中心静脉导管相关血流感染最新定义
最新:血流导管相关血流感染的管理2023

最新:血流导管相关血流感染的管理20232023年2月国家卫健委针对医疗质量安全薄弱环节和关键点,明确行业改进方向提出3个领域涵盖10个重大疾病的医疗质量改进目标,其中“降低血管内导管相关性血流感染发生率”为10大目标之一。
国家卫健委于2023年3月17日印发"血流导管相关感染预防与控制指南(2023年版)”的通知,重点改善中心静脉导管及经外周静脉置入中心静脉导管的相关血流感染问题,以保证医疗安全和患者权益。
血管导管相关感染的定义血管导管相关感染(Vesse1CatheterAssociatedInfection,简称VCA1)是指留置血管导管期间及拔除血管导管后48小时内发生的原发性、且与其他部位感染无关的感染,包括血管导管相关局部感染和血管导管相关血流感染(CRBS1)。
患者局部感染时出现红、肿、热、痛、渗出等炎症表现,血流感染除局部表现外还会出现发热(>38。
C)、寒颤或低血压等全身感染表现。
血流感染实验室微生物学检查结果:外周静脉血培养细菌或真菌阳性,或者从导管尖端和外周血培养出相同种类、相同药敏结果的致病国OCRBS1的危害及疾病负担CRBS1死亡率明显升高,一项前瞻性、观察研究显示留置导管血流感染患者的死亡率显著高于无导管相关血流感染或导管细菌定植患者。
Id1F<0.009Aff1UXBff1,/⅛O,O55现f 粉皿侬的IIBmCfi)CRBS1分布科室多,成为常见院内感染之一,医院感染暴发流行的常见类型败血症占20%o 我国一项回顾性分析显示导管相关性血流感染分布在ICU,胃肠外科、急诊急救等科室;一项美国全国范围监测研究显示院内血流感染分布在ICU 、内科、普外科等科室。
CRBS1的危险因素导管类型:双腔导管和多腔导管感染率较单腔导管明显升高。
插管部位:股静脉置管感染率较颈内静脉、锁骨下静脉置管感染率 高。
导管留置时间:留置时间超过2周,导管相关感染明显升高。
患者因素:患者存在严重基础疾病,免疫功能低下以及低蛋白血症、因化联血*幽 导f 包他睢摘BSI疗所致粒缺。
医院感染与中心静脉导管相关感染

定期冲洗导管
用无菌生理盐水定期冲洗导管,防 止血液凝块和沉淀物堵塞导管。
严格消毒
每次接触导管前应进行手部消毒, 防止交叉感染。
中心静脉导管相关感染的监测和报告制度
监测指标
定期监测导管入口处皮肤有无红 肿、疼痛、分泌物等感染征象。
报告制度
一旦发现感染征象,应立即报告 医生,并进行相应的诊断和治疗
。
CHAPTER
中心静脉导管的合理使用
严格掌握适应症
导管选择合适
只有当患者病情需要时才考虑使用中 心静脉导管,避免不必要的置管。
根据患者病情和需要选择合适的导管 型号和材质。
置管操作规范
确保置管过程严格遵守无菌原则,减 少污染机会。
中心静脉导管的维护和消毒
定期更换敷料
保持导管入口处敷料的清洁干燥 ,定期更换敷料,防止细菌滋生
少部分感染由真菌引起,如念珠菌等 。
中心静脉导管相关感染的危险因素
01
02
03
04
患者自身因素
如年龄、性别、基础疾病、免 疫功能低下等。
导管留置时间
留置时间越长,感染风险越高 。
置管部位
颈部和腹股沟置管感染风险较 高。
护理措施
护理操作不规范、未能及时更 换敷料等会增加感染风险。
04 中心静脉导管相关感染的预防和控制策略
医院感染与中心静脉导管相关 感染
汇报人:可编辑
2024-01-07
目录
CONTENTS
• 医院感染概述 • 中心静脉导管相关感染概述 • 中心静脉导管相关感染的流行病学 • 中心静脉导管相关感染的预防和控制策略 • 中心静脉导管相关感染的治疗和管理
01 医院感染概述
CHAPTER
导管相关性血流感染
19
导管相关血流感染的培养方法
成对血培养:
方法:同时取两份样品做培养,一份取自导管 的静脉血,另一份经皮穿刺的周围血。 结果评价: 1) 持续监测这对血培养阳性出现的时间,当导 管出现阳性血培养的时间比周围血培养阳性提 早2小时以上,即确定差异时间培养阳性 2) 自导管的血培养菌落计数比周围血高5—10倍 预示导管相关性血流感染
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
Company LOGO
62
拔管后抗菌药物治疗在24h内有效则提示CRBSI;
12
关于血培养的正确观念
正确采集血培养标本的关键点:
采血时间 采血次数 接种血液数量 使用含树脂培养瓶
13
关于血培养的正确观念
Chills 寒战
Blood Cultures
血培养
Temp
体温
BACTEREMIA LEVEL 菌血症的水平
0
30 Time (min)
9
CRBSI的病原学
常见的病原微生物有:
凝固酶阴性葡萄球菌; 革兰阴性厌氧杆菌; 白色念珠菌
10
导管相关性感染分类 局灶性(外部)感染:蜂窝组织炎、脓肿、化 脓性血栓炎等。可伴有或不伴有血流感染 血流感染:菌血症、心内膜炎
11
CRBSI的诊断
CRBSI诊断目前尚没有金标准! 临床表现的非特异性和延迟性使诊断更难以把握; 血培养阳性是诊断CRBSI最简单方法;
医院感染的中心性静脉导管相关血流感染
首先确认患者有中心性静脉导管留置史,然后根据临床表现和实验室检查结果 进行诊断。临床表现包括寒战、高热、白细胞计数升高、血培养阳性等;实验 室检查包括导管血和外周血培养、导管尖端细菌培养等。
实验室诊断方法
80%
血培养
采集导管血和外周血进行培养, 以检测是否存在病原微生物。
100%
导管尖端细菌培养
03
中心性静脉导管相关血流感染的预防与控制
预防策略与措施
01
02
03
04
严格掌握置管适应症
仅在必要时使用中心静脉导管 ,尽量选择其他替代方案。
置管人员的培训
确保置管人员经过专业培训, 掌握正确的置管技术和操作规 范。
置管环境消毒
保持置管环境清洁卫生,定期 进行空气消毒。
导管材料的选择
选用高品质、具有抗菌性能的 导管材料。
06
中心性静脉导管相关血流感染的研究进展与展 望
研究现状与成果
中心性静脉导管相关血流感染(CRBSI)是医院感染 的重要类型之一,近年来受到广泛关注。
国内外研究者针对CRBSI的病原学、流行病学、诊断 与治疗等方面进行了大量研究,取得了一定的成果 。
已有研究证实,严格遵守无菌操作、定期更换敷料 、使用抗菌药物等措施可以有效降低CRBSI的发生率 。
导管置换
在特殊情况下,如导管功 能正常且感染得到控制, 可以考虑进行导管置换。
其他治疗措施
支持治疗
给予患者充足的营养、水和电解质, 维持身体正常代谢和内环境稳定。
对症治疗
免疫调节
对于免疫功能低下的患者,可以考虑 使用免疫调节剂或生物制剂进行治疗 。
针对患者的症状和体征,采取相应的 对症治疗措施,如降温、止痛等。
(完整版)中心静脉导管相关血流感染判断标准
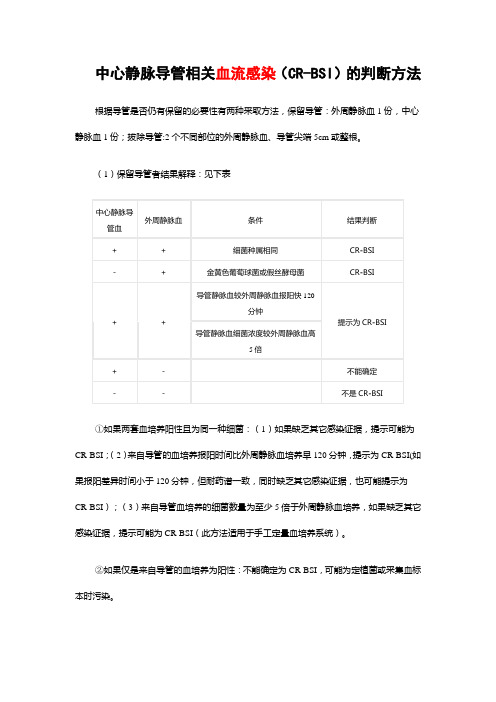
中心静脉导管相关血流感染(CR-BSI)的判断方法根据导管是否仍有保留的必要性有两种采取方法,保留导管:外周静脉血1份,中心静脉血1份;拔除导管:2个不同部位的外周静脉血、导管尖端5cm或整根。
(1)保留导管者结果解释:见下表
①如果两套血培养阳性且为同一种细菌:(1)如果缺乏其它感染证据,提示可能为CR-BSI;(2)来自导管的血培养报阳时间比外周静脉血培养早120分钟,提示为CR-BSI(如果报阳差异时间小于120分钟,但耐药谱一致,同时缺乏其它感染证据,也可能提示为CR-BSI);(3)来自导管血培养的细菌数量为至少5倍于外周静脉血培养,如果缺乏其它感染证据,提示可能为CR-BSI(此方法适用于手工定量血培养系统)。
②如果仅是来自导管的血培养为阳性:不能确定为CR-BSI,可能为定植菌或采集血标本时污染。
③如果仅是来自外周静脉的血培养为阳性:不能确定为CR-BSI;但如为金黄色葡萄球菌,或假丝酵母菌属,在缺乏其它感染证据则提示可能为CR-BSI。
④如果两套血培养为阴性:不是CR-BSI。
(2)已拔除导管结果解释:见下表
①如果一套或多套血培养阳性,且导管尖端培养或导管定量培养为阳性,根据鉴定结果和药敏谱两种培养为同一种细菌,提示可能为CR-BSI。
②如果一套或多套血培养阳性,而导管尖端培养或导管定量培养为阴性:如培养结果为金黄色葡萄球菌或假丝酵母菌属且缺乏其它感染的证据则提示可能为CR-BSI,确认可能要求额外的血培养阳性结果且是同一种细菌。
③如果血培养为阴性而导管尖端培养为阳性,提示为导管定植菌,不是CR-BSI。
④如果两套血培养为阴性和导管尖端培养/导管定量培养均为阴性,则不是CR-BSI。
医院感染预防控制中的中心静脉导管相关血流感染

患者个体差异大
不同患者的免疫状态、基 础疾病等个体差异大,影 响感染预防和控制的效果 。
未来研究方向与技术展望
新型检测方法研究
01
研发更快速、准确的检测方法,以便早期发现和诊断中心静脉
导管相关血流感染。
新型抗菌材料研究
02
研究开发具有抗菌性能的新型材料,用于制作中心静脉导管,
降低感染风险。
个体化治疗方案研究
医院感染预防控制中的中心静脉导 管相关血流感染
汇报人:可编辑 2024-01-06
目录
• 中心静脉导管相关血流感染概述 • 中心静脉导管相关血流感染的预防策略 • 中心静脉导管相关血流感染的控制措施 • 中心静脉导管相关血流感染的研究进展 • 中心静脉导管相关血流感染的挑战与展望
01
中心静脉导管相关血流 感染概述
新型导管护理敷料的研究
新型导管护理敷料的作用
传统的纱布敷料容易滋生细菌,导致感染发生。新型导管 护理敷料具有良好的透气性和保湿性,能够为导管提供良 好的保护和护理。
新型敷料的种类
包括水胶体敷料、泡沫敷料、透明敷料等,这些敷料具有 良好的透气性、保湿性和粘附性,能够为导管提供全面的 保护和护理。
临床应用常维护和自我观察,发现问 题及时报告。
03
中心静脉导管相关血流 感染的控制措施
感染监测与报告制度
监测
定期对医院所有中心静脉导管相 关血流感染病例进行监测,确保 及时发现并采取措施。
报告
建立中心静脉导管相关血流感染 报告制度,要求医护人员及时上 报感染病例。
定义与分类
中心静脉导管相关血流感染(Central Line-Associated Bloodstream Infections,CLABSI):指患者在留置中心静 脉导管期间或拔除导管48小时内发生的原发性、且与导管相 关的血行感染。
中心静脉导管相关血流感染
中心静脉导管相关血流感染北京积水潭医院李静血管内导管类型置入血管类型:周围静脉导管,中心静脉导管,动脉导管。
留置时间:临时或短期导管,长期导管。
穿刺部位:周围静脉导管,经外周中心静脉导管,锁骨下静脉导管,股静脉导管,颈静脉导管。
导管是否存在皮下隧道:皮下隧道式导管和非皮下隧道式导管。
导管长度:长导管,中长导管,短导管。
导管相关感染的概念出口部位感染:指出口部位2cm内的红斑硬结和触痛,导管出口部位的渗出液培养出微生物,可伴有其他感染征象和症状,伴或不伴有血行感染。
隧道感染:指导管出口位置,沿导管隧道的触痛,红斑或者大于2cm的硬结,伴或不伴有血行感染。
皮下囊感染:指完全植入血管内装置皮内囊内有感染性积液,常有表面皮肤组织触痛,红斑和硬结,自发的破裂或引流,表面皮肤的坏死,可伴或不伴有血行感染。
导管相关血行感染(CRBSI):指留置血管内装置的患者出现菌血症,经外周外周静脉抽取血液培养至少一次结果阳性,同时伴有感染的临床表现,且除导管外无其他明确的血行感染源。
导管相关感染仅限于导管感染导致的血性感染,能够排除其他部位感染,且导管尖端培养与血培养为同一致病菌。
发病机制微生物引起导管感染的方式有:1.皮肤表面的细菌在穿刺时或之后,通过皮下致导管皮内段至导管尖端的细菌定植,引起局部或全身感染。
2.另一感染灶的微生物通过血行播散到导管,在导管上粘附定植,引起CRBSI。
3.微生物污染导管接口和内腔,导致管腔内细菌繁殖,引起感染,其中,前两种属于腔外途径,第三种为腔内途径。
常见病原菌1.革兰阳性菌(最主要):表皮葡萄球菌感染主要是由于皮肤污染引起,约占CRBSI的30%。
金黄色葡萄球菌:曾经是CRBSI最常见的病原菌,目前约占院内血行感染的13.4%。
而耐万古霉素肠球菌感染的发生率也在增加。
2.革兰阴性菌:铜绿假单胞菌,嗜麦芽窄食单胞菌,鲍曼不动杆菌,放射性土壤杆菌也有报道。
绿脓杆菌和阴沟菌在大面积烧伤患者中比较多见。
中心静脉导管相关感染(CRBSI)定义预防与控制管理规程
中心静脉导管相关感染(CRBSI)定义感染前48小时内使用过中心静脉导管的患者有感染的临床表现(如发热、寒战和(或)低血压等),血培养至少可获得1个阳性的结果,(>15CFU/导管尖段5cm)或导管定量培养阳性(>103CFU/导管段),并且与外周静脉血中分离出的病原菌种类和抗菌谱相同,除血管内导管外,无其他明确的血液感染源。
中心静脉导管相关感染(CRBSI)预防与控制管理规程根据卫生部发布的《导管相关血流感染的预防与控制技术指南(试行)》(卫办医政【2010】187号)要求制定本制度,本制度适用于临床系统。
(一)导管置管时预防要点(1)严格执行无菌技术操作规程。
置管时应当遵守最大限度的无菌屏障要求。
置管部位应当铺大无菌巾(单);置管人员应当戴帽子、口罩、无菌手套,穿无菌手术衣。
(2)严格按照《医务人员手卫生规范》,认真洗手并戴无菌手套后,尽量避免接触穿刺点皮肤。
置管过程中手套污染或破损应当立即更换。
(3)置管使用的医疗器械、器具等医疗用品和各种敷料必须达到灭菌水平。
(4)选择合适的静脉置管穿刺点,成人中心静脉置管时,应当首选锁骨下静脉,尽量避免使用颈静脉和股静脉。
(5)采用卫生行政部门批准的皮肤消毒剂穿刺部位皮肤,自穿刺点有内向外一同心圆方式消毒,消毒范围应当符合置管要求。
消毒后皮肤穿刺点应当避免再次接触。
皮肤消毒待干后,在进行置管操作。
(6)患疖肿、湿疹等皮肤病或患感冒、流感等呼吸道疾病,以及携带或个人多重耐药菌的医务人员,在未治愈前不应当进行置管操作。
(二)导管置管后预防要点(1)应当尽量使用无菌透明、透气性好的敷料覆盖穿刺点,对于高热、出汗、穿刺点出血、渗出的患者应当使用无菌纱布覆盖。
(2)应当定期更换置管穿刺点覆盖的敷料。
更换间隔时间为:无菌纱布为1次/2天,无菌透明敷料为1—2次/周,如果纱布或敷料出现潮湿、松动、可见污染时应当立即更换。
(3)医务人员接触置管穿刺点或更换敷料时,应当严格执行手卫生规范。
导管相关性血流感染

CRBSI的预防
• 手卫生 • 无菌操作
手卫生和无菌操作
• 在触摸插管部位前、后,以及插入、重置、 触碰、维护导管及更换敷衍前、后时,均 应严格执行手卫生程序,可以是洗手或用 酒精擦手液。在对插管部位进行消毒处理 后,不应再触摸该部位,除非采用无菌技 术 • 在进行插管和维护操作时须无菌操作 • 进行中心静脉置管时,佩戴无菌手套
• 2次血培养标本采集时间至少间隔1小时。
样本采集
• 1套血培养:指一次静脉穿刺。 • 常规血培养,建议同时采集需氧瓶和厌氧 瓶的培养。 • 当采血量不能满足时,需氧瓶优先。
样本采集
• 抽血部位皮肤消毒: • 皮肤消毒前,先检查血培养瓶有无损坏或超保质 期,有75%酒精消毒瓶橡皮塞并干燥。 • 用2根复合碘棉签,以穿刺点为圆心,以约5㎝直 径画圈进行皮肤消毒,作用时间至少30秒。注意 消毒过的地方不能重复涂抹,在涂抹的过程中棉 签必须也要同时旋转。如果病人手臂皮肤不干净, 则需重新擦拭。在洁净后不要触摸穿刺部位。秒 • (美国CDC:75%酒精消毒穿刺部位皮肤,待干 30秒)
拔除导管标本采集方法
• 采取2套血培养,其中至少一套来自外周 静脉,另一套从导管采集。并作好标 记(采样部位和采样时间)
• 无菌状态下取出导管并用灭菌剪刀剪下导管尖端 5cm,导管半定量培养。
未留置CVC,怀疑血流感染
• 应在不同部位采血2套(至少2个部位2瓶)。 儿童除外。对怀疑亚急性心内膜炎,抽取3 套血培养。
保留导管的血培养结果解释2
• 如果2套血培养阳性,而且来自导管的血培 养的细菌数量为至少5倍于外周静脉血培养 的CFU/mL,如果缺乏其他感染证据,提示 可能为CRBSI(此方法适用于手工定量血 培养系统)
医院感染的中心静脉导管相关感染
定期检查导管
定期检查导管有无异常, 如发现异常应及时处理, 防止感染扩散。
培训医护人员
对医护人员进行培训,提 高其导管维护和管理技能 ,确保导管的正确使用和 维护。
03
中心静脉导管相关感染的诊 断与治疗
诊断标准与流程
诊断标准
中心静脉导管相关感染的诊断主要依据患者的临床表现、实验室检查和导管培养 结果。当患者出现与导管相关的感染症状,如发热、寒战、局部红肿等,且导管 培养阳性时,即可诊断为导管相关感染。
药物选择
在选择抗生素时,应综合考虑患者的病情、感染病菌种类及药敏试验结果。常用的抗生素包括头孢菌素类、青霉 素类、氨基糖苷类等。在拔除导管后,一般需要连续治疗7-14天,直至感染得到控制。
感染控制的效果评估
评估指标
感染控制的效果评估主要依据患者的临床表现、实验室检查 和导管培养结果。在治疗后,患者的症状应得到明显改善或 消失,实验室检查指标恢复正常,导管培养阴性,表明感染 得到有效控制。
建立置管技术质量控制标准,定期对 置管操作进行评估和监督,确保置管 技术的规范性和安全性。
建立完善的感染监测与报告制度
建立健全的医院感染监测体系,定期对中心静脉导管相关感染的发生情况进行监 测和评估。
建立感染报告制度,要求医护人员及时上报中心静脉导管相关感染病例,以便及 时采取防控措施。
THANKS
置管过程中的预防措施
无菌操作
在整个置管过程中,应遵循无菌操作原则,确保导管、连接器和注射器的无菌状态。
减少人员流动
在置管过程中,应尽量减少人员流动,避免交叉感染。
正确置管方法
采用正确的置管方法,避免因操作不当导致皮肤和血管的损伤,从而引发感染。
置管后的维护与管理
2024中心静脉导管透析CVC相关血流感染

2024中心静脉导管透析CVC相关血流感染血液透析是终末期肾脏病患者肾脏替代治疗的主要方法,血管通路首选自体动静脉内瘦。
中心静脉导管(CVC)也是血液透析患者最后的生命线,且随着医学观念的进步,以逐渐〃以内屡优先〃转向为〃以患者为中心〃,因此,患者的最优解并不一定就是自体动静脉内屡了。
随着透析患者逐年增多、透析龄延长、老龄化等原因,血透患者CVC的使用率逐渐增多。
导管相关的并发症,尤其是导管相关血流感染(CRBSI)对患者危害很大,严重者威胁患者的生命安全,日益引起人们的重视。
感染是目前已知的、较严重的血液透析并发症之一,其不仅会导致患者病情不断恶化,且易诱发其他并发症导致患者死亡。
维持性血液透析患者死亡原因主要是心血管、感染、脑血管意外,感染是维持性血液透析患者第2位死因。
所以,正确认识血透导管感染的危险因素及积极预防极其重要。
01临床表现和诊断血液透析开始数分钟至数10分钟,患者出现畏寒、寒战、发热等全身症状,这是血透导管感染的典型表现。
少数患者可以出现延迟发热,即血液透析结束后低热,这与感染的细菌数量和毒力有关。
当患者出现这些症状后,需要留取血培养标本确诊并指导下一步治疗。
血液透析导管相关血流感染的诊断需要抽取外周血培养标本,且要求从血透导管口直接抽取的血标本培养结果和外周相同,细菌数是外周标本的3倍以上;或从血透导管口直接抽取的血培养标本培养结果和外周相同,培养阳性报警时间至少比外周标本早2h;或导管尖端培养出和外周血标本一样的细菌(需要拔除导管)。
02导管相关感染专科原因分析1患者因素血液透析治疗清除患者体内毒素的过程中会有少量蛋白流失,老年透析患者消化功能减退,蛋白质、维生素、膳食纤维等摄入减少,导致营养不良,机体抵抗力低下。
尤其是糖尿病患者,糖代谢紊乱、免疫功能低下、防御功能降低发生感染的风险比普通人群高。
高龄、低蛋白血症.血红蛋白水平低.营养不良、糖尿病.使用免疫抑制剂是发生血透导管感染的危险因素。
医院感染的中心静脉导管相关血流感染风险与预防

汇报人:可编辑 2024-01-07
目 录
• 中心静脉导管相关血流感染概述 • 中心静脉导管相关血流感染的风险因素 • 中心静脉导管相关血流感染的预防策略 • 中心静脉导管相关血流感染的监测与控制 • 中心静脉导管相关血流感染的研究进展
01
中心静脉导管相关血流感染概 述
感染发生机制
微生物定植
中心静脉导管作为异物植入人体 后,皮肤表面的细菌容易黏附在 导管表面形成生物膜,进而引起
感染。
免疫逃避
微生物黏附在导管表面后,会通过 多种机制逃避机体免疫系统的清除 ,如产生生物膜、改变表面抗原等 。
血液反流
中心静脉导管作为异物改变了血液 的正常流动模式,可能导致血液反 流,为微生物进入血液提供机会。
严格手卫生
01
医务人员在接触中心静脉导管和患者前后应严格执行手卫生规
范。
无菌操作
02
在置管、换药和护理等操作中,应遵守无菌原则,降低感染风
险。
导管护理
03
定期对中心静脉导管进行清洁和消毒,保持导管的通畅和无菌
状态。
05
中心静脉导管相关血流感染的 研究进展
新型抗菌材料的研究与应用
抗菌涂层材料
利用抗菌物质与导管材料结合,降低感染风险。如银离子涂层、聚 合物抗菌涂层等。
个体化用药方案
根据基因检测结果,制定针对不同病原菌和耐药性的个性化用药 方案,提高治疗效果。
免疫治疗
研究利用免疫手段增强患者抵抗力,降低感染风险,如免疫调节 剂、疫苗等。
社会经济学评价与政策建议
1 2 3
成本效益分析
对新型抗菌材料、个体化治疗策略等进行成本效 益分析,评估其在预防医院感染中的经济价值。
中心静脉导管相关性感染
2011年CNS
患者平均年龄53.09±15.38岁,男女比为1.44:1
7.0%
6.3%
6.5%
6.0% 5.0%
5.3% 4.7%
5.2%
5.7% 4.5%
4.0% 3.0%
3.5% 2.8%
4.0% 男
3.0% 女
2.0%
1.6%
1.4%
1.0%
0.4%
0.4%
0.0% 0 20 25 30 35 40 45 50 55 60 65 70 75 80 85
感染率
流行病学
CRI感染率一般以次数/每100导管天数或次 数/每1000导管天数来表示。
美国每年大约
血管通路
感染率
无隧道的中心静脉导管 5.0例/1000导管日(3.8-6.5例/1000导管日)
股静脉插管 颈内静脉插管 锁骨下静脉插管 有隧道、带袖套的 中心静脉导管 聚四氟乙烯血管动 静脉内瘘 自体动静脉内瘘
血液透析中心静脉导管应用现状
新进入血液透析患者的血管通路 欧洲:31%使用中心静脉导管; 美国:80%使用中心静脉导管; 上海: 59-69%使用临时中心静脉导管; 云南:90%以上使用临时中心静脉导管; 。 本中心:98%使用临时中心静脉导管。
血液透析中心静脉导管应用现状
过去20年中,双腔中心静脉导管置管率和 使用寿命日益升高。在加拿大,维持透析 患者有33%使用CVC,而美国约47%,这已经 远远超过NKF – DOQI双腔导管使用不得超 过10%的推荐。
7.6 例/1000导管日(1周后感染率增加10%) 5.6例/1000导管日(2-3周后感染率增加10%) 2.7例/1000导管日(4周后感染率增加10%) 3.5例/1000导管日(1.6-5.5例/1000导管日)
中心静脉导管相关感染的定义是什么

中心静脉导管相关感染的定义是什么在现代医疗领域中,中心静脉导管(Central Venous Catheter,CVC)的应用越来越广泛。
它为患者提供了重要的治疗途径,如长期输液、化疗药物输注、血液透析、肠外营养支持等。
然而,与之相伴的是中心静脉导管相关感染(Central Venous CatheterRelated Infection,CVCRI)这一不容忽视的问题。
那么,究竟什么是中心静脉导管相关感染呢?简单来说,中心静脉导管相关感染是指在中心静脉导管置入体内后,由于各种原因导致的病原微生物在导管及周围组织的定植和繁殖,进而引起的局部或全身性感染。
从感染发生的部位来划分,中心静脉导管相关感染可以分为三类:首先是导管局部感染,这种感染通常局限于导管插入部位的皮肤和皮下组织。
表现为穿刺点周围的红肿、疼痛、渗液,有时还可能出现脓性分泌物。
其次是导管相关的血流感染(CatheterRelated Bloodstream Infection,CRBSI),这是一种较为严重的情况。
病原微生物通过导管内腔或导管外壁进入血液循环,引起发热、寒战、低血压等全身感染症状,同时血培养结果显示与导管尖端培养出相同的病原体。
最后是隧道感染,即沿着导管皮下隧道发生的感染,表现为皮下隧道部位的红肿、压痛。
导致中心静脉导管相关感染的原因是多方面的。
患者自身的因素起着一定的作用。
比如患者本身的免疫功能低下,患有糖尿病、营养不良、恶性肿瘤等基础疾病,这些都会使机体抵抗感染的能力下降,从而增加感染的风险。
导管的置入和维护过程中的操作不当也是重要原因。
如果在置管时没有严格遵守无菌操作原则,或者在后续的维护中,如更换敷料、输注药物时没有做好消毒工作,都容易将病原微生物带入体内。
导管留置时间过长也是一个不容忽视的因素。
随着导管在体内留置时间的延长,导管表面会逐渐形成一层生物膜,这为病原微生物的定植和繁殖提供了有利条件。
此外,导管的材质和类型也可能影响感染的发生。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Central Line-Associated Bloodstream Infection (CLABSI) Event Introduction: An estimated 41,000 central line-associated bloodstream infections (CLABSI) occur in U.S. hospitals each year.1 These infections are usually serious infections typically causing a prolongation of hospital stay and increased cost and risk of mortality.CLABSI can be prevented through proper management of the central line. These techniques are addressed in the CDC’s Healthcare Infection Control Practices Advisory Committee (CDC/HIPAC) Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011.2Settings: Surveillance will occur in any inpatient location where denominator data can be collected, which may include critical/intensive care units (ICU), specialty care areas (SCA), neonatal units including neonatal intensive care units (NICUs), step down units, wards, and long term care units. A complete listing of inpatient locations can be found in Chapter 15.NOTE: Surveillance for CLABSIs after the patient is discharged from the facility is not required. However, if discovered, any CLABSIs occurring within 48 hours of discharge should be reported to NHSN. No additional central line days are reported. Requirements: Surveillance for CLABSI in at least one inpatient location in the healthcare institution for at least one calendar month as indicated in the Patient Safety Monthly Reporting Plan (CDC 57.106).Definitions: As for all infections reported to NHSN, infections associated with complications or extensions of infections already present on admission, unless a change in pathogen or symptoms strongly suggests the acquisition of a new infection, are not considered healthcare associated. Therefore, infections that become apparent within the first few days of admission must be carefully reviewed to determine whether they should be considered healthcare associated.Primary bloodstream infections (BSI) are laboratory-confirmed bloodstream infections (LCBI) that are not secondary to a community-acquired infection or an HAI meeting CDC/NHSN criteria at another body site (see criteria in Chapter 17 and Appendix 1. Secondary Bloodstream Infection Guide). Report BSIs that are central line associated (i.e., a central line or umbilical catheter was in place at the time of, or within 48 hours before, onset of the event).NOTE: There is no minimum period of time that the central line must be in place in order for the BSI to be considered central line associated.Location of attribution: The inpatient location where the patient was assigned on the date of the BSI event, which is further defined as the date when the first clinical evidence appeared or the date the specimen used to meet the BSI criteria was collected, whichever came first.EXAMPLE: Patient, who had no clinical signs or symptoms of sepsis upon arrival to the Emergency Department, has a central line inserted there before being admitted to the MICU has a central line inserted in the Emergency Department and then is admitted to the MICU. Within 24 hours of admission to the MICU, patient meets criteria for BSI. This is reported to NHSN as a CLABSI for the MICU because the Emergency Department is not an inpatient location and no denominator data are collected there. EXCEPTION:Transfer Rule: If a CLABSI develops within 48 hours of transfer from one inpatient location to another in the same facility, or a new facility, the infection is attributed to the transferring location. This is called the Transfer Rule and examples are shown below: •Patient with a central line in place in the SICU is transferred to the surgical ward.Thirty six (36) hours later, the patient meets the criteria for BSI. This is reported to NHSN as a CLABSI for the SICU.•Patient is transferred to the medical ward from the MSICU after having the central line removed. Within 24 hours, patient meets criteria for a BSI. This isreported to NHSN as a CLABSI for the MSICU.•Patient with a central line in place is transferred from the medical ward to the coronary care ICU (CCU). After 4 days in the CCU, the patient meets the criteria for a BSI. This is reported to NHSN as a CLABSI for the CCU.•Patient on the urology ward of Hospital A had the central line removed and is discharged home a few hours later. The IP from Hospital B calls the next day toreport that this patient has been admitted to Hospital B with a BSI. This CLABSI should be reported to NHSN for, and by, Hospital A and attributed to the urology ward. No additional catheter days are reported.Central line: An intravascular catheter that terminates at or close to the heart or in one of the great vessels which is used for infusion, withdrawal of blood, or hemodynamic monitoring. The following are considered great vessels for the purpose of reporting central-line BSI and counting central-line days in the NHSN system: Aorta, pulmonary artery, superior vena cava, inferior vena cava, brachiocephalic veins, internal jugular veins, subclavian veins, external iliac veins, common iliac veins, femoral veins, and in neonates, the umbilical artery/vein.NOTES:1.Neither the insertion site nor the type of device may be used to determine if a linequalifies as a central line. The device must terminate in one of these vessels or in or near the heart to qualify as a central line.2.An introducer is considered an intravascular catheter, and depending on thelocation of its tip, may be a central line.3. A Hemodialysis Reliable Outflow dialysis catheter (HERO), that is located in oneof the great vessels and used for purposes outlined above, is considered a centralline.4.Pacemaker wires and other nonlumened devices inserted into central bloodvessels or the heart are not considered central lines, because fluids are not infused, pushed, nor withdrawn through such devices.5.The following devices are not considered central lines: extracorporeal membraneoxygenation (ECMO), femoral arterial catheters and intraaortic balloon pump(IABP) devices. If you have a question about whether a device qualifies as acentral line, please email us at NHSN@.Infusion: The introduction of a solution through a blood vessel via a catheter lumen. This may include continuous infusions such as nutritional fluids or medications, or it may include intermittent infusions such as flushes or IV antimicrobial administration, or blood, in the case of transfusion or hemodialysis.Umbilical catheter: A central vascular device inserted through the umbilical artery or vein in a neonate.Temporary central line: A non-tunneled catheter.Permanent central line: Includeso Tunneled catheters, including certain dialysis catheterso Implanted catheters (including ports)Laboratory-confirmed bloodstream infection (LCBI): Must meet one of the following criteria:Criterion 1: Patient has a recognized pathogen cultured from one or more blood culturesandorganism cultured from blood is not related to an infection at another site. (See Notes 1 and 2 below and Appendix 1. Secondary Bloodstream Infection Guide.)Criterion 2: Patient has at least one of the following signs or symptoms: fever(>38o C), chills, or hypotensionandsigns and symptoms and positive laboratory results are not related to an infection at another site (See Appendix 1. Secondary Bloodstream Infection Guide.)andcommon commensal (i.e., diphtheroids [Corynebacterium spp. not C. diphtheriae], Bacillus spp. [not B. anthracis], Propionibacterium spp., coagulase-negative staphylococci [including S. epidermidis], viridans group streptococci, Aerococcus spp., and Micrococcus spp.) is cultured from two or more blood cultures drawn on separate occasions.Criterion 3: Patient < 1 year of age has at least one of the following signs or symptoms: fever (>38o C core) hypothermia (<36o C core), apnea, or bradycardiaandsigns and symptoms and positive laboratory results are not related to an infection at another site (See Appendix 1. Secondary Bloodstream Infection Guide.)andcommon skin commensal (i.e., diphtheroids [Corynebacterium spp. not C. diphtheriae], Bacillus spp. [not B. anthracis], Propionibacterium spp., coagulase-negative staphylococci [including S. epidermidis], viridans group streptococci, Aerococcus spp., Micrococcus spp.) is cultured from two or more blood cultures drawn on separate occasions. (See Notes 3, 4 and 5 below.)NOTES:1.In criterion 1, the phrase “one or more blood cultures” means that at least onebottle from a blood draw is reported by the laboratory as having grown organisms(i.e., is a positive blood culture).2.In criterion 1, the term “recognized pathogen” does not include organismsconsidered common commensals (see criteria 2 and 3 for a list of commoncommensals). A few of the recognized pathogens are S. aureus, Enterococcusspp., E. coli, Pseudomonas spp., Klebsiella spp., Candida spp., etc.3.In criteria 2 and 3, the phrase “two or more blood cultures drawn on separateoccasions” means 1) that blood from at least two blood draws were collectedwithin two days of each other (e.g., blood draws on Monday and Tuesday orMonday and Wednesday would be acceptable for blood cultures drawn onseparate occasions, but blood draws on Monday and Thursday would be too farapart in time to meet this criterion), and 2) that at least one bottle from each blood draw is reported by the laboratory as having grown the same common commensal(i.e., is a positive blood culture). (See Note 4 for determining sameness oforganisms.)a.For example, an adult patient has blood drawn at 8 a.m. and again at 8:15 a.m.of the same day. Blood from each blood draw is inoculated into two bottlesand incubated (four bottles total). If one bottle from each blood draw set ispositive for coagulase-negative staphylococci, this part of the criterion is met.b.For example, a neonate has blood drawn for culture on Tuesday and again onSaturday and both grow the same common commensal. Because the timebetween these blood cultures exceeds the two-day period for blood drawsstipulated in criteria 2 and 3, this part of the criteria is not met.c. A blood culture may consist of a single bottle for a pediatric blood draw dueto volume constraints. Therefore, to meet this part of the criterion, each bottlefrom two or more draws would have to be culture-positive for the samecommensal.4.If the common commensal is identified to the species level from one culture, anda companion culture is identified with only a descriptive name (e.g., to the genuslevel), then it is assumed that the organisms are the same. The organismidentified to the species level should be reported as the infecting pathogen alongwith its antibiogram if available (see Table 1 below).Table 1. Examples of how to report speciated and unspeciated common commensals Culture Report CompanionReport as…Culture ReportS. epidermidisS. epidermidis Coagulase-negativestaphylococciBacillus spp. (not anthracis) B. cereus B. cereusS. salivarius Strep viridans S. salivarius5.Only genus and species identification should be utilized to determine thesameness of organisms. No additional comparative methods should be used (e.g., morphology or antibiograms) because laboratory testing capabilities and protocols may vary between facilities. This will reduce reporting variability, solely due tolaboratory practice, between facilities reporting LCBIs meeting criterion 2.Report the organism to the genus/species level only once, and if antibiogram data are available, report the results from the most resistant panel.6.LCBI criteria 1 and 2 may be used for patients of any age, including patients < 1year of age.7.Specimen Collection Considerations:Ideally, blood specimens for culture should be obtained from two to four blooddraws from separate venipuncture sites (e.g., right and left antecubital veins), not through a vascular catheter. These blood draws should be performedsimultaneously or over a short period of time (i.e., within a few hours).3,4 If your facility does not currently obtain specimens using this technique, you must stillreport BSIs using the criteria and notes above, but you should work withappropriate personnel to facilitate better specimen collection practices for bloodcultures.REPORTING INSTRUCTIONS:•Report organisms cultured from blood as BSI – LCBI when no other site of infection is evident.•When there is a positive blood culture and clinical signs or symptoms of localized infection at a vascular access site, but no other infection can be found, the infection is considered a primary BSI.•Purulent phlebitis confirmed with a positive semiquantitative culture of a catheter tip, but with either negative or no blood culture is considered a CVS-VASC, not a BSI or an SST-SKIN or ST infection.•Occasionally a patient with both peripheral and central IV lines develops a primary bloodstream infection (LCBI) that can clearly be attributed to the peripheral line (e.g., pus at the insertion site and matching pathogen from pus and blood). In this situation, enter “Central Line = No” in the NHSN application. You should, however, include the patient’s central line days in the summary denominator count.Numerator Data: The Primary Bloodstream Infection (BSI) form (CDC 57.108) is used to collect and report each CLABSI that is identified during the month selected for surveillance. The Instructions for Completion of Primary Bloodstream Infection Form (Tables of Instructions, Tables 2 and 2a.) contains brief instructions for collection and entry of each data element on the form. The Primary BSI form includes patient demographic information and whether a central line was present, and, if so, the type of central line the patient had if appropriate to the location; these data will be used to calculate line-specific infection rates. Additional data include the specific criteria met for identifying the primary BSI, whether the patient died, the organisms isolated from blood cultures, and the organisms’ antimicrobial susceptibilities.REPORTING INSTRUCTION:•If no CLABSIs are identified during the month of surveillance, the Report No Events box must be checked on the appropriate denominator summary screen,e.g., Denominators for Intensive Care Unit (ICU)/Other locations (Not NICU orSCA), etc.Denominator Data: Device days and patient days are used for denominators (see Chapter 16, Key Terms). Device-day denominator data that are collected differ according to the location of the patients being monitored; however, they should be collected at the same time each day. When denominator data are available from electronic databases, these sources may be used as long as the counts are not substantially different (+/- 5%) from manually-collected counts, validated for a minimum of 3 months.For locations other than specialty care areas (SCAs) and NICUs, the number of patients with one or more central lines of any type is collected daily, at the same time each day, during the month and recorded on the Denominators for Intensive Care Unit (ICU)/Other Locations (Not NICU or Specialty Care Area (SCA)) (CDC 57.118). Only the totals for the month are entered into NHSN. When denominator data are available from electronic sources (e.g., central line days from electronic charting), these sources may be used as long as the counts are not substantially different (+/- 5%) from manually-collected counts, validated for a minimum of 3 months.For specialty care areas, the number of patients with one or more central lines is dichotomized into those with permanent central lines and those with temporary central lines on the Denominators for Specialty Care Area (CDC 57.117) form. Each is collected daily, at the same time each day. Only the total for the month are entered into NHSN. This distinction in lines is made because permanent lines are commonly used in patients frequenting these areas and may have lower rates of associated infection than central lines inserted for temporary use. If a patient has both a temporary and a permanent central line, count the day only as a temporary line day. The Instructions for Completion of Denominators for Intensive Care Unit (ICU)/Other Locations Form (Tables of Instructions, Table 6) and Instructions for Completion of Denominators for Specialty Care Areas (SCA)Form (Tables of Instructions, Table 7) contain brief instructions for collection and entry of each data element on the forms.In NICUs, the number of patients with central lines is stratified by birthweight in five categories since risk of BSI varies by birthweight. These data are collected on the Denominators for Neonatal Intensive Care Unit (NICU) (CDC 57.116) form.NOTE: The weight of the infant at the time of BSI is not used and should not be reported. For example, if a neonate weighs 1006 grams at birth but remains in the NICU for two months and has a body weight of 1650 grams when it develops a CLABSI, record the birthweight of 1006 grams on the BSI form. The Instructions for Completion of Denominators for Neonatal Intensive Care Unit (NICU) form (Tables of Instructions, Table 8) contains brief instructions for collection and entry of each data element on the forms.Data Analyses: The SIR is calculated by dividing the number of observed infections by the number of expected infections. The number of expected infections, in the context of statistical prediction, is calculated using CLABSI rates from a standard population during a baseline time period as reported in the NHSN Report.NOTE: The SIR will be calculated only if the number of expected HAIs (numExp) is ≥ 1.While the CLABSI SIR can be calculated for single locations, the measure also allows you to summarize your data across multiple locations, adjusting for differences in the incidence of infection among the location types. For example, you will be able to obtain one CLABSI SIR adjusting for all locations reported. Similarly, you can obtain one CLABSI SIR for all specialty care areas in your facility.The CLABSI rate per 1000 central line days is calculated by dividing the number of CLABSI by the number of central line days and multiplying the result by 1000. TheCentral Line Utilization Ratio is calculated by dividing the number of central line days by the number of patient days. These calculations will be performed separately for different types of ICUs, specialty care areas, and other locations in the institution. Separate rates and ratios will also be calculated for different types of catheters in specialty care areas and for birthweight categories in NICUs.1CDC Vital Signs. Making healthcare safer: reducing bloodstream infections. March 2011. Available at: /VitalSigns/HAI/index.html.2 O’Grady NP, Alexander M, Burns LA,, Dellinger EP, Garland J, Heard SO, Maki DG, et al. Guidelines for the prevention of intravascular catheter-related infections, 2011. Clinical Infectious Diseases 2011; 52(a):1087-99.3 Clinical and Laboratory Standards Institute (CLSI). Principles and Procedures for Blood Cultures; Approved Guideline. CLSI document M47-A (ISBN 1-56238-641-7). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania, USA, 2007.4 Baron EJ, Weinstein MP, Dunne Jr WM, Yagupsky P, Welch DF, and Wilson DM. Blood Cultures IV. ASM Press: Washington, DC; 2005.Appendix 1. Secondary Bloodstream Infection (BSI) GuideWhat is the meaning of the statement “not related to infection at another site” in relation to a positive blood culture?The purpose of using the CDC/NHSN infection criteria is to identify and consistently categorize infections that are healthcare-associated into major and specific infection sites or types. Several of the criteria include the caveat that signs, symptoms, and/or laboratory findings may not be related to infection at another site. When assessing positive blood cultures in particular, one must be sure that there is no other CDC-defined primary site of HAI that may have seeded the bloodstream secondarily; otherwise the bloodstream infection may be misclassified as a primary BSI or erroneously associated with the use of a central line, i.e., called a CLABSI.If the criteria for the primary infection site require a culture, then at least one organism cultured from that site must match an organism in the blood culture. NOTE: As of 1/1/11, antibiograms of the blood and site isolates do not have to match. In these instances and others where a culture of the involved site is not required for the criteria, and no such culture is collected, it is necessary to use clinical judgment regarding the likelihood of the organisms causing a secondary bloodstream infection. The graphic below may be used to help determine the relatedness of a primary site of infection to a positive blood culture. In addition, if the blood isolate by itself does not meet BSI criteria (e.g., only one positive blood culture of a common commensal), then that isolate may not be used to indicate the presence of a secondary BSI. For example, the patient has an HAI meeting criteria for symptomatic urinary tract infection due to E. coli and a single positive blood culture with E. coli and S. epidermidis, the SUTI should be reported as having a secondary bloodstream infection, but only E. coli should be listed as the infecting pathogen.。