学,2023,16(5):497-500.[10]LiaoCC,LinYS,LinYC,etal.Ararecaseofsynchronousmultipleprimarylungcancerwithdifferentresponsestogefitinib[J].RespirMedCaseRep,2020,31:101270.[11]TianH,BaiG,YangZ,etal.Multipleprimarylungcancer:updatesofclinicalmanagementandgenomicfeatures[J].FrontOncol,2023,13:1034752.[12]FuF,ZhangY,WenZ,etal.DistinctprognosticfactorsinpatientswithstageⅠnon⁃smallcelllungcancerwithradiologicpart⁃solidorsolidlesions[J].JThoracOncol,2019,14(12):2133-2142.[13]LaiJ,LiQ,FuF,etal.Subsolidlungadenocarcinomas:radiological,clinicalandpathologicalfeaturesandoutcomes[J].SeminThoracCardiovascSurg,2022,34(2):702-710.[14]MiyazakiT,YamazakiT,SatoS,etal.Surgeryorstereotacticbodyradiotherapyformetachronousprimarylungcancer?Apropensityscorematchinganalysis[J].GenThoracCardiovascSurg,2020,68(11):1305-1311.[15]ZhaoL,LiuC,XieG,etal.Multipleprimarylungcancers:anewchallengeintheeraofprecisionmedicine[J].CancerManagRes,2020,12:10361-10374.[16]DongB,ChenR,ZhuX,etal.Comparisonofstereotacticbodyradia⁃tiontherapyversussurgeryformultipleprimarylungcancersafterpriorradicalresection:amulticenterretrospectivestudy[J].ClinTranslRadiatOncol,2023,40:100601.[17]ChmuraS,WinterKA,RobinsonC,etal.Evaluationofsafetyofster⁃eotacticbodyradiotherapyforthetreatmentofpatientswithmultiplemetastases:findingsfromtheNRG⁃BR001phase1trial[J].JAMAOncol,2021,7(6):845-852.[18]MilanoMT,MihaiA,KangJ,etal.Stereotacticbodyradiotherapyinpatientswithmultiplelungtumors:afocusonlungdosimetriccon⁃straints[J].ExpertRevAnticancerTher,2019,19(11):959-969.[19]LiuB,ZhangY,SuL,etal.Treatmentoptionsforpulmonarymul⁃tifocalgroundglassopacitytypeadenocarcinoma:surgerycombinethermalablation?[J].JIntervMed,2020,3(4):180-183.[20]LiuB,YeX.Managementofpulmonarymultifocalground⁃glassnod⁃ules:howmanyoptionsdowehave?[J].JCancerResTher,2020,16(2):199-202.[21]TaftiBA,GenshaftS,SuhR,etal.Lungablation:indicationsandtechniques[J].SeminInterventRadiol,2019,36(3):163-175.[22]谭晓刚,刘宝东.射频消融治疗肺磨玻璃结节的临床价值[J].中国肺癌杂志,2021,24(10):677-682.[23]LiM,HaoB,ZhangM,etal.Melatoninenhancesradiofrequency⁃inducedNKantitumorimmunity,causingcancermetabolismrepro⁃grammingandinhibitionofmultiplepulmonarytumordevelopment[J].SignalTransductTargetTher,2021,6(1):330.[24]NiY,XuH,YeX.Image⁃guidedpercutaneousmicrowaveablationofearly⁃stagenon⁃smallcelllungcancer[J].AsiaPacJClinOncol,2020,16(6):320-325.[25]HanX,WeiZ,ZhaoZ,etal.Costandeffectivenessofmicrowaveablationversusvideo⁃assistedthoracoscopicsurgicalresectionforground⁃glassnodulelungadenocarcinoma[J].FrontOncol,2022,12:962630.[26]NiY,PengJ,YangX,etal.Multicentrestudyofmicrowaveabla⁃tionforpulmonaryoligorecurrenceafterradicalresectionofnon⁃small⁃celllungcancer[J].BrJCancer,2021,125(5):672-678.[27]QuR,TuD,HuS,etal.Electromagneticnavigationbronchoscopy⁃guidedmicrowaveablationcombinedwithuniportalvideo⁃assistedtho⁃racoscopicsurgeryformultiplegroundglassopacities[J].AnnThoracSurg,2022,113(4):1307-1315.[28]张㊀肖,肖越勇,李成利.影像学引导下肺结节冷冻消融专家共识(2022版)[J].中国介入影像与治疗学,2022,19(1):2-6.[29]KimKY,JinGY,HanYM,etal.Cryoablationofasmallpulmonarynodulewithpureground⁃glassopacity:acasereport[J].KoreanJRadiol,2015,16(3):657-661.[30]李向阳,穆㊀峰,陈继冰,等.CT引导下经皮冷冻消融治疗肺磨玻璃结节的研究[J].介入放射学杂志,2021,30(10):1072-1076.[31]WangM,HerbstRS,BoshoffC.Towardpersonalizedtreatmentapproa⁃chesfornon⁃small⁃celllungcancer[J].NatMed,2021,27(8):1345-1356.[32]YangY,YinW,HeW,etal.Phenotype⁃genotypecorrelationinmul⁃tipleprimarylungcancerpatientsinChina[J].SciRep,2016,6:36177.[33]YeC,WangJ,LiW,etal.Novelstrategyforsynchronousmultipleprimarylungcancerdisplayinguniquemolecularprofiles[J].AnnThoracSurg,2016,101(2):e45-e47.[34]AredoJV,DiehnM,BerryGJ,etal.TargetedtreatmentofmultipleprimarylungcancersharboringdistinctEGFRorRETalterations:acasereport[J].ClinLungCancer,2021,22(5):e673-e677.[35]QuR,TuD,PingW,etal.SynchronousmultiplelungcancerswithlymphnodemetastasisanddifferentEGFRmutations:intrapulmo⁃narymetastasisormultipleprimarylungcancers?[J].OncoTar⁃getsTher,2021,14:1093-1099.[36]XuL,ShiM,WangS,etal.Immunotherapyforbilateralmultiplegroundglassopacities:anexploratorystudyforsynchronousmultipleprimarylungcancer[J].FrontImmunol,2022,13:1009621.[37]LinX,QiuG,LiF,etal.Casereport:ararecaseofmetachro⁃nousmultipleprimarylungcancersinapatientwithsuccessfulman⁃agementbyswitchingfromanti⁃PD⁃1therapytoanti⁃PD⁃L1therapy[J].FrontImmunol,2021,12:683202.[38]ZhangC,YinK,LiuSY,etal.Multiomicsanalysisrevealsadis⁃tinctresponsemechanisminmultipleprimarylungadenocarcinomaafterneoadjuvantimmunotherapy[J].JImmunotherCancer,2021,9(4):e002312.[39]TakamoriS,MatsubaraT,HaratakeN,etal.Surgicallyresectedsecondprimarylungadenocarcinomaafterpembrolizumabadminis⁃tration[J].AnnThoracSurg,2020,110(5):e377-e379.[40]WuS,LiD,ChenJ,etal.TailingeffectofPD⁃1antibodyresultsintheeradicationofunresectablemultipleprimarylungcancerpresen⁃tingasground⁃glassopacities:acasereport[J].AnnPalliatMed,2021,10(1):778-784.[收稿日期㊀2023-04-27][本文编辑㊀韦㊀颖]本文引用格式亓㊀涛,李㊀论,褚㊀恒,等.多发性肺结节非手术治疗的研究进展[J].中国临床新医学,2023,16(9):973-977.。
羟基乙基羧基螺吡喃衍生物对有机胺的识别研究
收稿日期:2020-10-14基金项目:山东省自然科学基金面上项目(ZR2018MB011)作者简介:薛 瑞(1993—),女,山东德州人,硕士研究生,主要从事功能材料研究;通信作者:田进涛(1971—),工学博士,副教授,硕士生导师,主要从事光功能材料研究。
羟基/乙基/羧基螺吡喃衍生物对有机胺的识别研究薛 瑞,田进涛(中国海洋大学材料科学与工程学院,山东青岛 266100)摘要:研究了三种带有不同端基的螺吡喃衍生物对四类有机胺的变色和发光识别。
结果表明:通过辨析紫外-可见吸收光谱和荧光发射光谱,三种螺吡喃衍生物能够较好地区分四类有机胺。
对识别产物的分析表明,三种螺吡喃与第一类及第二类有机胺发生了不可逆的化学反应,与第三类有机胺之间是可逆的酸致变色作用,与第四类有机胺之间不发生较强的相互作用。
关键词:螺吡喃衍生物;紫外-可见吸收光谱;荧光发射光谱;有机胺中图分类号:O626.1 文献标识码:A 文章编号:1008-021X(2020)02-0035-03RecognitionsofOrganicAminesViaSpiropyransoftheSPOH/SPET/SPCOOHXueRui,TianJintao(SchoolofMaterialsScienceandEngineering,OceanUniversityofChina,Qingdao 266100,China)Abstract:ThreekindsofspiropyransoftheSPOH/SPET/SPCOOHwereappliedtorecognizeorganicamines.Theresultsshowedthatthespiropyranscaneffectivelydividetotally16kindsoforganicaminesintofourclassesbydistinguishingtheUV-Visspectraandthefluorescenceemissionspectra.Theexplorationsoftherecognitionmechanismshowedthatirreversiblechemicalreactionsoccurredbetweenthespiropyransandaliphaticprimaryamines/aromaticprimaryamineswhileinthecasesofaliphaticsecondarytertiaryaminesitisareversibleacid-inducedprocess.Nostronginteractionoccurredbetweenthespiropyransandaromaticsecondarytertiaryamines.Keywords:spiropyranderivative;ultraviolet-visible(UV-Vis)absorptionspectrum;fluorescenceemissionspectrum;organicamines 螺吡喃(Spiropyran)类化合物是最早研究的光致异构化材料[1-2],在光激发下可发生闭环体(Spiropyran,SP)与开环体部花菁(Merocyanine,MC)之间的可逆转换[3-4]。
库欣综合征

库欣综合征
肾上腺分泌的激素
肾上腺皮质
球状带---盐皮质激素(醛固酮) 束状带---糖皮质激素 网状带---性激素 肾上腺髓质 儿茶酚胺 髓质素
肾上腺疾病
o 皮质 功能亢进 功能减退 先天性肾上腺皮质增生 肾上腺意外瘤 o 髓质 嗜铬细胞瘤 肾上腺髓质增生 神经母细胞瘤神经节细胞瘤
糖皮质激素的生理作用
Female 11 1
Male 2 5 3
1
2 1 1
1
Pancreatic carcinoma
Colonic carcinoma Phaechromocytoma Gall bladder carcinoma Total 1 16 1
1
1
16
临床表现
一、皮质醇过多引起的表现 1、脂肪代谢紊乱和脂肪重新分布 2、蛋白分解加速, 合成减少 3、葡萄糖利用减少,糖原异生作用增加 4、电解质紊乱 5、GH分泌减少,作用受抑制 6、性腺功能受抑制 7、精神异常 8、抵抗力下降 二、 其他激素分泌过多的临床表现 1、雄激素过多 2、盐皮质激素过多 3、ACTH过多 三、 肿瘤本身引起的临床表现 1、腹块 2、蝶鞍扩大 3、异源性ACTH综合症引起的局部症状(肺癌、支气管类癌、胸腺癌等)
o
Causes of hypercortisolism
Physiological states Pregnancy Stress Chronic excessive exercise Malnutrition Pathological states Cushing's syndrome Diabetes mellitus Hyperthyroidism Severe chronic disease Glucocorticoid resistance Psychological states Anorexia nervosa Panic disorder Melancholic depression Obsessive-compulsive disorder
瞬态磁共振弹性成像的仿真与算法研究

瞬态磁共振弹性成像的仿真与算法研究朱霞丽;向馗;李炳南【摘要】磁共振弹性成像技术可以量化人体组织弹性属性。
磁共振弹性成像的弹性波激励方式有稳态和瞬态两种。
由于人体组织的特殊性,弹性波在组织中传播情况复杂。
文章通过建立一个磁共振弹性成像的有限元仿真平台,对瞬态磁共振弹性成像技术进行数值建模,并针对瞬态磁共振弹性成像设计了基于到达时间的弹性重构算法。
通过 MATLAB编程处理仿真得到的瞬态磁共振弹性成像数据,最终导出瞬态磁共振弹性成像的结果。
数值平台仿真的稳态和瞬态磁共振弹性成像对比实验表明,瞬态磁共振弹性成像对于反射和衍射具有较好的抗干扰能力,对于深处的小尺寸组织,具有较高的灵敏度和较好的精准度,而基于到达时间的算法能够实现瞬态磁共振弹性成像的弹性重构。
%Magnetic resonance elastography (MRE) can noninvasively quantify tissue elastic properties. There are two kinds of dynamic actuation in MRE, namely harmonic excitation and transient excitation. Due to the complexity of human organs and tissues, the propagation of elastic waves suffers from relfection, diffraction and other interfering effects. In this study, a numerical platform was established to simulate transient MRE. Furthermore, an algorithm of elasticity reconstruction was developed in accordance with time of arrival. A series of numerical experiments were carried out for harmonic and transient MREs. The results show that transient MRE has good anti-interference ability on relfection and diffraction, and the developed algorithm can perform elasticity reconstruction for transient MRE successfully.【期刊名称】《集成技术》【年(卷),期】2016(005)006【总页数】12页(P24-35)【关键词】弹性成像;磁共振弹性成像;瞬态磁共振弹性成像;数值仿真;弹性重构【作者】朱霞丽;向馗;李炳南【作者单位】合肥工业大学生物医学工程系合肥 230009;武汉理工大学自动化学院武汉 430070;合肥工业大学生物医学工程系合肥 230009【正文语种】中文【中图分类】R814人体组织弹性的变化往往伴随着某些病变,组织的弹性检查已经成为疾病诊断过程中的重要部分,因为它能给诊断带来新的信息,现已被大量用在组织病灶评估诊断方面的研究[1,2]。
考研心理学专业名词中英文对照表
考研心理学专业名词中英文对照表(一)感觉记忆(SM)-sensory memory短期记忆(STM)—short—term M.长期记忆(LTM)—long—term memory复诵-—rehearsal预示(激发)--priming童年失忆症——childhood amnesia视觉编码(表征)-—visual code(representation)听觉编码—acoustic code运作记忆—-working memory语意性知识-semantic knowledge记忆扫瞄程序—memory scanning procedure竭尽式扫瞄程序—exhaustive S.P。
自我终止式扫瞄-self-terminated S。
程序性知识—procedural knowledge命题(陈述)性知识——propositional(declarative)knowledge 情节(轶事)性知识—episodic K。
讯息处理深度-depth of processing精致化处理-elaboration登录特殊性-coding specificity记忆术—mnemonic位置记忆法—method of loci字钩法—peg word(线)探索(测)(激发)字—prime关键词-—key word命题思考--propositional thought心像思考——imaginal thought行动思考——motoric thought概念—-concept原型-—prototype属性——property特征——feature范例策略——exemplar strategy语言相对性(假说)-linguistic relativity th。
音素——phoneme词素——morpheme(字词的)外延与内涵意义—denotative &connotative meaning (句子的)表层与深层结构-surface &deep structure语意分析法——semantic differential全句语言—holophrastic speech过度延伸——over—extension电报式语言—telegraphic speech关键期——critical period差异减缩法——difference reduction方法目的分析——means-ends analysis倒推——working backward动机——motive自由意志——free will决定论——determinism本能-—instinct种属特有行为——species specific驱力——drive诱因-—incentive驱力减低说——drive reduction th.恒定状态(作用)—homeostasis原级与次级动机-primary & secondary M。
肿瘤疗效评价标准中英文

Response Evaluation Criteria in Solid Tumors (RECIST) Quick Reference:Eligibility·Only patients with measurable disease at baseline should be included in protocols where objective tumor response is the primary endpoint. Measurable disease - the presence of at least one measurable lesion. If the measurable disease is restricted to a solitary lesion, its neoplastic nature should be confirmed by cytology/histology. Measurable lesions - lesions that can be accurately measured in at least one dimension with longest diameter ³20 mm using conventional techniques or ³10 mm with spiral CT scan.Non-measurable lesions - all other lesions, including small lesions (longest diameter <20 mm with conventional techniques or <10 mm with spiral CT scan), i.e., bone lesions, leptomeningeal disease, ascites, pleural/pericardial effusion, inflammatory breast disease, lymphangitis cutis/pulmonis, cystic lesions, and also abdominal masses that are not confirmed and followed by imaging techniques; and.·All measurements should be taken and recorded in metric notation, using a ruler or calipers. All baseline evaluations should be performed as closely as possible to the beginning of treatment and never more than 4 weeks before the beginning of the treatment. ·The same method of assessment and the same technique should be used to characterize each identified and reported lesion at baseline and during follow-up. ·Clinical lesions will only be considered measurable when they are superficial (e.g., skin nodules and palpable lymph nodes). For the case of skin lesions, documentation by color photography, including a ruler to estimate the size of the lesion, is remended. Methods of Measurement –·CT and MRI are the best currently available and reproducible methods to measure target lesions selected for response assessment. Conventional CT and MRI should be performed with cuts of 10 mm or less in slice thickness contiguously. SpiralCT should be performed using a 5 mm contiguous reconstruction algorithm. This applies to tumors of the chest, abdomen and pelvis. Head and neck tumors and those of extremities usually require specific protocols.·Lesions on chest X-ray are acceptable as measurable lesions when they are clearly defined and surrounded by aerated lung. However, CT is preferable. ·When the primary endpoint of the study is objective response evaluation, ultrasound (US) should not be used to measure tumor lesions. It is, however, a possible alternative to clinical measurements of superficial palpable lymph nodes, subcutaneous lesions and thyroid nodules. US might also be useful to confirm the plete disappearance of superficial lesions usually assessed by clinical examination.·The utilization of endoscopy and laparoscopy for objective tumor evaluation has not yet been fully and widely validated. Their uses in this specific context require sophisticated equipment and a high level of expertise that may only be available in some centers. Therefore, the utilization of such techniques for objective tumor response should be restricted to validation purposes in specialized centers. However, such techniques can be useful in confirming plete pathological response when biopsies are obtained.·Tumor markers alone cannot be used to assess response. If markers are initially above the upper normal limit, they must normalize for a patient to be considered in plete clinical response when all lesions have disappeared.·Cytology and histology can be used to differentiate between PR and CR in rare cases (e.g., after treatment to differentiate between residual benign lesions and residual malignant lesions in tumor types such as germ cell tumors).Baseline documentation of “Target〞and “Non-Target〞lesions·All measurable lesions up to a maximum of five lesions per organ and 10 lesions in total, representative of all involved organs should be identified as target lesions and recorded and measured at baseline. ·Target lesions should be selected on the basis of their size (lesions with the longest diameter) and their suitability for accurate repeated measurements (either by imaging techniquesor clinically). ·A sum of the longest diameter (LD) for all target lesions will be calculated and reported as the baseline sum LD. The baseline sum LD will be used as reference by which to characterize the objective tumor.所有目标病灶的最长长径总和将会被计算和汇报成基线的长径和,该和作为有效缓解记录的参考基线。
PET与WB-DWI诊断肿瘤及炎症疾病的研究进展
PET与WB-DWI诊断肿瘤及炎症疾病的研究进展李可心;孙洪赞;郭启勇【摘要】正电子发射断层显像通过检测病灶对示踪剂的摄取程度反映细胞及组织的功能代谢状态,从而进一步显示全身肿瘤及非肿瘤性病变.磁共振全身弥散加权成像是崭新的磁共振成像技术,在评价肿瘤分期、筛查良恶性病变方面具有广阔的应用前景.作为两种可以进行全身显像的技术,明确各自优势并合理选择是十分必要的.本文主要针对二者在肿瘤及炎症疾病中的诊断价值及研究进展展开综述.%Position emission tomography detects the uptake of tracer to reflect the functional and metabolic status of cells and tissues in order to further diagnose malignant and benign lesions. Whole body diffusion-weighted imaging is a new tech-nique of functional magnetic resonance imaging. It has a broad prospect in screening lesions and evaluation of cancer staging. As two kinds of techniques that can be used for whole body imaging, it is necessary to make clear the advantages and rea-sonable choices of each of them. This article reviews the diagnostic value and research progress of the two in tumor and in-flammatory diseases.【期刊名称】《中国临床医学影像杂志》【年(卷),期】2018(029)004【总页数】4页(P291-294)【关键词】肿瘤;炎症;正电子发射断层显像术;磁共振成像【作者】李可心;孙洪赞;郭启勇【作者单位】中国医科大学附属盛京医院放射科,辽宁沈阳110004;中国医科大学附属盛京医院放射科,辽宁沈阳110004;中国医科大学附属盛京医院放射科,辽宁沈阳110004【正文语种】中文【中图分类】R73;R364.5;R817.4;R445.2正电子发射断层显像(Position emission tomography,PET)通过检测病灶对示踪剂的摄取程度反映细胞及组织的功能代谢状态,从而进一步显示全身肿瘤及非肿瘤性病变。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
© 2008 Nature Publishing Group /naturemedicine
Simultaneous PET-MRI: a new approach for functional and morphological imaging
spectroscopy (MRS) and functional MRI (fMRI)2. Thus, to combine two or more imaging modalities providing complementary information, such as morphology and function, is a worthwhile goal. Although the combination of PET and CT has already been realized3 in clinical and preclinical scanners, PET-CT has many limitations. Its major drawback is that the imaging is performed sequentially rather than simultaneously. In preclinical studies, this adds considerable time under anesthesia for the subjects and eliminates any temporal correlation between the two modalities, such as CT perfusion measurements and PET tracer kinetics. Furthermore, CT has limited soft-tissue contrast, and the necessary dose of radiation can be high enough to perturb the animal model under study. Hence, a preferred choice would be to combine PET and MRI, not only because of the absence of ionizing radiation in MRI but also for its excellent soft-tissue contrast, its flexible scan protocols and its capability to perform fMRI and MRS. The simultaneous acquisition of different functional parameters using PET, fMRI or MRS, in addition to high-resolution anatomic MRI information, creates enormous possibilities and provides completely new opportunities to study pathology and biochemical processes in vivo. By contrast, two stand-alone systems, allowing only sequential data acquisition and subsequent image fusion, cannot provide such powerful information. In addition, post-acquisition image fusion by software, especially in high-resolution abdominal or thoracic animal studies, is extremely difficult and inaccurate. This is mainly because of the variation of breathing depth during a protracted anesthesia time and because of visceral movement. Likewise, sequential imaging of functional parameters as in fMRI and PET would necessitate reproducibility of functional processes to allow a temporal correlation to be made after acquisition.
Combining PET and MRI is challenging, as conventional PET detectors incorporate photomultiplier tubes (PMTs), which are extremely sensitive to magnetic fields. Thus, alternate PET-MRI approaches
1Laboratory for Preclinical Imaging and Imaging Technology of the Werner Siemens Foundation, Department of Radiology, Eberhard Karls University of Tu¨ bingen, Ro¨ ntgenweg 13, 72076 Tu¨ bingen, Germany. 2Siemens Preclinical Solutions, 810 Innovation Drive, Knoxville, Tennessee 37932, USA. 3Department of Biomedical Engineering, University of California, Davis, One Shields Avenue, Davis, California 95616, USA. 4Bruker BioSpin MRI GmbH, Rudolf-Plank-Strasse 23, 76275 Ettlingen, Germany. 5Max Planck Institute for Biological Cybernetics, Spemannstrae 41, 72076 Tu¨ bingen, Germany. 6Clinic of Dermatology, Eberhard Karls University of Tu¨ bingen, Liebermeisterstr. 25, 72076 Tu¨ bingen, Germany. 7Department of Medical Biometry, Eberhard Karls University of Tu¨ bingen, Westbahnhofstr. 55, 72070 Tu¨ bingen, Germany. 8Department for Molecular Pathology, Institute of Pathology, Eberhard Karls University of Tu¨ bingen, Liebermeisterstr. 8, 72076 Tu¨ bingen, Germany. 9Radiopharmacy, PET-Center, Eberhard Karls University of Tu¨ bingen, Ro¨ ntgenweg 15, 72076 Tu¨ bingen, Germany. Correspondence should be addressed to B.J.P. (Bernd.Pichler@med.uni-tuebingen.de).
Technologies for functional or anatomic in vivo imaging of small laboratory animals can assess functional processes such as perfusion, metabolism, and gene and receptor expression, or reveal highresolution morphology1. Several dedicated small-animal imaging technologies are commercially available, including X-ray computed tomography (CT), MRI, optical imaging, ultrasound, single photon emission computed tomography and PET. These systems provide a wealth of information that is highly complementary and rarely redundant. The unrivaled advantage of PET stems from the ability to track radiolabeled biomarkers with a detection sensitivity reaching below the picomolar range for functional imaging, whereas MRI and CT provide high-resolution anatomic information. MRI also permits a large variety of tissue contrasts, diffusion imaging, magnetic resonance
Martin S Judenhofer1, Hans F Wehrl1, Danny F Newport2, Ciprian Catana3, Stefan B Siegel2, Markus Becker4, Axel Thielscher5, Manfred Kneilling6, Matthias P Lichy1, Martin Eichner7, Karin Klingel8, Gerald Reischl9, Stefan Widmaier4, Martin Ro¨cken6, Robert E Nutt2, Hans-Ju¨rgen Machulla9, Kamil Uludag5, Simon R Cherry3, Claus D Claussen1 & Bernd J Pichler1